
Abstract
This study examined the specific and potential joint contribution of early onset of gambling participation (GP) and substance use (SU) in preadolescence to the frequency and characteristics of both behaviors in late adolescence, while controlling for confounders. Participants (N = 1,270; 51.2% boys) were part of a Canadian birth cohort. Age 10–12 years self-reports of GP and SU over the past year (collected 2007–2009) were used to identify preadolescents with either no onset of GP or SU (reference group), onset of GP-only, onset of SU-only, or onset of both GP and SU. Results showed that (1) preadolescent onset of either GP or SU is associated with corresponding behaviors and characteristics reflecting their seriousness at age 17 (collected 2014); (2) preadolescent onset of GP-only constitutes a risk for adolescent SU, but not the reverse; and (3) among preadolescents who initiated either GP or SU, those initiating both showed a higher number and severity of both types of outcomes at the end of adolescence. These findings are consistent with developmental models of addictive behaviors and highlight the importance of assessing both GP and SU for a comprehensive evaluation of preadolescents’ early involvement and underlying risk for addictive behaviors in late adolescence.
Introduction
From a public health perspective, the age at onset of mental health problems is critical because it often predicts more serious maladjustment later in life (De Girolamo et al., 2019). Establishing the age of onset is therefore fundamental both for planning timely preventive interventions and for understanding the etiology of mental disorders, including the developmental processes linking distinct conditions across time (Sroufe & Rutter, 1984). In the field of addictions, the early initiation of gambling participation (GP) and substance use (SU), respectively, has been highlighted in regard to adolescent gambling frequency and related problems (Delfabbro & King, 2020; Derevensky & Gilbeau, 2017) and adolescent SU, abuse and disorder (Kelly et al., 2019; Trucco & Hartmann, 2021), as well as the development of corresponding disorders in adulthood (Grant & Dawson, 1998; Mayes & Suchman, 2006; Quinn et al., 2023). However, most studies are retrospective and thus vulnerable to recall bias. In addition, the majority investigated either GP or SU in isolation, despite the accumulated evidence of their interrelatedness throughout adolescence (Wanner et al., 2009). As a result, it remains unknown whether an early onset of both behaviors (i.e., before age 13) confers greater risk than an early onset of only one, and whether early involvement in one domain may influence later involvement and problems in the other.
From a developmental perspective, several influential theoretical models posit that vulnerability to different addictive behaviors arises from shared predisposing processes unfolding across childhood and adolescence. Both the General Theory of Addictions (Jacobs, 1986) and the Syndrome Model of Addiction (Kim & Hodgins, 2018; Shaffer et al., 2004; Shaffer & Martin, 2011; Shaffer & Shaffer, 2016) propose that common genetic, neurobiological, psychological, and social factors contribute to the initiation and progression of multiple addictive behaviors. These addiction-focused models align closely with developmental frameworks of substance use (Cicchetti & Rogosh, 2018; Mayes & Suchman, 2006; McCrory & Mayes, 2015) and with broader biopsychosocial models of psychopathology emphasizing multilevel, person–environment transactions across development (Forbes et al., 2021; Lahey et al., 2017; Tully & Iacono, 2016).
Across these models, a central proposition is that a general underlying liability contributes to the emergence of multiple risk behaviors, including GP and SU, while behavior-specific factors account for differences in form, timing, and expression. Consistent with these frameworks, co-occurring risk behaviors like GP and SU are expected to signal greater underlying liability, risk antecedents and severity, as well as poorer outcomes (Shaffer et al., 2004, 2011). It is also acknowledged that each addictive behavior may have unique features (Grant & Chamberlain, 2020; Rash et al., 2016; Shaffer et al., 2004, 2018). Finally, as circumstantial opportunity may play a stronger role than the specific object of addiction in initiating new addictive behaviors (Shaffer et al., 2004), engagement in any addictive behavior may indicate heightened risk for developing others (Shaffer & Shaffer, 2016).
Taken together, developmental models of psychopathology and addiction suggest that (1) different addictive behaviors share common etiological pathways involving individual, family, and social risk factors; (2) susceptibility develops through multilevel, person–environment processes beginning in childhood; (3) co-occurring addictive behaviors are linked to more severe pathways and long-term consequences; (4) each addictive behavior may also involve distinct features; and (5) cross-behaviors associations are possible.
Although few empirical studies have examined the shared and unique correlates of GP and SU simultaneously, existing evidence supports the above developmental propositions. Shared risk factors for GP and SU are well documented (Carbonneau et al., 2024; Delfabbro & King, 2020; Derevensky & Gilbeau, 2017; Wanner et al., 2009), as are their co-occurrence and the greater severity associated with this dual condition in adolescents and adults (Barnes et al., 2009; Brunelle et al., 2012; Carbonneau et al., 2023; Grant & Chamberlain, 2020; Peters et al., 2015). At the same time, emerging research suggests that GP and SU differ in meaningful ways, including in coping mechanisms, emotion regulation, neurocognitive profiles, neural responses to reward, parental involvement in GP or SU, cultural acceptability, situational opportunities, and associations with suicidality (Grant & Chamberlain, 2020; Leeman & Potenza, 2012; Luijten et al., 2017; Panayiotou et al., 2023; Rash et al., 2016; Shaffer et al., 2018). These distinct features may contribute to differences in the developmental pathways of GP and SU (Grant & Chamberlain, 2020; Shaffer et al., 2004). Regarding cross-behavior effects, findings range from positive associations between adolescent SU and adult GP (Merkouris et al., 2021; Vitaro et al., 2019; Werner et al., 2020) to null effects (Wanner et al., 2009) and, conversely, from positive associations between adolescent GP and adult SU (Werner et al., 2020), to null effects (Vitaro et al., 2019). To our knowledge, the only study focusing on adolescence found that SU predicts an increase in GP, but no association between earlier GP and later SU in boys from age 16 to 17 (Vitaro et al., 2001). Overall, temporal cross-involvement between GP and SU remains unclear and warrants further investigation.
Considering this empirical evidence, several questions remain from a developmental perspective. First, it is unclear whether early onset of GP or SU independently confers elevated risk for later related problems once concurrent common risk factors are taken into account. Second, it is unknown whether the combination of early GP and SU represents a greater risk than early involvement in only one behavior. Third, the possibility of cross-domain effects—where early onset in one behavior predicts later involvement or problems in the other—has yet to be examined. In particular, no study has investigated whether the age of initiation of GP and SU predicts later outcomes across behaviors.
Addressing these gaps is important for advancing developmental models of addictive behaviors and for helping policymakers improve prevention strategies. If early onset of GP or SU does not predict later involvement once common risk factors are accounted for, prevention efforts should focus on these shared antecedents. Conversely, if early onset remains predictive above and beyond shared risk factors, age of initiation should be considered a key marker for identifying youth at heightened risk of involvement with addictive behaviors. Differences between early GP-only, SU-only, and combined early onset would further imply the need to consider behavior-specific and co-occurrence-specific risk factors, as well as factors related to eventual cross-domain pathways.
