
Abstract
Parental incarceration (PI) is negatively associated with emotional, educational, and psychological child outcomes. However, few studies explore potential mechanisms through which these outcomes are transmitted or the means by which prosocial outcomes might develop. This study used data from two waves of a population cohort study of children aged 9 years and followed up aged 13 years living in Ireland. Children and parents (N = 8,568) completed measures of PI, primary caregiver (PCG) depression, PCG-child relationship quality, and child behavioral adjustment. We then conducted a secondary analysis on this national longitudinal study of children in Ireland. Using sequential mediation models, we observed a mediated indirect effect of PI on prosocial outcomes via PCG depression and PCG-child relationship quality. PI at age 9 was associated with increased difficulties and reduced prosocial behavior at age 13. Additionally, PI at age 9 affected PCG depression and the PCG-child relationship quality. Additionally, child prosocial outcomes, and emotional and behavioral difficulties were less apparent where PI had a weaker effect on PCG depression and the quality of PCG-child relationship. Supports that can mitigate the impact of PI for vulnerable caregivers and children are discussed.
Growing up in a home affected by parental incarceration (PI) is associated with increased vulnerability for children across social, educational, and psychological domains (Murray et al., 2012). This association is particularly important in light of increases in prison populations (Wildeman, 2009), estimated to be over 11 million people worldwide (International Centre for Prison Studies, 2013). While research has demonstrated the detrimental child outcomes associated with PI, such as lower academic achievement, anti-social behavior, and poorer psychological well-being (Murray et al., 2012), the mechanisms through which PI affects developmental outcomes are poorly understood (Murray & Farrington, 2008). Additionally, research that explores the associations between PI and prosocial outcomes, such as volunteering or providing comfort, support or kindness to others, has remained largely absent (Haskins, 2015). We address these gaps first by evaluating the impact of PI on both child prosocial outcomes and emotional and behavioral difficulties in a nationally representative longitudinal cohort study, and second, by considering two possible mechanisms that may influence the PI-child outcome associations, namely primary caregiver (PCG) depression and the quality of the PCG-child relationship.
Existing research on the impact of PI for children reveals mixed results. Murray and colleagues (2012) found that PI had a negative consequence on children’s educational, behavioral, and emotional outcomes, while others report null or even positive effects (Turanovic et al., 2012; Wildeman & Turney, 2014). Greater attention to the impact of PI on family systems may clarify the contexts in which PI leads to adverse child outcomes. Indeed, little research has attended to the impact of the other family members such as the partners of those incarcerated on child outcomes (Miller et al., 2013). The dearth in research is surprising given the emphasis within developmental psychology on the importance of family systems and relationships. PI by definition disrupts the caregiving environment for children (Poehlmann, 2010); however, it also comprises a stressor for the remaining parent. Thus, we propose that PI may confer an elevated risk of depression for the non-incarcerated parent. This in turn influences parent–child relationship quality, which in turn influences child outcomes (see Figure 1).

Proposed Serial Mediation Model of the Effect of Time 1 Parental Incarceration on Time 2 Strength and Difficulty Questionnaire Through Changes in Primary Caregiver Depression and Primary Caregiver–Child Relationship Quality (N = 8,618).
PI and PCG Depression
Unsurprisingly, PCGs of children impacted by PI are under particular strain and are at increased risk of physical and mental health difficulties (Chui, 2016). Arditti (2012) observed increased levels of stress in those caring for dependent children while also supporting an imprisoned partner. In a qualitative study, PCGs described isolation and disconnection from their own communities, and sometimes even their own families, because of the negative connotations associated with imprisonment (Bradshaw & Muldoon, 2019). PI has been associated with an increased risk of depression among the PCGs of children affected (Chui, 2016; Turanovic et al., 2012). Despite these potential adverse impacts, few studies have considered the potential disruption of one parent’s imprisonment on the remaining parent’s capacity to parent and the associated cost to children in their care.
One way in which PI may affect children is via disrupted caregiver–child relationships. PCG depression can undermine PCG-child relationships (Coyl et al., 2002). Previous research highlights how parental responsivity and sensitivity to a child’s needs enhance positive PCG-child relationships (Bakermans-Kranenburg et al., 2003). Naturally, due to their confinement, imprisoned parents are restricted from engaging in day-to-day activities with their children. Equally, contextual stressors such as imprisonment of a partner may influence the PCGs well-being. For example, Richter (2004) argues that PCG depression can undermine PCGs’ capacity to give proper care and attention to their children, the effects of which can have lasting influences on future disruptive adolescent behaviors. Consequently, we hypothesize that the adverse impact of PI on the remaining parent may reduce their ability to optimally parent children already made vulnerable by PI.
