
Abstract
This preregistered study examined whether child temperament predicts social-emotional functioning and moderates the associations between parental distress, COVID-19–related stressors, and children’s social-emotional outcomes during the pandemic. The participants were 1,305 Finnish children (46% girls) from the FinnBrain Birth Cohort, with temperament assessed at age 2.5 years and follow-ups conducted from ages 5 to 9 years. Across five time points, parents reported their distress (anxiety and depressive symptoms) and family COVID-19–related stressors, and rated their children’s social-emotional functioning (i.e., emotional symptoms, conduct problems, hyperactivity, peer problems, and prosocial behavior) at four follow-ups (data from up to 568 children). Covariate-adjusted linear regression and mixed-effects models were used to test the main and moderating effects. Higher negative affectivity and lower effortful control in children predicted greater emotional and behavioral problems and fewer prosocial behaviors, while higher surgency was linked with fewer internalizing but more externalizing problems. Temperament also moderated the associations between COVID-19–related stressors and social-emotional functioning. Children high in negative affectivity showed stronger links to emotional symptoms early in the pandemic, whereas, unexpectedly, those low in negative affectivity exhibited more conduct problems under higher stress. Effortful control mitigated the effects of parental distress on conduct problems and hyperactivity. These findings highlight the role of temperament in influencing children’s resilience and vulnerability under prolonged stress, emphasizing the importance of identifying temperamental risk profiles for guiding future prevention and support efforts.
Keywords
Introduction
The COVID-19 pandemic profoundly disrupted family life, altering routines, increasing stress, and impacting family well-being (Prime et al., 2020). Measures like home confinement, limited caregiving resources, and job losses particularly affected families with young children (Essler et al., 2021; E. A. Holmes et al., 2020). Globally, the pandemic has negatively impacted mental health, with children’s well-being disproportionately affected, leading to increased social-emotional problems (Essler et al., 2021, 2024; Kauhanen et al., 2023; Martiny et al., 2022; Prime et al., 2020). In Finland, mitigation strategies differed somewhat from those implemented elsewhere. Early childhood education and primary schools closed only briefly in spring 2020, and many child care centers remained open for families needing support. Restrictions focused mainly on limiting gatherings, reducing mobility, and encouraging remote work, with the strictest measures occurring during spring and again in December 2020, which also affected children’s extracurricular activities and hobbies. Although infection rates remained comparatively low relative to many other countries, families experienced substantial uncertainty and disruptions to routines, contributing to elevated stress during the early phases of the pandemic (Hale et al., 2021).
Social-emotional functioning, rooted in individuals’ interactions with their environments, encompasses the ability to understand, express, and respond to one’s own and other’s emotions in socially appropriate ways (Denham et al., 2009). Early proficiency in these skills is critical for children’s well-being and is a strong predictor of future mental health outcomes (Arslan et al., 2021; Jones et al., 2015; Korhonen et al., 2018). These competencies are vital for developing empathy and sympathy, which in turn foster prosocial behaviors—voluntary actions that benefit others, independent of personal gain (Paulus, 2018). Conversely, when social-emotional development is disrupted or underdeveloped, children face heightened risk for problem behaviors, including externalizing problems (e.g., aggression, hyperactivity) and internalizing problems (e.g., anxiety, depression) (Arslan et al., 2021; Huber et al., 2019). Epidemiological estimates from Nordic child psychiatric work suggest that approximately 15 to 20 percent of children show clinically significant mental health or social-emotional problems (Kumpulainen et al., 2016), underscoring both immediate and long-term stakes for early identification and intervention.
Prolonged parental distress, including stress, anxiety, and depression, is known to pose a significant risk to children’s social-emotional functioning through its impact on negative parenting behaviors (Hakanen et al., 2019) and is frequently linked to higher social-emotional problems in children (Honda et al., 2023). During the COVID-19 pandemic, heightened parental distress—driven by chronic uncertainty, financial strain, and social isolation—further disrupted parent–child interactions and undermined family climate, leading to marked increases in children’s social–emotional problems, including internalizing and, in some cases, externalizing symptoms (Essler et al., 2021, 2024; López-Morales et al., 2023; Martiny et al., 2022; Prime et al., 2020; Spinelli et al., 2020; Sun et al., 2022).
According to the transactional model (Sameroff, 2009), development unfolds through continuous, bidirectional exchanges between children and their environments, meaning that children both shape and are shaped by their surrounding contexts. Importantly, in this framework, broader societal stressors influence children primarily through their proximal environments, particularly the family, where parental stress and well-being function as key mechanisms linking external demands to child adjustment. Within this framework, temperament provides a key source of individual differences that influence how children respond to stressors such as parental distress. Temperament refers to early-emerging, stable, biologically based differences in emotional reactivity and regulation (Rothbart & Bates, 2006), typically conceptualized through three core dimensions: negative affectivity (propensity toward negative emotions), surgency/extraversion (positive emotionality and approach motivation), and effortful control (capacity for deliberate self-regulation). Prior work shows that temperamental characteristics—including negative affectivity, effortful control, and social withdrawal—can strengthen or weaken the effects of early-life stress, contextual risk, and parenting on children’s internalizing and externalizing problems (de Maat et al., 2022; Lengua et al., 2008; Northerner et al., 2016; Zarra-Nezhad et al., 2014). Longitudinal evidence further suggests that children’s social–emotional difficulties may, in turn, shape later parenting, particularly when children exhibit higher social withdrawal (Zarra-Nezhad et al., 2022).
Three theoretical models guide our understanding of temperament–environment interactions. The diathesis–stress model (Belsky & Pluess, 2009) proposes that traits such as high negative affectivity and low effortful control increase vulnerability under adversity, elevating risk for internalizing and externalizing problems (Brajsa-Zganec, 2014; Lengua et al., 2008; Northerner et al., 2016; Salley et al., 2013). Although broader frameworks such as differential susceptibility (Belsky & Pluess, 2009; Pluess, 2015) and vantage sensitivity (Belsky & Pluess, 2009; Pluess & Belsky, 2013) suggest that some children are more responsive to both negative and positive environments, the present study is primarily grounded in the diathesis–stress perspective, given its emphasis on vulnerability under adverse conditions.