To address these gaps, a multilevel, integrative model is required—one that accounts for individual (e.g., sex, internalizing, and externalizing problems), familial (e.g., family adversity), and social risk factors (e.g., low socioeconomic status and deviant peers) associated with both the onset and the development of GP and SU (Delfabbro & King, 2020; Derevensky & Gilbeau, 2017; Mayes & Suchman, 2006; Trucco & Hartmann, 2021). The unique contribution of age of initiation (i.e., early onset) must be examined net of these influences.
The Present Study
The present study investigated the specific and joint contributions of preadolescent (ages 10–12) onset of GP and SU to the involvement in both behaviors in late adolescence (age 17), while controlling for concurrent individual, familial, and social risk factors associated with both types of behaviors. Given the characteristics of the sample (i.e., French-Canadian adolescents), it is noteworthy that—although gambling is illegal for minors in Canada—approximately 37% of Québec high school students reported gambling in 2008, that is, at the time the data used in this study were collected (Martin et al., 2009). Among students, 4.1% were classified as at-risk gamblers and 2% as probable pathological gamblers. The most popular games of chance are instant lotteries, card games and sports betting.
Drawing on prior research (Delfabbro & King, 2020; Derevensky & Gilbeau, 2017; Kelly et al., 2019; Trucco & Hartmann, 2021) and on developmental models of addiction (Cicchetti & Rogosh, 2018; Jacobs, 1986; Kim & Hodgins, 2018; Mayes & Suchman, 2006; Shaffer et al., 2004; Shaffer & Martin, 2011), we hypothesized that, compared to adolescents with no early onset, (1) early GP onset would predict greater GP frequency and other GP-related characteritics (variety of activities, gambling-related problems) at age 17; (2) early SU onset would predict greater SU frequency (daily smoking, alcohol use, marijuana use, and use of other drugs) and other SU-related characteristics (variety of substances used, substance abuse, and substance-related problems); and (3) early onset of both GP and SU would predict the highest levels of both GP- and SU-related outcomes among participants showing an early onset for either behavior. These longitudinal associations were expected even after controlling for (multilevel) common early risk factors. Cross-domain effects were also examined, but no specific hypotheses were formulated, given inconsistent prior findings.
Methods
Participants
Participants were drawn from a birth cohort of 2,226 infants (92% White of European ancestry, 51.2% boys) representative of single births in Quebec, Canada, in 1997–1998. Mothers who gave birth between 24 and 42 weeks of gestation and spoke either of Canada’s official languages (English or French) were eligible (see Orri et al., 2021, for comprehensive cohort details). Children were first assessed with their families at 5 months of age. Valid data on GP and SU early onset and risk factors were available for 1,435 participants (64.5% of the cohort) at ages 10–12 years. Of these, 88.5% had valid data at age 17, yielding a final study sample of 1,270 participants (57.1% of the cohort). Further details on participant attrition and data handling are provided in the “Data Analysis” section. Descriptive statistics are presented in Online Supplemental Material Table S1.
Ethics
The protocol for the Québec Longitudinal Study of Child Development (QLSCD), including all data collection procedures related to participants’ health, safety, rights, privacy, confidentiality, and data storage, was approved by the Ethics Committee, Institutional Review Board (IRB) of the Institut de la Statistique du Québec (ISQ; Ethical statement: June 14, 2023). Informed written consent was obtained separately from participants and/or their parents for each assessment wave. This study used anonymized QLSCD data (Orri et al., 2021) from a shared repository and was conducted in accordance with APA ethical standards.
Measures
Parent and teacher reports consisted of self-administered questionnaires sent by mail. Children’s self-reports at age 10–12 consisted of a paper-and-pencil questionnaire administered to the child alongside an in-person interview. This questionnaire was completed either at school (6.7%) or at home (93.3%), depending on the parents’ preference. At age 17, participants completed an online questionnaire without the assistance of an interviewer.
Early onset of GP was based on children’s self-reported gambling activities over the past year at the age of 10 or 12 years. At age 10, the three following items were used, coded from 0, never to 3, often: how many times during the past 12 months . . . did you play games for money with (1) family members; (2) friends; . . . (3) did you bet on sporting events or games for money. Item ratings were summed and then recoded into a binary indicator of whether the child had participated or not in gambling activities, coded as yes, 1 or no, 0. At age 12, the frequency of GP was assessed with the South Oaks Gambling Screen for adolescents (SOGS-RA; Wiebe et al., 2000; Winters et al., 1993). Participants indicated how often they had engaged in 12 gambling activities over the past 12 months (e.g., purchased lottery tickets, played online sports betting games, bought scratch offs, played bingo for money, bet on games on the internet, played video lottery terminal games, played cards or games with others for money, bet on sporting events/games for money, gambled at a casino, bet on games of skill (pool, basketball), played dice games for money, and bet on other games). Participants rated the frequency of each activity on a scale ranging from 0 (never) to 6 (daily). Item scores were summed, and the result was recoded as whether the participant had (1) or had not (0) engaged in any gambling activities over the past year. Finally, having a positive GP code at either age 10 or 12 warranted the participant a positive code for early onset of GP.
Early onset of SU was based on children’s self-reported use over the past year of tobacco and alcohol (age 10 and 12) as well as cannabis or other illicit drugs (age 12). The items for each substance (e.g., “have you used alcohol in the past 12 months?”) were initially coded 0, never to 3, often at age 10, and 0, never to 6, daily at age 12. Items were summed and coded as yes, 1 or no, 0 at each age and then aggregated into a binary indicator of SU onset at ages 10–12 years. The information on GP and SU onset was then aggregated in a 4-level preadolescent early onset indicator as follows: no onset, onset of GP only, onset of SU only, onset of both GP and SU.
Risk Factor Covariates
The strategy for measuring risk factors leveraged the diverse information available in this study at the individual, family, and social levels during preadolescence. To this end, assessments conducted at ages 10 and 12 were utilized, incorporating reports from parents, teachers, and the children themselves. Using multiple informants aimed to enhance the validity of risk factor measurements (Kraemer et al., 2003), while assessments at both ages improved the representativeness and reliability (Monach, 2012) of preadolescent indicators. Unless otherwise specified, continuous or discrete measurements at ages 10 and 12 were aggregated, with the reported coefficients (below) representing the average of the statistics from both time points. Further details on item selection, variable and scale construction, and sample statistics at each age are available in the Online Supplemental Material (“Measures” section, p. 1).
Individual risk factors were participants’ Sex and their Internalizing and Externalizing problems. Internalizing and externalizing items originated from the Social Behavior Questionnaire (Collet et al., 2023). Specifically, Internalizing problems included age 10 and 12 years measures of Anxiety (e.g., “fearful or anxious” and “worried”; average α: .73) and Emotional problems (e.g., “seemed unhappy/sad” and “has difficulty having fun”; α: .73) based on teacher and child reports, and Depressive symptoms (e.g., “I always felt alone” and “Nobody really loved me”; α: .75) based on child reports. Sub-scales scores were standardized, then averaged per informant and age of assessment, and finally combined into a global preadolescent Internalizing indicator. The correlation between age 10 and 12 years measures was .42.
