
Abstract
Socioeconomic inequalities are important determinants of children’s mental health, yet evidence from socially vulnerable populations is limited. This study investigates the associations between parental socioeconomic factors and children’s mental health and well-being in disadvantaged schools. In this cross-sectional, analytical study, 735 children (51.7% boys) and their parents were included. Socioeconomic status (SES) was measured through parental education, occupation, employment, and household income and a Slope Index of Inequality quantified. Children’s mental health was assessed using the Strengths and Difficulties Questionnaire, and health-related quality of life using the Kidscreen-10. Lower parental education was associated with higher total difficulties in unadjusted models (father: b = 1.91, 95% CI = [0.15, 3.68]; mother: b = 4.18, 95% CI = [2.44, 5.92]). After adjusting for covariates, associations remained significant for father’s education (b = 1.89, 95% CI = [0.10, 3.68]) and mother’s occupation (b = 3.90, 95% CI = [2.09, 5.71]). Parental employment was the only SES predictor of prosocial behavior (adjusted b = −0.99, 95% CI = [−1.53, −0.45]). Socioeconomic inequalities persist in children’s mental health. Addressing these disparities requires policies that target structural determinants, enhance family support, and promote equitable access to mental health resources. Prioritizing early interventions can generate long-term societal benefits by reducing future burdens on health care, education, and social systems.
The social determinants of health encompass a range of factors that shape health outcomes and are influenced by political, socioeconomic, and cultural contexts. Operating through systems such as health care and education, as well as through environmental and housing conditions, these determinants exert a profound influence on population health. They help explain persistent health disparities, with lower socioeconomic positions consistently linked to poorer health indicators [World Health Organization (WHO), n.d.]. Within this framework, socioeconomic status (SES) stands out as one of the strongest predictors of morbidity and premature mortality worldwide (Haraldstad et al., 2023; Iguacel et al., 2017; Stringhini et al., 2017). Its impact is comparable to that of other major health determinants, including lifestyle behaviors and environmental exposures, underscoring the importance of integrating socioeconomic adversity into public health strategies and policies (Otto et al., 2021). In childhood, SES reflects the socioeconomic circumstances of the family. Although parental education, occupation, and household income remain the most frequently employed indicators (Bradley & Corwyn, 2002; Gaspar et al., 2023), there is no consensus on the most accurate measures to capture socioeconomic position in pediatric populations (Ribeiro et al., 2020). Such measures, while widely used, often fail to fully capture the multifaceted nature of socioeconomic disadvantage.
Health-related quality of life (HRQoL) refers to an individual’s subjective perception and evaluation of their health and well-being within their cultural context (Ravens-Sieberer et al., 2014). In recent years, HRQoL has gained increasing prominence in pediatric health research, with greater emphasis on incorporating children’s self-reports as a key source of information (Gaspar et al., 2023; Ravens-Sieberer et al., 2014). As a central indicator for public health monitoring, HRQoL is aligned with the United Nations Sustainable Development Goal 3, which aims to ensure healthy lives and promote mental health and well-being (Befus et al., 2023; Instituto Nacional de Estatística, 2018). Children’s HRQoL is shaped by a complex interplay of social, cultural, and environmental factors, including family context, SES, gender, and age.
Low SES has been repeatedly associated with poorer HRQoL and higher prevalence of mental health difficulties in children (Gautam et al., 2023). For instance, Mulraney et al. (2021) and Yang et al. (2022) found that socioeconomic disadvantage is linked to a greater risk of psychological problems in childhood, while Grüning Parache et al. (2023) demonstrated that such difficulties often persist into adulthood, increasing the likelihood of mental disorders and adverse social outcomes. These associations are underpinned by multiple mechanisms: socioeconomic adversity can restrict access to health care, educational opportunities, and supportive social environments, while increasing exposure to stress, instability, and unsafe living conditions. Together, these pathways are likely to influence both the perceived quality of life and the psychological well-being of children.
