
Abstract
Self-regulation is integral to human well-being. Previous research established associations between self-regulation and life outcomes, although mostly based on cross-sectional or longitudinal research with relatively short follow-up periods. We aimed to investigate associations between self-regulation during childhood and low education, psychiatric diagnosis, conviction for non-violent and violent crime, and premature mortality up to 50 years later. The sample consisted of boys born between 1943 and 1951 in Stockholm, Sweden, who were initially interviewed as part of the Clientele Study and followed up until they were 58–66 years of age as part of the Stockholm Life Course Project (N = 251). Our measure of self-regulation was indicated by five dimensions extracted from multiple sources and informants when study members were children. Information on life outcomes were extracted from Swedish national registry data available through 2009. Results from logistic regression and survival analyses showed that lower self-regulation during childhood was associated with a higher risk of conviction for non-violent and violent crime, receiving a psychiatric diagnosis and premature mortality up until late adulthood. Self-regulation was not associated with low education. Analyses were adjusted for intelligence and parental socioeconomic status. While based on a relatively small sample and measurement of self-regulation using data from the 1960s, our study supports the notion that self-regulation during childhood is central for well-being across the lifespan.
Keywords
The ability to self-regulate is at the core of human well-being. Individuals who are better able to self-regulate are more likely to be healthier, financially successful and to refrain from deviant behavior (e.g., Moffitt et al., 2011; Robson et al., 2020). By extension, the inability to self-regulate incurs substantial costs to society (Algan et al., 2022). Since interventions that target cognition, social skills, and behavior are more likely to be effective during youth rather than adulthood (Knudsen et al., 2006), earlier predictors of later outcomes are of particular interest. However, most empirical research on the association between self-regulation and diverse outcomes is based on cross-sectional studies. Although longitudinal studies do exist, most have had shorter follow-up periods (Robson et al., 2020). Our aim was to extend previous research on the association between self-regulation and life outcomes in multiple domains by examining self-regulation during childhood and low educational attainment, criminal behavior, psychiatric diagnoses and premature mortality at 58–66 years of age.
The concept of self-regulation is used in several disciplines, particularly psychology but also neuroscience, economics, and criminology. This, in part, has contributed to a lack of consensus on the definition of self-regulation and to it being used interchangeably with the terms self-control, cognitive control, effortful control, and trait impulsivity. Here, we follow recent work toward integrating and synthesizing the research in different fields (Inzlicht et al., 2021; Nigg, 2017) and refer to self-regulation as an umbrella concept encompassing the process of determining a desired end state. It involves regulating behavior, thoughts, and emotions to achieve a goal. This differs from the more narrowly defined concept of self-control which is characterized by resolving conflicts between goals, often short- versus long-term goals (Inzlicht et al., 2021). However, we note that the definition of self-regulation above is similar to previous definitions of self-control. For example, self-control has often been defined as the ability to regulate behavior, cognition and emotion (e.g., de Ridder et al., 2012). Much of the previous literature on this concept in relation to outcomes in various domains used the terms self-control and self-regulation interchangeably. We use self-regulation as defined above and focus on trait aspects of self-regulation, or differences between individuals, rather than state aspects.
The concept of self-regulation is closely linked to that of executive functioning. Executive functioning is a set of higher-order functions controlled by the frontal lobe and involved in regulating cognition and behavior (Miyake et al., 2000). It is comprised of three subcomponents: updating working memory, attentional shifting, and inhibition of responses (Karr et al., 2018). While self-regulation is considered to be an inherent part of executive functioning in some work (e.g., Karr et al., 2018; Munakata & Michaelson, 2021), other work regards executive functioning as a separate, though linked, facet that subserves or supports successful self-regulation (Hofmann et al., 2012; Roebers, 2017). Our study follows this latter reasoning and is embedded in the developmental psychobiological framework of self-regulation (Blair & Raver, 2015). Within this framework, self-regulation is an allostatic process that operates on multiple levels: biological, social-emotional, behavioral, and cognitive. A hierarchy consisting of executive functions, attention, emotion, physiology, and genetic processes feed-forward and feedback on each other in the process of self-regulation (Blair & Raver, 2015). In this way, the ability to self-regulate is supported by executive functioning in addition to other psychological and biological processes, all of which are shaped by social and environmental factors.
Self-regulation is a complex trait. It spans species and is phylogenetically related to brain size (MacLean et al., 2014). Like most complex traits, self-regulation is determined by genetic, epigenetic, and environmental factors. Among humans, the intergenerational transmission of self-regulation is well established and is considered to be the result of both genes and environmental socialization (Bridgett et al., 2015). A meta-analysis showed a heritability estimate of 60% (Willems et al., 2019). Environmental socialization is also fundamental to self-regulation, of which parenting style is considered to be the most important (Tehrani & Yamini, 2020; Vazsonyi & Huang, 2010). Of course, as with other traits, an individual’s ability to self-regulate in particular situations is context-dependent, as highlighted by recent work on executing functioning (Munakata & Michaelson, 2021). The overall ability to self-regulate is thus the result of the interplay between genetic factors, acting via biological processes such as frontal lobe and stress system functioning, and the social environment (Blair & Raver, 2015; Bridgett et al., 2015).
The ability to self-regulate develops during youth. It increases during childhood, adolescence, and into early adulthood after which the variation within individuals decreases. This pattern seems to be evident across countries and cultures (Steinberg et al., 2018). Scholars believe that maturational changes in the functionality, structure, and connectivity of brain regions underlie these developmental changes (Casey et al., 2019). However, while mean-level changes in self-regulation occur into early adulthood, rank-order stability is thought to remain fairly stable from early childhood on (Bridgett et al., 2015). Thus, self-regulation during childhood may predict diverse outcomes later in life.
