
Abstract
Children prenatally exposed to opioids exhibit impairments in cognitive functioning and have an increased likelihood of experiencing other forms of adversity. Given that these other forms of early life adversity are linked to lower levels of cognitive functioning, it is important to determine whether the association between opioid exposure and cognitive functioning is better explained by other forms of adversity. The current study used a practical design (i.e., caregiver report of a preschool-aged child’s exposure to opioids during gestation) to examine the associations between prenatal opioid exposure status (i.e., presence or absence of exposure), postnatal adversity, and preschool-age cognitive functioning. Forty-four preschool-age children, 21 with prenatal opioid exposure (20 of whom were adopted) and 23 comparison children, and their caregivers were invited to a laboratory session during which the child completed a neuropsychological assessment battery while caregivers were interviewed about their child and completed questionnaires. Regression analysis was conducted to examine whether prenatal opioid exposure status explained variation in cognitive functioning over and above child adversity. Children with prenatal opioid exposure had lower full-scale IQ scores than comparison children (Cohen’s d =−0.86). After accounting for exposure to postnatal adversity, prenatal opioid exposure status explained 6.01% of the variance in full-scale IQ scores. Taken together, our results suggest that the association between prenatal opioid exposure status and cognitive functioning at preschool age is not better explained by postnatal adversity. These findings underscore efforts to reduce opioid use among people who are pregnant or likely to become pregnant.
The opioid epidemic is a major public health crisis (Lyden & Binswanger, 2019). In addition to those who directly use, opioids have the potential to influence fetal development when used during pregnancy (Beckwith & Burke, 2015). Opioid use during pregnancy is increasing, as the number of women with opioid-related diagnoses documented at delivery increased by 131% from 2010 to 2017, and the number of infants born with neonatal opioid withdrawal syndrome increased by 82% nationally from 2010 to 2017 (Hirai et al., 2021). In fact, every 15 minutes an infant is born in the United States with neonatal opioid withdrawal syndrome (Jenkins et al., 2021).
Although little is known about longer-term outcomes for children with opioid exposure during gestation, there is some evidence that these children are at increased risk for impairments. Recent mixed methods and community-initiated analysis examining developmental outcomes among 148 school-age children prenatally exposed to opioids found that nearly half of the children in the sample were diagnosed with multiple developmental delays and specific learning disorders (Wilkinson et al., 2023). Another study found that children aged 3–8 years who were born with prenatal opioid exposure, relative to comparison children matched by sex, race and/or ethnicity, socioeconomic status, age, and region of residence at birth, are more likely to meet criteria for disability (15.6% vs. 11.7%) and receive classroom therapies or services (15.3% vs. 11.4%) (Nygaard et al., 2015). These challenges may be, at least in part, driven by differences in cognitive performance. Specifically, examination of full-scale IQ scores among children with and without prenatal opioid exposure revealed lower scores among the exposed group, which grew from a mean difference of 6.5 (0.43 SD) (95% CI [2.2, 10.8]) at age 1 year to a mean difference of 18.3 (1.22 SD) (95% CI [12.3, 24.2]) at age 8.5 years—a difference that is more than one standard deviation (i.e., 15 points) (Nygaard et al., 2015). These findings suggest that children exposed to opioids prenatally may exhibit lower levels of cognitive functioning compared to non-exposed children, with those differences increasing across development.
Examining potential outcomes related to opioid use can benefit from a lens provided by the systems model. A systems model emphasizes the complex and interconnected associations between parental opioid use, social determinants of health, social supports, and potential negative impacts on children’s physical and mental health as well as risk for future substance misuse (Smith et al., 2021). Several biological and socio-environmental risk factors, ranging from neurodevelopment to postnatal environment could either exacerbate risk or buffer children from the negative effects of opioid exposure (Lee, Bora, et al., 2020). For example, a study examining associations between mother–child interactions on children’s cognitive development in a group of children prenatally exposed to opioids and a non-exposed comparison group found that the exposed group scored significantly lower on measures of cognitive development and that scores were associated with both group status and mother–child interaction (Konijnenberg et al., 2016). Further, adverse experiences tend to be co-occur (i.e., children who experience one form of adversity are at increased likelihood of experiencing others) (Dong et al., 2004). This is also true for prenatal opioid exposure, as individuals who are prenatally exposed to opioids are more likely to experience poverty, caregiver psychopathology, and disruptions in family care, relative to those non-exposed (Conradt et al., 2018). Given that these other types of early life adversity are linked to lower levels of cognitive functioning (Johnson et al., 2021), postnatal adversity may be an intervening factor to consider when examining the association between prenatal opioid exposure and cognitive functioning (Conradt et al., 2018). Therefore, it is important to determine whether the association between prenatal opioid exposure and cognitive functioning is better explained by exposure to other types of adversity. While some studies indicate that the associations between prenatal opioid exposure and negative developmental outcomes persist when covarying for adverse childhood experiences (Wilkinson et al., 2023), others find that prenatal opioid exposure is no longer associated with cognitive outcomes in childhood after covarying for these associated stressors (Hans & Jeremy, 2001) and demographic factors (Konijnenberg & Melinder, 2015). These findings underscore the importance of examining potential psychosocial correlates that may better account for the association between prenatal opioid exposure and cognitive functioning, which in turn has implications for identifying timing and targets for intervention.
