
Abstract
Attention deficit/hyperactivity behaviors in children are often unnoticed until they reach school age; however, evidence suggests that attention deficit hyperactivity disorder (ADHD) tends to develop at an earlier age. Recent studies also indicate that perinatal maternal mental health is associated with ADHD symptoms in offspring. This study examines the association between maternal postpartum depression, early hyperactive/aggressive behavior, and later ADHD symptoms. This longitudinal cohort study used data from health checkups and surveys. Mothers with a postpartum Edinburgh postnatal depression scale score ⩾ 9 were considered as having postpartum depression symptoms. The presence of early hyperactive/aggressive behavior was determined based on 3-year-old children’s health checkup data. The ADHD rating scale (ADHD-RS) answered by the caregivers of 182 sixth-grade children was used for the analysis. ADHD-RS scores were significantly higher in children with early hyperactive and/or aggressive behavior (p = .002) and for children of mothers who had postpartum depression symptoms (p < .001). Early hyperactive/aggressive behavior did not mediate the predictive association of maternal postpartum depression symptoms with ADHD symptoms in sixth grade. ADHD symptoms in the sixth grade were independently associated with childhood hyperactive/aggressive behavior at age 3 and maternal postpartum depression symptoms.
Keywords
Introduction
Attention deficit/hyperactivity disorder (ADHD) is a common childhood neurobehavioral disorder. Evidence has shown a recent increase in the number of children diagnosed with this disorder (Sasayama et al., 2022). While the reasons for this apparent increase is not fully understood, expanding awareness of the disorder, changes in public perception, and improved access to healthcare services are likely to play a part (Sasayama et al., 2022; Visser et al., 2014; Xu et al., 2018). Attention deficit/hyperactivity behaviors in children are often identified only when children reach school age. This could be because feedback from teachers at school is one of the most common reasons for seeking an ADHD evaluation (Hodgkins et al., 2013). However, previous studies have suggested that the tendency to develop ADHD occurs at an earlier age (Berger & Nevo, 2011; Lahey et al., 2004).
In Japan, a health checkup is performed for all children at age three, and it is an opportunity to screen for behavioral problems. Children with suspected developmental problems are screened during the health check-up with a follow-up by public health professionals. However, as in other countries (Rocco et al., 2021; Visser et al., 2014), children with ADHD in Japan often go undiagnosed until the age of 7 (Sasayama et al., 2022).
Recent studies have indicated that perinatal maternal mental health may be associated with ADHD symptoms in offspring (Christaki et al., 2022). One study showed that high levels of maternal postpartum depression were associated with higher hyperactivity, inattention, and impulsivity scores in children at age 4 (Koutra et al., 2017). Another showed that maternal postpartum depression was associated with ADHD symptoms in children aged 3–6 years (Wolford et al., 2017).
The role of maternal depression in the development of ADHD symptoms in children has yet to be elucidated. Previous studies have suggested that family environment and lifestyle factors contribute to the development of inattention and hyperactivity symptoms (Holton & Nigg, 2020; Huang et al., 2018). Therefore, the influence of maternal depression on children’s growth environment may be a contributing factor. In particular, postpartum depression hampers a mother’s capacity to care for her infant and causes difficulties in responding to the baby through social interactions (Murray et al., 2003). Another study reported that depressed mothers are more likely to discontinue breastfeeding at an early stage (Dennis & McQueen, 2007). Other possible explanations for the association between maternal depression and ADHD symptoms in offspring include shared risk factors. Pregnancy complications are known risk factors for postpartum depression (Burger et al., 1993) and ADHD (Sciberras et al., 2017). A young maternal age is also a risk factor for postpartum depression (Centers for Disease Control and Prevention, 2008; Pooler et al., 2013) and ADHD (Gao et al., 2023). Furthermore, previous studies suggest that common genes confer liability to both ADHD and depression (Cole et al., 2009; Powell et al., 2021).
Okaya is a city in central Japan with a population of 46,524 as of 1 January 2023. In Okaya, mothers are routinely administered the Edinburgh postnatal depression scale (EPDS) approximately 2 weeks to 1 month after delivery. At the child’s health checkup at age 3, their caregivers are asked to complete questionnaires to assess their child’s hyperactive and aggressive behaviors. All children with possible developmental concerns are followed up by public health nurses and, if necessary, referred to a medical institution where pediatricians provide a diagnosis and suggest care options (Sasayama et al., 2021).
This study uses this health checkup data to investigate the association between early behavior and exposure to maternal postpartum depression and later ADHD symptoms in offspring. ADHD symptoms were assessed in sixth-grade children using the ADHD rating scale (ADHD-RS), and their associations with hyperactive/aggressive behavior at age 3 and the EPDS scores of their mothers were also examined.
Methods
Study Resources
EPDS data from postnatal health checkups in Okaya, Japan, for mothers of children born between 2 April 2009 and 1 April 2011 were retrospectively collected. Japan’s fiscal year begins in April, and children who have their sixth birthday on or before 1 April enter elementary school that year. Therefore, the children whose EPDS scores were retrieved for this study, were sixth graders in 2021 and 2022. ADHD-RS questionnaires were sent to all caregivers of sixth graders in public elementary schools in Okaya between November 2021 and November 2022. An information sheet explaining the details of the study was enclosed with the questionnaire, and only caregivers who provided their consent to participate, for themselves and their child, were asked to complete the questionnaire. Consent was confirmed by the voluntary completion and return of the questionnaire using the enclosed return envelope. The information sheet included in the ADHD-RS questionnaire also explained that participants would be offered a 1,000-yen gift card after completing the questionnaire. Responses from caregivers of children whose mothers’ EPDS data were available were used in this study. Participants whose checkup data at age 3 were unavailable or whose responses to the ADHD-RS were invalid were excluded from further analysis (see Figure 1). The study was approved by the ethics committee of Shinshu University School of Medicine (approval number 5129).
