
Abstract
Exposure to war is known to impact children’s physical and mental health. Recent research reveals that war exposure might even affect the developmental outcomes of children who are yet to be conceived. In this study, we sought to extend such prior work by investigating longitudinal associations between pre-conception war exposure and the accompanying maternal emotional distress on child sleep. Israeli mothers, who conceived within a year after the Lebanon war in 2006 (N = 68), were followed until their children reached 10 years of age. At that age, child sleep problems were measured through mother and child reports. Results from analyses of covariances (ANCOVAs) showed that war exposure prior to conception itself did not predict child sleep. However, hierarchical regression analyses showed that higher levels of maternal emotional distress, as a result of pre-conception war exposure, predicted more sleep problems in girls. Further exploratory analyses revealed that these associations showed themselves in both maternal and child reports on various sleep domains. In boys, no evidence was found for associations between maternal emotional distress during wartime and sleep 10 years later. These results indicate that war-related pre-conception stress might have long-term, sex-specific effects on child sleep, though replication with larger samples is needed to corroborate the findings.
War is known to profoundly impact the psychological and physical well-being of those who are exposed to it, including children. Several reviews indicate that children exposed to war may suffer from compromised physical and mental health, including sleep problems (Slone & Mann, 2016; Yahav, 2011). In addition, not only direct exposure but also maternal exposure to war (Keasley et al., 2017; Kertes et al., 2016) and maternal war-related stress (Punamäki et al., 2018) during pregnancy have been associated with child development outcomes. Such results signal the potential impact of both direct and indirect war exposure on the next generation.
A growing literature suggests that ontogenetic pathways for the development of physical and mental health problems do not begin at conception. Rather, exposure to war and maternal war-related stress might even affect the lives of children who are yet to be conceived. Such transgenerational effects could be explained by changes in maternal mental health and parenting (Dashorst et al., 2019; Kaitz et al., 2009), or biological mechanisms such as epigenetic alterations in ova or prenatal stress physiology (Keenan et al., 2018; Yehuda & Lehrner, 2018; Zaidan et al., 2013). For example, a review of Holocaust survivors demonstrated compromised mental health in their unexposed children (Dashorst et al., 2019). Moreover, a recent prospective study found higher maternal symptoms of posttraumatic stress disorder prior to conception to be predictive of greater child negative affectivity, adjusting for concurrent maternal depressive symptoms and sociodemographic covariates (Swales et al., 2022). Similarly, studies from our own research group identified longitudinal associations between war-related maternal emotional distress prior to conception and poorer child adaptive behavior and socio-emotional functioning (Beijers et al., 2022; Shachar-Dadon et al., 2017).
In the current study, we seek to extend that work, by investigating child sleep in relation to pre-conception (1) war exposure and (2) maternal war-related emotional distress. Sleep plays a crucial role in the health and development of children. For example, insufficient sleep and sleep problems in children are associated with deficits in higher-order and complex cognitive functions and an increase in behavioral problems (Astill et al., 2012; Short et al., 2018). As such, it is important to unravel the ontogenetic pathways for the development of sleep problems, starting even before conception. A previous study by Baird and colleagues (2009) has already demonstrated that pre-conception maternal distress was a strong predictor of infant night waking at both 6 and 12 months of age, independent of the effects of confounders such as postnatal depression and bedroom sharing. In the current study, we investigate the associations of maternal pre-conception (1) war exposure versus non-exposure and (2) the degree of war-related emotional distress, with a spectrum of long-term sleep outcomes in childhood.
War exposure is defined as the objective, contextual exposure to war. Emotional distress refers to the subjective wartime experience in terms of emotional or physical reactions (Beijers et al., 2022; Shachar-Dadon et al., 2017). While the two types of stress are inevitably positively related (Beijers et al., 2022; Shachar-Dadon et al., 2017), the distinction serves the accuracy of causal attribution and identification of appropriate sites for intervention. Moreover, studies on the effect of maternal exposure to (natural) disasters during pregnancy indicate that both objective hardship and psychological distress compromise all spheres of child development; therefore, it is important to study both (for reviews, see Lafortune et al., 2021; Schoenmakers et al., 2022).
There is a scarcity of studies on the potential effects of stress during the pre-conception period. For obvious reasons, animal studies have focused on the found effects of contextual pre-conception stress exposure on offspring development (Bock et al., 2016; Franklin et al., 2010; Jenkins et al., 2022; Leshem & Schulkin, 2012; Shachar-Dadon et al., 2009; Zaidan et al., 2013). Human studies typically, though not solely (Class et al., 2013; Khashan et al., 2008), emphasize the importance of the subjective experience of stress in the formation of transgenerational effects (Baird et al., 2009; Beijers et al., 2022; Shachar-Dadon et al., 2017; Swales et al., 2022). In line with prior studies on pre-conception war-related stress (Beijers et al., 2022; Shachar-Dadon et al., 2017), we hypothesized that war exposure itself would not, but higher levels of maternal emotional distress during wartime would, forecast more child sleep problems 10 years later.