The current study sought to examine the association between prenatal opioid exposure status (i.e., whether or not children were prenatally exposed to opioids per caregiver report) and preschool-age cognitive functioning—a developmental period when cognitive difficulties can be reliably identified (Keenan & Wakschlag, 2000). To do this, we used a practical design (i.e., caregiver report of a preschool-aged child’s exposure [yes/no] to opioids during gestation) for two reasons: (1) early childhood professionals and school personnel who work with preschool-age children have few details about specific aspects of the method, frequency, timing, and potency of opioid use, as well as co-occurring use of other substances and (2) caregiver report of use is a parsimonious approach for use in determining potential needs for allocation of resources and support services to groups of qualifying children. Schools, health care providers, and social services can use this information to tailor their approaches to meet the specific needs of children who have been prenatally exposed to opioids. Further, we explored whether the association persisted over and above the potential effects of postnatal adversity. Given prior literature, we had two competing hypotheses. One hypothesis was that prenatal opioid exposure status would be associated with lower general cognitive functioning (i.e., full-scale IQ scores), even with minimal postnatal risk (Nygaard et al., 2015) or covarying for adversity (Wilkinson et al., 2023). Alternatively, and in concert with past work (Hans & Jeremy, 2001), the second hypothesis was that variations in stress during the postnatal environment may better explain differences in full-scale IQ scores associated with prenatal opioid exposure status and that after accounting for stressful experiences there would be no significant association between prenatal opioid exposure status and cognitive functioning.
Method
Participants
Forty-four caregiver–child dyads were recruited for this study (21 children with prenatal opioid exposure and 23 healthy comparisons; see Table 1 for participant demographics) via social media advertisements on Facebook and Instagram, flyers and brochures posted in physician offices, as well as via distribution of flyers to providers of early intervention services (e.g., Tennessee Early Intervention Services). All study procedures were approved by the Vanderbilt University Institutional Review Board (IRB #192231). Those interested in hearing more about the study filled out an online interest form via REDCap (a secure, web-based software platform designed to support data capture for research studies) (Harris et al., 2009, 2019) and were contacted via phone to provide a detailed description of the study as well as to conduct a phone screen to confirm eligibility. Prenatal opioid exposure was determined based on caregiver report on the eligibility phone screen. The primary caregiver was required to be at least 18 years of age, a parent or legal guardian of the child, and able to read and speak English fluently. Exclusion criteria were caregiver report of child history of neurological injury, impairment, or disability, as well as caregiver endorsement of a severe learning disability that would interfere with the completion of study tasks. Four participants (two in the exposed group and two in the comparison group) opted to participate only in the online components of the study (i.e., questionnaire measures and interview) and four other participants (three in the exposed group and one in the comparison group) did not complete the online questionnaire measures (see “Statistical Analyses” section for the sample size for each analysis). The comparison group (i.e., children without a history of prenatal opioid exposure) did not statistically differ from the exposed group on child sex, child age, child race, child ethnicity, highest level of caregiver education, and income-to-needs ratio (see Table 1). Of the 21 participants with a history of prenatal opioid exposure, 20 participants were adopted; none of the comparison children were adopted. Because of this, children in the exposed group were much more likely to be adopted than children in the comparison group (χ2 = 40.16, p < .001). Children were placed into their current home at a mean age of 5.32 months (SD = 10.97, range 0–36 months). The age of placement was not statistically significantly correlated with child adversity (p = .497) or cognitive functioning (p = .836). Further, given that children adopted in Tennessee are eligible for TennCare (Medicaid program in the state of Tennessee), our analyses indicated that children in the exposed group (most of whom were adopted) were more likely to receive TennCare than comparison children (χ2 = 23.24, p < .001).
Participant Demographics for Opioid Exposure and Comparison Groups.