Despite growing recognition of these interconnections, the joint examination of SES, HRQoL, and mental health in pediatric populations remains rare. Existing research has predominantly focused on relatively advantaged populations, often overlooking school-based samples in socially vulnerable areas. Schools located in areas characterized by high levels of social and economic vulnerability benefit from the Priority Intervention Educational Territories Program [PT: Territórios Educativos de Intervenção Prioritária- TEIP]. This program, promoted by the Ministry of Education, is a positive discrimination measure aimed at reducing early school dropout, academic failure, and indiscipline, as well as promoting academic success and educational equity. The identification of TEIP areas is based on regional social vulnerability criteria, defined using objective indicators, namely the percentage of students benefiting from school social assistance, the proportion of mothers with less than a 12th-grade education, and the percentage of migrant students. TEIP schools benefit from additional resources and greater organizational autonomy, allowing for the implementation of strategic intervention plans tailored to the specificities of local contexts. Moreover, some studies examine HRQoL or mental health in isolation, neglecting the potential interplay between these outcomes in contexts of socioeconomic disadvantage.
To address these gaps, the present study investigates the extent to which family socioeconomic inequalities are associated with HRQoL and mental health in primary school children attending schools located in socially vulnerable areas.
Method
This cross-sectional, analytical study forms part of the broader BeE-school research project, which evaluates the effectiveness of a health promotion program targeting children and families from primary schools located in socially vulnerable contexts.
Validated and widely used instruments were selected to ensure robust assessment of key constructs: Kidscreen-10 was chosen for its brevity and strong psychometric properties in capturing children’s HRQoL in large epidemiological studies; the Strengths and Difficulties Questionnaire (SDQ) was employed due to its established reliability and extensive use in child mental health research, including adaptation for the Portuguese population.
Participation required written informed consent from the children’s parents, in accordance with the principles outlined in the Declaration of Helsinki. The study received ethical approval from the Ethics Committee for Research in Life and Health Sciences at the University of Minho (CEICVS 009/2022).
Participants
All children meeting the inclusion criteria (aged 6–12 years and without physical or psychological conditions preventing participation) were invited to take part, along with their parents or legal guardians. Guardians received an information letter describing the study’s objectives and procedures. The research was conducted in 10 primary schools, encompassing 1,101 eligible children from two school clusters. In total, 735 children participated (51.7% boys, n = 380), with a mean age of 7.7 years (SD = 1.2).
Parents or guardians were asked to complete questionnaires covering socioeconomic information and the SDQ. The mother was the most frequent respondent (82.3%, n = 466; mean age = 38.6 years, SD = 5.6).
Socioeconomic Indicators
Socioeconomic data were reported by the children’s parents or legal guardians. Maternal and paternal education levels were measured in years of schooling and categorized into three levels: basic (⩽9 years of education, CITE/ISCED—International Standard Classification of Education = 0–2); secondary (10–12 years, ISCED = 3); and higher education (⩾13 years, ISCED = 4–6) (UNESCO Institute for Statistics, 2012). The highest educational level between parents was also identified.
Parental occupation was classified according to the Portuguese Classification of Occupations (Instituto de Emprego e Formação Profissional, 2011), mapped to ISCO-08 (International Standard Classification of Occupations), and grouped into three hierarchical classes: high (upper white-collar, ISCO-08 = 1–3), middle (lower white-collar, ISCO-08 = 4–5), and low (blue-collar, ISCO-08 = 6–9) (Wirth, 2023). The highest occupational status between parents was used in analysis. Employment status was coded as whether neither, one, or both parents were unemployed.
Household income was reported in six categories: ⩽€500, €501–1,000, €1,001–1,500, €1,501–2,000, €2,001–2,500, and ⩾€2,501. Given the minimum monthly wage in the study district in 2022 was €988 (Gabinete de Estratégia e Planeamento, 2023), household income was recoded into four categories: ⩽€1,000, €1,001–1,500, €1,501–2,000, and ⩾€2,001. In this sample, 23.3% of households reported parental unemployment, typically relying on a single income.
Socioeconomic Inequality
Socioeconomic inequality was quantified using the Slope Index of Inequality (SII), an absolute measure of disparity in health outcomes derived from regression modeling. The SII represents the difference in a health indicator between the most and least socioeconomically advantaged groups, capturing the entire social gradient (Hyldgård et al., 2021). In this study, the SII was computed for each socioeconomic indicator (parental education, occupation, employment status, household income).