The ability to self-regulate is fundamental to success and well-being across multiple domains, including financial success, physical and mental well-being, and the avoidance of deviant behavior (Moffitt et al., 2011; Robson et al., 2020). Because self-regulation is the result of genetic and biological processes that are shaped by the social environment during development particularly during childhood (Blair & Raver, 2015; Bridgett et al., 2015), it may be that self-regulation measured during childhood is related to outcomes in multiple domains later in life. Indeed, the association between self-regulation and life outcomes, including socioeconomic indicators, criminal behavior, and mental and physical health, has been empirically established through meta-analyses. In one meta-analysis, self-regulation was associated with performance at school and work, eating and weight, interpersonal functioning, well-being and adjustment, addictive behavior, deviant behavior, and planning and decision-making (de Ridder et al., 2012). Another meta-analysis among children found that skills related to self-regulation were associated with academic achievement and performance as well as mental health problems, but not body mass index (Smithers et al., 2018). The most recent meta-analysis of self-regulation and functioning across multiple life outcomes investigated both cross-sectional and longitudinal associations (Robson et al., 2020). Cross-sectionally, self-regulation was associated with academic achievement, interpersonal behaviors (including peer victimization and aggressive behavior), mental health, and healthy living (including substance use and physical health). Most of the associations found were also evident when examining self-regulation during childhood and outcomes later in life, although the number of studies was fewer and the effect sizes smaller (Robson et al., 2020).
Further work on specific life outcomes provided more detail and nuance to these associations. For example, higher self-regulation seems to be robustly associated with multiple aspects of academic achievement and performance during youth, both cross-sectionally and longitudinally (Duckworth et al., 2019). Low self-regulation, on the other hand, is also considered to be a key component in criminal behavior (Burt, 2020). In a recent meta-analysis, results showed that the association between low self-regulation and violent behavior was stronger than for other types of deviance such as theft (Vazsonyi et al., 2017). Low self-regulation is also associated with mental health. It does not seem to be specific to certain disorders, but has rather been shown to be associated with psychopathology in general (Nigg, 2017), including substance use disorder (McClure & Bickel, 2014; Volkow et al., 2019). Self-regulation is furthermore associated with physical health, with higher self-regulation being related to healthy practices such as physical activity and healthier eating and sleep practices (Andrade & Hoyle, 2023). At the same time, low self-regulation is conceptualized as a critical factor underlying risk for disease (Hall et al., 2018) and has been modeled as a factor predicting earlier death (Strulik, 2019). Empirical work furthermore established a reciprocal association between low self-regulation and obesity (Lowe et al., 2019), which is a key determinant of disease and mortality later in life (Abdelaal et al., 2017). Thus, an extensive body of literature from different fields has established that self-regulation is associated with multiple life outcomes.
Although the bulk of the current understanding of self-regulation is drawn from cross-sectional studies, a substantial number of longitudinal cohort studies also exist. The majority of longitudinal studies had shorter follow-up periods during childhood or adolescence (see, for example, Robson et al., 2020), but there are studies that had longer follow-up periods, considering self-regulation in childhood in relation to outcomes in early to middle adulthood. For example, attention span-persistence (a measure of self-regulation) during preschool was associated with educational outcomes at age 25 (McClelland et al., 2013). In a smaller study, preschoolers with poorer delay of gratification (related to self-regulation) who consistently demonstrated low self-control as adults performed worse than preschoolers with a better day of gratification at an impulse-control task (alluring cues condition only) 40 years later (Casey et al., 2011). In a New Zealand complete birth cohort study, self-regulation during childhood predicted physical health, substance dependence, financial success, and criminal offending at 32 years (Moffitt et al., 2011) and the pace of aging and financial and social preparedness for old age at 45 years (Richmond-Rakerd et al., 2021). Similarly, research from a Finnish longitudinal study demonstrated that childhood self-regulation was related to psychological well-being at age 42 years among females (Pulkkinen et al., 2011) and that childhood cognitive skills and antisocial propensity (both related to self-regulation) were associated with severe economic disadvantage at age 50 years (Savolainen et al., 2017). Thus, childhood indicators of self-regulation seem to be associated with outcomes later in life.
The purpose of the current study was to investigate the association between self-regulation during childhood and outcomes later in life. We strove to include outcomes in line with previous studies (e.g., Robson et al., 2020) as much as possible given our data. We included the outcomes of low educational attainment, non-violent and violent criminal conviction, psychiatric diagnosis, and premature mortality at 58–66 years of age. While empirical studies have established these associations cross-sectionally as well as longitudinally (e.g., de Ridder et al., 2012; Robson et al., 2020), most longitudinal follow-up times have been shorter. To inform interventions, it is necessary to further investigate to what extent childhood self-regulation predicts outcomes later in life. While a few studies have examined these associations into middle adulthood, using self-reports (Moffitt et al., 2011; Richmond-Rakerd et al., 2021), to our knowledge, the current study is the first to investigate the associations between low self-regulation during childhood and diverse life outcomes in late adulthood and using administrative data. To do this, we utilized a sample of boys who were followed from childhood through late adulthood. Because there is evidence for some overlap between self-regulation and intelligence (Inzlicht et al., 2021) and socioeconomic status (Richmond-Rakerd et al., 2021) in predicting life outcomes, we controlled for these factors in our analysis as we were interested in the independent contribution of self-regulation. We hypothesized that low self-regulation during childhood would be associated with low educational attainment, and greater risk of non-violent and violent criminal behavior, psychiatric diagnosis, and premature mortality (i.e., death before the age of 65 years) at 58–66 years of age.
Method
Sample and Procedure
To test the association between childhood self-regulation and life outcomes, we used the Stockholm Life Course Project’s (SLCP) 1956 Clientele Study. The Clientele Study and its inclusion in the SLCP have been described elsewhere (Beckley et al., 2022; Swedish Government Official Reports (SOU 1971:49), 1971). Briefly, the Clientele Study was initiated in 1956 with the aim of investigating antecedents of juvenile crime. Members of the Clientele study included in the SLCP (N = 282; 98% of original Clientele Study members) comprised two groups of boys. The “delinquent” group (n = 187) was established through randomly drawn Stockholm police reports of crime committed between January 1959 and June 1963 by boys aged 15 years and younger (born 1943 to 1951). The Clientele Study “control” group (n = 95) consisted of young men who did not appear in the Stockholm Police reports and who matched roughly every other member of the delinquent group on demographic factors of age, parent socioeconomic status, and family type. The delinquent/control group distinction was not used in the present study. Previous studies in this sample have examined criminal career measures (Sivertsson & Carlsson, 2015) but not measures of self-regulation or other life outcomes.