The effects of maternal war exposure and war-related emotional distress might be moderated by child sex. Prior research in animals (Bock et al., 2016; Franklin et al., 2010; Jenkins et al., 2022; Leshem & Schulkin, 2012; Shachar-Dadon et al., 2009; Zaidan et al., 2013) and humans (Beijers et al., 2022; Li et al., 2010) indicates that pre-conception stress may affect offspring outcomes in a sex-dependent manner. A study on war-related pre-conception stress and socio-emotional development reported transgenerational effects solely in girls (Beijers et al., 2022), while a different study found maternal pre-conception stress effects in increased risk for attention-deficit hyperactivity disorder (ADHD) exclusively in boys (Li et al., 2010). Animal studies indicate that the direction of the sex-specific effects may depend on the type of outcome investigated (Bock et al., 2016; Franklin et al., 2010; Jenkins et al., 2022; Leshem & Schulkin, 2012; Shachar-Dadon et al., 2009; Zaidan et al., 2013). Due to inconsistent previous findings, and a lack of knowledge on pre-conception stress in relation to child sleep, we did not formulate a directional sex-specific hypothesis and instead investigated the interaction between pre-conception war-related stress and offspring child sex on child sleep problems in an exploratory manner.
To investigate associations between pre-conception war exposure, and the accompanying maternal emotional distress, on child sleep, we conducted a longitudinal investigation of mothers who conceived 1–12 months after the Israel–Lebanese Hezbollah war in the north of Israel in 2006. This war was characterized by its circumscribed nature, both in terms of duration (34 days, sharply contrasted with the preceding and post-war periods of normality in terms of stress) and type of threat (missile bombardment), which makes it a unique natural experiment for the investigation of war exposure and war-related emotional distress. Mother–child dyads were recruited in the north of Israel, an area exposed to bombardment during the war, and compared to mother–child dyads in central Israel (beyond missile range).
Methods
Participants
Ethical approval for the study was obtained from the participating hospitals and the University of Haifa (#174/17). Mothers and children signed informed consent. As part of a longitudinal investigation of the impact of pre-conception stress on child development (Beijers et al., 2022; Shachar-Dadon et al., 2017), 377 mothers were recruited after giving birth at The Western Galilee Hospital in the north of Israel (an area exposed to bombardment during the war) or Sheba Medical Center in central Israel (beyond missile range) (T0). Inclusion criteria for the study were conception between the second and 12th month after the war, birth to a healthy, full-term infant with no apparent developmental difficulties, and absence of clinical levels of posttraumatic stress disorder symptoms (Shachar-Dadon et al., 2017).
When the children were 3 years old (T1), 107 mother–infant dyads participated in an assessment (Shachar-Dadon et al., 2017). When the children were 10 years old (T2), 68 of the dyads were enlisted from the T1 assessment. Non-participation was mainly due to incomplete contact details, scheduling difficulties, and families not interested. The only significant difference between participants and non-participants at T2 was that participants had lower T1 maternal separation anxiety (M = 94.86, SD = 12.68) than non-participants (M = 100.57, SD = 14.29; p = .03) (Beijers et al., 2022). Of the 68 mother–child dyads at T2, 30 dyads were directly exposed to the bombardment, and 38 dyads were not directly exposed. Demographic characteristics of the final sample are presented in Table 1.
Demographics.
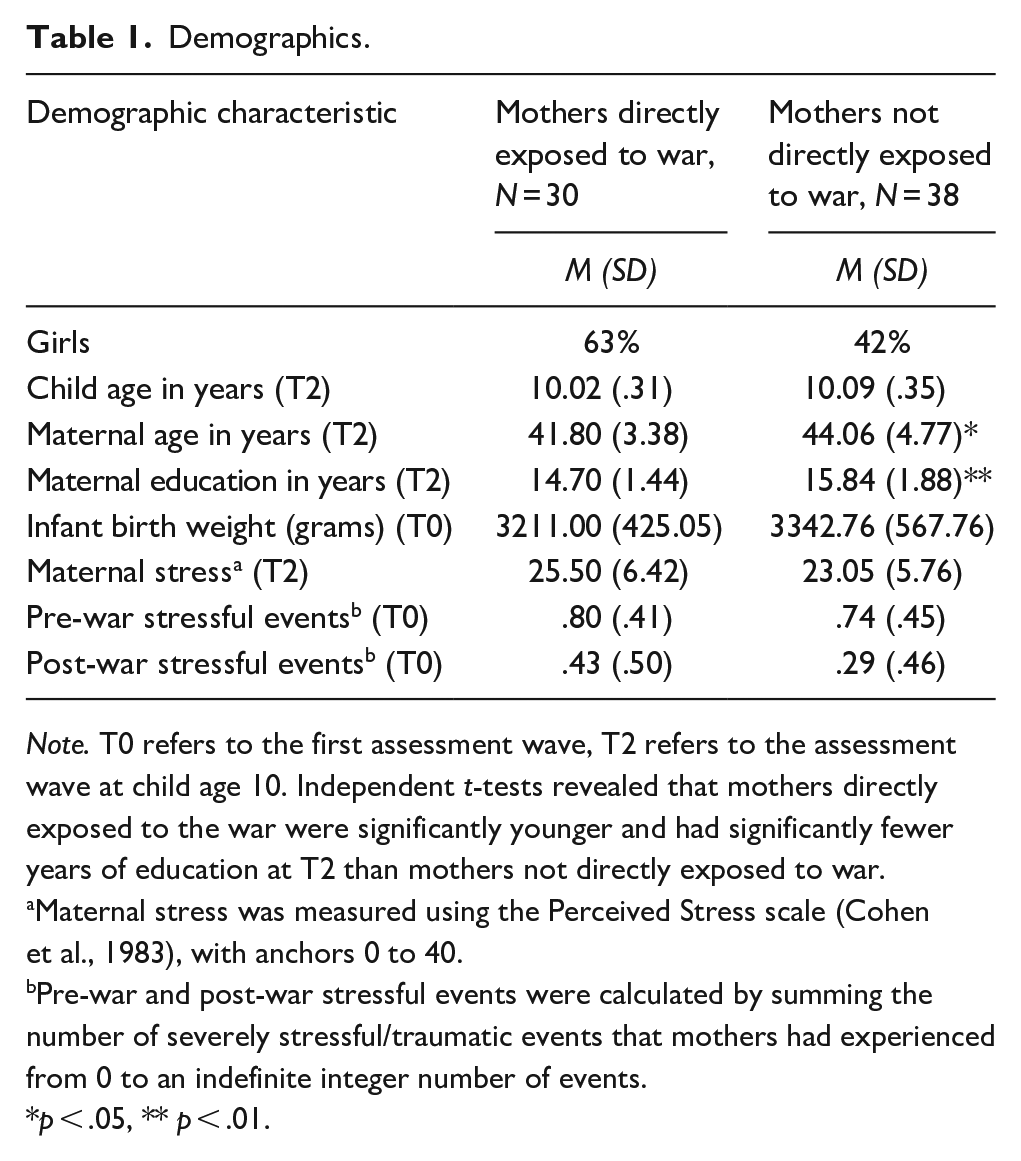
Note. T0 refers to the first assessment wave, T2 refers to the assessment wave at child age 10. Independent t-tests revealed that mothers directly exposed to the war were significantly younger and had significantly fewer years of education at T2 than mothers not directly exposed to war.
Maternal stress was measured using the Perceived Stress scale (Cohen et al., 1983), with anchors 0 to 40.
Pre-war and post-war stressful events were calculated by summing the number of severely stressful/traumatic events that mothers had experienced from 0 to an indefinite integer number of events.