Externalizing problems included age 10 and 12 years measures of Hyperactivity-Impulsivity (e.g., “could not sit still” and “difficulty taking turns”; average α: .75), Inattention (e.g., “easily distracted”; “inattentive”; α: .80), Opposition (e.g., “rebellious or refused to obey” and “got angry quickly”; α: .72), and Conduct problems (e.g., “stole things” and “got into a fight”; α: .75) based on teacher and child reports. Sub-scales scores were standardized, then averaged per informant and age of assessment, and finally combined into a global preadolescent Externalizing indicator. The correlation between the age 10 and 12 years measures was .56.
The Family adversity indicator was based on maternal age at the birth of her first child, maternal and paternal age at the birth of the target child, and family structure (coded as “intact: living with both biological parents” or “non-intact: not living with both biological parents”). Using these baseline socio-demographic indices (Table S1 in Online Supplemental Material), a value at or below the sample’s 30th percentile for the age variables or a non-intact family was coded as one adversity point. The resulting indicators were averaged to obtain a family adversity index ranging from 0 to 1.
Social risk factors were Household Socio-Economic Status (SES) and Association with deviant peers. Household SES was a standardized measure based on parents’ occupational prestige score, education level, and income (Statistics Canada, 1995). The correlation between age 10 and 12 years measures was .91. Association with deviant peers was based on two items. One item (“I hang out with a group of peers who do bad things”) originates from children’s reports and the other (“my child hangs out with disruptive children”) from maternal reports. Both items were coded as yes, 1 or no, 0, and were summed across informants and assessment times to obtain a 4-point index of whether the child associated with deviant peers while also reflecting a possible degree of severity (i.e., whether both informants reported this fact and whether it was reported at both assessment times or not).
Age-17 GP Outcomes
Similar to age 12, the frequency of GP was assessed at age 17 years with the South Oaks Gambling Screen for adolescents (SOGS-RA; Winters et al., 1993). Participants indicated how often they had engaged in 12 gambling activities over the past 12 months (see description above). Participants rated the frequency of each activity on a scale ranging from 0 (never) to 6 (daily) and item scores were summed into a gambling participation scale (α: .80). Variety of gambling activities at age 17 was calculated by summing the different types of gambling activities a participant had engaged in over the past 12 months, based on the activities listed above in regard to gambling participation, resulting in a 12-point scale (Ordinal α: .81).
Problems related to gambling at age 17 were assessed with the SOGS-RA in reference to the last 12 months, based on the following 12 items: “Try to win back money you have lost, claim to be winning money gambling although you were not, feel you have a problem with gambling, gamble more than you intended to, have been criticized for your betting or told you had a problem, feel guilty about the way you gamble, feel like you would like to stop gambling but do not think that you could, hide signs of betting or gambling from people in your life, have money arguments centered on your gambling, have borrowed from someone and not paid them back as a result of your gambling, have lost time from work or school due to gambling, have borrowed money to gamble or to pay gambling debts.” Coded yes or no (1, 0), the items were summed up, resulting in a 12-point scale of gambling-related problems (Ordinal α: .81). Based on the SOGS-RA score sheet, a score of 1 or 2 indicates some problems with gambling, and a score of 3 or more suggests probable problem gambling (Winters et al., 1993). Using these criteria, 1.6% of participants at age 17 could be classified as having some problems related to gambling and 0.6% as probable problem gamblers. Because of the small number of participants reporting gambling-related problems, both categories were collapsed to represent problem gambling (i.e., gamblers with one or more problems; 2.2%).
Age-17 SU Outcomes
Frequency over the past year of tobacco, alcohol, marijuana and other illicit drugs was assessed using adolescents’ self-reports at age 17 years. Participants were asked about their use of tobacco and whether they had been a daily smoker or not, coded as yes (1) or no (0). For alcohol, marijuana and other illicit drugs, the following three items from the Personal Experience Screening Questionnaire (Henly & Winters, 1989; Winters et al., 1990) were used: “In the last 12 months: How many times did you use alcohol? How many times did you use marijuana? How many times did you use other illicit drugs like cocaine, stimulants, speed, amphetamine, tranquilizers, inhalants, heroin, opiates, hallucinogens, psychedelics, or other narcotics or hard drugs?” Each item was coded on a similar scale: 0, Never; 1, Just once to try; 2, Less than once a month; 3, About once a month; 4, Weekends or once-twice a week; 5, Three times or more a week, but not every day; 6, Daily.
An indicator of substance abuse was obtained by asking the participants how many times they had five drinks or more on the same occasion over the past year. Variety of substances used was calculated by summing the different types of substances a participant had used over the year, resulting in an 7-point scale (Ordinal α: .70). Problems related to Substance use were based on the following items reported by participants as related to their use: psychological difficulties, harmed family relationships, harmed friendships or romantic relationships, school problems, committing an act of delinquency, feeling that the same amounts have less effect, and consulting regarding own substance use. Each item referred to the past year and was coded yes (1) or no (0). Items’ responses were collapsed into a 0 (none) to 1 (one or more) indicator.
Data Analysis
The study sample with valid data (N = 1,270; 57.1% of the cohort) was compared to children for whom no data were available during the periods of interest (N = 956; 42.9%) based on socio-demographic variables assessed at 5 months of age. These variables included maternal age at the birth of the first child, paternal age at the birth of the target child, parental education, family income and structure (i.e., intact or not), number of siblings, and child sex. Small (.20 ⩽ d, h < .50; Cohen, 1988) but significant differences were observed, with younger motherhood (d = .22), lower maternal (h = .19) and paternal (h = .19) education, lower family income (d = .27), more boys (h = .22), and a slightly higher likelihood of parental separation (h = .10) in lost participants.
To account for differential attrition, inverse probability weighting was applied in the analyses. The goal of IPW is to correct for the missing data and provide a less biased estimate in relation to selective participation than simply deleting participants (Seaman & White, 2013; Thompson & Arah, 2014). IPW uses the complete cases to create a pseudo-population by weighting them to represent the entire study sample, including those with missing data. This strategy is particularly suited when missingness primarily reflects attrition-related non-response (Hughes et al., 2019). Specifically, a logistic regression model was used to estimate the probability of a participant having valid study data based on baseline differences noted above between retained and lost participants. The observations included in the study were then weighted by the inverse of these estimated probabilities. Applying inverse probability weighting in longitudinal studies has been shown to reduce bias associated with differential attrition (Thompson & Arah, 2014).
Multicollinearity among the risk factors was assessed and found to be within acceptable limits. Among the 15 bivariate associations between risk factors (range: .01–.61), only two correlation coefficients exceeded .4 but remained below the critical threshold of .70, accounting for less than 38% of the variance in the correlated measures (Table S2 in Online Supplemental Material).