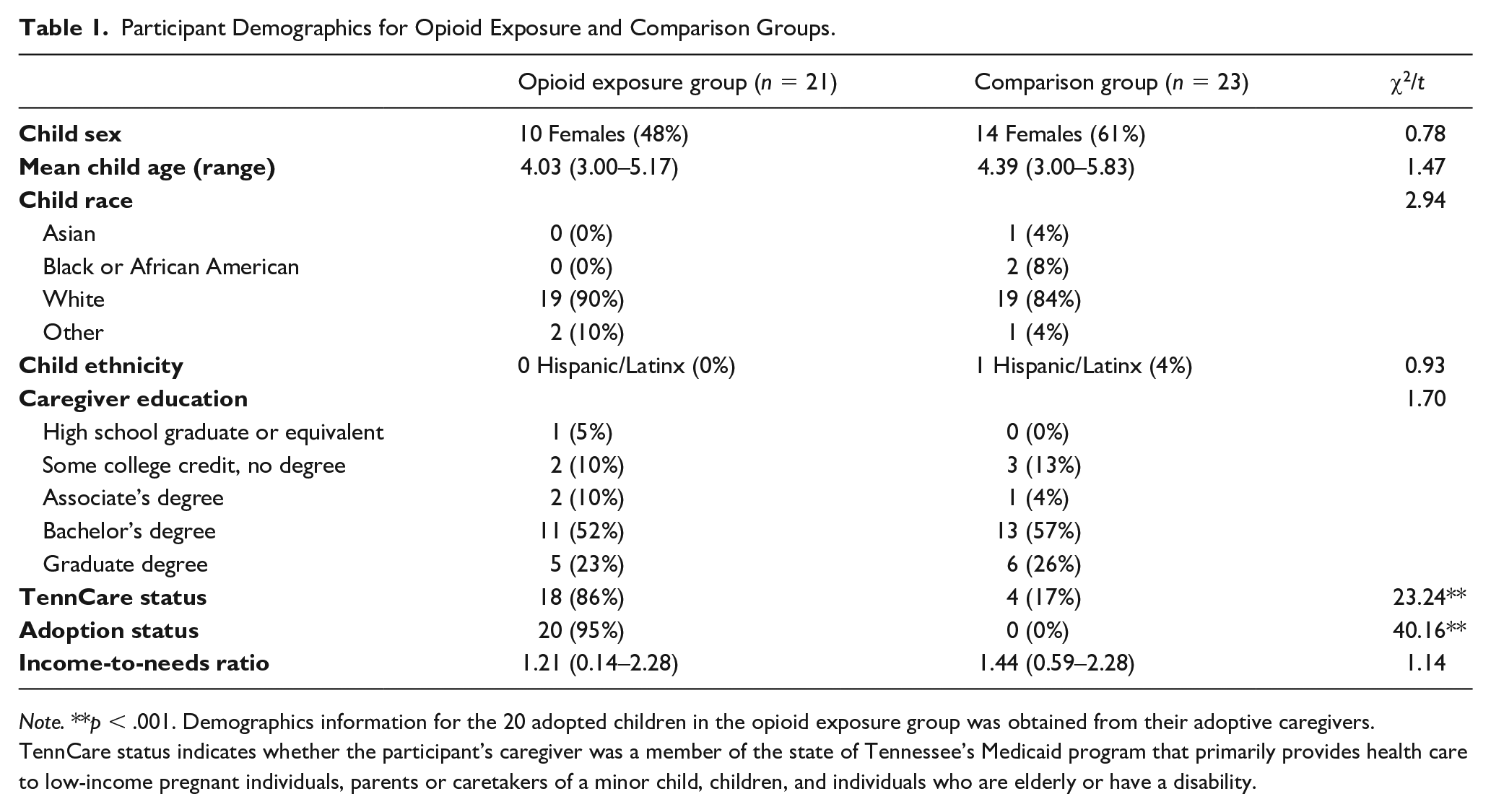
Note. **p < .001. Demographics information for the 20 adopted children in the opioid exposure group was obtained from their adoptive caregivers. TennCare status indicates whether the participant’s caregiver was a member of the state of Tennessee’s Medicaid program that primarily provides health care to low-income pregnant individuals, parents or caretakers of a minor child, children, and individuals who are elderly or have a disability.
Procedures
Caregiver–child dyads were invited to a laboratory session during which informed consent and child assent were obtained. Caregivers (including adoptive parents) completed an interview about their child’s birth history, medical and developmental history, and their child’s social and emotional behavior. Caregivers also completed questionnaires online on REDCap while their child completed an assessment battery that included standardized neuropsychological measures. Dyads were compensated with $50 for their participation in the study.
Measures
Child Adversity
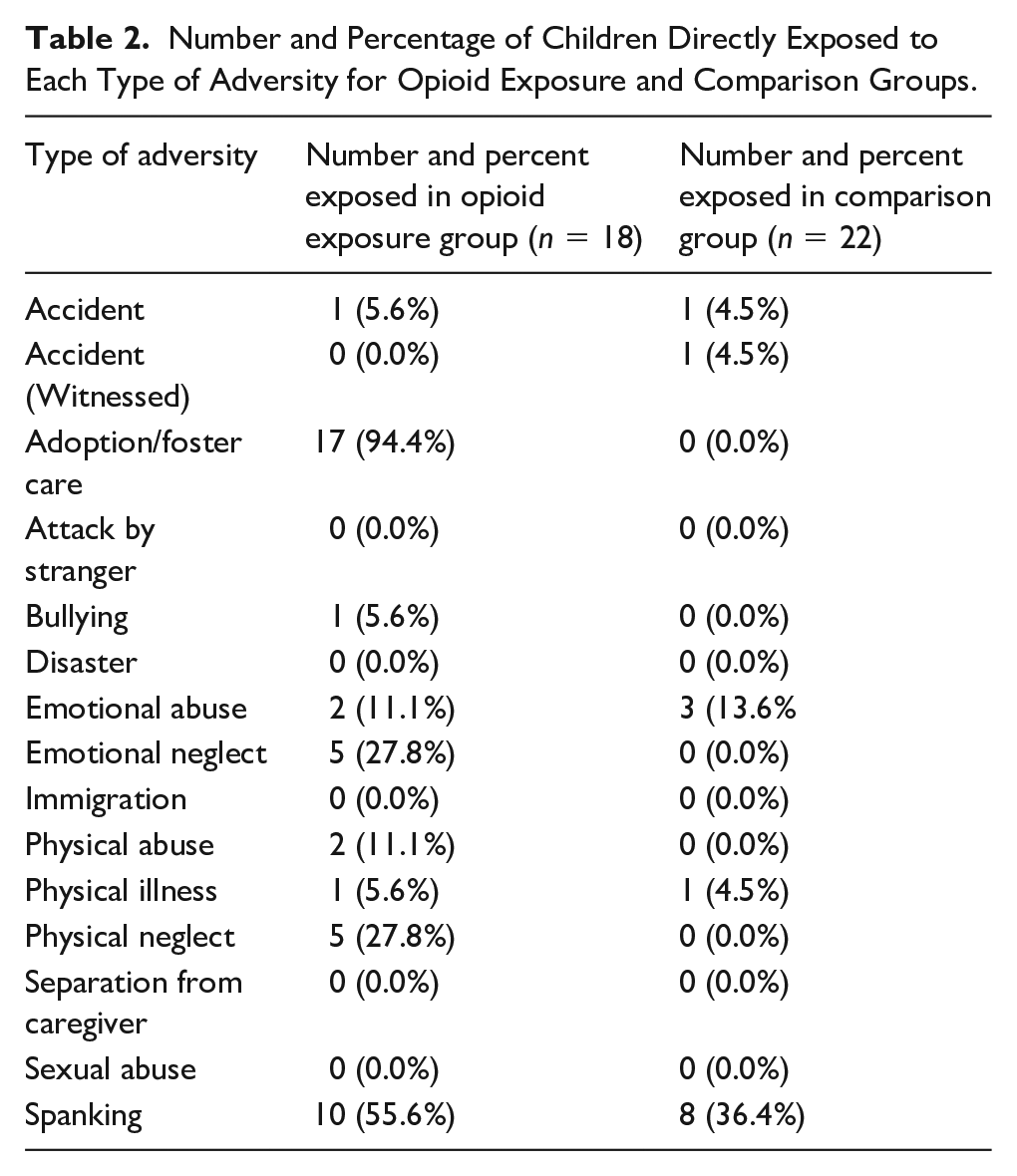
Child’s exposure to stress was assessed using the Assessment of Parent and Child Adversity questionnaire (APCA) (King et al., 2023). For the current study, we focused on the APCA’s assessment of child exposure to 15 types of direct adversity (i.e., accident, witnessed accident in the absence of caregiver, adoption, attack by stranger, bully, disaster, emotional abuse, emotional neglect, immigration, physical abuse, physical neglect, separation from caregiver, sexual abuse, and spanking). Caregivers completed the questionnaire indicating the types of adversity their child was directly exposed to. Nearly all children in the exposed group have been adopted, and at an early age (the average age of adoption/foster care was 5.32 months [SD = 10.97, range 0–36 months]). Adoptive caregivers were instructed to complete the assessment to their best knowledge (i.e., including exposures that they were informed of even if it was prior to the child’s placement with them). The