
Abstract
In the context of the COVID-19 pandemic, gaining insights into how academia has responded to this urgent challenge is of great significance. This article presents academic response patterns at a global, regional and national level from an analysis of publication volume versus reported cases of COVID-19, scientific collaboration and research focus. We also compare academic activity associated with this newly emerging infection to that related to long-standing infections. Our results show that the research community has responded quickly to COVID-19. The highly developed countries, which have the highest number of confirmed cases, are also the major academic contributors. National-level analysis reveals diverse response patterns from different countries. Specifically, academic research in the United Kingdom remained at a relatively constant level throughout the whole year (2020), while the global share of China’s research output was prone to shift as its domestic pandemic status changed. Strong alliances have formed among countries with academic capabilities in response to the COVID-19 pandemic. The distribution of disciplines is relatively decentralised, indicating that a diverse and broad knowledge base contributes to the COVID-19 literature. Most of the analysed countries show dynamic patterns of research focus that vary over time as the pandemic evolves, except India. As one of the world’s biggest suppliers of vaccines, India makes consistent efforts on vaccine research, especially those related to pharmaceutical preparations. Our findings may serve as resources for fostering strategies to respond to future threats of pandemics.
1. Introduction
COVID-19 wreaked havoc across the world at the beginning of 2020, and has now become the most challenging health crisis since World War II [1]. Beyond its impacts in the health and medical fields, the crisis has had unprecedented economic impacts and has affected almost every aspect of society [2]. Rapid responses by governments, academia, businesses and citizens have been required to cope with this emergency. Among these, the rapid response from academia and global collaborations in terms of COVID-19 research have been essential to overcome the crisis. The urgent need to understand a new virus, develop treatment protocols, implement controls and recover socially and economically has greatly relied on intensive academic research. From this standpoint, a publishing boom on the subject of COVID-19 was to be expected. Analysing that boom now could yield insights into how academia has responded to COVID-19 from a global, regional and national perspective – insights that are especially valuable for policymakers.
Although every society is vulnerable to adverse events, a global shock such as COVID-19 often highlights how unequally distributed responsive capabilities can be among countries. Existing inequalities between countries on the economic, health and research capabilities are exacerbated. Moreover, these three aspects play vital roles in determining the impact of the crisis and the recovery times for a country [3]. Many studies have looked at the changing patterns of academic activity globally during times of crisis [4–8]. Now we need to understand academic responses and contributions from countries with varying levels of development and research capabilities, as this is the interface where urgent health needs meet science. The insights gained could facilitate public discussion and be beneficial to policymakers to improve scientific strategies towards solving the world’s stickier problems.
This study explores academic response patterns to COVID-19 on multiple levels – globally, regionally and nationally. Here, the regional-level analysis is conducted on the basis of categorising countries into different regions according to their development levels. This study uses the United Nation’s Human Development Index (HDI) to classify countries into different development levels, which is a summary measure of average achievement in key dimensions of human development for a country – a long and healthy life, knowledge and a decent standard of living [9]. For national-level analysis, we select the five most prolific countries of COVID-19 publications as representative examples to conduct a more fine-grained study, namely the United States, China, Italy, the United Kingdom and India. The widely varied situations of COVID-19 in these five countries provide more insights in interpreting the response pattern of each country at different phases of the pandemic.
A great number of studies have stated that the unprecedented outbreak of COVID-19 has been accompanied by a bulk of academic research that has challenged traditional patterns of scientific production [10–12]. However, understanding the specific features of these patterns is extremely difficult because they are shaped by many interacting social, economic and political factors. Therefore, in addition to the geographical analysis mentioned above, we have also chosen to analyse three effort-driven dimensions of the academic response – research effort versus reported cases, scientific collaboration and research focus.
The significant role of urgent health needs and global challenges in shaping academic research trajectories is fully illustrated in the large-scale concerted action of researchers and their quick responses to historical pandemics [7,13]. Several studies stand out as good examples and provide an international view on medical and multidisciplinary research efforts on pandemics, such as mapping the response to Zika [14,15], analysing severe acute respiratory syndrome (SARS) publication patterns [16,17] and the continuous stream of emerging studies on various forms of coronavirus [18–20], especially COVID-19 [8,21,22]. Notably, most studies on COVID-19 were published in the first half of 2020 [18,21,23–26]. However, it is virtually impossible to exhaustively explore academic response patterns in such a limited time window of publications. A longer-period of study is necessary to investigate academic response patterns from a dynamic perspective. Indeed, the pace of academic research into COVID-19 has been described as extraordinary, even when compared with the work that accompanied the SARS epidemic in 2002–2003 [27]. However, few studies have attempted to align daily reported cases with publication data to reveal the pace of research effort against the evolution of the disease, particularly in countries with different HDI levels and at different phases of the pandemic. Hence, the time-sensitive nature of this disease’s spread makes the co-evolution between reported cases and research effort one of the major focuses of this study.
Academic collaboration is the second prominent dimension through which we investigate how scholars worldwide collaborate to improve the scientific understanding of the pandemic. With the boom in information and communications technology, global networks have expanded and become increasingly interconnected [28]. This has brought new opportunities and efficiency gains to academia. When the global pandemic first hit, many scholars and practitioners called for wide and timely dissemination of relevant information [29,30]. Furthermore, consortia of research centres, university laboratories and hospitals in different parts of the world are making specific efforts to optimise scientific resources in response to the pandemic, such as the COVID-19 Clinical Research Coalition [31] (https://covid19crc.org/), RDA COVID-19 Working Group (https://www.rd-alliance.org/groups/rda-covid-19) and Single Cell Consortium for COVID-19 in China (SC4) [32]. According to Fry et al. [33], the geographic loci of coronavirus research generally, as well as the structure of academic teams, were shifted by the onset of COVID-19. Yet, although most studies on COVID-19 involve some collaborative analysis [6,7,22], little attention has been given to examining the collaboration patterns, particularly among countries at various HDI levels and during different stages of the pandemic’s spread. In a prior study on long-standing infectious and parasitic diseases (IPDs) that caused epidemics in undeveloped areas, scholars verified that collaborations between highly developed nations and those regions suffering most from IPDs are often intensive [34]. However, what we do not know is how countries at different HDI levels collaborate on a newly emerging infectious disease such as COVID-19.
Analysing the response pattern in terms of research focus is the third aspect of this study. It has been well recognised that the needs aroused by pandemics are not confined to biomedicine but rather widely affect society [35]. Some are in the realm of broader public health considerations, such as governance and infrastructure. Others involve engagement, communication and other aspects of social sciences [36]. Several studies have already examined the distribution of fields COVID-19 research has touched [7,26]. However, these have been macroscopic analyses, and there is room for a more fine-grained investigation of the various research foci – in particular, to understand how research focus changed in different phases of the pandemic. This study uses medical subject headings (MeSH) of publications to conduct an evolutionary analysis on research focus through 2020 by month. The details of acquiring MeSH terms of publications will be further explained in the ‘Data and Methodology’ section.
As mentioned, it is difficult to thoroughly capture the features of academic response patterns to the urgent needs caused by COVID-19. However, those patterns should become more visible when we compare recent research to the traditional academic responses to long-term infections – that is, the infections that have, for centuries, been the leading causes of death and disability [37,38]. Long-standing threats differ widely from emerging ones in terms of severity and impacts. Generally speaking, long-standing infectious diseases are those that have existed for a long time in human history. Such conditions do not constantly emerge as pandemics globally but are prevalent in specific geographical areas. In contrast, the emerging one, which refers to COVID-19 in this study, is a disease whose incidence has increased at an incredible speed. Moreover, such a disease spreads globally regardless of national or intercontinental boundaries [39]. These two types of infections also carry varying health burdens and social consequences and, so, might require different responses [40]. In this study, the scientific response pattern on COVID-19 is further interpreted through the comparison with that of long-standing infections.
In short, the major research questions to be answered in this study are as follows:
What are the evolutionary features of the COVID-19 confirmed cases/deaths versus publication volume: globally, by region with varying levels of development, and by country?