Study members were initially assessed in 1961 about their behavior, activities, and attitudes. Interviews were conducted with study members and their parents and later coded by a research team which comprised child psychologists, sociologists, and medical professionals. Study members’ teachers were given questionnaires to assess study members’ behaviors and attitudes in school. In 2011, longitudinal data from Swedish population registers was gathered and added to the Clientele interview data. The unique nature of the data, a high-risk sample in which childhood interview information from multiple reporters was combined with a roughly 50-year follow-up to late adulthood, makes this sample ideal for studying how childhood factors may predict later life outcomes among individuals at risk for negative outcomes. The analytic sample size for the present study was limited to Clientele study members with data on all study variables from the date of the beginning of the study through their date of emigration, death, or 2009, the last year during which all study variables were available (N = 251).
Informed consent was given by the parents and teachers of participants during the first data collection wave. All data were anonymized and the study was approved by the regional ethical board in Stockholm (2010/79-31) and is in accordance with the 1964 Declaration of Helsinki and its later amendments.
Measures
Life Outcomes
Life outcomes consisted of low education, psychiatric diagnosis, conviction for non-violent crime, conviction for violent crime, and premature mortality. Low education was measured as educational attainment at or below the level of comprehensive school (grade 9) according to the Longitudinal integrated database for health insurance and labor market studies (LISA). In 1962, when study members were aged 11–19 years, schooling up to grade 9 became compulsory. National statistics indicate that in 2011 roughly 25% of males in Sweden aged 55–64 years had an education at or below grade 9 (Statistics Sweden, 2024). In contrast, 30% had an education beyond high school. In the analytic sample, all but 26 individuals had values on all other variables except low education. To fill in missing data on low education we used multiple imputation based on employment classification throughout the study members’ lives. This classification, developed by the Swedish Tax Authority, corresponds roughly to the level of education required for a job (Statistics Sweden, 2019). Employment classification was measured every 5 years 1965–1985 and annually 1990-2003. Psychiatric diagnosis was measured the first instance of receiving a psychiatric diagnosis (ICD Eighth [ICD-8; code 290–315], Ninth [ICD-9; code 290–319], and Tenth [ICD-10; code F00–F99] Revisions) in either Sweden’s inpatient hospital register (available since the 1960s) or outpatient care register (available since 2001). Both non-violent and violent criminal conviction were measured by an individual’s first appearance in archival criminal records before 1973 or, from 1973 onwards, the Conviction Register (also known as the Prosecution Register or Swedish Crime Register). Conviction for violent crime comprised conviction for crimes of homicide, assault, sexual assault, threat, and robbery. All other convictions were coded as non-violent. Nearly all study members who were convicted of violent crime also committed non-violent crime. However, a number of study members committed only non-violent crime. For both analyses, individuals convicted of a crime were compared to individuals who had not been convicted of the given type of crime. Premature mortality was registered as presence in the Cause of Death register. As all study members were 66 years of age or younger in the follow-up period, any registered death was considered to be premature (Mazzuco et al., 2021).
Self-Regulation
The measurement of self-regulation remains unstandardized, although it has been measured with a variety of contemporary instruments (Pilcher et al., 2022). These instruments capture, for example, lack of attention, lack of focus, lack of emotional control, impulsivity, volatile temper, low frustration tolerance, acting out, and more (Enkavi et al., 2019; Inzlicht et al., 2021; Nigg, 2017). Contemporary instruments used to measure self-regulation were unavailable when study members were initially assessed in the early 1960s. Nonetheless, the Clientele Study’s original investigators gathered measurements that are mirrored in contemporary operationalizations of self-regulation. We used contemporary operationalizations of self-regulation as a guide to select items from the initial assessment (see Supplementary Table S1). We then conducted an exploratory and subsequent confirmatory factor analysis and found five separate self-regulation factors (see Supplementary Table S1). The first factor, Teacher-rated carelessness, included measures of orderliness/carelessness, attention and concentration difficulties, fabrication/lying, and caution/destructiveness with objects as rated by teachers via a questionnaire. The second factor, Teacher-rated motor activity, included measures of impulsive aggression and motor activity as rated by teachers via a questionnaire. The third factor, Motor activity, included measures of overactivity and aggression as established during the parent interview and child assessment by a child psychologist. The fourth factor, Poor judgment, included a measure of judgment and a measure assessing remorse for/acceptance of hypothetical crime as rated by a child psychologist. The fifth factor, Immaturity, included social maturity—a measure of impulsivity, future outlook, and empathy—and immorality/amorality—a measure assessing the extent to which social norms may constrain behavior—both measured using the Adolescent Apperception Test (AAT). All self-regulation factors were mean centered and coded so that higher values indicated stronger presence of the factor (i.e., less self-regulation).
Covariates
We adjusted all models for intelligence (Inzlicht et al., 2021) and low parental socioeconomic status (Richmond-Rakerd et al., 2021) based on previous research. Individual intelligence was measured with the Terman-Merrill intelligence test during initial data collection. Population mean intelligence was 100 with a standard deviation of 15. Higher scores indicated higher intelligence. Low parental socioeconomic status was indicated by parents’ “social group,” a measure based on occupation used by Statistics Sweden until the early 1980s (Haldorson, 2016). The original three-level social groups were: (1) high-level civil servant, large-business owner, or professionals with an academic education; (2) low-level civil servant or small-business owner; and (3) worker in a private or public position, or unemployed. This measure was dichotomized so that those with parents in groups two or three were considered to have low parental socioeconomic status.