p < .05, ** p < .01.
Procedure
Initial assessment of the mothers (T0) took place after they had given birth, about a year after the war (M = 1.1 years, SD = 0.4). Mothers completed questionnaires on pre-conception war exposure and emotional distress. Demographics, pre- and post-war stressful events were also queried at T0. At the child age of 10 years (T2), mother and child were visited at home, and independently completed questionnaires about child sleep.
Measures
Independent Variables (T0)
War Exposure
At T0 levels of pre-conception exposure to war were assessed with a questionnaire designed specifically for the overarching longitudinal study (Beijers et al., 2022; Shachar-Dadon et al., 2017), querying two aspects of war exposure: proximity to missile explosions and war-related injury and damage. Mothers rated their proximity to missile explosions on an 8-point scale ranging from 1 (none of the missiles fell in proximity to my location or to people I know) to 8 (missiles fell in close proximity to my location and endangered the lives of me or my close family). Mothers rated exposure to several types of war-related damage (personal injury, familiarity with injured, familiarity with killed, damage to personal property, familiarity with others who experienced damage to property, personal damage to livelihood, and familiarity with others who experienced damage to livelihood) on a 5-point Likert-type scale ranging from 1 (not at all) to 5 (very much). Scores on these seven items representing exposure to war-related damage were summed to a composite (score range: 7–21), with higher scores indicating higher exposure to war-related damage. We used a latent factor that included proximity to bombed areas and exposure to war-related damage as a measure of pre-conception war exposure.
Emotional Distress During the War
Mothers’ emotional distress during the war was also measured with a questionnaire specifically designed for the overarching longitudinal study (Beijers et al., 2022; Shachar-Dadon et al., 2017), comprising the two scales: anxiety/helplessness and physical reactions. Anxiety/helplessness was measured with 12 items (e.g., “To what extent did you experience feelings of anxiety throughout the war?”, α = .83). Physical reactions were measured with 13 items (e.g., “To what extent did you experience abdominal pain during the war?”, α = .83). Mothers rated their experiences on a 5-point Likert-type scale ranging from 1 (not at all) to 5 (very much) for each item. A total emotional distress score was created by summing the z-scores of the anxiety/helplessness and physical reactions subscales (α = .91).
Dependent Variables (T2)
Child Sleep
Child sleep was measured through mother and child reports on the Children’s Sleep Habits Questionnaire (CSHQ) for school-aged children (Owens et al., 2000). The frequency of several child sleep-related behaviors, over a typical week, is scored using a 3-point Likert-type scale (rarely = 0–1 night per week; sometimes = 2–4 nights per week; usually = 5–7 nights per week). Hence, higher scores indicate more sleep problems. The mother report version of the CSHQ consists of eight subscales (bedtime resistance, sleep onset delay, sleep duration, sleep anxiety, night wakings, parasomnias, sleep-disordered breathing, and daytime sleepiness), and the child report version consists of six subscales (bedtime resistance, sleep onset delay, sleep duration, sleep anxiety, night wakings, and daytime sleepiness). Summing the scores on these subscales yielded total scores for mother-reported (α = .79) and child-reported (α = .82) child sleep. Comparable to other child samples (Owens et al., 2000; Peled & Scher, 2021; Schlarb et al., 2015), no significant gender differences in scores on total or subscale sleep problems were found. Children of mothers who scored higher on pre-war stressful events reported significantly more total sleep problems (see Table 3), in line with earlier research that has shown a positive relation between maternal trauma and child sleep difficulties (Hairston et al., 2011). There was a trend toward lower levels of child-reported sleep problems for children from mothers who had received more years of education (Table 3). This complements research showing a positive relation between parental education and sleep duration and quality (Cameron et al., 2022).
