
Abstract
Early-life family relationships have been linked to childhood emotional (internalising) and behavioural (externalising) problems and adolescent social functioning but developmental pathways between them remain underexplored. We examined whether trajectories of children’s internalising and externalising problems mediate between low-quality early family relationships and adolescent social outcomes, including interpersonal distrust and low perceived social support (perceived social isolation). Using a UK-representative cohort (
Introduction
Social functioning is a multi-dimensional domain of youth development (Dirks et al., 2007), becoming particularly salient during adolescence (Andrews et al., 2021) and associated with later health outcomes (Sawyer et al., 2012). Two key dimensions of social functioning are perceived social support and interpersonal trust. Defined as the perception of helpful, warm, and reliable interpersonal connections, perceived social support has been found to buffer against numerous physical and mental health challenges (Cohen & McKay, 2020; Taylor, 2011; Uchino et al., 2018). In adolescence, higher levels of perceived social support correlate with reduced risk of emotional disorders (Rueger et al., 2016), whereas low levels of perceived social support (i.e., a form of perceived social isolation) have been associated with increased likelihood of anxiety, depression, and many other psychological difficulties (Almeida et al., 2021; Auerbach et al., 2011; Fitzpatrick et al., 2024; Ren et al., 2018; Rueger et al., 2010; Stice et al., 2011; Väänänen et al., 2014). Related to, yet distinct from, perceived social isolation is interpersonal distrust – broadly defined as a lack of confidence in the motives, intentions, or reliability of others (Simpson, 2007). Though less studied, interpersonal distrust is recognised as a critical element in adolescent socioemotional development, closely related with perceptions of social threat (Bi et al., 2025; Clarke et al., 2021; Rotenberg, 2010; Tsomokos & Slavich, 2024; Wang et al., 2022). Its link with psychiatric symptoms has received much interest, however. For example, interpersonal distrust and depression are robustly associated during adolescence and young adulthood, both cross-sectionally and longitudinally (Kim et al., 2012; Tsomokos & Dunbar, 2023; Tsomokos & Slavich, 2024).
Most research to-date has investigated the prospective associations between impaired social functioning, including (perceived) social isolation and distrust, and poorer adolescent mental health (Almeida et al., 2021; Cohen & McKay, 2020; Patalay & Fitzsimons, 2018; Uchino et al., 2018), particularly internalising (i.e., emotional and relational) and externalising (behavioural and attentional) difficulties. There are two broad theoretical frameworks that can be used to understand these associations: the social causation hypothesis and social safety theory, which we discuss in turn.
The social causation hypothesis posits that the social environment – including socioeconomic conditions and social experiences – shapes health outcomes (Jin et al., 2020; Mossakowski, 2014; Ren et al., 2018; Wickham et al., 2017; Windle, 1992; Young et al., 2005) through various mechanisms. In adolescence, for instance, perceptions of social isolation and distrust towards others can erode coping resources and impede help-seeking, exacerbating internalising (emotional or relational) and externalising (behavioural or attentional) difficulties. In turn, these difficulties can undermine day-to-day social functioning (e.g., increasing risks for peer conflict and social withdrawal), setting up trajectories that culminate in poorer social outcomes. In the present study, we align this framework with our constructs by treating family relationships (mother–child and interparental relationship quality in early life) as core features of the child’s social environment that may shape childhood mental health trajectories and, ultimately, adolescent distrust and perceived social isolation.
From an evolutionary perspective, social safety theory emphasises the fundamental human need for relational security, bonding and belonging, positing that a sense of social safety (i.e., feeling protected, accepted, and supported within one’s social network) is critical for both physical and mental wellbeing (Slavich, 2020). When that perception of safety is undermined in some way – for instance, through social rejection and isolation, leading to deficits in trust or social support – an individual’s stress-response systems (including neuroendocrine and inflammatory pathways) are activated and, over time, these psychobiological adaptations may contribute to the development of mental health difficulties (Allen et al., 2021; Slavich et al., 2010, 2023; Tsomokos & Slavich, 2024). In this study, we start from the premise that higher-quality mother–child and interparental bonds should cultivate children’s felt safety, which then lowers levels of internalising and externalising symptoms and, by buffering against threat sensitivity and dysregulated behaviour, reduces the sense of distrust and perceived social isolation in adolescence.
Extant research has mostly mapped how adverse social experiences (including perceived social isolation and distrust) contribute to mental health problems. By contrast, the reverse pathway appears not to have been investigated sufficiently in longitudinal studies: whether earlier (e.g., childhood) trajectories of internalising or externalising problems predict subsequent (e.g., adolescent) interpersonal distrust and perceived social isolation. This matters as internalising difficulties can bias threat appraisal and promote withdrawal, whereas externalising difficulties can provoke conflict and rejection – processes that plausibly consolidate distrust and increase perceived social isolation over time.
Early family relationships are a likely upstream influence on these pathways, yet large-scale tests of whether children’s mental health mediates links between these early relationships and adolescent social outcomes are scarce, to our knowledge. The impact of early-life social bonds – primarily the quality of the parent–child and interparental relationships during early childhood – on children’s mental and physical health is now firmly established (Bakker et al., 2012; Chen, 2022; Gutman & Eccles, 2007; Morgan et al., 2012; Patalay & Fitzsimons, 2018; Weich et al., 2009), and several biological mechanisms for this have been examined (Bhutta et al., 2023; Gaspar et al., 2022; Izett et al., 2021; McLaughlin et al., 2014; Nusslock & Miller, 2016; Taylor, 2010; Thomas et al., 2024; Yu et al., 2024). Positive dyadic interactions between parents and children, and stable emotional connections within the family, can foster children’s trust expectations, social competencies and coping strategies. Negative or volatile dynamics, on the other hand, may predispose children to view social interactions with suspicion and isolate themselves socially. Despite the known importance of these early relational patterns, to our knowledge, no study has simultaneously examined early family relationship quality, the development of childhood internalising and externalising difficulties over time, and adolescent social outcomes in a large, nationally representative sample. This gap is important, as it may help clarify how early relationships and emerging mental health problems shape adolescent perceptions of interpersonal distrust and perceived social isolation, potentially revealing new targets for early intervention.