The process involved (1) ranking categories from lowest to highest socioeconomic position; (2) assigning each category a value between 0 and 1 based on the midpoint of its cumulative frequency distribution; and (3) using these ranked variables in regression models to estimate the SII. An SII of 0 indicates no inequality; positive values indicate worse outcomes in lower SES groups, whereas negative values suggest the reverse (Moreno-Betancur et al., 2015; World Health Organization, 2017).
HRQoL Assessment
HRQoL was assessed at school using the Kidscreen-10 questionnaire. For children aged 6–7 years, the questionnaire was completed with the assistance of trained researchers who read the questions aloud; those aged 8–10 years completed the instrument independently. The Kidscreen-10 captures physical, emotional, mental, social, and behavioral aspects of well-being as perceived by children themselves (Ravens-Sieberer et al., 2014). This version is recommended for epidemiological studies involving large samples, due to its ease of administration and minimal respondent burden (Gaspar & Gaspar De Matos, 2008). It is considered a valid and reliable instrument for the population under study (Befus et al., 2023). The 10 questions were answered using a 5-point Likert-type scale—ranging from “not at all,” “a little,” “moderately,” “very much,” to “totally” (Questions 1 and 9)—or “never,” “rarely,” “sometimes,” “often,” and “always” (Questions 2 to 8 and Question 10). All items were summed and used to calculate scores based on the Rasch model. According to this model, the so-called “personal parameters” were estimated based on responses to the items, which were then transformed into T-values. A higher score indicates better HRQoL, while a lower score indicates poorer HRQoL (Ravens-Sieberer et al., 2006). Internal consistency in this study was acceptable (Cronbach’s α = 0.71).
Mental Health
Children’s and adolescents’ mental health was assessed using the SDQ, adapted for Portugal by Fleitlich et al. (2005). The SDQ assesses multiple dimensions of children’s psychosocial functioning, combining indicators of both difficulties and strengths. The SDQ contains 25 items rated on a 3-point scale (“not true,” “somewhat true,” “certainly true”), yielding five subscale scores, each ranging from 0 to 10: emotional symptoms, conduct problems, hyperactivity, peer problems, and prosocial behavior (Goodman, 1997). Collectively, these subscales provide a comprehensive profile of emotional, behavioral, and social functioning, supporting early identification of psychosocial difficulties.
The total difficulties score (sum of the first four subscales) reflects overall psychological difficulties, with higher scores indicating more problems. Higher prosocial scores indicate more positive social behaviors. The SDQ is widely used in epidemiological studies (Aarø et al., 2022).
Internal consistency in this study was good for the total difficulties scale (α = 0.81) but lower for prosocial behavior (α = 0.53).
Statistical Analysis
The descriptive analysis of the variables was carried out using measures of central tendency and dispersion, according to the type of variable. Associations between socioeconomic inequality (independent variable) and outcomes—HRQoL T-values, total difficulties score, and prosocial behavior—were analyzed using generalized linear models. Separate models were computed for each socioeconomic indicator (parents’ highest education, mother’s education, father’s education, parents’ highest occupation, mother’s occupation, father’s occupation, parental employment status, and household income). Model 1 was unadjusted; Model 2 adjusted for child’s sex and age; and Model 3 adjusted for child’s sex and age and mother’s age, given her predominance as the respondent (82.3%).
Analyses were conducted using IBM SPSS Statistics, version 29, with statistical significance set at p < .05.
Results
Most fathers had completed secondary education, while mothers more frequently held higher education degrees. Mothers were predominantly middle class, whereas fathers were largely lower class; however, when considering parents’ highest occupation, the upper class predominated. Household income was concentrated between €1,001 and €1,500 (27.5%), and 23.3% of households reported unemployment (Table 1).
Descriptive Analysis.
