
Abstract
This study investigates the associations between distinct childhood stressors (i.e., health threats, financial hardship, and interpersonal trauma) and cardiovascular diseases (CVD) in later life, with a focus on loneliness as a mediator and the moderating roles of family and friend support. Cross-sectional data were used in this study, including 5,007 Hong Kong residents aged 50 and above. CVD was assessed via self-reported diagnoses of heart diseases or stroke. All three childhood stressors were associated with increased CVD risk in old age, with loneliness significantly mediating these associations. Friend support consistently buffered the effects of all stressors on loneliness, whereas family support was protective only in case of financial hardship. These findings advance understanding of the psychological pathways connecting childhood stress to CVD. It highlights that the efficacy of social support varies based on the type of social relationship and stressor domain, rather than serving as a generic buffer.
Introduction
Cardiovascular diseases (CVD) remain the leading cause of mortality worldwide (World Health Organization, 2021a). In Hong Kong, heart diseases ranked as the third most common cause of death, accounting for 13% of all deaths in 2020 (Department of Health HKSAR, 2022). Notably, older adults face an increased risk of CVD due to age-related deterioration in cardiovascular functionality (Seki & Fishbein, 2022). With aging, the prevalence of diagnosed ischemic heart disease drastically increases from 0.01% among individuals aged 15-24 to 7.7% among those aged 85 or above in Hong Kong (Department of Health HKSAR, 2022). Beyond personal health consequences, the burden of CVD extends to aged care services and hospitalization costs within health systems (Hsu et al., 2021). Given these substantial societal and economic impacts, it is imperative to understand the risk factors associated with CVD to promote cardiovascular health among older adults.
From the perspective of life course epidemiology, diseases in later life are viewed as the result of long-term influences originating from early-life events (Kuh et al., 2003). Childhood stress, encompassing chronic exposures to adverse experiences, has been identified as a potential trigger for major cardiac events (Smith & Pollak, 2020). Cumulative childhood stressors, such as famine, maltreatment, and parental death, are recognized as independent risk factors for CVD in later life (Lei et al., 2020; Zhang & Lu, 2021). Although a substantial body of research has documented associations between childhood stress and adult cardiovascular outcomes, comparatively fewer studies have explicated the specific psychological mechanisms linking childhood stress to CVD in old age. In particular, traumatic childhood experiences have been shown to predict feelings of loneliness in adulthood (Landry et al., 2022). Loneliness, a growing public health concern among aging population, is also associated with adverse health outcomes, including cardiovascular disorders (Lee et al., 2025). Therefore, it is plausible to examine the potential psychological pathway of loneliness in the relationships between different childhood stressors and CVD.
According to stress-buffering theory, social support protects health by attenuating the impact of stress on emotional responses and psychological distress, thereby reducing downstream physiological dysregulation and illness risk (Cohen & Wills, 1985). Building on this framework, a substantial body of empirical work (Aldomini et al., 2025; Buchanan et al., 2024; Lee et al., 2024) has conceptualized social support as a moderator in the association between early-life stress and later psychological status (e.g., depression, anxiety), placing support within the stress–psychological distress link. A systematic review by Buchanan et al. (2023) further identifies social support as a robust protective factor for mental health following childhood adversity, which are known predictors of subsequent physical morbidity. Taken together, this literature suggests that social support is most often modelled as buffering how stress is psychologically processed, with physical illness outcomes emerging further downstream in the pathway. On this basis, our conceptual model focuses on the moderating role of social support in the pathway from childhood stress to loneliness, because loneliness represents a proximal psychosocial consequence of early stress that is both theoretically sensitive to social support and empirically linked to cardiovascular risk.
Despite the crucial role of social support in stress-buffering framework, most existing studies treat it as a unitary construct and pay limited attention to the potentially distinct functions of support from family members versus friends (Antonucci et al., 2014). Yet family and friend support differ systematically in typical closeness, expectations, availability, and role norms (Amati et al., 2018). For instance, in the cultural context of Chinese familism, kin-based obligations occupy a particularly central position in social and personal networks, suggesting that family support may carry unique psychological salience relative to non-kin ties (Zhou & Kang, 2025). It is therefore plausible that family support and friend support may operate differently in buffering the psychological consequences of specific childhood stress. However, research has rarely examined whether and how family and friend support differentially moderate the associations between distinct forms of childhood stress and later-life loneliness. By positioning family and friend support as moderators of the childhood stress–loneliness link, our study addresses this gap and provides a theoretically meaningful examination of the psychological pathway through which early stress may ultimately shape cardiovascular outcomes.
To provide a clear roadmap, the subsequent analysis proceeds in three stages. First, we examine the empirical associations between different forms of childhood stress and CVD to show that distinct stressors may be linked to different psychological pathways in later life. Next, drawing on the chain-of-risk model, we propose loneliness as a key psychological pathway through which childhood stress increases the likelihood of CVD. Finally, we argue that family support and friend support may exert differential buffering effects on the association between specific types of childhood stress and loneliness, thereby conditioning the indirect psychological pathway from childhood stress to CVD risk.
Different Childhood Stress and CVD in Later Life
The perspective of life course epidemiology posits that exposure to childhood stress induces long-term maladaptive physiological dysregulation (e.g., cardiometabolic changes) that undermines cardiovascular health across the life span (Johnson-Lawrence et al., 2015). According to Chiang et al. (2022), childhood stressors can be broadly classified into three dimensions: health threats, financial deprivation, and interpersonal trauma. Previous studies have consistently documented significant associations between socioeconomic disadvantage (Falkstedt et al., 2011), abusive experiences (Chen et al., 2023), and poor health conditions during childhood (Zhang & Lu, 2021) and elevated cardiovascular risk in later life. However, different types of childhood stress appear to be linked to CVD through partially distinct psychological pathways. For instance, Chen et al. (2026) distinguishes the influences between threat-related and deprivation-related childhood stress on CVD in the Chinese context, showing that threat-related experiences primarily via emotion dysregulation, whereas deprivation-related experiences are more closely tied to reduced perceived control and adoption of unhealthy behaviors as coping strategies. Moreover, the association between childhood abuse and CVD has been shown to be largely mediated by anxiety and depression (Soares et al., 2022). These findings underscore the need to differentiate subtypes of childhood stress with specific psychological pathways that shape cardiovascular outcomes in later life.