The Present Study
Our study aims to fill these gaps. We address three research questions using data from a large, nationally representative birth cohort in the United Kingdom. First, we examine whether developmental trajectories of mental health difficulties during childhood (at ages 3–11 years) are associated with adolescent distrust and perceived social isolation (at age 14 years). Specifically, we hypothesise that higher baseline levels of internalising or externalising problems from ages 3 to 11, or an increasing trend in these problems across childhood, predict heightened distrust and social isolation at age 14. Second, we examine whether the quality of early-life mother–child and interparental relationships (at age 3 years) is associated with these outcomes in mid-adolescence. Third, we explore whether the trajectories of mental health difficulties in childhood mediate the links between early-life family relationships and adolescent distrust and perceived isolation. We anticipated that family relationships would exert both direct effects on later social outcomes (distrust and isolation) and indirect effects via childhood mental health. We also expected that these associations would persist even after adjusting for a range of child (including biological sex, ethnicity, developmental delays, and verbal ability), family (income, family structure, maternal education and mental health), and neighbourhood characteristics (including area disadvantage and urbanicity). We controlled for these factors as they have been associated with early family relationships, childhood mental health, and adolescent social adjustment (Adjei et al., 2022; Bakker et al., 2012; Barnett et al., 2021; Colins et al., 2025; Evans et al., 2018; Gaspar et al., 2022; Hosokawa & Katsura, 2017; Keogh et al., 2014; McGorry et al., 2024; Rubin et al., 2014).
Finally, we highlight that, in this work, we distinguish between structural social isolation (an objective paucity of social roles, relationships, interactions, or resources) and perceived social support (subjective evaluations of being able to rely on others, feel close to and trust others, or receive help if needed). These constructs are related but not interchangeable: an adolescent may have many social contacts yet perceive low support from others, or have few contacts yet feel well supported. It is also important to note that one of these two constructs – perceived social isolation (or, simply, ‘social isolation’) – indexes low levels of perceived social support. It does not measure level of structural isolation.
Methods
Participants and Analytic Sample
The Millennium Cohort Study (MCS) is an ongoing, nationally representative birth cohort survey that follows the lives of more than 19,000 children from the four UK countries, born between September 2000 and early January 2002 (Joshi & Fitzsimons, 2016). In the present study, we use data from the first six waves (‘sweeps’) of the survey. In the first wave, the age of cohort members was approximately 9 months, while in waves two to six, their age was approximately 3, 5, 7, 11, and 14 years. The sampling frame was based on the UK’s electoral wards, and there was a deliberate over-sampling of participants living in areas of high child poverty, those from the smaller UK countries, and those with high proportions of ethnic minorities in England (Plewis et al., 2004). Data collection only proceeded after obtaining all ethical approvals (with the process overseen by UK Multi-Centre Ethics Committees led by the National Health Service), and after primary caregivers had provided informed consent (children provided their assent at age 11 and informed consent from age 14 years). The final, anonymised dataset includes information collected via interviews and questionnaires completed in the family’s home by the primary caregiver (i.e., the mother in the vast majority of cases), as well as the children and their teachers. Cognitive and neuropsychological test batteries and observations by trained interviewers augmented the information about the cohort.
At the age 14 survey sweep, more than 11,800 adolescents took part in the survey (data collection took place between January 2015 and March 2016). Our analyses included 11,717 cohort members who were singletons or first-born twins or triplets and were further restricted to those with complete data on the outcomes (distrust and low social support). As a result, the final sample included 11,069 adolescents (51% female, 20% non-White; 44% living in disadvantaged areas). Further details on the demographic profile of included and excluded participants (with a sample bias analysis) are provided in Table 1. We note that full information about the study variables, methodology, and the complete code output of all statistical analyses can be found in the Supplemental Online Material (SOM, 2025).
Demographics and Sample Bias Using Key Measures Comparing Those Excluded From the Sample at Age 14 (Sixth MCS Wave) With Those Included in the Analytic Sample.
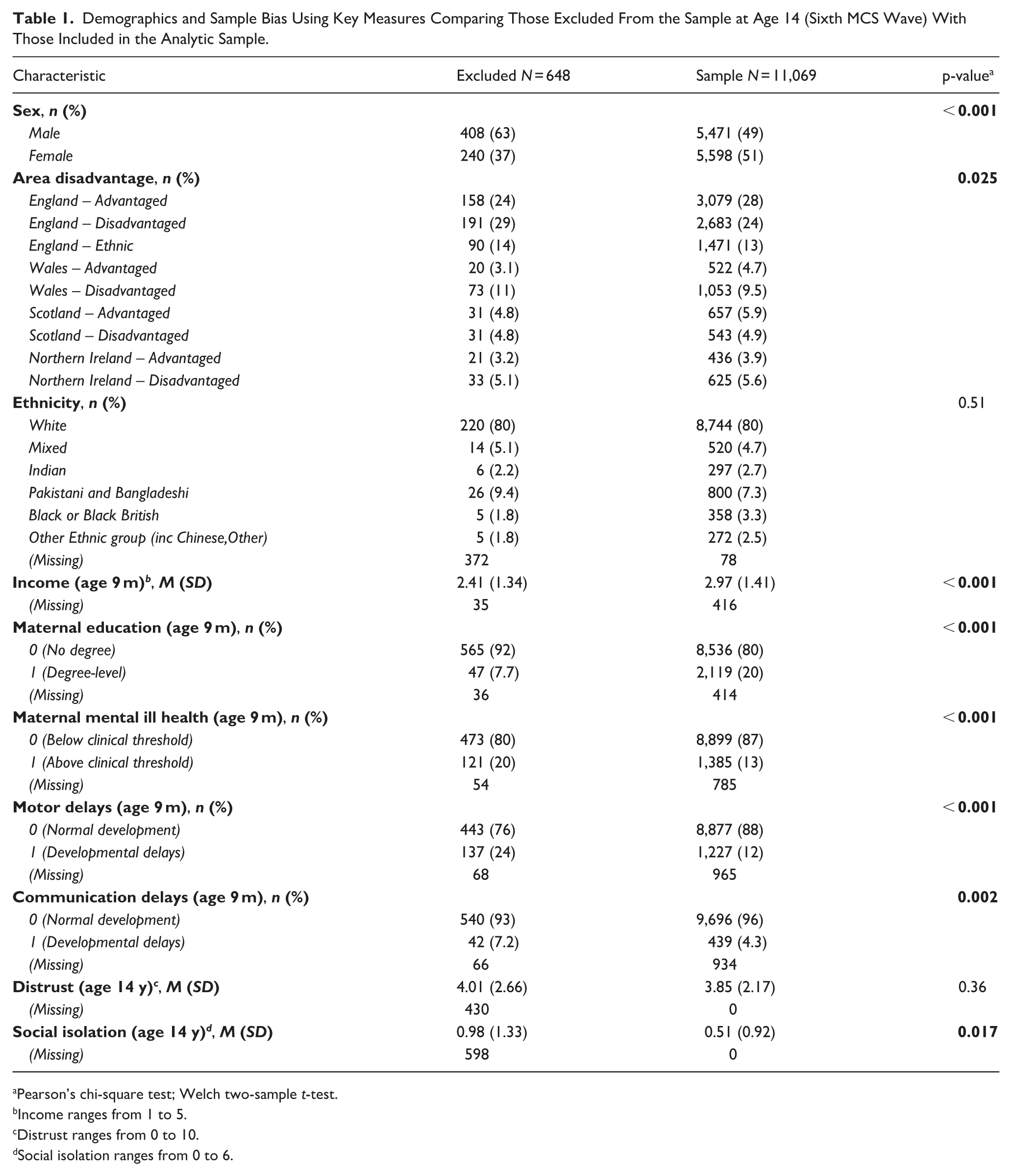
Pearson’s chi-square test; Welch two-sample t-test.
