
Abstract
This study examines the association between self-rated health (SRH) and chronic diseases on planned retirement age, and whether these relationships differ by race and ethnicity among adults 50 years and older in the US. Using the 2018 Health and Retirement Study (N = 3,161), linear regression models assessed associations and tested race as a moderator. The results showed that respondents with poorer SRH reported an earlier planned retirement age. Overall, chronic disease was not associated with planned retirement age for the sample. Rather, a higher number of chronic diseases was significantly associated with earlier planned retirement among Hispanic respondents and marginally associated among non-Hispanic Black respondents when compared to White respondents. Older adults who report being healthier plan to work longer than those reporting worse health. To support the aging workforce, chronic disease prevention efforts for Hispanic adults are crucial. Future research should examine how health impacts different industries’ workforce.
Introduction
Over the past several decades, people have been living longer, healthier lives due to advances in technology, public health, and medicine (Vespa, 2018). As global populations continue to age and life expectancy rises, governments face increasing pressure to sustain public pension systems and promote prolonged workforce participation. In the United States, the last of the Baby Boomer generation will be 65 years old by 2030 (America Counts, 2019). Consequently, issues related to retirement policy, economic security, and the viability of intergenerational support structures will become increasingly salient in public discourse and policy development (Cho et al., 2018; Datta Gupta & Larsen, 2010; McGarry, 2004; Pietiälinen et al., 2011).
Oftentimes, retirement signifies that individuals have ended their working careers and are transitioning to nonworking, social roles (van Zon et al., 2016). On average, people in the United States retire around age 65, which roughly coincides with the age individuals become eligible for Social Security retirement benefits or when pension benefits mature (Munnell et al., 2019). Individuals approaching this stage of life may also experience increasing health and functional challenges that influence their retirement decisions.
Between 1970s and 1990s, policies encouraged older workers to retire (Axelrad & McNamara, 2018Axelrad & Mcnamara, 2018). Earlier retirement offered opportunities for younger age-cohorts to enter the workforce (Mirkin, 1987). Additionally, earlier retirement in the 70s and 90s were implemented in a demographic context characterized by substantially lower life expectancy, which made shorter post-retirement periods appear economically and socially sustainable. Since the 1990s, there has been a growing emphasis on older adults remaining in the workforce longer which has been driven by both economic necessity and evolving social norms (Robinson & Lewis, 2005). To match the shifting cultural landscape among the aging workforce, U.S. policy shifts have increased the age that beneficiaries could retire at to receive full social security benefits. Over time, these changes carried assumptions that aging populations can remain in the workforce longer (Cho et al., 2018; Datta Gupta & Larsen, 2010; Pietiälinen et al., 2011). These changes underscore the importance of examining who is able (or unable) to plan for later retirement, especially given persistent disparities in health and employment opportunities.
Those planning for retirement must carefully determine the optimal age to retire. For most people, transitioning into retirement requires adjusting to a lifestyle without the obligation to work and diminished income (McGarry, 2004). In addition to financial factors, McGarry (2004) analyzed data from the Health and Retirement Study (HRS) and found that individuals’ expectations for retirement are significantly affected by their health status, even more so than by their income or accumulated wealth. Thus, the expectation of living longer, healthier lives likely affect peoples’ retirement plans (McGarry, 2004).
However, the relationship between health and retirement may vary across individuals. Poor health may accelerate retirement among some, but people working less physically demanding jobs or facing financial hardship may delay retirement, regardless of their health (Datta Gupta & Larsen, 2010). Given that retirement often occurs as individuals age and is accompanied by age-related declines in health and rising healthcare needs, understanding how health status shapes retirement planning may inform more equitable and effaceable allocation of resources for aging populations (Nordenmark & Stattin, 2009).
Physical Health’s Role in Retirement
In the United States, chronic diseases account for nearly 75% of all healthcare expenditures, estimated at $5,300 per person per year (Raghupathi & Raghupathi, 2018). Chronic disease is defined as a long-lasting health condition that requires the need for ongoing medical care typically lasting over a year and often limits daily activities (Centers for Disease Control and Prevention [CDC], 2021), and include conditions such as heart disease, cancer, chronic lung disease, stroke, Alzheimer’s disease, diabetes, chronic kidney disease, and emotional-related mental illnesses (National Institute of Mental Health [NIMH], 2024). The latest trends show that three-fifths of adults ages 18 and older have one chronic disease and two-fifths of adults ages 18 and older have more than two (CDC, 2021). Chronic diseases can have debilitating impacts on an individual’s workforce participation such as diminished productivity, increased absences, or leaving the workforce entirely (Raghupathi & Raghupathi, 2018).
Individuals self-perception of their health links with their plans for retirement (Vanajan et al., 2020). Self-rated health indicators serve as a cornerstone to evaluate physical well-being and offer a subjective perspective of one’s own health status (Manderbacka, 1998). However, it is crucial to acknowledge that self-rated health can vary significantly across races and ethnicities, introducing complexities when attempting to make “objective” comparisons across different demographic groups (Bardage et al., 2005). Despite the nuances in self-rated health assessments, researchers still regard them as valuable predictors of future health outcomes (Pietiälinen et al., 2011).
Chronic disease plays a pivotal role in shaping an individual’s health trajectory (Miah & Wilcox, 2007). The burden of chronic disease does not typically lead to a rapid deterioration of an individual’s health, but it does necessitate frequent treatment and medication, which ultimately affects self-rated health (Miah & Wilcox, 2007). The pain and functional limitations arising from a chronic disease may prompt individuals to retire early (Saastamoinen et al., 2012).
The interplay between self-rated health and chronic disease provides important context when an individual considers retiring. Chronic disease may gradually impair the functional status of individuals who are approaching retirement age, thereby potentially forcing them to retire. Individuals with chronic disease(s) may take a long time adapting their work life to accommodate decreasing functioning before ultimately deciding to retire (Miah & Wilcox, 2007).