How have scholars from different countries of various development levels collaborated to improve the understanding of COVID-19? What are the features of collaborative relationships for countries at varying levels of development?
Which scientific fields have mainly produced and/or applied knowledge to address the needs raised by COVID-19? Are there differences in the research focus of countries at various development levels? How have research foci changed over time?
2. Data and methodology
Figure 1 depicts several important procedures used to conduct this research, including data acquisition and methods.
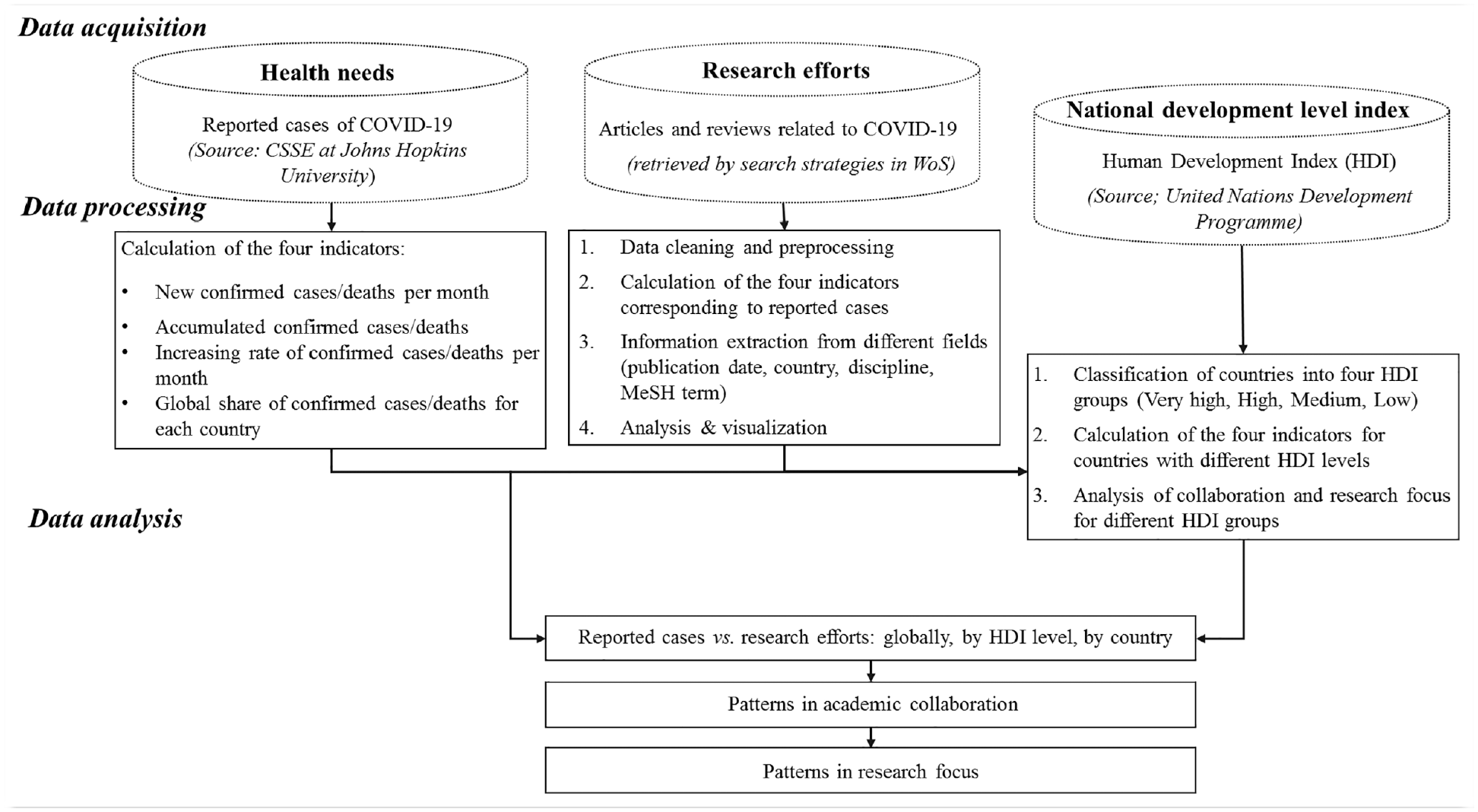
Research flow.
2.1. Reported cases
The COVID-19 outbreak has affected all aspects of society and all segments of the population. Its impacts and the urgent needs it has generated go far beyond health, stretching into human, economic and social crises. However, the most direct and intuitive quantitative index for reflecting the health needs caused by this pandemic is reported cases. Hence, we draw on real-time monitoring of confirmed cases and deaths to chart the spread of this infection. Open-source data on daily country-level statistics from the COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (https://github.com/CSSEGISandData/COVID-19) has been extensively used in COVID-19 related studies [41]. We use these data in this study also. Taking confirmed cases and deaths from 22 January 2020 to 31 December 2020, we further calculate the following four indicators globally, by HDI level, and nationally:
New confirmed cases/deaths per month
Accumulated confirmed cases/deaths
The increasing rate of confirmed cases/deaths per month
The global share of confirmed cases/deaths for each country
2.2. Scientific publications
Being the most common outlet for scholars to communicate, academic publications are used as the proxy for research efforts in this study [42]. For consistency with the study on long-standing infections [34], we collect articles and reviews related to COVID-19 published during 2020 from the Web of Science (WoS) Core Collection. The publication data were collected on 04 February 2021. Our search strategy is executed on the title and author keywords fields. It comprises the following terms: (‘2019-nCoV’ OR ‘SARS-CoV-2’ OR (‘COVID19’ OR ‘COVID-19’ OR ‘COVID-2019’) OR ((Coronavirus NEAR/0 2019) OR (‘Corona* Disease’NEAR/0 2019) OR (‘Corona* Virus’NEAR/0 2019) OR (‘Corona* Virus Disease’NEAR/0 2019)) OR ‘2019 Novel Coronavirus’ OR (‘Novel Coronavirus’ AND Pneumonia) OR ‘2019 Novel-COV’).
After removing duplicates, 42,943 publications are acquired as the dataset for this research. From this sample, we proceed to calculate our four indicators corresponding to confirmed cases/deaths. Publications are assigned to a country according to the institutional address of each author with the full counting approach. Hence, national publication counts reflect how many articles the country has contributed to. We count the number of publications for different human development groups directly on the aggregate level, instead of summing the number of publications for each country within a specific HDI level. For instance, since the United States and the United Kingdom are in the same HDI group, an article co-authored by researchers affiliated with institutions from these two countries can only be counted once for this HDI group. This approach can avoid the repetitive computation for publications collaborated by countries within the same HDI level.
In addition, many of the publication date fields in WoS are missing data, so we acquire these values through an alternative approach as follows:
If the article has a ‘publication date’ in WoS, we directly use it.
If the article does not have a ‘publication date’ but does have a PubMed ID, we match the article to PubMed and use the ‘Entrez Date’ in PubMed, which is the date the record was added to PubMed.
Publication dates for 38,049 articles are secured in this way.
We also extract MeSH terms from the publications for our research focus analysis. MeSH stands for Medical Subject Headings, which is a controlled vocabulary maintained by the US National Library of Medicine (NLM). The primary reason for using MeSH terms as subject terms rather than keywords provided by authors is that keywords are not standardised. It is common for authors to use different expressions for the same concept, and the bias this creates is problematic. Moreover, MeSH vocabulary contains terms not only in biomedicine but also in anthropology, sociology, agriculture and several other fields [43]. One of the major applications of MeSH terms is as labels for articles in PubMed (MEDLINE) to characterise the content of the articles [44].