In a first step, descriptive analysis was used to examine the 4-level preadolescent early onset indicator (no onset, onset of GP only, onset of SU only, onset of both GP and SU). Specifically, the four groups were compared on (1) the initial scales of GP and SU at age 10 and 12 years in order to determine whether differences existed between onsetters in their early level of GP or SU, and (2) each risk factor used as a covariate in the main analysis. To that end, Generalized Linear Models (GLM) were used. The same method was employed to examine the association between early onset GP or SU and age-17 outcomes. This approach accommodates normal and non-normal data, including skewed distributions and binary outcomes, providing a unified framework for analyzing outcomes with different distributions (Hardin & Hilbe, 2018). In the second step of analysis, the four-level preadolescent early onset indicator served as the independent variable, with participants who had no preadolescent onset as the reference group. Given that the analysis was conducted for ten outcomes, False Discovery Rate control was applied to adjust for multiple comparisons (Glickman et al., 2014). For each outcome, an initial model including only risk factor covariates was estimated, followed by a second model incorporating the early onset indicator. The Likelihood Ratio Test (LRT) was used to assess model fit and determine whether adding the preadolescent onset indicator significantly improved the model. Complementary analyses compared the onsetter groups (i.e., onset of GP only, onset of SU only, and onset of both SU and GP) within the full model, controlling for covariates. To evaluate the magnitude of observed associations, effect size estimates corrected for differences in sample sizes between groups were computed using Cohen’s d for mean differences and Cohen’s h for differences in proportions (Cohen, 1988).
Results
GP and SU Onset Groups
Generating the four-level preadolescent early onset indicator of GP and SU resulted in the following groups of participants: 931 participants (73.3% sample) did not report GP or SU by age 12 and represented the reference, no-preadolescent onset group. A second group of 227 participants (17.9%) reported an early onset of GP only. A third group of 63 participants (5.0%) reported an early onset of SU only. Finally, 49 participants (3.9%) reported an early onset of GP and SU. Thus, overall, 21.8% of participants had initiated or experimented with GP and 8.9% SU in preadolescence.
In descriptive analysis (Table 1), the between-group comparison on the initial GP and SU scales at ages 10 and 12, as well as on the aggregated two-age measures, showed that participants in the GP-only and GP-and-SU onset groups did not differ on the scores of GP frequency scales, and that the latter did not differ from SU-only onsetters on the scores of the SU frequency scales. Furthermore, analysis revealed statistically significant association with the GP and SU onset indicator for all risk factor covariates but family adversity. The latter, however, met the minimal significance criterion (p < .25) to be included in multivariate analysis (Hosmer & Lemeshow, 2000). The three groups of onsetters were significantly linked with 3–5 risk factors when compared to the reference group of no-onset, with participants in the GP and SU onset group showing the highest number, as well as significant differences with one or both other onsetter groups on 4 risk factors. These results supported further the pertinence of using these risk factors as covariates in the main analysis.
Differences between the Different Onset Groups on Preadolescent Covariates and GP and SU Measures: Bivariate Results.
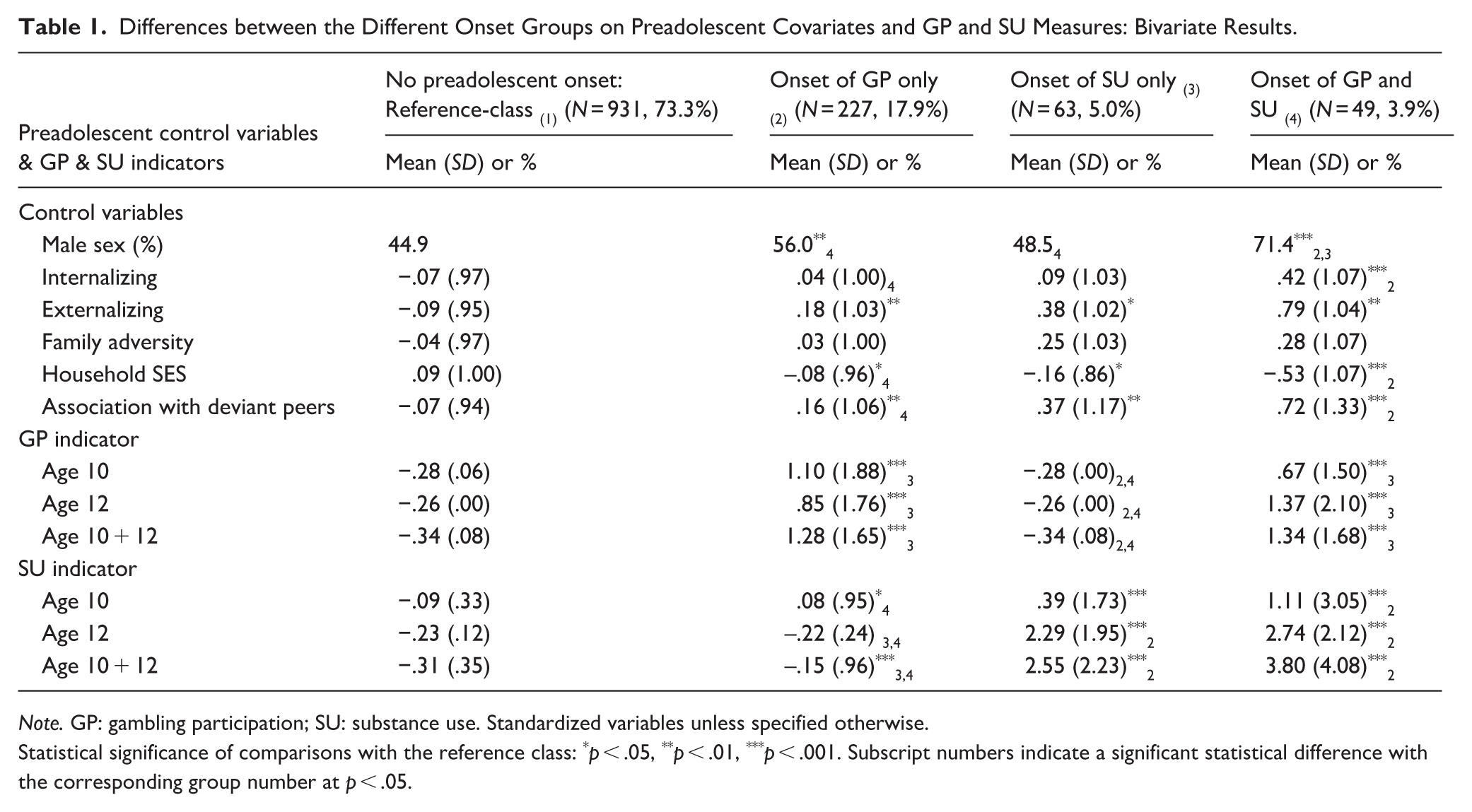
Note. GP: gambling participation; SU: substance use. Standardized variables unless specified otherwise.
Statistical significance of comparisons with the reference class: *p < .05, **p < .01, ***p < .001. Subscript numbers indicate a significant statistical difference with the corresponding group number at p < .05.
Distribution and Descriptive Statistics of Age-17 Outcomes
Figure S1 in Online Supplemental Material displays the distribution of participants for each outcome of frequency of GP and SU at age 17 years. Among participants, 6.9% reported daily smoking, 82.8% reported alcohol use at least once, 40.7% reported cannabis use, 10.1% reported other illicit drug use, and 14.0% reported gambling participation over the previous 12 months. Furthermore, regarding the characteristics of age-17 GP and SU (Figure S2 in Online Supplemental Material), 66.6% had abused alcohol at least once, 4.6% had used two or more substances, 5.3% reported two or more varieties of gambling activities, 20.6% at least one problem related to SU, and 2.2% at least one problem related to GP. Descriptive statistics for the sample are shown at the top of Tables 2 and 3.