Income ranges from 1 to 5.
Distrust ranges from 0 to 10.
Social isolation ranges from 0 to 6.
Measures
Mother–Child and Interparental Relationship Quality (3 Years)
The quality of family relationships was assessed in early childhood via two variables. First, mother–child relationship was assessed at age 3 with the mother-reported Child-Parent Relationship Scale short-form (CPRS-SF) – a 15-item scale adapted from Pianta and Nimetz (2001). Total relationship quality was derived by the sum of all items (each item on a Likert-type scale from 1 to 5), ranging from 30 to 75, with higher scores corresponding to improved relationship quality (Cronbach’s
Second, (inter-) parental relationship quality was measured using a 7-item questionnaire completed by the primary caregiver at the age 3 sweep. Adapted from the Golombok Rust Inventory of Marital State (Rust et al., 1990), it was completed by those with a resident spouse or partner, and included items such as ‘My [husband] is usually sensitive to and aware of my needs’; ‘My [husband] doesn’t seem to listen to me’ (reverse-coded); ‘Our relationship is full of joy and excitement’; and ‘I suspect we may be on the brink of separation’ (reverse-coded). Each item was rated on a Likert-type scale from 1 to 5, with higher scores indicating better relationship quality (
Childhood Mental Health (3, 5, 7, and 11 Years)
Children’s mental health difficulties were operationalised as the total scores for internalising and externalising symptoms, assessed via the parent-reported Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997; Goodman & Scott, 1999), that is, scores from 20 items corresponding to four SDQ subscales: emotion problems, peer problems, conduct problems, and hyperactivity/inattention (with 5 items per scale and responses rated on a 3-point Likert-type scale from 0 to 2), with higher scores corresponding to more symptoms. Internalising problems are the sum of emotion and peer problems, and externalising problems are the sum of conduct and hyperactivity/inattention problems. In terms of their reliability, in our sample across sweeps, Cronbach’s
Interpersonal Distrust (14 Years)
The first outcome was derived from a single item of the Young Person Questionnaire (YPQ) at age 14: ‘On a scale from 0 to 10, where 0 means not at all and 10 means completely, how much would you say you trust other people?’ (recoded so that 10 corresponded to most distrustful).
Perceived Social Isolation (14 Years)
The second outcome was derived from the YPQ ‘social support grid’, which asked participants to rate their level of agreement with the statements: ‘I have family and friends who help me feel safe, secure and happy’; ‘There is someone I trust whom I would turn to for advice if I were having problems’; and, ‘There is no one I feel close to’ (reverse-coded). Possible responses were ‘Not true at all’ (score of 2); ‘Partly true’ (1); and ‘Very true’ (0). Therefore, this scale’s scores ranged from 0 to 6, with 6 corresponding to maximal social isolation. Perceived social isolation had a reliability of
Confounders (9 Months–3 Years)
Biological sex was provided by the primary caregiver. Ethnicity was based on the UK Census classification of White, Mixed, Black or Black British, Indian, Pakistani and Bangladeshi, or Other Ethnic group. Developmental delays at 9 months (dichotomous variable) indicated the presence of fine motor, gross motor, or communicative function delays based on the Denver Developmental Screening Test (Frankenburg & Dodds, 1967) and the MacArthur Communicative Development Inventories (Fenson et al., 1993). Verbal ability (age 3 years, normalised T-score ranging from 20 to 80) was provided by a trained assessor using the British Ability Scales II Naming Vocabulary, capturing expressive language ability (Hill, 2005; Sullivan et al., 2021).
Each household’s income (9-month wave) was provided in OECD equivalised income quintiles; maternal education (9-month wave) was a dummy variable based on whether the main respondent was university-educated; maternal mental ill-health (9-month wave) was a dichotomous variable (yes/no) using the standard cut-off
Regarding the child’s social environment, this was captured using measures of urbanicity and sampling stratification. There was an advantaged and a disadvantaged stratum in each UK country. The disadvantaged stratum in each UK country included areas that were in the upper quartile (i.e., the poorest 25%) of the Child Poverty Index (Plewis et al., 2004). In England, a third stratum was included, the ethnic minority stratum, composed of neighbourhoods that had an ethnic minority indicator of at least 30%. Urbanicity was determined from linked data provided by the Office for National Statistics, based on the rural-urban classification in the 2001 Census (Church & Midouhas, 2016), and this was a binary indicator (urban v. rural).
Analytic Strategy
The main analysis was carried out in two stages. First, we explored the data with plots and descriptive statistics, performed a sample bias analysis, and estimated rates of data missingness which informed the data imputation approach. Second, we imputed missing data and fitted a survey-weighted latent growth curve and path analysis model for each outcome (distrust and social isolation), with mother–child and interparental relationships as exposures, and the intercept (baseline score), linear slope (rate of change) and quadratic slope (non-linear curvature) of internalising and externalising problem trajectories as mediators, controlling for biological sex, ethnicity, developmental (i.e., motor and communicative) delays, verbal ability, family structure and household composition (i.e., presence or not of both parents and siblings in household), maternal education and maternal mental ill health, urbanicity, household income, and area disadvantage. Therefore, there were a total of four imputed, survey-weighted structural equation models.
In an additional analysis, given the well-established sex differences in the prevalence and growth of internalising/externalising symptoms across childhood and adolescence, we fitted these models separately for male and female cohort children (sex-stratified analysis). Survey design characteristics were taken into account, and survey weights were applied in all analyses to correct for the stratified, clustered sampling and the differential non-response/attrition patterns of MCS, thereby yielding population-representative estimates for UK adolescents and appropriately adjusted standard errors. Calculations were performed in R 4.4.1 (R Core Team, 2021) using ‘lavaan’ and ‘survey’ packages (Rosseel, 2012). Missing data were imputed with the ‘mice’ package (m = 30 runs, seed = 223) using multiple imputation for chained equations and combining results with Rubin’s rules (Rubin, 1987). More information about each analysis step and the complete output can be found in the Supplemental Online Material (SOM, 2025).