Statistical Analyses
We first conducted descriptive analysis of the data to understand the prevalence of life outcomes in the analytic sample. We plotted the prevalence of the outcomes over time using cumulative distribution function graphs. We analyzed the distribution of self-regulation factors using Kernel density plots. We tested for bivariate correlations between life outcomes as it was possible, and perhaps likely, for individuals to have more than one life outcome. We additionally tested for correlations between life outcomes and self-regulation factors as well as between self-regulation factors. Phi correlations with chi-square tests of statistical significance were used for binary-binary correlations; Pearson’s/point biserial correlations with t-tests were used for all other bivariate correlations. Finally, to answer our research questions, we tested whether self-regulation factors were associated with life outcomes using logistic regression modeling and Cox proportional hazard modeling. Logistic regression modeling was used for the outcome of low education, an outcome that does not constitute finality as education levels could increase at any point during life. For outcomes which indicated a state change (psychiatric diagnosis, criminal conviction, and premature mortality), we used Cox proportional hazard modeling. Participants were censored upon their first emigration, after which we could not determine whether an outcome occurred. 1 Across all models, we tested crude associations between each dimension of self-regulation, separately, and life outcomes (see Supplemental Material). Then we adjusted the analyses for intelligence and low parental socioeconomic status. Associations between the five self-regulation factors and each outcome were Bonferroni corrected (i.e., each analysis was corrected for testing self-regulation five times). R (R Development Core Team, 2019) was used for all analyses.
Results
Descriptive results (Table 1) showed that non-violent conviction was the most prevalent among life outcomes, with over half of the sample having been convicted of a non-violent crime. The least prevalent among life outcomes was violent conviction, with 15% of the sample having been convicted of a violent crime. Figure 1 shows the cumulative distribution function of each outcome. It was not possible to plot educational attainment due to too much missing data. The self-regulation factors of teacher-rated carelessness, teacher-rated motor activity, and immaturity had a similar, normal-type distribution. Motor activity had a right skew, whereas judgment had a strong mode (see Table 1).
Descriptive Statistics for Study Measures.
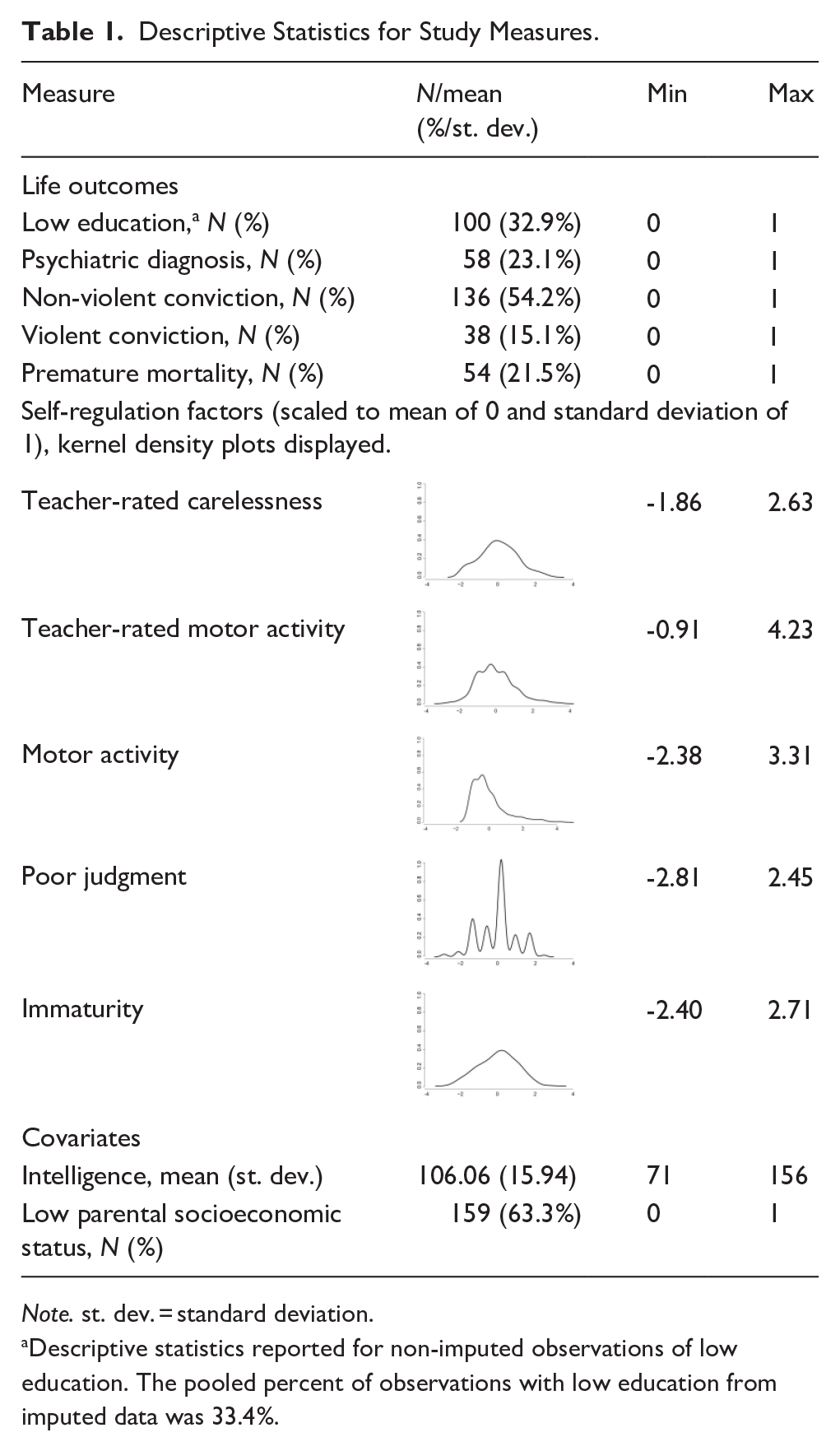
Note. st. dev. = standard deviation.
