
Abstract
The mechanisms within the home environment by which early life experiences of intimate partner violence (IPV) might affect children’s social functioning remain unclear. The aim of this study was to investigate the extent to which maternal depressive symptoms and maternal engagement (at 4 years postpartum) mediated the relationship between children’s early life experiences of IPV (first year of life) and social functioning in middle childhood (10 years of age). A second aim was to determine whether child sex moderated these relationships. Drawing data from a community sample of 1,507 Australian mothers and their firstborn children, we found that IPV occurring in the first 12 months of a child’s life was associated with high maternal depressive symptoms at 4 years postpartum, which in turn were associated with lower child social skills, higher peer problems, peer victimisation and bullying at age 10 years. Higher levels of maternal engagement at 4 years was associated with higher social skills at age 10 years. The patterns of relationships between IPV, maternal depressive symptoms, maternal engagement and social functioning were found to be similar for boys and girls. The findings highlight the importance of supporting mothers’ mental health and engagement in home learning during early childhood to facilitate children’s social development following IPV exposure.
Keywords
It is estimated that one in three Australian children grow up in homes where intimate partner violence (IPV) is occurring (Gartland et al., 2021; Scott & Mathews, 2023). IPV is defined as physical, sexual and/or psychological harm inflicted by a current or former intimate partner, including coercive and controlling behaviours (World Health Organization [WHO], 2021). Children who are exposed to IPV are at risk of poor social development (Bender et al., 2022; Lee et al., 2022; Schulz et al., 2023). Traumatic and stressful experiences such as IPV during early childhood can impact brain development and be detrimental to the development of social skills and peer relationships (Agorastos et al., 2019; Alink et al., 2012; Doyle & Cicchetti, 2017). While it is established that children with experiences of IPV are at risk of poor social functioning, there is limited longitudinal research investigating the mechanisms which affect this relationship (Bender et al., 2022; Lee et al., 2022). Understanding the mechanisms within a child’s family environment that may lead to poor social functioning are particularly important to consider as they provide insight into factors which might promote resilience and potential points of intervention (Holmes et al., 2022). Therefore, the aim of the current research was to investigate maternal mental health and maternal engagement which are two important aspects of the caregiving/family environment that might mitigate the risk of poor social functioning in children exposed to IPV.
Impact of IPV on Social Development
It is well recognised in the field, that IPV exposure whether directly witnessed or not can have deleterious impacts on development across the lifespan (Øverlien, 2009; Vu et al., 2016; Wood & Sommers, 2011), including poor social functioning (Bender et al., 2022; Lee et al., 2022). This has been supported by studies showing that children are profoundly aware of the dynamics within their environment, and can be aware of IPV occurring by hearing or seeing the abuse occurring, intervening in violence, or witnessing the aftermath of abuse such as tension or conflict, or remorse and distress from caregivers (Øverlien, 2009; Edleson, 1999; Fusco & Fantuzzo, 2009). Children can demonstrate social functioning across a range of domains, including their use of social skills, peer relationships and problematic social behaviour such as bullying or aggression towards peers (Beauchamp & Anderson, 2010; Bishop et al., 2019; McQuade et al., 2013). Several studies have found IPV between caregivers in childhood to be associated with higher levels of social-emotional problems, bullying, victimisation and poorer social skills (Bowes et al., 2009; Fusco, 2015; Holmes et al., 2015; Hsieh et al., 2021; Katz et al., 2007; Mastorakos & Scott, 2019; Williamson et al., 2018). However, findings from recent systematic reviews highlighted the need for further longitudinal research on IPV exposure and social outcomes (Bender et al., 2022; Lee et al., 2022). The majority of studies included in these reviews are cross-sectional and include pre-school or school-aged children with few studies focusing on IPV exposure during infancy and long-term social outcomes (Bender et al., 2022). There are also mixed findings regarding sex differences, with only three articles in Lee et al. (2022) examining sex differences between boys and girls. However, a recent longitudinal study found that IPV occurring between caregivers during infancy to be associated with lower social skills, higher levels of peer problems and peer victimisation at 10 years of age, with no difference found between boys and girls (Schulz et al., 2023). The findings from this body of research highlighted the need for longitudinal designs to investigate risk and protective pathways between early IPV exposure and child social outcomes, such as parent mental health and parenting (Bender et al., 2022; Holmes et al., 2022; Lee et al., 2022; Schulz et al., 2023).
Mechanisms Between IPV Exposure and Children’s Social Functioning
Understanding the family factors which impact the relationship between IPV and social development is important given children’s dependence on caregivers for emotional nurturance and social role modelling during early childhood (Cameranesi & Piotrowski, 2020). One potential pathway by which IPV may affect children’s social functioning is via maternal mental health difficulties. The impact of IPV on maternal mental health has been well documented, with women who experience IPV at increased likelihood of mental health difficulties including symptoms of post-traumatic stress disorder (PTSD), depression, anxiety and suicidality following experiences of IPV (Beydoun et al., 2012; Brown et al., 2020; Greene et al., 2018; White et al., 2023). In particular, numerous studies have highlighted the presence of depressive symptoms during the postpartum period for mothers experiencing IPV (Ankerstjerne et al., 2022; Beydoun et al., 2012).
Mothers experiencing depressive symptoms following IPV may have more difficulty forming secure attachment with their child (Badovinac et al., 2018; Boeckel et al., 2015) which is vital in supporting the skills needed for children to independently manage their own social and emotional functioning with peers (Groh et al., 2014). A caregiver who has difficulties regulating negative emotions might face barriers that limit their capacity to engage in sensitive and attuned caregiving or to model and respond to positive social behaviours and skills (Śliwerski et al., 2020). While there has been longitudinal research highlighting maternal depressive symptoms as a mediator between early IPV exposure and child emotional-behaviour difficulties at age 10 years (Skinner et al., 2019), there has been less research focusing on social outcomes. However, a cross-sectional study of 981 mother–child dyads found maternal depressive symptoms mediated the relationship between physical and sexual IPV and child socioemotional functioning (Ramos de Oliveira et al., 2022). Furthermore, a longitudinal study using a sample of children involved in child protection found that children’s exposure to physical IPV at age 2–3 increased maternal depression, which in turn was associated with increased overt aggressive behaviour at 4–5 years old (Holmes et al., 2017). However, this study only focused on physical IPV and overt aggressive behaviours. Understanding maternal depressive symptoms as a mechanism between emotional and physical IPV during infancy and multiple domains of social development during middle childhood may further our understanding of the long-term impacts of IPV during early childhood.