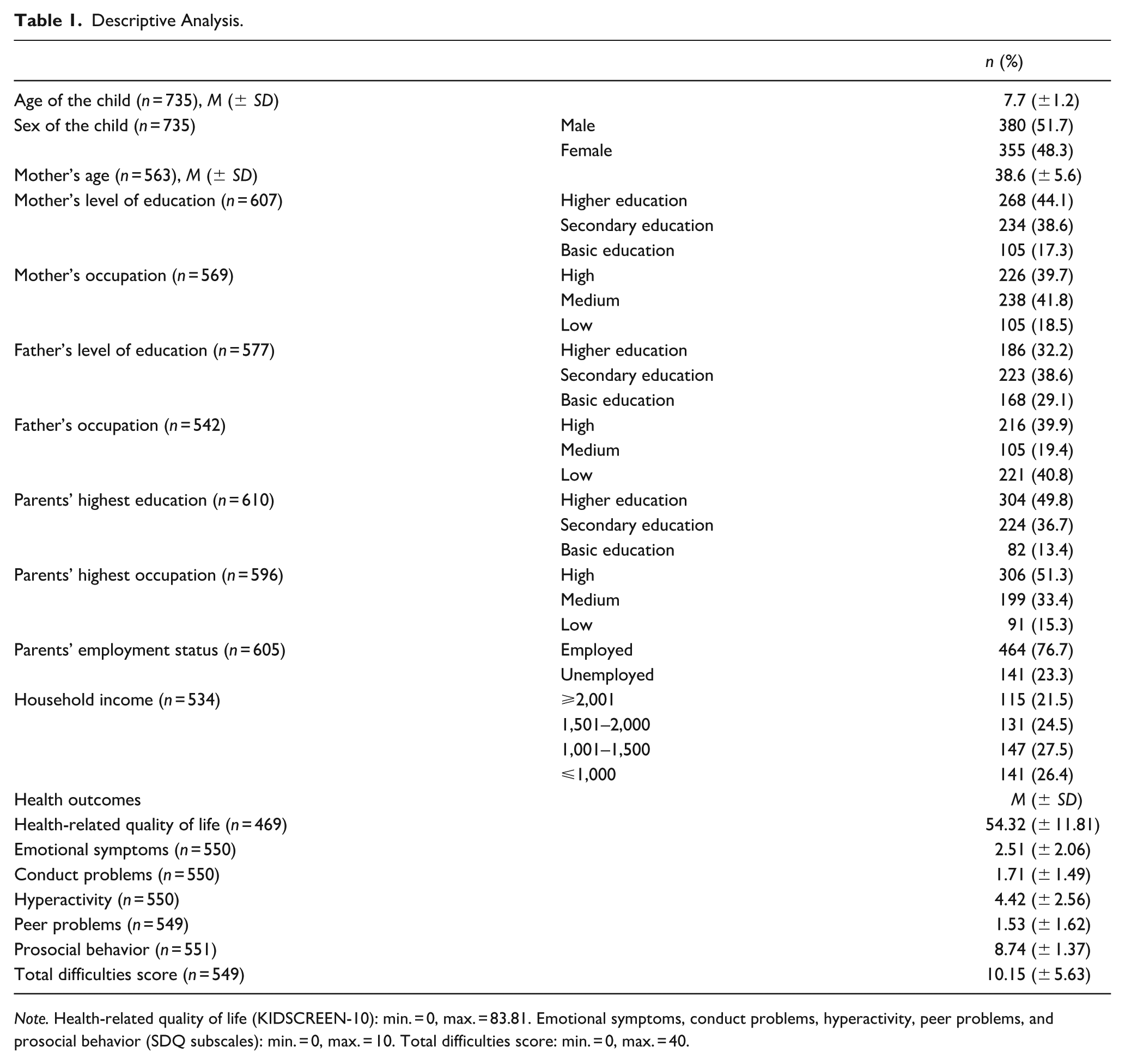
Note. Health-related quality of life (KIDSCREEN-10): min. = 0, max. = 83.81. Emotional symptoms, conduct problems, hyperactivity, peer problems, and prosocial behavior (SDQ subscales): min. = 0, max. = 10. Total difficulties score: min. = 0, max. = 40.
Children’s average HRQoL score was 54.32 (SD = 11.81). On the SDQ, 74.7% scored within the normal range for total difficulties and 97.1% for prosocial behavior.
No significant associations were found between socioeconomic inequalities and HRQoL. However, clear social gradients emerged in children’s mental health. In unadjusted models, lower parental education was strongly associated with higher total difficulties, ranging from father’s education (b = 1.91; 95% CI = [0.15, 3.68]) to mother’s education (b = 4.18; 95% CI = [2.44, 5.92]). A lower parental occupation was associated with higher total difficulties, ranging from father’s occupation (b = 3.19; 95% CI = [1.38, 5.00]) to mother’s occupation (b = 4.17; 95% CI = [2.38, 5.96]). Similarly, lower household income was significantly associated with total difficulties (b = 2.99; 95% CI = [1.25, 4.72]).
