
Abstract
Research has consistently shown that difficulties in facial emotion recognition (FER) are associated with peer problems and internalizing symptoms during middle childhood. However, no longitudinal research has investigated the direction of effects, that is, how these constructs influence each other across time. In this preregistered three-wave panel study, we tested the directional effects between FER, peer problems, and internalizing symptoms among Finnish school-aged children (n = 3,607; Mage = 8.20, SDage = 0.86; 51% female). The results of random-intercept cross-lagged panel models showed that a low FER accuracy and high biases toward happiness and sadness correlated with higher levels of peer problems and internalizing symptoms at the between-person level. However, we found no evidence of directional effects at the within-person level. Overall, our findings suggest that these constructs might be associated because of shared underlying causes, rather than mutually influencing one another in middle childhood.
Understanding others’ emotions is crucial for human interaction. Facial emotion recognition (FER), involving the identification and labeling of facial expressions, is an important part in this process (Camras & Halberstadt, 2017). FER difficulties include poor accuracy, indicating challenges in correctly interpreting emotions, and recognition biases, which reflect a systematic tendency to misinterpret other’s emotions such as perceiving anger where other expressions are present (Ciucci et al., 2014). In middle childhood, FER difficulties are associated with social-emotional problems, including peer relationship problems and internalizing symptoms (e.g., Dede et al., 2021; Wang et al., 2019). Children with poor FER accuracy face a higher risk of peer victimization (Woods et al., 2009) while those exhibiting depressive symptoms show specific bias patterns, involving an increased sadness bias and reduced happiness bias (Schepman et al., 2011). This raises questions about whether FER difficulties are outcomes of or contributors to these problems. Moreover, it is unclear if there are more complex dynamics, such as bidirectional or mediating processes involved (Dede et al., 2021). Since acquiring and maintaining peer relationships is an important developmental task of middle childhood and failing in it can potentially cause mental health problems (Del Giudice, 2017; Rubin et al., 2015), clarifying these longitudinal associations is crucial to enhance understanding of socio-emotional development and its impact on children’s well-being in middle childhood.
Facial Emotion Recognition and Peer Problems
Theories on socio-emotional processing view FER as an early-stage process necessary for successful social interaction (Camras & Halberstadt, 2017; Crick & Dodge, 1994; Lemerise & Arsenio, 2000). Therefore, it is expected that FER supports the achievement of the salient developmental tasks of middle childhood, such as forming mutual friendships and establishing one’s status in peer groups (Del Giudice, 2017; Rubin et al., 2015). There is robust empirical support for the idea that children who have difficulties in FER are more likely to struggle with peer relationships. For example, poor FER accuracy is related to lower peer status and poor friendship quality (Wang et al., 2019), negative peer nominations (Miller et al., 2005), being relationally victimized (Woods et al., 2009), and general peer problems (White et al., 2021). Moreover, misinterpreting others’ expressions as anger and acting accordingly can have undesirable consequences on peer relationships (Schultz et al., 2004).
Complementing the socio-emotional processing viewpoint, the evolutionary-developmental framework highlights the significance of environmental influences (Del Giudice, 2017). From this perspective, middle childhood, typically spanning from ages 6 to 11, is a period during which children are highly sensitive to their peer experiences (Del Giudice, 2017). Interestingly, some research proposes that challenging socio-emotional environment, such as maltreatment or prolonged social exclusion, may accelerate, rather than delay, the development of FER accuracy (Castro et al., 2015; Pickett & Gardner, 2005; Pollak et al., 2009). Moreover, maltreatment (Pollak et al., 2000) and cyberbullying (Ciucci et al., 2014) have been found to be associated with FER biases toward negative emotions, such as anger, fear, and sadness. Such FER alterations might reflect an adaptation to harsh or unpredictable environments, as they might help children anticipate social conflicts, protect themselves from aggression (Bjorklund & Ellis, 2014), and heighten sensitivity to signals of acceptance or rejection by peers (Pickett & Gardner, 2005). Yet, other research suggests that challenging socio-emotional environments hinder FER accuracy (Wang et al., 2019), possibly due to limited opportunities for socially excluded children to learn recognition skills.
While cross-sectional studies have consistently linked FER difficulties to peer problems in middle childhood (e.g., Wang et al., 2019; Woods et al., 2009), longitudinal research in this developmental period has been relatively limited. White et al. (2021) found that low FER accuracy and high biases at 8.5 years of age predicted peer problems at 10–11 years. Similarly, Miller et al. (2005) found that in kindergarteners and first graders, low FER accuracy in the fall of a school year predicted negative peer nominations and victimization in the spring semester, even after controlling for the initial level of social functioning (Miller et al., 2005). However, both studies are limited by their single-time-point assessment of FER, thereby not controlling autoregressive effects (i.e., a variables effect on itself from one timepoint to the next). To the best of our knowledge, no longitudinal cross-lagged studies have elucidated the directional associations between FER and the social-emotional factors. Thus, based on existing research, it is still unclear whether FER predicts changes in peer relationships or if peer relationships influence FER development. In addition, the effects between FER and peer problems might be bidirectional, in which case, both constructs influence each other over time. Unraveling the direction of effects between FER and peer relationships is critical for understanding the processes underlying social-emotional development.
Facial Emotion Recognition, Peer Problems, and Internalizing Problems
FER and peer relationship problems have also been linked to childhood internalizing problems, such as anxiety and depression (e.g., Christina et al., 2021; Collin et al., 2013). Cognitive models of psychopathology propose that atypical emotional information processing increases vulnerability to and maintains internalizing symptoms (Kircanski et al., 2012), suggesting a direct connection between FER and these problems. Indeed, cross-sectional studies indicate that children with generalized anxiety show perceptual sensitivity to specific emotions, such as happiness, fear, and anger, potentially reflecting increased vigilance to safety or threat cues (Mobach et al., 2022; Rappaport et al., 2021). Similarly, children at high risk of depression have shown greater sensitivity to sad expressions (Lopez-Duran et al., 2013), and those suffering from depression show a heightened bias toward sadness and reduced bias toward happiness compared to their non-depressed peers (Schepman et al., 2011). In a rare longitudinal cross-lagged study (N = 117), Castro et al. (2018) found that generally low FER accuracy at first grade predicted a higher level of internalizing problems at third grade, but not vice versa. Previous studies, however, have not separated the temporarily fluctuating within-person effects from stable trait-like between-person effects, which is necessary for predicting individual changes (Hamaker et al., 2015). Exploring such directional within-person effects from FER to internalizing problems in children is important, as it might offer novel ways to promote children’s socio-emotional well-being (Penton-Voak et al., 2012).
Finally, it is important to consider the more complex interplay between FER, peer relationship problems, and internalizing symptoms. One possibility is that the associations between these constructs occur because of common causes, such as factors related to family environment (Castro et al., 2015). Nevertheless, abundant research indicates a bidirectional association between children’s peer problems and internalizing symptoms (for a review and meta-analysis, see Christina et al., 2021). Moreover, the association between FER, peer problems, and internalizing problems is well established (Dede et al., 2021). This leads to at least three theoretically plausible pathways for how FER may be part of the “vicious circle” between peer relationships and internalizing problems. First, one path involves inadequate FER hindering children’s chances of forming friendships, which may in turn lead to later internalizing problems (Dede et al., 2021). Second, FER difficulties and biases may predispose children to internalizing problems, which may appear as behaviors disliked by peers (e.g., withdrawal or lack of smiling) and lead to problems in peer relationships (Castro et al., 2018; Luchetti & Rapee, 2014). Third, since adverse peer environment is expected to alter children’s social information processing (Crick & Dodge, 1994; Lemerise & Arsenio, 2000), it would be plausible to assume that FER might be a mediator between peer problems and internalizing problems. However, to our knowledge, no previous study has tested the longitudinal mediating paths between these constructs, despite their potential to guide us toward possible intervention targets.