The Present Study
We use a national longitudinal cohort study to examine the impact of PI at age 9 on prosocial and emotional and behavioral outcomes in children at age 13 years old. Further, we focus on PCG depression and PCG-child relationship quality as potential mediators of associations between PI and child outcomes. The longitudinal design allows us to control for the effects of Time 1 (T1) measures of each of our attributes of interest, namely PCG depression, PCG-child relationship quality, prosocial, and emotional and behavioral outcomes at Time 2 (T2), allowing us to consider the unique effect of PI.
Importantly, children affected by PI are at increased risk of experiencing multiple social and economic stressors (Bradshaw et al., 2020). Gender differences in children’s social and emotional development are well-established (e.g., Farrington et al., 2012); besides this, household socioeconomic status (SES), stressful life events (SLEs) (Kjellstrand et al., 2020), PCG age, and PCG level of education (Pogarsky et al., 2006) can all have negative consequences for children’s emotional and behavioral development. Arditti (2012) maintains that this context of social inequality may exacerbate negative outcomes for families affected by PI. Therefore, in addition to demographic control variables (gender of the child, SES, PCG education, PCG age), we control for number of SLEs other than PI, as a measure of this wider risk environment. In summary, we test the hypothesis that there is a relationship between experience of PI by age 9 and child outcomes at age 13, which is serially mediated by PCG depression and PCG-child relationship quality. We test this for prosocial outcomes as well as for emotional and behavioral difficulties.
Method
Participants and Procedure
This study used data from the first two waves of the Growing Up in Ireland National Longitudinal Study of Children (GUI), a nationally representative cohort study of children living in the Republic of Ireland which commenced in 2007/2008 when the children were aged 9 (T1) and aged 13 (T2). A representative sample of 910 primary schools (82% response rate) agreed to participate; from these, 15,000 families were randomly selected and 8,568 (57%) agreed to participate. The second study wave was carried out in 2011/2012 (Wave 2) when the children were aged 13 with an 87% follow-up rate (n = 7,423). Data collection for children and PCGs was performed at each family’s residence by trained interviewers. Informed consent was obtained from all participants. GUI was subject to ethical review by the Irish Health Research Board’s Research Ethics Committee.
Measures
Control variables
Socio-demographical information was reported by the PCG and included age, gender, and highest level of education (primary, secondary, tertiary) of the PCG, whether the PCG was the biological parent of the child, and the percentage of the household’s income (<50%, ≥50%) derived from social welfare payments.
Stressful life events
All PCGs indicated whether the study child had ever experienced 12 potentially stressful events (e.g., “Has the study child experienced drugs in the immediate family” yes/no). Individual items were summed to create a total SLEs score.
Predictor variable
Parental incarceration was measured at T1 by a single item. All PCGs indicated whether the study child had ever experienced PI, by answering yes or no to the question “Has the child ever experienced a parent in prison?”.
Mediators
PCG depression was measured at both waves using an 8-item self-report version of the Center of Epidemiological Studies Depression Scale (CES-D) (Roberts & Vernon, 1983). The CES-D was developed as a screening instrument for use in the general population. Items are summed to yield a total score (e.g., “I felt everything I did was an effort”). Lower scores indicate lower symptoms (GUI, 2010). Cronbach’s α was .87 (Nixon, 2012).
Child-PCG relationship was measured using the Pianta Child-Parent Relationship Scale (Pianta, 1992) at T1 and T2. This is a 10-item scale assessing PCGs perceptions of their relationship with their child (e.g., “I share an affectionate, warm relationship with my child”). Items are rated on 5-point Likert-type scales and summed into a total score. Higher scores indicate higher relationship quality. If a participant did not answer more than one question belonging to a subscale, they did not get a score for that subscale. Cronbach’s α was .75 (Thornton et al., 2016).
Outcome variables
Prosocial behavior was measured using the prosocial behavior subscale of the Strengths and Difficulties Questionnaire (SDQ) (Goodman et al., 1998). The SDQ is a 25-item behavioral screening questionnaire administered to children’s PCG. This was completed by PCGs at both T1 and T2. The prosocial behavior subscale contains five items summed to give a total score (e.g., “My child is kind to younger children”). Responses to each item were measured on a Likert-type scale ranging from 0 (not true) to 2 (certainly true). Cronbach’s α for prosocial behavior was .63 (Nixon, 2012).