The Influence of Race and Ethnicity on Retirement
The direction of the health–retirement response may differ by race/ethnicity due to structural conditions. Racial and ethnic minority groups often experience structural disadvantages and socioeconomic inequities (Folorunsho, 2025; Williams et al., 2010) that impact their employment opportunities (Francis & Weller, 2021; Pager & Shepherd, 2008) and access to healthcare (Bulatao et al., 2004; Francis & Weller, 2021; Miller, 2020) which can impact their retirement planning. Studies have shown that individuals from racial and ethnic minority groups tend to face higher rates of financial insecurity in retirement (Francis & Weller, 2021; Rhee, 2013). Racial and ethnic minority Americans have lower wages and financial literacy, less retirement savings, experience more workplace discrimination, and receive less intergenerational wealth transfers as compared to White Americans (Francis & Weller, 2021; Viceisza et al., 2022). Regarding retirement preparation, literature shows that Black adults are paid less, have higher unemployment levels, have a lower likelihood of employer-based retirement benefits, are less likely to receive wealth inheritances, and have smaller savings for emergencies than White adults (Markowitz, 2023; Miller, 2020). Also, Black adults currently in the workforce experience more challenges with health care coverage and retirement saving than White adults (Miller, 2020). Therefore, socioeconomic and workplace inequities may inhibit racial and ethnic minority populations retirement planning compared to majority populations.
Health disparities across racial and ethnic groups are well-documented, with racial and ethnic minority populations experiencing higher rates of chronic disease, lower life expectancy, premature death, and limited access to quality healthcare (Bulatao et al., 2004; National Academies of Sciences, Engineering, and Medicine, 2017National Academies of Sciences et al., 2017; Williams et al., 2010). Due to these inadequate and systemic barriers, racial and ethnic minority groups may retire sooner than White groups (Miller, 2020). Furthermore, racial and ethnic groups report different reasons for early retirement compared to White groups. Specifically, Black Americans often retire early due to impaired health or disability, whereas White Americans retire early because they are financially stable (Viceisza et al., 2022).
While race is often acknowledged as a factor influencing aging experiences and health, the structural and systemic roots of racial inequities are frequently overlooked (Torres, 2020). Marginalized groups are more likely to experience unstable employment, lower job quality, and limited opportunities to extend their working lives due to structural inequities like occupational segregation, cumulative health disadvantage, and disparities accessing healthcare and educational opportunities (Moen et al., 2022). These uneven work trajectories impact later life, including retirement. These findings underscore that the associations between health and anticipated retirement age are not uniform across racial groups, highlighting important heterogeneity in how health influences retirement planning in later life.
Overall, minoritized workers report mixed factors which predict earlier and later retirement. Lower wages, physically demanding jobs, and limited employment benefits can make continued employment less feasible when health deteriorates, favoring earlier retirement. Conversely, financial strain, weaker access to disability benefits, or lack of alternative income may compel some to delay retirement, despite poor health. These countervailing forces underscore the need to examine race/ethnicity as a moderator of the health–retirement association rather than only as a main-effect predictor.
Theoretical Framework
We incorporate Nilsson’s (2012) emphasis on health as a key retirement driver and Beehr’s (1986) model of retirement decisions, which distinguishes between voluntary vs. involuntary and early vs. on-time retirement. These models guide our interpretation of health-related predictors and the variability in retirement planning across social groups. This study is informed by Cumulative Disadvantage Theory, which suggests that inequalities in education, employment, and health accumulate over the life course and shape the ability to plan for retirement in later life (Dannefer, 2003; Moen et al., 2022). These disadvantages such as lower lifetime earnings, higher prevalence of physically demanding jobs, and cumulative health challenges are often more pronounced among racial and ethnic minorities and can limit both their ability to remain employed in later life and their access to formal retirement planning options (Dannefer, 2003; Moen et al., 2022). We also reference Engagement and Disengagement Theory (Cumming & Henry, 1961), which views retirement as part of a natural process of social withdrawal in aging. However, when applied to marginalized groups, this disengagement is often not the result of voluntary withdrawal but rather forced by structural barriers. These include earlier onset of chronic disease, limited access to flexible or accommodating work environments, and insufficient retirement benefits. In this context, retirement may occur prematurely—not because of personal choice, but due to declining health or lack of viable work options, highlighting the inequitable conditions under which some older adults exit the labor force.
The Present Study’s Objectives
Previous research on the relationship between health and planned retirement age has produced mixed findings. Some studies have shown that poor health is associated with earlier retirement (Datta Gupta & Larsen, 2010; McGarry, 2004), while others have found conflicting or no associations once financial constraints or job characteristics are taken into account (Stenholm et al., 2019). One reason for this inconsistency is conceptual: individuals retiring for health reasons may exaggerate symptoms to qualify for benefits, which can introduce reporting bias (Datta Gupta & Larsen, 2010). Methodologically, studies vary widely in how they define and measure health—some using self-rated health, others using diagnosed conditions or functional limitations—resulting in different conclusions (McGraw & Mandl, 2021). Additionally, cross-national research highlights that institutional and policy differences (e.g., disability insurance rules, early retirement incentives) can shape how health effects retirement expectations (Datta Gupta & Larsen, 2010; Pietiälinen et al., 2011). These variations in data, methods, and context make it difficult to draw uniform conclusions. This study addresses these gaps by examining both self-rated health and chronic disease count as predictors, while considering how race and ethnicity may further modify these associations.
This study will examine the association between people’s subjective (i.e., self-rated health) and objective (i.e., chronic diseases) health and their planned retirement age. Importantly, retirement is often defined as the voluntary withdrawal from the labor force (Wheaton & Crimmins, 2013). However, in this study, we operationalize retirement using the Health and Retirement Study’s definition, where retirement is the expected age respondents plan to stop working for pay—regardless of whether that decision is driven by voluntary or involuntary reasons (Health and Retirement Study, 2017). Furthermore, this research will examine individuals who are 50 years old or older and are still working. Therefore, the research questions for this study are: (1a) Is self-rated health associated with an individual’s planned retirement age? (1b) Does the association between self-rated health and planned retirement age vary by race/ethnicity? (2a) Is the number of chronic diseases associated with an individual’s planned retirement age? (2b) Does the association between chronic disease count and planned retirement age vary by race/ethnicity?