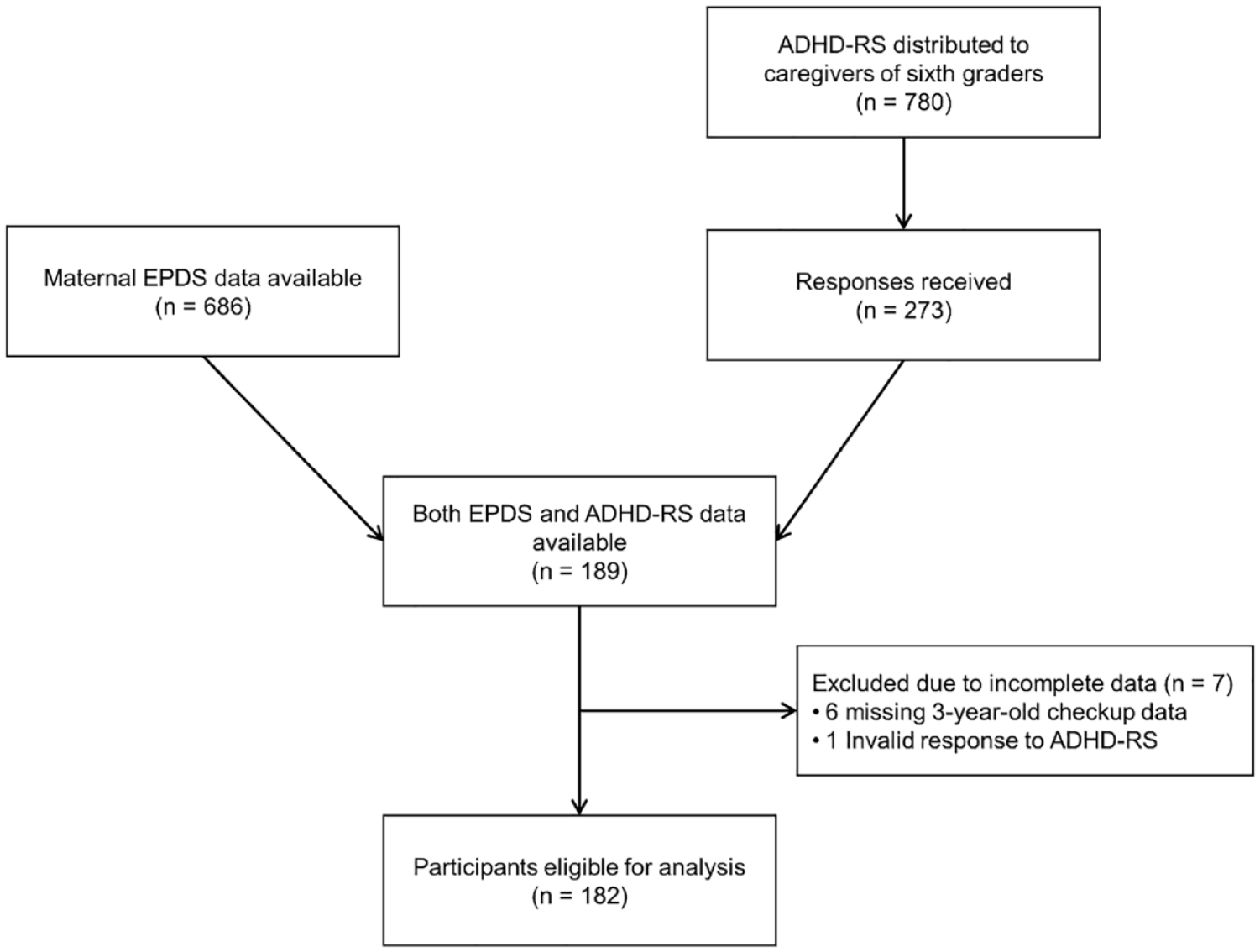
Flowchart of the Inclusion Procedure. EPDS data from postnatal checkups in Okaya were available for mothers of 686 children born between 2 April 2009 and 1 April 2011. The ADHD-RS data were retrieved from 189 caregivers of 686 children. After excluding participants whose checkup data at age 3 were unavailable or whose responses to the ADHD-RS were invalid, 182 participants were eligible for further analysis.
Maternal Depression
Maternal depression was assessed using the EPDS data retrieved from postnatal health checkups in Okaya. The EPDS is administered to all mothers in Okaya at approximately 2 weeks to 1 month postpartum. The EPDS is a 10-item self-report scale designed to screen for postpartum depression in community samples. The Japanese version of the EPDS showed a sensitivity of 75% and specificity of 93% in a Japanese community sample using a cut-off point of ⩾ 9 (Okano et al., 1996), and its psychometric properties have been well examined (Kubota et al., 2014). Mothers with EPDS scores of ⩾ 9 were considered to have postpartum depression symptoms, whereas those with scores < 9 were considered to have no relevant symptoms.