Descriptive statistics reported for non-imputed observations of low education. The pooled percent of observations with low education from imputed data was 33.4%.
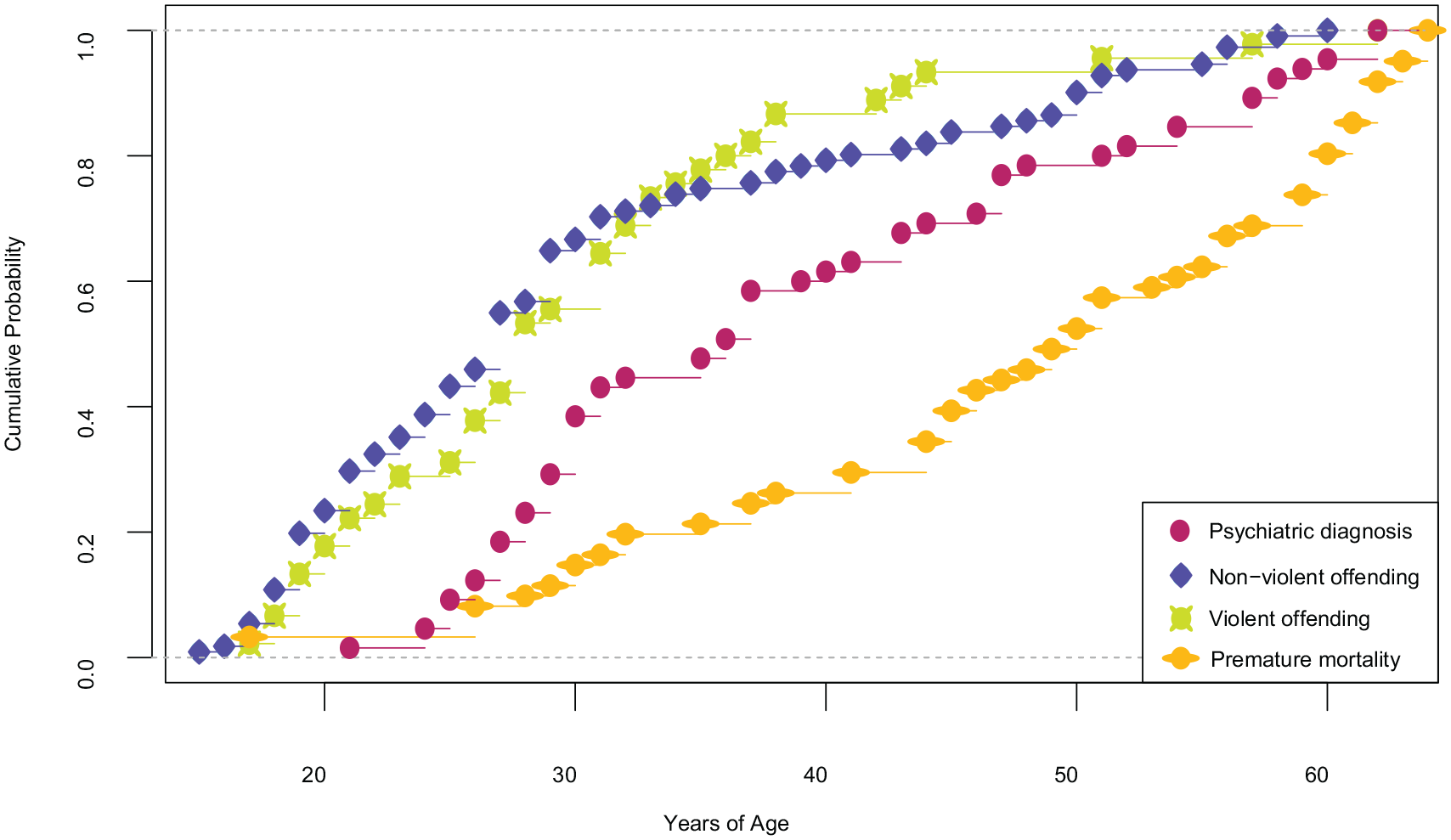
Cumulative Distribution Functions of Outcomes. This figure displays the cumulative distribution functions of outcomes across age. The cumulative probabilities are based on the total number of observed events: psychiatric diagnosis (n = 58), non-violent offending (n = 136), violent offending (n = 38), and premature mortality (n = 54).
We observed significant correlations between all life outcomes, with the exception of low education (see Supplementary Table S2). Likewise, nearly all self-regulation factors, except teacher-rated motor activity and immaturity, were significantly correlated with one another. Roughly half of the correlations between self-regulation factors and life outcomes reached the threshold of statistical significance, indicating some support for the hypothesis that low self-regulation was associated with increased odds of the analyzed life outcomes.
Statistical models which adjusted for intelligence and low parental socioeconomic status maintained modest support of the hypothesis that low self-regulation increased the risk of the various life outcomes (Figure 2).
