
Abstract
Spouses often influence each other’s health behaviors through social control, yet most research relies on cross-sectional data from different-sex couples. Far less is known about how these dynamics unfold in same-sex marriages or evolve with age, despite their importance for population health. Using longitudinal survey data (n = 614) and daily diary data (n = 524) from mid-to-later-life same- and different-sex couples, we track six-year changes in social control tactics, reactions, and effectiveness. Supportive tactics decline, appreciation decreases, and irritation increases across couple types, although women married to women initially report greater appreciation. Over time, however, they experience the steepest declines in appreciation and the effectiveness of direct regulatory control. In contrast, joint health activities grow more effective for encouraging exercise across couples. These findings highlight the limits of regulatory control and the potential importance of collaborative approaches, with implications for interventions aimed at supporting healthy aging in diverse couples.
Introduction
Legal recognition of marriage has improved health for gay and lesbian couples (Reczek et al., 2017), yet sexual minority disparities in stress and health persist in later life (Lampe et al., 2024). Understanding marital dynamics that promote health is therefore essential for supporting aging sexual minority populations (National Academies of Sciences, Engineering, and Medicine [NASEM], 2020). Marriage improves health in part because spouses monitor and regulate each other’s health behaviors—a process known as social control (Lewis & Butterfield, 2007). Most spouses in gay, lesbian, and straight marriages report engaging in social control (Umberson et al., 2018), yet women are more likely than men to serve as agents of control in both different-sex couples (August & Sorkin, 2010; Markey et al., 2008) and same-sex marriages (Umberson et al., 2018).
The gender gap in social control may shift as couples age. Women are more likely to provide care to aging spouses even while facing their own health challenges (Thomeer et al., 2015), and more likely to view themselves as managers of family health (Reczek et al., 2018), which may make them less receptive to having their own behaviors managed. Yet, gendered patterns of social control may unfold differently for aging gay, lesbian, and heterosexual couples. Although same-sex spouses face higher levels of stress, they often display greater similarity in health habits (Holway et al., 2018), more reciprocity in health-related regulation (Umberson et al., 2018), and more equality in caregiving (Umberson et al., 2017), while different-sex couples are characterized by more partner inequality. Yet prior studies have not examined whether the frequency, reception, or effectiveness of social control change over time—or whether these dynamics differ for same-sex and different-sex couples. This gap is critical, given that social control is linked to improved health habits (Craddock et al., 2015), and that LGBTQ + older adults often contend with minority stress and healthcare inequities that heighten health risks (Fredriksen-Goldsen et al., 2023; Lampe et al., 2024).
Because most existing studies are cross-sectional (Scholz et al., 2021), they offer only snapshots and cannot capture how social control changes as spouses age. Longitudinal data—especially rare for same-sex couples (NASEM, 2020)—are essential as spouses develop age-related health conditions that increase the salience of social control (Burke & Segrin, 2017; Tucker et al., 2024). We analyze a longitudinal dataset of mid-to-later-life same- and different-sex spouses with two waves of survey and diary data collected six years apart. The two types of data address different questions about social control for mid to later life couples. The survey data allow us to consider how social control dynamics (types and amount of social control, reactions to social control) change over six years. The diary data allow us to consider how daily fluctuation between social control and a spouse’s health habits changes over the six-year period—shedding light on change in the potential effectiveness of social control in relation to a spouse’s health behavior. Dyadic data which include both spouses in same-sex and different-sex couples are uniquely suited to addressing how these relationship dynamics compare for men and women in same- and different-sex marriages.
Background
Marriage, Health, and Sexual Minority Populations
Marriage benefits health by providing social, emotional, and economic resources that promote longevity (Hughes & Waite, 2009; Rendall et al., 2011) and these benefits extend to same-sex as well as different-sex spouses (NASEM, 2020). For sexual minority adults, marital relationships may be particularly consequential because they occur in the context of persistent exposure to sexual minority stress (defined as the unique experiences of stigma and discrimination that sexual minority individuals face due to their sexual orientation (NASEM, 2020)) as well as health disparities across the life course (Fredriksen-Goldsen & Muraco, 2010; Lampe et al., 2024). One recent study found that although same-sex and different-sex spouses are initially similar in self-rated health, same-sex spouses experience a more significant decline over time (Wang, 2022), perhaps reflecting these challenges. In later life, many lesbian and gay adults have smaller family networks and are less likely than heterosexuals to have children to rely on for support (Reczek & Umberson, 2012), making spouses an especially important source of care and health regulation (NASEM, 2020). Spousal involvement may partially offset gaps in structural support, since LGBTQ + older adults are less likely to have access to affirming healthcare, long-term care, or public benefits (Lampe et al., 2024).