Another pathway through which IPV might impact social functioning is via parent-child interactions or parenting behaviour. Research has documented that IPV experiences can be associated with a range of negative or suboptimal parenting behaviours such as physical aggression, hostile or harsh parenting, neglect, and lower engagement and warmth (Chiesa et al., 2018; Krishnakumar & Buehler, 2000). Experiencing IPV may impede a mothers’ capacity to engage in everyday activities such as reading, storytelling, social play and spending time together, which in turn may limit opportunity to respond to positive social behaviours during everyday activities. These everyday activities can help to promote children’s social skills and understanding of relationships in early childhood (Sénéchal & LeFevre, 2002). However, few studies have examined parenting as an underlying mechanism between IPV and child outcomes. One cross-sectional study of 15,202 children aged 3 and 4 years old and their mothers found that the relationship between IPV and early childhood development (cognitive, literacy, numeracy, socioemotional and physical development) was partially mediated by maternal and paternal stimulation including activities such as reading, looking at pictures together, telling stories and playing (Jeong et al., 2020). Another study of 497 families with 3- to 5-year-old children found that psychological IPV was associated with using more restrictive/punitive parenting, and in turn higher levels of externalising behaviours (Greene et al., 2018). While both studies suggest the early parent–child relationship is a possible mechanism linking IPV to child outcomes, they are limited to cross-sectional designs and do not investigate social outcomes such as peer relationships and social skills specifically. The identification of potential family factors (i.e., maternal depressive symptoms and parenting) which might mitigate the risk of poor social functioning in children exposed to IPV is critical in informing points of intervention and approaches to prevent the negative developmental trajectories following IPV exposure.
The Current Study
The current study draws on an Australian community-based longitudinal study of 1,507 women and their firstborn children. The first aim of the study was to determine the extent to which maternal depressive symptoms and maternal engagement (at 4 years postpartum) mediated the relationship between children’s early life experiences of IPV (first year of life) and social functioning in middle childhood (10 years of age). It was hypothesised that IPV exposure would be associated with higher levels of maternal depressive symptoms and lower levels of maternal engagement, and in turn lower social skills, higher peer problems, and higher bullying and victimisation at age 10 years. A second aim was to determine whether child sex moderated these relationships. Given the ambiguity of findings regarding sex differences for outcomes of IPV, the second hypothesis was exploratory.
Method
Study Design and Participants
Data were drawn from the Mothers’ and Young People’s Study, a longitudinal study of the health and well-being of 1,507 first-time mothers and their firstborn child. Women were recruited during early pregnancy from April 2003 and December 2005 across six public hospitals in Melbourne, Australia. Women were given information about the study during antenatal appointments and childbirth education class and were mailed an invitation by maternity hospitals. Women were eligible to participate if they were: (a) nulliparous, ⩽24 weeks’ gestation, (b) aged ⩾18 and (c) sufficiently proficient in English to complete study questionnaires. Follow-up data were collected at 3, 6, 12 and 18 months, and 4 and 10 years postpartum. In this article, demographic data were drawn from questionnaires completed at baseline (in pregnancy ⩽ 24 weeks gestation) and 3 months postpartum, IPV at 1-year postpartum, maternal depressive symptoms and maternal engagement at 4 years postpartum and social functioning at 10 years postpartum. We were particularly interested in maternal depressive symptoms and maternal engagement as potential mechanisms when the children were 4 years of age, which is a critical time for children’s pre-school development. Ethics approval was obtained via research ethics committees of participating hospitals, the Royal Children’s Hospital, La Trobe University and Swinburne University of Technology (20226560-10174).
A total of 1,507 eligible women were eligible and enrolled in the study. A range of basic demographic characteristics were collected from women during pregnancy and in the first 3 months after birth (i.e., age, employment, relationship status and country of birth; see Table 1). At the time of enrolment, the majority of mothers were aged between 25 and 34 years at the time of enrolment, were in paid employment during pregnancy and were born in Australia. Follow-up questionnaires were completed by 1,357 women at 12 months postpartum, and 950 at 10 years postpartum after their first baby. Selective attrition was observed whereby women who completed the 10-year follow-up more likely to be university educated, Australian born, not on a government benefit and less likely to have reported depressive symptoms in the first year postpartum (Brown et al., 2021). Mothers who had experienced IPV were less likely to be in paid employment, and more likely to have a lower educational qualification, be divorced or living with a partner, and to have a health care card compared to mothers who had not experienced IPV.
Demographic Characteristics of the Sample (N = 1,507).
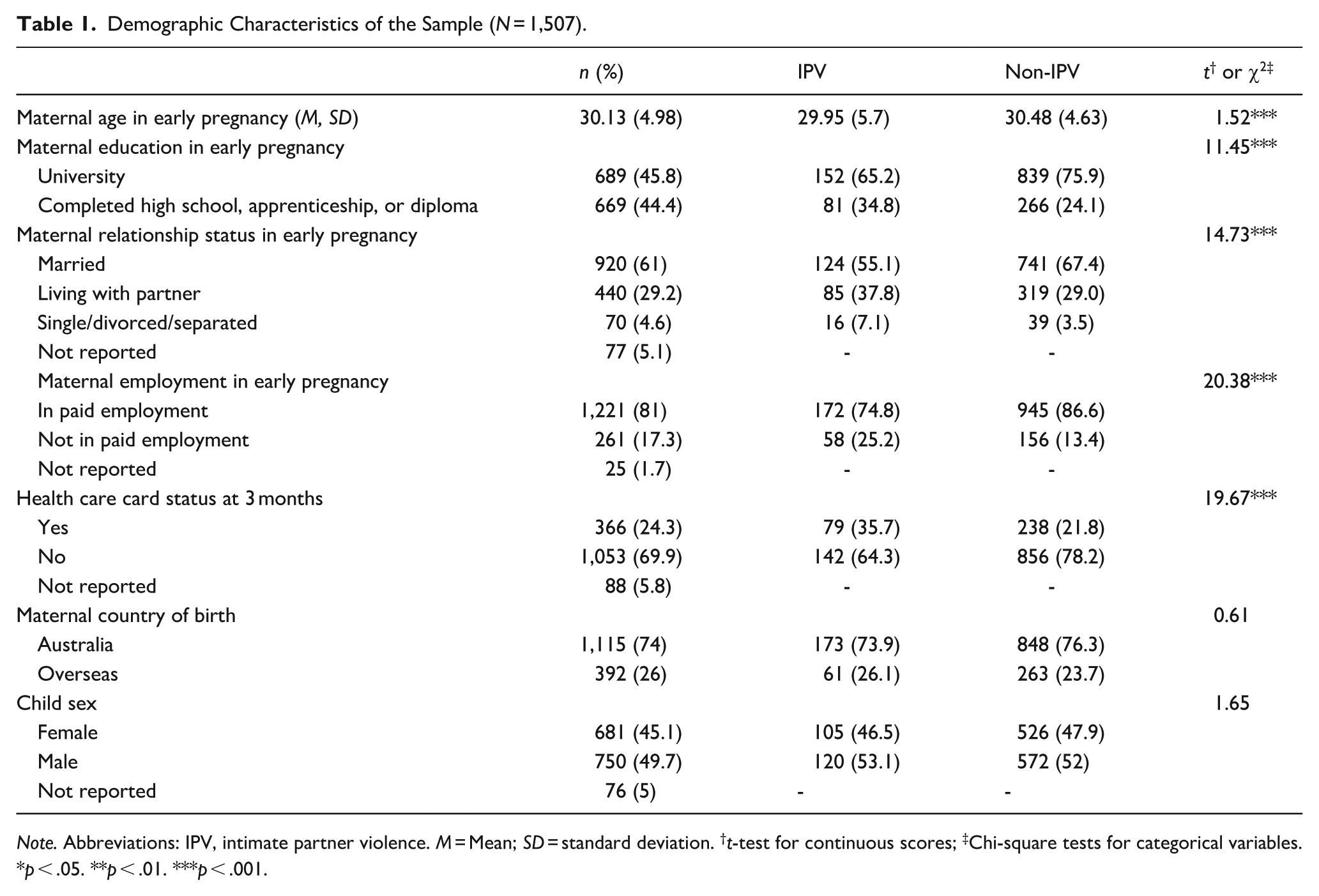
Note. Abbreviations: IPV, intimate partner violence. M = Mean; SD = standard deviation. †t-test for continuous scores; ‡Chi-square tests for categorical variables.