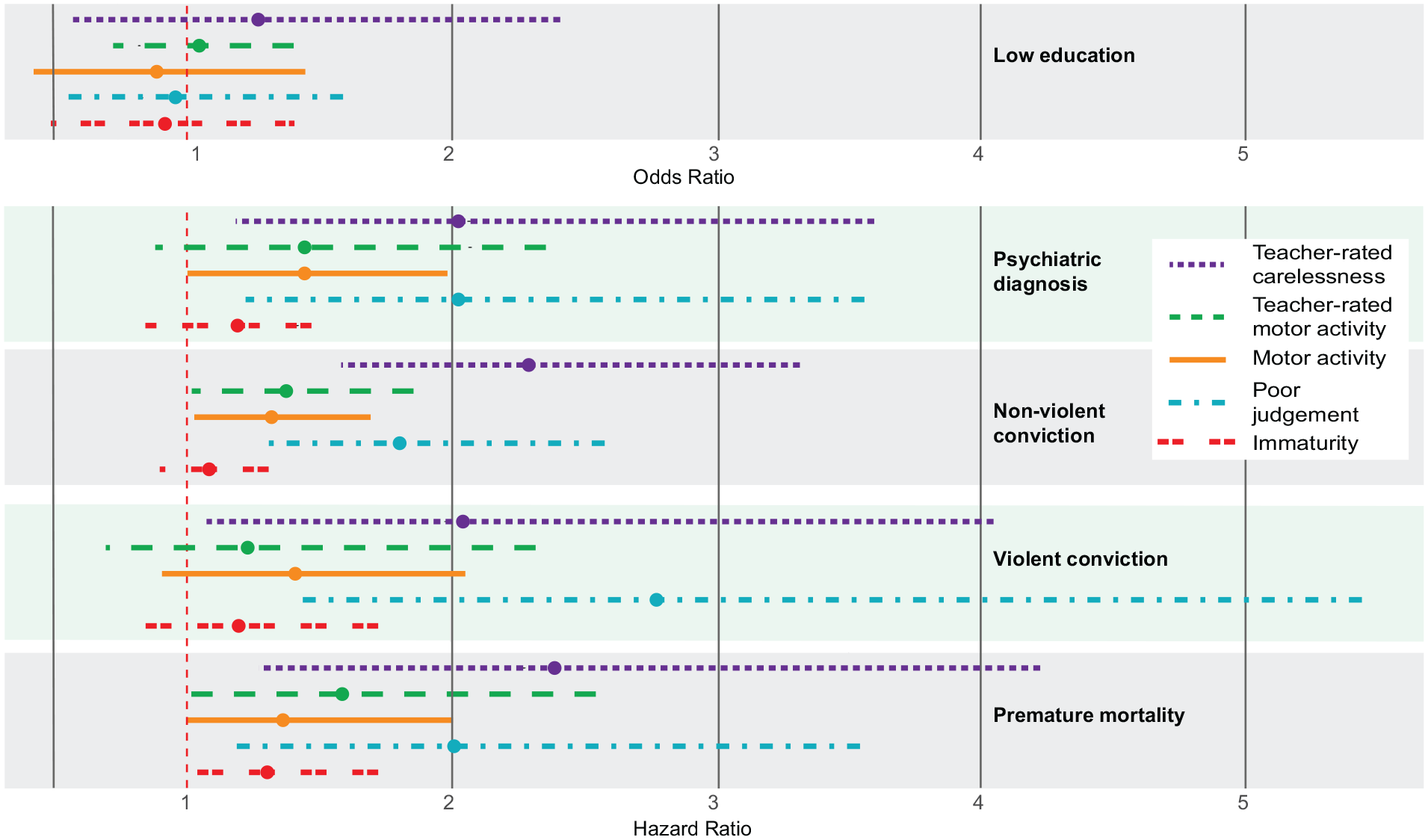
Self-Regulation Factors’ Association With Life Outcomes. This figure displays the associations between self-regulation factors and life outcomes. Points represent results from logistic regression (odds ratios) and Cox proportional hazards models (hazard ratios), respectively (n = 251 for all models; see Supplemental Material, Tables S3–S7, for full results). Horizontal lines indicate Bonferroni-corrected 95% confidence intervals for the hazard ratios. All models are adjusted for IQ and low parental socioeconomic status.
Low Education
None of the self-regulation factors had significant associations with low education. Moreover, some of the estimates indicated that lower self-regulation, relative to higher self-regulation, was associated with a decreased risk of low educational attainment (see Supplementary Table S3).
Psychiatric Diagnosis
Lower self-regulation was associated with an increased risk of psychiatric diagnosis. These associations were significant across two of the five self-regulation factors (teacher-rated carelessness: hazard ratio [HR], 2.02; 95% Bonferroni-corrected confidence interval [CI], 1.16–3.52 and poor judgment: HR, 2.09, 95% CI, 1.22–3.59; see Supplementary Table S4).
Non-Violent Conviction
Lower self-regulation was associated with an increased risk of non-violent conviction. These associations were significant across four of the five self-regulation factors (teacher-rated carelessness: HR, 2.19; 95% CI, 1.52–3.18; teacher-rated motor activity: HR, 1.40; 95% CI, 1.04–1.89; motor activity: HR, 1.32; 95% CI, 1.04–1.67; and poor judgment: HR, 1.83; 95% CI, 1.28–2.63; see Supplementary Table S5).
Violent Conviction
Lower self-regulation was associated with an increased risk of violent conviction. These associations were significant across two of the five self-regulation factors (teacher-rated carelessness: HR, 2.03; 95% CI, 1.04–3.98; and poor judgment: HR, 2.84; 95% CI, 1.45–5.57; see Supplementary Table S6).
Premature Mortality
Lower self-regulation was associated with an increased risk of premature mortality. These associations were significant across two of the five self-regulation factors (teacher-rated carelessness: HR, 2.33; 95% CI, 1.30–4.21 and poor judgment: HR, 1.99, 95% CI, 1.13–3.49; see Supplementary Table S7).
Discussion
The aim of this study was to examine the association between self-regulation in childhood and life outcomes up to approximately 50 years later, at 58–66 years of age. Previous research established associations between self-regulation and various life outcomes, although not yet with a follow-up period reaching into late adulthood, nor using administrative data. Our results showed that lower self-regulation during childhood was associated with a higher likelihood of receiving a psychiatric diagnosis, of being convicted of a non-violent as well as a violent crime, and of premature mortality later in life. Self-regulation was not associated with low education. As in earlier studies, these models were adjusted for intelligence and low parental socioeconomic status. Our findings are largely consistent with an extensive body of literature on the association between self-regulation and life outcomes in various domains. Our results extend previous work by including a longer follow-up period and by using objective, administrative data to index the outcomes.