Association between Preadolescent Onset of Gambling Participation (GP) and Substance Use (SU) and Frequency of GP and SU at Age 17 Years.
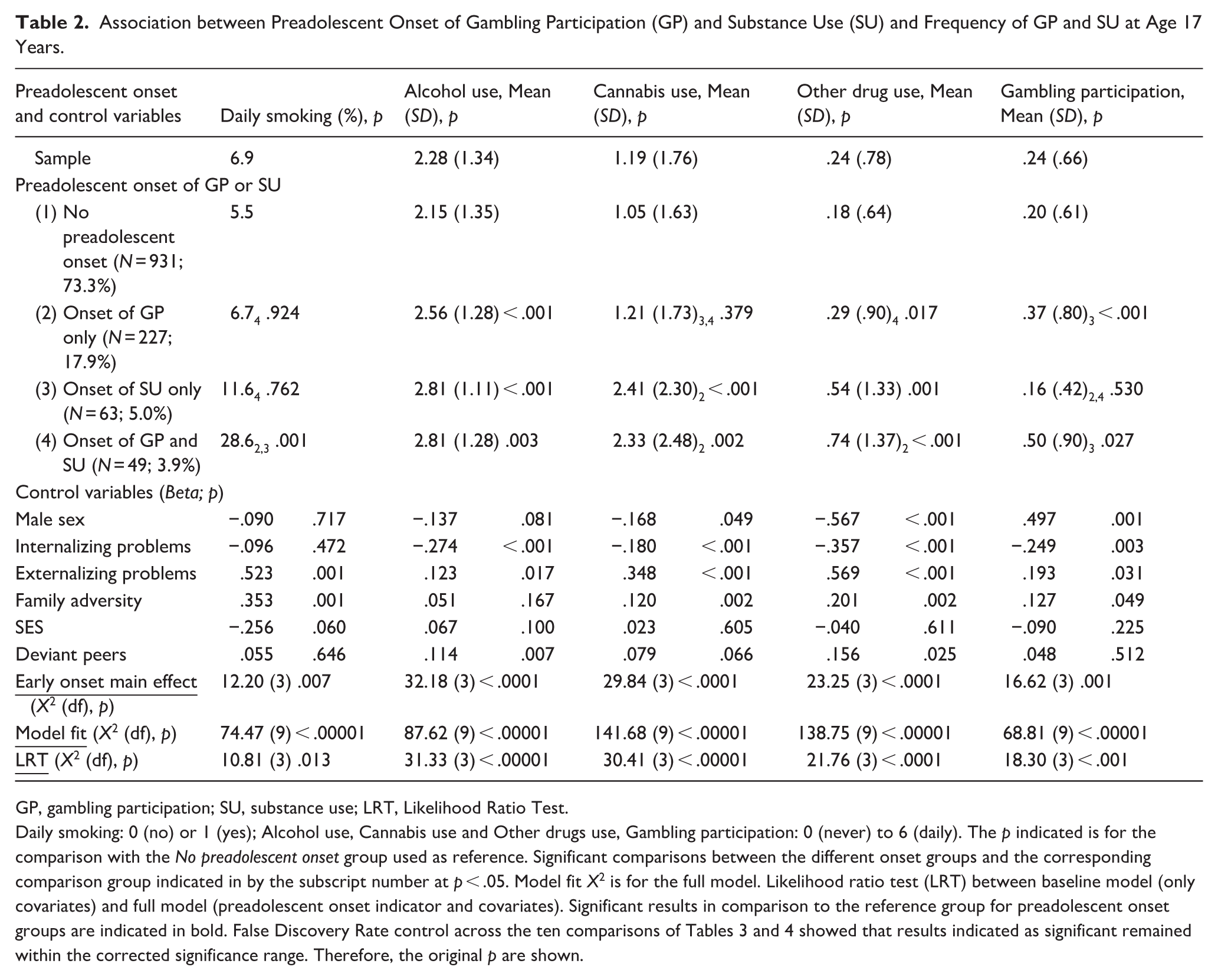
GP, gambling participation; SU, substance use; LRT, Likelihood Ratio Test.
Daily smoking: 0 (no) or 1 (yes); Alcohol use, Cannabis use and Other drugs use, Gambling participation: 0 (never) to 6 (daily). The p indicated is for the comparison with the No preadolescent onset group used as reference. Significant comparisons between the different onset groups and the corresponding comparison group indicated in by the subscript number at p < .05. Model fit X2 is for the full model. Likelihood ratio test (LRT) between baseline model (only covariates) and full model (preadolescent onset indicator and covariates). Significant results in comparison to the reference group for preadolescent onset groups are indicated in bold. False Discovery Rate control across the ten comparisons of Tables 3 and 4 showed that results indicated as significant remained within the corrected significance range. Therefore, the original p are shown.
Association between preadolescent onset of gambling participation (GP) and substance use (SU) and characteristics of GP and SU at age 17 years.
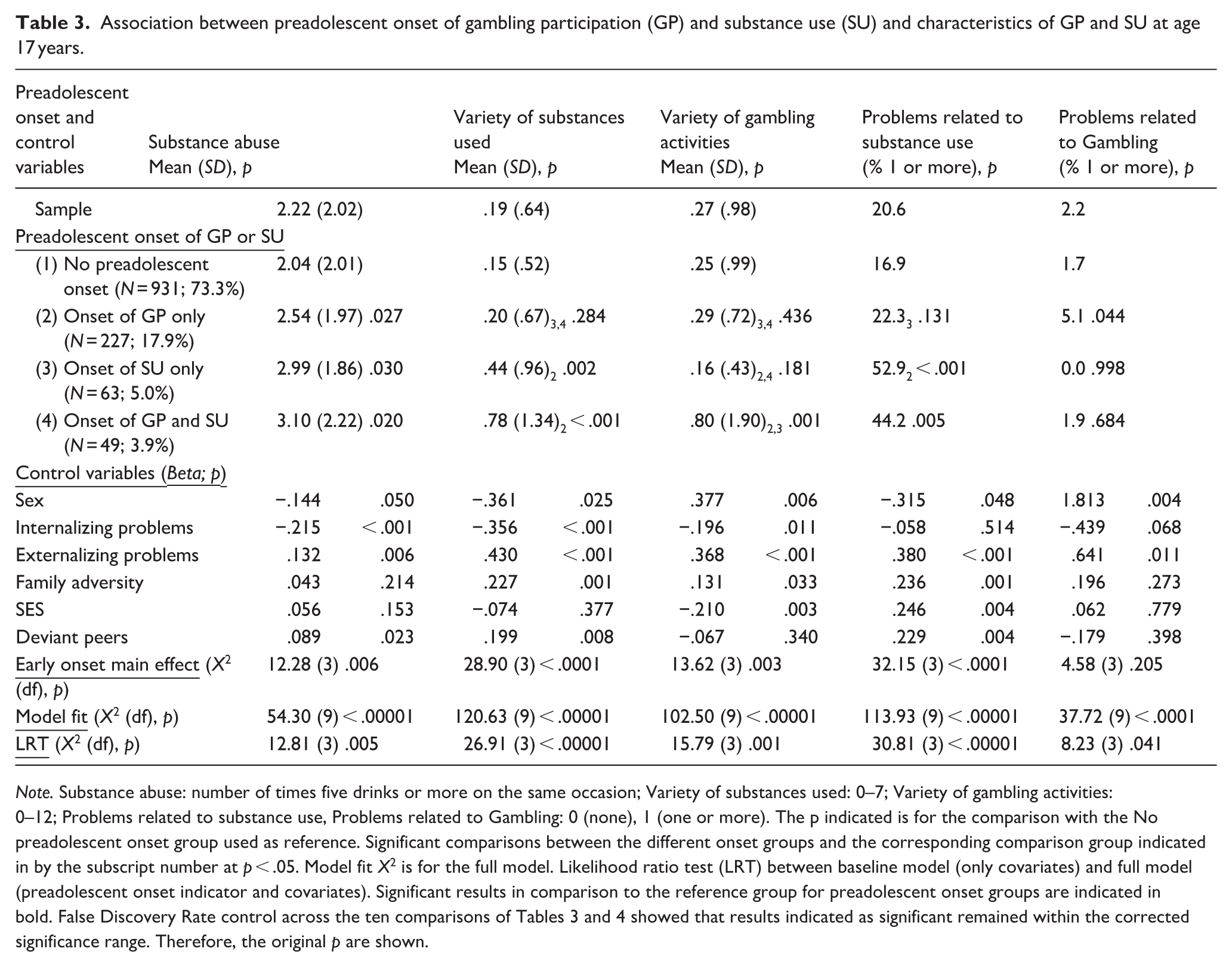
Note. Substance abuse: number of times five drinks or more on the same occasion; Variety of substances used: 0–7; Variety of gambling activities: 0–12; Problems related to substance use, Problems related to Gambling: 0 (none), 1 (one or more). The p indicated is for the comparison with the No preadolescent onset group used as reference. Significant comparisons between the different onset groups and the corresponding comparison group indicated in by the subscript number at p < .05. Model fit X2 is for the full model. Likelihood ratio test (LRT) between baseline model (only covariates) and full model (preadolescent onset indicator and covariates). Significant results in comparison to the reference group for preadolescent onset groups are indicated in bold. False Discovery Rate control across the ten comparisons of Tables 3 and 4 showed that results indicated as significant remained within the corrected significance range. Therefore, the original p are shown.
Association of Preadolescent Onset of GP or SU and Age-17 Frequency of GP and SU
Results regarding the association between preadolescent onset of GP or SU and the frequency of GP and SU at age 17 years are presented in Table 2. For all five outcomes, the model including the preadolescent onset indicator as predictor provided a significant improvement in fit over the baseline model with preadolescent covariates only. In comparison with their peers in the no-preadolescent onset group, participants with an early onset of GP only reported a higher frequency of GP, but also of alcohol and other drugs use at age 17. Adolescents with an early onset of SU only reported a higher frequency of alcohol, cannabis and other illicit drugs use at age 17, but not a higher frequency of GP, than their peers with no-preadolescent onset. Finally, participants with an early onset of GP and SU were more likely to be daily smokers and reported a higher frequency of alcohol, cannabis and other drug use as well as GP at age 17 than their peers with no-preadolescent onset. In comparisons among preadolescent onsetters, participants with an early onset of GP only reported a higher frequency of GP at age 17 than peers with an early onset of SU only, who in turn reported a higher use of cannabis than the former. Adolescents with a preadolescent onset of GP and SU were more likely to be daily smokers at age 17 than both preadolescent GP-only and SU-only onsetters, reported a higher frequency of cannabis and other illicit drugs than their GP-only peers, and a higher frequency of GP than participants with an early onset of SU only.