To extract MeSH terms, we first use the article’s PubMed ID to match them to PubMed and, if MeSH terms are available, we copy them directly. For publications without a PubMed ID or where MeSH terms has not (yet) been assigned, we apply Medical Text Indexer (MTI) (https://ii.nlm.nih.gov/MTI/index.shtml) to extract the corresponding terms from the abstracts and titles of the articles. NLM uses MTI to pre-process MEDLINE citations that are then indexed by human indexing staff at the National Institute of Health (NIH). It is a tool that has been used for about 20 years and has steadily improved over time [45,46]. In total, MeSH terms for 38,049 publications are acquired from this process.
2.3. National development level index
The HDI was created by the United Nations Development Programme (UNDP) as a comprehensive measure to assess the development level of a country. Its unique point of difference is that it considers multiple aspects of a country rather than taking a purely economic stance [47]. The HDI is meant to be ‘a summary measure of average achievement in key dimensions of human development: a long and healthy life, being knowledgeable and having a decent standard of living’, which equals the geometric mean of normalised indices for each of the three dimensions. A country can fall into one of four groups according to its HDI value – very high, high, medium and low. HDIs for each country are updated every year. The latest HDI data and classification available from its official website (http://hdr.undp.org/en/content/download-data) is the HDI for 2019 (updated in 2020), which has been used in this study to explore the distinct response patterns from countries with different HDI levels.
3. Results and analysis
Following the above research flow, this section presents three parts of the analysis required to answer our research questions.
3.1. Publication volume versus confirmed cases/deaths
3.1.1. Overall
The global number of reported cases and publications relating to COVID-19 across the three different indicators are illustrated in Figure 2.

Confirmed cases/deaths versus publications from a global perspective. (a) New cases/publications per month, (b) accumulated cases/publications and (c) increasing rate of new cases/publications per month.
As expected, the number of confirmed cases/deaths and publications both increased substantially as the pandemic spread (Figure 2(a) and (b)). Interestingly, monthly increases in cases slowed down in March with the same pattern following for publications in April 2020, which may reflect a lag between the perception of need and publishing times (Figure 2(c)). Despite the fact that publishing in scholarly peer-reviewed journals usually entails long delays from submission to publication [48], a study of 11 medical journals in the first half of 2020 found that coronavirus articles were reviewed and published much faster than normal [49,50]. Such speedy publications are also reflected in the fast-growing publication volume. In general, consistent increases in the number of publications reflect academia’s quick response to public health needs.
3.1.2. By human development level
To gain deeper insights into how research communities in countries with varying degrees of development confront global public emergencies, we conduct a comparative analysis of confirmed cases versus publication volume for different HDI groups, as shown in Figure 3. As expected, the very high group, the one with the highest and constantly growing number of confirmed cases, has contributed most to the research on COVID-19, accounting for more than 70% of the world’s publications. Overall, the countries with the most cases (both cumulative and new) also publish the most; countries with the least cases publish the least. This observation is consistent with the significant positive correlation between the incidence of COVID-19 and HDI levels, as verified by Khazaei et al. [51] with data up to April 2020.

Confirmed cases versus publications – countries with different HDI levels. (a) Accumulated confirmed cases/publications and (b) new confirmed cases/publications per month.
For the high-development group, it is worth noting that their relatively high number of confirmed cases and publications in the first 2 months of 2020 correlates to the situation in China. As a country with a large number of confirmed cases in the initial period, China played a pivotal role in academic research on COVID-19 [7]. The evolution trend of the low-development group cannot be displayed clearly in Figure 3 due to the considerable differences in the number of confirmed cases and publications among the four groups. Specifically, the monthly number of publications from the low-level group shows an overall upward trend with a peak in September 2020. While the number of new confirmed cases per month fluctuated throughout the year, there were constant increases from March to June and steady decreases from June to November 2020.
Figuratively, the proportion of confirmed cases in the very-high- and high-development groups showed a ‘swapping’ pattern from January to March (Figure 4), which we attribute to the quick spread of COVID-19 in European countries and the United States in March 2020. It is also worth noting that the decline in the percentage of confirmed cases in the very-high group in April was not because the situation of COVID-19 was improving, but rather because of the spread of the pandemic to countries in the medium- and low-development groups. Of these, India is perhaps the most prominent country (with a medium HDI). The percentage of reported cases for the medium-development group peaked in September (35.29%), but its research effort was less than 9% on average. Another notable point is that although the high-development group accounted for 41.07% of global publications in January, an apparent downward trend in later periods can be seen, with a nadir of 22.17% in December.

The global share of confirmed cases/publications for different HDI groups.
In summary, our results reflect the diverse patterns of academic responses from countries within different human development groups to the urgent needs raised by COVID-19. In general, the levels of research efforts basically correspond with their degrees of needs in the four groups. The very-high- and low-development groups, especially, fit this pattern. Variations in both trends for the high- and medium-development groups were mainly driven by the pandemic’s status in that country – with China and India being stand-out examples in the two groups, respectively. One point worth emphasising is that countries in the very-high-development group had already conducted a great deal of relevant research when there was no large-scale outbreak in their local area. This is suggestive of their broader concerns over global issues. Such tendencies conform to observations from one previous study, where developed countries tended to pay attention to research that could extend its impact outside its borders [46].
3.1.3. By country
By the end of 2020, the United States topped 20 million cumulative confirmed cases, which accounted for nearly a quarter of the worldwide total [52]. India, Brazil and Russia follow in that order. Combined with the population data in 2020 from the World Bank [53], we calculate the ‘intensity’ of confirmed cases and further visualised its geographical distribution in Figure 5. Here, the ‘intensity’ of COVID-19 cases for a country equals the number of confirmed cases divided by the total population of that country. The United States and several less-populated countries in Europe (e.g. Andorra, Montenegro, Luxembourg) have the highest intensity of COVID-19, followed by countries in South America (e.g. Brazil, Argentina, Peru).

The intensity of COVID-19 (accumulative confirmed cases from 22 January 2020 to 31 December 2020).
Contrary to the prediction that Africa would suffer catastrophically in this crisis [54], Africa has accounted for a small number of coronavirus cases during the pandemic in 2020. Several scholars have stated that the limited testing capacity, poor reporting systems and inadequate health systems are the main reasons of Africa’s low number of reported cases [55,56]. However, some scholars argued that long history of experience with infectious diseases, early government community-wide actions and population distribution are also crucial factors to the low African case count [57]. More specifically, Lawal [58] found that the lower population mean age, lower pre-COVID-19 era ‘65yr+ mortality rate’, and smaller pool of people living with cardiovascular diseases explain Africa’s lower COVID-19 mortality rate.
In terms of scientific effort, the United States played the most prominent role in conducting research, followed by China, Italy, the United Kingdom and India. We analyse the five countries producing the most publications to gain further insights into how specific countries respond to the pandemic. Figure 6 depicts the number of confirmed cases/publications (Figure 6(a)) and the global share of those indicators (Figure 6(b)) for the five countries.