Results
Participant Demographics and Descriptive Analyses
The final analytic sample (
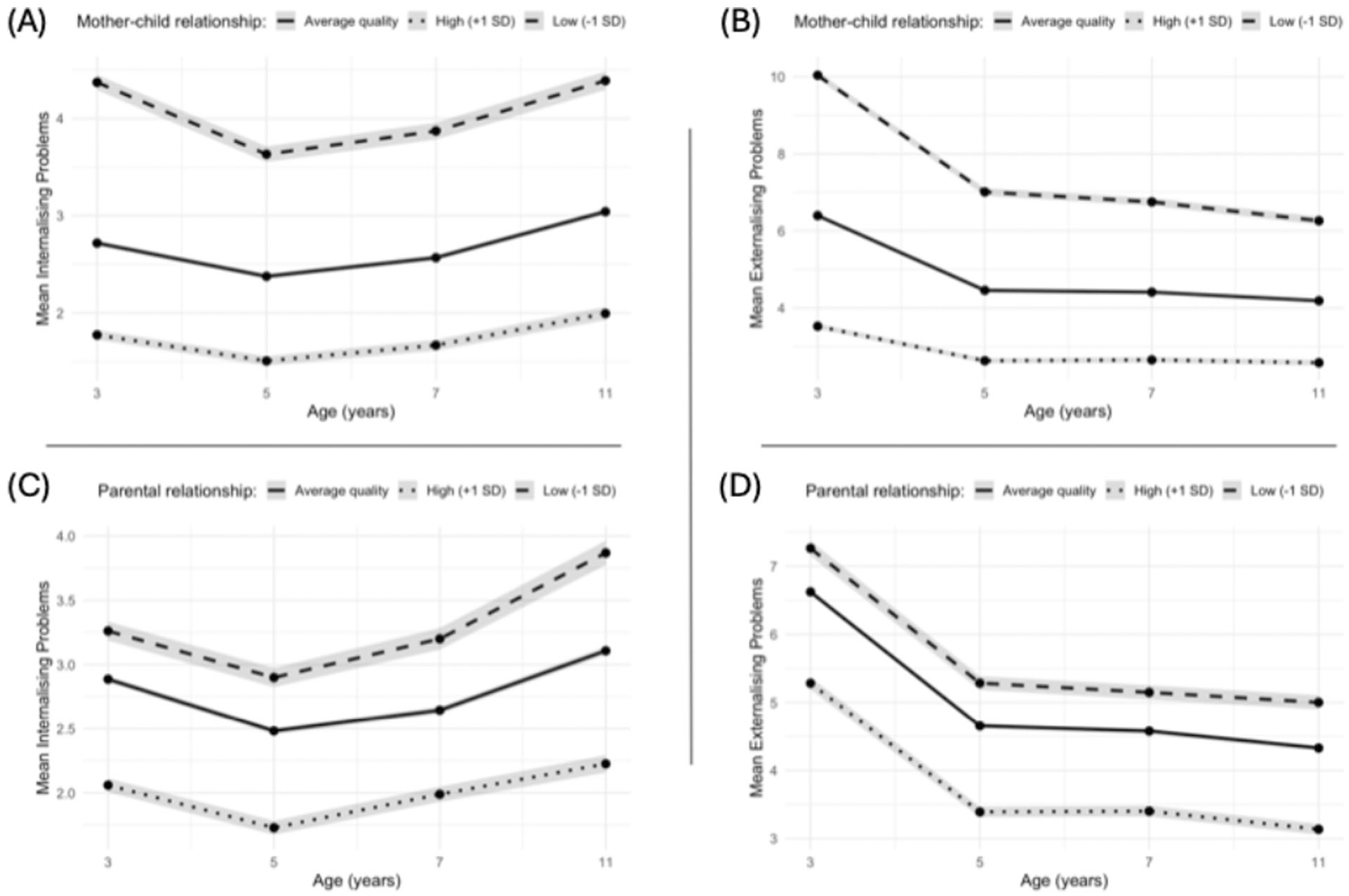
Mean Scores of Internalising and Externalising Difficulties From Ages 3 to 11 Years Stratified by the Quality of Early-Life Family Relationships. (a) Mean internalising (N = 7,676), (b) mean externalising scores per wave stratified by mother–child relationship quality (N = 7,692), (c) mean internalising (N = 6,809) and (d) mean externalising scores per wave stratified by interparental relationship quality (N = 6,828). Internalising/externalising scores range from 0 to 10.
Family Relationships, Internalising Problem Trajectories, and Social Outcomes
Figure 2 shows a simplified illustration of the fully adjusted, survey-weighted model – with internalising problems as a mediator – and presents the main results for the key paths when distrust was the outcome. Figure 3 presents the same information for social isolation as the outcome. Table 2 summarises the main findings for both models (with full details in the SOM, Section B1). The linear slope and curvature (quadratic component) of internalising problem trajectories were both significantly positively associated with subsequent distrust and social isolation (standardised effects from 0.12 to 0.34).
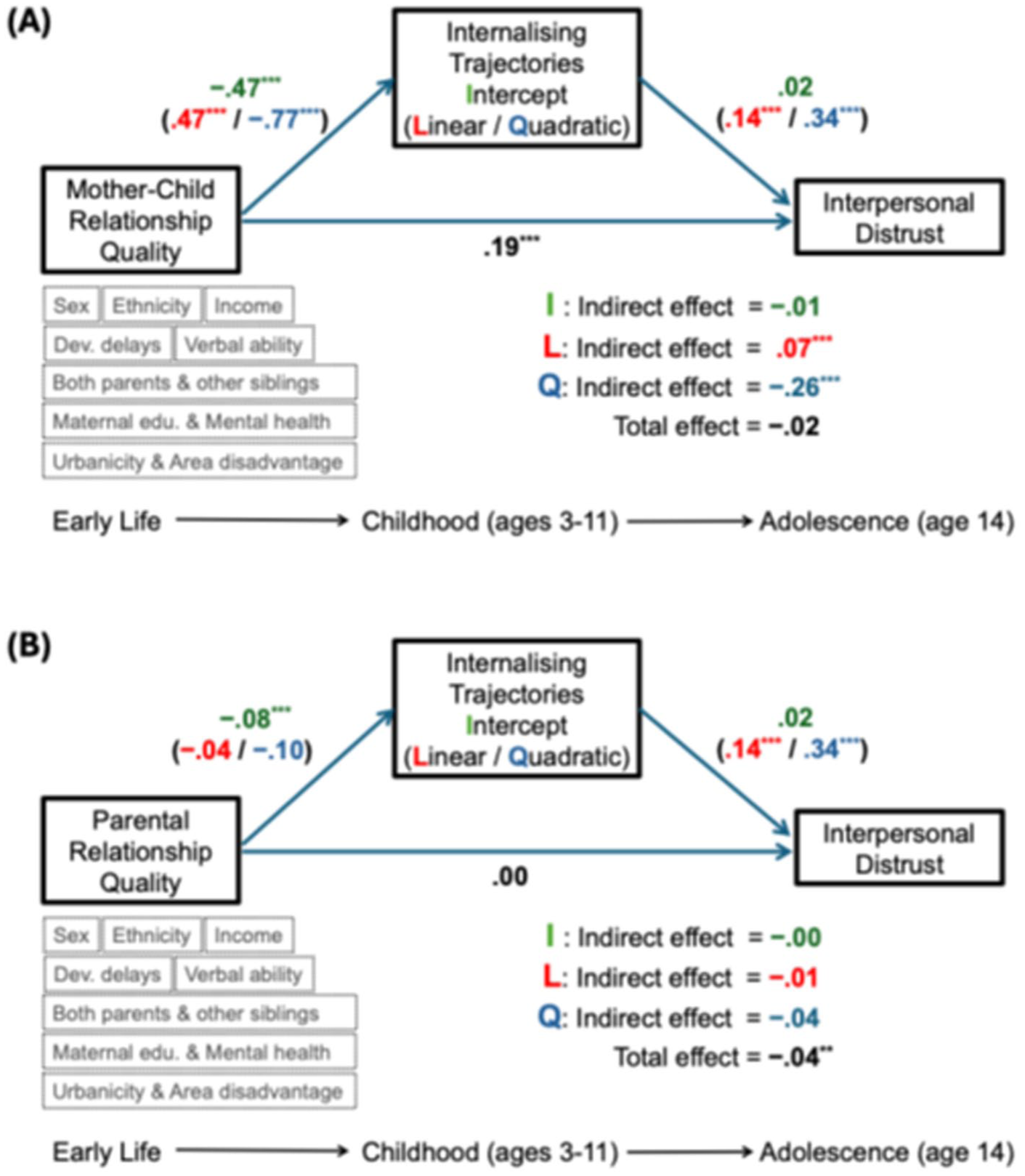
Simplified Schematic of the Main Model Showing Only Internalising Trajectories and Distrust (Survey-Weighted, Imputed, N = 11,069). Internalising problem trajectories from age 3 to 11 (intercept, linear and quadratic slope) as mediators of the prospective associations between (a) mother–child and (b) interparental relationship quality assessed at age 3 and interpersonal distrust (age 14). Standardised coefficients shown.