parent-report measure has been validated in a sample of mothers and their 3- to 5-year-old children (King et al., 2023) and used in other studies with young children (Lynn et al., 2022). See Table 2 for a list of adversities assessed, and number and percentage of children exposed to each type for both the exposed and comparison groups. The most common stressor experienced by those in the opioid-exposed group was adoption, followed by spanking. Spanking was the most common stressor experienced by those in the comparison group.
Number and Percentage of Children Directly Exposed to Each Type of Adversity for Opioid Exposure and Comparison Groups.
Child Cognitive Functioning
The Wechsler Preschool and Primary Scale of Intelligence—Fourth Edition (WPPSI-IV) (Wechsler, 2012), a norm-referenced battery of cognitive functioning for children aged 2 years 6 months to 7 years, 7 months (2:6–7:7), was administered by trained research staff, under the supervision of a licensed clinical psychologist, to assess participants’ cognitive functioning. Known to demonstrate strong psychometric properties (Syeda & Climie, 2014), the WPPSI-IV comprises two batteries of subtests, one for children from ages 2 years, 6 months to 3 years, 11 months (2:6–3:11) and one for children aged 4 years, 0 months to 7 years, 7 months (4:0–7:7). The battery of subtests for the younger age group (3:0–3:11) included the six core subtests (Block Design, Picture Memory, Information, Object Assembly, Zoo Location, and Picture Naming) designed to assess general cognitive functioning (full-scale IQ) and three subdomains: the Verbal Comprehension Index, Visual Spatial Index, and the Working Memory Index. The battery of subtests for the older age group (4:0–5:11) included the 11 core subtests (the subtests mentioned above and Bug Search, Cancelation, Matrix Reasoning, Similarities, and Picture Concepts) designed to assess full-scale IQ as well as five subdomains: the Verbal Comprehension Index, Visual Spatial Index, Working memory Index, Fluid Reasoning Index, and the Processing Speed Index.