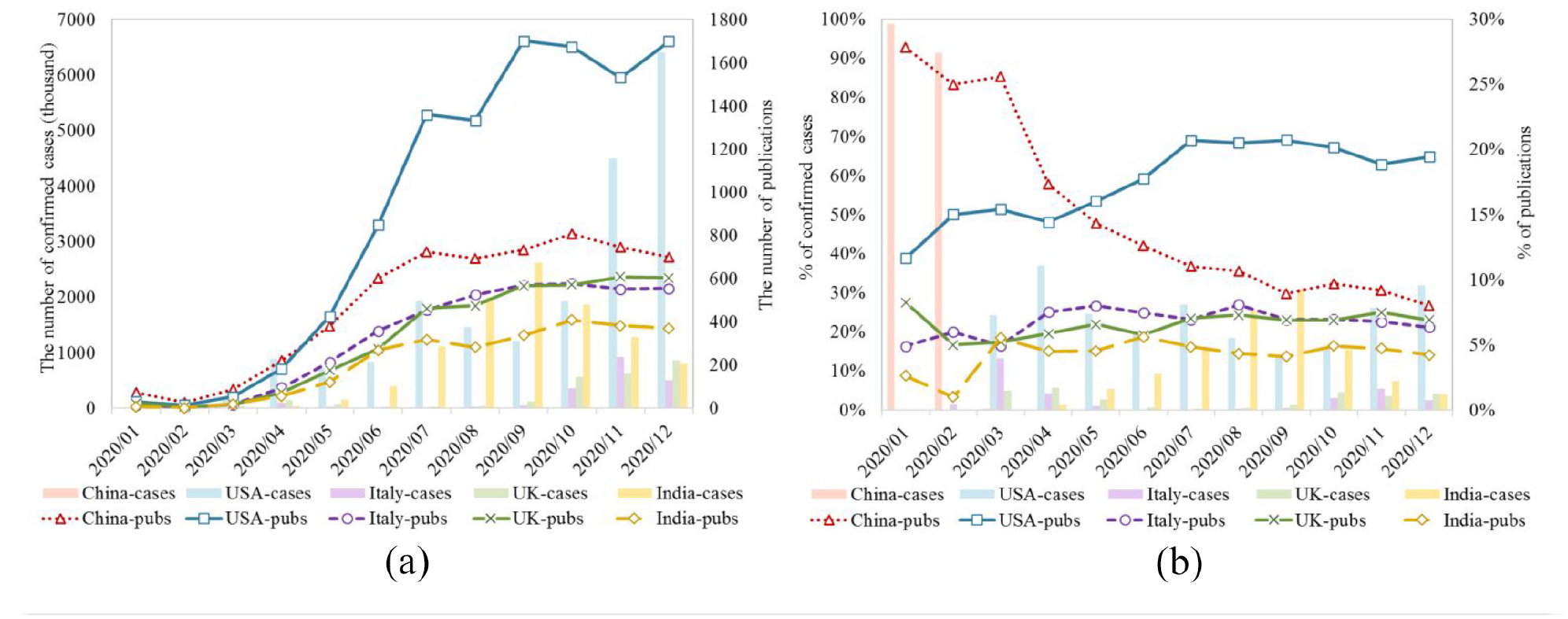
Confirmed cases versus publications for the five highest research-producing countries. (a) The number of confirmed cases/publications and (b) the global share of confirmed cases/publications.
As shown in Figure 6(a), the number of confirmed cases fluctuated greatly as the pandemic spread through the different countries. In particular, India showed astonishing growth in the case counts from June to September, while Italy and the United Kingdom (along with some other countries in Europe) faced a second wave starting from October. Despite the ups and downs of the pandemic, the academic outputs of all countries have been steadily increasing, albeit to varying degrees, with the exception of a minor drop in the latter 3 months of 2020.
The percentage of global confirmed cases/publications further reflects the dynamic of ‘relative’ health needs and research effort for the five countries (Figure 6(b)). In the early phases of the pandemic, China had the most significant global share of both confirmed cases and publications, as expected, reflecting a rapid response by Chinese academia. However, the relative research interest of Chinese scholars declined as China gained control of its outbreak. This result is in line with the findings of a recent study that confirmed the ‘sensibility’ of academic responses to the SARS epidemic in China [7]. Another point worth mentioning is the relative consistency of contributions from Italy and the United Kingdom, which appear to be less subject to the situation on the ground in their respective nations than China’s research effort. As for the United States, the proportion of confirmed cases remained relatively steady, while its proportion of publication rose dramatically from April to July. India, who was largely affected by a worsening epidemic starting in the third quarter of 2020, was also extensively involved in COVID-19 research.
The Pearson correlation coefficient (r) is applied to assess the relationship between scientific outputs of each country with its domestic and global pandemic status. The findings of correlation analysis are shown in Tables 1 and 2, where coefficient values (ranging from −1 to +1) denote the strength of linear association between the targeted two variables [59]. As Table 1 shows, only the percentage of publications from China has a significant positive correlation with its proportion of confirmed cases (r = 0.744), which implies that, during the crisis, China’s research effort tends to shift as its domestic pandemic status changed. More precisely, this result mathematically confirms the ‘sensibility’ of Chinese academia’s response pattern discussed before. In addition, the non-significant negative correlation coefficients for Italy and the United Kingdom can help explain, to some extent, their lower vulnerability of local epidemics and relative consistency of contributions throughout 2020.
Pearson correlation coefficients (r) between percentage of publications and percentage of confirmed cases for each country.

At 0.001 significance level; **at 0.01 significance level; *at 0.05 significance level.
Pearson correlation coefficients (r) between confirmed cases worldwide and publications of each country.

At 0.001 significance level; **at 0.01 significance level; *at 0.05 significance level.
Table 2 illustrates the correlation results of confirmed case counts worldwide with the number of publications worldwide and in different countries. Significant positive correlation coefficients between publication volume and confirmed cases are observed for all five countries. China has the lowest correlation coefficient (r = 0.793), indicating that it is less ‘sensitive’ to global pandemics compared with other countries. In addition, the correlation coefficient between the United Kingdom’s publication volume and confirmed cases worldwide (r = 0.896) is even higher than that between global publications and cases (r = 0.884). Combined with the findings in Table 1, this analysis reveals the high ‘consistency’ between UK academia’s response with the global pandemic status.
3.2. Patterns in academic collaboration
The major question to be answered in this section is whether and which academic communities in different countries have conducted collaborative research during the crisis. This section analyses the number of joint publications and the strength of collaborations, and presents the findings at three levels: globally, by human development level, and by country. Note that Salton's measure [60] is used to calculate the strength of collaborations (collaboration intensity), which is defined as the number of joint publications divided by the square root of the product of the two countries’ total publications (i.e. the geometric mean).
3.2.1. Overall
Among the 185 countries that produced research on COVID-19 in 2020, 45 contributed to more than 200 publications each. We choose these as representatives to build an international collaboration network, as shown in Figure 7.

International collaborations.
China, the United States and the United Kingdom play pivotal roles in this network, collaborating closely not just with one another, but also with a number of other countries. Although China and the United States produced the most joint publications, the most intensive collaborations were observed among European countries, especially between Belgium and the Netherlands. China’s position in the network is prominent – more prominent than findings from a previous study in a similar network mapping collaborations on long-standing diseases [34]. Fewer than 10 countries from Africa and the Middle East published more than 200 articles. Here, Egypt and Saudi Arabia are the closest allies. With fewer academic outputs and reported cases, underdeveloped regions exhibit lower levels of engagement in joint COVID-19 research. This is in contrast to their relatively high levels of involvement in research associated with diseases carrying a high local burden [34].
3.2.2. By human development level
For this analysis, we divide 2020 into four quarters and explore how collaborative relationships changed over the course of the year. The number of collaborative publications and the strength of collaboration are calculated for six ‘collaboration pairs’ established by four HDI groups, as shown in Figure 8. In general, the number of publications experienced dramatic increases from the first quarter to the fourth, but there was no discernible change in the overall strength of collaboration for various pairs. With the most collaborative publications, it is pretty apparent that the partnership between very high and high groups was the strongest. This is largely attributed to the joint studies conducted between the United States (very high) and China (high). Moreover, due to the extensive collaboration between India and several developed countries (e.g. the United States and the United Kingdom), the very-high- and medium-development groups also have a relatively close relationship.
