
Abstract
Peer sexual harassment (PSH) occurs frequently and across contexts during adolescence. The current study examined the relations among PSH in school, psychological distress, sexual experimentation, and sexual risk-taking in a sample of African American middle and high school girls. Results indicate that negative body appraisals mediated the relationship between PSH and psychological distress, suggesting that PSH is one way to operationalize interpersonal sexualization and sexual objectification. PSH was directly associated with sexual experimentation, but the association between PSH and sexual experimentation was not mediated by negative body appraisals. Neither PSH nor negative body appraisals were related to sexual risk-taking. This suggests that frequent exposure to high levels of sexualization and sexual objectification, in the form of PSH, is associated with more psychological distress and sexual experimentation, but not with sexual risk-taking, regardless of how girls feel about their bodies.
The healthy development of adolescent girls includes overcoming any number of challenges; among the challenges adolescents report they must navigate are sexualization, sexual harassment, violence, pregnancy, and negotiating their emerging sexuality (Nicolas & Whitt, 2013), and for girls of color, these challenges take place in a context nuanced by racial and ethnic identity. Peer sexual harassment (PSH), which occurs frequently and across contexts, is particularly likely to be encountered at school during adolescence (Hill & Kearl, 2011). In this study, we examine PSH as a form of interpersonal sexualization (Petersen & Hyde, 2013a, 2013b) with a sample of African American middle and high school students and its associations with psychological distress, sexual experimentation, and sexual risk-taking, as well as the mediating effects of negative body appraisals in these links.
The Sexualization of Girls and Women
Sexualization occurs when someone’s value is derived from their sexual appeal, when physical attractiveness is equated with sexiness, when someone is objectified, and/or when sexuality is imposed on someone inappropriately (American Psychological Association [APA], Task Force on the Sexualization of Girls, 2007). Sexualization can occur within three spheres: societal, interpersonal, and personal/self (APA, Task Force on the Sexualization of Girls, 2007). In the societal sphere, many Western cultures are inundated with images suggesting that the value of women is derived from their sexuality. A large body of research spanning decades has demonstrated the pervasiveness of media depictions of women and girls in a sexualized manner (e.g., Frisby & Aubrey, 2012; Ward, Seabrook, Manago, & Reed, 2016), and recent research suggests that exposure to sexualized images of women and girls is associated with gender harassment and activating harassment-related norms (Galdi, Maass, & Cadinu, 2014). Adolescents and young adults engage with media more than any other daily activity (Coyne, Padilla-Walker, & Howard, 2013), leading to high levels of exposure to sexualized images. Objectification Theory (Fredrickson & Roberts, 1997; Moradi & Huang, 2008) posited that exposure to sexualized images leads women to internalize these cultural body ideals, leading to self-objectification, which in turn leads to distortions in body image.
In the interpersonal sphere, girls and women may be treated as sexual objects in interactions with family, peers, and others (Fredrickson & Roberts, 1997), especially in the form of body evaluation, appearance remarks, unwanted sexual attention, and other forms of sexual harassment (Kozee, Tylka, Augustus-Horvath, & Denchik, 2007; Petersen & Hyde, 2013b). The subtle and not-so-subtle evaluation of women’s bodies by others (both men and women; Gurung & Chrouser, 2007) is epitomized by the “objectifying gaze,” defined as visually inspecting or staring at another’s body, dwelling on sexual body parts rather than faces (Gervais, Holland, & Dodd, 2013). Cultural body ideals are internalized when individuals adopt societal standards and engage in body surveillance comparing to the ideal (Kozee et al., 2007). Women’s exposure to the objectifying gaze is associated with increased body surveillance and internalized thinness ideals (Kozee et al., 2007, but see Gervais, Vescio, & Allen, 2011 for an exception), decreased cognitive performance (Gervais et al., 2011), and increased self-silencing (Saguy, Quinn, Dovidio, & Pratto, 2010). Fredrickson and Roberts (1997) noted the objectifying gaze is pervasive, but often underestimated, and a key contributing factor to PSH and unwanted sexual advances.
In the self or personal sphere, some girls internalize the objectifying messages that they receive and respond with heightened self-consciousness characterized by persistent monitoring of their appearance, or self-objectification, which, in turn, is related to greater depression, body shame, appearance anxiety, and disordered eating (Buchanan, Bluestein, Nappa, Woods, & Depatie, 2013; Grabe, Hyde, & Lindberg, 2007; Jones & Griffiths, 2015; Slater & Tiggeman, 2010). In the context of sexualization, this self-objectification can take the form of sexual self-objectification. For example, in girls as young as 6–9 years old, exposure to sexualized media was associated with the internalization of sexualization messages, operationalized as the desire for sexier clothing (Slater & Tiggeman, 2016). Petersen and Hyde (2013a) argued that sexual harassment as a type of sexual objectification may lead to increased self-surveillance and focus on attaining the ideal physical appearance in an effort to reduce unwanted sexual attention. Further, sexual violence is associated with self-objectification and body shame (Davidson & Gervais, 2015; Holmes & Johnson, 2017), which suggests that the internalization of sexualization may be associated with sexual behavior and sexual dysfunction.