The Present Study
The purpose of the present study was to investigate the directional effects between FER (i.e., total recognition accuracy and recognition biases for happiness, anger, fear, and sadness), peer problems, and internalizing symptoms in middle childhood. We utilized three-wave longitudinal design spanning 1.5 years. We used random-intercept cross-lagged panel modeling (RI-CLPM, Hamaker et al., 2015), which allows disentangling the stable trait-level associations (i.e., between-person effects) from the directional effects over time (i.e., within-person effects from one wave to another). If the associations exist primarily at the between-person level, it suggests that they are more likely explained by common causes rather than directional effects.
Our main hypotheses are represented in Figure 1. Our first research question considered the directional effects between FER and peer problems. In accordance with socio-emotional information-processing theories, we hypothesized that high FER accuracy decreases peer problems (H1), while bias toward anger increases peer problems (H2). Regarding H3, given conflicting previous research on whether an adverse social environment hinders or accelerates FER development (e.g., Pickett & Gardner, 2005; Wang et al., 2019), we presented two alternative hypotheses: Aligning with evolutionary-developmental framework (Del Giudice, 2017), we expected that peer problems result in high FER accuracy (H3a) or, consistent with some empirical findings (Wang et al., 2019), that peer problems result in low FER accuracy (H3b). We also expected that peer problems would increase bias toward negative emotions (i.e., anger, fear, and sadness) (H4).
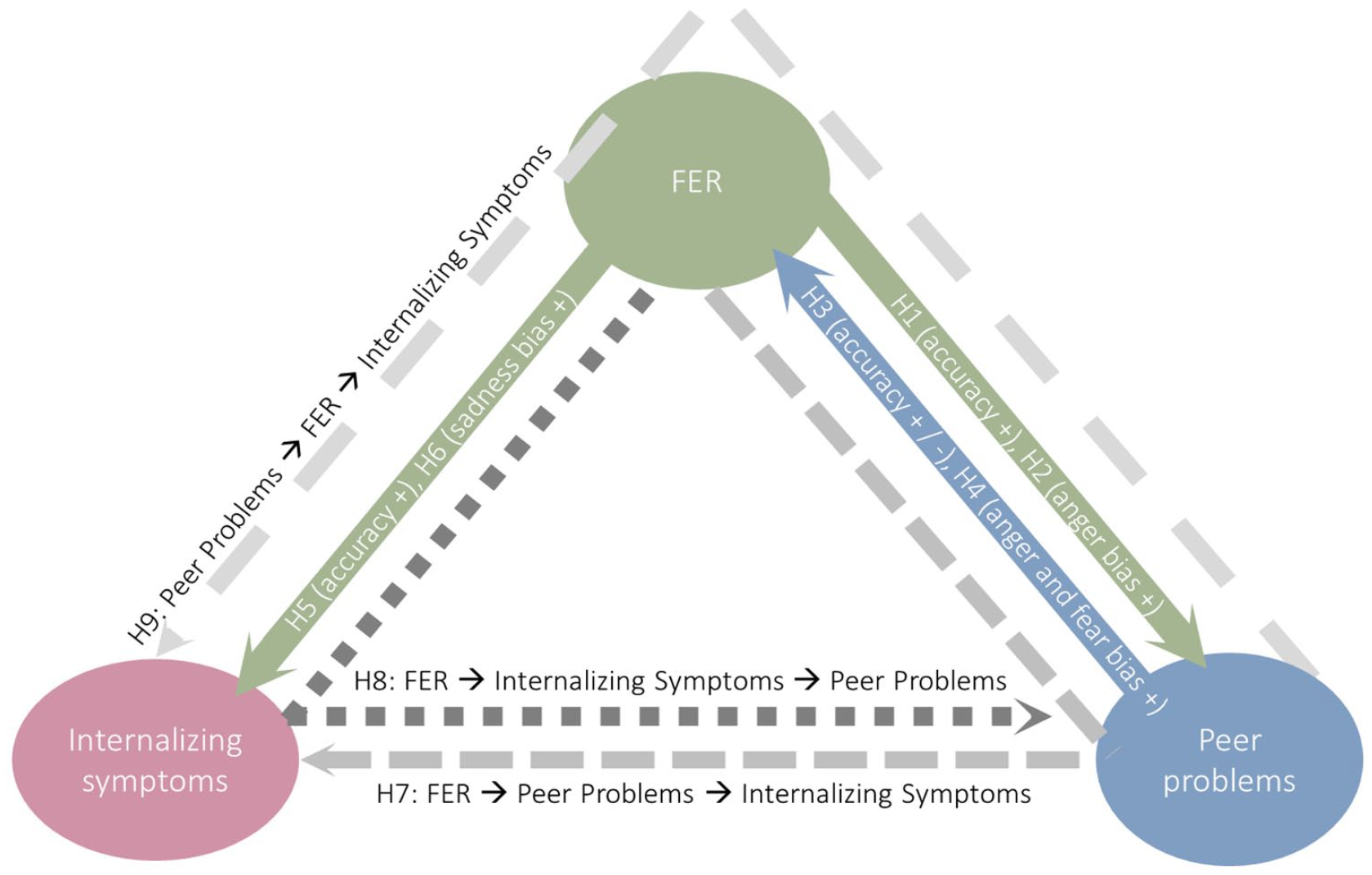
Conceptual Representation of the Hypotheses. Colored solid arrows represent hypotheses regarding directional effects between the constructs (H1–H6). Plus and minus signs refer to positive or negative association, respectively. Gray dashed lines represent mediation hypotheses (H7–H9). FER: facial emotion recognition.
Our second research question considered the directional effects between FER and internalizing symptoms. Based on previous empirical findings on children’s FER and internalizing problems (e.g., Castro et al., 2018), we hypothesized that low FER accuracy increases internalizing symptoms (H5) and that FER biases, especially bias toward sadness, increases internalizing symptoms (H6).
Our third research question considered mediated effects between FER, peer problems, and internalizing symptoms. Consistent with the previous studies (e.g., Dede et al., 2021), we hypothesized that high peer problems mediate the effects of low FER accuracy on internalizing symptoms (H7), high internalizing problems mediate the effects of low FER accuracy on peer problems (H8), and low FER accuracy mediates the effects of high peer problems on internalizing symptoms (H9).
Our hypotheses H1–H8 and analytical strategy were preregistered on Open Science Framework (https://osf.io/umvra). H9 was included after the preregistration upon closer examination of the existing literature.
Method
Sample
The three-wave longitudinal sample consisted of Finnish first, second, and third graders, who participated in a randomized control trial on “Together at School” socio-emotional learning intervention program (Björklund et al., 2014; Kiviruusu et al., 2016). The intervention was not the focus of the present study, yet the group status (i.e., intervention vs control) was controlled for in the analyses. The data were collected in three waves—autumn term 2013 (T1), spring term 2014 (T2), and spring term 2015 (T3). Informed consent was obtained from the parents and the teachers. The children performed computer-based tasks measuring FER in the classroom during a school day with teacher supervision. The teacher-reports were collected using electronic questionnaires. The data collection procedure is depicted in Figure 2. A more detailed description of the intervention study protocol is presented in Björklund et al. (2014). The trial protocol was approved by the Ethics Committee of the Finnish Institute for Health and Welfare (27.9.2012). The present study sample (N = 3,607, Mage = 8.20, SDage = 0.86; 51% females) included all those children who had completed the FER task, and their teachers had filled out the study questionnaires at least at one wave. Based on parental reports (n = 2,865), Finnish was the native language for 2,603 (96%) children, Swedish for 40 (1%) children, and 71 (3%) children had some other native language. Both Finnish and Swedish are official languages in Finland. At T1, 35% of the children were first graders, 40% were second graders, and 25% were third graders, and 55% belonged to the intervention group.