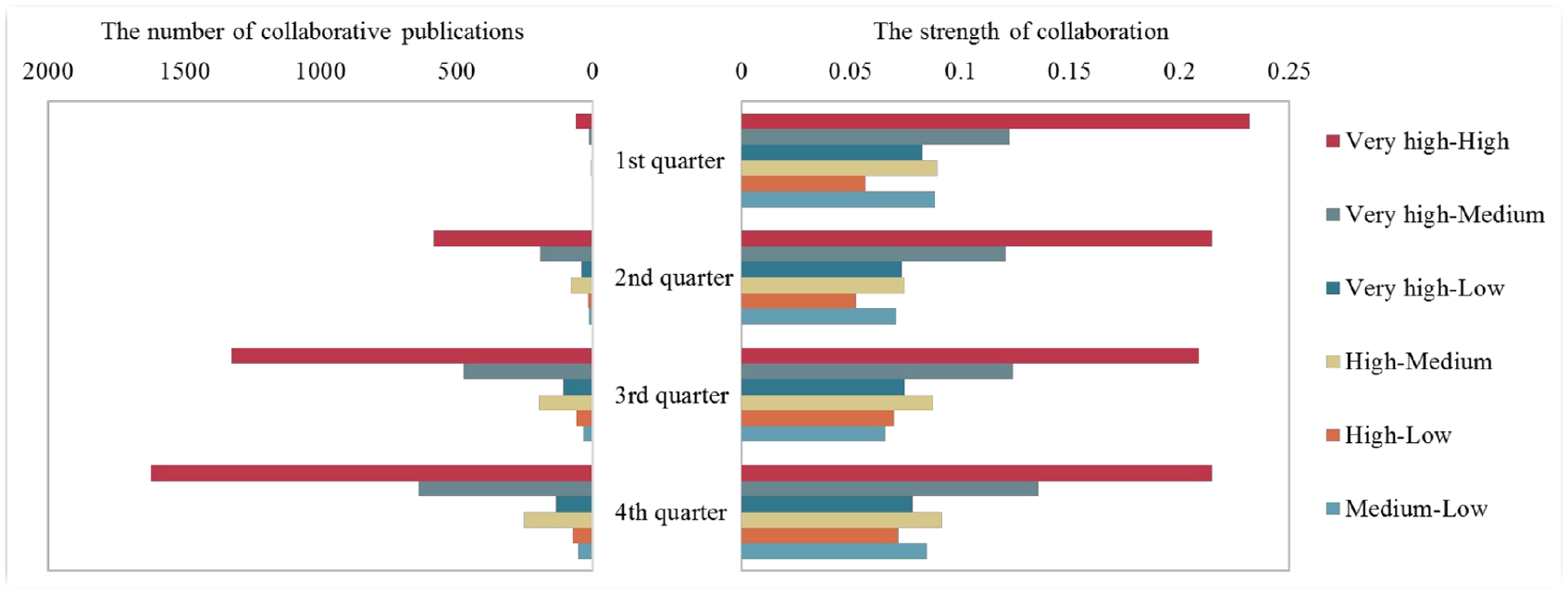
Collaborations by HDI level over the course of 2020.
The weakest collaborations were seen, on average, between the high and low groups. The partnership between very high and low groups was also relatively weak, which runs counter to the findings for long-standing diseases [34]. What we find is that the pair of very high–high groups is the most stable and has the strongest relationship to address the urgent health needs created by a global pandemic. As expected, alliances among countries with scientific research capabilities would more probably produce high-quality academic outputs and to do so more efficiently.
Due to the prediction of COVID-19’s catastrophic impacts in Africa that have not yet materialised, this continent and its related underdeveloped countries have attracted tremendous attention in this crisis [57,58,61]. Our study is no exception. Although underdeveloped countries play limited roles in the global collaboration network, the way they conduct international collaborations is worth investigating more. Figure 9 depicts a more detailed collaboration network for the top five countries (countries with asterisk (*) in Figure 9, that is, Nigeria, Sudan, Uganda, Congo (Democratic Republic of Congo (DRC)) and Ethiopia) in the low-development group by the number of publications.
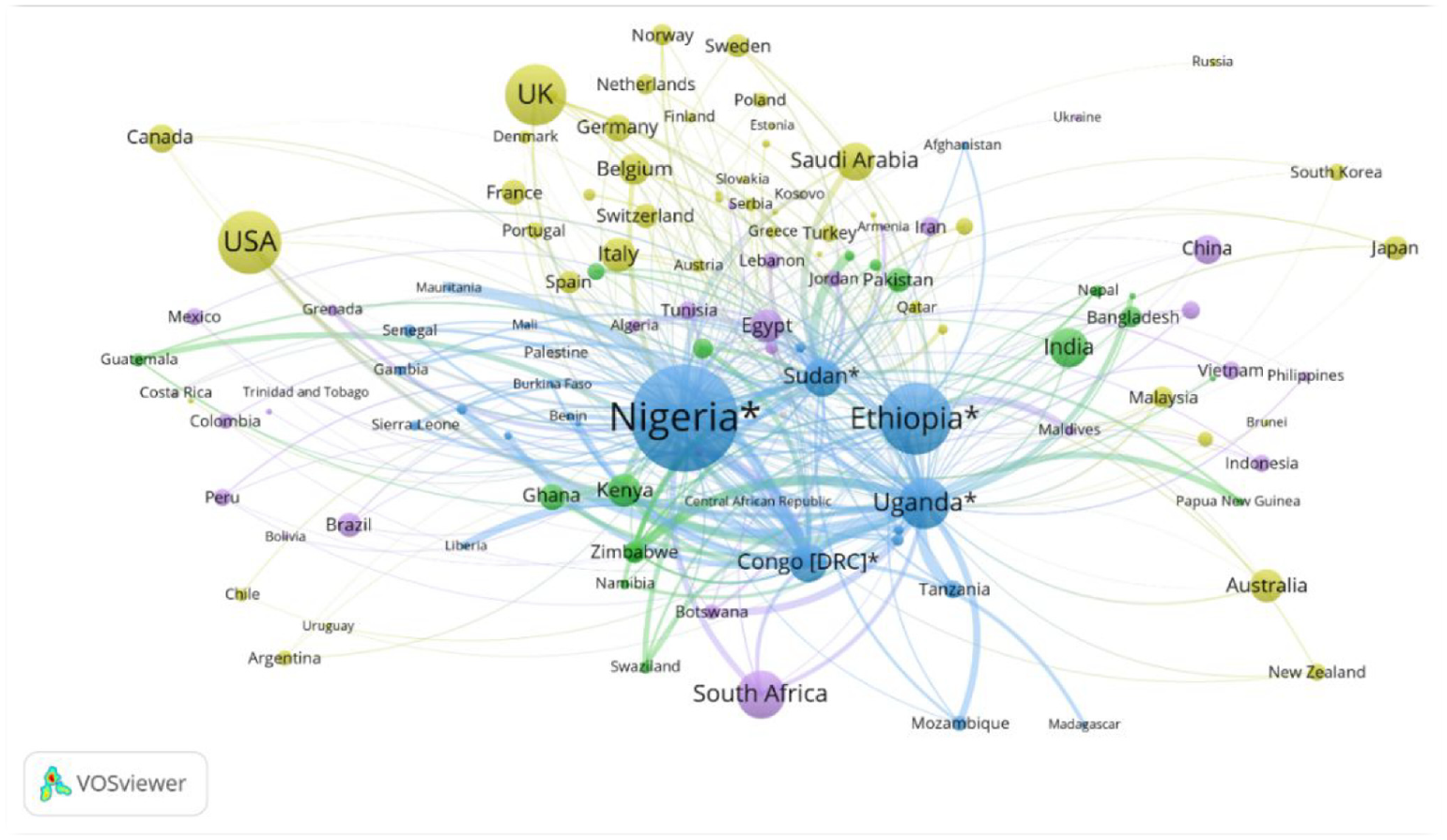
Collaboration networks of the five most prolific low-level (HDI) countries.
As Figure 9 shows, these five low-level countries have relatively extensive international collaborations with more than 120 other countries. Due to their low volume of collaborative publications (small size of the nodes) or proximity to other nations, certain countries’ names are not featured in Figure 9. In general, these five countries collaborate closely with each other and have intensive collaboration with countries in low and medium groups, such as Tanzania (low), Kenya (medium), Ghana (medium) and so on. South Africa stands out in the high-development group as a country that has collaborated closely with all five countries in terms of the number of collaborative publications and collaboration strength, particularly with Nigeria. It is worth noting that the African countries mentioned above (Nigeria, Sudan, Uganda, Congo (DRC), Ethiopia, Tanzania, Kenya, Ghana and South Africa) are among the 30 countries that have institutions as the founding members of the COVID-19 Clinical Research Coalition. This research coalition was founded in the early days of the COVID-19 pandemic with the goal of accelerating COVID-19 clinical research in resource-limited regions and ensuring that people in such areas benefit from scientific achievements [31]. A more in-depth investigation on the publication data shows that several coalition’s founding members from African countries had published a relatively high proportion of articles in the low HDI group. Makerere University of Uganda, for example, one of the coalition’s founding members, has the most publications in Uganda and the second-highest number of publications in the low HDI group. More than 80% of Makerere University’s publications are in collaboration with research institutions from 57 countries. To some degree, this finding is suggestive of the crucial role played by research consortia (e.g. the COVID-19 Clinical Research Coalition) in pooling research and development resources to tackle emerging threats.