Covariates (T0 and T2)
As in our previous studies (Beijers et al., 2022; Shachar-Dadon et al., 2017), the current study included the following covariates, assessed at the T0 or the T2 measurement wave: time interval between the end of the war and conception (T0), pre-war stressful events (T0), post-war stressful events prior to the birth of the child (T0), child age (T2), maternal age (T2), maternal education in years (T2), and maternal perceived stress at child age 10 years (T2). Stressful events were assessed by asking mothers about the occurrence of traumatic or stressful experiences, including events like exposure to terror, physical or sexual assault, catastrophic accidents, or other life-threatening events, as well as severe health, financial, or familial problems such as divorce, or death. For both pre-war and post-war stress, composite scores were calculated by summing the number of stressful/traumatic events that mothers had experienced. At T2 the Perceived Stress scale (Cohen et al., 1983) was used to measure maternal perceived stress over the past 30 days. For more information on the covariates, see Beijers et al. (2022) and Shachar-Dadon et al. (2017).
Data Analysis
Descriptives and correlations between the study variables and covariates were calculated. As a preliminary analysis, independent t-tests were performed to test group differences between the group of mothers who were directly exposed to the war (N = 30), and mothers not exposed to the war (N = 38). For the main analyses, two 2-way analyses of covariances (ANCOVAs) were conducted to test the effect of the categorical variable pre-conception war exposure assessed at T0, and its interaction with child sex, on mother- and child-reported total sleep problems at T2, while controlling for covariates. These analyses were followed by multiple hierarchical regression analyses to test the effect of the continuous variable pre-conception maternal emotional distress assessed at T0, and its interaction with child sex, on T2 mother and child-reported total sleep problems, while controlling for covariates. In these regression analyses, the covariates, including child sex, were entered in hierarchical Step 1, and the main effect of maternal emotional distress and its interaction with sex were entered in Step 2. Covariates were included only if they were (marginally) significantly correlated to both the main independent variable and at least one of the subscales or the total of the sleep outcomes. Only if results from the main analyses on mother- and child-reported total sleep scores were (at least marginally) significant, we continued with exploratory investigations of differences in sleep subscales. Finally, we repeated the ANCOVA and multiple hierarchical regression analyses while including the interaction term between T0 war exposure and emotional distress, to see if possible effects of these independent variables were dependent on the other variable. All analyses were performed using Statistical Package for the Social Sciences (SPSS) Statistics 28.
Sensitivity power analyses (G*power 3.1.9.7) indicated that we could find medium-sized effects with our sample size of 68 participants and an α of .05 and a β of .80. Specifically, for the independent samples t-test the suggested effect size for two-tailed testing was d = .69. For the ANCOVA, the suggested effect size for four groups (2 × 2), two covariates, and one numerator degrees of freedom (df) (2-1)(2-1) was f = .35. For the multiple hierarchical regression with two tested predictors and a total of five predictors, the estimated detectable effect size was f² = .15.
Results
Preliminary Analyses
Table 2 presents the descriptives of the study variables, grouped by war exposure. An independent t-test revealed that mothers who were directly exposed to the war experienced significantly more emotional distress during wartime than mothers who were not directly exposed to the war, t(66) = 3.579, p < .001. Furthermore, independent t-tests indicated that children of mothers who were directly exposed to war scored significantly higher on T2 mother-reported sleep anxiety than children of mothers who were not exposed to war, t(66) = 2.658, p = .010. The two groups (exposed vs. non-exposed) did not significantly differ on any of the other mother-reported subscales, nor any of the child-reported subscales. The correlations between study variables and covariates are presented in Table 3.
Descriptives of the Study Variables.