p < .05. **p < .01. ***p < .001.
Measures
Intimate Partner Violence
Exposure to emotional and physical IPV was assessed at 12 months using the 18-item Composite Abuse Scale (CAS; Hegarty et al., 1999, 2005). The CAS is a comprehensive multidimensional measure of IPV that includes items asking about emotional abuse (e.g., ‘tried to keep me from seeing or talking to my family’), and physical abuse (e.g., ‘pushed, grabbed, or shoved me’) by a current or former partner. Women were asked to indicate how often these actions happened in the previous 12 months on a 5-point Likert-type scale (never, only once, several times, once per week, or daily). In line with scoring instructions, women were categorised as experiencing physical abuse if they endorsed a score of ⩾1 on the physical IPV items, and emotional abuse if ⩾3 on emotional IPV items (Hegarty et al., 2005). The CAS has consistently demonstrated high reliability and validity (Hegarty et al., 2005). For the current sample, the internal consistency for emotional (Cronbach’s α = .85) and physical (Cronbach’s α = .89) abuse at 12 months was good.
Maternal Depressive Symptoms
Maternal depressive symptoms at 4 years postpartum was assessed using the 10-item Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987). The scale measures depressive symptoms such as ‘I have been so unhappy that I have been crying’, with higher scores indicating higher depressive symptoms severity. Women are asked to report the extent to which they have experienced symptoms in the last week (0 = never, 1 = not often, 2 = sometimes and 3 = most of the time). The EPDS is well validated within postnatal and non-postnatal populations, as well as Australian populations (Cox et al., 1996; Murray & Cox, 1990). The scale has also demonstrated good sensitivity and specificity in identifying women experiencing major depression (Levis et al., 2020). For the current sample the EPDS had good internal consistency (Cronbach’s α = .90).
Maternal Engagement
Maternal engagement in children’s home learning at 4 years postpartum was assessed using five items from the Longitudinal Study of Australian Children (LSAC; National Centre for Educational Statistics, 2000). The scale is used to measure the frequency that several parent–child activities occur in the home, including reading, storytelling, playing games and playing outdoors/exercising. Mothers were asked to indicate how often they engaged in these activities with their children on a 4-point scale (0 = none, 1 = 1 or 2 days, 2 = 3 to 5 days, 3 = 6 to 7 days). For the current sample there was good internal consistency for maternal engagement (Cronbach’s α = .73).
Children’s Social Functioning
Social Skills Improvement System
Social skills were assessed using four of the parent-reported subscales from the Social Skills Improvement System (SSIS) at age 10 (Gresham et al., 2010). The social skills subscales had good internal consistency and included responsibility (e.g., ‘takes responsibility for his/her actions’; Cronbach’s α = .82), self-control (e.g., ‘stays calm when teased; Cronbach’s α = .84), communication (e.g., ‘takes turns in conversations’; Cronbach’s α = .82) and cooperation (e.g., ‘completes tasks without bothering others’; Cronbach’s α = .77). Mothers indicated how often their child exhibits each social skill on a 4-point scale ranging from never to almost always. Lower scores indicated poorer social skills. Bullying was assessed using the five-item bullying subscale from the problem behaviours domain on the SSIS (e.g., ‘does things to make others feel scared’). For the current sample, the problem behaviours domain had good internal consistency (Cronbach’s α = .79). Mothers were asked to indicate how often their child exhibits bullying behaviours on a 4-point scale ranging from never to almost always. Higher scores indicated higher levels of bullying behaviour towards other children.
Strengths and Difficulties Questionnaire (SDQ) – Peer Problems Subscale
Peer problems were assessed using the five-item Peer Problems scale on the SDQ at age 10 (e.g., ‘rather solitary, refers to play alone’; Goodman, 1997). Mothers were asked to rate the extent to which behaviours were true of their child over the past 6 months on a 3-point scale ranging from not true to certainly true. Higher scores indicated higher levels of peer difficulties. For the current sample, the peer problems subscale had good internal consistency (Cronbach’s α = .67).
Social Experience Questionnaire
Peer victimisation was measured using the parent-report of the Social Experience Questionnaire (SEQ) which assesses peer victimisation (Crick & Grotpeter, 1996). Three items from the overt victimisation subscale (e.g., frequency with which peers attempt to harm child) and three items from the relational victimisation subscale (e.g., frequency with which peers attempt to harm child’s relationships with others) were used. For the current sample, the overt victimisation (Cronbach’s α = .88) and the relational victimisation subscale (Cronbach’s α = .81) had good internal consistency. Mothers rated their child’s behaviour on a 5-point scale ranging from never true to always true, where higher scores indicated higher levels of peer victimisation.
Data Analysis
Exploratory data analysis was conducted in SPSS version 28 (IBM Corp, 2012) for descriptive statistics and correlations. Structural equation modelling (SEM) in Mplus version 8.8 (Muthén & Muthén, 1998–2011) was used to test the hypothesised model specifying directional longitudinal relationships between early IPV exposure, maternal depressive symptoms and maternal engagement, and children’s social functioning. The hypothesised model for early IPV exposure and children’s social functioning is presented in Schulz et al. (2023). However, the current study extends upon this work, by testing mediators of maternal depressive symptoms and maternal engagement. All SEM models were estimated using robust maximum likelihood estimation due to skewness in some variables. Missing data were managed using Full Information Maximum Likelihood (FIML), which incorporated all independent, dependent and intervening variables as well as covariates which were also variables associated with study attrition (i.e., level of education, recipient of government benefit). Model fit was assessed using a range of fit indices including Satorra-Bentler Chi-square test, Tucker–Lewis index (TLI), comparative fit index (CFI) and root mean square error of approximation (RMSEA). Indices for the RMSEA are acceptable when close to or below 0.05, and values for the TLI and CFI should exceed 0.90 for acceptable fit (Hu & Bentler, 1999).