One key pathway linking marriage to health is spouses’ attempts to influence one another’s health behaviors—a process known as social control. Social control includes reminding a spouse to adopt healthier habits, changing the environment to facilitate healthier routines, and reinforcing health-promoting behaviors (Umberson et al., 2018). Such tactics, especially when direct and supportive, are associated with improvements in diet, exercise, and other health behaviors (Craddock et al., 2015). Understanding how these dynamics unfold in sexual minority marriages is essential for explaining health trajectories and improving health in aging populations.
Gendered and Relational Contexts of Social Control
Gender is a powerful structural system that leads men and women to conform to gendered scripts of care work (Thomeer et al., 2020), and social control is a form of care work that spouses perform for each other (Reczek et al., 2018). Throughout life, men and women experience different opportunities and constraints that encourage men to be stoic and independent and encourage women to attend to the needs of others (Thomeer et al., 2020). Men and women then enact gender in ways that conform to these scripts of masculinity and femininity (Calasanti & Bowen, 2006). A gender-as-relational perspective suggests that how one enacts gender further depends on whether they are interacting with a man or a woman (Thomeer et al., 2020). For example, cultural scripts that urge women to monitor the needs of others in juxtaposition to scripts that urge men to be emotionally and physically strong may result in women providing more social control to influence their spouse’s health. Spousal inequality in social control is then more apparent in different-sex relationships wherein women and men interact around a discourse of gender opposites (Thomeer et al., 2020).
For example, in heterosexual couples, women are more likely than men to monitor, manage, and provide care to their spouse in later life (Glauber, 2017), even when women feel unwell (Thomeer et al., 2015). Thus, women may be more likely than men to sustain their higher levels of care work, including social control, over time. The gender-as-relational approach suggests that cultural scripts about gender also influence women and men in same-sex couples. Among same-sex couples, women often engage in higher levels of care work than men (Umberson et al., 2017), consistent with broader patterns of caregiving. However, same-sex couples tend to show more reciprocity in the exchange of care and social control compared to different-sex couples, where equality in care work is more common (Reczek et al., 2018). For sexual minority couples, greater reciprocity may reflect egalitarian ideals, but differences between gay and lesbian couples also underscore how gender still organizes relational work in important ways.
Spouses’ reactions to social control also vary by both gender and couple type. Some reactions, such as feeling irritated, may lead to greater resistance in health behavior change whereas other reactions, such as feeling appreciative, may promote behavioral change (Rook et al., 2011; Scholz et al., 2021). Women in same-sex marriages are the most appreciative of their spouse’s health-related influence attempts and are the least likely to ignore them, whereas women in different-sex marriages are least appreciative and more likely to resist such efforts (Umberson et al., 2018). Men report similar reactions across same- and different-sex marriages but overall tend to be less appreciative than women in same-sex couples (August & Sorkin, 2010; Franks et al., 2006). These differences may help explain why social control is generally more effective in shaping men’s health behaviors than women’s (Cotter, 2012; Pollitt et al., 2020; Umberson et al., 2018). For aging sexual minority adults, these gendered and relational dynamics intersect with minority stress and health disparities, making spousal influence a potentially consequential mechanism for long-term health.
Change in Social Control Over Time
Spousal dynamics are not static; they evolve across the life course. As people age, social networks become increasingly spouse-centered (Cornwell et al., 2008), and for sexual minority adults—who may face reduced family support—close social ties are a central protective factor against the unique health disparities faced by sexual minority populations (Reczek & Umberson, 2012). This centrality suggests that social control efforts by spouses may intensify with age, as partners assume more responsibility for protecting each other’s health. Gendered patterns likely further shape these trajectories. Women may increase social control efforts more than men, given their heightened caregiving roles (Calasanti & Bowen, 2006; Glauber, 2017). In different-sex couples, caregiving inequality may exacerbate this gender divide (Reczek & Umberson, 2012). By contrast, same-sex couples may show greater balance and reciprocity over time, though, reflecting gendered patterns within relationships, women married to women are likely to exert higher levels of monitoring and influence than are men.