Emotional and behavioral difficulties were measured using the difficulties subscales of the SDQ as above. The SDQ total difficulties score is calculated using the sum of the four “difficulties” subscales, with higher scores indicating more emotional and behavior problems (e.g., “My child is often unhappy, down-hearted or tearful”). If any of the four sub-scores is missing (because fewer than 3 of the 5 subscale items are completed), then the total difficulties score is counted as missing. As recommended by scale developers, prosocial behavior was not included in the total score as the absence of prosocial behaviors is conceptually different to the presence of psychological difficulties (Goodman et al., 1998). Cronbach’s α for total difficulties was .79 (Nixon, 2012).
Analytic Approach
Means for independent, mediator, and dependent variables were compared across PI and non-PI groups using independent samples t-tests. Simple correlations were conducted for all variables at T1 and T2. We also examined associations between the variables across time while controlling for the independent effects of child gender and parental educational level and other SLEs using partial correlations (see Table 1). We tested our main hypotheses using a conditional process modeling program, PROCESS, to test for both direct and indirect effects (Hayes, 2012) using Model 6 for serial mediation. As such, in two separate models we tested for the direct effect of PI at T1 on prosocial behavior and emotional and behavioral difficulties at T2 in and for indirect effects via PCG depression and the child-PCG relationships. In both models, we controlled for the effect of T1 measures of mediator and outcome variables, so that we could examine the unique effect of PI. To establish the robustness of our model, we subsequently conducted our analysis controlling for PCG level of education, single parent household, household social welfare dependency, SLEs, and gender of study child.
Parental Incarceration vs. Non-Parental Incarceration Group Differences on Predictor, Mediator, and Outcome Variables.
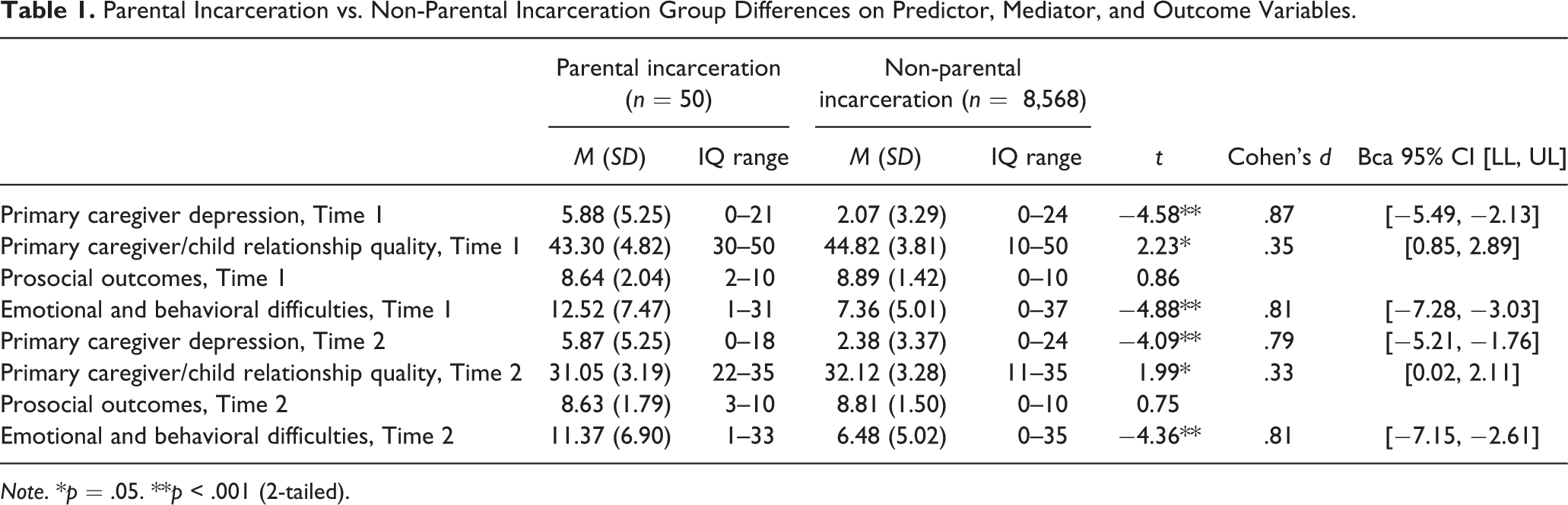
Note. *p = .05. **p < .001 (2-tailed).