The adequacy of the measurement model was assessed first by testing the construct validity of all the latent variables in the hypothesised model. Next, the structural model of the associations between the latent constructs were tested. The model tested the longitudinal relationship between early life IPV, maternal depressive symptoms, maternal engagement at 4 years and social functioning at 10 years. Given research indicating that a range of socioeconomic and demographic factors are associated with IPV and children’s social-emotional development (Bradley & Corwyn, 2002; Gartland et al., 2016), the following were included as covariates in the model: maternal age, highest level of education completed, employment status during pregnancy, health care card status at 3 months postpartum and number of children at 10 years postpartum. Maternal country of birth was not included as a covariate given that majority of mothers in the sample were born in Australia, and correlations indicated country of birth was not correlated with IPV or maternal depressive symptom subscales. The indirect effects were estimated using the product of coefficients approach (MacKinnon et al., 2002), with bootstrap confidence intervals (CIs) obtained using the bias-corrected bootstrap option (1,000 draws). A statistically significant estimate with CIs not crossing 0 is accepted as evidence of an indirect effect.
Finally, multigroup analyses were conducted to test whether child sex at birth (boy or girl) moderated the structural paths in the model. A model with all parameters freely estimated was compared to a model with all parameters constrained to be equal using the Satorra-Bentler nested chi-square difference test. A lack of significant difference between the models indicates there is no difference in the regression paths between boys and girls.
Results
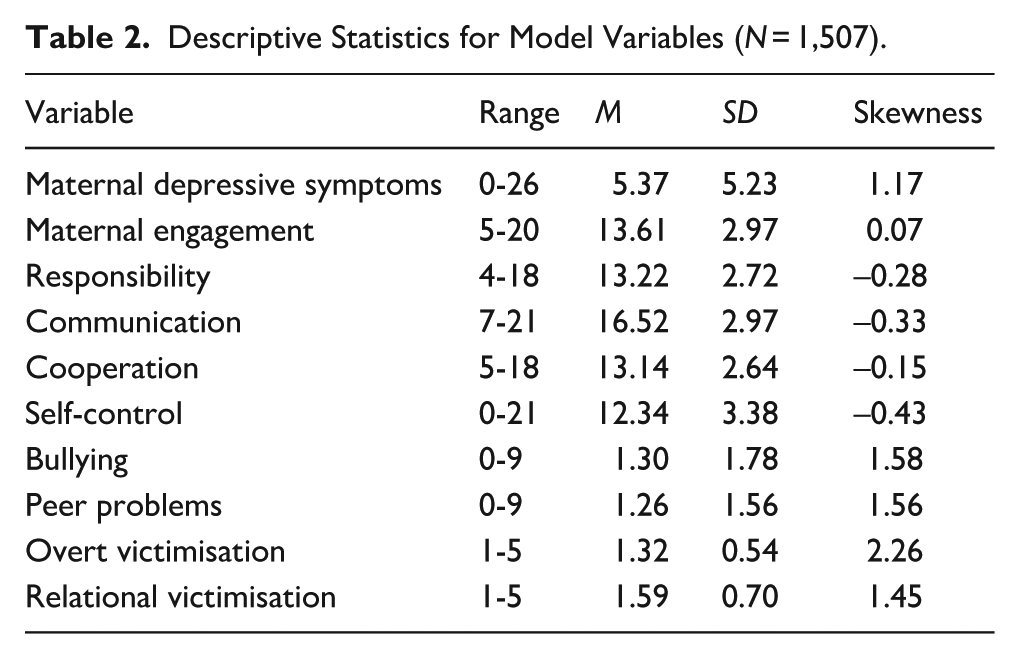
Missing data were 26.2% across all study variables. There was one case that did not have any data available on the model variables and was excluded from the analysis. Missing data was managed using Full Information Maximum Likelihood (FIML) and variables associated with selective attrition in the study were included as covariates. Table 2 presents descriptive statistics for all the model variables and Table 3 presents the correlations among all model variables. Physical and emotional abuse during the first 12 months, maternal depressive symptoms, bullying, peer problems, overt victimisation and relational victimisation were positively skewed. Communication, cooperation and responsibility were mildly negatively skewed. During the first year after birth, 17.4% (234/1,346) of mothers reported IPV. Of the women who reported IPV, 9.5% reported emotional abuse alone, 5.6% reported both physical and emotional abuse and 2.2% reported physical abuse alone.
Descriptive Statistics for Model Variables (N = 1,507).
Correlations for Model Variables and Covariates.