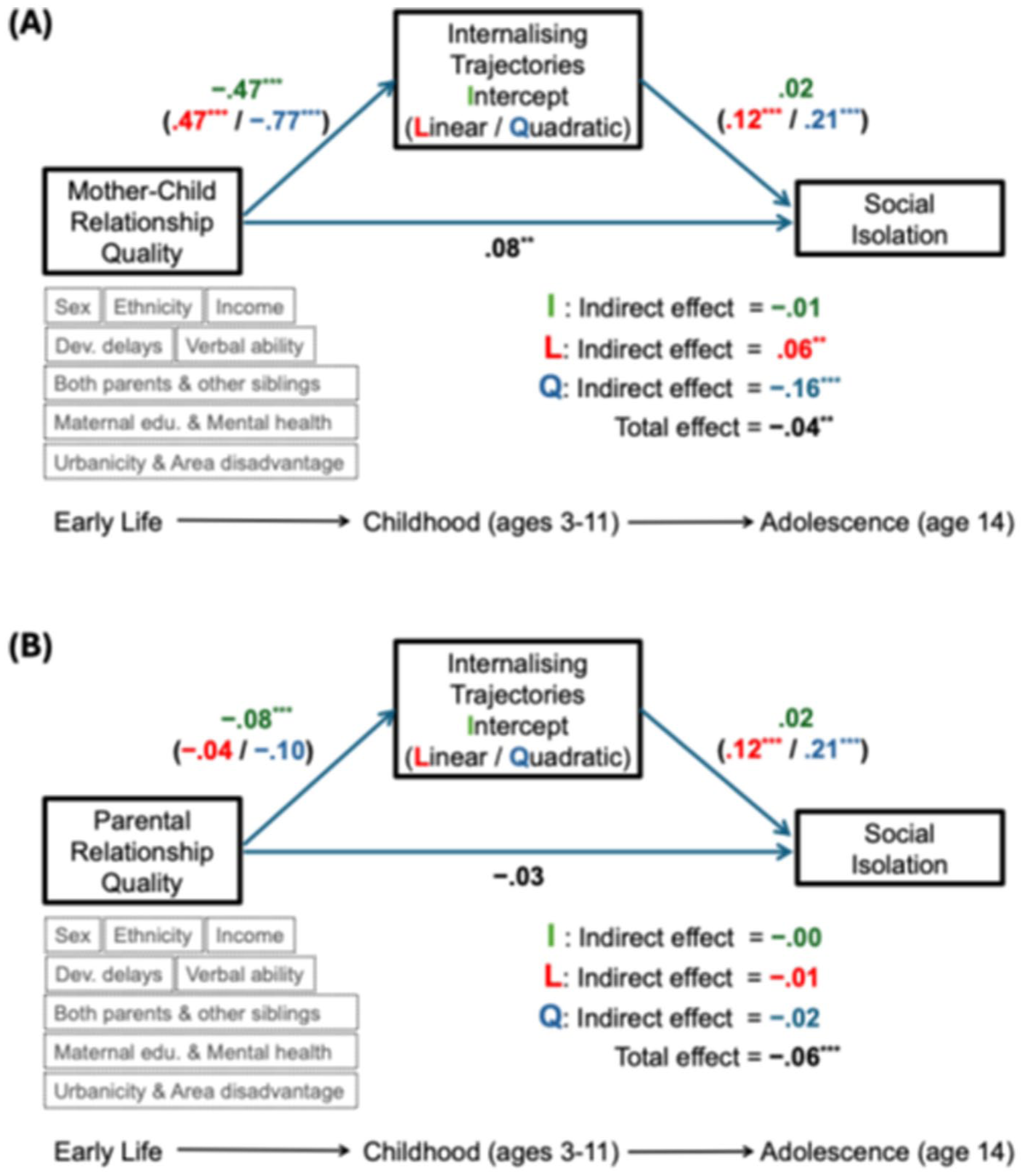
Simplified Schematic of the Main Model Showing Only Internalising Trajectories and Social Isolation (Survey-Weighted, Imputed, N = 11,069). Internalising trajectories from age 3 to 11 (intercept, linear and quadratic slope) as mediators of the associations between (a) mother–child and (b) interparental relationship quality (age 3) and social isolation (age 14). Standardised coefficients shown.
Main Results of the Imputed, Survey-Weighted Models, With Internalising Problem Trajectories as Mediators, and Interpersonal Distrust and Social Isolation as Outcomes, After Controlling for All Confounders (N = 11,069).