Because temperament shows moderate to high stability across childhood, early profiles can serve as useful markers for risk assessment and prevention (Kopala-Sibley et al., 2018; Rothbart & Bates, 2006). Identifying children who are high in negative affectivity or low in effortful control may help clinicians, educators, and other professionals recognize those who are more likely to experience difficulties under stress and who may benefit from closer monitoring and early emotional support (Kozlova et al., 2020). At the same time, temperament-related processes such as effortful control and other self-regulatory skills remain shaped by caregiving and environmental experiences and can be strengthened through parenting, educational, and self-regulation-focused interventions (Muir et al., 2023). Thus, understanding the role of child temperament is important not only for describing individual differences but also for informing targeted support strategies that aim to promote children’s resilience in the face of parental distress and other societal crises.
Most research to date has examined more localized adversities (e.g., parenting behaviors, socioeconomic risk) rather than the widespread, multifaceted, and prolonged stressors of the COVID-19 pandemic (de Maat et al., 2022; Lengua et al., 2008; Northerner et al., 2016). Findings are mixed regarding which traits confer risk or protection. For instance, while some research suggests that low surgency and high effortful control may buffer against behavioral problems, other studies have reported null or inconsistent associations (de Maat et al., 2022; Lengua et al., 2008; Northerner et al., 2016). Moreover, little work has examined whether temperament moderates children’s responses to multiple, cumulative, COVID-19–related stressors. Given the magnitude and unpredictability of COVID-19 and its substantial impact on parental well-being, understanding temperament-based vulnerability is essential for identifying which children may require additional support during future crises.
The Present Study
The current preregistered study extends on an earlier work by Nolvi et al. (2023) and closely follows its analytical approach. That study examined the trajectory of children’s social-emotional symptoms during the COVID-19 pandemic, finding that symptoms initially increased but later stabilized, with parental distress mediating the effects of COVID-19–related stressors. That study did not examine whether children’s pre-existing individual differences shaped their responses to prolonged stress. We addressed this gap by testing whether temperament assessed at age 2.5 moderates associations between parental distress, COVID-19–related stressors, and children’s social-emotional functioning from ages 5 to 9. Using reports from both mothers and fathers across five pandemic follow-ups, we examined how all three core temperament dimensions interact with cumulative stressors, providing new insights into mechanisms of vulnerability and resilience during large-scale crises.
Drawing on the diathesis–stress model (Belsky & Pluess, 2009), we addressed two research questions (RQs) and pre-registered the following hypotheses:
Methods
Our study hypotheses, methods, and analysis plan were preregistered on the Open Science Framework (https://osf.io/k8ge4/overview?view_only=aad6c64369cc43efae74dfa32b2dad82). Any deviations from the preregistered methodology are marked throughout the paper.
Participants
Participants were drawn from the FinnBrain Birth Cohort Study, which originally enrolled 3,808 families between December 2011 and April 2015 via maternal welfare clinics in Turku and the Åland Islands, Finland (Karlsson et al., 2018). Following the COVID-19 outbreak on February 28, 2020, all parents were invited to complete an electronic questionnaire in May 2020 to assess parental distress, COVID-19–related stressors, and children’s social-emotional functioning. Our sample comprised 1,305 children (46% girls; up to age 9) for whom data were available from mothers or fathers on (a) parental distress and/or SDQ when children were 4–5 years old, (b) child temperament at 2.5 years, and (c) at least one COVID-19 follow-up. Beginning in May 2020 (T1) and continuing in September 2020 (T2), December 2020 (T3), March 2021 (T4), and June 2021 (T5), parents completed online surveys assessing COVID-19–related stressors, child social-emotional functioning, and ongoing parental distress. In total, 568 children had parent-reported social-emotional outcomes at one or more of these follow-ups (528 reports at T1, 452 at T2, 398 at T3, 324 at T5; see Appendix Table A1 and Figure A1 for detailed distributions and longitudinal data across multiple time points).
Compared to the baseline cohort, parents who responded to the pandemic follow-up questionnaires were significantly older (p < .001) and more highly educated (p < .001) than non-respondents. Among mothers, respondents reported greater economic satisfaction at baseline (p < .001) and fewer depressive symptoms during the first and second trimesters of pregnancy (p < .002), though no differences were observed in postnatal depressive symptoms. No corresponding differences were found among fathers. At the pandemic baseline (T1), no significant differences were observed between follow-up participants and non-participants in age, education, economic satisfaction, depressive or anxiety symptoms, or exposure to COVID-19–related stressful events. More detailed attrition analyses can be found in Appendix Table A1.
Parental education (recorded during pregnancy) and child biological sex (at birth) served as covariates in all analyses. This multi-informant, longitudinal design allowed us to model pre-pandemic baseline functioning alongside changes across five pandemic time points while accounting for age-related trends. Family sociodemographic details (Table A2) and participant attrition analysis are provided in the Appendix. All parents provided written informed consent for data acquisition from the Well-being Services County of Southwest Finland (VARHA) records as part of the FinnBrain research. The study protocols were approved by the Ethics Committee of the Hospital District of Southwest Finland (approvals 57/180/2011 §168 and #17/1802/2020), in accordance with the Declaration of Helsinki.
Measures
The descriptive statistics of the child’s social-emotional functioning and temperament are reported in Table A3 in the Appendix. The scales were used as continuous measures in the present study.
Child Social-Emotional Functioning
The assessment of social-emotional functioning (T1, T2, T3, T5; child outcome data unavailable at T4) utilized the Strengths and Difficulties Questionnaire (SDQ), a validated and reliable tool for evaluating social-emotional well-being in children aged from 3 to 16 years (Goodman, 1997). The SDQ comprises 25 items, including a total difficulties scale made up of 20 items across four subscales: emotional problems (e.g., “many fears and easily scared”), conduct problems (e.g., “often fights with other children or bullies them”), hyperactivity (e.g., “restless, overactive, and cannot stay still for long”), peer relationship problems (e.g., “rather solitary and tends to play alone”), plus a 5-item prosocial behavior scale (e.g., “shares readily with other children”). Items are rated by parents on a 3-point Likert-type scale (0 = not true, 1 = somewhat true, 2 = certainly true), with higher scores indicating more symptoms, except for the prosocial scale, where higher scores indicate better skills. In our study, most scales showed acceptable to high internal consistency: total difficulties (Cronbach’s alpha .77–.81 for mothers, .73–.80 for fathers), conduct problems (.66–.70 for mothers, .65–.75 for fathers), hyperactivity (.77–.82 for mothers, .71–.78 for fathers), and prosocial behaviors (.68–.73 for mothers, .63–.71 for fathers). Although the emotional symptoms (.47–.62 for mothers, .34–.74 for fathers) and peer relationship problems (.46–.78 for mothers, .33–.54 for fathers) subscales showed lower internal consistency, consistent with previous Nordic studies (Smedje et al., 1999), all SDQ subscales were retained in the analyses to allow comparability with established literature and because the total difficulties score demonstrated acceptable reliability. Results for these two subscales were interpreted with caution, while the total difficulties score served as the primary outcome due to its acceptable reliability.