Reactions to social control may also shift with age. Emotional reactivity generally declines across the life course (Carstensen et al., 2011), yet women may remain more reactive to social control—both positively and negatively—than men (August & Sorkin, 2010). Among men in same-sex marriages, social control tends to occur in more situational, “on-demand” forms, consistent with cultural expectations of independence (Umberson et al., 2018). Lesbian couples, by contrast, experience more continuous monitoring and attempts at regulation, reflecting both women’s socialization and the heightened salience of spousal health for sexual minority adults with limited external support networks (Reczek & Umberson, 2012). Negative reactions could be particularly pronounced in different-sex marriages, where caregiving inequality fuels frustration perhaps especially for women who shoulder the bulk of the care work (Thomeer et al., 2015; Umberson et al., 2017). Same-sex couples, with more reciprocal exchanges, may be better buffered from such tensions as they age.
Does the Effectiveness of Social Control Change Over Time?
Although research has examined social control across different age groups, we know little about whether its effectiveness diminishes or persists as marriages endure. Given declines in emotional reactivity with age, spouses may become less responsive to influence attempts (Totenhagen et al., 2016). For aging sexual minority adults, this possibility is particularly important, since spousal efforts may represent one of the few consistent sources of health regulation. Since prior work suggests that continuously married couples are the ones who benefit most from marriage, especially in later life (Hughes & Waite, 2009), it is especially important to evaluate this dynamic for stably married same-sex couples. Decades of prior research on marital benefits, including social control, for heterosexual couples has generally focused on those who remain married, yet no comparable longitudinal studies have examined same-sex marriages over time.
Most prior research on social control effectiveness relies on short-term diary studies that capture daily fluctuations in influence and behavior (Craddock et al., 2015). While useful for understanding immediate dynamics, such studies cannot reveal whether these processes accelerate or erode across years. Because marriage benefits health through an accumulation of experiences over long periods of time (Rendall et al., 2011), it is precisely the durability of social control—and whether its effects fade—that determines its contribution to health in later life.
The Present Study
Despite the health benefits of marriage for aging sexual minority adults (NASEM, 2020), we lack longitudinal evidence on how social control evolves over time and whether its effectiveness changes. This study addresses these gaps by analyzing two waves of dyadic survey data to examine how spouses’ social control efforts and reactions change over six years, and whether these patterns differ for men and women in same- and different-sex marriages. We also use dyadic diary data (10 diary days, six years apart) to test whether the daily associations of social control with spouses’ diet and exercise behaviors remain stable, weaken, or strengthen over time, and how these trajectories vary by gender and couple type.
Method
Data
We draw on data from the Health and Relationships Project (HARP), a study of married same-sex and different-sex spouses aged 35–65 at Time 1 (T1; Umberson, 2022). Participants were recruited nationwide, with the first wave initiated in Massachusetts, the first state to legalize same-sex marriage. Using state vital records, we identified different-sex couples comparable to same-sex couples on age, relationship duration, and zip code. Seventy percent of same-sex couples and 40% of different-sex couples were recruited from state records; the remaining 30% of same-sex couples and 60% of different-sex couples were recruited through referrals from Massachusetts participants. Both spouses in each couple participated.
At T1 (2015–2016), 419 couples independently completed a 45-min online survey, and 378 couples (90%) also completed a 10-day daily diary (nightly 5–10-min surveys). In 2021–2022 (T2), 308 couples participated in the main survey (74% response rate) and 288 couples in the daily diary (69% response rate). Attrition analyses indicate that women, employed respondents, and those with higher education were more likely to participate at T2, while those with children in the household were less likely to do so. There were no attrition differences by age, sexual minority identity, self-rated health, relationship duration, social control, or desire to change a spouse’s health behaviors.