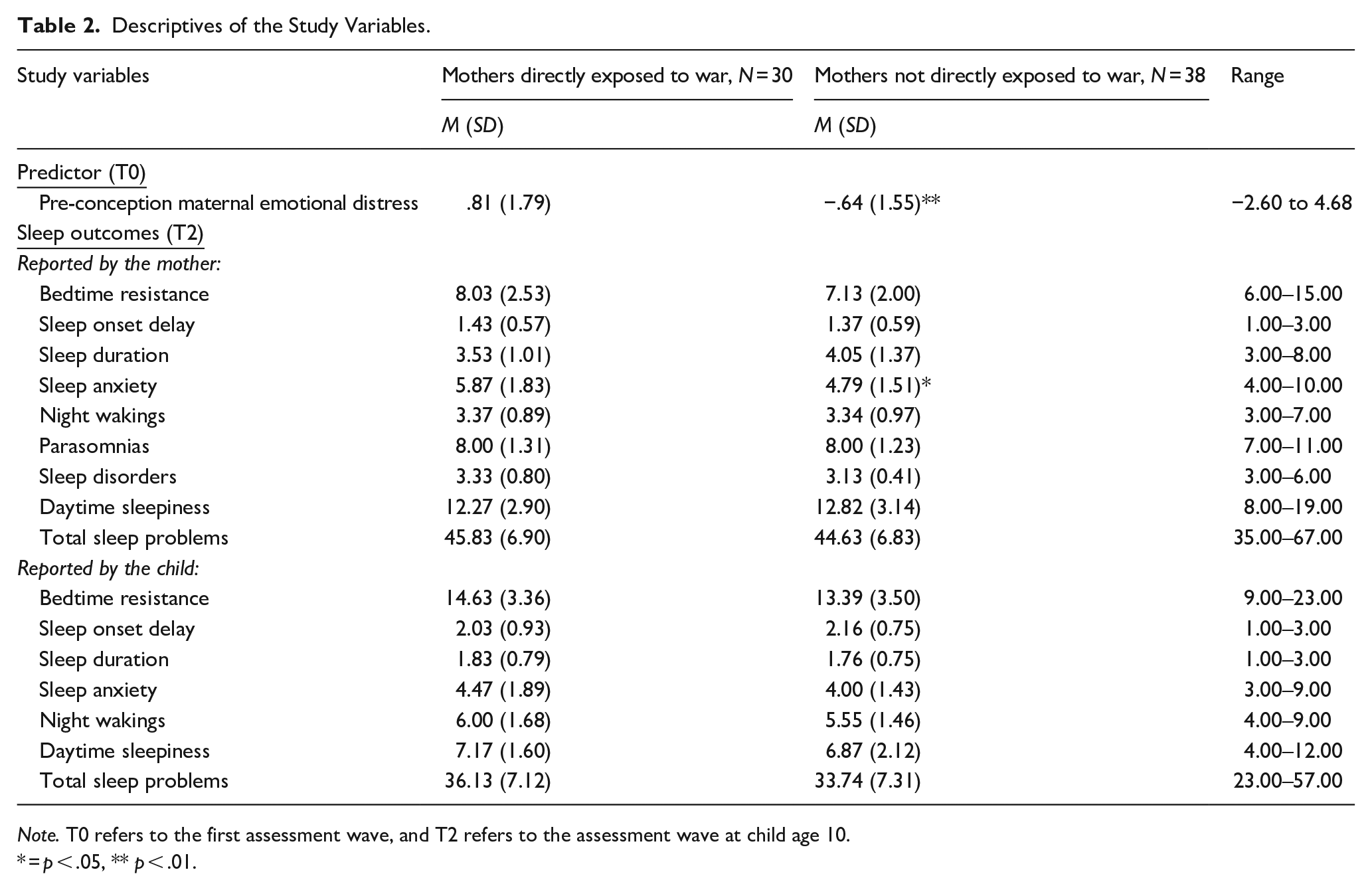
Note. T0 refers to the first assessment wave, and T2 refers to the assessment wave at child age 10.
= p < .05, ** p < .01.
Correlations Between Study Variables.
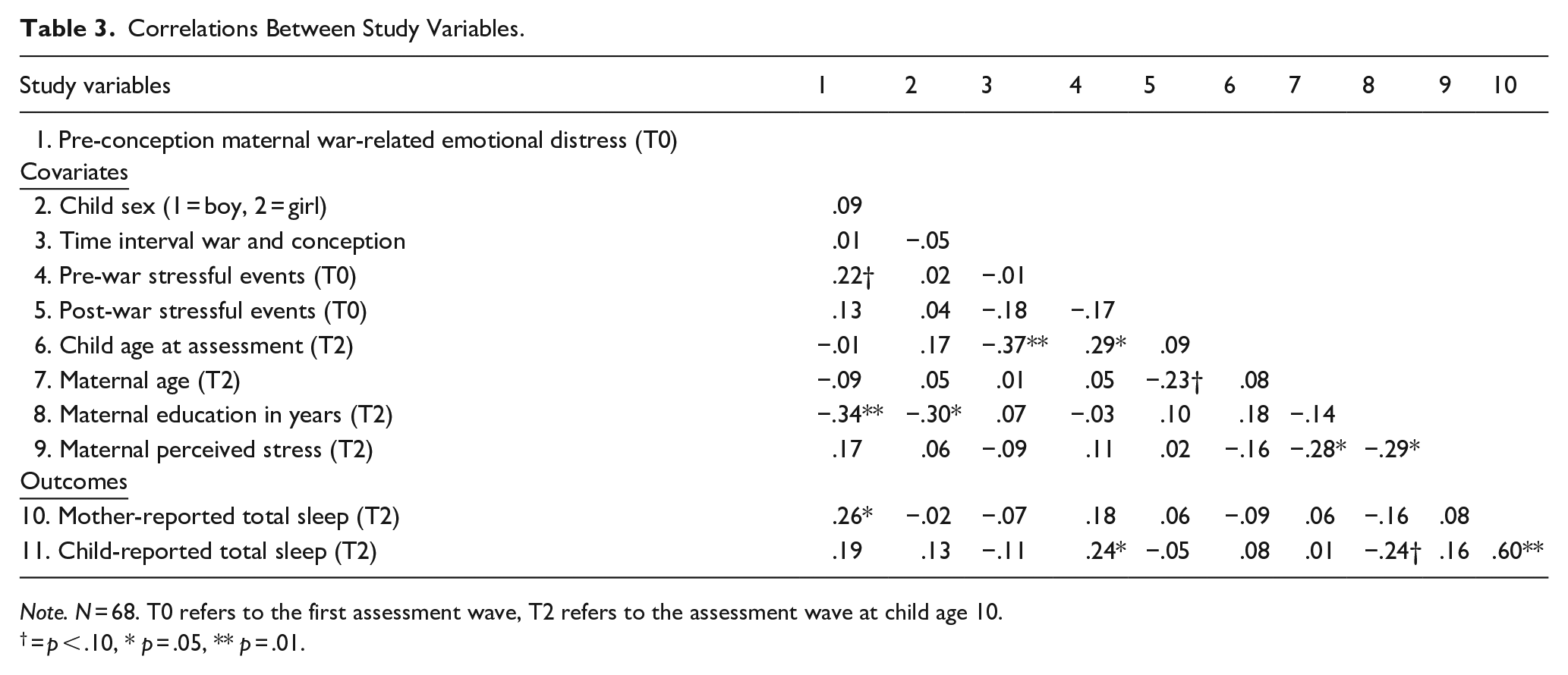
Note. N = 68. T0 refers to the first assessment wave, T2 refers to the assessment wave at child age 10.