Loneliness as a Mediator Between Childhood Stress and CVD
The chain of risk model, widely utilized in life course epidemiology, elucidates how cumulative exposures across developmental stages shape health outcomes in later life (Kuh et al., 2003; Surachman et al., 2019). This model posits that interconnected exposures throughout the life course contribute to the development of disease in old age (Kuh et al., 2003; Tsang et al., 2025). Each exposure to a risk factor increases the likelihood of subsequent exposures to additional experience in a sequential manner (Hendricks, 2012). Within this model, we propose loneliness, a psychological state arising from perceived inadequacies in social relationships (Cacioppo & Cacioppo, 2018), as a critical mediator linking childhood stress to CVD in older adulthood.
Loneliness has emerged as a pressing global public health concern among aging populations (WHO, 2021b). In Hong Kong, for instance, 46% of older adults report persistent loneliness (Chou, 2018). Among Chinese aging adults, it has been estimated that at age 55 they anticipate spending about 7–10 remaining years feeling lonely, accounting for one-third of their residual life expectancy (Wang, 2024). Loneliness often manifests as a significant psychological consequence of stressful early-life experiences (Furuya & Wang, 2023). Childhood stressors, such as emotional neglect, abuse, or chronic illness, impair the development of stable social bonds and effective emotional regulation (Lahousen et al., 2019; Parvin et al., 2024), therefore fostering enduring feelings of loneliness in later life. Additionally, research indicates that poor socioeconomic status in childhood increases psychosocial sensitivity, making individuals more vulnerable to feel lonely in later life (Kamiya et al., 2014).
Empirical studies demonstrate that loneliness is an independent risk factor for CVD. A recent two-cohort study shows that loneliness predicted incident CVD, with lonely older adults having approximately a 15–16% higher risk of developing CVD in both the USA and South Korea (Lee et al., 2025). Similarly, research from the United Kingdom (Bu et al., 2020) and Australia (Hu et al., 2021) reveal that higher levels of loneliness were associated with increased risks of CVD diagnoses (e.g., heart disease and stroke) and CVD-related hospital admission among older people. A review study further synthesizes that loneliness has been linked to higher rates of incident CVD and poor CVD patient outcomes (Paul et al., 2021). Given the existing evidence linking childhood stress to loneliness, and loneliness to CVD, it is essential to examine the mediating role of loneliness in the relationship between childhood stress and CVD. Therefore, a comprehensive investigation of the associations among childhood stress, loneliness, and CVD is warranted and timely.
Buffering Role of Family Support and Friend Support
Previous empirical research predominately focuses on the buffering effects of general social support, overlooking the nuanced roles of support sources (e.g., family vs. friends) in attenuating stress (Yuh & Choi, 2017). According to the task specificity model (Cantor, 1979), the effectiveness of social support in buffering stress contingent on how well the support aligns with the functional demands of the stressor (e.g., emotional, financial, and instrumental needs). In Chinese societies, where kinship and filial obligations are deeply rooted, family has been traditionally viewed as the core support system for older adults (Zhou & Bai, 2022), primarily providing instrumental and financial aid (Thomas et al., 2017; Zhou & Kang, 2025). For instance, family support has been shown to ameliorate depressive symptoms in older adults facing hospitalization, illustrating its protective role under health-related stress (Shulyaev et al., 2024). Conversely, friendships, typically formed through voluntary choices and shared interests or values, are more effective in addressing emotional needs (Amati et al., 2018).
Building on this perspective, we propose that family and friend support differentially moderate the psychological pathway linking childhood stressors to loneliness, and in turn, buffer CVD risk in later life. Distinct childhood stressors may require different forms and sources of support to alleviate their long-term socioemotional consequences. Childhood interpersonal trauma, for example, can disrupt trust and attachment security, and thus may require highly sensitive, emotionally attuned support from close relationships to offset its enduring effects on loneliness (Zhou & Zhou, 2024). Health-related threats in childhood may create ongoing vulnerability, making instrumental help from family and inclusive opportunities with peers especially relevant (Thomson et al., 2016). Financial hardship, in turn, often generates both material strain and social stigma, requiring a combination of tangible assistance and emotional validation from both family and friends (Secor et al., 2017).
Emerging empirical work supports this stressor–support specificity. Family support has been found to buffer psychological symptoms among socioeconomically disadvantaged adolescents by enhancing self-efficacy (Qian et al., 2024), and sustained family caregiving has been shown to buffer mental health problems in children with neurodevelopmental disabilities (Helson et al., 2024). While Amati et al. (2018) uncovered that childhood trauma often erodes trust within familial bonds, thereby positioning friends as primary emotional buffers. Recent research suggests that friend support may exert reverse buffering effects, whereby the association between interpersonal stress and loneliness is stronger when friends are primary source of support (Kim & Jung, 2025). Taken together, these findings suggest that family and friend support may differentially moderate the extent to which childhood stressors translate into loneliness later in life, thereby conditioning the indirect psychological pathway from childhood stress to CVD risks. Nevertheless, no study has systematically compared the buffering effects of family and friend support across distinct childhood stressors. This gap limits the development of tailored strategies that utilize the specific strengths of different support sources.
The Present Study and Research Hypotheses
Guided by life course epidemiology and the chain of risk model, this study proposes a conditional process framework to investigate how childhood stressors (i.e., health threats, financial hardship, and interpersonal trauma) shape CVD in later life through psychological pathways. Unlike prior research that often treats social support as a unitary construct, this study makes two key contributions: First, it examines loneliness as a critical psychological mediator, bridging early-life stressors to CVD in later adulthood. Second, it compares the differential moderating roles of family and friend support, grounded in the task specificity model, thereby clarifying how distinct support sources condition the stress–loneliness pathway.