After full adjustment, significant associations remained for lower parental education and occupation, ranging from father’s education (b = 1.89; 95% CI = [0.10, 3.68]) to mother’s occupation (b = 3.90; 95% CI = [2.09, 5.71]). Consistently, lower household income was significantly associated with total difficulties (b = 2.54; 95% CI = [0.72, 4.36]).
Parental employment status was the only socioeconomic factor significantly predicting prosocial behavior (b = −0.96; 95% CI = [−1.48, −0.42]), remaining robust after adjustment (b = −0.99; 95% CI = [−1.53, −0.45]) (Table 2).
Associations between Health-Related Quality of Life, Mental Health, and Socioeconomic Inequalities.
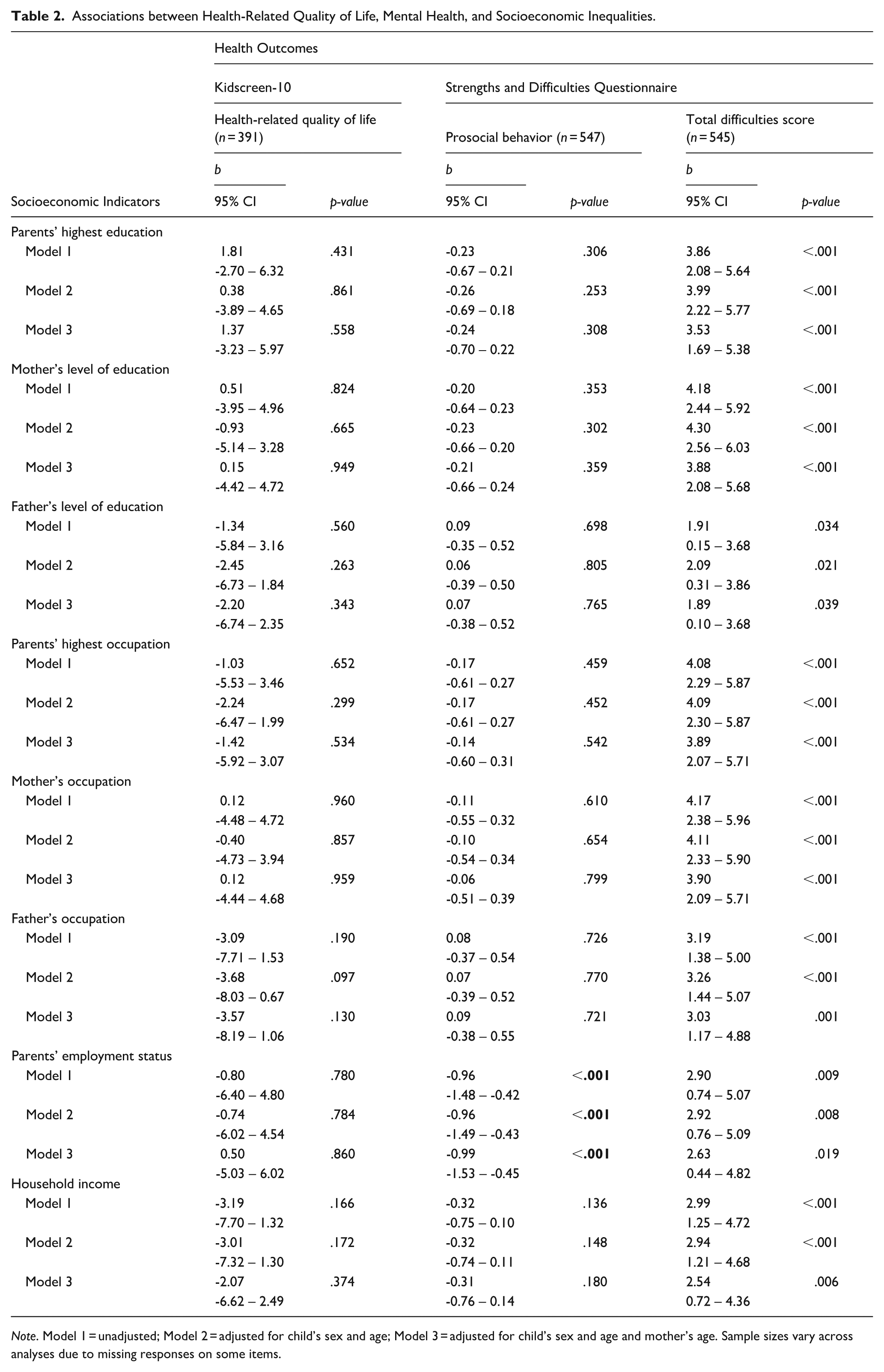
Note. Model 1 = unadjusted; Model 2 = adjusted for child’s sex and age; Model 3 = adjusted for child’s sex and age and mother’s age. Sample sizes vary across analyses due to missing responses on some items.