The Association Between Self-Regulation During Childhood and Outcomes Later in Life
Self-regulation is considered a core concept related to human health and behavior across multiple fields, including psychology, neuroscience, economics, and criminology. Decades of research, including several large-scale meta-analyses, firmly established that self-regulation was associated with outcomes in multiple domains, including socioeconomic indicators, criminal behavior, and mental and physical health (e.g., de Ridder et al., 2012; Robson et al., 2020; Smithers et al., 2018). These associations seem to hold longitudinally as well as cross-sectionally (e.g., Robson et al., 2020). Our findings are largely in line with this previous work. First, we observed that lower self-regulation during childhood was associated with an increased risk of psychiatric diagnosis later in life. This is consistent with a large body of literature on the association between self-regulation and psychopathology (Nigg, 2017). Second, we found that lower self-regulation was associated with an increased risk of being convicted of a non-violent and violent crime. While most previous studies on self-regulation and crime focused on any crime (Burt, 2020; Pratt & Cullen, 2000), we investigated risk for non-violent and violent crime separately given findings from the most recent meta-analysis that the association between self-regulation and violent behavior was stronger than for other types of deviant behavior (Vazsonyi et al., 2017). Finally, our results showed that lower self-regulation was associated with an increased risk of premature mortality. Self-regulation during childhood has not yet been studied in direct relation to premature mortality to our knowledge, although it has been modeled as a factor predicting earlier death (Strulik, 2019). In addition, an extensive body of work established associations between self-regulation and factors known to be related to premature mortality such as health-related behaviors and obesity (Andrade & Hoyle, 2023; Lowe et al., 2019).
In the current study, we failed to observe an association between self-regulation and low education, which is inconsistent with previous work and our hypotheses. Previous research reported robust associations between higher self-regulation and various aspects of academic achievement and performance (e.g., Duckworth et al., 2019; Smithers et al., 2018). That our study was not in line with this work may be unsurprising considering that we used a fairly low threshold for “low” education: failure to complete comprehensive schooling up to grade 9 (when most children are aged 15–16 years). This level of schooling became compulsory by law in Sweden in 1962 when participants in the study were aged 11–19 years. Assessing educational attainment between grades 9 and university is, however, difficult in Sweden given that there is no clear equivalent to the completion of high school, a commonly used threshold for dichotomous measures of educational attainment. Our results tentatively suggest low self-regulation may not be predictive of especially low levels of educational attainment in Sweden during the middle of the 20th century. Instead, it is likely that intelligence and perhaps intellectual disability play a larger role at this threshold of educational attainment, a notion also supported by our results (see Supplementary Table S3).
Measurement of Self-Regulation
We constructed a measure of self-regulation for the purpose of this study (see Supplementary Table S1). A wide range of instruments, both task- and report-based, have been used to measure self-regulation in contemporary research (see Pilcher et al., 2022). It was not possible to use well-established or validated instruments in our study since these were unavailable in the early 1960s when the data collection took place. Instead, we used current research on established components of self-regulation to guide which items we extracted from the interview, survey and assessment data that were available in our dataset. Research on self-regulation has established multiple components, including lack of attention, lack of focus, lack of emotional control, impulsivity, volatile temper, low frustration tolerance, acting out, and more (Enkavi et al., 2019; Inzlicht et al., 2021; Nigg, 2017). The items we extracted from the data were subjected to factor analysis to derive meaningful dimensions for our study (see Supplementary Table S1). Thus, although we could not operationalize self-regulation based on a validated instrument, the items we extracted as indicators of self-regulation were guided by the current understanding of self-regulation and its components.
The Clientele Study Sample
The findings from our study are based on a unique sample of boys followed from late childhood through late adulthood when the study members were 58–66 years old. Study members were followed for substantially longer than most longitudinal research on self-regulation and life outcomes (e.g., Robson et al., 2020). A few important longitudinal cohort studies have been conducted following participants up to 40 or 50 years of age (e.g., Richmond-Rakerd et al., 2021; Savolainen et al., 2017). Cumulative distribution function graphs of our outcomes demonstrated that following individuals beyond 50 years of age allowed us to capture an additional 5% of the total sample of individuals who committed crimes, an additional 20% of those who received a psychiatric diagnosis, and an additional 40% of those who died prematurely. Thus, our work shows that extending the follow-up time into late adulthood clearly contributes to our understanding of the extent to which self-regulation in childhood is associated with outcomes later in life.
Previous work on the association between self-regulation in childhood and outcomes into middle adulthood mainly utilized self-reported outcomes (e.g., Richmond-Rakerd et al., 2021; Savolainen et al., 2017). Self-reports allow for the assessment of detailed and comprehensive outcomes, but they are also subjective and may be influenced by recall bias, non-random attrition and infrequent follow-ups. In our study, we followed the Clientele study sample using administrative data from Swedish national registries. In doing so, we obtained objectively assessed outcomes which were continuously tracked across the lifespan of the participants. Such objectively assessed outcomes can be seen as complementary to self-reported assessments used in previous work.
The Clientele Study is unique because around two-thirds of study members had been registered by the police as involved in delinquency before 15 years of age. Comparisons to the Stockholm Birth Cohort (SBC), a study of all individuals born in 1953 and living in the greater metropolitan area of Stockholm in 1963 whose latest follow-up is to age 64 years (Almquist et al., 2020), indicate that the present sample was a high-risk sample. Of the current study members, 69% had been convicted of a non-violent or violent crime by late adulthood, whereas 48% of all males in the SBC were convicted of a crime (Carlsson & Sivertsson, 2021). The boys in the current study were also at a theoretically higher risk of mental health and premature mortality based on evidence demonstrating associations between those outcomes and crime (Beaudry et al., 2021; Hodgins et al., 2024; Siponen et al., 2023). Indeed, 23% of current study members had a psychiatric diagnosis relative to roughly 7% of males and females in the SBC (Almquist et al., 2020). However, contrasts in premature death were not as stark. In the present study, 22% of study members died before 66 years of age, relative to 19% of males followed to age 64 years in the SBC (Carlsson & Sivertsson, 2021). High-risk samples are advantageous for tests of lower-frequency outcomes such as criminal conviction, psychiatric diagnosis, and premature mortality. In addition, gathering data from a small, high-risk sample enables more extensive data collection. The current sample, for example, includes interviews, questionnaires, and psychological tests gathered from study members themselves, their parents, teachers, and psychiatrists. High-risk samples, however, are not suitable for establishing general population estimates, as they are likely to show stronger associations between risk factors and outcomes than would be found in the general population. Nonetheless, it is often the high-risk groups for which interventions are typically built and greater understanding of this group remains important.