Child Temperament
At age 2.5, children’s temperament was assessed using Rothbart’s Early Childhood Behavior Questionnaire (ECBQ; Putnam et al., 2001), completed by mothers and fathers. The ECBQ, with 107 items, measures temperament in children aged 18 to 36 months using a 7-point Likert-type scale (1 = never to 7 = always). Parents reported the frequency of specific behaviors observed in the past two weeks, and higher scores indicate a greater presence of each temperament trait. The ECBQ categorizes temperament into three main dimensions: negative affectivity (e.g., “gets easily upset”), surgency (e.g., “approaches new situations with enthusiasm”), and effortful control (e.g., “is able to wait patiently for a desired activity”). In our study, internal consistency for all scales was high (.86 for mothers, .90 for fathers for negative affectivity, .82 for mothers, .79 for fathers for surgency, .85 for mothers, and .87 for fathers for effortful control). Temperament measured at age 2.5 was used as an early indicator of stable individual differences in emotional reactivity and regulation.
Parental Distress: Anxiety and Depressive Symptoms
Parental anxiety was assessed before (children aged 4–5) and during the pandemic (T1–T5) using the 10-item anxiety subscale of the Symptom Checklist-90 (SCL-90), which includes items such as “nervousness or shakiness inside,” rated on a 4 point scale (1 = not at all to 4 = extremely) and total scores ranging from 0 to 50 (Derogatis et al., 1973).
Parental depression was evaluated using the Edinburgh Postnatal Depression Scale (EPDS) (Matijasevich et al., 2014), which consists of 10 items such as “I have felt sad or miserable,” rated on a 4 point scale (0 = not at all to 3 = most of the time), with scores up to 30; a score of 10 or above suggests potential depression. Both parents responded to each COVID-19 follow-up stage. In our sample, internal consistency was strong (for mothers, .85–.88 for the EPDS and .84–.88 for the SCL-90; for fathers, .78–.89 for the EPDS and .80–.84 for the SCL-90). For the statistical analyses, we created an individual parental distress score for each parent by standardizing and summing that parent’s EPDS and SCL-90 scores and then standardizing the resulting sum. This yielded one distress score for mothers and one for fathers. These parent-specific distress scores were included separately in the statistical models, and for each SDQ report, the distress score from the reporting parent (mother or father) was used.
COVID-19–Related Stressors
COVID‑19–related stressors (CovEvents) were assessed at T1–T5 using a 43-item yes/no questionnaire adapted from the Severe Acute Respiratory Syndrome (SARS)-related stressor measure (Main et al., 2011) and further modified for the COVID-19 context (Lindblom et al., 2024). The checklist covered multiple domains, including health-related issues (e.g., COVID-19 symptoms, treatment, hospitalization; maximum 24 items), social and leisure restrictions (e.g., quarantine, canceled activities; maximum 12 items), and financial challenges (e.g., job loss, economic difficulties; maximum 7 items). A summary of these domains and their relative frequencies across follow-up points is presented in Appendix Table A1. Because these domains represent distinct but relevant sources of pandemic-related adversity, and our conceptual interest was in the overall burden of stress on families rather than the unique effects of specific subdomains, we created a composite index treating these stressors as formative indicators of cumulative pandemic-related stress. This approach is consistent with previous FinnBrain studies using this measure (Lindblom et al., 2024; Nolvi et al., 2023) and with established cumulative stress frameworks such as the Holmes and Rahe Stress Scale (T. H. Holmes & Rahe, 1967).
The number and content of items varied slightly across time points (e.g., only health-related events were assessed at T2); therefore, composite scores at each wave were standardized before inclusion in analyses to ensure comparability across time.
Covariates
The analyses were controlled for the child’s sex (binary, obtained from the regional health records maintained by the well-being Services County of Southwest Finland, VARHA), rater parent (mother vs. father/spouse or parent who did not give birth), parental education, school attendance (estimated based on child age, > 7), the answering date of the questionnaires (baseline and COVID-19 follow-ups), and the age of the child. For the questionnaire answering date, we used a piecewise linear function with breakpoints at T0 (February 2020), T1, T2, T3, and T5. These breakpoints correspond to the data collection time points of the COVID-19 questionnaires. A piecewise linear function models time as separate linear segments between breakpoints, allowing the slope to vary within each segment. A similar approach was applied to child age, with breakpoints set at 5, 6, and 7 years.
Statistical Analyses
The analyses were conducted using R 4.0.5 ( R: The R Project for Statistical Computing , n.d.). Mixed models were fitted using the lmer function in the R package lme4 (Bates et al., 2015). Bootstrap intervals were calculated because the distribution of models’ residuals was skewed. For the linear models, the 95% Bca confidence intervals (Efron, 1987) were calculated using 5000 bootstrap samples. For the linear mixed-effects models, bootstrap samples (3000) were used to calculate 95% percentile intervals. Missing data in covariates were handled using multiple imputation (MI) procedures by chained equations (van Buuren & Groothuis-Oudshoorn, 2011). Outcome variables (SDQ scores) and temperament predictors were not imputed; instead, all available observations were retained in the mixed-effects models, which can accommodate missing outcome data under MAR assumptions. Unstandardized (b) and standardized (β) regression coefficients are reported alongside their 95% confidence intervals. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cohort studies v4 was followed in reporting. Model formulas are presented in the Appendix.
RQ1: Child Temperament and Social-Emotional Functioning Before and During the Pandemic
First, we analyzed how children’s temperament was related to social–emotional functioning before and during the COVID-19 pandemic (RQ1) using linear mixed-effects models. The SDQ total score and each subfactor were used as outcome variables in separate models. All available SDQ time points were included. Each child’s temperament dimension was entered as the main explanatory variable in separate models. All models were adjusted for the covariates described in the Covariates section. The model included child-level random intercepts and, where supported by model fit, child-level random slopes for questionnaire answering time and the responding parent (mother vs. father). Next, a stepwise analysis was conducted (not preregistered), extending the initial model from RQ1 by incorporating additional covariates to further explore the relationships within a longitudinal framework. Parental distress (combination of depressive and anxiety symptoms), examined separately for mothers and fathers, and COVID-19–related stressors were added to the model separately (Models 1a and 1b) and jointly (Model 1c) to better understand their impact on the associations between children’s temperament and social–emotional functioning.