The conceptual and analytical framework is presented in Figure 1 as a moderated mediation (conditional process) model. We hypothesize that (1) childhood stressors are associated with an increased risk of CVD in later life, with loneliness serving as a significant mediator (i.e. childhood stressors → higher loneliness → higher CVD risk); and (2) family and friend support differentially moderate the associations between specific childhood stressors and loneliness, such that higher levels of family or friend support attenuate (buffer) the positive association between childhood stress and loneliness, leading to weaker indirect effects of childhood stress on CVD through loneliness at higher levels of support. By integrating life course theory with stress buffering mechanisms within a conditional process framework, this study addresses critical gaps in understanding how different relational resources shape the psychological pathways from childhood stress to CVD. The findings are expected to inform targeted support models that align specific sources of support with particular types of stressors to more effectively reduce loneliness and, ultimately, CVD risk in aging populations. Conceptual framework of the study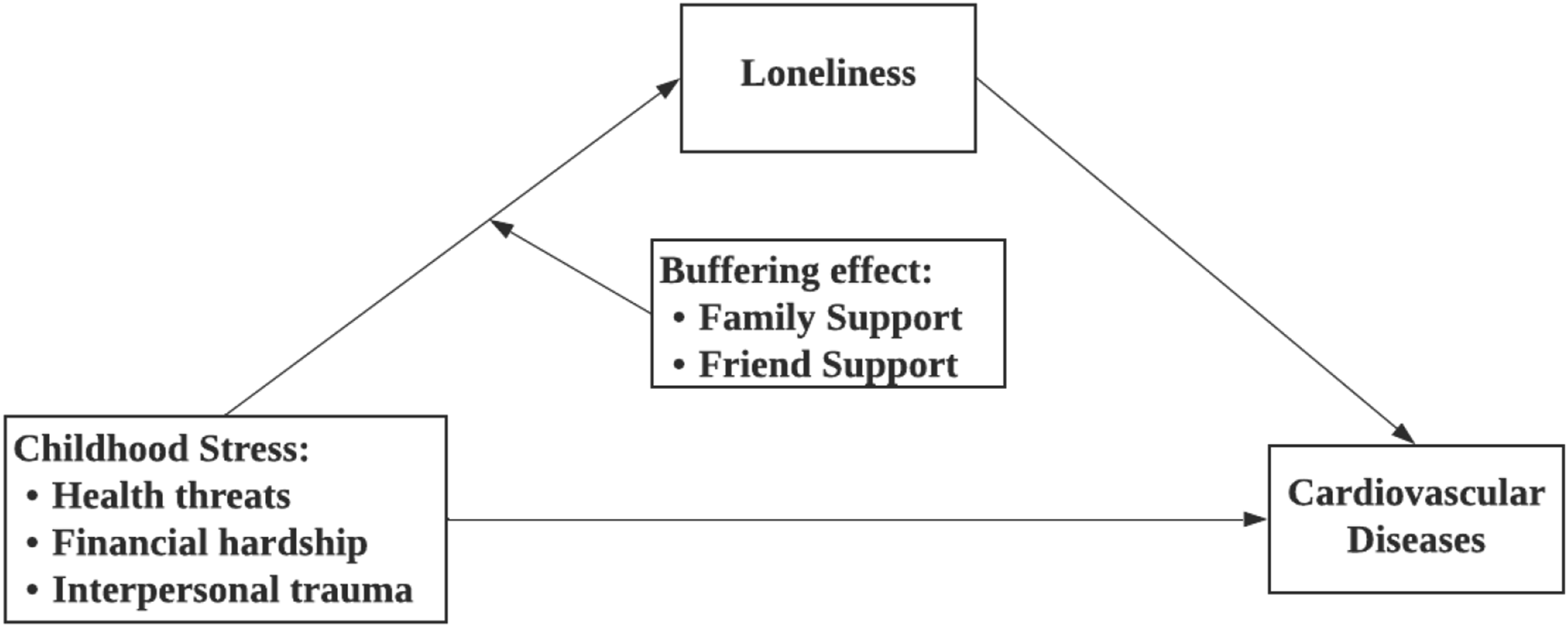
Method
Participants and Data Collection
This study employs a quantitative cross-sectional design. Data were used from the first wave of the Panel Study of Active Ageing and Society (PAAS) (Bai, Zhou, et al., 2025), which is a longitudinal and representative survey among adults aged 50 years and over in Hong Kong. The records of the sample were identified based on age and gender by using the frame of quarters from the Hong Kong Census and Statistics Department. Participants were evenly stratified by the age groups of 50-64 and 65 and over, with the proportion of respondents in each age-sex-district stratum determined by the population census data in 2021. After eliminating invalid and non-responsive numbers, 8,303 valid phone numbers were identified.
Data was collected through telephone surveys from June 2022 to November 2022. As the second wave of PAAS data collection is expected to be completed in 2026, only first-wave cross-sectional data are used in this study. Ethical approval was obtained from the institutional review board of the third author’s affiliated university (ethics approval number: HSEARS20220517001), and respondents’ informed consents were collected prior to the interview. Trained researchers conducted interviews with eligible respondents under on-site supervision using Web-based Computer Assisted Telephone Interview (Web-CATI). In this study, the analytical sample comprised 5,007 older adults who completed the interview out of 8,303 eligible respondents, corresponding to a response rate of 60.30%. The 3,296 unsuccessful cases included non-contacts (after at least five attempted calls) and refusals.
Measures
Outcome variable—Cardiovascular diseases were principally manifested as ischemic heart disease and stroke (Ammirati et al., 2020). Hence, CVD events were assessed by self-reported doctor-diagnosed heart diseases and stroke in this study. Respondents were queried with two questions: “Have you ever been informed by a doctor that you have been diagnosed with heart diseases?” and “Have you ever been informed by a doctor that you have been diagnosed with a stroke?” Respondents who indicated the presence of either heart diseases or stroke were identified as having CVD (1), and all others were coded as having no CVD (0).
Independent variable—Childhood stress encompasses three categories: health threats, financial hardship, and interpersonal trauma (Chiang et al., 2022). Health threats were measured by the presence of poor health status or serious illness experienced by participants before the age of 14. Financial hardship was assessed based on the occurrence of famine or a poor family economic status. Interpersonal trauma was indicated by any of the following events: death of a parent (7.61%), poor relationships with a parent or caregiver (8.73%), frequent physical abuse (4.41%), or frequent emotional abuse (1.2%). Each type of childhood stress was coded as a binary indicator denoting the presence versus absence of health threats, financial hardship, and interpersonal trauma.