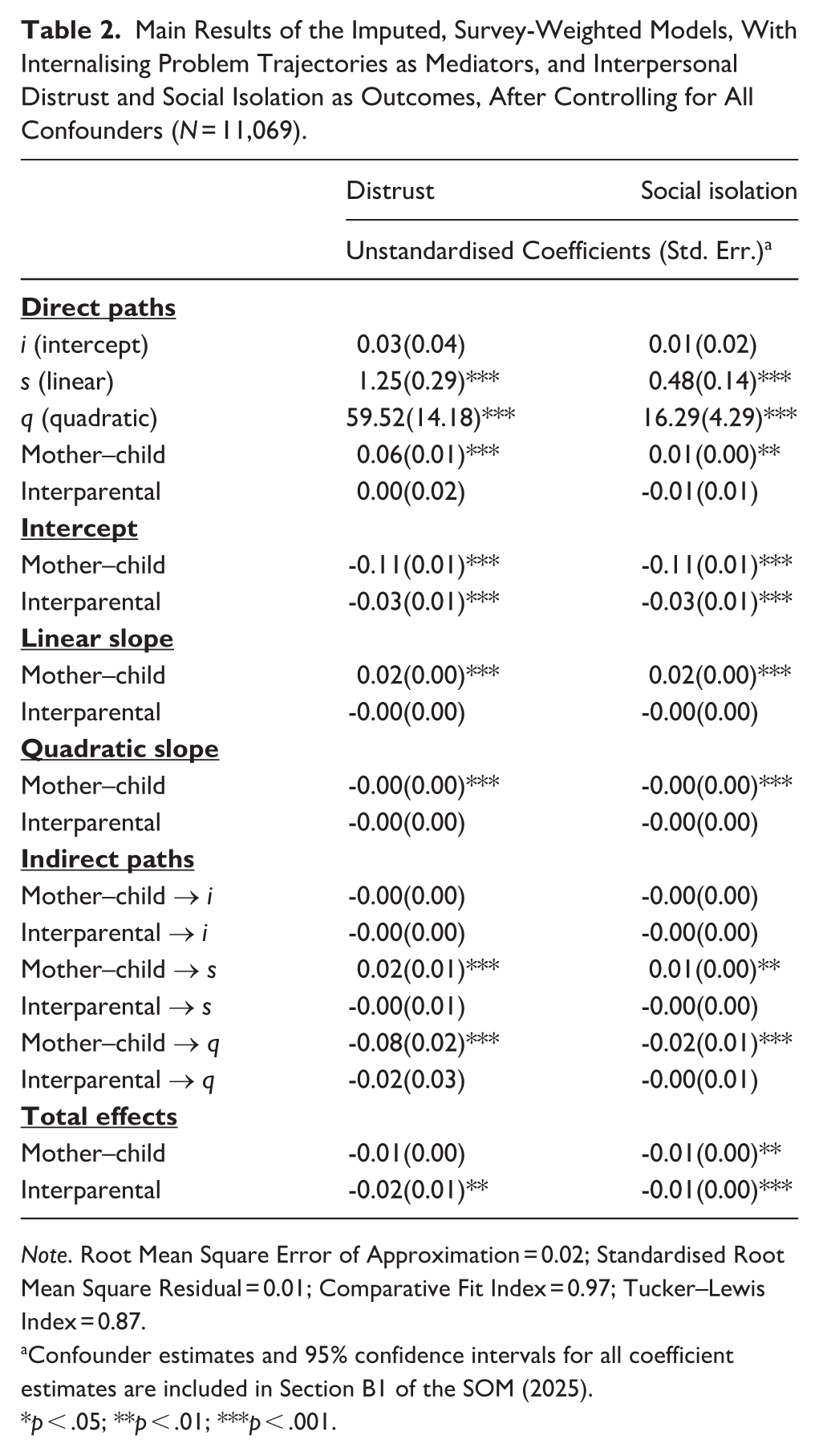
Note. Root Mean Square Error of Approximation = 0.02; Standardised Root Mean Square Residual = 0.01; Comparative Fit Index = 0.97; Tucker–Lewis Index = 0.87.
Confounder estimates and 95% confidence intervals for all coefficient estimates are included in Section B1 of the SOM (2025).
p < .05; **p < .01; ***p < .001.
Distrust
There was a positive direct association between higher mother–child relationship quality and distrust (standardised
Social Isolation
Results for social isolation are shown in Figure 3 and Table 2. First, for the mother–child relationship, there was a positive indirect effect via the linear slope (
Family Relationships, Externalising Problem Trajectories, and Social Outcomes
Table 3 summarises the main findings for both distrust and social isolation (full details in SOM, Section B2). The intercept, linear slope, and curvature of externalising problem trajectories were all significantly positively associated with subsequent distrust and social isolation (standardised effects from 0.11 to 0.27).
Main Results of the Imputed, Survey-Weighted Models, With Externalising Problem Trajectories as Mediators, and Interpersonal Distrust and Social Isolation as Outcomes, After Controlling for All Confounders (N = 11,069).
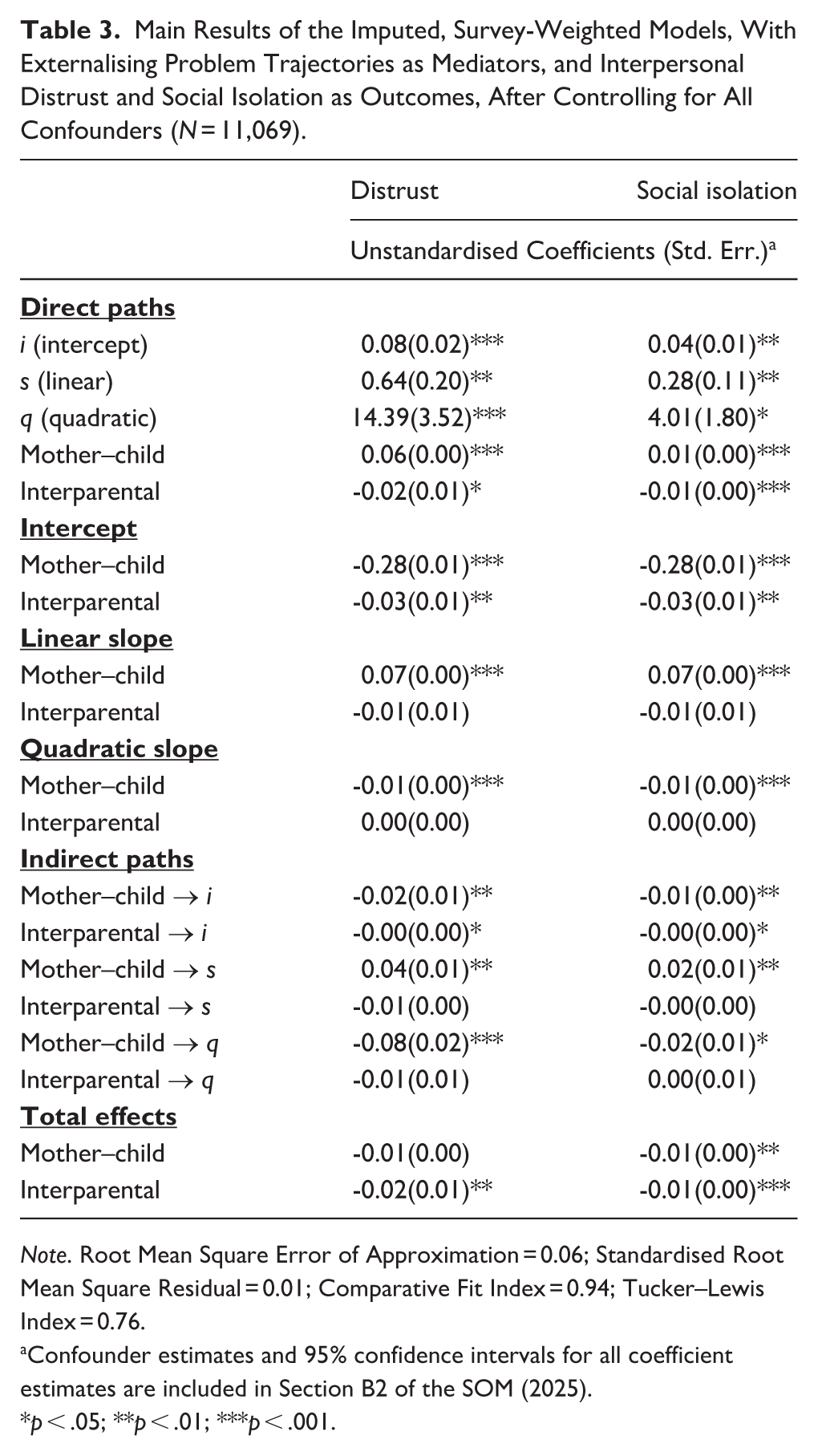
Note. Root Mean Square Error of Approximation = 0.06; Standardised Root Mean Square Residual = 0.01; Comparative Fit Index = 0.94; Tucker–Lewis Index = 0.76.