RQ2a: Temperament as a Moderator of COVID-19–Related Stressors and Children’s Social-Emotional Functioning During the Pandemic
Next, we examined how temperament mitigated or exacerbated the effects of COVID-19–related stressors and parental distress on children’s social–emotional functioning across the pandemic follow-ups, from ages 5 to 9 (RQ2). Mixed-effects models were run separately for each COVID-19 follow-up time point (T1–T5, excluding T4) using cross-sectional data. Model 2a included child temperament, COVID-19–related stressors, and their interaction as predictors of SDQ total scores and subfactors (tested one at a time). All models were adjusted for the covariates described in the Covariates section. A random intercept was included for each child. Mixed-effects models were used because each child could have multiple SDQ reports (from both parents or one), requiring the nesting of observations within children. Due to low responses from fathers, we also analyzed cross-sectional linear regressions only using the answers that mothers had reported, using a similar model formula as described above. We additionally analyzed the mean values of SDQ and COVID-19–related stressors over the whole study period using simple linear models (not preregistered). Model 2c (detailed in the Appendix) extended the RQ2 model to test whether this approach yielded different results from Model 2a (see Table A5). Due to low responses from fathers, only mothers’ answers were analyzed.
RQ2b: Temperament as a Moderator of Parental Distress and Children’s Social-Emotional Functioning During the Pandemic
Similar models were used as described above, except that the interaction term was specified between parental distress and individual temperament dimensions (Model 2b). Parental distress was included as a variable that corresponds to the parent who reported the SDQ. That is, if the SDQ report was from the father, paternal distress was used; if from the mother, maternal distress was used. Due to low responses from fathers, we also analyzed cross-sectional linear regressions only using the answers that mothers had reported, using a similar model formula as described above. We additionally analyzed the mean values of SDQ and parental distress over the whole study period using simple linear models (not preregistered, detailed in Appendix, see Table A5 and Figure A2). Due to low responses from fathers, only mothers’ answers were analyzed.
P-value Adjustments
In Models 2a and 2b, because multiple time points were tested and the SDQ subscales were treated as exploratory, post hoc analyses, p-values were adjusted using the Holm–Bonferroni method (Holm, 1979); however, because both exposures and outcomes (total score and subscales) are inherently correlated, this correction may be overly conservative.
Detailed model formulas and additional analytic outputs are provided in the Appendix.
Results
Descriptive Statistics
Descriptive statistics of the participating children are provided in Tables A2 and A3 in the Appendix. The overall data collection process and participant inclusion across time points are illustrated in Figure A1. All main analyses examining associations between temperament dimensions and social-emotional functioning were conducted using the maximum sample of 1,305 children with available data. When testing the moderating effects of parental distress and COVID-19–related stressors, analyses were conducted cross-sectionally at each follow-up time point, using the available sample for that specific wave.
RQ1: Main Effects of Temperament on Social–Emotional Functioning
Child Temperament and Social-Emotional Functioning Before and During the Pandemic
The associations between temperament dimensions and children’s social-emotional functioning across the whole study period, including baseline measurements at ages 4 and 5 and follow-ups during the COVID-19 pandemic (T1–T5, excluding T4), are presented in Table 1 (RQ1). After controlling for the covariates and the questionnaire answering date, effortful control was associated with fewer total social-emotional difficulties and fewer symptoms across all four subscales (emotional symptoms, conduct problems, hyperactivity, and peer relationship problems), while being positively associated with prosocial behaviors. Surgency was negatively correlated with emotional symptoms and peer relationship problems but positively correlated with conduct problems, hyperactivity, and prosocial behaviors. Negative affectivity was positively associated with total social-emotional difficulties and all four subscales but negatively associated with prosocial behavior.
Association Between Child Temperament and Social-Emotional Functioning Before and During the Pandemic.
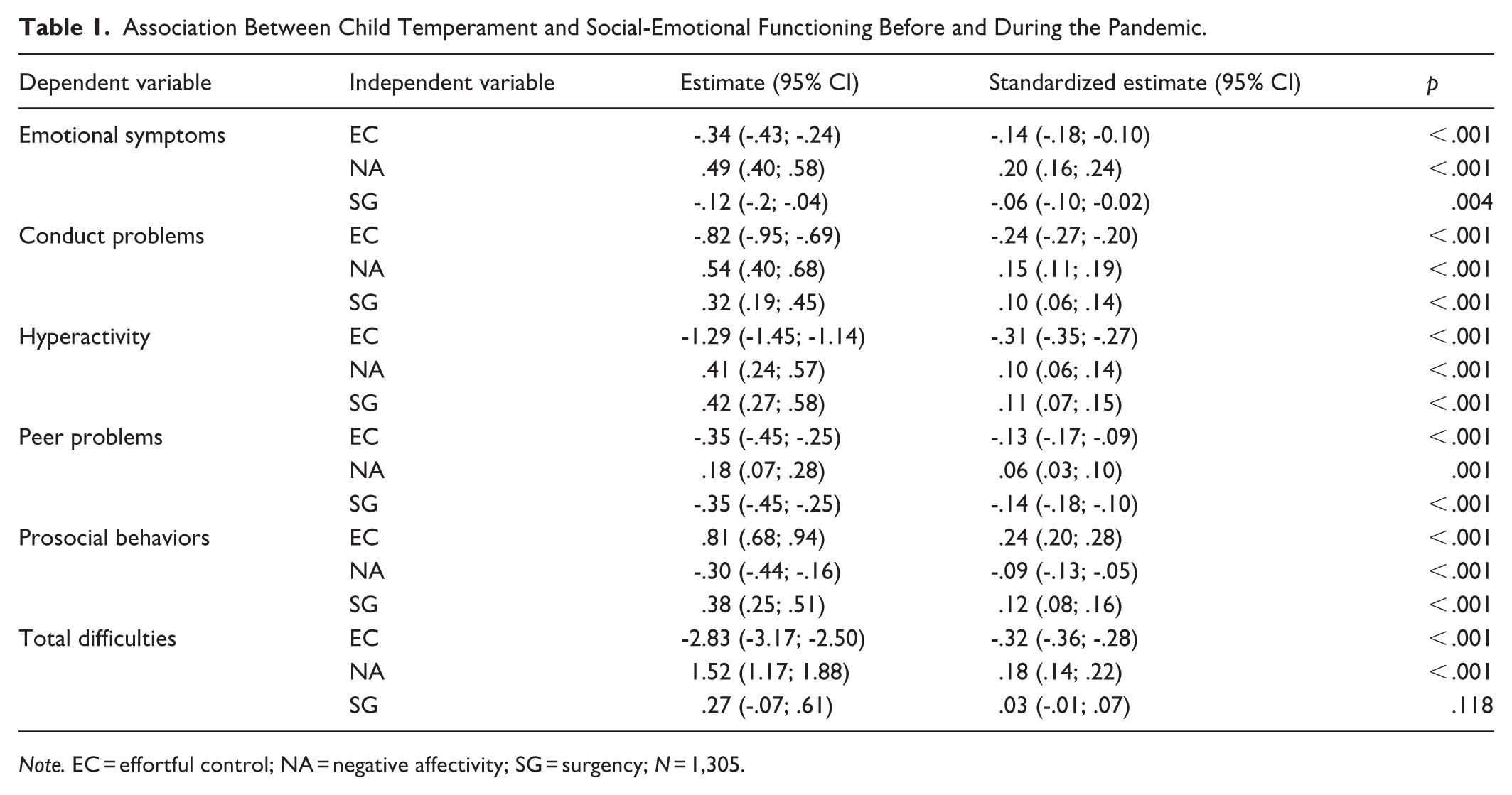
Note. EC = effortful control; NA = negative affectivity; SG = surgency; N = 1,305.