The intensity of the five countries’ collaboration with the very-high-development group is relatively low, which, theoretically, is primarily due to the very-high group’s large number of publications. Yet, the number of publications co-produced by the five countries and highly developed ones is higher than those co-produced by the five countries with high- or medium-level ones.
3.2.3. By country
We again section off the top five most prolific countries overall – the United States, China, India, the United Kingdom and Italy – to provide more fine-grained insights into the collaboration patterns of COVID-19’s major scientific contributors. Among these five countries, three are in the very high HDI group (the United States, the United Kingdom and Italy). China is high and India is medium.
The collaboration networks for each of the five countries, provided in Appendix 1, reveal that countries in the very-high-development group are core collaborators for all the five countries. More specifically, the top 10 strongest collaborators to Italy and the United Kingdom are all in the very-high group. For the United States, China is the only one among its top 10 strongest collaborators outside the very-high group. In the top 10 list of China, Pakistan is in the medium group but the other nine are from very-high group. Only India breaks from this pattern – the high and medium groups occupy a relatively vital position in its network. From a geographical point of view, scholars in India work more closely with their neighbours Saudi Arabia (very high) and Nepal (high) than with those in the United States and United Kingdom. Still, seven of India’s top 10 partners are in the very-high group. Furthermore, no significant changes in academic collaboration patterns for the five countries have been observed across the four quarters.
3.3. Patterns in research focus
The needs posed by a global-level pandemic concern more than just biological issues. Social, political and economic issues also come to the fore, all of which require a broader interpretation of relevant knowledge to address. To provide insights into which fields of knowledge are most relevant in responding to the COVID-19 pandemic, we map the disciplinary distribution of the publications in the sample in terms of WoS subject categories (WCs). Furthermore, we also combine this analysis with the geographic distributions to explore how the four HDI groups’ research focus has shifted over time. In a more fine-grained analysis of our top five countries, we also extracted MeSH terms from the publications and mapped research focus month by month.
3.3.1. By discipline
Using VOSViewer [62] and following the studies by Rafols et al. [63] and Carley et al. [64], we generate science overlay maps to illustrate the research fields most relevant to COVID-19, as shown in Figure 10. Obviously, ‘Infectious Diseases’ and ‘Clinical Medicine’ are the two most concentrated areas of research. A non-negligible share of articles can be found outside the core of the life sciences, such as in ‘Psychology’, ‘Social Science’, ‘Management’ and ‘Environmental Science’, reflecting a broader concern for the pandemic by academia.
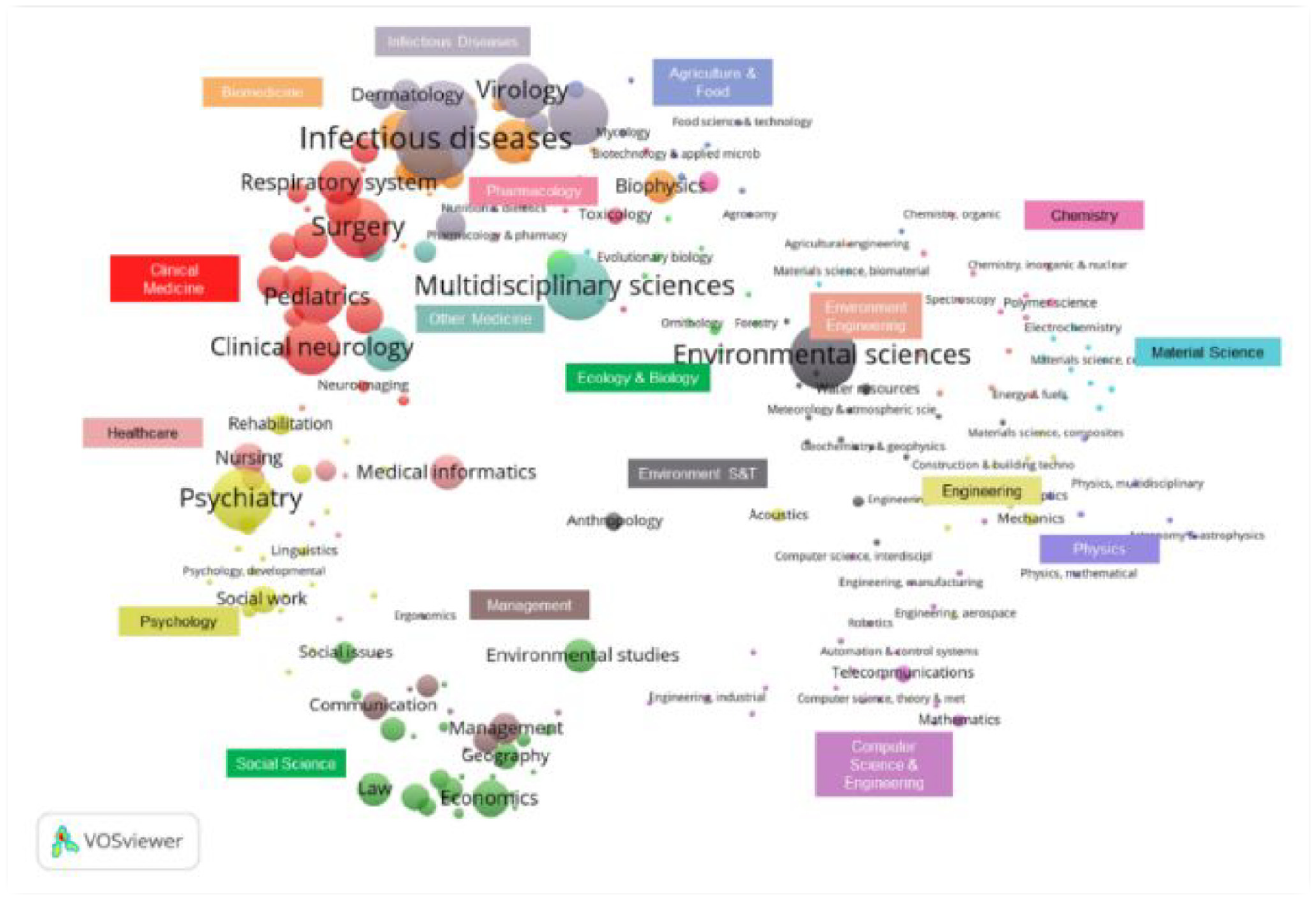
The science overlay map of publications on COVID-19.
To understand which fields were producing knowledge at different stages of the spread, we again divided the year into quarters and analysed the top 10 disciplines in each quarter for the different HDI groups, as shown in Figure 11. Here, the number of disciplines shown in Figure 11 for each HDI group differs, because they are identified according to the ‘union set’ of the top 10 disciplines in four quarters for the targeted group. In general, ‘Medicine, General & Internal’ has the most publications. In fact, several journals with a large volume of publications, including Cureus and Journal of Clinical Medicine, as well as some of the most prestigious journals, such as the Lancet and The New England Journal of Medicine, fall into this category. To some extent, containing journals with large publication volume and high reputation might partly explain the large share of articles in ‘Medicine, General & Internal’. A clear trend in all four HDI groups is that the research fields of interest were more evenly distributed in the later periods of 2020. Thus, knowledge production was broadening and diversifying in response to this emergent disease.

Top 10 disciplines by number of publications for each HDI level over 2020.