In examining the relationship between health and planned retirement age, it is essential to account for sociodemographic and economic characteristics that may confound or moderate this association. Prior research has identified several key variables that consistently influence retirement planning. Age, gender, education, marital status, and wealth have been shown to significantly shape individuals’ retirement expectations and health-related decisions (Datta Gupta & Larsen, 2010). Being older and male predict later planned retirements, while marital status resulted in mixed findings, often reflecting joint planning between spouses (Noone et al., 2010). Higher education generally predicted later retirement ages (Datta Gupta & Larsen, 2010). The relationship between wealth and retirement timing is less straightforward. Prior studies show that wealth can influence retirement decisions, but the direction of this effect varies by context (Datta Gupta & Larsen, 2010; Liu et al., 2023; Munnell et al., 2019). Parental responsibilities also play a role, as the presence of children may delay retirement due to ongoing financial obligations (Jeong & Kim, 2020). Renting versus owning a home is associated with later planned retirement, plausibly reflecting financial constraints (Nilsson, 2012). Guided by these findings, our analysis includes age, gender, marital status, education, household wealth, housing status, and number of children as covariates to provide a more accurate estimation of the health-retirement relationship.
Method
Data
This study used data from the Health and Retirement Study (HRS), which is sponsored by the National Institute on Aging and is conducted by the University of Michigan. The HRS is a comprehensive, nationally representative, longitudinal panel study that surveys participants about the challenges and opportunities of aging in the United States (Sonnega et al., 2014). The HRS specifically targets non-institutionalized U.S. adults aged 50 and older including their spouses or partners regardless of age. The data are focused on four topics: income and wealth; health, cognition and use of healthcare services; work and retirement; and family connections (Sonnega et al., 2014). The HRS public survey has been conducted biannually since 1992 and contains more than 37, 000 individuals across 23,000 households in the United States. Specifically, the 2018 wave of data contains 17,146 respondents (HRS, 2017). In addition, this study focused on the association between an individual’s current health status and retirement planning decisions, so a cross-sectional research design was adopted.
Descriptive Statistics of Study Variables for the Full Sample
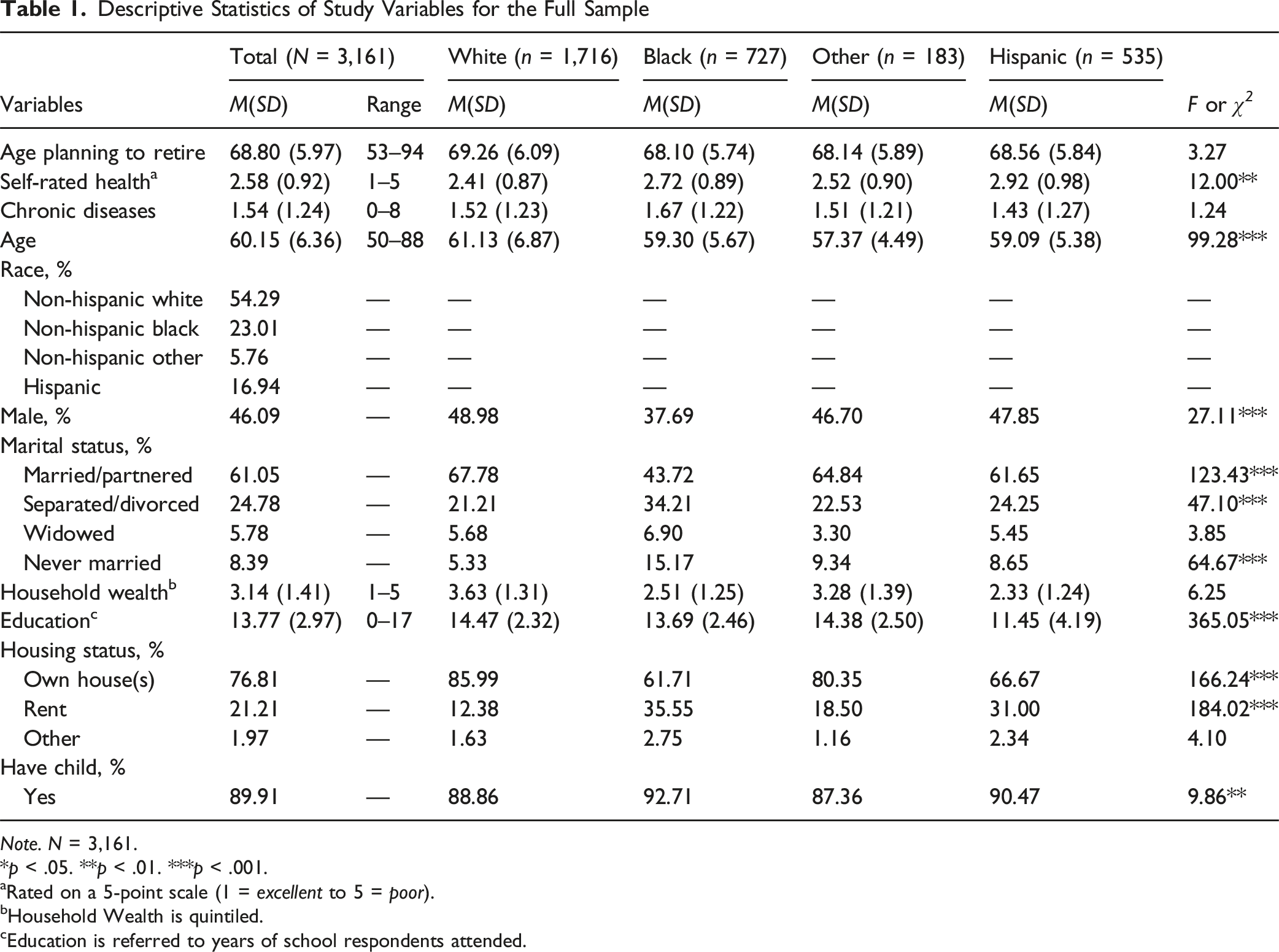
Note. N = 3,161.