Pregnancy Complications
Data regarding the presence of pregnancy complications were obtained from the health records used for postnatal health checkups. Mothers were considered to have pregnancy complications if they had anemia, severe hyperemesis gravidarum, threatened miscarriage, premature delivery, hypertension, or diabetes.
Hyperactive/Aggressive Behavior at Age 3
According to Japan’s Maternal and Child Health Act, health checkups are provided free of charge to all children at 18 months and 3 years. Questionnaires answered by caregivers during the child’s health checkup at age 3 were used to retrospectively assess the hyperactive and aggressive behavior of the child at age 3. The public health office of Okaya sends a reminder notice by mail to all caregivers of 3-year-old children to ensure that children go for their checkup. Caregivers are asked to complete a questionnaire before and during the checkup. Three questions pertain to hyperactive behavior and two to aggressive behavior in the child. The questions compiled by healthcare professionals are listed in Table 1. If the caregiver answered that one or more hyperactive/aggressive behaviors were present, the child was considered to have hyperactive/aggressive behavior at age 3.
Response Rate of Questions on Hyperactive/Aggressive Behavior at Age 3.
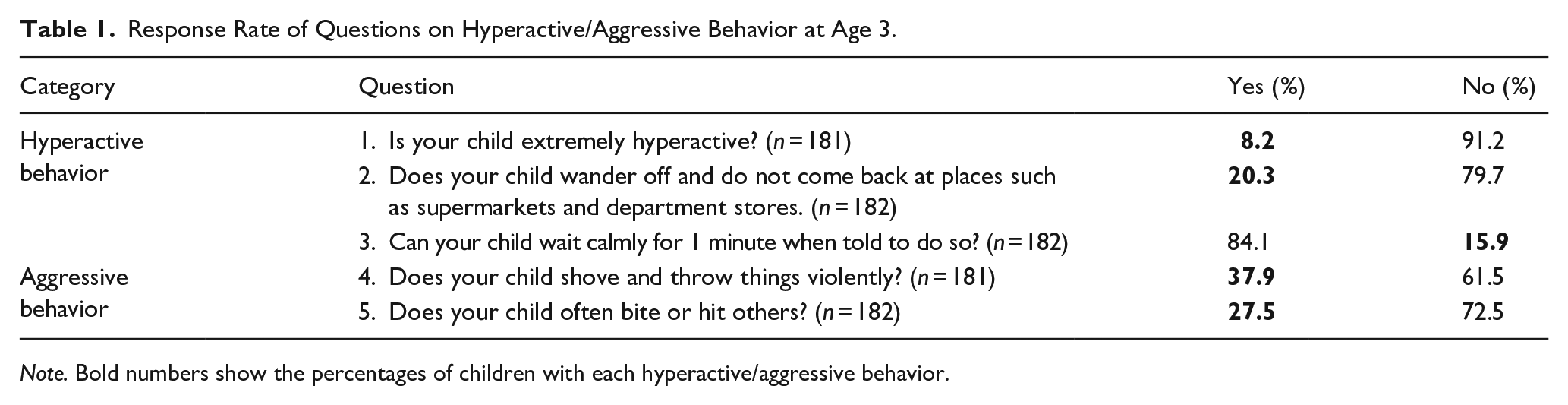
Note. Bold numbers show the percentages of children with each hyperactive/aggressive behavior.
Attention Deficit/Hyperactivity Symptoms in Sixth Grade
Attention deficit/hyperactivity symptoms in sixth-grade children were assessed using the Japanese version of the ADHD-RS. The ADHD-RS consists of 18 items and comprises an inattention and a hyperactivity-impulsivity subscale (DuPaul et al., 1998/2008). The Japanese version of the ADHD-RS has demonstrated adequate reliability and validity (Tani et al., 2010). Caregivers of sixth-grade children were asked to complete the ADHD-RS questionnaire. Scores ⩾ 85th percentile in the parent-reported ADHD-RS indicate a possible diagnosis of ADHD; sensitivity and specificity when applying the 85th percentile as the cut-off score in the parent-rated ADHD-RS are reported to be 0.67 and 0.40, respectively (DuPaul et al., 1998/2008). Therefore, children whose scores were ⩾ 85th percentile of the same age group in the Japanese general population (i.e., ⩾ 12 for boys and ⩾ 7 for girls; Tani et al., 2010) were considered to have significant ADHD symptoms.
Data Collection
The EPDS data from postnatal checkups in Okaya produced a sample of 686 children born between 2 April 2009 and 1 April 2011. In the sample, 108 (15.7%) had scores ⩾ 9 (cut-off score). The ADHD-RS questionnaires were retrieved from 189 caregivers of 686 children. Two of the retrieved ADHD-RS questionnaires had missing values for < 10% of the items (i.e., one missing item each); therefore, the missing items were imputed with the mean of the non-missing items in the same category. Health checkup data at age 3 were available for 183 of the 189 caregivers who responded to the ADHD-RS. After excluding one participant whose ADHD-RS questionnaire had > 10% missing values and six participants whose health checkup data were unavailable, 182 sets of EPDS, ADHD-RS, and health checkup data at age 3 were used for the analysis (see Figure 1).