In the first quarter, research in ‘Microbiology’, ‘Medicine, General & Internal’, ‘Immunology’ and ‘Infectious Diseases’ accounted for almost half of all publications in the very-high-development group. However, the proportion of publications in the four fields dropped dramatically in the following quarters. This reveals waning attention to studies at the microbial level, such as those pertaining to virus morphology and structure, as the understanding of the virus deepened through massive research in the initial stage. Another notable point is the increasing attention on ‘Surgery’ in the second and third quarters. With a more detailed inspection of the publication data, studies on ‘Surgery’ are highly connected with several other disciplines, such as ‘Cardiac & Cardiovascular Systems’ and ‘Clinical Neurology’. With a steadily increasing number of confirmed cases at this stage, scholars from these highly developed countries paid incremental attention to clinical studies of different pre-existing diseases that may complicate and cause more severe cases of COVID-19. Furthermore, the continuously growing proportion of ‘Psychiatry’ research also indicates concerns over public mental health.
Studies on ‘Mathematical & Computational Biology’ drew a certain level of attention from the high-development group in the initial stages of the pandemic. Here the focus was on using mathematical models to analyse the dynamics of the pandemic in China [65–67]. This tendency can also be observed in the disciplinary distribution of China in Appendix 2. Publications in the first quarter from the high group were mainly produced by Chinese scholars. However, once China took control of the pandemic in later periods, scholars paid less attention to research in mathematical fields and incrementally more effort to ‘Environmental Sciences’, ‘Virology’, ‘Psychiatry’ and ‘Pharmacology Pharmacy’. It is worth noting that ‘Chemistry, Medicinal’ and ‘Medicine, Research & Experimental’ are highly associated with pharmacological studies, indicating an inclination towards vaccine-related studies in the third and fourth quarters.
Both the medium- and low-development groups produced fewer publications on COVID-19 than the very-high and high groups. Hence, the variation tendencies of discipline proportion for these two groups would more probably present some ‘unusual’ features. For instance, the extremely high proportion of publications in ‘Gastroenterology & Hepatology’ for the medium-development group in the first quarter actually results from publications of Indian scholars. Such a pattern can also be observed in the disciplinary distribution of India in Appendix 2. Those articles mainly discussed techniques and practice of gastrointestinal endoscopy during the COVID-19 pandemic, since the aerosol-generating nature of procedures and the presence of virus particles in stool samples of infected persons may lead to the transmission of virus [68–70]. For the low group, the high concern in the field of public health is the most apparent feature.
3.3.2. By MeSH term
To capture the changes in research focus in greater detail, we chart the 20 most frequently used MeSH terms for publications generated by each of the five countries by month in 2020. Note that we delete MeSH terms without practical meaning or those that do not indicate an actual research focus, such as COVID-19, SARS-Cov-2, pandemic, human and so on. The results are given in Appendix 3, in which each colour represents a specific MeSH term, and the thickness of each ‘river graph line’ in different colours observed in the vertical direction indicates the frequency of each MeSH term.
As implied by the high-frequency term ‘China’ for all five countries, the outbreak in China in the first 3 months of the pandemic attracted considerable attention from the global academic community. Later, international articles published by those five countries tended to place more emphasis on COVID-19-related issues in their own countries. All five countries also shared a high level of concern for studies in epidemic control (‘Communicable Disease Control’) and public health, which are critical topics to the pandemic. Yet, the research focus for each country also shows diverse trajectories as the domestic status of the pandemic changed.
In China, terms such as ‘COVID-19 testing’, ‘cough’, ‘fever’, ‘tomography’ and ‘quarantine’ frequently appeared in the first 3 months, reflecting the academic response to an unknown disease in its early stages. This was academia attempting to understand disease symptoms, develop diagnostic techniques and enforce isolation and quarantine protocols. As the spread was gradually brought under control, studies on pathogenic mechanisms, possible treatments (‘antiviral agent’, ‘antibodies’) and related comorbidities (‘comorbidity’) started to receive more attention. ‘Angiotensin-converting enzyme 2’ (ACE-2) was identified as the receptor for SARS-CoV-2’s viral entry in a study published by Nature in February 2020 [71]. This was subsequently a topic of great interest to Chinese scholars, especially from April to August. The most apparent focus change in the later periods was the increasing attention given to mental health, which can be seen from the high frequency of ‘anxiety’ and ‘mental health’. Moreover, the remarkable rise in the rank of ‘vaccine’ conforms to the previous discussion on the incremental proportion of publications in chemistry-related fields, and demonstrates an emphasis on COVID-19 vaccine research and development.
In general, studies from the United States and China share a high similarity, with 14 out of 20 MeSH terms on the high-frequency list being identical. Related comorbidities (‘comorbidity’), pathogenic mechanisms (angiotensin-converting enzyme 2) and vaccine-related topics were major concerns for both China and the United States. Digging deeper into the data, the comorbidities of concern between the two countries are also highly similar. These include diabetes, hypertension and cardiovascular disease. Nevertheless, some differences in the research focus between the two countries can also be observed. For instance, continuously increasing attention on ‘COVID-19 testing’ reflects a high demand for testing technology due to the worsening situation of the pandemic in later periods. Another marked difference between the United States and China is the emphasis on the accessibility of healthcare by US academia, as implied by the high frequency of ‘telemedicine’ and ‘delivery of health care’. The United States, as a country with just 4% of the world’s population, has a quarter of the world’s confirmed COVID-19 cases and deaths [72]. Extensive studies on issues related to healthcare and telehealth reveal concerns for the underlying problems in their healthcare system and its failure to address such urgent health needs [73]. In addition, a substantial rise in the rank of ‘physical distancing’ in December and its high co-occurrence with ‘mental health’ illustrate the risk and impact of long-term social isolation [74–76].
In terms of the two European countries, Italy and the United Kingdom, they actually share a high level of similarities in both research focus and pandemic status. Notably, extensive research on mental health was undertaken in Italy and the United Kingdom from as early as March and April, reflecting their early attention to this issue. Starting from June, there was a substantial drop in the ranking of ‘personal protective equipment’ for both countries, which indicates a lessening demand for supplies to prevent the spread of infection and perhaps a matured adaptation process to COVID-19. Similar to the other countries, scholars in Italy and the United Kingdom had great concerns for ‘COVID-19 testing’, especially in the fourth quarter of 2020, which was their peak period of viral transmission. In terms of differences between the two countries, Italy had a remarkable rise in the ranking of ‘emergency service’ in the fourth quarter – the quarter with the highest number of confirmed cases. In the United Kingdom, terms such as ‘government’ and ‘policy’ yield clues into a higher emphasis on research related to government functions and management of the pandemic. In addition, vaccine-related studies were also given close attention by the UK academia from August to November. However, such studies gave way to research on public health and government functions in December, which could be related to the high intensity of the outbreak and accompanying demands on effective governance and control.
As a medium-HDI country, India presents a quite distinct pattern in research focus. The most notable feature is their extreme high concern over vaccine-related studies, which commenced in May 2020. A series of terms relevant to vaccine and possible drug treatments can be clearly found from the high-frequency terms of India, such as ‘vaccine’, ‘pharmaceutical preparations’, ‘molecular dynamics simulation’, ‘molecular docking simulation’, ‘COVID-19 drug treatment’ and ‘drug repositioning’. Molecular dynamics simulation is a mature technique to understand macromolecular structure-to-function relationships [77]. This is utilised to reveal immune targets on the SARS-CoV-2 spike protein and further propose novel strategies for vaccine development [78]. Molecular docking simulation, correspondingly, can be used to model the interaction between a small molecule and a protein at the atomic level, which is an essential tool for drug discovery. India, as one of the world’s largest suppliers of vaccines [79], has devoted a massive effort to vaccine research and development throughout the pandemic. Strikingly, ‘global health’ also appeared frequently in studies from India, which is not observed in other countries’ research. As a matter of fact, among all the publications involving the term of ‘global health’, 71.1% were solely conducted by Indian researchers. Furthermore, ‘global health’ often co-occurred with ‘WHO’, ‘China’ and ‘vaccines’.