*p < .05. **p < .01. ***p < .001.
aRated on a 5-point scale (1 = excellent to 5 = poor).
bHousehold Wealth is quintiled.
cEducation is referred to years of school respondents attended.
Measures
Planned Retirement Age
The main dependent variable was respondents predicted age of when they were either planning to retire or thinking of retiring. The survey instrument wording was, “At what age do you plan to stop working?” for individuals who indicated having a retirement plan. This measure does not distinguish between voluntary and involuntary exits from the workforce. Responses were coded as a continuous variable in years.
Self-rated health
Self-rated health was assessed by the question: “Would you say your health is excellent, very good, good, fair, or poor?”. The result was coded ordinally as 1 = excellent to 5 = poor and treated as a continuous variable.
Chronic disease
Distribution of Individual Chronic Diseases Across Racial/Ethnic Groups
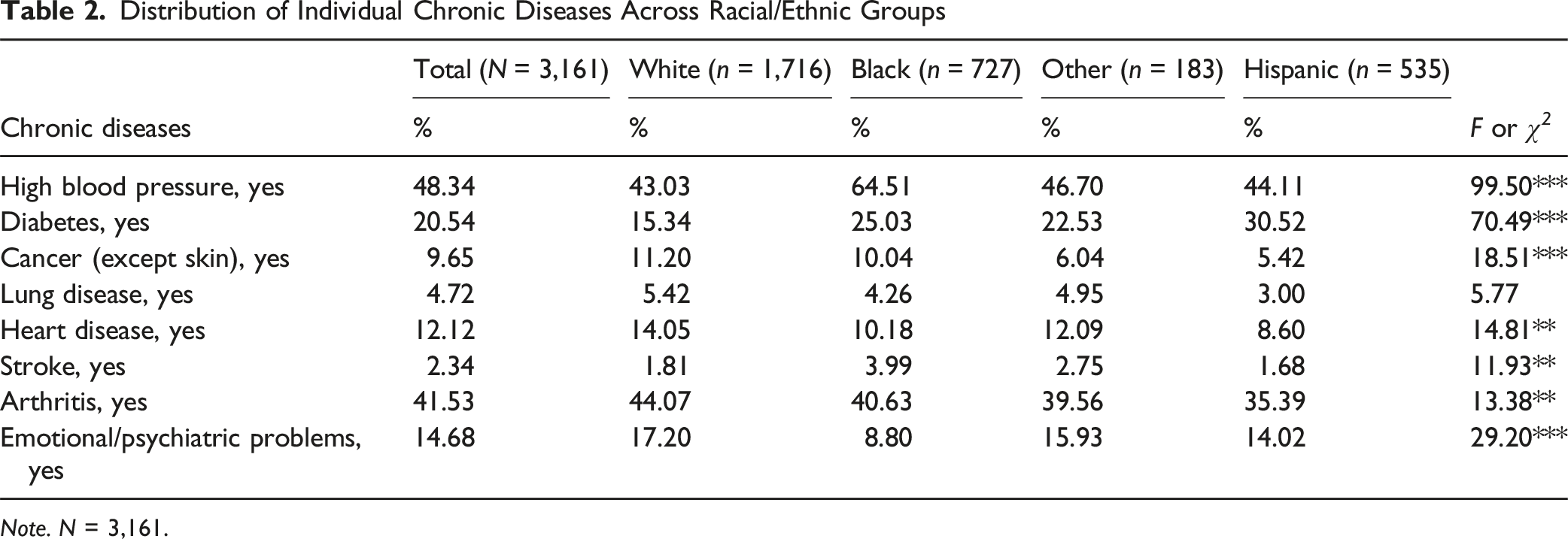
Note. N = 3,161.
Moderator
Race/ethnicity was treated as a moderator in this study. A moderator is a variable that affects the strength or direction of the relationship between two other variables. Race and ethnicity were first classified as two separate variables. Race included three categories: White, Black, and Other (i.e., Asian, Native American, or multiracial respondents). Ethnicity was coded as a binary variable indicating whether the respondent identified as Hispanic or Latino. The final combined race and ethnicity were recategorized as four categories: non-Hispanic White (reference group), non-Hispanic Black, non-Hispanic other, and Hispanic.
Covariates
Gender, age, race/ethnicity, marital status, education, household wealth, housing status, and having children were controlled in this study. Gender was coded as a dichotomous variable: female (reference group) and male. Age was assessed in years by how old respondents were in 2018 (range = 50 – 88 years). Marital status was coded as four categories: married/partnered (reference group), separated/divorced, widowed, and never married. Education was measured as years of completed schooling (range = 0 – 17+ years). Total household wealth was categorized into quintiles and entered as a categorical variable in the regression models to address the skewed distribution of wealth, with the lowest quintile serving as the reference group. Housing status was coded into three categories: own (reference group), rent, and other. Whether respondents had at least one child was coded as a dichotomous variable: respondents without children (reference group) and those with any number of children.
Analytic Strategy
Continuous variables, including self-rated health, chronic disease count, education years and age, were mean-centered to enhance interpretability of interaction effects. This procedure is commonly applied in regression models involving moderators (Alberth et al., 2024). Person-level analysis weights were applied to the analyses (HRS, 2017). Ordinary least squares (OLS) models examined the research questions and hypotheses. We test conventional measures of significance at the α = 0.05 level, denoted with stars at the 0.05, 0.01, and 0.001 levels. Additionally, p-values less than 0.10 were treated as marginally significant and interpreted cautiously as suggestive trends.