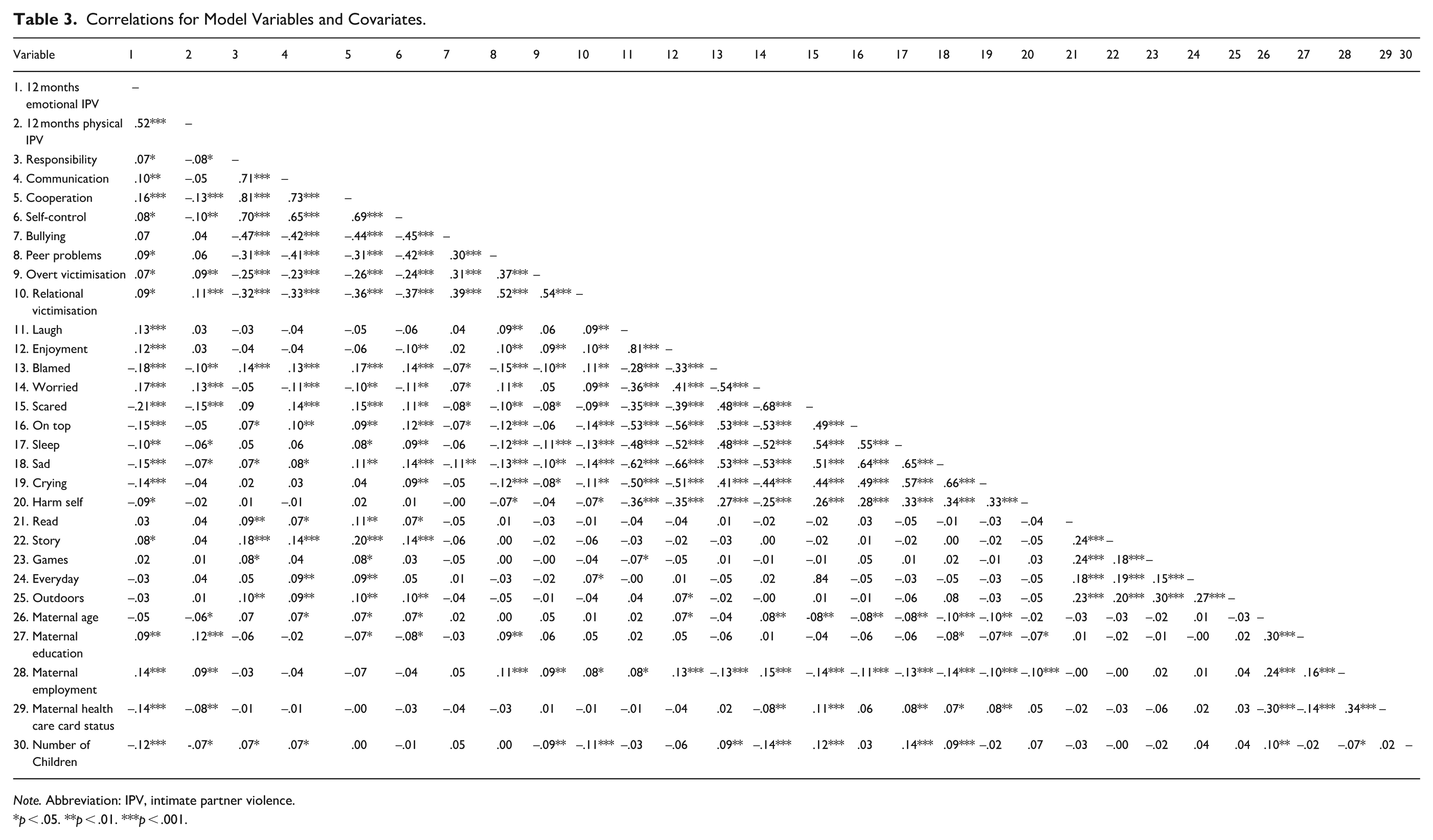
Note. Abbreviation: IPV, intimate partner violence.
p < .05. **p < .01. ***p < .001.
Testing the Measurement Models
Table 4 presents the fit statistics for each of the measurement models. The social skills latent construct was represented by four SSIS subscales (communication, cooperation, responsibility, self-control) and this was a good fit to the data. Model fit for the latent constructs represented by peer problems, peer victimisation and bullying could not be determined due to having less than four indicators. Peer victimisation was represented by two subscales from the SEQ (overt and relational victimisation), while peer problems and bullying were represented by single indicator latent variables created from subscales on the SDQ and SSIS, respectively, using Munck’s formula (Warren & Munck, 1980).
Measurement Models (N = 1,507).
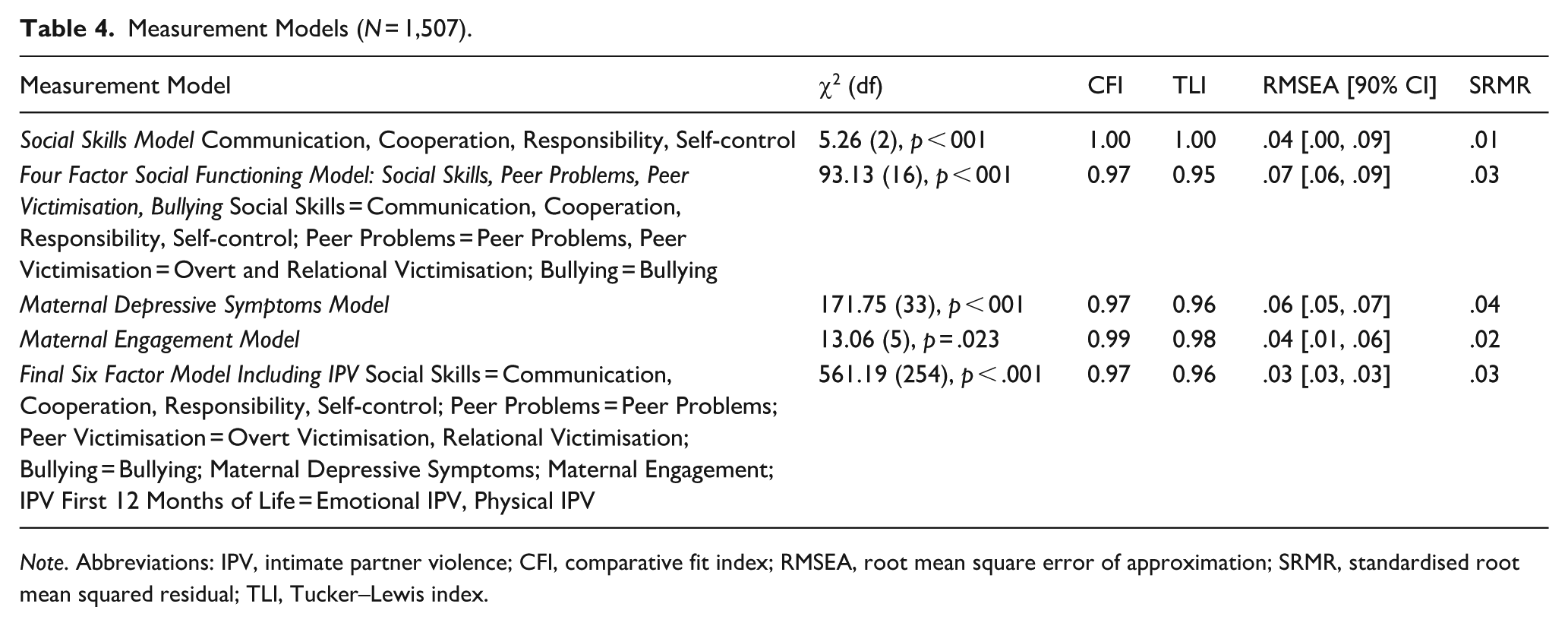
Note. Abbreviations: IPV, intimate partner violence; CFI, comparative fit index; RMSEA, root mean square error of approximation; SRMR, standardised root mean squared residual; TLI, Tucker–Lewis index.
Next, a four-factor model of social functioning including social skills, peer problems, peer victimisation and bullying was tested and found to be a good fit to the data. Maternal depressive symptoms and maternal engagement latent constructs were both found to be a good fit to the data. Finally, the full measurement model including each of the social functioning latent constructs, maternal depression and engagement at 4 years, and IPV in the first year of life measured by the CAS subscales (emotional and physical IPV) was a good fit to the data.