Together, the similarities and differences show a dynamically changing research focus for all five countries with the exception of India, which has consistently devoted most of its efforts towards vaccine research. Indeed, as one of the most effective strategies to prevent infections such as COVID-19, vaccines have attracted considerable scientific attention in most countries, especially in the later period. To further investigate the geographical and disciplinary distribution of vaccine-related research, we conduct a detailed search of publications using MeSH terms ‘vaccine’. Similarly, the five countries analysed above are also the top five countries with the highest number of vaccine-related publications. The differences are that India is the second-largest contributor for vaccine research (with only eight fewer publications than the United States), whereas Italy has the least quantity of vaccine research in the five countries. Italy is also the only country that does not include the term ‘vaccine’ in its Top 20 MeSH terms.
Figure 12 illustrates the publications’ proportion of five countries in 10 disciplines with the most vaccine-related publications. The radial lines represent the proportion of articles from each country on the listed disciplines. For example, more than 33% of publications in ‘Biophysics’ were contributed by India. Obviously, as the world’s leading vaccine manufacture, India presents a unique pattern in comparison to other countries. Specifically, the lion’s share of outputs in ‘Biochemistry & Molecular Biology’, ‘Biophysics’ and ‘Biotechnology & Applied Microbiology’ were generated by Indian researchers. In fact, the majority of publications in ‘Biophysics’ also belong to ‘Biochemistry & Molecular Biology’, as these two disciplines are closely related. The journal named Journal of Biomolecular Structure and Dynamics falls into these two categories and is the major source of these publications from India. Understanding the biophysical and biochemical characteristics of SARS-CoV-2, including cytokine storms, receptor binding, protein structural and functional features, molecular interactions and so on is the prerequisite for developing and manufacturing effective vaccines [80]. In addition, biotechnology is the technological application of biological organisms, systems and processes to develop products for specific uses, one of which major applications is the synthesis of peptides to be used as vaccines [81]. With India’s relatively high proportion of ‘Pharmacology & Pharmacy’ research, such a pattern partly reflects India’s emphasis on pharmaceutical preparations of vaccines. While academia in the United States is the most significant contributor to publications in the fields of ‘Immunology’, ‘Medicine, General & Internal’ and ‘Medicine, Research & Experimental’. Cureus and Vaccines, in particular, are the two journals with the most vaccine-related articles from the United States. Cureus is classified in ‘Medicine, General & Internal’, whereas Vaccines is in ‘Immunology’ and ‘Medicine, Research & Experimental’. In comparison to India’s research focus, studies from the United States appear to concentrate more on fundamental research and experiment of vaccines. China, the United Kingdom and Italy also have different fields of interest in vaccine research.

The proportion of publications by five countries for the 10 disciplines with the highest number of vaccine-related publications.
4. Conclusion and discussion
The recent global health emergency that COVID-19 represented has revealed just how destructive outbreaks can be to our lives. Intending to understand how academia globally and in countries with varying levels of development respond to such urgent health needs, we investigated academic response patterns in terms of research effort, collaborations and research focus. The summary and discussion of our findings are as follows.
4.1. Summary
The significant and constant growth in the number of publications on COVID-19 reflects a quick and intense reaction from academia globally. This is consistent with previous observations on several other health emergencies [7]. For the four groups of countries with varying levels of development, the group with the highest number of confirmed cases/deaths – the very-high-development group – has the largest publication volume. The low-development group, on the contrary, has the lowest number of confirmed cases/deaths and the lowest publication volume. One point worth emphasising is that countries in the very-high-development group had already conducted a great deal of relevant research while there were no large-scale outbreaks in their local areas. The patterns of high- and medium-development groups are mainly influenced by the scientific performance and the pandemic’s status in specific countries with large populations and publications, such as China (high) and India (medium).
The United States, China, India, the United Kingdom and Italy are the five countries that have made the most significant academic contribution to COVID-19. Despite the steady growth of academic outputs for all countries, distinct response patterns can still be observed from the proportion of global research outputs for each country. Specifically, academic research in the United Kingdom remained at a relatively constant level throughout the whole year (2020), which, to some extent, implies the ‘consistency’ between UK academia’s response with the global pandemic status. However, the global share of China’s research output was prone to shift as its domestic pandemic status changed.
Academic collaboration is our next point of analysis. The United States, China and several European countries play the most prominent roles in the global collaboration network through massive joint efforts among themselves and with other countries. According to the value of collaboration strength, we found the most intense collaborations between the very-high- and high-development groups, and the weakest between the high and low groups. The collaboration patterns show that strong alliances among countries with solid research capabilities are preferred to respond to emerging outbreaks. This tendency can be further observed from the top five countries’ core partners, most of which are highly developed nations. On one hand, the pattern of ‘strong alliances’ differs from that seen in long-standing infections, in which countries in the very-high-development group and undeveloped regions with high disease burdens form the closest partnership [34]. On the other hand, when the transmission areas of long-standing infections and COVID-19 are considered, the inclination of the very-high-development group to collaborate with regions with greater health needs could be regarded as a resemblance. In addition, the low inclination of the high-development group to collaborate with the underdeveloped areas, and the close collaborations within countries in the low-development group are the other two similarities between the collaboration patterns of emerging infections and long-standing ones.
In terms of research fields, biomedicine has contributed most to our understanding of the fast-developing COVID-19 situation. ‘Infectious Diseases’ and ‘Clinical Medicine’ are the two most concentrated research areas. Nevertheless, the distribution of disciplines is relatively decentralised across the health and social sciences. As time passed, knowledge production broadened and diversified in response to this emergent disease. A more detailed exploration of MeSH terms further demonstrates the shifts in research focus over time as the pandemic evolved for most nations – India being a notable exception. For instance, most countries focused on virus morphology and structure in the early stages of the pandemic, switching their interest to mental health and vaccine research in the later period. However, as one of the world’s major suppliers of vaccines, India has devoted a massive effort to vaccine research. In particular, it is also interesting that India seems to concentrate more on pharmaceutical preparations of vaccines, while the United States places more emphasis on research and experiment of vaccines.
4.2. Limitations and future research
This study contains several limitations that need to be addressed. With the aim of contributing a systematic analysis of the current biomedical research portfolio, we used academic publications as the object to represent the research effort on diseases. However, there are many other proxies for research effort, including grants, patents, clinical trials and so on, which could also be used to investigate response patterns for different sectors of the academic community. Moreover, to be regarded as a comparable study with the previous research of long-standing infectious diseases, we drew the publication corpus from WoS. This may mean that some relevant publications indexed in other scholarly databases were overlooked. Furthermore, although the indexing of Online First articles in WoS have reduced indexing delays, certain COVID-19 articles published in 2020 may have been missed since we retrieved data in early 2021. Another possible limitation is using the MeSH vocabulary as the basic corpus to reveal research focus, which is biased towards biomedical topics. Although MeSH indexes terms in diverse fields, it is primarily a medical vocabulary, which some content particular to social science will have inevitably been neglected.
Researchers wishing to expand upon this research might look to multi-dimensional objects and indexes to provide an in-depth analysis of how different sectors in academia respond to emergencies. Furthermore, publications or even preprints from diverse platforms could also be included for a more comprehensive study on the academic response. In addition, a more precise and sophisticated topic model could be applied to investigate research focus.
Footnotes
Appendix 1
Appendix 2
Appendix 3
Acknowledgements
The authors would like to acknowledge support from the National Laboratory Center for Library and Information Science in Wuhan University.
Author contributions
W.Z., L.Z. and L.W. contributed to the conception of the work. W.Z. and J.W. participated in data screening, extraction and quality assessment. W.Z. analysed the data and drafted the manuscript. L.Z. and L.W. provided critical comments and contributed to the interpretation of analysed results. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This article was financially supported by National Natural Science Foundation of China (Grant Nos. 71573085, 71974150).