PSH in School
According to the U.S. Department of Education, Office of Civil Rights (2001), “Sexual harassment is unwelcome conduct of a sexual nature. Sexual harassment can include unwelcome sexual advances, requests for sexual favors, and other verbal, nonverbal, or physical conduct of a sexual nature.” Behavioral dimensions of sexual harassment include gender harassment (verbal and nonverbal behaviors that convey hostility and degrading attitudes based on gender), unwanted sexual attention (unwanted and unreciprocated verbal and nonverbal sexual behavior), and sexual coercion (promise of positive or threat of negative outcomes in exchange for sexual cooperation; Fitzgerald, Gelfand, & Drasgow, 1995; Ormerod, Collinsworth, & Perry, 2008). Experiences of PSH are commonplace for middle and high school students (e.g., Espelage, Hong, Rinehart, & Doshi, 2016; Gruber & Fineran, 2016; Petersen & Hyde, 2009). A national survey of middle and high school students concluded that 88% of girls had experienced PSH during their school career (American Association of University Women [AAUW], 2001). The most common forms of PSH include making sexual comments, jokes, gestures, or looks, and touching, grabbing, or pinching in a sexual way (AAUW, 2001; Espelage et al., 2016; Hill & Kearl, 2011; Petersen & Hyde, 2009). Although both girls and boys are victims of harassment, girls experience higher frequency and more severe harassment than boys and tend to be more upset by harassment (Espelage et al., 2016; Hill & Kearl, 2011; Ormerod et al., 2008; Sagrestano, 2009; Schnoll, Connolly, Josephson, Pepler, & Simkins-Strong, 2015).
Research examining PSH among adolescents of color is limited. However, there is some indication that African American girls are more likely than their White and Latina counterparts to experience physical forms of PSH (AAUW, 2001; Clear et al., 2014; Espelage et al., 2016). African American girls may be more vulnerable to sexual harassment than other groups because of hypersexualized stereotypes. Additionally, harassment based on sex intersects with harassment based on other identities, such as race/ethnicity, putting girls and women with multiple stigmatized identities at higher risk (Buchanan, Bergman, Bruce, Woods, & Lichty, 2009; Buchanan & West, 2010; Fitzgerald & Cortina, 2018). African American girls may be particularly vulnerable to harassment at school because defending oneself from harassing behavior may carry disproportionate risks of exclusionary and punitive discipline by school or criminal justice authorities (Crenshaw, Ocen, & Nanda, 2015). That is, the harassment of African American girls may be especially likely because perpetrators are less likely to be detected and/or punished than if higher status group members were targeted.
A variety of negative psychological consequences have been linked to PSH, including embarrassment, low self-confidence, low self-esteem, depression, fear, anxiety, and doubt about whether one can have a happy romantic relationship (AAUW, 2001; Bucchianeri, Eisenberg, Wall, Piran, & Neumark-Sztainer, 2014; Dahlqvist, Landstedt, Young, & Gådin, 2016; Lindberg, Grabe, & Hyde, 2007; Ormerod et al., 2008). Educational consequences of PSH include difficulty studying, lack of concentration, lack of attention in the classroom, lower grades and academic self-esteem, feeling unsafe at school, school withdrawal, and increased avoidance behaviors (AAUW, 2001; Gruber & Fineran, 2016; Ormerod et al., 2008).
Developmental Trajectory of PSH and Sexual Behavior
PSH begins early, often before middle school, increases throughout middle school and high school, and then drops off in college (AAUW, 2001; Goldstein, Malanchuk, Davis-Kean, & Eccles, 2007; Petersen & Hyde, 2009). Although most existing data are cross-sectional, longitudinal studies also suggest that harassment increases from the middle school to high school years (Pellegrini, 2001; Petersen & Hyde, 2009, 2013a, 2013b). Some have argued that pubertal changes lead to increased interest in sexuality, and PSH is a clumsy attempt at expressing attraction for others (e.g., Pellegrini, 2001; Petersen & Hyde, 2009, 2013b). Indeed, girls with more advanced pubertal development report greater likelihood of being harassed than less developed girls (Goldstein et al., 2007; Petersen & Hyde, 2009; Skoog & Özdemir, 2016). However, few perpetrators indicate that their harassing behavior was an attempt to get a date or start a relationship (Hill & Kearl, 2011). It is also possible that early maturing girls experience increased harassment resulting from being sexually active, as early onset of puberty is also associated with earlier sexual debut (Skoog, Stattin, Ruiselova, & Özdemir, 2013), and earlier debut is associated with more partners over time. Further, early and frequent dating behavior is associated with experiencing PSH (Chiodo, Wolfe, Crooks, Hughes, & Jaffe, 2009; Mitchell, Ybarra, & Korchmaros, 2014). However, a recent study concluded that harassment of early maturing girls stemmed from their mature appearance, rather than from being sexually active (Skoog & Özdemir, 2016).