Mediator—Loneliness was assessed by the UCLA 3-item Loneliness Scale (Hughes et al., 2004). Participants were asked to rate the frequency at which they experienced the following three situations: (1) feeling a lack of companionship, (2) feeling left out, and (3) feeling isolated from others. Each statement was rated on a three-point Likert scale, ranging from 1 (hardly ever) to 3 (often). The total score ranged from 3 to 9, with a higher score indicating a greater level of loneliness. Internal consistency for the loneliness scale was satisfactory in this study, with the Cronbach’s alpha of 0.86. Although previous research suggests that loneliness levels vary across the lifespan (Mund et al., 2019), loneliness in our study is assessed in later life, when mean-level loneliness tends to be stable, and thus can be interpreted as a more enduring psychosocial state relevant to cardiovascular risk.
Moderators—Family support and friend support were assessed using the 6-item Lubben Social Network Scale (LSNS-6) (Cohen et al., 2000), which captures the structural dimension of social support by quantifying network size. For each domain, respondents were asked about how many families (e.g., spouse, children, parents) and, separately, how many friends they (1) “hear or see from at least once a month”, (2) “feel at ease with and can talk about private matters”, and (3) “can call for help”. Each item was rated on a six-point Likert scale from 1 (none) to 6 (nine or more). Total scores for family support and friend support were obtained by summing the scores of the three items for each dimension, resulting in separate total scores ranging from 3 to 18, with higher scores indicating larger and more supportive networks. The Cronbach’s alpha was 0.87 for both family support and friend support in this study, indicating satisfactory internal consistency.
Control Variables
Following previous studies (Bai, Cai, et al., 2025; Bai, Zhou, et al., 2025; Zhou & Zhou, 2024), we adjusted for a set of demographics, socioeconomic, and health-related variables to improve the precision of the estimation. Control variables included age (50–95 years), gender (1 = female, 0 = male), marital status (1 = married, 0 = divorced, never married, cohabiting, widowed), educational attainment (1 = illiterate, 2 = primary school, 3 = junior high school, 4 = high school, 5 = diploma and above), and self-perceived economic class (1–5, with higher scores indicating higher class). In addition, we also controlled variables related to health behaviours and health insurance, including smoking (1 = yes, 0 = no), drinking (1 = yes, 0 = no), doing aerobic exercise in the past month (1 = yes, 0 = no), and having health insurance (1 = yes, 0 = no).
Data Analyses
Firstly, descriptive and bivariate analyses were conducted to characterize the sample and to compare participants with and without CVD on key study variables. Subsequently, to examine the mediating role of loneliness, we applied the Karlson–Holm–Breen (KHB) method (Karlson & Holm, 2011) to decompose the total association between each childhood stressor and CVD into direct and indirect components through loneliness. This approach yielded scale-corrected estimates of direct and indirect effects and the proportion of the total effect of each childhood stressor on CVD statistically accounted for by loneliness.