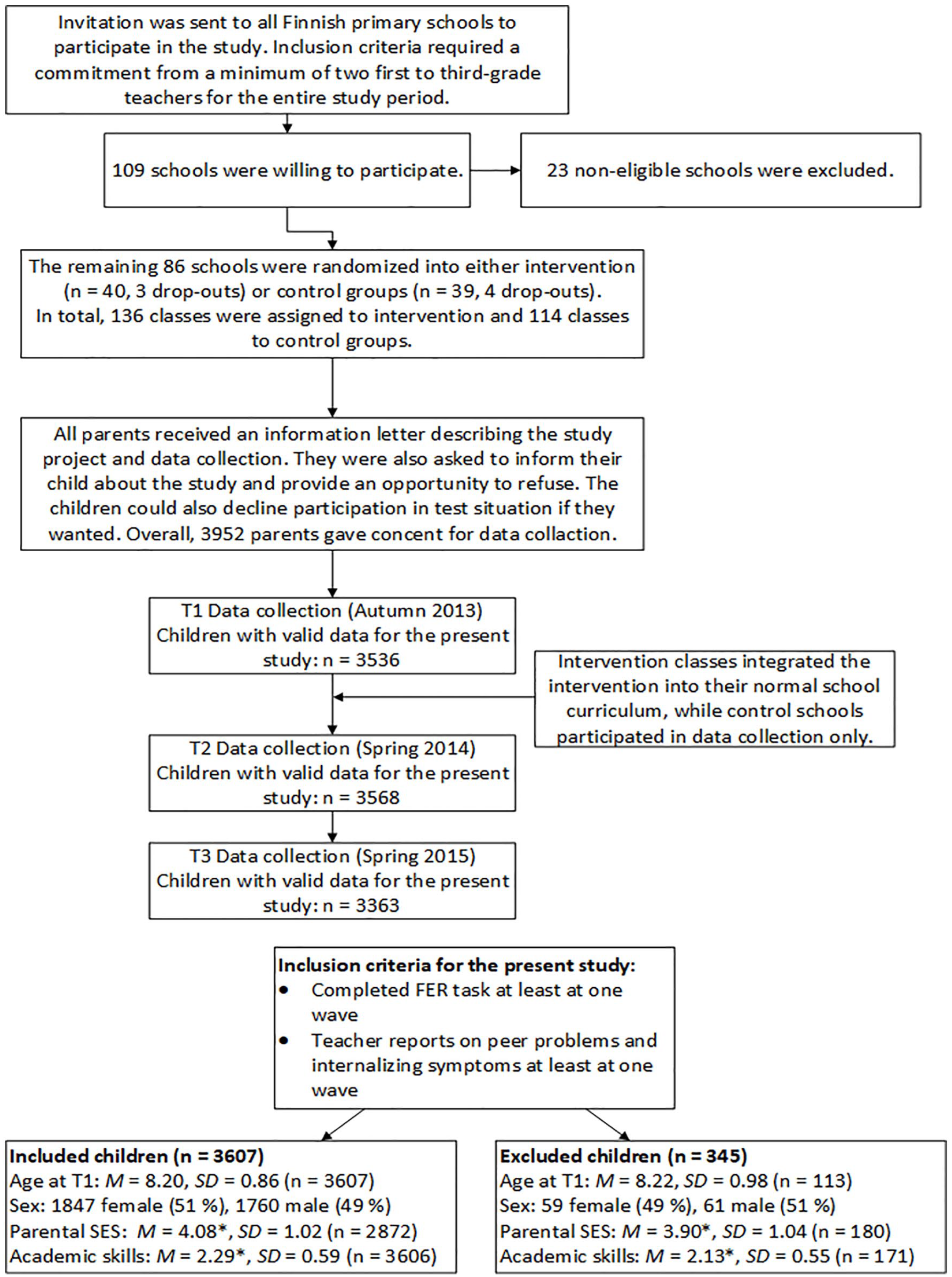
Data Collection Procedure. FER: facial emotion recognition.
Measures
Facial Emotion Recognition (FER T1–T3)
To assess children’s FER accuracy and biases, we used the Diagnostic Analysis of Nonverbal Accuracy 2 (DANVA-2, Nowicki & Duke, 1994). This computer-based test includes 24 photographs of child faces (12 females and 12 males) displaying anger, fear, happiness, or sadness, each at either high or low intensity. Participants viewed these images for 2 seconds and then identified the displayed emotion. DANVA-2 provides error scores, with lower scores indicating higher FER accuracy. We calculated the total error score by summing error scores for all emotions. In addition, we calculated bias scores (angry bias, fear bias, happy bias, sad bias) by summing misattributed responses to other emotions (e.g., fear responses, when anger, happiness, or sadness was presented). Cronbach’s α values for total error scores ranged from .71 to .74 at all assessment points, indicating good internal consistency, consistent with previous research findings (Nowicki & Duke, 1994; Nowicki et al., 2019). FER data were available for 78% of children at all three assessment points, 19% at any two points, and 3% at any one point.
Peer Problems and Internalizing Symptoms (T1–T3)
We assessed children’s peer problems and internalizing symptoms using the Strengths and Difficulties Questionnaire (SDQ, Goodman, 1997), a 25-item questionnaire. Teachers rated each item on a three-point scale (0 = “not at all true,” 1 = “somewhat true,” and 2 = “certainly true”). We focused on the Emotional Symptoms subscale (internalizing symptoms) and the Peer Problems subscale (peer relationships), each consisting of five items. The Cronbach’s α values were .69–.76 at all assessment points (T1, T2, and T3). SDQ scale scores were calculated by summing item scores when three or more responses were available, following the standard SDQ scoring manual (https://sdqinfo.org). SDQ data were available for 80% of children at all three assessment points, 16% at any two points, and 4% at any one point.
Covariates
Based on previous research (Dede et al., 2021; Wells et al., 2021; White et al., 2021), we expected that children’s age, sex, academic skills, and family socioeconomic status (SES) would influence our study variables, and therefore, they were included as covariates in our main analyses. Information on sex and intervention group was available for all 3,607 children. Age data were available for 3,549 (98%), and T1 grade level information was available for 3,596 (99%) participants. Missing age data were imputed using the mean age of the child’s grade level, and missing grade data were imputed based on a participant’s age.
Parental SES was assessed at each wave using the following question: “When including all the income in your household, how easy is it to cover the expenses?” (Likert-type scale: 1 = “very easy” to 6 = “very difficult”). Responses were reverse-coded. Parental SES data were available for 68% at T1, 62% at T2, and 51% at T3. Family SES used in the analyses was the mean across all waves, with high correlations between waves, rs = .72–.79, ps < .001.
Academic skills were measured as a mean of teacher-reported reading, writing, and mathematical skills at T1–T3, rated on a three-point scale (1 = “Below average,” 2 = “Average,” 3 = “Above average”). The Cronbach’s αs were in the range .82–.83 at T1–T3. Academic skills data were available for 94% at T1, 95% at T2, and 86% at T3. Academic skills used in the analyses were the mean across all waves, with high correlations between waves, rs = .74–.83, ps < .001.