= p < .10, * p = .05, ** p = .01.
Main Analyses
To test the longitudinal association between pre-conception war exposure measured at T0 and total child sleep problems at T2, while controlling for covariates and investigating a moderating effect of sex, two 2-way ANCOVAs were conducted: one for mother-reported total sleep problems, and the other for child-reported total sleep problems. Because maternal age and maternal education (T2) differed between the exposed and non-exposed group (see Table 1), these two variables were included as covariates. Results showed that mother-reported total child sleep did not differ between the war-exposed and non-exposed group, F(1, 62) = .029, p = .865, nor was there an interaction between war exposure and sex on mother-reported total child sleep, F(1, 62) = .090, p = .765. Similarly, groups did not differ significantly in child-reported total sleep, F(1, 62) = 1.320, p = .255, nor was there an interaction between war exposure and sex on child-reported total child sleep, F(1, 62) = .865, p = .356. Since no significant results on total sleep were found, group differences in scores on sleep subscales were not investigated.
To test the longitudinal association between maternal emotional distress during wartime as assessed at T0 and total child sleep problems as assessed at T2, while controlling for covariates and investigating a moderating effect of sex, we conducted two multiple hierarchical regressions: one for mother-reported total sleep problems, and the other for child-reported total sleep problems. Two covariates were included in these regression analyses: maternal years of education, and pre-war traumatic experiences, as these variables were significantly, or marginally, correlated with maternal emotional distress (see Table 3). Results from the regression analyses are presented in Table 4. While no main associations between maternal emotional distress and total child sleep were found, the interaction between maternal emotional distress and sex predicted significantly more mother-reported (β = .340, p = .045), and a trend for more child-reported (β = .277, p = .099) total sleep problems for daughters of mothers who experienced higher levels of emotional distress during wartime. This relation between maternal emotional distress and total sleep problems was not observed in boys.
Results of the Multiple Hierarchical Regression Analyses Predicting Child Sleep Outcomes.
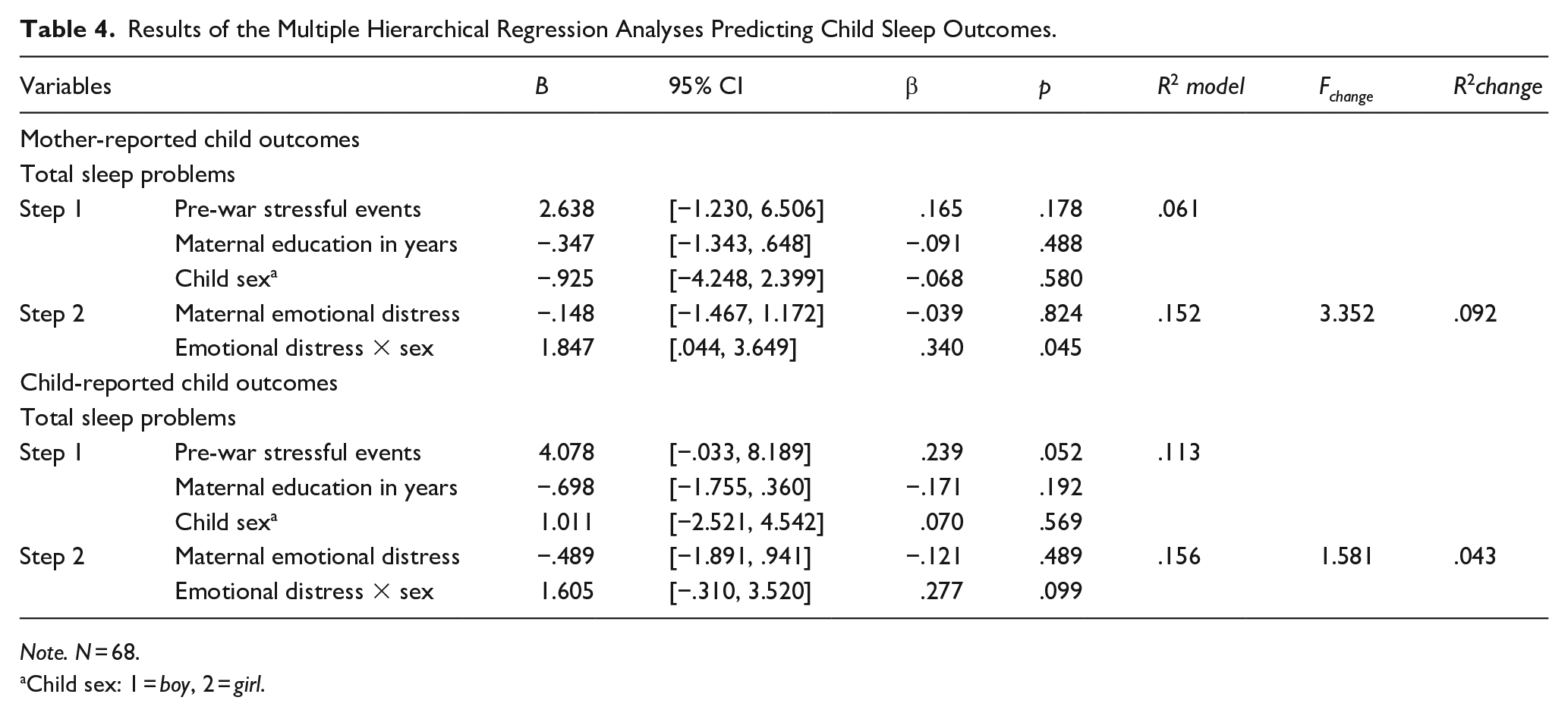
Note. N = 68.