Discussion
This study underscores the complex, multidimensional relationship between socioeconomic inequalities and the mental health of school-aged children. Across multiple indicators, socioeconomic disadvantage was consistently associated with higher total difficulties, while parental employment showed a more specific association with prosocial behavior. These findings align with prior research (Gautam et al., 2024; Yang et al., 2022) indicating that low educational attainment, precarious employment, and limited material resources expose children to multiple adverse conditions, including residence in deprived neighborhoods, poor housing, restricted access to social services and education, and increased environmental stressors (Huisman et al., 2010).
The associations observed between parental education and children’s total difficulties are consistent with previous studies (Bøe et al., 2012; Hadzic et al., 2013; Hosokawa & Katsura, 2018; Huisman et al., 2010; Rajmil et al., 2014; Rasciute, 2023; Reiss, 2013; Tamura et al., 2020). In this study, maternal education and occupation showed a more pronounced gradient in relation to children’s difficulties than paternal indicators. This pattern may reflect persistent sociocultural norms in Portugal, where, despite advances in gender equity, maternal roles remain closely linked to caregiving responsibilities (Wall et al., 2016). The fact that 68% of fathers had medium-to-low educational attainment and 60% held low-status occupations likely contributed to early labor market entry, job insecurity, and constrained household income. Fathers’ longer working hours to secure financial provision may limit their engagement in child care (Fakhrunnisak & Patria, 2022), while mothers often assume the primary caregiving role, as documented in Portuguese (Perista & Perista, 2022) and international contexts (Sonego et al., 2013).
Maternal education has consistently been identified as a protective factor, shaping cognitive stimulation, emotional support, and parenting knowledge (Bøe et al., 2012; Hosokawa & Katsura, 2018; Rasciute, 2023; Reiss et al., 2019). Conversely, demanding or unstable maternal work conditions may shape the resources and availability necessary to meet children’s developmental needs (Kopp et al., 2023). In this study, maternal, but not paternal, education was significantly associated with behavioral problems and peer relationship difficulties, highlighting the pivotal role of maternal influence in child development outcomes (see Supplementary Table).
While fewer studies have focused on parental occupation as a determinant of child mental health, evidence suggests that other socioeconomic indicators, such as family income and maternal education, often have stronger effects on behavioral outcomes than occupation alone (Tamura et al., 2020). Here, maternal occupation inequalities were more strongly associated with total difficulties than paternal occupation inequalities.
Regarding prosocial behavior, parental employment status was the only socioeconomic variable showing a significant association. Children from households with at least one unemployed parent had lower prosocial scores, likely reflecting the importance of employment stability in ensuring both economic security and opportunities for parental engagement (Fakhrunnisak & Patria, 2022; Hadzic et al., 2013; Kopp et al., 2023). However, the cross-sectional design precludes causal inference, and it is possible that parents of children with fewer difficulties are more likely to participate in the labor market.
Income-related inequalities are consistently linked to child mental health outcomes (Gaspar et al., 2023; Hovsepian et al., 2019; Maleki et al., 2023; Reiss, 2013; Reiss et al., 2019; Yang et al., 2022). Higher income provides better living conditions, educational opportunities, and access to services, whereas low income increases parental stress, fosters harsher parenting practices, and reduces the availability of learning resources at home (Rijlaarsdam et al., 2013). In this study, total difficulties scores were higher than those reported in Northern European populations (Befus et al., 2024; Obel et al., 2004), which may reflect cultural differences, maternal reporting patterns, and variations in perceptions of child behavior.