Statistical Analyses
Both child age and sex were considered as potential covariates, and neither was associated with either full-scale IQ or child adversity and thus were not included in the final models. For our primary analyses, we examined whether children with and without prenatal opioid exposure differed in their estimated full-scale IQ scores using independent samples t-test. Given the small sample size and that we expect prenatal opioid exposure to only be negatively associated with cognitive functioning, we used a one-tailed independent samples t-test (N = 40; 19 in the exposed group and 21 in the comparison group). Second, to test whether groups differed in experiences of adversity, we used a Mann–Whitney U test, a nonparametric test appropriate for count data (N = 40; 18 in the exposed group and 22 in the comparison group). Given that nearly all (95%) of the participants in the prenatal opioid exposure group were adopted, we found this variable to be largely redundant with exposure status. Thus, we removed adoption from the list of 15 forms of adversity for subsequent analyses. As such, analyses including both prenatal opioid exposure status and child adversity used this revised count of adversity. Third, we used ordinary least squares hierarchical regression analysis to examine whether prenatal opioid exposure status explained variation in full-scale IQ scores over and above child adversity (N = 36; 16 in the exposed group and 20 in the comparison group). This order of entry allowed for the examination of the contribution of prenatal opioid exposure after accounting for associations due to child adversity. Last, exploratory analyses examined subdomains of cognitive functioning as dependent variables.
See Table 3 for descriptive statistics for study variables.
Descriptive Statistics for Key Study Variables.
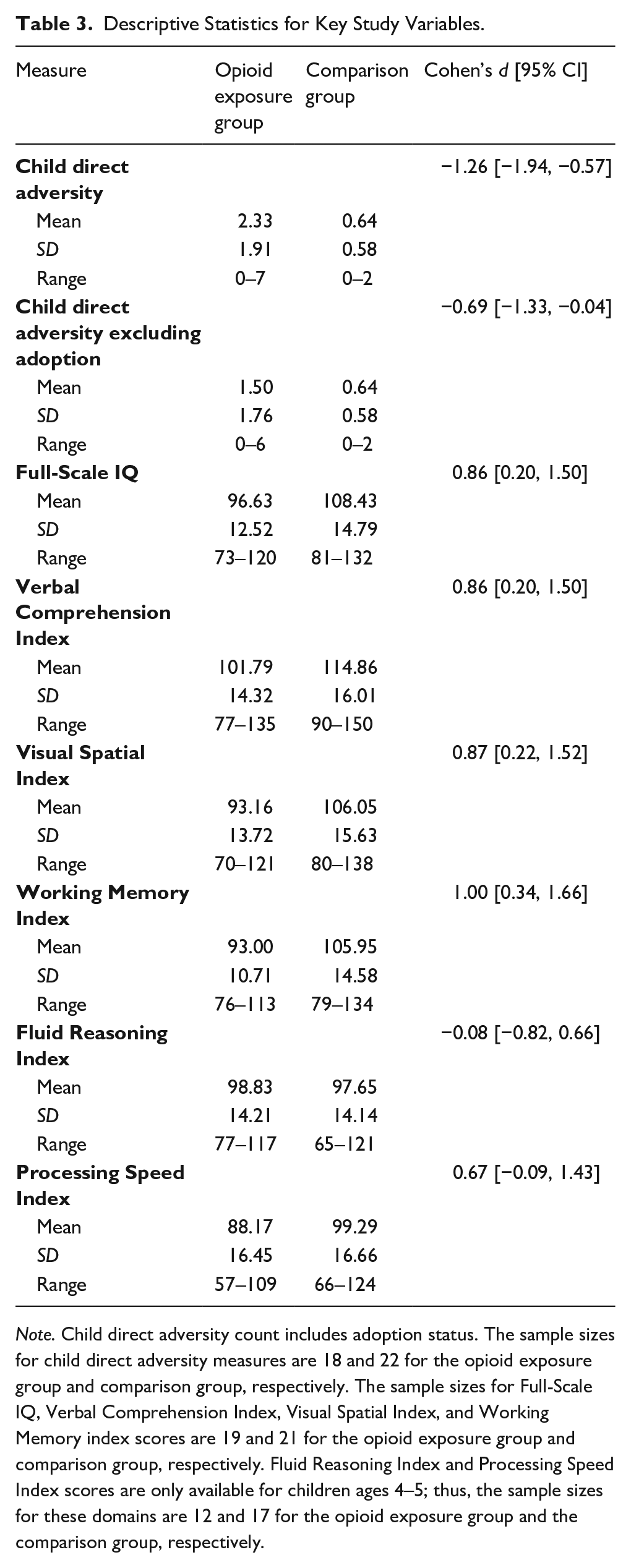
Note. Child direct adversity count includes adoption status. The sample sizes for child direct adversity measures are 18 and 22 for the opioid exposure group and comparison group, respectively. The sample sizes for Full-Scale IQ, Verbal Comprehension Index, Visual Spatial Index, and Working Memory index scores are 19 and 21 for the opioid exposure group and comparison group, respectively. Fluid Reasoning Index and Processing Speed Index scores are only available for children ages 4–5; thus, the sample sizes for these domains are 12 and 17 for the opioid exposure group and the comparison group, respectively.