To assess the moderating role of family support and friend support in the pathway between childhood stressors and loneliness, we estimated a series of moderated mediation models. For each childhood stressor, we first fitted linear regression models predicting loneliness from the stressor, family support, friend support, and their interaction terms (stressor × family support, stressor × friend support), adjusting for all covariates. No substantial skewness was observed for the moderating variables, supporting the statistical power and interpretability of the interaction estimates. All continuous variables included in interaction terms were meancentered to reduce multicollinearity. When an interaction term was statistically significant, we probed the interaction by plotting simple slopes and estimating the association between the childhood stressor and loneliness at low (−1 SD), mean, and high (+1 SD) levels of family or friend support.
Building on these first-stage moderation results, we then examined conditional indirect effects of childhood stressors on CVD through loneliness at different levels of relational support, that is, a moderated mediation (conditional process) model (Hayes, 2022). For each childhood stressor, we combined (a) the stressor → loneliness path (including its interaction with family/friend support) with (b) the loneliness → CVD path from the logistic regression model predicting CVD, and computed the indirect effect at specified values of the moderator (e.g., low, medium, and high family/friend support). This allowed us to quantify how the strength of the psychological pathway from childhood stress to CVD via loneliness varies according to the level of family or friend support, in line with our stress-buffering conceptual model. All statistical analyses were conducted using Stata 16.
Results
Descriptive Analysis and Bivariate Analysis (N = 5,007)
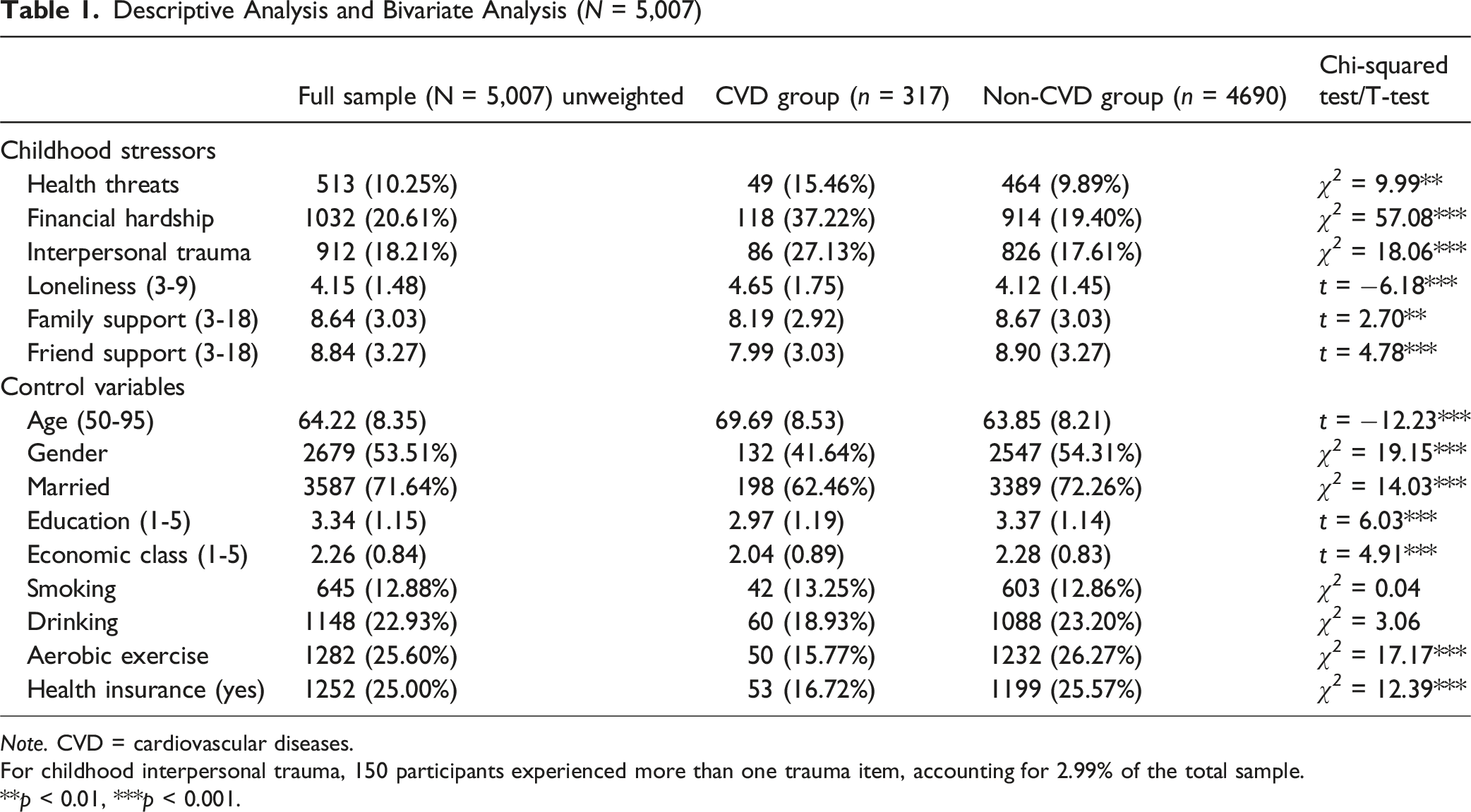
Note. CVD = cardiovascular diseases.
For childhood interpersonal trauma, 150 participants experienced more than one trauma item, accounting for 2.99% of the total sample.
**p < 0.01, ***p < 0.001.
A total of 317 aging adults in this study were diagnosed with CVD, accounting for 6.33% of the full sample. The prevalence rates for experiencing childhood health threats, financial hardship, and interpersonal trauma were 10.25%, 20.61%, and 18.21% respectively. Respondents with a CVD diagnosis were more likely to report all types of childhood stressors compared to the Non-CVD group. The mean loneliness score was 4.15 (SD = 1.48) out of 9. The average scores for family support and friend support were 8.64 (SD = 3.03) and 8.84 (SD = 3.27), respectively. Bivariate analyses show that the CVD group reported higher levels of loneliness (mean = 4.65, SD = 1.75) than those without CVD (mean = 4.12, SD = 1.45; t = −6.18, p < 0.001), as well as lower levels of family support (mean = 8.19, SD = 2.92 vs. mean = 8.67, SD = 3.03; t = 2.70, p < 0.01) and friend support (mean = 7.99, SD = 3.03 vs. mean = 8.90, SD = 3.27; t = 4.78, p < 0.001) compared to their counterparts.
Total, Direct, and Indirect Effects of Different Childhood Stressors on CVD via the Mediation of Loneliness (N = 5,007)
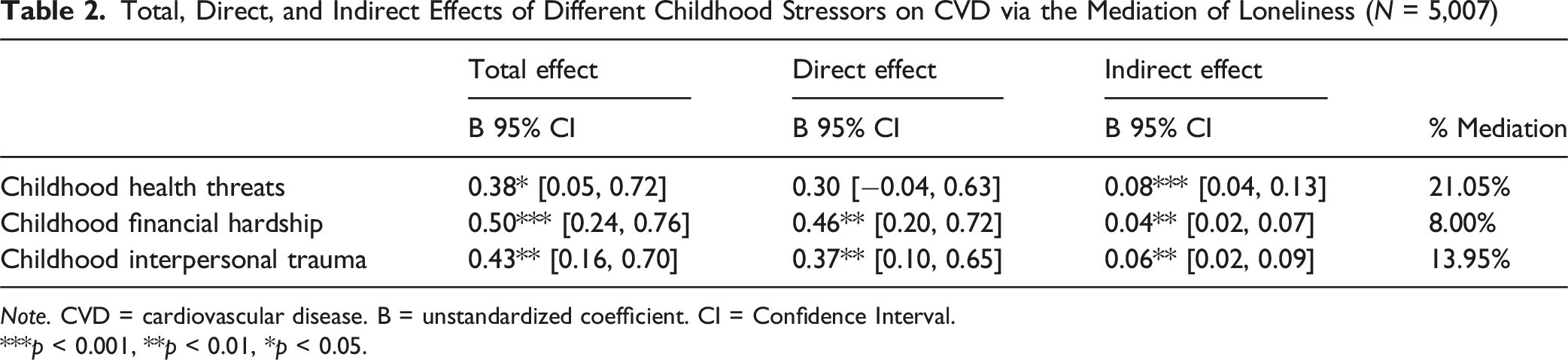
Note. CVD = cardiovascular disease. B = unstandardized coefficient. CI = Confidence Interval.