OLS Regression Results of Planned Retirement Age on Self-Rated Health/Chronic Diseases
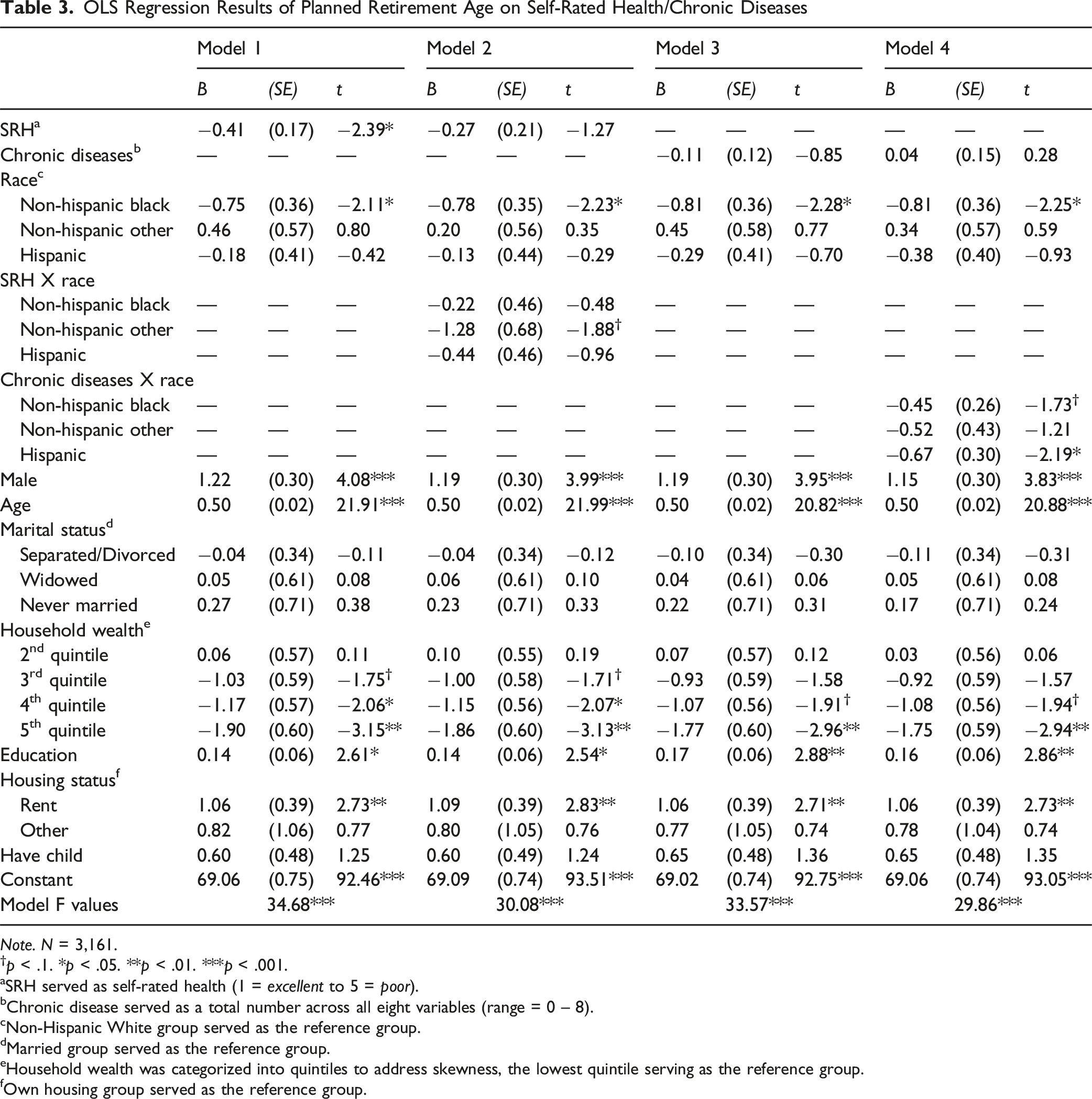
Note. N = 3,161.
†p < .1. *p < .05. **p < .01. ***p < .001.
aSRH served as self-rated health (1 = excellent to 5 = poor).
bChronic disease served as a total number across all eight variables (range = 0 – 8).
cNon-Hispanic White group served as the reference group.
dMarried group served as the reference group.
eHousehold wealth was categorized into quintiles to address skewness, the lowest quintile serving as the reference group.
fOwn housing group served as the reference group.
OLS Regression Results of Planned Retirement Age on Chronic Diseases
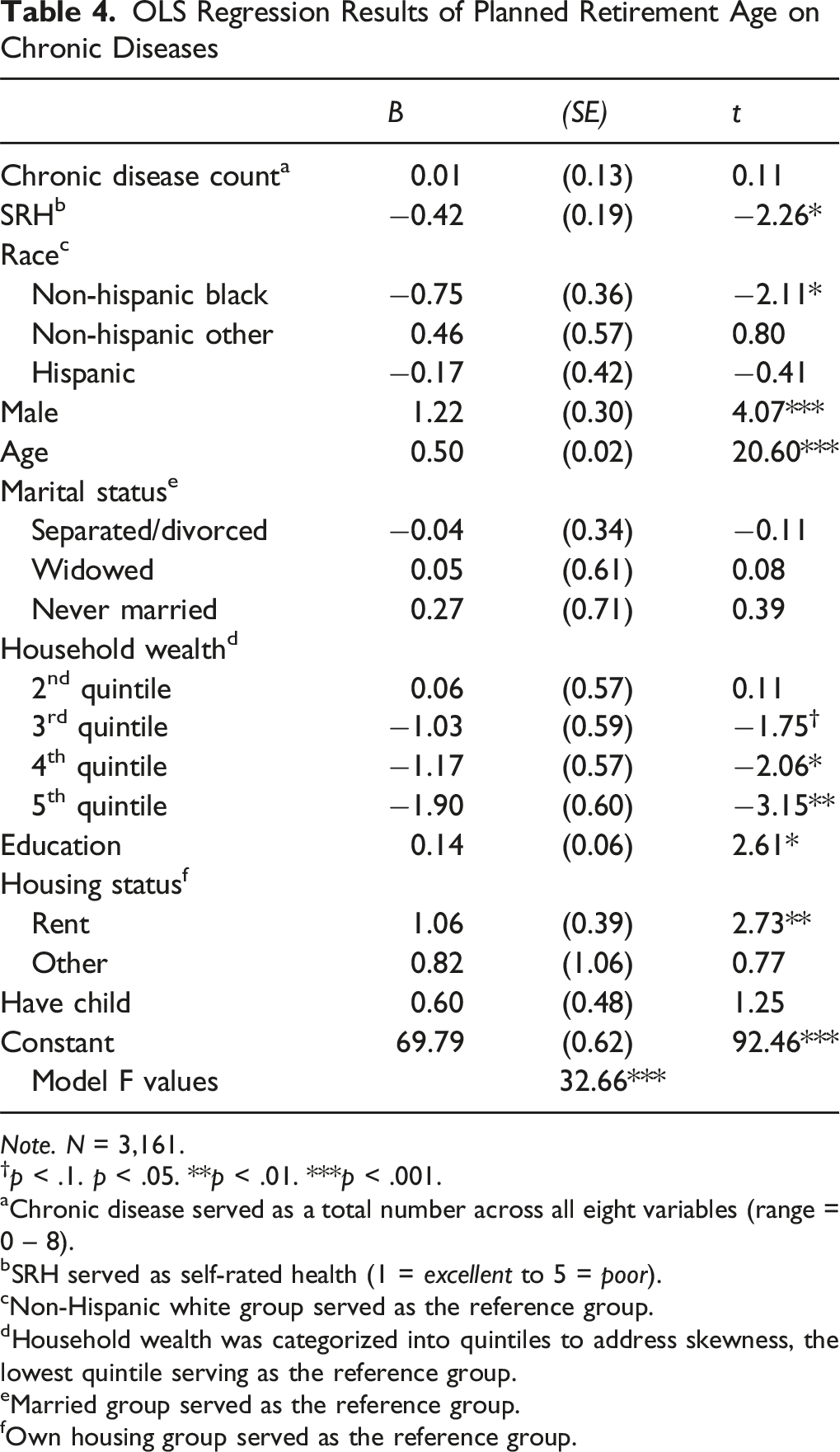
Note. N = 3,161.