Statistical Analysis
Differences in continuous variables between boys and girls, EPDS groups with scores of < 9 and ⩾ 9, and children with and without hyperactive/aggressive behaviors were assessed using the Mann–Whitney U test. Chi-square or Fisher’s exact tests were used to compare the frequencies of categorical variables. Missing ADHD-RS item values were imputed if the missing value was < 10% of the entire 18-item checklist (i.e., no more than one item). The missing value of the hyperactive-impulsive item was replaced with the mean value of the other hyperactive-impulsive items, and the missing value of the inattentive item with the mean value of the other inattentive items. These analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 26 (IBM Corp., Armonk, NY, USA).
A path analysis was performed to examine the relationships between sex, maternal postpartum depression symptoms, hyperactive/aggressive behavior at age 3, and attention deficit/hyperactivity symptoms in sixth grade. The presence of maternal postpartum depression symptoms was entered as the predictor, the presence of hyperactive/aggressive behavior at age 3 as the mediator, the ADHD-RS score as the dependent variable, and sex as the covariate for the mediator and dependent variable. An additional analysis was performed after including maternal age at delivery and the presence of pregnancy complications as covariates. The analysis was conducted using 5,000 bootstrap samples to generate bias-corrected 95% confidence intervals. The lavaan package version 0.6-14 (Rosseel, 2012) was used in R version 4.2.2. All tests were two-tailed and p < .05 was considered statistically significant.
Results
The mean (standard deviation) age at delivery of the 182 participating mothers was 32.2 (4.8) years. Pregnancy complications were observed in 30 mothers. The EPDS score was ⩾ 9 for 41 (22.5%) mothers of the 182 children analyzed. The proportion of EPDS scores ⩾ 9 was significantly higher for the mothers of the 182 children analyzed in this study when compared with those excluded from the analyses (i.e., 497 that were lost to follow-up and 7 that were excluded due to incomplete data; χ2 = 8.595, p = .003).
Table 1 shows the percentage of hyperactive/aggressive behaviors at the age of 3 years. A total of 100 children (54.9%) exhibited one or more hyperactive/aggressive behaviors listed in Table 1. Table 2 shows the maternal EPDS scores, hyperactive/aggressive behaviors at age 3, and ADHD-RS scores for each sex. Hyperactive/aggressive behaviors at age 3 was significantly more frequent in boys than in girls (p < .001). The ADHD-RS scores of sixth- grade children were significantly higher for boys than for girls (p < .001). The proportion of maternal postpartum depressive symptoms, as assessed by the EPDS, did not differ significantly between male and female offspring.
Maternal Postnatal Depression, Hyperactive/Aggressive Behavior at Age 3, and ADHD-RS Scores in Each Sex.
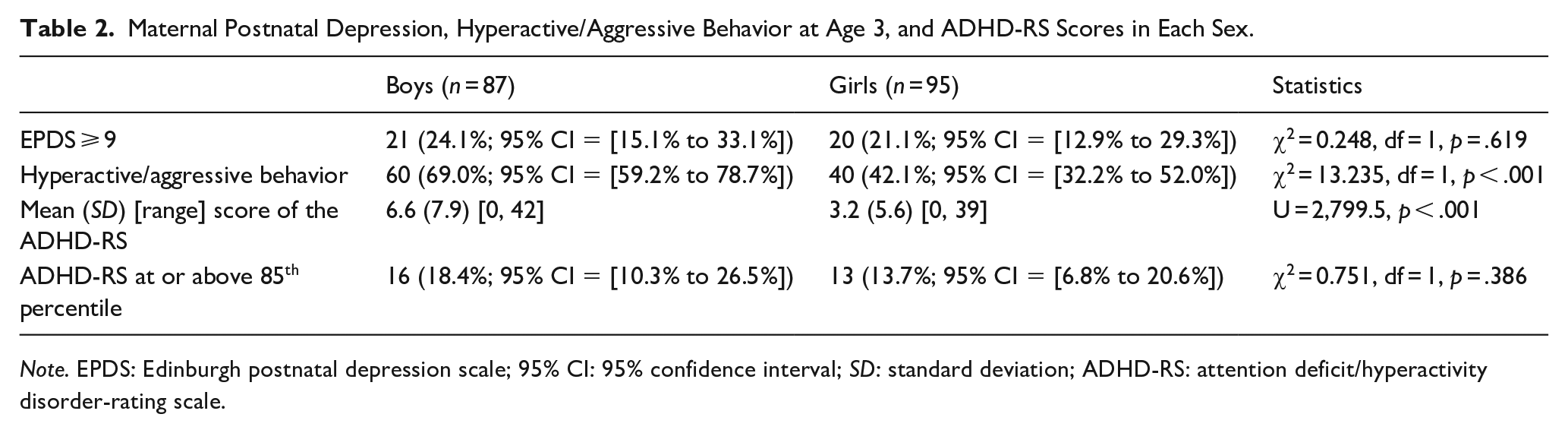
Note. EPDS: Edinburgh postnatal depression scale; 95% CI: 95% confidence interval; SD: standard deviation; ADHD-RS: attention deficit/hyperactivity disorder-rating scale.