Aim 1: Testing the Structural Model
A model of the association between IPV occurring in the first year of a child’s life and social functioning at age 10 years via maternal depressive symptoms and maternal engagement at 4 years was a good fit to the data, χ2 (349, N = 1,506) = 713.14, p < .001, RMSEA = .03 (90% CI [.02, .03]), TLI = 0.96, CFI = 0.97. Figure 1 presents the structural model and standardised path estimates. The model shows that early IPV was significantly associated with maternal depressive symptoms at 4 years, and in turn poorer social skills, higher levels of peer problems, peer victimisation and bullying at age 10 years. Early IPV was not significantly associated with maternal engagement at 4 years, and maternal engagement was not significantly associated with peer problems, peer victimisation or bulling at age 10. Maternal engagement at 4 years was significantly associated with higher levels of children’s social skills at age 10 years.
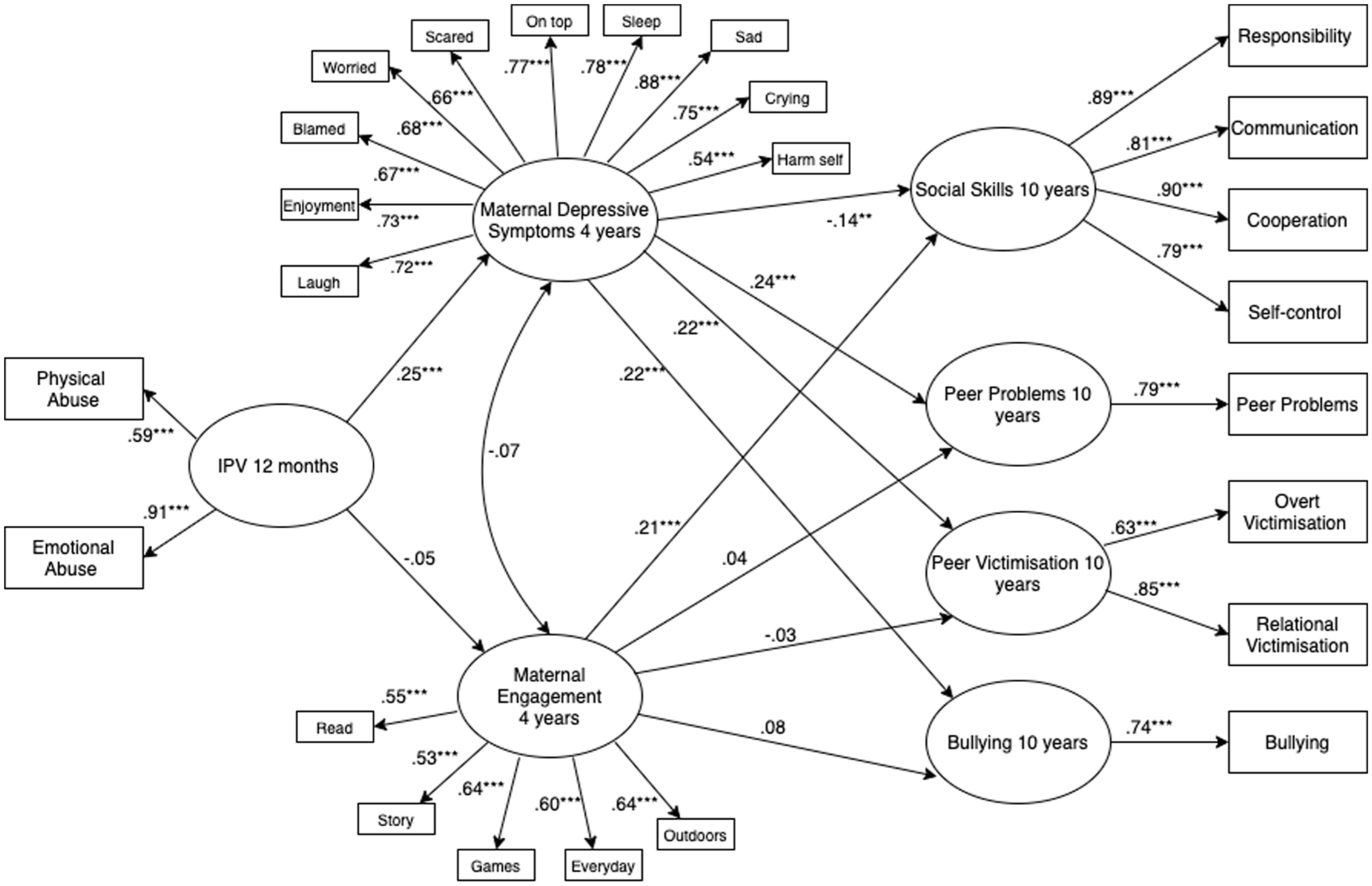
Association Between IPV 12 Months, Maternal Depressive Symptoms and Engagement at Age 4, and Social Skills, Peer Problems, Peer Victimisation and Bullying at Age 10.
Table 5 presents the standardised estimates and 95% CIs for the direct and indirect effects of early life exposure to IPV on social outcomes via maternal depressive symptoms and maternal engagement at 4 years. The indirect pathways from early IPV exposure to social skills, peer problems, peer victimisation and bullying at 10 years via maternal depressive symptoms at 4 years were significant. The indirect pathway from early IPV exposure to social skills, peer problems, peer victimisation and bullying at 10 years via maternal engagement at 4 years were not significant.
Standardised Estimates and Confidence Intervals for Direct and Indirect Paths for the Structural Model (N = 1,507).