***p < 0.001, **p < 0.01, *p < 0.05.
Moderation Effect of Family Support and Friend Support on the Relationships Between Childhood Stress Categories and Loneliness (N = 5,007)
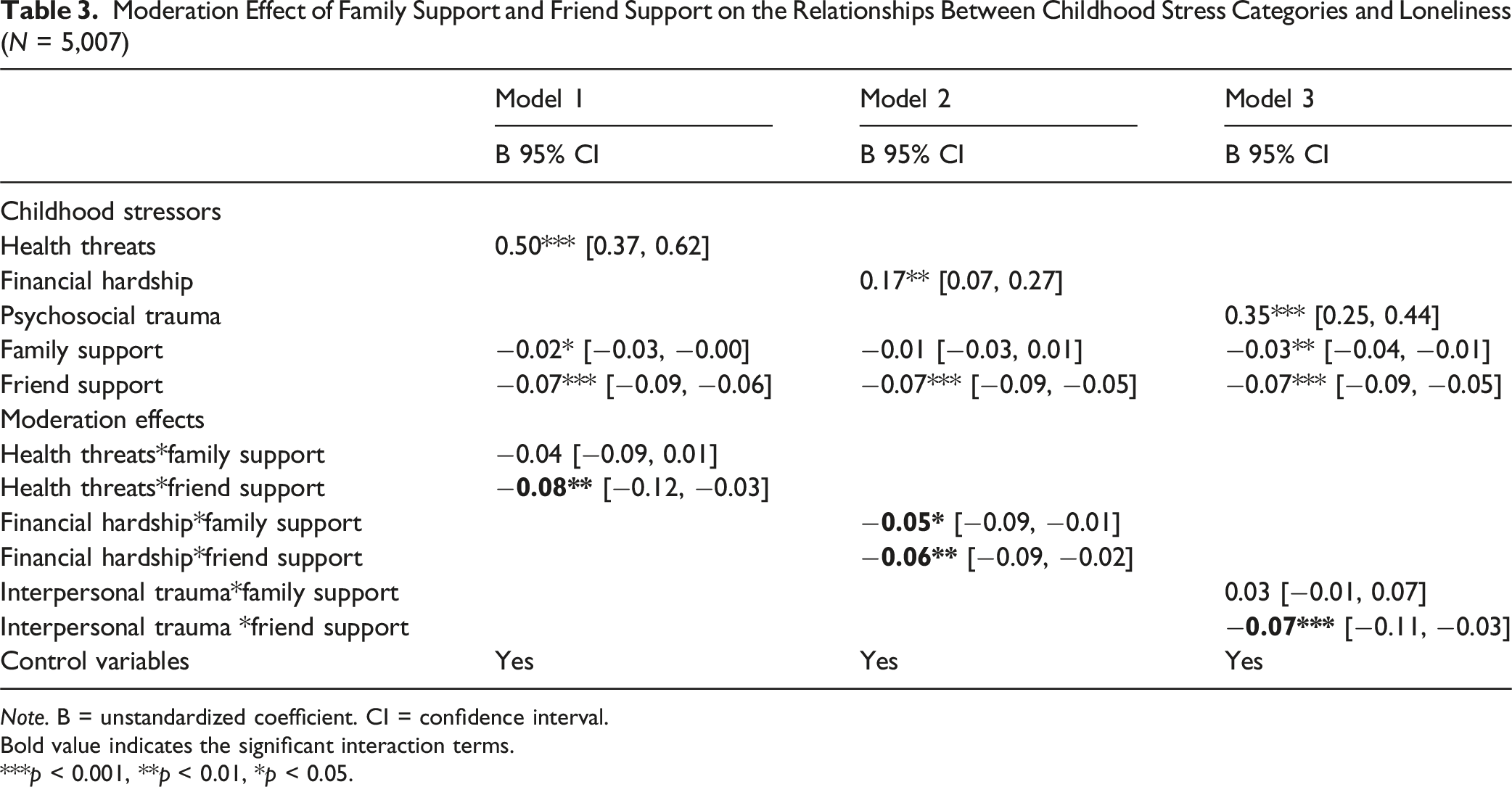
Note. B = unstandardized coefficient. CI = confidence interval.
Bold value indicates the significant interaction terms.
***p < 0.001, **p < 0.01, *p < 0.05.
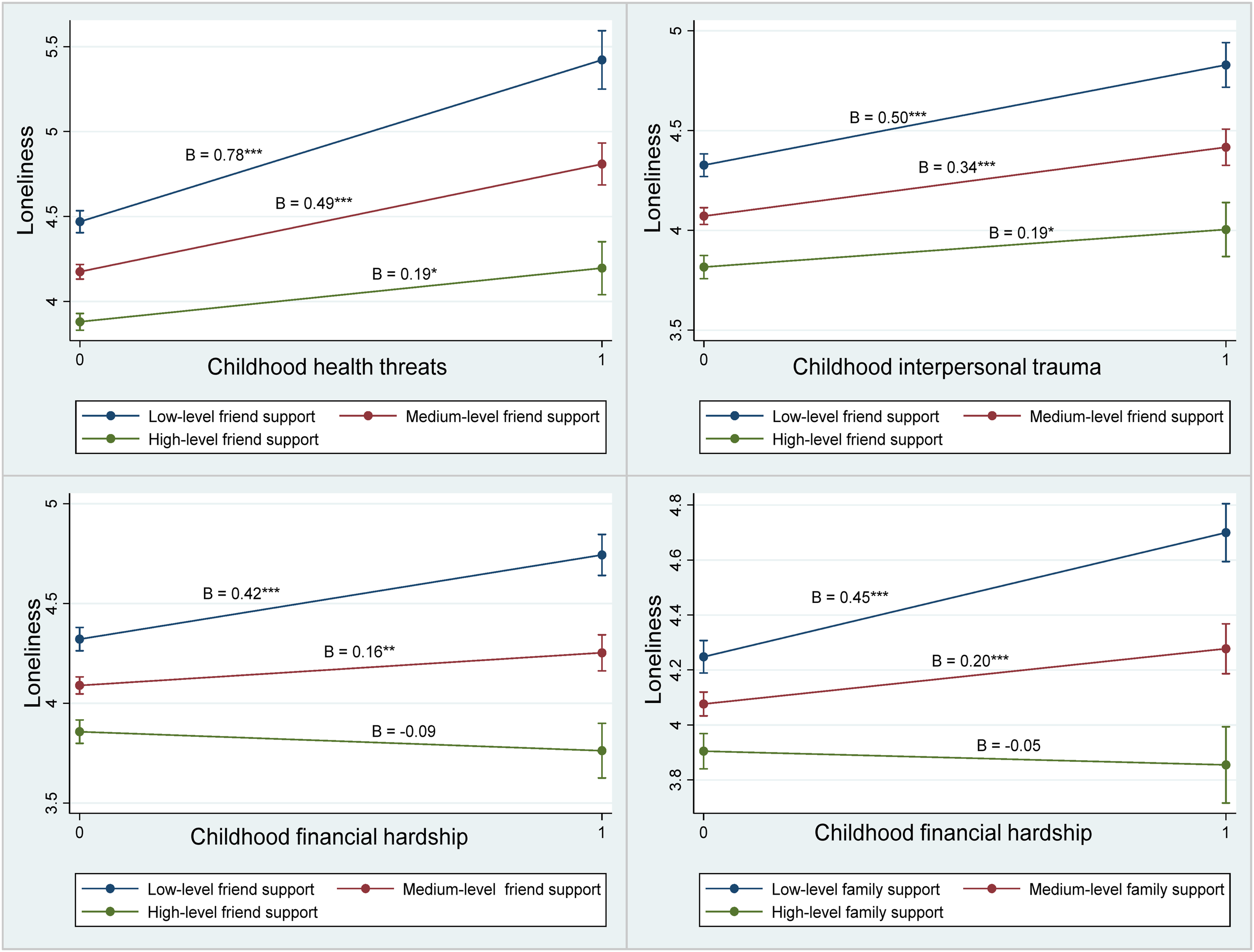
The associations between childhood stressors and loneliness at different levels of friend support and family support.