Statistical Analysis
Descriptive statistics, including number of observations, means, standard deviations, and Holm-corrected Spearman zero-order correlations for all study variables at each wave, were first explored. For descriptive purposes, we used Friedman’s test to assess changes in study variables over time across grade levels. Post hoc analyses using Holm-corrected pairwise Wilcoxon tests were performed when appropriate. As the primary approach for answering research questions, we used the RI-CLPM (Hamaker et al., 2015) for analyzing the relationships between children’s FER, peer problems, and internalizing symptoms from T1 to T2 and T2 to T3. RI-CLPM allows distinguishing between-person-level variance (i.e., mean differences between subjects) and time-varying within-person-level variance (i.e., individuals deviation from their own trait-like mean over time; Hamaker et al., 2015). All models included peer problems, internalizing symptoms, and one of the five FER variables: Total error, anger bias, fear bias, happy bias, or sad bias score. Thus, the following analytical approach was used separately for each FER variable.
In preliminary analyses, we tested the invariance assumptions for time intervals, sex, grade levels, and covariate effects by comparing nested models. First, we tested the invariance between time intervals by comparing models with freely estimated within-person autoregressive and cross-lagged effects from T1 to T2 and T2 to T3 to models where these effects were constrained to be equal. Second, we used multigroup RI-CLPM to examine whether autoregressive and cross-lagged effects were invariant between boys and girls and across grade levels (first, second, and third, as assessed at T1) (Mulder & Hamaker, 2021). If invariance was observed, results were reported separately for relevant subgroups; otherwise, we favored more parsimonious models. Third, we introduced covariates to the Baseline model which included only between-person effects and autoregressive effects (Model 0, see Figure 3). We sequentially tested whether each covariate’s effect on the observed study variables (e.g., age’s effect on total error score at T1–T3) could be constrained to be equal at each wave.
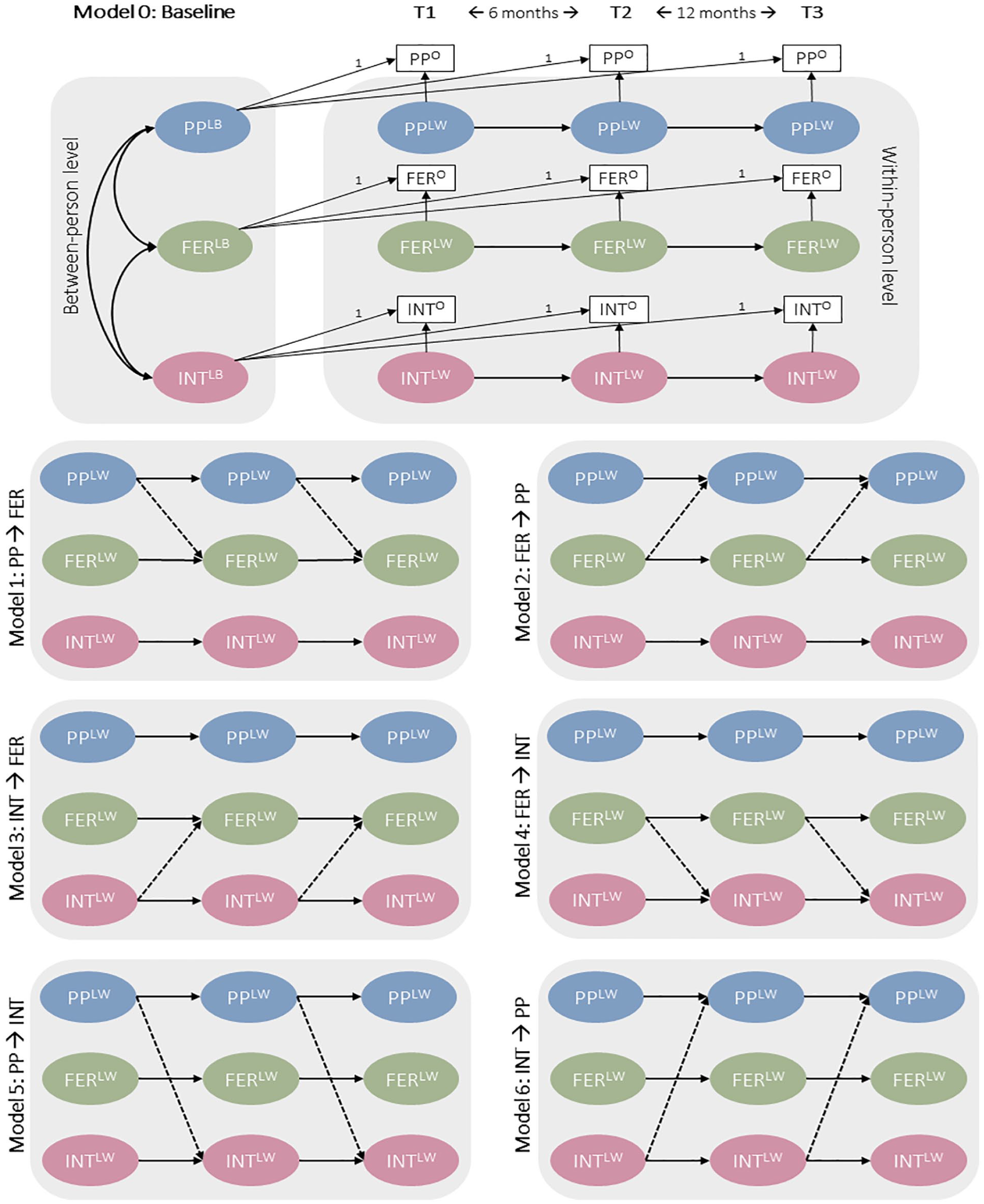
Schematic RI-CLPM Model. N = 3,607. Dashed lines depict cross-lagged effects in each model. Within-person covariances and covariates (sex, age, family SES, and academic skills) are included in all models but are excluded from the figure for simplicity. FER: facial emotion recognition; INT: internalizing symptoms; PP: peer problems; O: observed variable; LB: latent between-person variable; LW: latent within-person variable.
To answer our first and second research questions on directional effects between the study variables, we followed a similar procedure as in a prior RI-CLPM study with three constructs (Zhang et al., 2019). We specified models representing the six directional effects between the constructs (Models 1–6, see Figure 3) and compared them to the baseline model (Model 0). Based on these comparisons, we planned to specify a combined model that included all significant cross-lagged paths from previous steps. If this best-fitting model outperformed the model with freely estimated cross-lagged effects (Model 7), it was selected as the final model. We examined both standardized and non-standardized estimates, standard errors for between-person effects, and within-person autoregressive and cross-lagged effects from the final models. In addition to these preregistered analyses, we explored whether between-person correlations differed between sexes and grade levels. We assessed the significance of estimates using both p values and bias-corrected bootstrap confidence intervals. To answer our third research question regarding mediation hypotheses (H7–H9), we planned to use the bias-corrected bootstrap method for indirect effects (MacKinnon et al., 2004) if significant paths emerged from the RI-CLPM modeling.
In addition to our preregistered RI-CLPM analyses, we conducted the abovementioned analyses using traditional CLPM with total error to demonstrate the impact of including or excluding random intercepts in the model. We compared these models to the RI-CLPM to determine which better fit the data as CLPM is nested within RI-CLPM (Hamaker et al., 2015).