Results
PCGs reported that PI had affected 50 children (0.9%) by the age of 9. Results also indicate that 51% of children were female and were cared for by female PCGs (98%), who were biological parents (98%) with an average age of 39 years. PCGs caring for children affected by PI reported higher mean levels of depression, and emotional and behavioral difficulties as well as lower levels of PCG/child relationship quality than those in the non-PI group at T1 and T2. There was no significant difference in prosocial behavior between groups (see Table 1). No information was available regarding gender of the incarcerated parent or previous living arrangements of the child.
PI, Depression, PCG-Child Relationship and Child Outcomes
PI was negatively associated with PCG-child relationship quality at T1 and T2. PI was positively associated with PCG depression T1 and T2, and with SDQ difficulties at T1 and T2. PI was not associated with child prosocial behavior at either time point.
Correlations also indicated that PCG depression T1 was significantly associated with PCG depression T2; PCG-child relationship T1 and T2; prosocial behavior T1 and T2; and SDQ difficulties T1 and T2. PCG-child relationship T1 was significantly associated with for PCG-child relationship T2, prosocial behavior T1 and T2, and SDQ difficulties T1 and T2. Partial correlations indicated that associations held when accounting for control variables (see Table 2).
Descriptive Statistics and Correlations.

Note. N = 8,618.
^Indicates a count rather than a mean value.
#Control variables included partner in the house, study child gender, stressful life events, PCG age, PCG education, and % of income derived from social welfare.
*p = .05 level (2-tailed). **p < .001 level (2-tailed).
Predicting Prosocial Behavior
PI had no direct observable effect on prosocial outcomes at T2. However, supporting our first hypothesis, there was evidence of a significant sequentially mediated indirect effect (b = −.02, SE = .01; 95% CI: −.05: −.003) with experience of PI associated with increased levels of PCG depression (b = 1.93; 95% CI: .74, 3.12), which in turn was associated with poorer PCG-child relationship (b = −.08; 95% CI: −.11, −.06), which in turn was associated with lower prosocial behavior (b = .25; 95% CI: .14, .16). These effects were observed controlling for both T1 measures of these attributes and confounding variables (see Figure 2).

Serial Mediation Model of the Effect of Time 1 PI on Time 2 Prosocial Behavior Through Changes in PCG Depression and PCG-Child Relationship Quality. Unstandardized Coefficients β are Presented. *p = .05 level. **p < .001. (N = 6,616).
Predicting Emotional and Behavioral Difficulties
We also found the corollary was true in relation to emotional and behavioral difficulties (b = .04, SE = .02; 95% CI: .004: .09). PI had no direct observable effect on emotional and behavioral difficulties at age 13 when controlling for confounding variables. In contrast to prosocial outcomes, PCG depression was associated with increased levels of emotional and behavioral difficulties (b = .17, 95% CI: .15, .21). Additionally, experience of PI associated with increased levels of PCG depression (b = 1.87; 95% CI: .69, 3.05), which in turn was associated with poorer PCG-child relationship (b = −.08; 95% CI: −.10, −.05), which in turn was associated with higher total emotional and behavioral difficulties (b = −.30; 95% CI: −.33, −.27). These effects were apparent when controlling for T1 levels of these attributes and confounding variables (see Figure 3).

Serial Mediation Model of the Effect of Time 1 PI on Time 2 Emotional and Behavioral Difficulties Through Changes in PCG Depression and PCG-Child Relationship Quality. Unstandardized Coefficients β are Presented. *P = .05 level. **P < .001 level. (N = 6,597).
Discussion
Our hypothesis that the relationship between experience of PI at age 9 and prosocial and emotional and behavioral outcomes for children aged 13 is mediated by PCG depression and the quality of the PCG-child relationship was supported. Indeed, children who had experienced PI by the age of 9 had higher levels of emotional and behavioral difficulties at age 9 and 13. PI had no direct observable effect on prosocial outcomes at age 13. It is worth noting in the context of concerns around intergenerational transmission of criminality, that children affected by PI do not have significantly lower levels of prosocial behavior than those who have not experienced PI.