Confounder estimates and 95% confidence intervals for all coefficient estimates are included in Section B2 of the SOM (2025).
p < .05; **p < .01; ***p < .001.
Distrust
As before, there was a positive direct association between higher mother–child relationship quality and distrust (standardised
Social Isolation
A more positive mother–child relationship was directly associated with higher social isolation (
Additional Analysis by Biological Sex
The sex-stratified models produced results consistent with the main analyses, with a similar pattern of associations for both male and female cohort children. For the mother–child relationship and interpersonal distrust, there was significant partial mediation through the internalising problems trajectory’s linear slope (
Summary of the Sex-Stratified Analyses (Imputed, Survey-Weighted) After Controlling for All Confounders, N = 11,069.
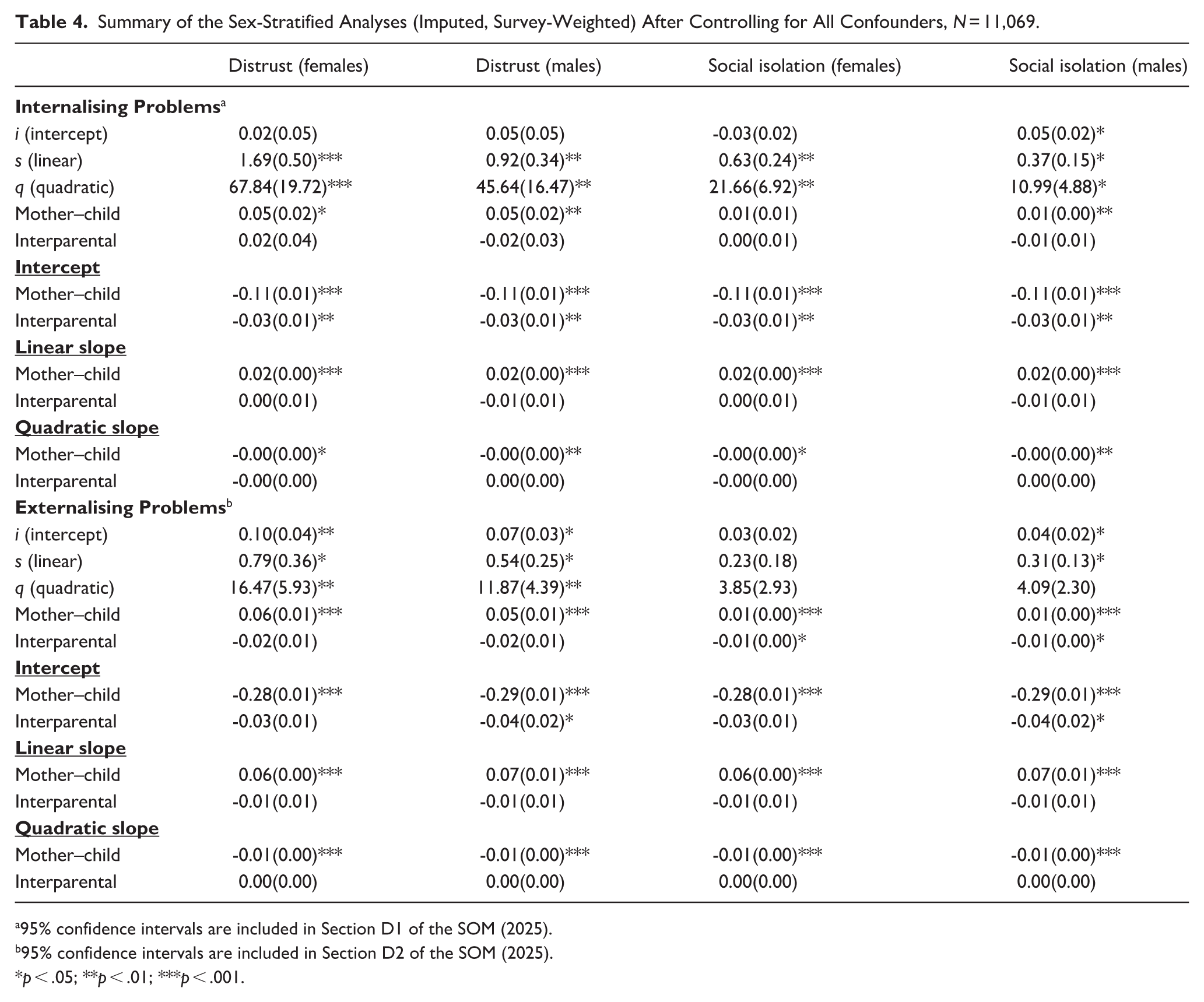
95% confidence intervals are included in Section D1 of the SOM (2025).
95% confidence intervals are included in Section D2 of the SOM (2025).
p < .05; **p < .01; ***p < .001.
Discussion
The present study provides evidence that childhood trajectories of internalising and externalising problems (ages 3 to 11) are prospectively associated with interpersonal distrust and perceived social isolation in mid-adolescence (age 14). Early family relationships (between mother and child, and between parents) are also strongly associated with the onset (at age 3) and development (ages 3–11) of both internalising and externalising problems in childhood. Specifically, we showed that (a) better interparental relationship in early childhood significantly predicts less distrust and social isolation in mid-adolescence, both directly and indirectly via lower baseline externalising problems; (b) better mother–child relationship significantly predicts less social isolation overall, through all the direct and internalising or externalising paths. Together, these findings confirm our hypothesis that increasing levels of internalising and externalising symptoms from early childhood into early adolescence place youth at higher risk of interpersonal distrust and perceived social isolation, and that the onset or development of these trajectories partly mediate the effects of early-life family relationships.