We conducted statistical analyses using Mplus version 8.8 (Muthén & Muthén, 1998–2017) through the MplusAutomation package in R (Hallquist & Wiley, 2018). We employed the maximum likelihood estimator with non-normality robust errors (MLR) for the analyses. To address the clustered data structure (children nested in classrooms), we utilized the TYPE = COMPLEX command in all models. Model fit was assessed using various indices, including chi-square (χ²), Tucker-Lewis Index (TLI), Comparative Fit Index (CFI), Root-Mean-Square Error of Approximation (RMSEA), and Standardized Root Mean Squared Residual (SRMR). Model comparisons were based on Satorra–Bentler scaled chi-squared test for nested models (Satorra & Bentler, 2001, 2010), and the most parsimonious model was preferred. We employed the full information maximum likelihood (FIML) approach to address missing data.
Results
Descriptive Results
Means, standard deviations, and zero-order correlations between study variables are presented in Supplementary Table S1. Overall, concurrent correlations between FER variables and peer problems/internalizing symptoms were generally small (range .04–.12), while those between peer problems and internalizing symptoms were medium-sized (range .36–.37). Autocorrelations ranged from .22 to .68 from T1 to T2 and .23 to .57 from T2 to T3. For descriptive purposes, means and standard deviations are displayed for first, second, and third graders in Figure 4. On average, total error decreased from T1 to T2 and T2 to T3 for all grade levels (all ps < .001), indicating improved FER accuracy. Happy bias, fear bias, and sad bias also decreased from T1 to T2 and T2 to T3 across all grade levels, all ps < .05, suggesting reduced tendencies to misinterpret facial expressions as happy, fearful, or sad. However, anger bias decreased only among first and second graders, all ps < .05. Peer problems scores decreased from T1 to T3 for first and second graders, all ps < .05, while other changes over time were not significant. No significant changes occurred in internalizing symptoms scores across time, all ps > .05.
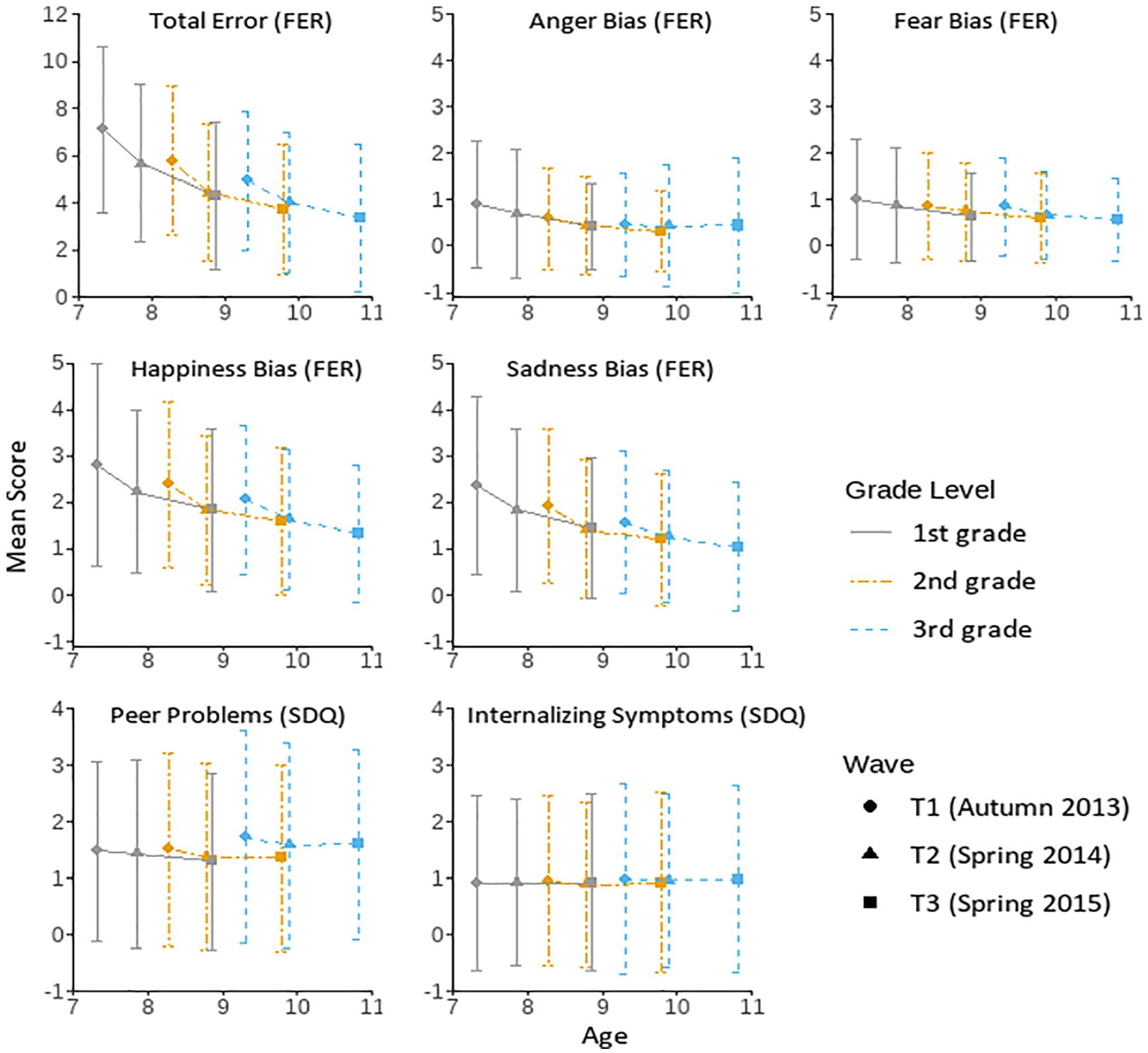
Means and Standard Deviations for Study Variables Grouped by Grade Level. FER: facial emotion recognition; SDQ: Strengths and Difficulties Questionnaire. Total error scores ranged from 0 to 24. Anger bias, fear bias, happiness bias, and sadness bias scores ranged from 0 to 18. Peer problems and internalizing symptoms scores ranged from 0 to 10. The mean ages of first graders (n = 1,271) were 7.33, 7.86, and 8.84 years from T1 to T3, respectively. The mean ages of second graders (n = 1,426) were 8.28, 8.81, and 9.81 years from T1 to T3, respectively. The mean ages of third graders (n = 910) were 9.31, 9.85, and 10.8 years from T1 to T3, respectively.
Preliminary Model Tests and Model Selection
Fit indices and model comparisons for invariance over time between sexes and grade levels are presented in Supplementary Materials. The results indicated that the within-person effects (i.e., autocorrelations and cross-lagged effects) between time intervals could not be constrained to be equal as the model fit was significantly worse in all FER models, all ps < .001 (Supplementary Table S2). Therefore, these within-person effects were freely estimated from T1 to T2 and T2 to T3 in subsequent analyses. Comparisons between girls and boys indicated invariance in all FER models, all ps > .050 (Supplementary Table S3). Also, the effects were invariant between first, second, and third graders in total error, anger bias, happy bias, and sad bias models, all ps > .050, but they differed in fear bias model, ∆χ2 (36) = 52.80, p = .035 (Supplementary Table S4). Further examination indicated that the cross-lagged effects were invariant, ∆χ2(24) = 27.90, p = .264, but autocorrelations were not, ∆χ2(12) = 22.83, p = .029. Therefore, in main analyses, the cross-lagged effects were constrained to be equal in the fear bias models between the grade levels while autocorrelations were freely estimated.