Association of Preadolescent Onset of GP or SU with Age-17 Characteristics of GP and SU
Results regarding the association between preadolescent onset of GP or SU and age 17 characteristics of GP and SU are presented in Table 3. As observed with frequency outcomes, for all five measures, the model including the preadolescent onset indicator as a predictor provided a significant improvement in fit over the baseline model with preadolescent covariates only. In comparison with their peers in the no-preadolescent onset group, participants with an early onset of GP only reported a higher frequency of substance abuse at age 17. Of note, although (a) the comparison between the latter two groups on problems related to GP was significant (p = .044) and (b) the model with the preadolescent onset indicator for that outcome fit better than the model with covariates only (LRT X2(3) = 8.23, p = .041), the effect of the preadolescent onset indicator was not significant (p = .205). The low statistical power and small effect size for this specific comparison likely explain the observed discrepancy between the omnibus test and specific p-values. Adolescents with a preadolescent onset of SU only or of both GP and SU reported more substance abuse, a higher variety of substances used, and a higher likelihood of reporting at least one problem related to SU at age 17 than their peers with no-preadolescent onset. Participants with an early onset of GP and SU also reported a higher variety of gambling activities than participants in the reference group.
In comparisons among preadolescent onsetters, participants with an early onset of GP only reported a higher variety of gambling activities at age 17 than those with an early onset of SU only, and the latter reported a higher variety of substances used and had a higher likelihood of reporting at least one problem related to SU than the former. Adolescents with a preadolescent onset of GP and SU reported a higher variety of gambling activities than their peers with either an early onset of GP only or SU only, and a higher likelihood of reporting at least one problem related to substance use than those with an early onset of GP only.
Of note, running the analysis without the weights computed to compensate for differential attrition resulted in the same significant associations shown in Tables 2 and 3, with the single exception of age-17 GP frequency. For that outcome, the higher frequency reported by participants with a preadolescent onset of GP and SU in comparison to the reference group (Table 2), originally significant (p = .027), dropped below the significance level (p = .054).
Strength of the Observed Associations
The strength estimates (and their respective 95% CI) of the above associations between preadolescent onset of GP or SU and age-17 frequency and characteristics of GP and SU are presented in Table 4. Across four significant age-17 comparisons with the reference group with no-preadolescent onset, participants with an early onset of GP only showed, on average, a small (i.e., .20 to < .50) effect size (Cohen’s d or h) of .25, which was similar for the GP-related (average .26) and the three SU-related (average .24) measures. For their six significant comparisons (all substance-related) with the reference group, participants with a preadolescent onset of SU only showed, on average, a medium (i.e., .50 to < .80) effect size of .60. Finally, out of nine significant comparisons with their peers with no-preadolescent onset, participants with an early onset of GP and SU showed, on average, a medium effect size of .66 (i.e., .50 for GP-related and .70 for SU-related measures).