Figure 2 shows the ADHD-RS scores of sixth-grade children. Children whose mothers’ EPDS scores were at or above the cut-off of 9 had significantly higher ADHD-RS scores than those whose mothers’ EPDS scores were < 9 (p < .001). ADHD-RS scores were significantly higher among children with hyperactive and/or aggressive behaviors at age 3 than among those without (p = .002). Children with at least one of these two risk factors (i.e., children with hyperactive/aggressive behavior at age 3 and/or exposure to maternal postpartum depression symptoms) had a more than twofold risk of having significant ADHD symptoms (i.e., ⩾ 85th percentile on ADHD-RS) in the sixth grade (relative risk = 2.31, 95% confidence interval [CI] = [1.02–5.26]; p = .021 [Fisher’s exact test]) compared to those without either of the risk factors.
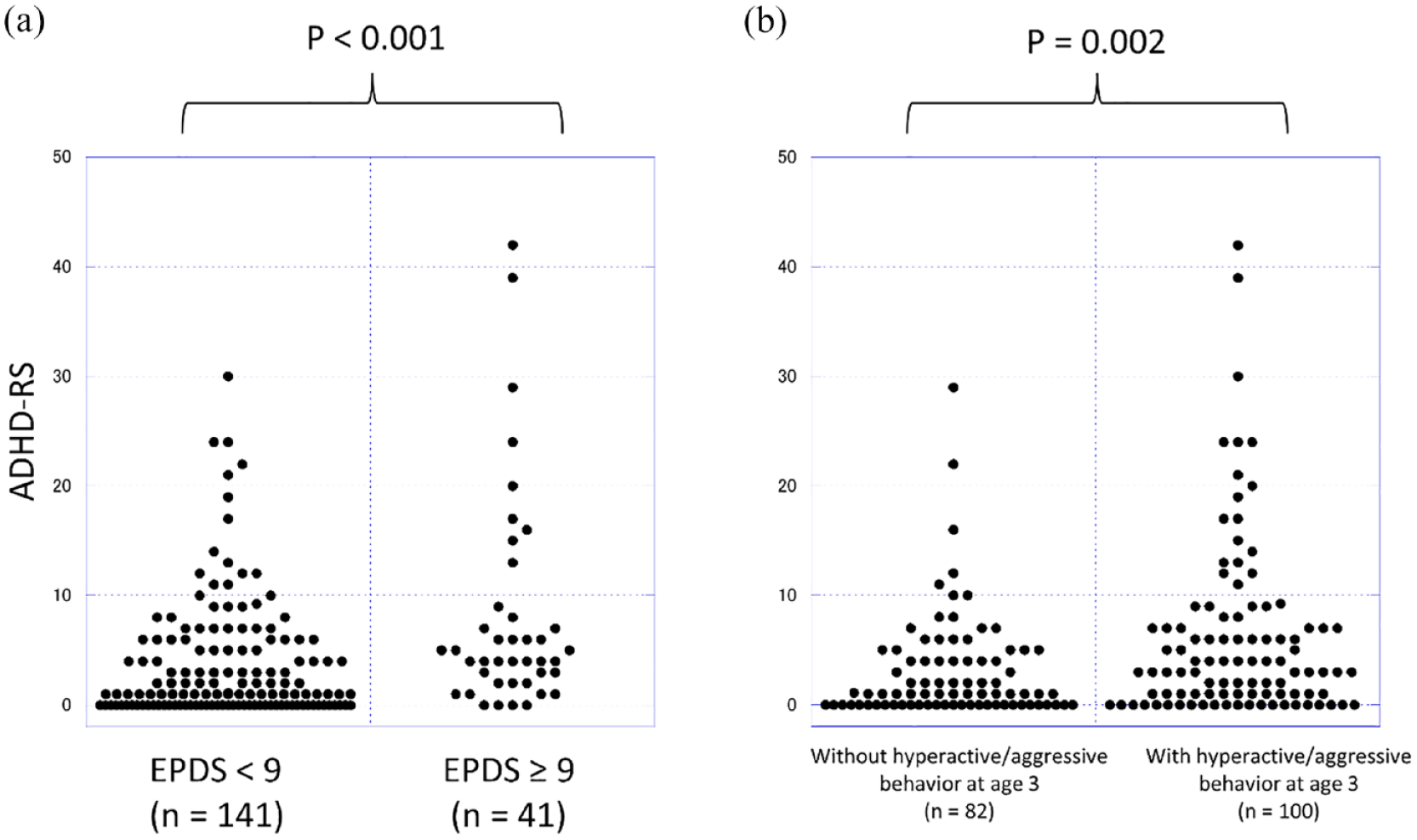
ADHD-RS Scores in Sixth-Grade Children. (a) The ADHD-RS scores of the children of mothers with postpartum depression symptoms were significantly higher than those of their counterparts (p < .001, Mann–Whitney U test). (b) The ADHD-RS scores of children who had hyperactive/aggressive behaviors at age 3 were significantly higher than those of their counterparts (p = .002, Mann–Whitney U test).
Table 3 and Figure 3 show the results of the path analysis. Significant direct effects of sex on hyperactive/aggressive behavior at age 3 (p < .001) and on ADHD-RS scores in the sixth grade (p < .01) were observed. Maternal postpartum depressive symptoms had a significant direct effect on ADHD-RS scores in sixth grade (p < .01). Maternal postpartum depressive symptoms had no significant effect on hyperactive/aggressive behaviors at age 3 (p = .44). The indirect effect of maternal postpartum depressive symptoms on ADHD-RS through hyperactive/aggressive behavior at age 3 was not significant (p = .51).
Path Analysis Results (N = 182).