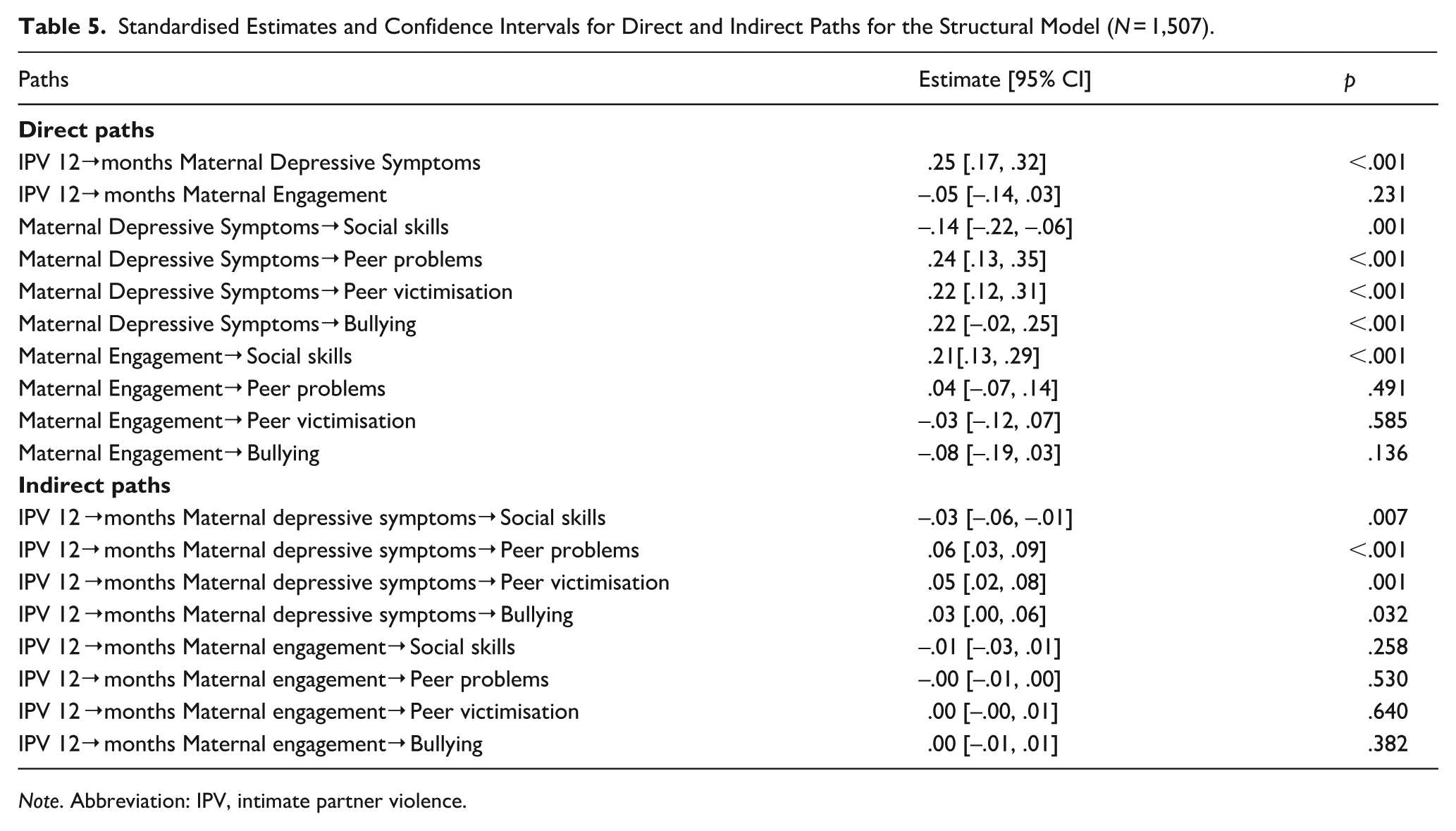
Note. Abbreviation: IPV, intimate partner violence.
Aim 2: Multi-Group Analyses to Test Moderation by Child Sex
Multigroup analyses to test whether child sex moderated the model of the association between early IPV and social functioning at 10 years via maternal depressive symptoms and maternal engagement revealed no evidence of moderation, Satorra-Bentler Δχ2 (11) = 8.90, p = .631.
Discussion
This study used a longitudinal cohort to examine the role of maternal mental health and maternal engagement as mechanisms between IPV occurring during the first 12 months of a child’s life and social functioning during middle childhood. This study found that IPV occurring during the first year of life was associated with maternal depressive symptoms at 4 years, which in turn were associated with poorer social skills, higher levels of peer problems, peer victimisation and bullying at age 10 years. These findings suggested that maternal depressive symptoms are a mechanism by which early IPV exposure can indirectly affect children’s long-term social functioning during middle childhood. Early IPV was not associated with maternal engagement in home learning activities at 4 years, and this in turn was not associated with peer problems, peer victimisation, or bullying at age 10. However, maternal engagement at 4 years was associated with higher levels of children’s social skills underscoring the importance of maternal engagement for the development of children’s social skills. The findings along with the implications for theory and practice will now be discussed.
Maternal depressive symptoms were identified as a key mechanism underlying the association between IPV during infancy and children’s social skills reflecting responsibility (e.g., ability to follow rules), communication (e.g., communicate in appropriate tone of voice), cooperation with others (e.g., take turns) and self-control (e.g., remain calm when disagreeing with others) during middle childhood. Maternal depressive symptoms were also a mechanism through which children experiencing early IPV displayed more peer problems and had more difficulties making friends, were more likely to be bullied or have their relationships with others harmed by peers and were also more likely to bully others. Building on research documenting the impact of IPV on women’s mental health (Ankerstjerne et al., 2022; Beydoun et al., 2012; Brown et al., 2020) and the flow on effects to emotional-behavioural outcomes (Holmes et al., 2017; Ramos de Oliveira et al., 2022; Skinner et al., 2019) our study is the first known to show maternal depressive symptoms as a pathway by which IPV during infancy impacts on multiple domains of social functioning in middle childhood. These findings can best be understood from a developmental psychopathology and trauma perspective.
Infancy and early childhood represent one of the most vulnerable periods in brain maturation, placing younger children at increased risk of poor development due to early life trauma (Mueller & Tronick, 2020). Mothers experiencing depressive symptoms might have limited resources to engage in attuned and consistent caregiving, potentially impacting children’s early attachment (Badovinac et al., 2018). This may be particularly salient for mothers’ who have also experienced traumatic events associated with IPV (Boeckel et al., 2015; Noonan & Pilkington, 2020). Disruption to attachment during the early years of life could impact on children’s developing social skills and capacity for future peer relationships (Groh et al., 2014; Howell et al., 2016). Mothers without experiences of IPV and depressive symptoms might have more capacity to manage stress and engage in social role modelling and reinforcement of positive social behaviours displayed by their children during early childhood (Śliwerski et al., 2020). Children may also have heightened awareness of potential threats in the environment such as signs of aggression or conflict from family or peers which may be exacerbated by parental mental health difficulties such as depressive symptoms (Agorastos et al., 2019; Howell et al., 2016). These processes may have a flow on effect to the development of children’s social skills, ability to feel safe and engaged in peer relationships outside of the home environment, and capacity to manage conflict or friendship difficulties (Howell et al., 2016; Lee et al., 2022). These difficulties may not manifest or be noticeable until there is an increased importance and reliance on peer relationships during middle childhood (Holmes et al., 2015).
Despite research documenting a relationship between IPV and parenting behaviours such as hostile or harsh parenting, physical aggression, and lower engagement and warmth (Chiesa et al., 2018; Krishnakumar & Buehler, 2000) we did not find an association between IPV and engagement in early home learning activities. This is an important finding suggesting that mothers’ capacities to engage in enriching activities such as reading, playing, storytelling and spending time outdoors are not necessarily affected by experiences of IPV. It has been also been suggested that some mothers experiencing IPV may compensate for children’s adverse experiences by being warmer, more nurturing and striving to protect their children (Fogarty et al., 2019b; Lapierre, 2010) as well as being more engaged during play time (Letourneau et al., 2013). Engagement in enriching home learning activities may be important in strengthening mother–child relationships, and protect against the potential impact of early life IPV on children’s social development.