Analyses regarding covariate effects indicated that intervention group did not influence any of the study variables, all ps > .100, and therefore, this variable was excluded from further analyses. Fit indices and model comparisons for time invariance of age, sex, academic skills, and SES effects on study variables are presented in Supplementary Table S5. The results indicated that effects of sex and SES could be constrained to be equal from T1 to T3 for all study variables, all ps > .050. Furthermore, the effect of age could be constrained to be equal from T1 to T3 for peer problems, internalizing symptoms, and happy bias and the effect of academic skills for peer problems, internalizing symptoms, and fear bias.
Main Analyses of the Within-Person Effects
To test our main hypotheses, we compared models reflecting hypothesized directional effects between FER variables (i.e., total error, anger bias, fear bias, happy bias, and sad bias), peer problems, and internalizing symptoms to the baseline model, which excluded all directional (i.e., cross-lagged) effects. Against our hypotheses, adding directional effects to the baseline model did not significantly improve model fit, all ps > .050 (see Supplementary Table S6). That is, the more complex models did not show better fit than the most parsimonious model. In other words, the results provided no support for our hypotheses (H1–H6) regarding any directional effects between the constructs. Model fit indices for the final models (i.e., the baseline models) are shown in Table 1.
Fit Statistics for the Final RI-CLPM Models.
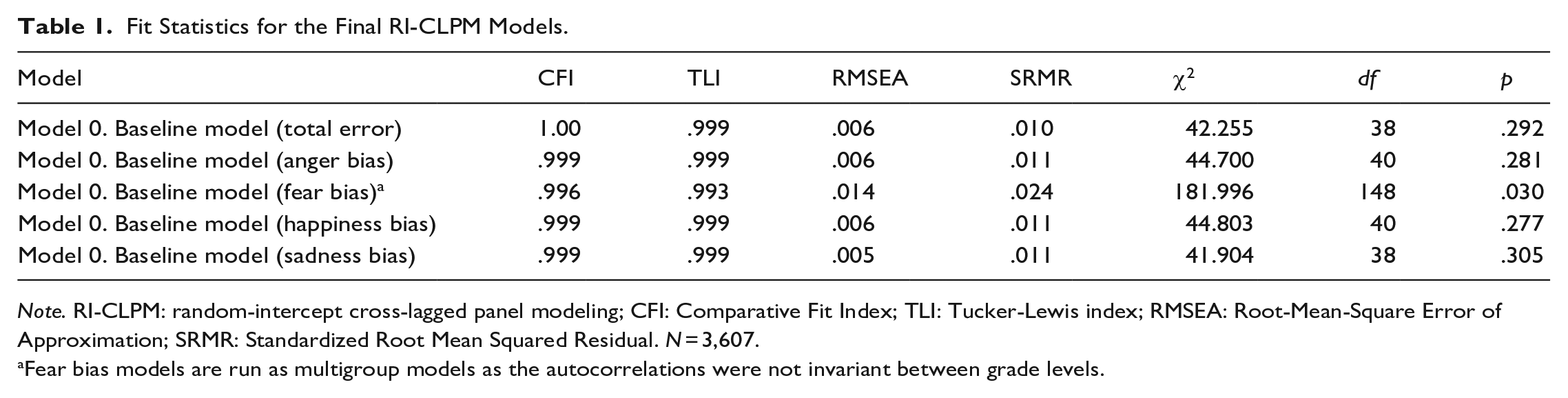
Note. RI-CLPM: random-intercept cross-lagged panel modeling; CFI: Comparative Fit Index; TLI: Tucker-Lewis index; RMSEA: Root-Mean-Square Error of Approximation; SRMR: Standardized Root Mean Squared Residual. N = 3,607.
Fear bias models are run as multigroup models as the autocorrelations were not invariant between grade levels.
Parameter estimates for autocorrelations from the best fitting models (i.e., baseline models) are provided in Supplementary Table S7. Autoregressive paths from T1 to T2 and from T2 to T3 were significant for total error, anger bias, sad bias, peer problems, and internalizing symptoms, all ps < .05. Standardized coefficients ranged from 0.08 to 0.17 for total error, anger bias, and sad bias and from 0.19 to 0.44 for peer problems and internalizing symptoms. These findings suggest carryover effects across time points in these variables, indicating that deviations from one’s own average score predict subsequent deviations in the same variable. For example, children showing less anger bias than their own average are likely to show less anger bias at the subsequent timepoint. Somewhat surprisingly, happy bias showed a significant autocorrelation from T1 to T2 but not from T2 to T3, implying that deviations in happiness bias at T2 do not predict deviations at T3. In the fear bias model, autocorrelations were significant from T1 to T2 and from T2 to T3 for first graders and from T1 to T2 for third graders. However, there were no significant autocorrelations for second graders from T1 to T2 and from T2 to T3, nor for third graders from T2 to T3.
Between-Person Associations
While our directional hypotheses (H1–H6) were not supported, we observed significant between-person correlations (i.e., trait-level associations) in the best fitting models (i.e., baseline models; see Table 2). Results indicated small positive associations between total error, happy bias, and sad bias with both peer problems and internalizing symptoms. In other words, children with lower FER accuracy or a tendency to respond with happiness or sadness when other emotions were depicted experienced more peer problems and internalizing symptoms. Furthermore, there was a small positive association between anger bias and fear bias with peer problems, but not with internalizing symptoms. That is, children showing biases toward angry and fearful faces had slightly more peer problems, with no such association found for internalizing symptoms. As could be expected, there was also a large positive association between peer problems and internalizing symptoms.
Between-Person Correlations From the Baseline Models (Model 0).
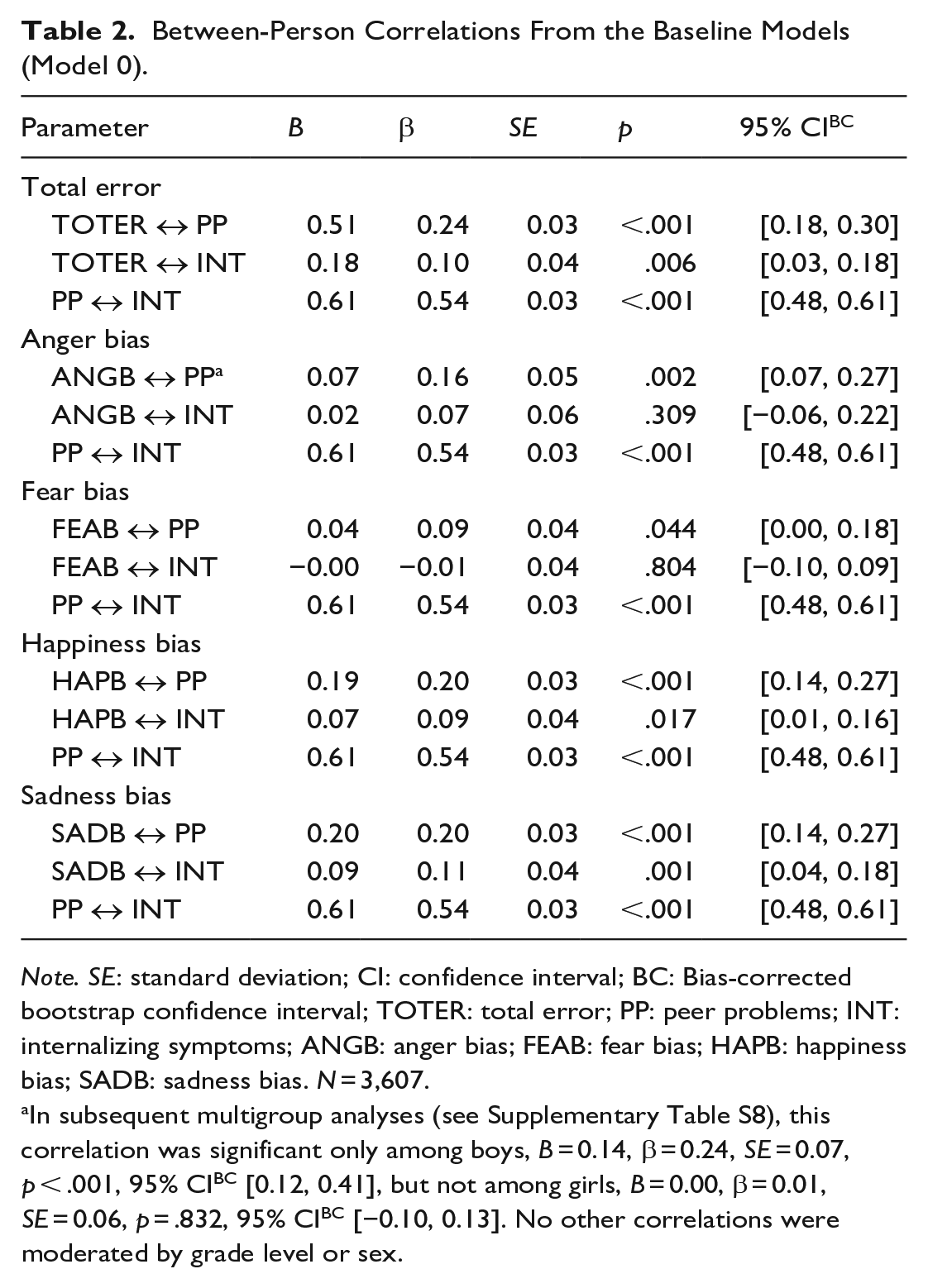
Note. SE: standard deviation; CI: confidence interval; BC: Bias-corrected bootstrap confidence interval; TOTER: total error; PP: peer problems; INT: internalizing symptoms; ANGB: anger bias; FEAB: fear bias; HAPB: happiness bias; SADB: sadness bias. N = 3,607.