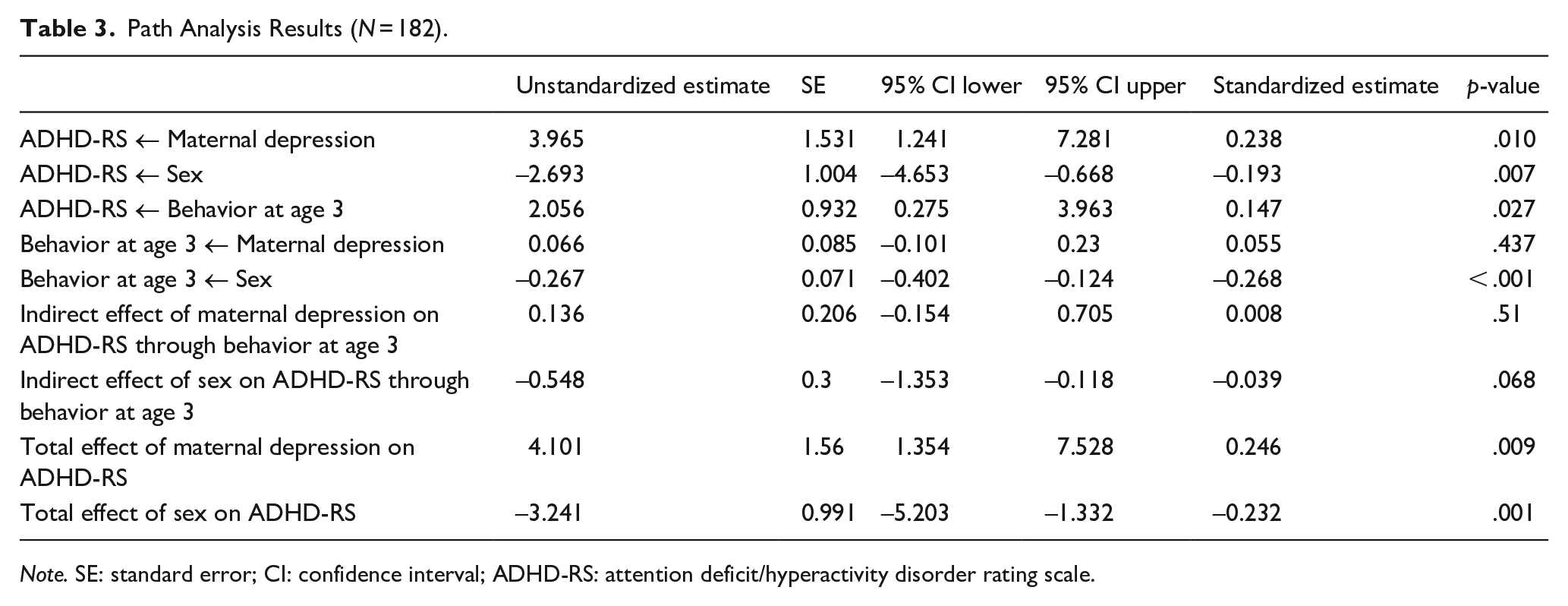
Note. SE: standard error; CI: confidence interval; ADHD-RS: attention deficit/hyperactivity disorder rating scale.
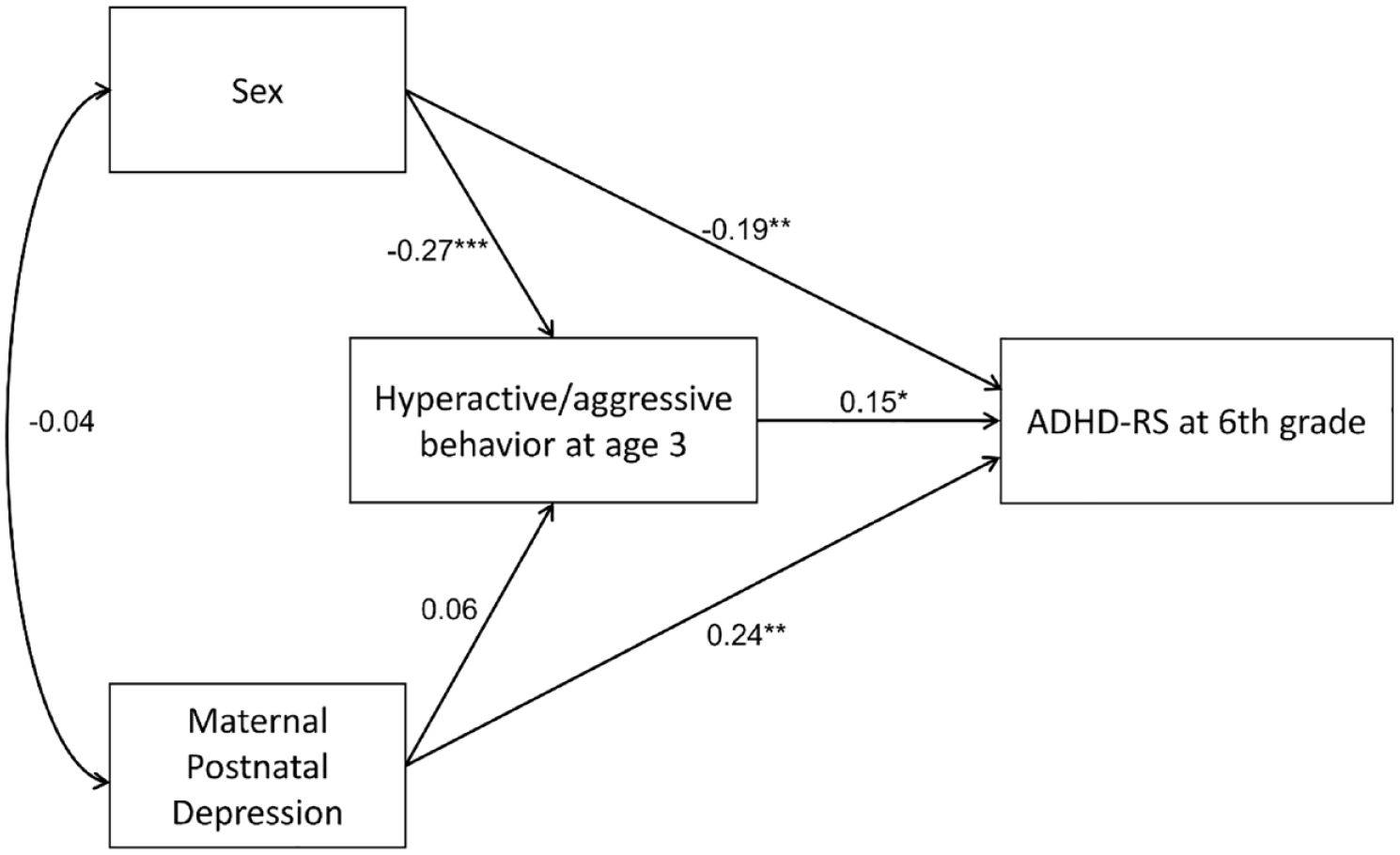
Path Analysis. A path analysis showed significant direct effects of sex on hyperactive/aggressive behavior at age 3 (p < .001) and on ADHD-RS in the sixth grade (p < .01). Maternal postpartum depressive symptoms had a significant direct effect on ADHD-RS scores in the sixth grade (p < .01). Maternal postpartum depressive symptoms had no significant effect on hyperactive/aggressive behavior at age 3 (p = .44). The indirect effect of maternal postpartum depressive symptoms on ADHD-RS through hyperactive/aggressive behavior at age 3 was not significant (p = .51).
Table S1 and Figure S1 in the supplementary material show the results of the path analysis after including maternal age at delivery and the presence of pregnancy complications as covariates. The inclusion of these covariates did not alter the significant associations observed between maternal postpartum depressive symptoms and ADHD-RS or between hyperactive/aggressive behavior at age 3 and ADHD-RS. Pregnancy complications and maternal age at delivery were not significantly associated with hyperactive/aggressive behavior at age 3 or with ADHD-RS in sixth grade.
Discussion
This study examined the association between maternal postpartum depression, early hyperactive/aggressive behavior, and later ADHD symptoms. Significant associations were observed between early behavior and exposure to maternal postpartum depression and later ADHD symptoms in offspring. The findings suggest that the presence of maternal postpartum depression symptoms and hyperactive/aggressive behavior in children at age 3 were predictors of high ADHD-RS scores in the sixth grade. Postpartum depression symptoms of the mother were not significantly associated with hyperactive/aggressive behavior at age 3, and these two indexes were independently associated with ADHD symptoms in the sixth grade.
In line with previous studies, boys were more likely than girls to have hyperactive/aggressive behavior at age 3 and higher ADHD-RS scores in sixth grade (Tani et al., 2010). Studies have shown that physical aggression is more common in males than in females across all age groups and countries (Archer, 2004), but the cause of sex differences in aggression remains debatable. Two contrasting possible explanations are provided by sexual selection theory and social role theory (Archer, 2004).