Child sex: 1 = boy, 2 = girl.
The (marginally) significant interaction between maternal emotional distress and sex on total child sleep led to an exploratory investigation of the association between maternal emotional distress and its interaction with sex on scores on the sleep subscales. These analyses showed that daughters of mothers who experienced more emotional distress during wartime had significantly more mother-reported night wakings (β = .433, p = .010), parasomnias (β = .410, p = .013) and sleep-disordered breathing (β = .391, p = .021), and tended to more mother-reported bedtime resistance (β = .309, p = .068) and sleep anxiety (β = .283, p = .088). In addition, these girls also reported significantly more sleep anxiety (β = .387, p = .024). No other (marginally) significant effects were found. A complete overview of the results on all subscales can be found in Supplementary Table S1.
The inclusion of the interaction term between war exposure and emotional distress in the ANCOVA and multiple hierarchical regression analyses did not lead to any significant results.
Discussion
The aim of this study was to investigate the longitudinal relation between maternal pre-conception (1) war exposure and (2) war-related emotional distress on child sleep 10 years later. While we did not find evidence that exposure to war was associated with child sleep, higher levels of maternal emotional distress during the war predicted significantly more mother-reported, and marginally significantly more child-reported, sleep problems in children. Interestingly, these associations were observed only in girls, not in boys. Exploratory analyses revealed that in girls, these associations with maternal emotional distress showed in various sleep domains: night wakings, parasomnias, sleep-disordered breathing, sleep anxiety, and bedtime resistance.
Our study resonates and contributes to a new and growing body of research on the long-term developmental outcomes of pre-conception stress (Baird et al., 2009; Beijers et al., 2022; Dashorst et al., 2019; Keenan et al., 2018; Shachar-Dadon et al., 2017; Swales et al., 2022; Yehuda & Lehrner, 2018). Although the objective, contextual severity of prenatal and pre-conception stressors has previously been linked to transgenerational outcomes in humans (Class et al., 2013; Khashan et al., 2008; Lafortune et al., 2021) and animals (Bock et al., 2016; Franklin et al., 2010; Jenkins et al., 2022; Leshem & Schulkin, 2012; Shachar-Dadon et al., 2009; Zaidan et al., 2013), our study did not find evidence for a similar effect. Instead, our results are in line with previous studies on the same sample (Beijers et al., 2022; Shachar-Dadon et al., 2017), indicating that war exposure itself does not predict child outcomes, whereas maternal emotional distress during war exposure does. While these findings suggest that it is not the direct maternal exposure to a stressor, but rather the subjective experience of distress, that impacts the development of future generations, underscoring the importance of resilience to stress (Masten & Narayan, 2012), more research on both the objective hardship and psychological distress during war and disasters is clearly needed.
The sex-specificity of the current findings also corresponds with findings from earlier studies on pre-conception stress. A prior study on war-related pre-conception distress, for example, also reported effects solely in girls, but not boys (Beijers et al., 2022). However, it is not always the female sex that experiences the most consequences of pre-conception stress (Bock et al., 2016; Franklin et al., 2010; Jenkins et al., 2022; Zaidan et al., 2013). A study on pre-conception stress and ADHD, for example, found an increased risk for ADHD following maternal pre-conception stress exclusively in males (Li et al., 2010). Although pre-conception stress has repeatedly been found to affect development in a sex-specific manner, why and under which circumstances it might affect sexes differently is a question that remains to be answered. The answer to this question may lie (partly) in the underlying mechanisms explaining the associations between pre-conception stress and child developmental outcomes.
One mechanism that could explain the transgenerational effects is a spillover of pre-conception stress into the prenatal period. Because of the known stability of mental health problems (Kee et al., 2021), mothers who become stressed during the pre-conception period likely continue to feel so when they become pregnant. In turn, maternal prenatal stress is associated with long-term sleep problems in offspring (for a review, see Palagini and colleagues, 2015). Moreover, as the fetal adaptations to stress in the prenatal environment are known to vary according to fetal sex, for example, because the placenta functions in a sex-specific manner (Beijers et al., 2014), this mechanism might explain our sex-specific results associated with pre-conception stress.