Results
Results revealed a significant group difference in full-scale IQ scores, t(38) = 2.73, p = .005 (Cohen’s d = 0.86, 95% CI [0.20, 1.50]), such that the comparison group (M = 108.43, SD = 14.79) scored higher than the exposed group (M = 96.63, SD = 12.52). Overall, both groups had mean scores in the “average range” and only five children (12.5%; three in the exposed group and two in the comparison group) were in the “low average” category (which ranges from Full-Scale IQ 80–89) and an additional two children (5%; both in the exposed group) were in the “borderline” category (which ranges from Full-Scale IQ 70–79). Children in the exposed group were three times more likely to have scores below 90 than children in the exposed group (OR = 3.01, 95% CI [0.53, 26.20]). Although groups also differed in the number of reported child adversity experiences (W = 72.50, p < .001), such that the comparison group (M = 0.62, SD = 0.59) experienced fewer events than the exposed group (M = 2.16, SD = 1.38), this difference was no longer statistically significant when adoption was excluded from the count of potentially stressful experiences (W = 148, p = .146).
Hierarchical regression was used to examine whether prenatal opioid exposure status was associated with full-scale IQ over and above child adversity (see Table 4). Child adversity explained 3.43% of the variance in full-scale IQ scores and prenatal opioid exposure status explained an additional 6.01% of variance in full-scale IQ scores. The percent of variance in full-scale IQ scores explained by prenatal opioid exposure status without this covariate was 9.44%. Examination of percent overlap in confidence intervals of the change in effect size for the association between prenatal opioid exposure status and cognitive functioning before (β =−0.70, 95% CI [−1.35, −0.05], 9.92% of the variance in full-scale IQ scores) and after the addition of postnatal adversity (β = −0.61, 95% CI [−1.29, −0.08]) as a covariate revealed a 46.42% overlap. These results suggest that the association between prenatal opioid exposure status and cognitive functioning is not better explained by direct exposure to stress during the postnatal period.
Regression Results for Child Direct Adversity and Prenatal Opioid Exposure Predicting Cognitive Functioning (N = 36).
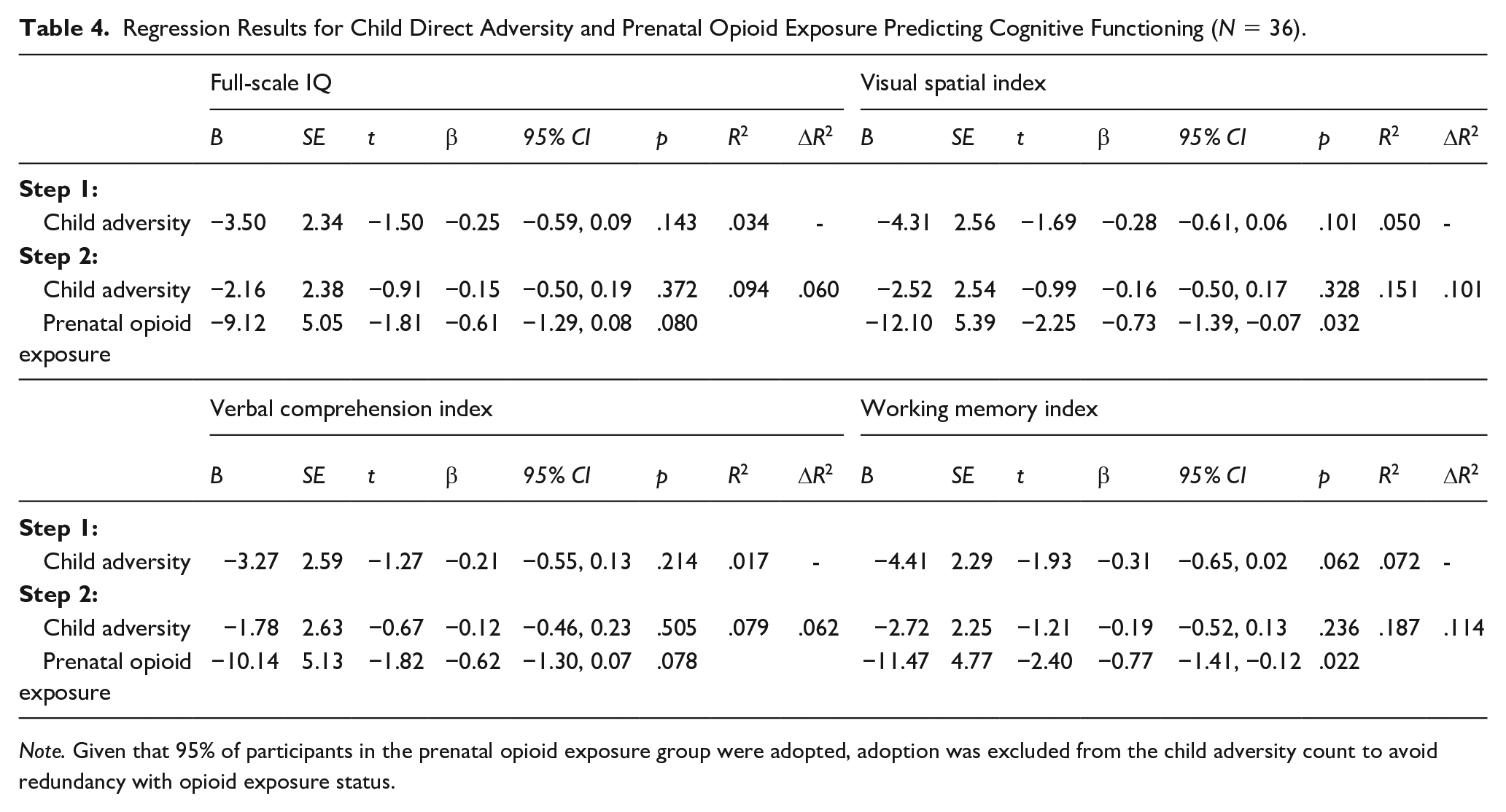
Note. Given that 95% of participants in the prenatal opioid exposure group were adopted, adoption was excluded from the child adversity count to avoid redundancy with opioid exposure status.