Sexual selection theory proposes that the biological differences between sexes were shaped over evolutionary time. This theory suggests that males favor aggression because of its benefits in securing mates and protecting resources required for reproduction. In contrast, social role theory proposes that differences in aggression are culturally determined by social gender roles (Campbell & Muncer, 1994). Social role theory is based on a process of learning, where differences between sexes become apparent when children try to fit into their gender role. Thus, the differences in hyperactive/aggressive behavior observed at age 3 between sexes in this study may be occurring too early to be considered elements of gender role acquisition. In contrast, sexual selection theory emphasizes the early emergence of sex differences in behavior (Bjorklund & Pellegrini, 2000). Therefore, the sex differences observed at age 3 in this study are likely caused by biological differences between boys and girls.
Social role theory may contribute to the differences in hyperactive/aggressive behavior observed in our study between sexes in sixth-grade children; however, the significant correlation between hyperactive/aggressive behavior between age 3 and sixth grade indicates that biological factors are also involved in sex differences in sixth-grade children. In line with this interpretation, recent findings indicate that social role theory plays a partial role in sex differences in aggression, but that biological factors are responsible for more of the differences between males and females (Nivette et al., 2014).
Our finding that hyperactive/aggressive behavior at age 3 predicts higher ADHD-RS scores in sixth grade supports previous evidence of parental assessments of ADHD behaviors during preschool years having predictive validity in diagnosing ADHD (Berger & Nevo, 2011). This study’s results indicate that a simple questionnaire administered during a health checkup at age 3 can predict later ADHD symptoms. Thus, further investigation is needed to develop a screening tool for identifying children with ADHD at an early age.