Contrary to some prior evidence (Befus et al., 2024), no significant socioeconomic differences were observed in children’s HRQoL. Overall HRQoL scores were comparable to previous studies (Haraldstad et al., 2023), suggesting that children perceive a generally good quality of life regardless of SES. This may be partly explained by Portugal’s social protection model, which provides universal health care, social support, and free education, potentially mitigating the effects of socioeconomic disadvantage (Befus et al., 2024; Rijlaarsdam et al., 2013). Educational policies promoting inclusion, cooperative learning, and extracurricular engagement (Costa, 2022; Palmeirão et al., 2024) may also serve as protective factors.
Targeted investments in mental health promotion, particularly for socioeconomically disadvantaged households, are both socially just and economically strategic, yielding long-term returns by reducing expenditures in health care, education, child protection, and the justice system (Barican et al., 2022; Tamura et al., 2020).
This study has several strengths. The use of the SII provides a robust measure of social gradients (Hyldgård et al., 2021), while adjustment for relevant confounders strengthens the validity of findings. The use of validated instruments and self-completion methods enhances accuracy, as third-party reports often underestimate children’s perceived HRQoL (Jozefiak et al., 2008; Maria et al., 2017; Khanna et al., 2022). In addition, applying these instruments to children aged 6 and above with trained researcher support offers reliable data, even though their use in this age group is not universally established (Riiser et al., 2020).
Limitations include the design of the study (cross-sectional), reliance on parent-reported measures, which may introduce social desirability bias, a sample size that may limit statistical power, and potential under-representation of parents with lower educational attainment (Bonevski et al., 2014).
Overall, these findings emphasize the importance of considering child mental health within the broader context of family and social determinants. Reducing socioeconomic inequalities is not only a matter of social justice but also a strategic imperative to promote healthy developmental trajectories and reduce the long-term societal burden of mental health difficulties.
Conclusion
This study provides robust evidence of significant and direct associations between socioeconomic inequalities and mental health outcomes in school-age children. The results highlight the urgency of implementing integrated public policies that recognize families as central agents in mitigating health disparities and promoting children’s mental well-being.
Addressing these inequalities demands coordinated action across sectors, sustained monitoring, and a commitment to equity-driven strategies that guarantee all children, regardless of their socioeconomic background, the opportunity to thrive. By ensuring that every child can grow, learn, and participate fully in society, we are not only advancing public health goals but also strengthening the social fabric upon which future generations will depend.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254251396276 – Supplemental material for Social inequalities in child mental health: Evidence from vulnerable families
Supplemental material, sj-docx-1-jbd-10.1177_01650254251396276 for Social inequalities in child mental health: Evidence from vulnerable families by Cristiana Lopes, Luísa Barros, Ana Duarte, Juliana Martins, Silvana Martins, Maria José Silva, Cláudia Augusto and Rafaela Rosário in International Journal of Behavioral Development
Footnotes
Acknowledgements
We express our heartfelt gratitude to all participants who contributed to this study.
ORCID iDs
Ethical Considerations
This study was approved by the Ethics Committee for Life and Health Sciences (CEICVS 009/2022) of the University of Minho.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
Not applicable.
Author Contributions
Conceptualization: C.L., L.B., A.D., J.M., S.M., C.A., and R.R. Data curation: C.L., J.M., R.R. Formal analysis: C.L., L.B., J.M., S.M., and R.R. Funding acquisition: R.R. Investigation: C.L., L.B., A.D., J.M., S.M., C.A., M.J.S., and R.R. Methodology: C.L., L.B., A.D., J.M., and R.R. Project administration: R.R. Resources: A.D., R.R. Software: C.L., A.D., J.M., and R.R. Supervision: L.B., S.M., and R.R. Validation: C.L., L.B., J.M., S.M., and R.R. Visualization: C.L., S.M., and R.R. Writing—original draft: C.L., R.R. Writing—review & editing: C.L., L.B., A.D., J.M., S.M., C.A., M.J.S., and R.R.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação para a Ciência e a Tecnologia, I.P. (PTDC/SAU-ENF/2584/2021).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.