Our sample consisted of males only and therefore the results almost certainly are not generalizable to females. Studies have shown that measures of self-regulation may be expressed differently among females compared to males in a way that the multiple dimensions from this study would possibly not be found among females or the dimensions would comprise different measures (Longshore et al., 1996). Previous work is inconclusive regarding potential sex differences in the associations between self-regulation and life outcomes. For example, whereas one meta-analysis reported that the association between trait self-regulation and undesirable behaviors was stronger for males (de Ridder et al., 2012), another meta-analysis reported that the association between self-regulation and deviant behavior was weaker in studies with a higher proportion of males (Vazsonyi et al., 2017). Other meta-analyses reported no moderation by sex in the association between self-regulation and criminal behavior (Pratt & Cullen, 2000) or life outcomes in multiple domains (Robson et al., 2020). One longitudinal cohort study reported that the association between childhood self-regulation and psychological well-being during adulthood was only observed among females, and not males (Pulkkinen et al., 2011). Potential sex differences may vary by outcome, and more research is needed. However, research prior to our own seems to indicate minimal evidence for sex differences in the associations between self-regulation and outcomes in multiple domains. Nonetheless, our findings should only be interpreted regarding males.
Our sample included only ethnic Swedes and therefore the results are likely not generalizable to racial and ethnic minorities. International research indicates clear racial or ethnic disparities in educational attainment (Cohen et al., 2022), arrest rates (Barnes et al., 2015), mental health (Alvarez et al., 2019), and premature mortality (Best et al., 2018). Part of this, of course, may be due to factors such as racial discrimination or access to health care. Thus, the patterning of these life outcomes among racial and ethnic minorities is important for future research.
Implications for Practice and Future Research
That self-regulation measured during childhood is predictive of outcomes into late adulthood has implications for interventions targeting health and behavior. It suggests, in line with a bulk of other research, that self-regulation is central to well-being. This does not mean that self-regulation is static and unchangeable. Rather, research indicates that the ability to self-regulate develops during youth and into early adulthood (Piquero & Rocque, 2020; Steinberg et al., 2018). Consequently, interventions that target self-regulation during later childhood and adolescence may be effective in promoting healthy behaviors and well-being. Indeed, there is substantial evidence for the effectiveness of programs that aim to improve self-regulation among youth (Friese et al., 2017; Piquero et al., 2016; Smith et al., 2019).
Further research is needed to determine how self-regulation in childhood may be associated with outcomes into late adulthood. Longitudinal cohort studies showed, for example, that the association between childhood self-regulation and outcomes in adulthood was mediated by crime and deviance as well as socioeconomic conditions (Savolainen et al., 2017), and by social network (Pulkkinen et al., 2011) in early adulthood. Although the sample size was small in these studies, they point to key directions for future research in determining pathways to health and behavioral outcomes in later life. Another avenue for further work would be to investigate the association between childhood self-regulation and future outcomes with more specificity. For example, a more detailed understanding of the extent to which self-regulation is associated with timing of psychiatric diagnosis or criminal conviction would be valuable. We emphasize here the necessity of larger samples in order to investigate these questions.
Limitations
There are some limitations of this study. First, due to the small sample size, we included a single measure of any psychiatric diagnosis rather than separate types of psychiatric diagnoses. However, research has indicated that low self-regulation is associated with psychological well-being or psychopathology in general, rather than with specific disorders (Nigg, 2017; Pulkkinen et al., 2011). Second, our measure of socioeconomic status was crude as it was based on a dichotomous measure of parents’ “social group.” Unfortunately, it was the only measure of socioeconomic status available in our data. Finally, there is some indication that our study was under-powered to detect small effects. We performed a post hoc power analysis in G*Power (Faul et al., 2009), which indicated that, with our final sample size of N = 251, our study had sufficient power to detect effects with odds ratios of 1.75 and higher. A larger sample size would have been necessary to detect smaller effects with greater certainty.
Conclusion
In conclusion, we investigated the association between self-regulation during childhood and life outcomes up to 50 years later in a sample of boys. Approximately two-thirds of the boys in the sample had been registered by the police as involved in delinquency before 15 years of age. We observed that lower self-regulation during childhood was associated with a higher risk of psychiatric diagnosis, conviction for non-violent and violent crime and premature death later in life. Self-regulation was not associated with low education. Our study confirms earlier studies on the link between self-regulation and life outcomes and extends this by including a follow-up period into late adulthood and by utilizing objective, administrative data. Keeping in consideration the small sample of males only and the assessment of self-regulation based on data collected in the 1960s, our study supports the notion that self-regulation is integral to human well-being across the lifespan.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254251358185 – Supplemental material for Childhood self-regulation and life outcomes in a 50-year follow-up study
Supplemental material, sj-docx-1-jbd-10.1177_01650254251358185 for Childhood self-regulation and life outcomes in a 50-year follow-up study by Brittany Erlissa Evans, Joakim Berglund, Jerzy Sarnecki and Amber L. Beckley in International Journal of Behavioral Development
Footnotes
Acknowledgements
We would like to sincerely thank Michael Rocque for his helpful comments on this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from Riksbankens Jubileumsfond (P18-0639:1) and Örebro University Research Infrastructure (ORU 1.3.1-01548/2018).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.