Exploratory Analyses
To investigate whether specific domains of cognitive functioning were potentially driving the associations found with full-scale IQ, we separately examined each domain from the WPPSI-IV. The same hierarchical regression approach was used to examine associations with the prenatal opioid exposure status after accounting for child adversity. For all domains obtained with the full sample (i.e., Verbal Comprehension Index, Visual Spatial Index, and Working Memory Index), the same general pattern was found, such that prenatal opioid exposure status explained greater variance in cognitive functioning over and above child adversity (see Table 4). In all cases, lower scores were found among the group with prenatal exposure to opioids. For the two domains (i.e., Fluid Reasoning Index and Processing Speed Index) obtained only in a subset of children (n = 27; as only those children at least 4 years old were eligible for these subtests of the WPPSI-IV), neither child adversity (β =−0.06, 95% CI [−0.46, 0.33]; Fluid Reasoning Index; β = −0.25, 95% CI [−0.63, 0.13]; Processing Speed Index) nor prenatal opioid exposure status (β = 0.52, 95% CI [−0.41, 1.45]; Fluid Reasoning Index; β = −0.26, 95% CI [−1.18, 0.66]; Processing Speed Index) explained significant variance in scores.
Discussion
Preschool-age children with (n = 21) and without (n = 23) prenatal exposure to opioids were assessed to examine associations between prenatal opioid exposure status, postnatal adversity, overall cognitive functioning, as well as performance on specific domains of cognitive functioning. Our results indicated that although children from both groups had mean scores in the average range, preschool-age children with exposure to opioids, as a group, exhibited lower levels of cognitive functioning than children reported to have no exposure to opioids during gestation, and the magnitude of this difference was large. Further, we sought to test whether such associations persisted above and beyond the variance explained by children’s direct exposure to stress, given that children’s exposure to opioids may be characterized by greater levels of adversity. As expected, children with prenatal opioid exposure had exposure to more postnatal adversity relative to comparison children, although this difference was no longer statistically significant after adoption was excluded. After accounting for the potential association between adversity and cognitive functioning, prenatal opioid exposure status explained more than 6% of the variance in cognitive functioning thereby suggesting that the association may not be fully explained by differences in postnatal stress exposure.
The results from the current study provide evidence for the unique association between prenatal opioid exposure status and preschool-age children’s cognitive functioning beyond psychosocial stressors. Our two competing hypotheses were (1) prenatal opioid exposure status would be associated with lower levels of cognitive functioning, even after accounting for postnatal stress and (2) variation in postnatal stress exposure status would better explain differences in cognitive functioning associated with prenatal opioid exposure. The findings from the present study are more in line with the first hypothesis, suggesting the possibility of lasting impact of prenatal opioid exposure that is not better explained by postnatal experiences.
Indeed, opioids are associated with neurogenesis (Wu et al., 2014) and oligodendrocyte-mediated white matter myelination (Vestal-Laborde et al., 2014). Non-human animal research suggests that drugs impact the brain via the mesocorticolimbic reward pathway, beginning in the ventral tegmental area and affecting various cortical and subcortical regions such as the prefrontal regions, amygdala, striatum, thalamus, and insula, regions that are primarily involved in salience, executive function, and working memory networks (Radhakrishnan et al., 2021). While limited, there is also evidence in human research suggesting that brain alterations associated with opioids such as decreased regional brain volumes and changes in white matter microstructure may be associated with later cognitive delays (Merhar et al., 2019; Yuan et al., 2014). In concordance with past work, the results of this study suggest that prenatal opioid exposure may have a persistent impact on developing cognitive functioning.
Given that prior literature examining the impact of opioid exposure on cognitive functioning used full-scale IQ scores as their outcome measure, we conducted exploratory analyses examining performance on other cognitive domains as well and found that the results were largely consistent with the primary analyses. This suggests that prenatal opioid exposure status’ impact may not be specific to any one domain (i.e., working memory, verbal comprehension, etc.) and that lower performance on the various domains may equally contribute to the differences in overall cognitive functioning. However, we found no significant associations between child adversity or prenatal opioid exposure status with fluid reasoning or processing speed. The sample size available for those domains was smaller, given that only 4- to 5-year-olds were eligible for these subtests or that prenatal opioid exposure is associated with relative sparing in some domains. Such conclusions require replications in larger sample sizes.
Notably, the mean IQ scores for both the exposed and comparison groups were in the average range, and this may be indicative of the Flynn effect (i.e., the potential for scores to be higher as test norms become outdated due to a gradual increase in the ability of the general population) (Lee, Pritchard, et al., 2020). Past work examining neurodevelopment of children born to opioid-dependent mothers has emphasized the importance of including a comparison group in the study design to reduce reliance on test norms and likelihood of underestimating risks associated with prenatal opioid use (Lee, Pritchard, et al., 2020). Indeed, our results indicated that children in the exposed group exhibited lower levels of cognitive functioning relative to the comparison group, with the magnitude of this difference being large. Thus, the findings from this study underscore the importance of reducing risks related to opioid use in pregnant people as well as providing intervention services for preschool-age children prenatally exposed to opioids.