Adding parental distress (not preregistered) preserved the direction of the relationships between children’s temperament and social-emotional functioning, though the effect sizes slightly decreased. Introducing COVID-19–related stressors did not significantly change the direction, magnitude, or significance of these relationships. When both parental distress and COVID-19–related stressors were included in one model, the original direction and significance were maintained, but there was a slight reduction in the effects (see Table A4 in the Appendix).
RQ2a: Moderation by COVID-19–Related Stressors
The Moderating Effect of Temperament on the Association Between COVID-19–Related Stressors and Child Social-Emotional Functioning During the Pandemic
All analyses were adjusted for covariates and corrected for Holm-corrected multiple-comparison procedures (RQ2). Table 2 presents only those interactions that survived correction, while the full set of findings is available in Appendix Table A5. A significant interaction was found at T1 (May 2020) for emotional symptoms, indicating that negative affectivity moderated the association between COVID-19–related stressors and emotional symptoms (Table 2, Figure 1(a)). At high levels of negative affectivity (+ 1 SD), higher COVID-19–related stressors were significantly associated with more emotional symptoms (b = .08, 95% CI [.02, .14], p = .006). In contrast, at low levels of negative affectivity (–1 SD), this association was not statistically significant (b = –.02, 95% CI [–.09, .04], p = .487). This pattern suggests that children high in negative affectivity may be particularly vulnerable to emotional difficulties under conditions of elevated stress.
Moderating Effect of Temperament on the Association Between COVID-19–Related Stressors and Child Social-Emotional Functioning.
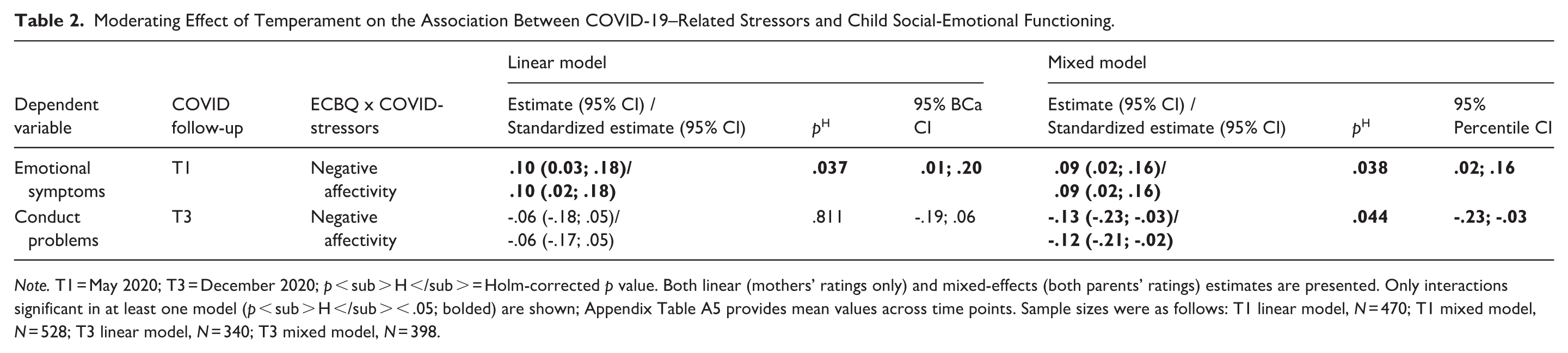
Note. T1 = May 2020; T3 = December 2020; p < sub > H </sub > = Holm-corrected p value. Both linear (mothers’ ratings only) and mixed-effects (both parents’ ratings) estimates are presented. Only interactions significant in at least one model (p < sub > H </sub > < .05; bolded) are shown; Appendix Table A5 provides mean values across time points. Sample sizes were as follows: T1 linear model, N = 470; T1 mixed model, N = 528; T3 linear model, N = 340; T3 mixed model, N = 398.