Developing a sense of sexual well-being is a normative part of adolescence. As youth mature, they typically initiate romantic relationships, which allow opportunities to develop healthy relationship skills. Indeed, healthy sexual development (i.e., healthy emotional, physical, attitudinal, and social well-being related to sexuality) is associated with positive social and mental health outcomes (Hensel, Nance, & Fortenberry, 2016; Tharp et al., 2013). Sexual experimentation is a natural part of this developmental trajectory and, when it is consensual and respectful, can be associated with positive psychological health. Nonetheless, certain aspects of adolescent sexual behavior put them at risk for sexually transmitted infections, unintended pregnancy, and other undesirable outcomes (Halpern, 2010; Harden, 2014). A healthy sexuality approach suggests that sexual experimentation is a separate construct from sexual risk-taking, with different antecedents and consequences. Although the links among PSH, sexual experimentation, and sexual risk-taking have only recently begun to be examined, a recent Finish study found that PSH was associated with more advanced sexual experiences and risk-taking behavior (e.g., more partners; Kaltiala-Heino, Savioja, Fröjd, & Marttunen, 2018). Additional research is needed to better understand how these constructs are related to each other and to mental health outcomes.
Current Study
We examined the relation between PSH in school and (a) psychological distress, (b) sexual experimentation, and (c) sexual risk-taking among African American middle and high school girls. Additionally, we examined whether negative body appraisals mediate the relation between PSH and these three outcomes. Specially, we tested three mediation models. In the first test of mediation, we hypothesized that interpersonal objectification (operationalized as PSH) would be related to psychological distress, both directly and indirectly through negative body appraisals. In the second test of mediation, we hypothesized that PSH would be related to greater sexual experimentation, both directly and indirectly through negative body appraisals. In the third test of mediation, we hypothesized that PSH would be related to great sexual risk-taking, both directly and indirectly through negative body appraisals. Our hypothesized models are presented in Figure 1. Age was considered as a covariate in all models because of the developmental nature of our variables of interest.
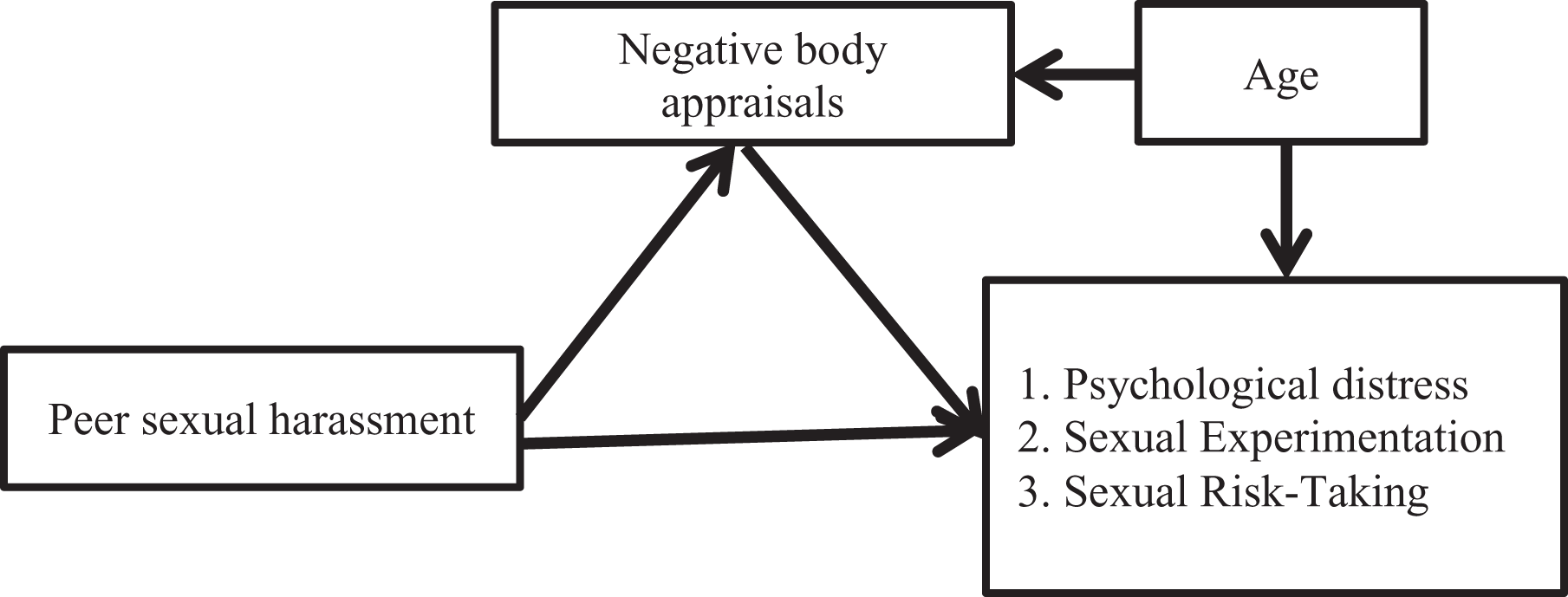
Theoretical Models of Mediation.