In subsequent multigroup analyses (see Supplementary Table S8), this correlation was significant only among boys, B = 0.14, β = 0.24, SE = 0.07, p < .001, 95% CIBC [0.12, 0.41], but not among girls, B = 0.00, β = 0.01, SE = 0.06, p = .832, 95% CIBC [−0.10, 0.13]. No other correlations were moderated by grade level or sex.
Finally, we conducted multigroup model comparisons to explore potential moderators of between-person correlations in the best-fitting models (see Supplementary Tables S8 and S9). The results revealed no differences between first, second, and third graders in any of the models, or between girls and boys in total error, fear bias, happy bias, and sad bias models, all ps > .050. However, constraining between-person correlations between girls and boys in the anger bias model resulted in a worse model fit. Further examination of model parameters suggested that the positive association between anger bias and peer problems was present in boys but not in girls.
Additional Comparisons between RI-CLPM and CLPM
The additional CLPM analyses are presented in Supplementary Table S10. Compared to the RI-CLPMs, all CLPMs showed worse model fit, all ps < .001. CLPM suggested bidirectional paths between total error and peer problems across all waves. Also, there was a unidirectional path from peer problems to internalizing symptoms from T1 to T2 and bidirectional paths between these constructs from T2 to T3. As RI-CLPMs did not reveal any directional paths, we assume that these associations reflect between-person effects.
Discussion
Recent theories relevant to socio-emotional development suggest directional effects between FER, peer problems, and internalizing symptoms (Crick & Dodge, 1994; Del Giudice, 2017; Kircanski et al., 2012; Lemerise & Arsenio, 2000). While previous research provides some empirical support for this idea (e.g., Castro et al., 2015; Dede et al., 2021; Wang et al., 2019), no study has evaluated the direction of effects between these constructs using modern statistical approaches. To achieve this, we utilized RI-CLPM that disentangles the trait-like between-person effects from the within-person effects. First, we hypothesized that FER would predict changes in peer problems, and vice versa. Second, we hypothesized that FER would predict changes in internalizing symptoms. Finally, we hypothesized multiple mediated paths between FER accuracy, peer problems, and internalizing symptoms. Contrary to our expectations, we found no directional within-person effects among the constructs. At the between-person level, however, lower FER accuracy, higher happiness bias, and higher sadness correlated with higher peer problems and internalizing symptoms. Moreover, boys showing bias toward anger were more likely have peer problems. Altogether, our findings suggest that the observed associations among FER, peer problems, and internalizing symptoms during middle childhood may arise from common causes rather than causal relationships.
Associations of FER, Peer Problems, and Internalizing Symptoms at the Between-Person Level
While we observed no directional effects between FER with peer problems and internalizing symptoms, we did find multiple trait-like associations. Consistent with previous research, children with lower FER accuracy experienced more peer problems (Wang et al., 2019; Woods et al., 2009) and displayed higher levels of internalizing symptoms (Rappaport et al., 2021) than their more accurate peers. Furthermore, those showing biases toward fear, happiness, and sadness were more likely to have peer problems. Notably, anger bias was only positively linked to peer problems in boys, indicating that expressions of anger may hold greater significance in boys’ peer interactions. Concurring with this, anger-related attribution biases have been found to associate with aggressiveness among boys but not among girls (Schultz et al., 2004).
Partly compliant with Schepman et al. (2011), we found that children with internalizing symptoms show bias toward sadness, which may reflect depression-related negative interpretation bias (Kircanski et al., 2012). Interestingly, in our study, the internalizing symptoms were associated with higher happiness bias, while Schepman et al. (2011) reported lower happiness bias in children with depressive symptoms. The reason for this discrepancy is unclear but may relate to our focus on the broader internalizing dimension rather than solely depressive symptoms. This finding is consistent with studies on anxiety symptoms (e.g., Mobach et al., 2022) indicating that sensitivity toward happy faces possibly results from vigilance toward safety cues (Rappaport et al., 2021). Altogether, our between-person results support prior research indicating associations between children’s FER alterations and social-emotional problems (e.g., Rappaport et al., 2021; Wang et al., 2019). Importantly, however, our results clarify that these associations are specific to between-person differences.
Cross-Lagged Associations between FER, Peer Problems, and Internalizing Symptoms
Surprisingly, and contrary to our hypotheses, our within-person-level results indicated no directional effects between FER and peer problems. This finding contradicts the social-emotional information-processing models, which suggest that children’s FER influences their social interactions and the development of peer relationships (Camras & Halberstadt, 2017; Lemerise & Arsenio, 2000). Perhaps in typically developing children who do not show severe alterations in FER, misunderstandings with peers do not occur often enough to affect their relationships. These children may also rely on other aspects of social information processing, such as contextual or verbal cues (Lemerise & Arsenio, 2000) and use other skills to compensate for their FER deficits (Menting et al., 2011).
Similarly, the lack of directional effects contradicts the evolutionary-developmental framework, which posits that children’s social-emotional development adapts to their social environment (Bjorklund & Ellis, 2014; Del Giudice, 2017). It is possible, however, that the variance in children’s peer problems was not significant enough to alter children’s developmental trajectories. Relatedly, in middle childhood, children may still primarily rely on their parents for social support, so the quality of family relationships might have a more substantial impact on shaping their FER than peer interactions. For instance, parental emotion socialization practices have shown to explain a significant portion of the variation in children’s FER in middle childhood (Castro et al., 2015). Finally, by middle childhood, children’s FER may have matured and became less malleable, making it more resistant against the influence of current social environment (Leppänen, 2011).