Conditional Indirect Effects of Childhood Stressors on CVD at Different Levels of Friend Support and Family Support (N = 5,007)
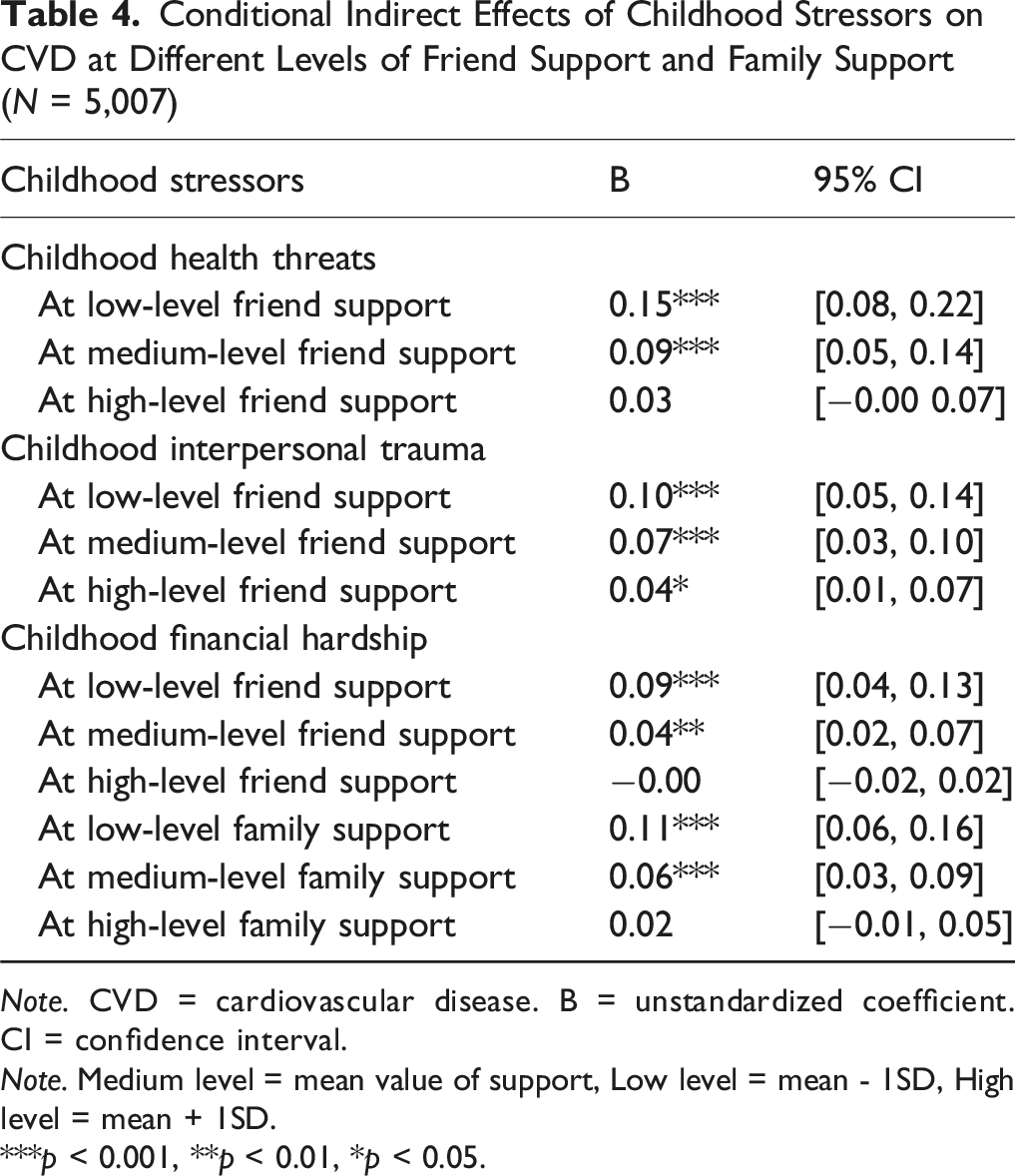
Note. CVD = cardiovascular disease. B = unstandardized coefficient. CI = confidence interval.
Note. Medium level = mean value of support, Low level = mean - 1SD, High level = mean + 1SD.
***p < 0.001, **p < 0.01, *p < 0.05.
Discussion
This study advances life course epidemiology by classifying how childhood stressors shape CVD risk through a moderated mediating process within in an integrated framework. We conceptualize loneliness as a psychological pathway linking early-life stress to later CVD, and family and friend support as relational buffers that condition the strength of this pathway. Three key innovations emerge from this study: First, we identify loneliness as a critical mediator that connects distinct early-life stressful events to CVD, thereby extending previous work that primarily focused on overall stress-CVD relationship. Second, we demonstrate that different sources of social support are not interchangeable in buffering the effects of childhood stressors: support from friends consistently ameliorates loneliness across all three types of stress, while family support is particularly effective in the context of financial hardship. These findings challenge traditional assumptions about the primacy of family in Chinese society and underscores the underrecognized role of friend support in recovery from trauma and health-related stress. Third, by integrating moderation (loneliness) and mediation (family/friend support) with stressor-specific analyses, we provide a more nuanced framework of how relational support intersect with life course stress. In other words, family and childhood support shape how strongly childhood stress translates into loneliness, which in turn carries forward to CVD risk. These contributions inform insights for designing programs that align particular sources of support with specific childhood stress, to improve cardiovascular health in older adults.