Method
Participants
Participants included 323 African American adolescent girls in middle and high school (grades 6–12, mean grade = 9.24, SD = 2.65, 53% middle school, 47% high school). The majority of the sample was enrolled in public schools (94.7%; 5.3% private/parochial). The students ranged in age from 11 to 19 (M = 14.68, SD = 2.16).
Procedures
Participants were recruited through 23 local organizations that serve adolescents in Memphis/Shelby County, TN, USA (see Sagrestano, 2009 for more details). Organizations were contacted by mail with a letter and brochure explaining the issue and project. Partnering organizations were given packets that included a description of the project and a parental consent form for distribution to middle and high school students who were participating in their programs. Students who returned completed consent forms were included in the study. Following informed consent, trained members of the research team administered the survey to small groups of adolescents. Surveys were completed anonymously with girls sufficiently spaced so as to protect their privacy. Upon completion of the survey, participants were provided with an information sheet and US$5 gift card.
Measures
Peer sexual harassment
Experiences of PSH in school were measured by a 15-item school version of the Sexual Experiences Questionnaire (SEQ; Collinsworth, 2000; Ormerod et al., 2008). Items assessed three related types of unwanted, sexually harassing behavior from school peers (gender harassment, 6 items; unwanted sexual attention, 7 items; sexual coercion, 2 items). Participants rated how often each behavior had happened to them at their current school along a 3-point rating scale (0 = never, 1 = once, 2 = twice or more). Items were summed to form a total score with higher scores indicating more frequent PSH.
The SEQ (Fitzgerald et al., 1995) was adapted for use in a high school context by Collinsworth (2000). It has been used with middle and high school students across various studies with Cronbach’s α coefficients for middle school students ranging from .86 to .95 (Felix & McMahon, 2006, 2007; Lichty & Campbell, 2011) and high school girls from .89 to .92 (Collinsworth, 2000; Ormerod et al., 2008). Following item analysis, one item reflecting gender harassment was dropped from the current analyses. The α coefficient for the current sample of African American girls was .88.
Psychological distress
Psychological distress was assessed using an abbreviated version of the Brief Symptom Inventory (Derogatis & Spencer, 1982; Ormerod et al., 2008), a measure of the symptoms of psychopathology. Items assessing depression (5 items; e.g., “Feeling blue”), anxiety (7 items; e.g., “Feeling fearful”), and phobic anxiety (2 items; e.g., “Feeling afraid you will faint in public”) were rated on a 5-point Likert-type scale from not at all to extremely (coded from 0 to 4) and summed such that higher scores reflect greater distress. The α coefficient was .89.
Negative body appraisal
To assess intensity of preoccupation with body image, including body surveillance and body shame, a modified version of the Body Shape Questionnaire (Mazzeo, 1999) was used. Eight items were rated on a 6-point Likert-type scale from never to always (coded from 0 to 5) and summed to create a total score for each participant, with higher scores indicating more negative body image/higher levels of preoccupation with body image. Past work indicates that the unidimensional scale, which has been used with samples of adolescent girls of different ethnic backgrounds and ages, is highly reliable (e.g., α = .96 and .97 in Ormerod et al., 2008, and Carey, Donaghue, & Broderick, 2014, respectively). The α coefficient was .91.
Sexual experimentation and sexual risk-taking
To assess sexual experimentation and sexual risk-taking, items were drawn from the Youth Risk Behavior Surveillance Survey (YRBSS). YRBSS items are not typically combined into scales. However, researchers in Finland have argued that advanced sexual behaviors should be grouped together, but separately from sexual risk-taking, because sexual experimentation is normative, age appropriate, and not inherently risky (Kaltiala-Heino et al., 2018). Thus, two scales were created for the present study.
The Sexual Experimentation Scale included 6 items assessing advanced sexual behavior (touching another’s genitals, another touching your genitals, touching breasts, oral sex, anal sex, intercourse) that were coded as 0 (no) or 1 (yes). Higher scores indicated more sexual experimentation. The α coefficient for sexual experimentation was .75.
The Sexual Risk-Taking Scale included 3 items that have consistently been identified in the literature as increasing risk for negative outcomes, coded such that higher scores indicated more risk. Age of first intercourse was coded continuously with 16 as the cutoff for early debut (0 = never intercourse, 0 = age 17 years or older, 1 = 16 years old, 2 = 15 years old, 3 = 14 years old, 4 = 13 years old, 5 = 12 years old, 6 = 11 years old). Although early debut is typically not explicitly defined, there is some consensus that debut at age 16 is early, and thus we chose to code 16 as 1, and so forth (de Looze et al., 2012; James, Ellis, Schlomer, & Garber, 2012; Udell, Sandfort, Reitz, Bos, & Dekovic, 2010). Lifetime number of partners was coded continuously (0 = never intercourse, 1 = 1 partner, 2 = 2 partners, 3 = 3 partners, etc.). Use of condom at last intercourse was coded as 0 = never intercourse, 1 = used condom, and 2 = did not use condom, to reflect that having sex with a condom does still incur some risk over not having intercourse (Bradley, Polis, Bankole, & Croft, 2019). Given that the response options differed for these 3 items, the items were standardized (z-scores) prior to creating the scale. The α coefficient for the standardized items was .78.