In the models using internalising symptom trajectories as the mediator, the quality of the mother–child relationship displayed opposite-signed mediation through the linear and quadratic growth factors. Specifically, better mother–child relationship quality was associated with a slightly steeper linear increase in internalising from ages 3 to 11 (yielding a positive indirect effect on adolescent distrust and isolation), but also with a more negative quadratic curvature (i.e., a greater deceleration or rate of decline of these problems towards late childhood, yielding a negative indirect effect). It is important to note that a higher linear slope increased risk for adolescent interpersonal distrust and social isolation – as would be expected, since increasing internalising difficulties over time predict poorer social outcomes – whereas a more negative quadratic slope decreased risk, reflecting improvement in symptoms towards later childhood, that is, a protective effect. In fact, the quadratic (protective) pathway predominated, resulting in a small net protective mediation for social isolation and a near-zero net mediation for distrust. This pattern suggests that developmental change proximal to adolescence – specifically, a steeper decline in internalising symptoms by late childhood – may represent a key mechanism linking the quality of early mother–child relationship quality to adolescent interpersonal distrust and perceived social isolation.
These findings extend our understanding of how the development of mental health difficulties in childhood can shape adolescents’ relational experiences and social-cognitive schemas. While social causation theory (Mossakowski, 2014; Ren et al., 2018) and social safety theory (Slavich, 2020; Tsomokos & Slavich, 2024) provide frameworks that help explain the opposite direction of the association – from distrust or social isolation to the development of mental health difficulties – the direction established in the present work can be interpreted through the interpersonal domain of mental health (Fearey et al., 2021; Joiner & Timmons, 2009; Pritchard, 2021; Schwartz-Mette et al., 2021). From this perspective, worsening emotional or behavioural problems in childhood can set in motion multiple interrelated processes, including heightened stress and anxiety in social contexts, distorted interpretations of social cues, impaired social competence, and excessive reassurance-seeking that can deplete available support. Alone or in combination, these processes can undermine social relationships and degrade interpersonal trust and social support perceptions over time (Camara et al., 2017; Chin, 2014; Clarke et al., 2021). Stated differently, children who exhibit early or escalating emotional or behavioural difficulties may find themselves in social environments offering fewer trusting, reliable, and protective relationships – whether due to chronic stress, disrupted peer or family relationships, or internalised negative expectations. In the present study, we demonstrate that the quality of family relationships in early childhood, particularly the mother–child bond and interparental relationship quality, plays an important role in shaping children’s mental health trajectories, which, in turn, influences adolescents’ perceptions of trust and social support.
Although high-quality early childhood family relationships were indirectly associated with fewer mental health problems, and consequently with lower levels of distrust and social isolation in adolescence, we unexpectedly observed a direct association between better quality mother–child relationship and poorer social outcomes at age 14. This is a counter-intuitive finding that merits further investigation (i.e., the fact that, in bivariate analyses, higher-quality mother–child relationship correlated with lower distrust and lower perceived social isolation, but in the fully adjusted models the direct path from mother–child relationship to both outcomes was positive, whereas indirect paths via children’s symptom trajectories were protective overall). One plausible interpretation is that a suppression effect may be operating, whereby the indirect (protective) and direct (adverse) paths act in opposite directions, resulting in an apparent positive direct association after accounting for mental health trajectories. In this scenario, once the variance explained by internalising and externalising symptom trajectories is accounted for, a residual direct path may emerge in the opposite direction, reflecting distinct and possibly unmeasured processes in the mother–child relationship that relate to social outcomes independently of mental health. For instance, while a high-quality mother–child relationship generally promotes better mental health, it may also foster heightened interpersonal vigilance or limit adolescents’ exposure to diverse social experiences, ultimately contributing to heightened distrust. Future studies could also investigate bidirectional processes, whereby distrust or social isolation in turn reinforces mental health difficulties over time. Such investigations would clarify whether children already on an adverse mental health trajectory are more prone to distrust and to negatively appraise the social resources available to them.
The strengths of the present study include the use of a large, nationally representative birth cohort, longitudinal data spanning from infancy through adolescence, and statistical models that accounted for a range of ecological confounders. Nonetheless, several limitations should also be acknowledged. First, mental health problems were based on parent-reported SDQ scores, which may be subject to reporting bias. Second, our measures of distrust and social support relied on self-reported or single-item indicators, which, despite their practicality and brevity, may not fully capture the complexity of these constructs. Third, although we adjusted for a range of confounders, the possibility of residual confounding cannot be entirely excluded. Finally, the study was conducted within the United Kingdom, which may limit the generalisability of our findings to other cultural or socioeconomic contexts.
Despite these limitations, our results have certain implications for clinicians and educators. Interventions aimed at identifying and addressing emotional and behavioural difficulties during childhood may yield long-term benefits for adolescents’ interpersonal functioning, supporting both individual youth and their broader communities beyond immediate mental health outcomes. The same applies to key relationships in a child’s early life, particularly the mother–child bond and the quality of the relationship between the parents. Clinicians should be attentive to children whose early emotional or behavioural difficulties, or exposure to early parental discord, place them at risk for social disconnection, distrust, and low perceived social support. Educators can foster supportive school climates through peer-mentoring programmes, teacher training, and accessible mental wellbeing services that promote trusting relationships among students.
In conclusion, the present study provides evidence that the development of emotional and behavioural problems in childhood predicts both interpersonal distrust and low perceived social support by mid-adolescence, a critical developmental period for the emergence of psychopathology. In addition, poor early-life family relationships can exacerbate the development of internalising and externalising problems, which are, in turn, strongly linked to the development of distrust and social isolation.
Footnotes
Ethical considerations
The Millennium Cohort Study obtained ethical approval from the London Multicentre Research Ethics Committee for the age 14 sweep (REC ref: 13/LO/1786), which includes the present study’s outcomes. Ethical approvals have been obtained for all waves of the Millennium Cohort Study through the National Research Ethics Service Research Ethics Committee, and the most recent approval was obtained in October 2017, REC Ref: 17/NE/0341. Written consent by the primary caregiver was provided prior to any data collection taking place, and participants provided their assent at age 11 and consent from age 14 years.
Author contributions
D.I.T., E.P., and E.F. conceived and designed research. D.I.T. analysed the data and wrote the first draft of the manuscript. E.P. and E.F. edited the manuscript and supervised. All authors approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: D.I.T. was partially supported by Alphablocks Nursery School Ltd. The funding source had no involvement in the design of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data used in this study is freely available under licence through the custodians of the Millennium Cohort Study (University College London, UCL Social Research Institute, Centre for Longitudinal Studies. (2024). Millennium Cohort Study. [data series]. 16th Release. UK Data Service. SN: 2000031, DOI: ![]() ).
).