Sample Descriptives at Time 1 (T1) and Time 2 (T2)
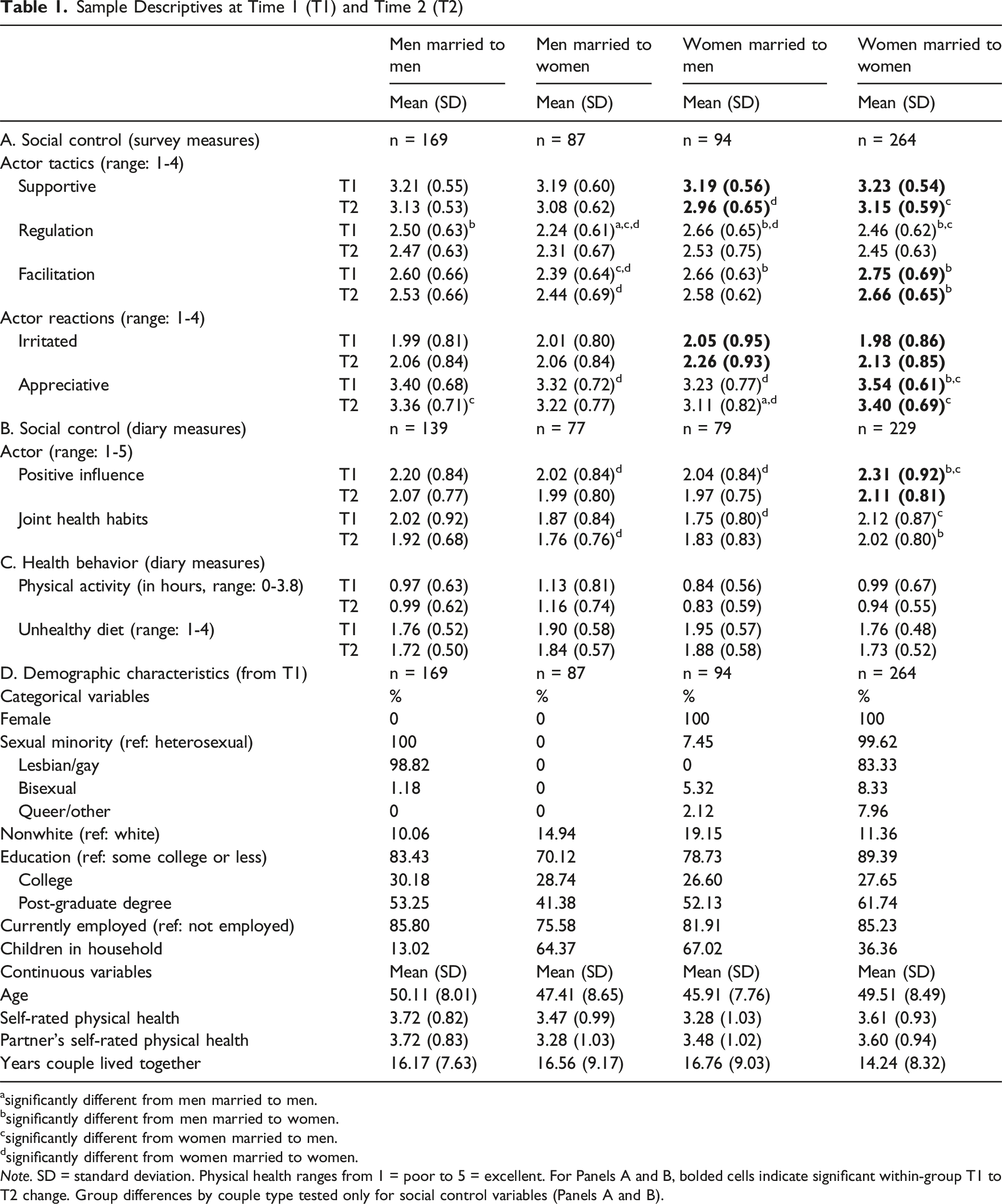
asignificantly different from men married to men.
bsignificantly different from men married to women.
csignificantly different from women married to men.
dsignificantly different from women married to women.
Note. SD = standard deviation. Physical health ranges from 1 = poor to 5 = excellent. For Panels A and B, bolded cells indicate significant within-group T1 to T2 change. Group differences by couple type tested only for social control variables (Panels A and B).
Longitudinal Survey Measures
The survey data include three types of social control tactics— Supportive tactics include providing encouragement, praise/compliments, or humor. Regulation tactics include reminding a spouse to change habits, expressing worry or frustration, stressing importance, dropping hints, or reasoning logically. Facilitation tactics include modeling healthy behavior, offering to make changes with one’s spouse, or altering the environment.