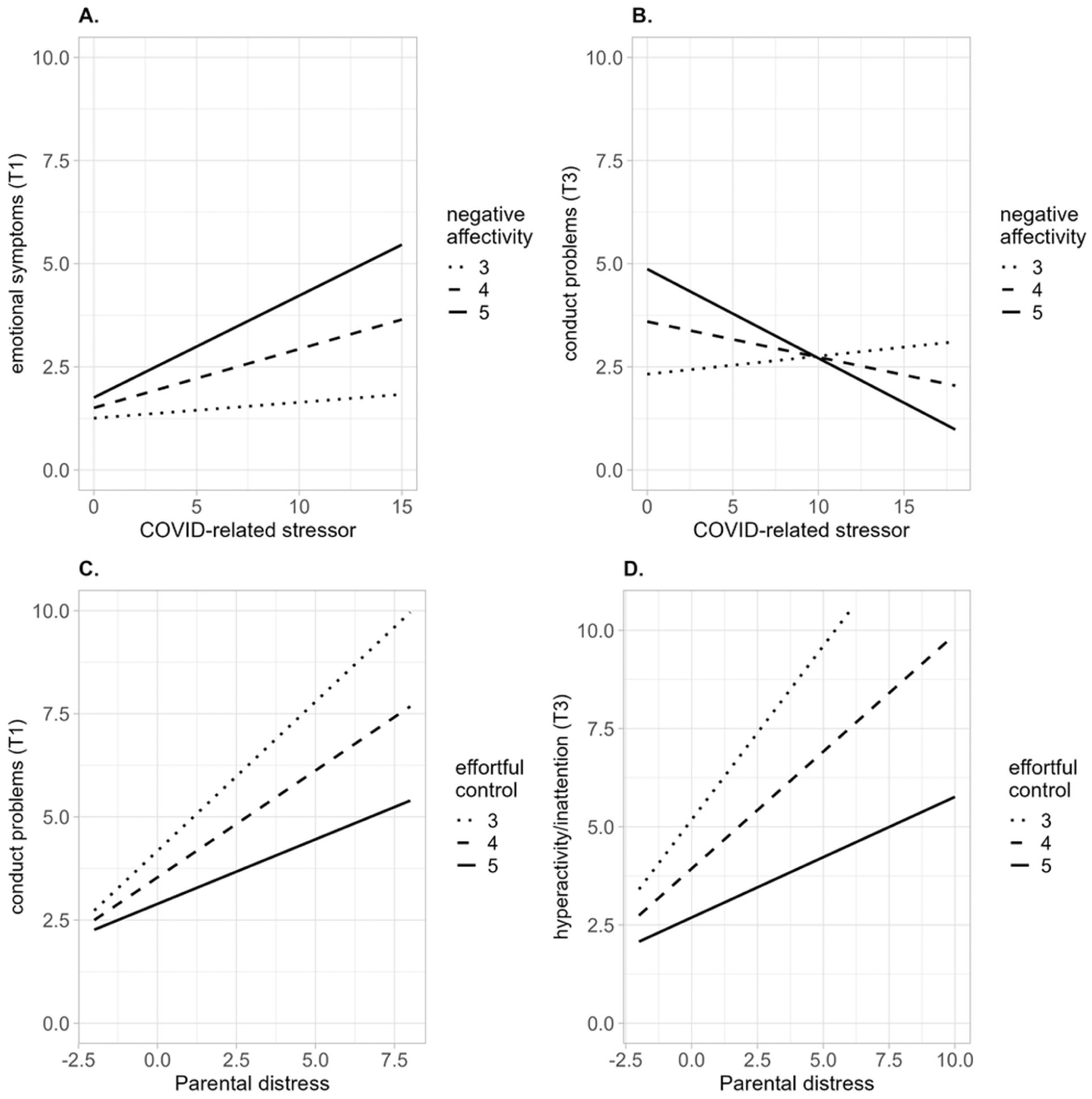
Moderating Effect of Temperament on the Association Between COVID-19–Related Stressors, Parental Distress, and Child Social-Emotional Functioning. For illustrative purposes, simple slopes were estimated at temperament values of 3, 4, and 5 on negative affectivity and effortful control. Sample sizes were T1, N = 528; T3, N = 398.
Further, a significant interaction was also observed at T3 (December 2020) between negative affectivity and COVID-19–related stressors in predicting conduct problems (Table 2, Figure 1(b)). At low levels of negative affectivity (–1 SD), higher COVID-19–related stress was significantly associated with more conduct problems (b = .13, 95% CI [.04, .21], p = .003). In contrast, at high levels of negative affectivity (+ 1 SD), the association was substantially weaker and not statistically significant (b = –.02, 95% CI [–.09, .06], p = .661), with a trend in the opposite direction. This pattern suggests that low negative affectivity may confer greater vulnerability to stress-related increases in conduct problems, whereas high negative affectivity may play a protective role under prolonged stress.
RQ2b: Moderation by Parental Distress
The Moderating Effect of Child Temperament on the Association Between Parental Distress and Child Social-Emotional Functioning During the Pandemic
All analyses were adjusted for covariates and corrected for Holm-corrected multiple-comparison procedures (RQ2). Table 3 presents only the interactions that were statistically significant after correction; the full results are shown in Appendix Table A5. A significant interaction was observed at T1 (May 2020) between effortful control and parental distress in predicting conduct problems (Table 3, Figure 1(c)). At low levels of effortful control (–1 SD), higher parental distress was strongly associated with increased conduct problems (b = .43, 95% CI [.32, .54], p < .001). At high levels of effortful control (+ 1 SD), the association remained statistically significant but was substantially weaker (b = .20, 95% CI [.10, .30], p < .001). This pattern suggests that higher effortful control reduces the impact of parental distress on conduct problems, indicating a protective role during the early stages of the pandemic.
Moderating Effect of Temperament on the Association Between Parental Distress and Child Social-Emotional Functioning.
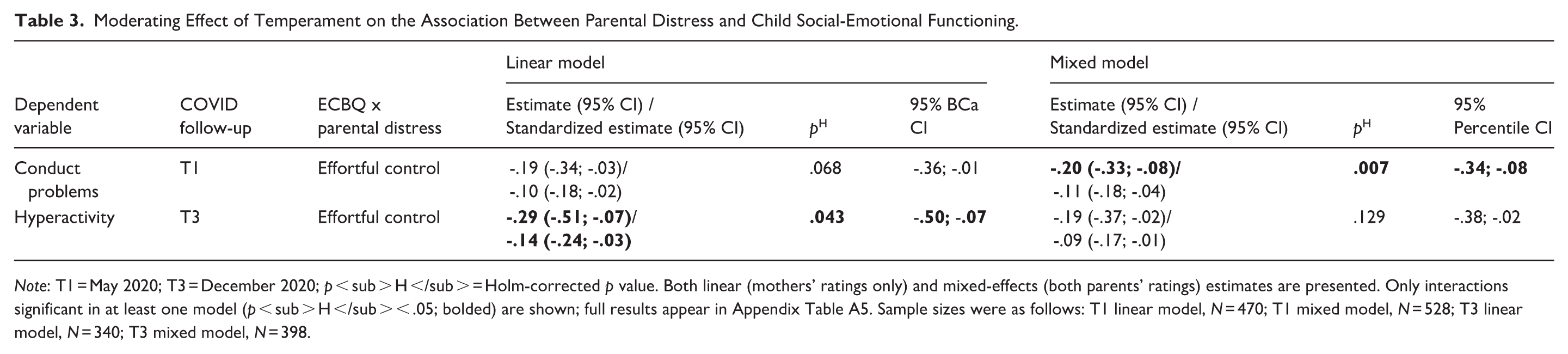
Note: T1 = May 2020; T3 = December 2020; p < sub > H </sub > = Holm-corrected p value. Both linear (mothers’ ratings only) and mixed-effects (both parents’ ratings) estimates are presented. Only interactions significant in at least one model (p < sub > H </sub > < .05; bolded) are shown; full results appear in Appendix Table A5. Sample sizes were as follows: T1 linear model, N = 470; T1 mixed model, N = 528; T3 linear model, N = 340; T3 mixed model, N = 398.