Effect Size for Age-17 Differences in Frequency and Characteristics of Gambling Participation (GP) and Substance Use (SU) by Preadolescent Onset of GP and SU. a
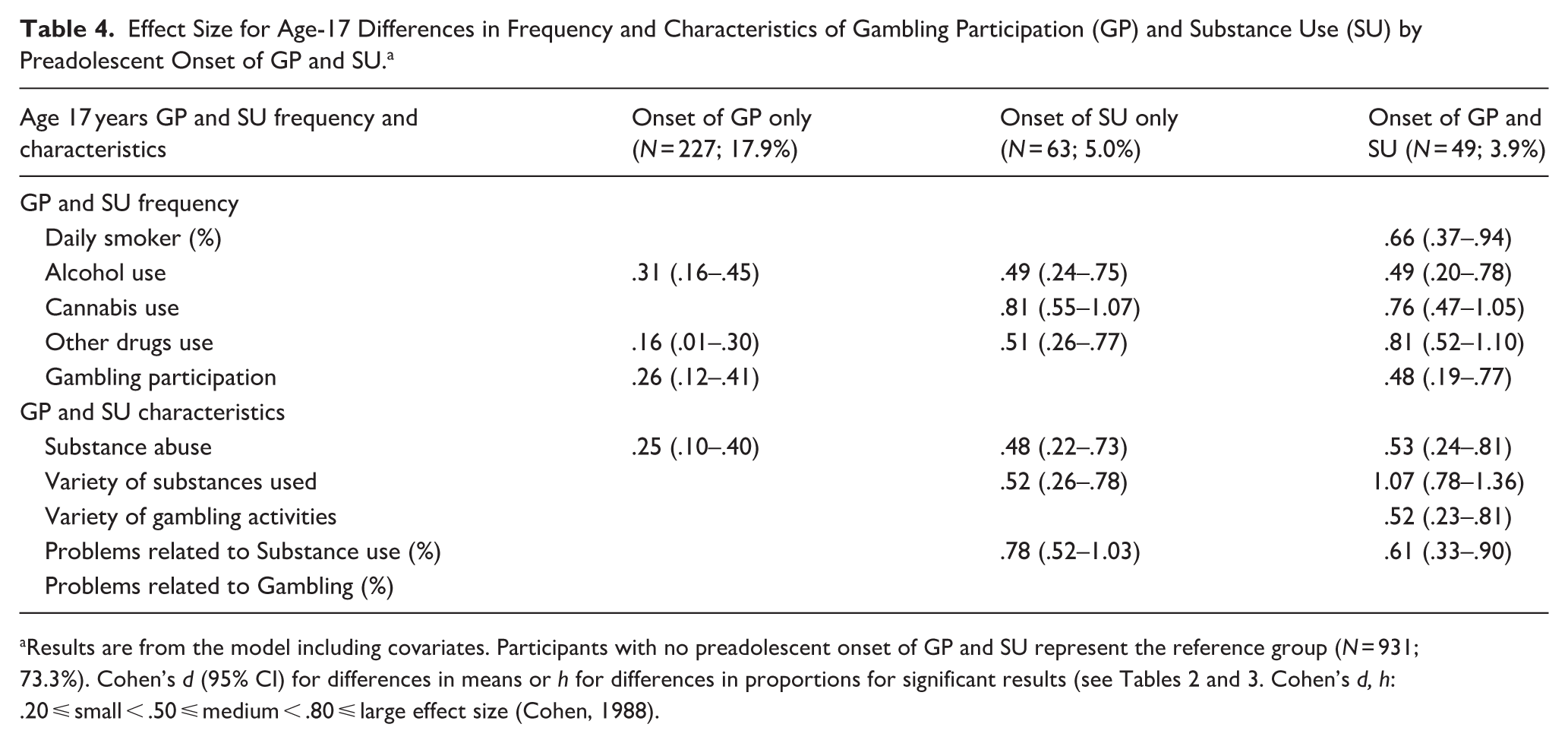
Results are from the model including covariates. Participants with no preadolescent onset of GP and SU represent the reference group (N = 931; 73.3%). Cohen’s d (95% CI) for differences in means or h for differences in proportions for significant results (see Tables 2 and 3. Cohen’s d, h: .20 ⩽ small < .50 ⩽ medium < .80 ⩽ large effect size (Cohen, 1988).
Discussion
The critical roles of an early onset of GP or SU in the development of these addictive behaviors have mostly been studied independently, despite theoretical frameworks contending that they reflect different manifestations of a common underlying syndrome (Jacobs, 1986; Kim & Hodgins, 2018; Shaffer et al., 2004, 2011). The aim of this study was to investigate the specific—and potential joint—contribution of preadolescent onset of GP and SU to the frequency and characteristics of these behaviors in late adolescence, while controlling for individual, familial and social risk factors associated with both behaviors.
As expected, and consistent with previous research (Derevensky & Gilbeau, 2017; Trucco & Hartmann, 2021), youth who initiated GP before adolescence showed a higher level or likelihood of gambling-related behaviors at age 17, and those with an early onset of SU showed elevated substance-related behaviors, compared to the reference group with no preadolescent onset. These findings, which are independent of shared concurrent risk factors, underscore the developmental continuity between a preadolescent onset and late adolescence involvement with either GP or SU. Consequently, they emphasize the importance of early initiation as a key indicator for identifying youth at heightened risk of addiction-related behaviors in adolescence.
Notably, participants who initiated both GP and SU before adolescence exhibited the most pervasive and severe patterns of addictive behaviors in late adolescence. This was evident in three ways. First, they showed the largest number of significant outcomes at age 17 compared with the reference group: nine of ten GP- and SU-related outcomes, versus four for the GP-only group and six for the SU-only group. Second, across eight direct comparisons, adolescents with an early onset of both behaviors demonstrated higher levels or likelihood of age-17 outcomes—reflecting the frequency as well as the characteristics of GP and SU—than peers with a single-behavior onset. Third, associations relative to the no-onset group were consistently stronger for the dual-onset group than for the GP-only or SU-only groups.
Together, these findings suggest that co-occurring early addictive behaviors signal a more complex developmental pathway and more severe long-term consequences than the early onset of only one behavior. This pattern is consistent with the addiction-syndrome model (Kim & Hodgins, 2018; Shaffer et al., 2004, 2011), as well as substance-use models (Mayes & Suchman, 2006) and developmental psychopathology frameworks (Cicchetti & Rogosh, 2018), all of which posit that co-occurring conditions or polysubstance involvement confer heightened risk relative to isolated behavior patterns. The elevated outcomes among youth with dual early onset emphasize the need to identify risk factors specifically associated with early initiation of both GP and SU—an important direction for future research.
Regarding cross-behavior associations, adolescents with a preadolescent onset of GP-only reported higher alcohol use, alcohol abuse, and use of other drugs at age 17 than those with no early onset, indicating that early GP may elevate risk for later SU even in the absence of early SU. By contrast, early SU-only predicted exclusively substance-related outcomes, suggesting that in the absence of early GP, early SU onset did not appear to generalize to adolescent gambling. These asymmetrical cross-behavior patterns may reflect differences in opportunities for early exposure. In this sample, early GP was far more common (21.8%) than early SU (8.9%), consistent with previous research in early teens (Barnes et al., 2009). At this early age, gambling may be more accessible, socially tolerated, and perceived as benign by parents, who may not pay attention to their children’s exposure to this activity or be alarmed by their children’s gambling (Barnes et al., 2009). Consequently, preadolescents may have more opportunities to engage and to express underlying vulnerabilities in GP than in SU (Grant & Chamberlain, 2020; Shaffer et al., 2004). Children themselves may also view activities such as betting on sports or card games—which may also be more accessible to them—as relatively harmless compared with SU. However, as accessibility to substances increases over adolescence, early GP may provide a behavioral platform that later extends to SU. This could occur through shared mechanisms such as an overconfident attitude toward risk-taking (Derevensky & Gilbeau, 2017; Trucco & Hartmann, 2021), although this explanation is less likely in the present study because early individual dispositions toward risk-taking and externalizing behaviors were controlled. Alternatively, GP may provide a gateway to SU, possibly through affiliation with new deviant peers who offer access to illicit substances and who endorse, model, and reward their consumption (Mason et al., 2007), which may co-occur with decreases in parental supervision and familial norms (O’Reilly & Mohan, 2023). Given inconsistent findings in prior longitudinal work (Merkouris et al., 2021; Vitaro et al., 2001, 2019; Wanner et al., 2009, 2020), the present asymmetrical cross-behavior result warrants replication and further investigation of potential risk factors and underlying mechanisms.