This study demonstrates that childhood stressors are associated with an increased risk of developing CVD in later life, which is consistent with previous findings (Zhang & Lu, 2021). Aligning with the chain of risk model (Kuh et al., 2003), our results reveal a significant mediating role of loneliness in the relationship between various forms of childhood stress and CVD. Echoing the work of Furuya and Wang (2023), we find that individuals exposed to stressful events in childhood are more likely to experience difficulties in meeting their social and emotional needs in later life. This unmet need manifests as loneliness, which, in turn, elevates the risk of CVD. Notably, this study is the first to explicitly investigate the psychological pathway of loneliness as a mediator connecting early-life stressors to CVD risk in old age, thereby advancing our understanding of the mechanisms underlying the long-term health consequences of childhood stress.
By comparing the protective roles of family support and friend support in buffering childhood stressors, our study highlights the unique capacity of friend support to moderate all three stressors against loneliness. Friendships are typically voluntary relationships rooted in shared interests, values, and mutual respect, fostering a greater sense of emotional companionship compared to familial bonds (Amati et al., 2018). These relational dynamics enable friends to provide consistent validation and social engagement, directly counteracting feelings of loneliness that arise from stressful experiences (Secor et al., 2017). For instance, by fostering identity continuity and belonging, friend support can help reframe traumatic narratives, thereby reducing isolation-driven psychological distress (de Moor et al., 2021). Additionally, friend support also facilitates the reconstruction of social networks for those experienced illness-related social exclusion. These findings contribute to the existing literature by emphasizing the importance of social networks beyond familial ties. It underscores the need for targeted grograms that promote peer relationships as a vital component of mental health strategies for individuals with a history of childhood stress.
Family support emerged as a significant moderator against loneliness only for individuals who experienced childhood financial hardship. This finding aligns with the well-established role of families in providing material assistance during economic adversity (Qian et al., 2024; Wu et al., 2023). By contrast, family support did not attenuate loneliness stemming from childhood illness or interpersonal trauma. One plausible interpretation, supported by qualitative evidence in Chinese contexts (Chen et al., 2013; Lee et al., 2024), is that when early stressors centered on disrupted health or trust, family ties may become ambivalent sources of support—offering caring while being emotionally constrained by obligations, stigma, or “face saving” norms, which may limit open disclosure and emotional processing. In such circumstances, friends and other non-kin may be better positioned to provide nonjudgmental companionship and conversational space that validates feelings and facilitates the re-interpretation of difficult experiences to alleviate loneliness (Sánchez-Moreno et al., 2025; Woodward et al., 2024). In Chinese communities, friendship-based support embedded in community engagement has also been shown to reduce loneliness through high-quality, trusting peer relationships (Xie et al., 2023).
The findings of this study have significant implications for societal strategies aimed at improving cardiovascular health among aging adults. First, the positive association between childhood stress and CVD in later life underscores the need for prevention strategies that reduce cardiovascular risk beginning in early life by fostering supportive and nurturing childhood environments (e.g., parenting and support programs, chronic care programs). Furthermore, childhood stress history can be incorporated into geriatric assessments for middle-aged and older adults, helping identify “hidden” social determinants that underlie conventional cardiovascular risk profiles in aging populations. Second, this study identifies loneliness as a critical risk factor mediating the relationship between childhood stressors and CVD in older age. Accordingly, there is an urgent need to implement measures that alleviate loneliness among older adults. Such programs may include social skills training, community support groups, and the development of age-friendly digital platforms to help isolated older individuals maintain meaningful social connections. Third, our research provides evidence on how different relational support can be optimized to reduce both loneliness and CVD risk across the life course. For example, public health campaigns should be expanded to promote friendship-building across all ages, particularly for survivors of childhood stress. Additionally, family-based initiatives, such as subsidized financial counseling and debt-relief programs, should be targeted toward those affected by financial deprivation in childhood.
Limitations
Several limitations should be noted in this study. First, although the study is informed by a life course perspective, the use of cross-sectional data does not allow us to capture the trajectories of psychosocial processes and CVD outcomes over time. This design may restrict the ability to establish causal relationships between childhood stressors, loneliness, and CVD in later life. Future research should employ longitudinal data to track changes in loneliness and cardiovascular health to more rigorously examine life course pathways. Second, reliance on retrospective reports of childhood stress introduces the possibility of memory bias. However, previous evidence has confirmed the reliability of retrospective measures in predicting cardiovascular risk (Lei et al., 2020), suggesting that the impact of recall bias on the study’s findings may be minimal. Third, this study used data from older adults in Hong Kong, and the identified relationship between childhood stressors, loneliness, CVD, and relational support may not be generalizable to other sociocultural or healthcare contexts.
Conclusion
This study advances our understanding of the long-term pathways linking childhood stressors to CVD risk in later life by highlighting the mediating role of loneliness and the moderating effects of different relational support. Our findings demonstrate that while family support effectively buffers the impact of childhood financial hardship on loneliness, friend support uniquely ameliorate loneliness across a broader range of childhood stressors. These results refine the task specificity model by illustrating that the buffering efficacy of social support is contingent upon both the type of stressor and the nature of the support relationship. Importantly, the study underscores the need for targeted approaches that address loneliness and leverage appropriate relational resources across the life course. By elucidating these nuanced mechanisms, our research provides a foundation for more precise relational strategies aimed at reducing CVD risk among aging adults, particularly those with histories of early-life stress.
Footnotes
Acknowledgments
The authors would like to express gratitude to all the participants in the study.
Ethical Consideration
Ethical approval was obtained from the institutional review board of the third author’s affiliated university (Reference number: HSEARS20220517001).
Consent to Participate
Respondents’ consent to participation were collected prior to the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZeShan Foundation; The General Research Fund from the Research Grants Council of the Hong Kong Special Administrative Region, China (grant number: 15613022); and The Hong Kong Polytechnic University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data of this study are available from the corresponding author upon reasonable request.