Results
Descriptive Statistics and Correlations for the Sample
Analyses were conducted in SPSS version 24. Table 1 presents the psychometric and descriptive information for the major study variables with the full sample of African American girls. In all analyses, age in years (11–19) was used as a continuous variable. Table 2 presents descriptive data for major variables by school group (middle [Grade 6–8] or high school [Grade 9–12]).
Psychometric and Descriptive Information of the Major Study Variables for the Full Sample.
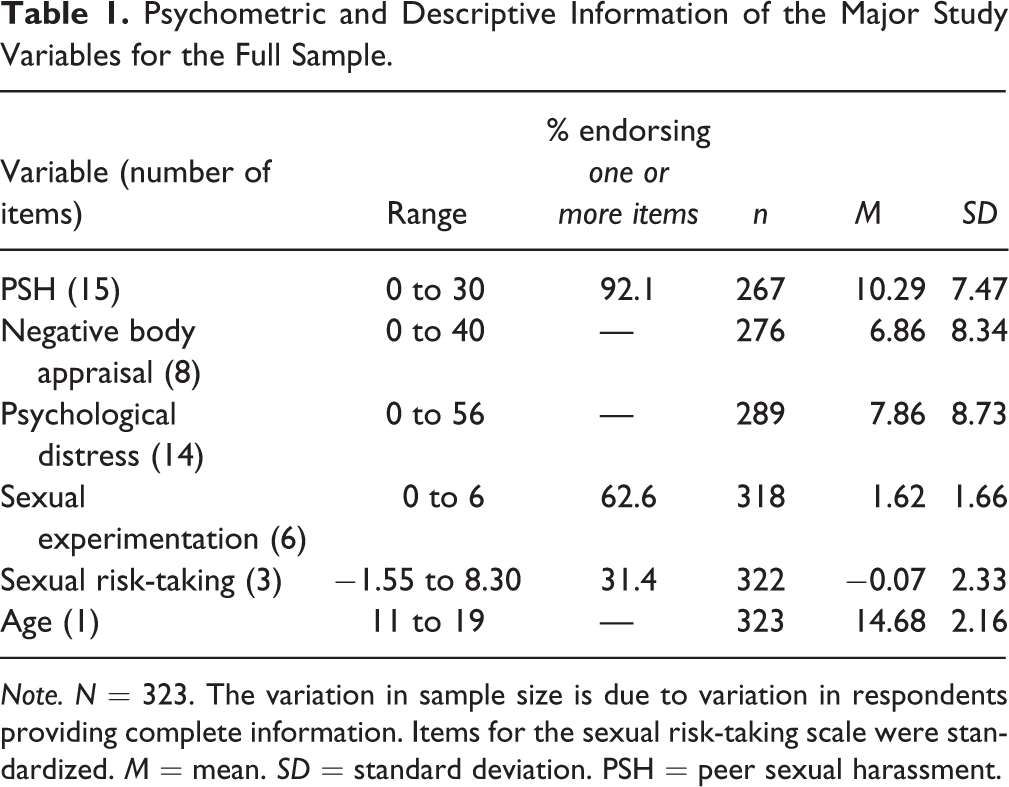
Note. N = 323. The variation in sample size is due to variation in respondents providing complete information. Items for the sexual risk-taking scale were standardized. M = mean. SD = standard deviation. PSH = peer sexual harassment.
Psychometric and Descriptive Information for the Major Study Variables by Middle and High School.