†p < .1. p < .05. **p < .01. ***p < .001.
aChronic disease served as a total number across all eight variables (range = 0 – 8).
bSRH served as self-rated health (1 = excellent to 5 = poor).
cNon-Hispanic white group served as the reference group.
dHousehold wealth was categorized into quintiles to address skewness, the lowest quintile serving as the reference group.
eMarried group served as the reference group.
fOwn housing group served as the reference group.
Results
Table 1 presents the descriptive characteristics of the analytic sample (N = 3,161) for all study variables, along with the multivariate analysis results, including a Scheffé post hoc test for comparisons across race/ethnicity. The mean planned retirement age for the full sample was 68.80 (SD = 5.97) years old, with a mean self-rated health score of 2.58 (SD = 0.92), and a mean number of chronic diseases of 1.54 (SD = 1.24). The mean age for the full sample was 60.15 (SD = 6.36) years old. The majority of the analytic sample included female, non-Hispanic White, homeowners, and who had at least one child. Of respondents, 54.29% were non-Hispanic White, 23.01% non-Hispanic Black, 5.76% non-Hispanic other, and 16.94% Hispanic. Self-rated health varied significantly across racial/ethnic groups. Hispanic respondents reported the poorest self-rated health on average (M = 2.92, SD = 0.98), followed by non-Hispanic Black respondents (M = 2.72, SD = 0.89). Non-Hispanic White respondents reported the best self-rated health (M = 2.41, SD = 0.87), with non-Hispanic Other respondents falling between these groups (M = 2.52, SD = 0.90). Differences in chronic disease counts were not statistically significant.
Table 2 presents the descriptive statistics on the prevalence of specific chronic diseases across racial and ethnic groups. Non-Hispanic Black respondents showed notably higher rates of hypertension and diabetes compared to non-Hispanic Whites. Hispanic respondents also had a higher prevalence of diabetes, although their hypertension prevalence was similar to that of non-Hispanic Whites. Non-Hispanic Whites had higher rates of arthritis and exhibited slightly higher rates of cancer relative to other groups. These differences, although varying in magnitude, indicate that chronic disease burden is not evenly distributed across racial/ethnic groups.
Table 3 shows the results for OLS regression models of self-rated health and planned retirement age (Model 1 – 2). Model 1 shows that self-rated health is significantly associated with retiring earlier (β = −.41, p = .018), indicating that poorer self-rated health (higher scores) was associated with a lower planned retirement age, suggesting that individuals reporting worse health tended to plan to retire earlier. Also, non-Hispanic Black respondents planned to retire earlier than non-Hispanic White respondents (β = −0.75, p = .036). Respondents who were older planned to retire later (β = 0.50, p < .001). Male respondents planned to retire later than female (β = 1.22, p < .001). Respondents in the higher household wealth quintile group planned to retire earlier (5th quintile: β = −1.90, p = .002). Respondents who had more years of education planned to retire later (β = 0.14, p = .010). Moreover, respondents who rented their home (β = 1.06, p = .007) planned to retire later than respondents who owned their home. Model 2 presents the OLS regression results with the interaction of self-rated health and race/ethnicity on planned retirement age. The main effect of self-rated health on planned retirement age and the interaction terms were not statistically significant, indicating that the association between self-rated health and planned retirement age do not differs across racial/ethnic groups. However, the marginally significant interaction between planned retirement age and the non-Hispanic Other group (β = −1.28, p = .061) indicates a possible trend, where the non-Hispanic Other group retires sooner than the non-Hispanic White group. Model 2 maintained significant effects between the non-Hispanic Black group compared to non-Hispanic White group (β = −0.78, p = .028) on planned retirement age. All other covariates remained the same as in Model 1.
Model 3 shows the main effects of the association between chronic diseases and planned retirement age, demonstrating that the main effect was insignificant (β = −.11, p = .396). Non-Hispanic Black respondents planned to retire earlier than non-Hispanic White respondents (β = −.81, p = .023). The direction and significance patterns of the covariates remained largely consistent with those observed in Model 1. Model 4 presents the OLS regression results with the interaction of chronic diseases and race/ethnicity for planned retirement age. The main effect of chronic diseases in Model 4 stayed insignificant when including interactions; that is, there were no significant differences for non-Hispanic White participants. The interaction effect of chronic diseases on planned retirement age was marginally significant for non-Hispanic Black respondents (β = −0.42, p = .084) and statistically significant for Hispanic respondents (β = −0.67, p = .029). These results suggest that, compared to non-Hispanic Whites, chronic diseases were significantly associated with expectations of earlier retirement among Hispanic respondents, and showed a marginal association among non-Hispanic Black respondents. All other covariates kept the same significant association as Model 3.