Families can be supported in multiple ways including beginning with prenatal interventions to effectively support and reduce opioid use. For example, patient navigation intervention is aimed at assisting pregnant women with opioid use disorder to identify their needs, determine their behavioral health, identify their medical and psychosocial goals, and help them engage with targeted services to reduce threats to maternal and neonatal health (Cochran et al., 2019). Interventions utilizing motivational incentives have also been successful with increased substance use treatment retention (Brigham et al., 2010). While the cognitive functioning in the present study tended to be in the average range, the likelihood that a child with prenatal opioid exposure would exhibit cognitive functioning in the borderline category was high. Thus, while the present study is small and merits replication, the evidence suggests that efforts to reduce exposure during gestation are critical. The findings also underscore the importance of provision of intervention services for preschool-age children prenatally exposed to opioids. Indeed, when children reach preschool age, cognitive difficulties can be reliably identified (Keenan & Wakschlag, 2000). Further, in preschool-age clinical samples with attention-deficit hyperactivity disorder or oppositional defiant disorder, cognitive interventions led to improvements in executive function (i.e., cognitive processes such as working memory involved in behavioral regulation and goal-directed action) (Pauli-Pott et al., 2021), suggesting a potential avenue for intervention to address the difficulties that may follow from prenatal opioid exposure. Future research examining the utility of such interventions for children with prenatal opioid exposure is an important next step.
This research study has six notable limitations. First, the nature of substance exposure in humans does not allow for random assignment. Our comparative design identifies potential pathways from exposure to outcome (Schenker & Rumrill, 2004); however, it cannot determine causality or rule out all plausible rival hypotheses (e.g., that links between opioid use and child cognitive functioning are better explained by inherited characteristics). Alternative research designs, including within-family designs in which children vary in whether they were exposed to opioids during gestation, and longitudinal designs with measures of postnatal environment are better situated to address potential confounds as well as intervening factors. Second, and as a related point, the comparison group, while similar on most demographic factors (i.e., child sex, child age, child race, and highest level of caregiver education), was not an exact match to the exposed group. Third, we did not have access to birth records in this sample, evidence of substance use histories of birth parents during pregnancy including the duration, severity, and chronicity of opioid use and polysubstance use, as well as medical records regarding whether the infant met criteria for neonatal opioid withdrawal syndrome, which are all likely relevant in explaining variation in functioning among the exposure group. Indeed, this is not an etiological study and is not equipped to examine whether the observed difference in cognitive functioning is caused by prenatal opioid exposure. Importantly, however, providers who interact with families with young children exposed to opioids would not typically have more nuanced information about substance histories to guide their practice. Thus, while there is scientific value in studying the sequelae of different forms of exposure, examining children based on group status may be most aligned with the information health care providers and early childhood professionals use to guide decisions. Fourth, our inclusion of postnatal stress attempted to examine a relevant potential intervening factor. However, variability in child adversity was somewhat low and information was acquired through use of retrospective reports. Given a gap in contact between birth and adoption for many children (an average of 5 months for those in the exposed group), those caregivers may be more likely to have been unaware of some of their child’s exposure to adversity and may have trouble recalling information about past events accurately. Further, given all but one child in the exposed group were adopted, these children, relative to those raised in drug-using environment, may be exposed to less adversity and in turn may be why number of adverse events children were directly exposed to was not statistically significantly associated with cognitive functioning. Indeed, other studies with samples of children who experienced more severe stress tend to find that stress is negatively associated with cognitive functioning (Pechtel & Pizzagalli, 2011). Fifth, it is important to note that 95% of the children in the exposed group, and no children in the comparison group, were adopted. Adoptive parents may differ from nonadoptive parents in measurable (e.g., education, income) and less able to be measured (e.g., qualities that lead someone to adopt a child) characteristics (Perry & Henry, 2009). In addition, the extent to which group differences persist when accounting for prenatal care factors such as birth parents’ socioeconomic status would be important (Hurt et al., 1995). Last, the sample was small in size and may not be representative of the larger populations from which they were drawn, thereby limiting the generalizability of the findings.
To conclude, the present study indicates that prenatal opioid exposure status is associated with cognitive functioning above and beyond child adversity, such that children with prenatal opioid exposure had significantly lower full-scale IQ scores relative to the non-exposed group. These findings motivate efforts to reduce opioid use among people who are pregnant or likely to become pregnant, given the association with cognitive functioning among offspring assessed later in development (Saunders et al., 2018).
Footnotes
Acknowledgements
We thank Lauren Bailes and Michael Scudder for their contributions to the manuscript preparation by assisting with data analyses and proofreading of the manuscript, respectively. We also wish to thank all the families that participated in this study and Elizabeth Estes, who was the study coordinator.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vanderbilt Kennedy Center Hobbs Discovery Grant, Nashville, TN to AK; and the Ford Foundation Predoctoral Fellowship from the National Academies of Science, Engineering, and Medicine to EFC.