A similar interaction was observed at T3 (December 2020) in predicting hyperactivity (Table 3, Figure 1(d)). At low levels of effortful control (–1 SD), parental distress was again strongly associated with more hyperactivity symptoms (b = .46, 95% CI [.30, .62], p < .001). In contrast, at high levels of effortful control (+ 1 SD), the association was substantially weaker and did not reach statistical significance (b = .15, 95% CI [-.01; .31], p = .059). This pattern indicates that effortful control may have reduced the impact of parental distress on hyperactivity symptoms over time, highlighting its potential as a regulatory buffer in prolonged stress contexts.
Discussion
This study highlights the crucial role of early childhood temperament in shaping social-emotional functioning during the COVID-19 pandemic, particularly through its interaction with parental distress and COVID-19–related stressors. As expected (H1), higher effortful control was consistently linked to fewer social-emotional difficulties and greater prosocial behavior, whereas higher negative affectivity predicted more difficulties and lower prosociality. Surgency showed a mixed pattern, relating to fewer emotional and peer problems but more conduct and hyperactivity symptoms. We also found partial support for H2, revealing that temperament moderated the impact of environmental stressors at specific phases of the pandemic. At T1 (May 2020), higher negative affectivity amplified the effects of COVID-19–related stressors on emotional symptoms, whereas at T3 (December 2020), lower negative affectivity unexpectedly predicted stronger links between stressors and conduct problems. Effortful control moderated the effects of parental distress as well: at T1, children low in effortful control showed a stronger association between parental distress and conduct problems, and at T3, a similar pattern emerged for hyperactivity. Contrary to expectations, surgency did not moderate associations between stressors and outcomes.
Our findings align with previous studies (Brajsa-Zganec, 2014; Northerner et al., 2016) showing that high effortful control functions as a robust protective factor, associated with fewer internalizing and externalizing problems and greater prosocial behaviors. This pattern underscores the role of self-regulation in managing behavior, mitigating emotional distress, and supporting positive social interactions. Surgency showed a divergent pattern: higher surgency was linked to fewer emotional and peer problems but also to elevated conduct problems, hyperactivity, and prosocial behavior. This combination reflects the dual nature of surgency, characterized by sociability and positive emotionality on the one hand, and impulsivity and high activity levels on the other, which can lower risk for internalizing symptoms while increasing externalizing tendencies (de Maat et al., 2022; Northerner et al., 2016). As in prior Nordic studies, the emotional symptoms and peer problems subscales showed lower reliability (Smedje et al., 1999); therefore, interpretations of these outcomes were made cautiously, and the total difficulties score served as our primary indicator of overall functioning.
High negative affectivity was, as expected, linked to greater social-emotional difficulties, consistent with the literature (Brajsa-Zganec, 2014; Northerner et al., 2016). Children high in negative affectivity are prone to emotional and behavioral challenges, likely due to their heightened sensitivity to stress and difficulty regulating negative emotions. Interestingly, higher negative affectivity was also related to greater prosocial behavior. This may reflect a complex dynamic where emotionally reactive children, despite challenges, engage in prosocial actions as a compensatory mechanism or due to heightened emotional awareness, potentially linked to environmental sensitivity (Pluess, 2015).
Importantly, temperament not only predicted overall levels of social-emotional functioning but also moderated the impact of environmental stressors. Even when accounting for parental distress and COVID-19–related stressors, temperament remained a significant contributor to children’s adjustment, consistent with prior evidence demonstrating that temperament shapes sensitivity to environmental influences (de Maat et al., 2022; Lengua et al., 2008; Masten, 2021; Northerner et al., 2016; Slagt et al., 2016; Zarra-Nezhad et al., 2014). The presence of both amplifying and buffering effects in our results underscores the critical role of temperament in shaping children’s responses to stress. These combined amplifying and buffering effects highlight the importance of individual differences in children’s responses to stress and have direct implications for tailoring prevention and intervention strategies.
After multiple-comparison corrections, high negative affectivity emerged as a vulnerability factor early in the pandemic (T1), when emotional symptoms increased more steeply in response to COVID-19–related stressors. This finding aligns with the diathesis–stress model (Belsky & Pluess, 2009) and prior evidence showing that children high in negative affectivity are especially susceptible to the effects of cumulative or contextual stress (Northerner et al., 2016; Slagt et al., 2016). Although emotional symptoms had lower reliability, this pattern is theoretically coherent and suggests that children with high emotional reactivity may need targeted support during acute societal disruptions. Children with low negative affectivity showed no significant increase in emotional symptoms under early pandemic stress, indicating resilience during the initial crisis period.
By the mid-pandemic period (T3), however, moderation patterns shifted: unexpectedly, children low in negative affectivity showed stronger links between COVID-19–related stressors and conduct problems, whereas no such increase was observed among highly reactive children. This exploratory finding, observed at one time point and not preregistered, should be interpreted with caution. One possibility is that children low in negative affectivity, who typically show low emotional reactivity, may rely more heavily on external structure and routine—both of which were substantially disrupted in late 2020. In contrast, children high in negative affectivity may have benefited from increased parental attention or previously developed coping strategies. Heightened family presence during lockdowns may have provided the structure and support needed to buffer behavioral problems in these children. Although the pattern superficially resembles the differential susceptibility model (Belsky & Pluess, 2009), we cannot evaluate “for better” responsiveness because positive environmental contexts were not assessed. Instead, these findings may reflect domain-specific sensitivity, where negative affectivity predicts vulnerability to emotional symptoms such as fear and uncertainty (as seen early in the pandemic), but not necessarily to externalizing behaviors. Further research is needed to determine whether this pattern generalizes to other forms of sustained stress.