Table 4 presents the results of the OLS regression examining the association between chronic disease and planned retirement age, with self-rated health included. The main effect of chronic disease is not statistically significant (β = 0.01, p = .916). However, self-rated health remains a significant predictor of planned retirement age (β = −0.42, p = .025), suggesting that individuals’ subjective perceptions of their health may play a more decisive role in shaping retirement expectations than the number of diagnosed chronic diseases.
As a robustness check, we also estimated all models restricting the analytic sample to adults aged 50–69. The overall pattern of results was largely consistent with the full age sample, particularly for the significant interaction between chronic disease and Hispanic ethnicity. However, marginally significant interaction effects observed in the full sample, specifically for self-rated health among non-Hispanic Other respondents and chronic disease among non-Hispanic Black respondents, were no longer statistically significant in the restricted age sample. This suggests that these interaction effects may be sensitive to age composition and should be interpreted cautiously.
Discussion
The current study examined whether self-rated health and chronic disease are associated with planned retirement age and whether this association varies for differing racial/ethnic groups using the 2018 wave of the HRS. Due to the theoretical importance of health in the retirement decision-making process (Beehr, 1986; Nilsson, 2012), this study presents a timely and essential investigation into racial/ethnic disparities in how health conditions are associated with planned retirement age among older working adults.
Our results found that adults age 50 and older with poorer self-rated health intended to retire earlier compared to those who had better self-rated health. Further, we found no association between planned retirement age and frequency of chronic diseases. This reinforces the notion that subjective assessments of health are meaningful predictors of retirement intentions, potentially reflecting physical capacity and psychological readiness to exit the workforce (Van Solinge & Henkens, 2010). Furthermore, while limited, we found evidence suggesting that race and ethnicity moderated the association between self-rated health and planned retirement age. Although the interaction between self-rated health and non-Hispanic Other race reached marginal statistical significance, this finding should be interpreted cautiously. In contrast, stronger evidence of the role chronic disease and racial/ethnic variation emerged on planned retirement age. Specifically, chronic disease was significantly associated with earlier planned retirement among Hispanic respondents and showed a marginal association among non-Hispanic Black respondents, compared to non-Hispanic Whites.
These findings suggest that health may play a role in shaping retirement plans, and that individuals’ subjective appraisals of their health could be more influential than the presence of chronic diseases. Prior research shows that poor self-rated health increases the likelihood of early retirement and may exert a stronger influence on retirement timing than other factors such as income or marital status (Homaie Rad et al., 2017). This pattern is somewhat consistent with our findings. Seemingly, individuals plan to retire earlier when they rate their health as poor, while others with better self-rated health tend to perceive themselves as more capable, energetic, and resilient (Zhang et al., 2022). Plausibly, this optimistic self-perception may lead older adults to believe that they can sustain their current level of productivity and engagement in the workforce for a longer duration.
When considering objective measures of health, previous studies showed that older people with multiple chronic diseases may choose to retire early due to uncertainty about the future and to protect themselves from future disease-related impacts (Holman, 2020). As a result, this study hypothesized that adults 50 years and older experiencing fewer chronic diseases planned to retire later than respondents with more chronic diseases. However, we found that planned retirement age is not associated with individuals’ chronic diseases. This may be due to the fact that the number of chronic diseases may not immediately affect the physical health of the individual (Miah & Wilcox, 2007). With appropriate symptom management, the negative health effects of chronic diseases may be effectively mitigated or delayed. Therefore, individuals may not change their retirement age decisions as a result of differing conditions.
While previous research often highlights health as a central factor in retirement timing, our findings suggest that the influence of health may depend on how it is measured. In our analysis, the number of diagnosed chronic diseases was not significantly associated with planned retirement age. One possible explanation is that individuals with chronic diseases face countervailing forces when planning for retirement. Although chronic diseases may reduce physical functioning and increase the desire to retire earlier, other factors such as financial necessity, limited access to disability benefits, or lack of alternative income sources may compel individuals to remain in the workforce despite their health conditions (Yuan et al., 2022). As a result, the presence of chronic diseases may not translate directly into earlier planned retirement age. Instead, individuals may continue working while managing their conditions, particularly if the diseases are well controlled or do not immediately limit work capacity. These competing forces may help explain the insignificant association between chronic disease count and planned retirement age observed in this study. Together, these factors may explain the overall association between self-rated health and planned retirement age among working population aged 50 and above.
Our moderation analyses provide partial evidence that associations between chronic diseases and planned retirement age varies across racial/ethnic groups. Specifically, the interaction between chronic disease and Hispanic ethnicity was statistically significant, indicating that a higher number of chronic diseases is associated with earlier planned retirement among Hispanic respondents compared to White respondents. In contrast, the interaction term for non-Hispanic Black respondents was marginally significant and should therefore be interpreted cautiously. Certain racial and ethnic groups may face higher rates of chronic diseases and limited access to quality healthcare, leading to earlier retirement (Williams et al., 2010). The stress associated with discrimination and unequal treatment may further exacerbate health issues (Pascoe & Smart Richman, 2009), necessitating early exits from the workforce. Evidence also points to large racial differences in industry patterns (Moore et al., 2019).
Research findings have consistently underscored the existence of pronounced disparities, particularly among these groups, with a specific focus on Black and Hispanic communities (Rhee, 2013). For Hispanic older adults, chronic diseases may be compounded by systemic barriers such as language access issues, immigration-related employment constraints, and disproportionate representation in physically demanding or informal sector jobs, all of which can heighten the impact of chronic disease on early retirement planning (Vega et al., 2009). These disparities permeate various facets of life, ranging from financial stability to access to educational and employment opportunities, and even the overall median household income. Such disparities, when examined in contrast to their White counterparts, reveal a disheartening gap in the quality of life experienced by these marginalized groups (Rhee, 2013). Future research should examine whether specific types of chronic diseases (e.g., cardiovascular disease) or the severity of conditions vary by race/ethnicity, which may help clarify the observed interaction between chronic disease count and race/ethnicity in shaping retirement expectations.