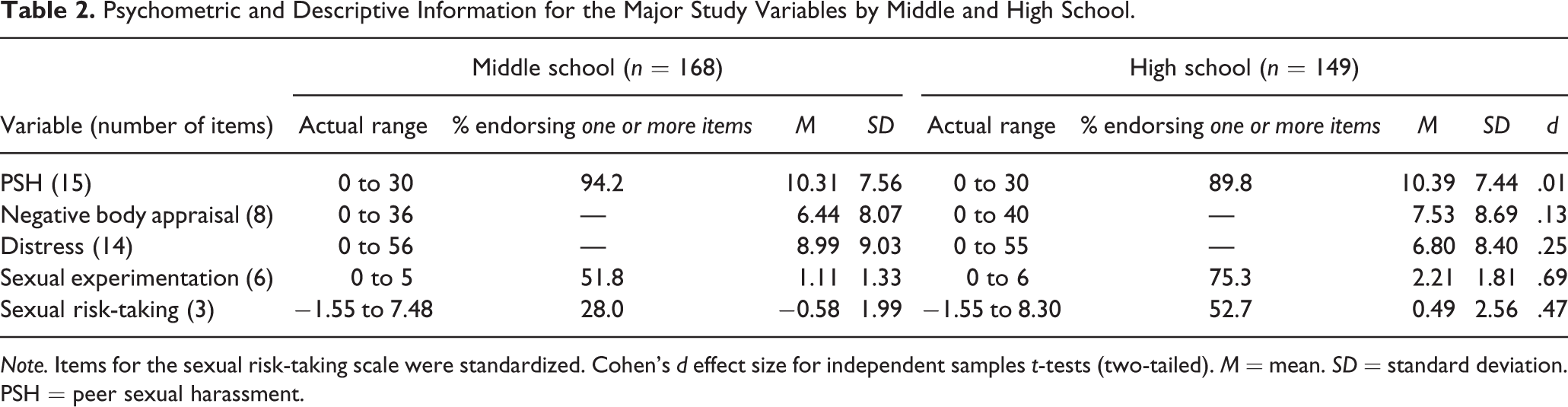
Note. Items for the sexual risk-taking scale were standardized. Cohen’s d effect size for independent samples t-tests (two-tailed). M = mean. SD = standard deviation. PSH = peer sexual harassment.
Approximately 8% (Table 1) of the full sample of African American girls reported no experiences of PSH (5.8% in middle school, 10.2% in high school; Table 2), whereas 92% of this volunteer sample reported one or more experiences with PSH across their current school tenure (94.2% middle school girls, 89.8% high school girls). In the full sample (Table 1), 37.4% reported no sexual experimentation (48.2% in middle school, 24.7% in high school; Table 2) and 68.6% reported they had not engaged in any of the sexual risks (72% middle school girls, 47.3% high school girls; Table 2).
We examined the mean score differences for the major variables via independent sample t-tests with a Bonferroni correction for multiple comparisons (p < .01) based on school group. Effect sizes are reported in Table 2. The findings indicated that girls in high school endorsed more sexual experimentation, t(310) = −6.15, p < .001, and risk-taking behaviors, t(314) = −4.18, p < .001, than girls in middle school and that these differences were in the medium range (sexual experimentation, d = .69; sexual risk, d = .47). No significant mean differences between school groups were found for PSH, t(262) = −0.08, p = .938, or negative body image, t(269) = −1.07, p = .285, and although the difference between school groups for psychological distress symptoms approached significance, t(283) = 2.11, p = .035, Cohen’s d = .25, it did not meet the Bonferroni corrected p value of .01.
Table 3 presents the bivariate correlations among the variables. Correlations were in the expected direction and provided initial support for the majority of our theorized relationships among the variables with the exception of sexual risk-taking, which was not associated with PSH or the hypothesized mediator (negative body appraisals).
Bivariate Correlations Among the Major Variables for the Full Sample.
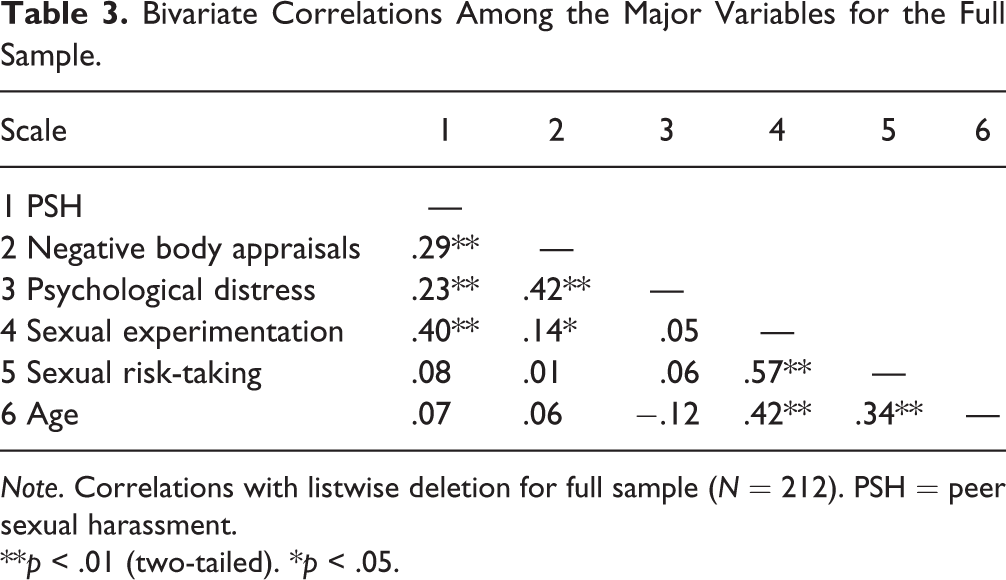
Note. Correlations with listwise deletion for full sample (N = 212). PSH = peer sexual harassment.