The association between maternal postpartum depression and ADHD symptoms in sixth-grade children observed in this study is consistent with accumulating evidence that maternal postpartum depression is a risk factor for ADHD in children (Christaki et al., 2022). One reason for this association may be the environmental influence of maternal depression on a child’s growth (Murray et al., 2003). The novelty of study’s findings was that hyperactive/aggressive behavior at age 3, a predictive factor for future ADHD symptoms, was not significantly influenced by maternal depressive symptoms.
Our results are inconsistent with previous studies that showed an association between ADHD symptoms in young children and depression in their mothers (Gutierrez-Galve et al., 2015; Koutra et al., 2017; Wolford et al., 2017). There are two possible explanations for this discrepancy. First, the sample size was too small. The correlation between postpartum depression in mothers and ADHD symptoms in their children reported in previous studies was relatively weak, although significant (Gutierrez-Galve et al., 2015; Koutra et al., 2017; Wolford et al., 2017); a larger sample size may have yielded significant results. Nevertheless, our findings are novel in that a stronger association of maternal postpartum depression symptoms was observed with ADHD symptoms in the sixth grade than with hyperactive/aggressive behavior at age 3. Second, children were screened for hyperactive/aggressive behaviors during routine health checkups using a simple questionnaire. Since many of the “positive” children had mild hyperactive/aggressive behavior, 54.9% were considered to have hyperactive/aggressive behavior. Thus, our study’s results indicate that nonpathological hyperactive/aggressive behavior is unrelated to maternal depression. If so, the present findings suggest that even mild nonpathological hyperactive/aggressive behavior is associated with ADHD symptoms in the sixth grade. These findings emphasize the importance of screening for hyperactive/aggressive behaviors during routine checkups in early aged children.
One possible interpretation of our findings may be that the mother’s interaction with the child may affect how aggressive behavior identified as early as 3 years old persists into the school-going years. This interpretation is consistent with a previous study that reported that the mother’s perceived difficulty with a child was strongly associated with continued aggression (Kingston & Prior, 1995). Thus, maternal depressive symptoms may contribute as an environmental risk factor in the development of ADHD symptoms at a later stage of growth. Therefore, family-based interventions may be desirable for preschool at-risk children to improve their long-term behaviors.
Further investigation is necessary to determine how maternal postpartum depression affects ADHD symptoms in children. As mentioned above, the environmental influence of maternal depression on children’s development is likely one of these factors. However, other factors may also be involved. For example, shared genes may increase the chances of children developing ADHD symptoms and mothers developing depression. This explanation is supported by the finding that the prevalence of postpartum depression is higher in women with ADHD (Dorani et al., 2021). This shared genetic explanation could explain the present results if this particular subtype of ADHD does not manifest as hyperactive/aggressive behavior at an early age.
Although the factors underlying this association remain to be investigated, the present findings emphasize the importance of screening mothers for postpartum depression and children for early hyperactive/aggressive behaviors. Children whose mothers have postpartum depression and children who have hyperactive/aggressive behaviors at age 3 should be carefully monitored for the early detection of ADHD.
This study has several limitations that should be considered when interpreting the findings. First, maternal depressive symptoms and children’s ADHD symptoms were assessed using questionnaires and the participants were not clinically diagnosed. Second, data were collected from only one region of Japan; therefore, the findings may not be generalizable to other populations. Third, the follow-up rate was low, raising concerns about selection bias. The proportion of postpartum depressive symptoms was higher for the mothers included in this study than for those excluded from the analyses. Therefore, the present sample was biased toward mothers with depression. However, the children’s ADHD-RS scores were similar to those previously reported in a large community sample of same-aged Japanese children (Tani et al., 2010). Fourth, hyperactive/aggressive behaviors at age 3 were assessed using questions asked during routine health checkups and not by a validated scale. Fifth, the replacement of missing values with the mean could reduce variance and increase bias. That said, the impact on the results was likely negligible because only one missing value from each of the two participants was imputed. Finally, we did not examine several confounding factors related to childhood development. Factors such as socioeconomic status, family composition, and parental education may also be confounding factors in the association between maternal postpartum depression and child development.
In conclusion, the presence of maternal postpartum depression symptoms and hyperactive/aggressive behavior in children at age 3 independently predicted increased ADHD symptoms in offspring in the sixth grade. These findings highlight the importance of careful screening for maternal postpartum depression and early hyperactive/aggressive behaviors in children during routine health checkups. We hope that the results of this study will help improve the sensitivity of ADHD screening in young children.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254231218285 – Supplemental material for Maternal postpartum depression symptoms and early childhood hyperactive/aggressive behavior are independently associated with later attention deficit/hyperactivity symptoms
Supplemental material, sj-docx-1-jbd-10.1177_01650254231218285 for Maternal postpartum depression symptoms and early childhood hyperactive/aggressive behavior are independently associated with later attention deficit/hyperactivity symptoms by Daimei Sasayama, Tomonori Owa, Tetsuya Kudo, Wakako Kaneko, Mizuho Makita, Rie Kuge, Ken Shiraishi, Tetsuo Nomiyama, Shinsuke Washizuka and Hideo Honda in International Journal of Behavioral Development
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant-in-Aid for Scientific Research, JSPS KAKENHI Grant Number 21K07542. The funder had no role in the design and conduct of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.