Effortful control also moderated the impact of parental distress, supporting its role as a protective factor for externalizing symptoms. At T1, parental distress was strongly associated with conduct problems among children with low effortful control, whereas this association was notably weaker among those with high effortful control. A similar pattern emerged at T3 for hyperactivity. This aligns with the diathesis–stress model (Belsky & Pluess, 2009) and prior evidence showing that children with stronger self-regulatory skills cope more effectively with stressors, particularly those involving disruptions in family functioning (Lengua et al., 2008; Masten, 2021). Because effortful control is modifiable, these findings highlight a promising target for early intervention, especially for families exposed to heightened stress.
Notably, the strongest moderation effects occurred at time points when pandemic measures were most stringent in Finland—spring 2020 and December 2020 (Hale et al., 2021). These periods involved intensified social restrictions and heightened uncertainty, suggesting that temperament-related vulnerabilities become most apparent under acute or prolonged stress. Our results underscore the importance of considering the pandemic’s unprecedented challenges in current and future research. This aligns with broader research priorities during and after major societal disruptions, including documenting mental health impacts, assessing long-term consequences, identifying risk and resilience factors, and guiding interventions (Wade et al., 2023). Our findings underscore the importance of considering the societal context when interpreting children’s adjustment. Finland’s relatively moderate restrictions and robust social support systems may have buffered some adverse effects, and caution is warranted in generalizing to settings where disruptions were more severe. Nevertheless, the processes identified here likely extend beyond COVID-19 and may apply to other large-scale crises, such as economic downturns or natural disasters.
Finally, the absence of moderation effects for surgency can be better understood in light of the functional characteristics of this trait. Surgency combines sociability and positive emotionality with impulsivity and high behavioral activation; these competing tendencies may counterbalance each other, reducing the likelihood of consistent interaction effects under adverse conditions. Moreover, if surgency operates partly as a vantage-sensitivity trait (Pluess & Belsky, 2013), its moderating effects may emerge only in contexts involving clear environmental benefits, which were not included in the present study. These considerations may help explain why surgency did not moderate associations with either parental distress or COVID-19–related stressors.
This study has several limitations. First, it relies solely on parental reports for child temperament, social-emotional functioning, and COVID-19–related stressors, which may introduce reporter bias, although this limitation is partly mitigated by the inclusion of paternal reports despite their lower participation. Second, sample size decreased across follow-up waves, reducing statistical power; however, the repeated-measures design helps offset this concern by leveraging multiple observations per child. Third, our findings are drawn from a general population sample with relatively low levels of symptoms, which may limit generalizability to children with more severe mental health difficulties. Fourth, the emotional symptoms and peer relationship problems subscales of the SDQ showed low internal consistency, particularly in fathers’ reports, which is consistent with previous Nordic studies (Smedje et al., 1999); therefore, results based on these subscales should be interpreted cautiously.
The study also has notable strengths. We investigated all three key temperament dimensions—negative affectivity, effortful control, and surgency—including the less-studied role of surgency in stress responses, for which previous findings have been mixed (de Maat et al., 2022; Northerner et al., 2016). Our focus on both risk and adaptive processes provides valuable insights for identifying points of intervention. Additional strengths include the use of data from both mothers and fathers and a large longitudinal cohort. Temperament was assessed in toddlerhood, when traits can be reliably measured, and importantly, these assessments were conducted several years before the pandemic, ensuring that temperament reflects pre-existing individual differences rather than responses to COVID-19–related stressors. Further strengths include preregistration of hypotheses and rigorous correction for multiple comparisons. Finally, by leveraging naturally occurring variation during the COVID-19 pandemic, the study offers a unique opportunity to examine how temperament interacts with environmental stressors and family context to shape children’s social-emotional development.
Conclusion
This study underscores the critical role of early childhood temperament in both predicting social-emotional functioning during the COVID-19 pandemic and moderating the impact of environmental stressors. Consistent with the diathesis–stress model (Belsky & Pluess, 2009), traits such as negative affectivity and effortful control shaped children’s vulnerability or resilience in the face of adversity. From an applied perspective, our findings highlight the value of supporting effortful control and other self-regulatory skills in early childhood, reducing parental distress through accessible family support services, and providing targeted emotional support for children high in negative affectivity. Tailoring prevention and intervention efforts to children’s temperamental profiles and family circumstances may help promote emotional well-being and buffer against the negative effects of sustained adversity, both during pandemics and in other societal crises.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254261430624 – Supplemental material for The Moderating Role of Child Temperament in the Face of Parental Distress During Covid-19: Associations with Long-Term Social-Emotional Functioning
Supplemental material, sj-docx-1-jbd-10.1177_01650254261430624 for The Moderating Role of Child Temperament in the Face of Parental Distress During Covid-19: Associations with Long-Term Social-Emotional Functioning by Maryam Zarra-Nezhad, Laura Perasto, Katja Tervahartiala, Jallu Lindblom, Jetro J. Tuulari, Max Karukivi, Noona Kiuru, Linnea Karlsson, Hasse Karlsson, Riikka Korja and Saara Nolvi in International Journal of Behavioral Development
Footnotes
Acknowledgements
We thank the FinnBrain Study participants and personnel for their invaluable efforts in conducting this study.
Ethical Considerations
The study protocol was approved by the Ethics Committee of the Hospital District of Southwest Finland (approval nos. 57/180/2011 §168 and 17/1802/2020), in accordance with the Declaration of Helsinki.
Preregistration
Informed Consent
Written informed consent was obtained from all parents for participation in the FinnBrain study and for access to Well-being Services County of Southwest Finland (VARHA) records.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Research Council of Finland [grant numbers 346121 (Centre of Excellence in Learning Dynamics and Intervention Research), 358924 and 358947 (EDUCA Flagship, to Maryam Zarra-Nezhad), and 342748], the Strategic Research Council (SRC) within the Academy of Finland (352648, subproject 352655), the Juho Vainio Foundation, the Signe & Ane Gyllenberg Foundation, and State Research Funding from Turku University Hospital. The writing (review and editing) of this manuscript was supported by the Hospital District of Southwest Finland and Finnish State Grants for Clinical Research (VTR) awarded to Jetro J. Tuulari.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to Finnish national legislation, the data cannot be made publicly available. However, data may be shared through a Data Transfer Agreement as part of a research collaboration. Requests for collaboration should be directed to the Board of the FinnBrain Birth Cohort Study via Linnea Karlsson (
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.