A final noteworthy finding is that, while both groups with early GP (GP-only and dual-onset) reported a similarly higher frequency of GP at age 17 than the no-onset and SU-only groups, youth with dual onset also reported a greater variety of gambling activities at age 17 than all other groups. This is an important marker, as a greater variety of gambling in adolescence predicts increased risk of adult gambling problems beyond adolescent gambling severity (Carbonneau et al., 2015). It suggests that a dual onset may represent an elevated risk for later GP-related problems than the early onset of GP only.
In conclusion, consistent with converging evidence from addiction-syndrome theory (Jacobs, 1986; Shaffer et al., 2004; Shaffer & Martin, 2011), genetically informed research (Slutske et al., 2013; Vitaro et al., 2019), neuropsychological (Potenza, 2008; Yücel et al., 2019), and longitudinal studies (Barnes et al., 2009; Carbonneau et al., 2023; Grant & Chamberlain, 2020), results of the present study suggest that GP and SU are intertwined as early as preadolescence, and that these early manifestations shape later involvement in both behaviors. However, the mechanisms through which early onset of one or both behaviors confers risk for later domain-specific or cross-domain outcomes remain unclear. Familial and peer exposure are likely influential (Delfabbro & King, 2020; Trucco & Hartmann, 2021), but future research is needed to disentangle how such exposures combine with individual vulnerabilities and other environmental influences across adolescence.
Strengths and Limitations
A key strength of this study is its use of a large population-based birth cohort with assessments of GP and SU in both preadolescence and late adolescence. The integrated longitudinal-multivariate design enabled a precise examination of the contribution of early onset of each behavior while adjusting for individual and socio-familial risk factors. Incorporating multiple informants (child, parent, and teacher) for early risk factors further reduced potential inflation of associations due to shared source variance, thereby strengthening the study’s conclusions.
However, several limitations must be considered. First, GP and SU were assessed via adolescent self-report, which may be affected by self-presentation or recall biases. Yet, self-report remains the most practical and commonly used method for assessing GP and SU in large population studies (Barnes et al., 2009; Johnston et al., 2022). Furthermore, prior validation studies suggest acceptable accuracy for both GP (Edgren et al., 2016) and SU (Harrison et al., 2007) self-reports in youth. Second, some relevant risk factors were not included, notably early exposure to GP and SU within the family and peer contexts, despite evidence that such exposure may influence early initiation or later escalation (Delfabbro & King, 2020; Trucco & Hartmann, 2021). Future work should examine these influences in combination with early onset to clarify their roles in later addictive behaviors. Third, although socio-demographic differences between participants and those lost to attrition were small and statistical weighting was applied to reduce bias, attrition from infancy to late adolescence was substantial. As is typical in long-term cohort studies, the final sample was likely somewhat less at risk than the original cohort, which may have resulted in conservative estimates of associations. The precise impact of attrition remains uncertain.
Fourth, although the observed associations were statistically significant (i.e., indicating that an association/effect exists within the certainty reflected by p-values), the low statistical power in some smaller onset groups and for less frequent outcomes resulted in wider confidence intervals (Table 4), reflecting reduced precision of effect size estimates. Therefore, replication in larger samples is important to refine the magnitude of these associations. Fifth, the small size of some onset groups precluded examination of potential sex differences. Sixth, it is important to emphasize that the study results are associative rather than causal. Finally, generalizability is limited by the fact that the sample primarily consisted of French-speaking Canadian adolescents. Replication in other cultural and legal contexts, particularly where underage gambling is less regulated, is needed. In addition, the cohort was assessed between 2007 and 2014. Changing trends in adolescent SU since the study’s inception (Johnston et al., 2022; Peiper et al., 2016) and shifts in the legal and social landscape of both behaviors in Canada—legalization of adult cannabis use, expansion of online and sports gambling, increases in vaping (Health Canada, 2024; Institut national de santé publique du Québec (INSPQ), 2022; Tremblay et al., 2023) influence patterns of early onset and adolescent outcomes today. Although earlier cohort findings remain informative, caution is required when extrapolating to contemporary youth. Given the dynamic nature of GP and SU and their sensitivity to person–environment transactions, continuous monitoring through population-based longitudinal research is essential to understanding and keeping track of these moving targets in changing social contexts (Johnson & Guttmannova, 2019; Oldehinkel & Ormel, 2023).
Despite these limitations, the findings indicate that preadolescent onset of GP or SU is associated with corresponding behaviors and their severity at age 17. Moreover, early GP appears to confer some risk for later SU, whereas early SU does not appear to generalize to gambling. Most importantly, among preadolescents who initiate either GP or SU, youth who initiate both behaviors display the greatest number and severity of adverse outcomes across both domains by late adolescence. These results align with developmental models of addiction and underscore the importance of assessing both GP and SU for a comprehensive evaluation of preadolescents’ involvement in and susceptibility to addictive behaviors. From a prevention perspective, the results confirm the importance of addressing upstream factors that may contribute to the early onset of these two behaviors, thus mitigating the risk of escalation into adolescent GP and SU involvement. Attention should also be directed toward factors promoting early GP as a potential gateway to later SU. From a public health policy perspective, it is important to raise public awareness of the potential consequences of early GP and SU, and to implement early screening to identify young people involved in either, and especially both, of these activities. Addressing common and specific risk factors through universal and targeted prevention strategies could be a promising approach.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254261432793 – Supplemental material for Association Between Early Onset of Gambling Participation and Substance Use in Preadolescents and Age-17 Frequency and Characteristics of Addictive Behaviors
Supplemental material, sj-docx-1-jbd-10.1177_01650254261432793 for Association Between Early Onset of Gambling Participation and Substance Use in Preadolescents and Age-17 Frequency and Characteristics of Addictive Behaviors by Rene Carbonneau, Frank Vitaro, Mara Brendgen, Michel Boivin, Sylvana M. Côté and Richard E. Tremblay in International Journal of Behavioral Development
Footnotes
Acknowledgements
We thank the families and the participants of the Québec Longitudinal Study of Child Development and the Institut de la Statistique du Québec for data collection and management.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Quebec Government Ministry of Health, the Fond Quebecois de la Recherche sur la Societe et la Culture, and Canada’s Social Science and Humanities Research Council for their financial support of the research presented in this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.