The effects of PI on children’s development appear to be driven, at least in part, by its impact on the child’s PCG. PI has an effect on PCG depression and the quality of the PCG-child relationship. PI can be seen to create a risky context that makes PCGs vulnerable, which in turn has an adverse effect on their ability to manage their relationship with their child. In this way, it shapes development across middle childhood. These associations have consequences for both prosocial development and emotional and behavioral development. Our findings are consistent with previous research showing that PCG-child relationships mediate associations between maternal distress and child socio-emotional development in infancy (Mason et al., 2011) and in middle childhood (Dubois-Comtois et al., 2013). Taken together, these results emphasize the importance of supporting PCGs in order to protect the emotional and behavioral development of children affected by PI.
Studies examining positive outcomes, though fewer in number (Wang & Dix, 2015), also report that mothers’ responsiveness to their children mediates the association between maternal depression and children’s social competence. Our findings are comparable; poorer PCG mental health impacts child–caregiver relationship, which in turn affects our measure of prosocial outcomes. Stigma and depression of PCG could have a marked effect on prosocial development of this very at-risk group. Indeed, previous work highlights the impact of stigma on women and families affected by incarceration. Future research could usefully consider stigma as an antecedent of PCG well-being in order to understand this process more fully. Turanovic and colleagues (2012) suggest that stigma places caregivers’ well-being at risk with consequent impact on children.
Turanovich and colleagues (2012) identify that the size and quality of the PCGs support network can mitigate potentially negative outcomes and offer possible avenues for future research. Our findings suggest that PCG depression may be an especially valuable target for intervention in families affected by PI. Supporting PCG well-being is likely to support children negatively impacted as a consequence of PI. Therefore, families characterized by PI, and PCGs of children in particular, warrant additional supports as they negotiate their unique challenges (McLaughlin et al., 2016). However, well-being and the PCG-child relationship have been identified in other studies as moderators of individuals’ engagement with family systems-focused interventions, and thus, it may be important to think of them as moderators of intervention effects. For instance, Berlin et al. (2011) observed that associations between depression and engagement in early intervention programs might be attributable to the varying degrees of risk that characterize program participants. Therefore, examining the impact of PCG depression and PCG-child relationship quality on engagement with interventions to support families affected by PI is a worthwhile endeavor.
Several strengths of this study are noted. First, we use a population-based, longitudinal study to demonstrate the effects of PI across time. Our study was conducted in Ireland, where levels of incarceration are low relative to many other countries (International Center for Prison Studies, 2013). Thus, supports for families affected by PI may be less established, exacerbating the PI-related stigma (Murray et al., 2014). For example, a cross-national comparison study (Mulready-Jones, 2011) concluded that children with incarcerated parents in Sweden benefit from number and effectiveness of support services available. This rehabilitative approach may buffer against potential harm caused by stigma (Murray et al., 2014). Finally, we controlled for additional adversities experienced by children that are also implicated in maladaptive outcomes. Children affected by incarceration tend to differ from those not so affected on a number of risk-related variables other than PI status (Johnson & Easterling, 2012). The inclusion of comprehensive measures of cumulative stress in the GUI alongside the large population sample meant we could undertake meaningful controls for the effects of cumulative adversity. Finally, our study evaluated both prosocial behavior, and socio-emotional and behavioral difficulties within the same sample.
Some limitations are noted. First, few longitudinal data sets are designed to address the specific needs of families affected by PI (Ahalt et al., 2012). A relatively small proportion of the GUI sample had experienced PI which may limit the generalizability of study findings. However, this is representative of the low proportion of the population incarcerated in Ireland relative to other Western countries such as the U.S. Second, although the longitudinal study design facilitates evaluation of mediators of relationship between PI and children’s outcomes, causality cannot be established. Importantly, PI is a precursor to the first measurement of PCG depression available in GUI; therefore, it is possible that PI has already influenced the onset of depression before T1 measurement. Third, detailed information relating to PI (e.g., the duration of or frequency of separate instances of PI, of gender of the incarcerated parent) was not collected. Lastly, all variables are assessed using PCG reports and are liable to reporter bias that potentially inflates associations among variables.
Nonetheless, this study usefully identifies parental depression and its link with PCG-child relationship as a mechanism underlying the impact of PI on prosocial behavior, as well as emotional and behavioral problems. Interventions targeting these factors, particularly PCG depression, may lessen the adverse impact of PI on at-risk families.