**p < .01 (two-tailed). *p < .05.
Tests of Mediation
We conducted three separate tests of mediation utilizing Model 4 of the PROCESS 2.16.3 macro for SPSS (Hayes, 2018). The purpose was to examine whether negative body appraisals mediated the relationship between PSH and psychological distress, sexual experimentation, and sexual risk-taking, respectively, when controlling for age. In the tests of mediation, age was coded as the individual’s self-reported age ranging from 11 years to 19 years (see Table 1).
To examine whether PSH functions as a sexual objectification experience within Moradi and Huang’s (2008) model of objectification theory relations, we tested the hypothesis that negative body appraisals would mediate the relationship between PSH and psychological distress (controlling for age). More frequent experiences of PSH were positively and directly related to negative body appraisals (b = .32, p < .001) after controlling for age of the adolescents (b =.24, p = .353). When controlling for age (b = −.56, p = .008), negative body appraisals (b = .32, p < .001) and PSH (b = .14, p = .035) were positively related to psychological distress. Using the bias-corrected bootstrapping procedure based on 5,000 samples, the indirect effect of PSH on psychological distress through negative body appraisals was significant (.11, SE = .03, 95% confidence interval (CI) = .05 to .18). The full model accounted for 20.24% of the variance in psychological distress (F [3, 212] = 17.93, p < .001) and supported PSH as a sexual objectification experience that has direct and indirect effects—through negative body appraisals on psychological distress. Thus, as PSH increases, so do girls’ negative body appraisals, which in turn are related to increased psychological symptoms, regardless of age. When looking at age in relation to psychological distress, younger girls appeared to be more distressed than older girls, although caution should be used when considering this relationship as the girls on average had few symptoms of psychological distress.
In the second test of mediation, negative body appraisals were hypothesized to mediate the relationship between PSH and sexual experimentation (controlling for age). More frequent experiences of PSH were positively and directly related to negative body appraisals (b = .33, p < .001) after controlling for age (b = .14, p = .584). Given missing values, there are slight variations in the coefficient from PSH to negative body appraisals across models. When controlling for age (b = .30, p < .001), more frequent experiences of PSH were positively and directly related to sexual experimentation (b = .09, p < .001); however, negative body appraisals were not related to sexual experimentation behavior (b = .004, p = .715). Using the bias-corrected bootstrapping procedure based on 5,000 resamples, the indirect effect of PSH on sexual experimentation through negative body appraisals was not significant (.007, SE = .018, 95% CI = −.031 to .042). The full model accounted for 33.75% of the variance in sexual experimentation (F [3, 225] = 38.21, p < .001). Thus, although the mediation was not significant, as PSH increases, so does the frequency of girls’ negative body appraisals and their sexual experimentation, regardless of age. Examining age and sexual experimentation, older girls engage in more sexual experimentation than younger girls.
In the final test, we hypothesized that negative body appraisals would mediate the relationship between PSH and sexual risk-taking behavior (controlling for age). More frequent experiences of PSH were positively related to negative body appraisals (b = .31, p < .001) after controlling for age (b = .22, p = .373). When controlling for age (b = .33, p < .001), negative body appraisals were not significantly related to sexual risk-taking behavior (b = −.02, p = .387), and neither was the relationship between PSH and sexual risk-taking behavior (b = .03, p = .222). Using the bias-corrected bootstrapping procedure based on 5,000 resamples, the indirect effect of PSH on sexual risk-taking through negative body appraisals was also not significant (−.016, SE = .018, 95% CI = −.057 to .015). The full model accounted for 9.86% of the variance in sexual risk-taking (F [3, 228] = 8.32, p < .001). Thus, neither PSH or negative body appraisals were related to sexual risk-taking. Examination of the covariate indicated that older students were more likely to be engaged in sexual risk-taking than their younger counterparts.
Discussion
We examined the relations among PSH in school, psychological distress, sexual experimentation, and sexual risk-taking in a sample of African American middle and high school girls. This study contributes to the literature by (a) examining PSH as a way of operationalizing interpersonal objectification; (b) examining the relations between PSH and psychological distress, sexual experimentation, and sexual risk-taking as mediated by negative body appraisals; and (c) using a sample of African American adolescents to better understand PSH in school and test objectification theory.
The first mediational model indicated that negative body appraisals mediated the relationship between PSH and psychological distress, controlling for age, as hypothesized. The interpersonal sexualization of girls and women has previously been operationalized as sexual objectification, and objectification theory suggests that these types of experiences lead to self-objectification, expressed as high levels of self-surveillance and body shame, ultimately leading to negative mental health outcomes (Moradi & Huang, 2008). We have demonstrated that PSH in school can act as a form of interpersonal sexualization and objectification of girls, as posited by Petersen and Hyde (2013a). Specifically, by operationalizing interpersonal objectification with PSH in this mediational model, we demonstrate that PSH follows the same pattern of results, suggesting that PSH is one way of conceptualizing and operationalizing interpersonal sexualization and sexual objectification. Our work builds on the research of Holmes and Johnson (2017), who examined sexual victimization (including both childhood and adult sexual assault) and self-surveillance in a test of objectification theory. Because PSH can be a highly sexualizing, pervasive part of the daily environment for many adolescent girls, in this study, we examine PSH in the sexual victimization role and demonstrate that it has similar impact in a sample of African American girls.