Next to the spillover of maternal distress to the prenatal period, another mechanism associating pre-conception stress and child developmental outcomes is parenting. Several studies suggest that compromised mother–child interaction—(with possible different parenting of boys and girls)—could be responsible for the transgenerational effects of pre-conception and prenatal stress (Dashorst et al., 2019; Kaitz et al., 2009; Qouta et al., 2021; Shachar-Dadon et al., 2017). A prospective study on Palestinian mother–child dyads, for example, showed lower postpartum mental health in mothers who were exposed to traumatic war events while pregnant, which in turn was associated with lower mother–infant interaction quality (Qouta et al., 2021). Studies on a cohort of Israeli mothers exposed to war demonstrated lower levels of maternal sensitivity, reciprocity, and synchronicity in mother–child interactions compared to non-exposed controls (Feldman & Vengrober, 2011; Feldman et al., 2013; Halevi et al., 2017). Moreover, a prior study on the current cohort reported higher maternal separation anxiety and lower emotional availability at child age 3 in mothers who experienced greater pre-conception emotional distress during the war (Shachar-Dadon et al., 2017). In turn, compromised mother–child interaction is linked to compromised child development (Groh et al., 2017).
Other studies point to epigenetic alterations in the germline as a possible mechanism associating pre-conception stress and child development outcomes (Franklin et al., 2010; Yehuda & Lehrner, 2018; Zaidan et al., 2013). In the current study, such alterations would not necessarily be restricted to the maternal germline, but might also have taken place in the paternal germline, as fathers were exposed to the war and likely experienced war-related emotional distress as well. Interestingly, the sex-specific signatures following DNA demethylation in germ cells are currently being unraveled (Huang et al., 2021).
Due to the correlational nature of the study, alternative explanations that do not assume transgenerational effects of pre-conception stress cannot be excluded. Mothers who are more vulnerable to stress could, for example, be more alert to child sleep problems. However, several findings in our study make this explanation less likely, including the lack of association between maternal emotional distress during wartime and maternal perceived stress at T2 when child sleep was reported, the lack of association between maternal perceived stress at T2 and mother-reported child sleep problems, and the strong association between mother and child sleep reports.
It is also possible that stress-vulnerable mothers and children with disrupted sleep share a genetic make-up, for example in terms of personality or hyperarousal, which could explain both the maternal stress vulnerability and the child’s sleep problems. In fact, such an explanation pertaining to gene expression might also clarify the sex-specific findings found in our current study. For example, the study by Yamagata and colleagues (2016) examined the degree of association in corticolimbic circuitry, which has been implicated in mood regulation, between parents and offspring in 35 healthy families. The positive correlation of corticolimbic circuitry between mothers and daughters appeared to be significantly greater compared to other parent–offspring dyads, which suggests that the potential neuroanatomical basis of circuit-based transgenerational transmission patterns might be female-specific. Nevertheless, experimental animal studies do provide evidence of a causal transgenerational impact of pre-conception stress (Bock et al., 2016; Franklin et al., 2010; Jenkins et al., 2022; Leshem & Schulkin, 2012; Zaidan et al., 2013). Future research should elucidate the extent to which these various mechanisms can explain the current findings in humans.
This study has both strengths and limitations. A major strength is its quasi-experimental longitudinal design. The inclusion of both mother report and child report experiences of child sleep, which notably correlated strongly with each other, is also an important advantage, as together they create a more complete and less reporter-biased picture of long-term child sleep outcomes. A limitation concerns approximately a year’s delay between the war and the reports on war exposure and maternal emotional distress, which may have introduced recall bias. Another limitation is the sample size. As the power analyses indicated, we were able to detect medium-sized effects, meaning that small effects may have gone undetected. This could possibly explain the lack of a direct effect of war exposure on child sleep, as well as other null findings. Moreover, limited study power implies that the domain-specific findings from the multiple exploratory analyses should be interpreted with caution.
To conclude, this study adds to the growing body of research that marks the pre-conception period as a formative period in the life of a child. As war exposure per se was not predictive, whereas maternal emotional distress during wartime was predictive of child sleep problems, even after controlling for maternal pre-war stressful events, post-war stressful events prior to childbirth (including pregnancy), and current perceived stress, the outcomes of this study suggest that interventions aimed at decreasing maternal distress and increasing maternal resilience during the pre-conception period might benefit both mother and child, as animal findings also suggest (Zaidan et al., 2018). In designing such interventions, one should take into account that maternal education could be among the moderators of the link between maternal stress and child outcomes (see Table 3). Future studies investigating such interventions should be valuable to unravel causality and aid our understanding. Moreover, they would be an important step in the mitigation of war-related adverse developmental child outcomes in a world in which war unfortunately is a reality for many.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254231215063 – Supplemental material for War exposure prior to conception: Longitudinal associations between maternal emotional distress and child sleep 10 years later
Supplemental material, sj-docx-1-jbd-10.1177_01650254231215063 for War exposure prior to conception: Longitudinal associations between maternal emotional distress and child sleep 10 years later by Emma Bolhuis, Anat Scher, Hanit Ohana, Rotem Ad-Epsztein, Micah Leshem and Roseriet Beijers in International Journal of Behavioral Development
Footnotes
Acknowledgements
The authors would like to thank all families for their participation, and Sandra Zukerman for data management.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Netherlands Organization for Scientific Research VENI grant (016.195.197-to Beijers), an Early Career Award and a Sara van Dam Project Grant of the Royal Netherlands Academy of Arts and Sciences (to Beijers), and the Israel–U.S. Binational Foundation Grant (2005383-to Leshem). The funding bodies had no role in the design of the study, in the collection, analysis, and interpretation of the data, in the writing of the manuscript, and in the decision to submit the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.