Racial health inequalities have far-reaching implications, especially when we consider their impact on the retirement expectations and planning of individuals within these racial minority communities. Financial insecurity, often an unfortunate consequence of lower household incomes and restricted economic opportunities, casts a shadow over the retirement prospects for many individuals (Quinn & Cahill, 2016). Consequently, these pervasive disparities can engender a sense of uncertainty and unease among individuals belonging to racial minority groups when contemplating their retirement. Thus, retiring early as a consequence of suffering from poor health may represent additional problems and detrimental circumstances related to lost wages, benefits, and financial security. This reality may cascade and cause a wider, more pronounced racial and ethnic disparity with aging in later life.
The sensitivity analysis results indicate that the disappearance of marginal interaction effects when restricting the sample to adults aged 50–69. These results may reflect differences in the life-course stage at which health begins to more strongly constrain retirement planning. Individuals in their early to mid-50 s and 60 s are less likely to face imminent retirement or severe functional limitations. Therefore, health-related disparities in planned retirement age may be less pronounced. In contrast, older adults closer to retirement ages face cumulative health burdens, such as multiple chronic diseases and age-related functional limitations, as well as structural disadvantages, including age discrimination in the labor market, limited access to workplace accommodations, and fewer opportunities for reemployment, all of which may exert a stronger influence on planned retirement age. As a result, marginal interaction effects observed in the full age sample may be sensitive to age composition and should be interpreted cautiously.
There are limitations in this study. First, this study used a cross-sectional design. While a cross-sectional research design could reflect an individual’s current assessment of their physical condition, a longitudinal study design would provide more evidence about changes in an individual’s health and whether future retirement plans are affected by changes in an individual’s health condition. Future research should leverage panel data to evaluate whether such expectations align with actual retirement behavior, especially in the context of health shocks or job instability. Second, other factors not available in the HRS data sets may heavily influence the decision-making of when to retire. For example, an individual’s current occupation, job satisfaction, and retention of health insurance after retirement may influence their planned retirement age (Lytle et al., 2015). As a result, this study does not adjust for occupational or industry characteristics, which are likely correlated with both race and health. This omission limits our ability to disentangle structural job-related exposures from health-related retirement expectations.
Third, although this study included both subjective health indicators (i.e., self-rated health) and relatively objective indicators (i.e., number of chronic diseases), both measures are based on self-reports and may contain inherent biases. Moreover, this approach treats all chronic diseases as equal, without accounting for differences in severity or functional impact. For example, controlled asthma may affect retirement decisions differently than terminal cancer, but both are coded identically in our analysis. Furthermore, detailed symptomology and illness progression are not available in the public HRS data. Future research should utilize clinically verified or severity-weighted indicators to improve precision in assessing health-related retirement planning. More precise health indicators may help to draw more effective inferences about associations between health and planned retirement age (Ilmakunnas & Ilmakunnas, 2018). Moreover, chronic diseases may vary in severity with age, or by race, ethnicity, and gender. As a result, future research could focus on the effects of different chronic diseases as well as their severity on planned retirement age.
Moreover, our sample includes only individuals aged 50 and older who are currently employed. This selection may introduce bias, as individuals who are unemployed, retired, or otherwise unable to complete the HRS are excluded. As such, the findings may underestimate the overall impact of health disparities on retirement expectations, particularly among marginalized populations who may have exited the labor force earlier due to chronic disease or structural disadvantages.
Finally, this analysis used data from 2018, before the COVID-19 Pandemic (which began in March 2020 in the United States). During the pandemic, many people may have altered their retirement plans due to sudden unemployment or furloughs, changes in work patterns, or experiences of pandemic-related stress (e.g., the death of a loved one). People whose work arrangements shifted from in-office to remote work may have delayed retirement due to increased workplace flexibility. At the same time, there were also a significant number of individuals who exited the workforce because employers offered early retirement incentive packages during this period (D'Angelo et al., 2024). Furthermore, long-COVID-19 may add additional nuance when considering the connection between chronic disease and retirement planning. As the data and theory surrounding long-COVID-19 continues to evolve, future research should explore its implications more deeply. In addition, continued research should examine the role of workplace flexibility and employer-initiated retirement incentives as important factors influencing retirement decisions in the post-pandemic era.
It is important to recognize that the outcome variable used in this study reflects respondents planned retirement age, which may be shaped by both voluntary and involuntary factors. For example, some individuals may plan to stop working due to poor health or caregiving responsibilities, even if they do not view that decision as traditional “retirement”. Future research should strive to disaggregate different motivations for retirement when more granular data becomes available.
Despite these limitations, this study contributed to the literature by providing empirical evidence on the association between individuals’ subjective and objective health and planned retirement age. Additionally, this study also revealed racial/ethnic disparities on retirement planning. This study found that people with better self-rated health plan to retire at older ages. Chronic disease was not associated with planned retirement age; however, it was significantly related to earlier planned retirement among Hispanic adults, with only a marginal trend observed for non-Hispanic Black adults. The results of this study help to inform employers that they may need to be concerned about employees’ health and provide appropriate support to help employees with relatively poor health. The government, at the federal and state levels, may also promote educational and awareness programs to support healthy aging and early planning for retirement so that older people who want to keep working are not forced to retire because of poor health.
Supplemental Material
Supplemental Material - Chronic Diseases, Self-Rated Health, and Planned Retirement Age: The Moderating Role of Race and Ethnicity
Supplemental Material for Chronic Diseases, Self-Rated Health, and Planned Retirement Age: The Moderating Role of Race and Ethnicity by Yan-Jhu Su, Andrew G. Alberth, Alison Rataj, Elisabeth J. Stam, Jeffrey Stokes, Shu Xu in Research on Aging
Footnotes
Acknowledgments
The authors thank Dr. Elizabeth Dugan and Dr. Qian Song for their expertise and assistance throughout the writing and analyses in our study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are public data from the Health and Retirement Study (HRS).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.