It is noteworthy that the two existing longitudinal studies indicating a positive effect of FER accuracy on peer relationships were unable to disentangle stable trait-like effects from within-person effects (Miller et al., 2005; White et al., 2021). To evaluate the impact of separating these two sources of variance on the results, we ran additional analyses using the CLPM. Indeed, different from our main analyses (i.e., RI-CLPMs), the CLPMs indicated a bidirectional association between these constructs. However, as the CLPM does not control for between-person effects, its estimates of cross-lagged effects should be considered tentative at best (Hamaker et al., 2015). Overall, our results suggest that the previously observed longitudinal associations between FER and peer relationships may be attributed to trait-level effects. Nevertheless, more longitudinal research measuring FER with methods that better imitate real-life situations and consider broader social influences is needed.
Furthermore, FER accuracy or biases did not predict changes in later internalizing symptoms. This result contradicts cognitive models which suggest that disruptions in FER influence the development of internalizing symptoms (Kircanski et al., 2012). This finding is also in contrast with a previous CLPM study that found significant cross-lagged effect from FER accuracy to internalizing symptoms over a 2-year period in middle childhood (Castro et al., 2018). Interestingly, we could not replicate these results in our additional CLPM analyses. While the reason for this remains unclear, it is possible that the effects of FER difficulties accumulate over a longer time and may only manifest in emotional well-being over an extended period (e.g., over 1 year).
Furthermore, the effects of FER might be more evident in clinical populations suffering from more severe mental health problems, such as diagnosable anxiety disorders. Intriguingly, a few experimental intervention studies suggest that emotion-recognition training can influence mental health (Penton-Voak et al., 2012; Wells et al., 2021). Wells et al. (2021) found that brief emotion recognition training in 7- to 10-year-olds improved FER accuracy and reduced the total SDQ score 6 months after the intervention. However, this study did not separate distinct dimensions like internalization and peer problems. In addition, in a randomized controlled trial, young adults trained to recognize happiness over sadness showed increased positive mood at a 2-week follow-up compared with the control group (Penton-Voak et al., 2012). These findings indicate that modulating FER can influence short-term mental health. Yet, it is possible that such effects only occur with intentional training, as suggested by the lack of directional effects in our results. To clarify the causal effects of FER on mental health, future research combining longitudinal and experimental designs is needed.
In summary, our results indicate consistent associations between FER, peer problems, and internalizing symptoms at the between-person level, but not at the within-person level. This finding is important, as it suggests that these constructs may share some common causes, such as parenting and biological factors. For example, harsh parenting has been linked to both FER deficits and socio-emotional problems, indicating that poor modeling of socio-emotional skills could contribute to a range of difficulties (Burley et al., 2022; Hess, 2022). Furthermore, shared biological factors, such as shy temperament (Schermerhorn, 2019; Sette et al., 2016) or genetic susceptibility (Anokhin et al., 2010), may explain the co-occurrence of FER and socio-emotional problems. Moreover, these constructs might have influenced each other during earlier developmental stages, such as negative peer experiences affecting FER during preschool years or vice versa. However, these processes may have stabilized by middle childhood.
Finally, it is essential to consider alternative conceptualizations of the directional effects between FER, peer problems, and internalizing symptoms. Although not examined in our study, children with FER difficulties might be more prone to develop internalizing symptoms when experiencing peer relationship problems. There is some evidence of such moderating role of FER on the relation between mother’s parenting quality and child’s mental health (Song et al., 2022). Furthermore, while our study focused on the relatively short-term changes in these constructs, focusing on longer-term trajectories might provide a different picture. Indeed, in some studies, the intervals have been at least 2 years (Castro et al., 2018; White et al., 2021), while in our study, they were only 6 and 12 months. Alternatively, modeling growth curves might further our understanding of how the long-term development of FER, peer problems, and internalizing symptoms relate to each other. At the same time, it is possible that some of the directional associations between the constructs are more immediate, in which case, even the time span of this study might have been too long to detect them. For instance, a study with adults has shown that social rejection and acceptance can influence mood within a day (Bernstein et al., 2021). Further research is required to analyze the significance of the timespan and to model how the short-term experiences influence long-term development.
Strengths and Limitations
To our knowledge, this is the first longitudinal study testing the directional effects between FER, peer problems, and internalizing symptoms. To provide transparency and confirmatory hypothesis testing, our hypotheses and analytical strategy were preregistered prior to accessing data. Our large representative sample of Finnish school-aged children enabled employing the robust RI-CLPM approach, which should provide more accurate estimates of within-person changes than the traditional CLPM (Hamaker et al., 2015). Indeed, our supplementary analyses demonstrated that RI-CLPMs fit the data better than CLPMs. However, our analytical approach was only able to capture linear associations. Thus, future studies might benefit from modeling nonlinear (e.g., quadratic) relations between the constructs, such as how varying levels of peer problems might affect FER accuracy. In addition, the time span and the developmental timing of our study may not have been optimal to capture the effects. Thus, our results do not exclude the possibility of directional effects between FER, peer problems, and internalizing symptoms over different time periods or in various age groups.
There are also some neurodevelopmental disorders in which FER difficulties are pronounced, such as autism spectrum disorders (Leung et al., 2022). As the sample was drawn from the general population, some children may have had neurodevelopmental disorders or their subclinical forms. However, we did not collect systematic data on these conditions. In the future, it is important to assess to what extent FER alterations in neurodevelopmental disorders contribute to the dynamics between FER and social-emotional difficulties.
Furthermore, we used well-established and widely used measures for assessing FER (DANVA) and social-emotional problems (SDQ), but these measures also have some inherent limitations. DANVA is a relatively simple task with basic facial expressions that may not capture the more fine-grained differences in FER. Some learning effects may have also occurred from the repeated administrations of the task. Regarding the SDQ, we relied only on teacher-reports, which may provide a one-sided perspective on children’s socio-emotional problems and underreporting of internalizing symptoms. In the future, employing multi-informant methods (e.g., including child or parent perspective as well) should be considered.
Conclusion
The findings of the current study show that children’s FER continues to develop throughout the early school years. However, at the individual level, changes in FER do not seem to influence children’s peer relationships or internalizing symptoms, nor do they vice versa. The trait-level associations found in this study indicate a potential common source that links social cognitive difficulties to socio-emotional problems in middle childhood. While it is important to continue investigating the potential of FER as a target of intervention, further research is needed to scrutinize whether the observed correlations reflect causal processes. Meanwhile, assessment of FER difficulties provides an informative indicator of broader socio-emotional problems for clinicians working with young children.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254241233522 – Supplemental material for Facial emotion recognition and social-emotional problems in middle childhood: Assessment of directional effects
Supplemental material, sj-docx-1-jbd-10.1177_01650254241233522 for Facial emotion recognition and social-emotional problems in middle childhood: Assessment of directional effects by Petra Laamanen, Noona Kiuru, Olli Kiviruusu and Jallu Lindblom in International Journal of Behavioral Development
Footnotes
Acknowledgements
The authors are thankful to the participating families and teachers, as well as to all research assistants involved, for their time and commitment. The authors thank the former PI Dr. Päivi Santalahti for her supervising role during the study project.
Data Availability Statement
The data underlying this article cannot be shared publicly due to legal restrictions (Finnish Data Protection Act 1050/2018) and the nature of the data (individual level data). Data are available upon request (contact ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from Jenny and Antti Wihuri Foundation, OLVI Foundation, Oskar Öflund’s Foundation, Otto A. Malm’s Foundation, and Emil Aaltonen Foundation. Manuscript preparation was also supported by the Strategic Research Council (SRC) established within the Academy of Finland (352648 and 352657).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.