Indeed, we found that maternal engagement in early home learning activities at 4 years was associated with well-developed social skills including responsibility, communication, cooperation and self-control in middle childhood. This finding suggests that maternal engagement in home learning activities is important in the development of social skills in all families. From a social learning theory perspective, parents and other caregivers’ model and reinforce children’s development and use of these fundamental social skills that are key to healthy relationships including those with peers as they get older. Despite this, we did not find that maternal engagement in everyday activities was associated with children’s peer problems, being bullied or bullying others. Navigating peer relationships, friendship difficulties and conflict, and bullying are complex social situations that children who have experienced IPV may have difficulty managing despite their experiences of maternal engagement and development of important social skills. There is a growing body of research that children who have experienced IPV in early life including physical IPV and co-occurring child maltreatment are at increased risk of bullying and peer victimisation during middle childhood (Hsieh et al., 2021; Lee et al., 2022; Williamson et al., 2018). Further research is needed to better understand how children who have experienced IPV can be supported to manage conflict and difficulties in peer relationships. Finally, our study found that the pattern of relationships between IPV, maternal depressive symptoms, maternal engagement and social functioning are similar for boys and girls. This is an important finding as there have been mixed findings about the impact of IPV on girls and boys (Lee et al., 2022).
Strengths, Limitations and Future Research
The current study provided a unique contribution to the evidence of maternal depressive symptoms as a mechanism between children’s early life exposure to IPV and long-term social outcomes. First, the study drew upon data from a community-based sample of mothers and their firstborn child, rather than clinical populations or samples from domestic violence shelters. The study addressed limitations of previous research by assessing multiple domains of social functioning, as well as incorporating a comprehensive measure of IPV assessing both physical and emotional abuse. The study also utilised a longitudinal design to investigate pathways through which early IPV impacts social outcomes, adding to our understanding of family factors which might exacerbate as well as mitigate the risk of poor social functioning in children exposed to IPV. However, there were also several limitations to consider. While the sample was representative in terms of infant birthweight and gestation it consisted predominately of English-speaking women who were Australian born, university educated and more socioeconomically advantaged. Therefore, the findings are unlikely to fully capture the experiences of ethnic minorities or families experiencing poverty who may be at increased risk of IPV (Skafida et al., 2021). The measures used were entirely based on mothers’ reports. Other sources of information such as teachers’ and children’s reports and standardised assessments of children’s social functioning along with clinical tools to determine mental health difficulties would allow for a more comprehensive and objective measurement. Maternal engagement was also measured based on quantity of time mothers spent engaging in everyday activities, limiting the study to only the frequency of engagement rather than the quality of time spent between mother and child. Future research could also utilise a larger sample of children exposed to IPV to identify potential differences between pathways from IPV to social functioning for girls and boys.
While the study investigated mechanisms of maternal depressive symptoms and maternal engagement between early IPV and social functioning, there may also be other co-occurring adversities such as child abuse and neglect, and other family, child or environmental factors to consider. For instance, other mental health difficulties such as post-traumatic stress disorder (PTSD) or emotion dysregulation experienced by mother or child may be important factors to consider, as well as external supports such as the pre-school or primary school environment in fostering social development outside of the family home. Importantly, many children who have experienced IPV in their family environment show resilience (Fogarty et al., 2019a). Ongoing longitudinal research is needed to assess mediating or moderating factors that promote resilience, as well as further understanding environmental factors that promote positive peer relationships and social functioning. Consideration of patterns of exposure to IPV between infancy and middle childhood along with understanding different trajectories of mothers’ mental health following IPV is also needed to determine social outcomes at specific developmental periods associated with different patterns of exposure (Fogarty et al., 2023; Holmes et al., 2022). Finally, pathways to long-term trajectories of social functioning including peer and intimate relationships in adolescence and early adulthood should be examined to help identify key time points and areas for intervention (Holmes et al., 2022).
Implications for Policy and Practice
The current research supports developmental psychopathology and trauma theory perspectives that highlight the caregiving environment as an important factor influencing children’s developmental trajectory following early life trauma (De Bellis et al., 2001; Holmes et al., 2017). The study provides evidence for the role of maternal depressive symptoms as a mechanism through which early life IPV impacts children’s social skills, peer problems, peer victimisation and bullying during middle childhood, as well as the importance of maternal engagement for the development of children’s social skills. Given the impacts of IPV experiences on women and children during the first 12 months postpartum policy and service prevention efforts are necessary to prevent and reduce the impact of IPV during this vital period. Early intervention programmes prior to conception, during pregnancy and post birth can support parents and families to develop healthy communication, positive relationships and parenting, and may also prevent IPV or reduce its’ impact (Giallo et al., 2022). Identifying and increasing access to treatment for mothers experiencing depressive symptoms following IPV is important in supporting mothers to manage mental health difficulties, foster early attachment and attuned caregiving, and engage in positive social role modelling during early childhood. This may have a positive impact on children’s social outcomes reducing the risk of poor social skill development, peer difficulties and bullying experiences. Continuing to support all mothers’ engagement in everyday activities such as reading and playing with their children could also contribute to the learning of social skills during early childhood, facilitating long-term social skills.
Providing early intervention for women experiencing IPV as well as those using violence is important in preventing and reducing the impact of IPV on caregivers’ mental health. Early intervention focused on social skills and relationships for children with experiences of IPV during infancy along with caregivers may also facilitate healthy attachment and emotion regulation capabilities that may support engagement in positive peer relationships. To support health and community services, further research is needed on the development and viability of evidence-based early intervention programmes for social functioning (Australian Government, 2022). Children whose caregivers are/or have experienced depressive symptoms in particular might benefit from further support or intervention. Group programmes that allow children to practice social skills and healthy peer interactions may provide children with opportunities for social role modelling and positive reinforcement where this may be limited in the home environment. Wider implementation of group programmes for pre-school or school-aged children might assist children exposed to IPV in developing social skills and healthy peer relationships.
Footnotes
Acknowledgements
Madison L. Schulz received support through an Australian Government Research Training Program Scholarship.
Ethical Considerations
The Mothers’ and Young People’s Study received ethical approval from La Trobe University (2002/38), Royal Women’s Hospital (2002/23), Southern Health (2002-099B), Angliss Hospital and The Royal Children’s Hospital (27056A).
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Mothers’ and Young People’s Study was supported by the Australian National Health & Medical Research Council (NHMRC) Grants 199222, 433006 and 491205, and by Australian Rotary Health. Stephanie Brown is supported by a Leadership Investigator Grant awarded by the NHMRC (2018144). Research conducted at the Murdoch Children’s Research Institute is supported by the Victorian Government Operational Infrastructure Support Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The data and analytic code necessary to reproduce the analyses presented here are not publicly accessible, as well as the materials necessary to attempt to replicate the findings. The analyses presented here were not preregistered.