The second and third mediational models examined the relationship between PSH and adolescent sexual experimentation and sexual risk-taking, respectively, as mediated by negative body appraisals. Results indicated that PSH directly predicted sexual experimentation, but not indirectly through negative body appraisals. In contrast, PSH did not directly predict sexual risk-taking, nor was there evidence of mediation. The overall model predicting sexual experimentation explained a statistically significant amount of variance, whereas the model for sexual risk-taking did not. This is, in part, a reflection of the strong association between PSH and sexual experimentation, in contrast to an insignificant association between PSH and sexual risk-taking. Although we did not hypothesize different findings for sexual experimentation versus sexual risk-taking, one could argue that daily exposure to high levels of sexualization and sexual objectification in the form of PSH would be associated with more curiosity about sexuality and sexual experimentation, regardless of how girls feel about their bodies. In contrast, sexual risk-taking could be construed as a problem behavior (Jessor & Jessor, 1977), clustering with other externalizing behaviors with a different profile of antecedents. Indeed, early initiation of sexual behavior tends to cluster with other problem behaviors, including substance abuse and low school attachment (Madkour, Farhat, Halpern, Godeau, & Gabhainn, 2010). Further, the levels of risky sex in the sample were relatively low, which may explain why there was not a relationship with PSH.
We hypothesized that PSH would predict sexual experimentation and sexual risk-taking, and be mediated by negative body appraisals, based on recent research concluding that harassment of early maturing girls stemmed from their mature appearance rather than from being sexually active (Skoog & Özdemir, 2016). However, Kaltiala-Heino, Savioja, Fröjd, and Marttunen (2018) hypothesized that sexually active girls become targets of PSH. From this perspective, negative body appraisals would be irrelevant and it could be that sexual experimentation leads to more sexual attention, including harassment, from peers. Additional, prospective, longitudinal research is needed to clarify the causal relations among PSH and sexual experimentation.
The theoretical models and bodies of literature on objectification, body image, and PSH are built primarily on the findings from predominantly White, heterosexual women. Our study, like a handful of others (Mitchell et al., 2014; Rogers Wood & Petrie, 2010; Toomey & Russell, 2016; Watson, Ancis, White, & Nazari, 2013), examined whether these hypothesized relations generalize to more diverse samples. Our findings suggest that objectification theory is applicable to African American adolescent girls. Nonetheless, there remains a need for data from adolescents with a range of backgrounds and experiences to better understand the complexities of how intersecting identities and sources of power and privilege impact adolescent girls’ experiences with sexual harassment and other forms of interpersonal sexualization (Bucchianeri, Eisenberg, & Neumark-Sztainer, 2013; Toomey & Russell, 2016).
There are several limitations of the current research. Most notably, the data are cross-sectional, which limit the extent to which we can reach causal conclusions. Although we hypothesize causal directions in the mediational models, without prospective research, our findings should be interpreted with caution. Our data are limited by two additional factors. First, the variability in sexual experimentation and sexual risk-taking is linked to age, which is not evenly distributed in this sample. Many of the girls in the study had not yet started to experiment with their sexuality. As would be expected, girls in high school were significantly more likely to have engaged in experimentation and risk-taking than those in middle school. Second, PSH is only one of many things that we would expect to explain sexual experimentation and sexual risk-taking. Although we believe it is an important piece of the puzzle, there are other important school, family, and social contexts that have been demonstrated to influence adolescent sexuality. Nonetheless, our models explain a moderate portion of variance in psychological distress and sexual experimentation, which suggest this is a promising line for future inquiry.
This study examined the impact of PSH in school on psychological distress, sexual experimentation, and sexual risk-taking in a sample of African American middle and high school girls. The findings indicate that middle and high school girls continue to contend with school environments marked by sexualization and interpersonal objectification, which is then linked to higher levels of psychological distress. In addition, PSH is associated with increased sexual experimentation. The findings highlight the need to prioritize PSH and gender-based violence prevention programs in schools. These programs must not only address the issue of sexualization, but must take an intersectional approach that acknowledges the role of multiple vulnerabilities on power and privilege in various situations, from peer interactions to how students cope with or report injustice. To do so requires adults creating culturally appropriate safe spaces for open communication about these issues. Thus, it is incumbent upon us all to take responsibility for the social norms and values that are communicated to our children, shift to a more positive set of images and messages that discourage sexual harassment and other gender-based violence, and promote respect for all.
Footnotes
Authors’ Note
Lynda M. Sagrestano was previously at the Center for Research on Women, The University of Memphis.
Acknowledgment
Special thanks to Deborah Clubb, Regina Lowry, Janelle Williams, Teresa Diener, and the community organizations involved in data collection and to the adolescents who participated in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by The Urban Child Institute, Memphis, TN, USA, and The University of Memphis, Faculty Research Grant Program awarded to the first author.