The survey data also include two types of
Diary Measures
Spouses’
Covariates
All models included sociodemographic and health covariates that are found to be significant correlates of social control and health behaviors: respondent age (in years), educational attainment (some college or less = reference, college degree, more than college degree), race (1 = nonwhite), relationship duration (in years), and self-rated health of both actor and partner (1 = poor to 5 = excellent).
Analytic Plan
Survey Data Analysis
We used mixed-effects multilevel models to analyze longitudinal survey data. We include both fixed and random effects while accounting for the nested structure of the data by modeling couple-level interdependence as exchangeable. This approach allows dyadic data analysis with indistinguishable and distinguishable dyads (West et al., 2008). Time was coded 0 = T1 and 1 = T2; the coefficient for time represents overall change in social control across six years. We employed the factorial method, an extension of the actor–partner interdependence model to test whether changes differed by actor (respondent) gender, partner gender, and couple type. Specifically, models included: (1) Time × actor gender interactions (to test whether changes differed for men vs. women), (2) Time × partner gender interactions (to test whether changes differed for spouses married to men vs. women), and (3) Time × actor gender × partner gender interactions (to test whether changes differed by couple type: men married to men, women married to women, women married to men, men married to women).
Diary Data Analysis
To examine change in the daily association of social control with spouses’ diet and exercise behaviors, we first estimated multilevel models with crossed random effects for each wave (T1, T2). We regressed spouses’ reported levels of health behaviors on respondents’ social control and obtained fixed (sample average) and random (individual deviations from the sample average) effects of the slope of social control (i.e., strength of the daily association between respondents’ social control and spouses’ health habits). We sum fixed and random effects to calculate each spouse’s slope. Slopes were rescaled by multiplying by 10 to facilitate interpretation. Slope estimates were then entered as person-level variables into mixed-effects multilevel models, with the coefficient for time representing change in the strength of the daily association between social control and spouses’ health behaviors across six years. All models were estimated in Stata 16 (StataCorp, 2020).
Sensitivity Analyses
We performed sensitivity analyses to assess the robustness of our findings and added the following covariates to account for potential confounding factors: household income, geographic region, financial strain, overall stress, caregiving responsibilities, minority stress (discrimination), and the presence of children in the household. We conducted sensitivity analyses in two ways: (1) by entering each variable separately into models, and (2) by including all variables simultaneously. Because the findings remained substantively unchanged with the inclusion of these variables, we omitted the additional covariates in the final models presented below for parsimony. These sensitivity analyses results strengthen confidence that the patterns we found are not artifacts of omitted variable bias or modeling assumptions.
Results
Descriptive Statistics
Table 1 presents descriptive statistics for main study variables. Panel A (survey data) shows baseline (T1) group differences, including greater use of supportive tactics among women married to women than women married to men at T2, and fewer regulation tactics among men married to women than all other groups at T1. Men married to women also reported less facilitation than women married to women (at both waves) and women married to men (at T1). Women married to men reported more regulation at T1 than women married to women. Women married to women reported higher appreciation than women married to men (at both waves) and men married to women (at T1), while men married to men reported higher appreciation than women married to men at T2. There were no group differences in irritation at either wave. Paired t-tests indicate significant declines in supportive tactics (t = 2.95, Cohen’s d = 0.31) and increases in irritation (t = −2.24, Cohen’s d = −0.23) for women married to men. For women married to women, supportive (t = 2.29, Cohen’s d = 0.14) and facilitation (t = 2.20, Cohen’s d = 0.14) tactics and appreciation reactions (t = 3.14, Cohen’s d = 0.19) declined while irritation reactions (t = −2.61, Cohen’s d = −0.16) increased over time.
Panel B (diary data) shows that women married to women reported more daily positive influence attempts than women married to men and men married to women at T1, as well as more daily collaborative activities than women married to men (T1) and men married to women (T2). Paired t-tests indicate that women married to women significantly decreased their daily positive influence tactics from T1 to T2 (t = 3.85, Cohen’s d = 0.25).
Longitudinal Survey Data, Multilevel Model Results
Multilevel Models Testing Longitudinal Change in Actors’ Social Control Tactics and Reactions to Social Control (Survey; n = 614)
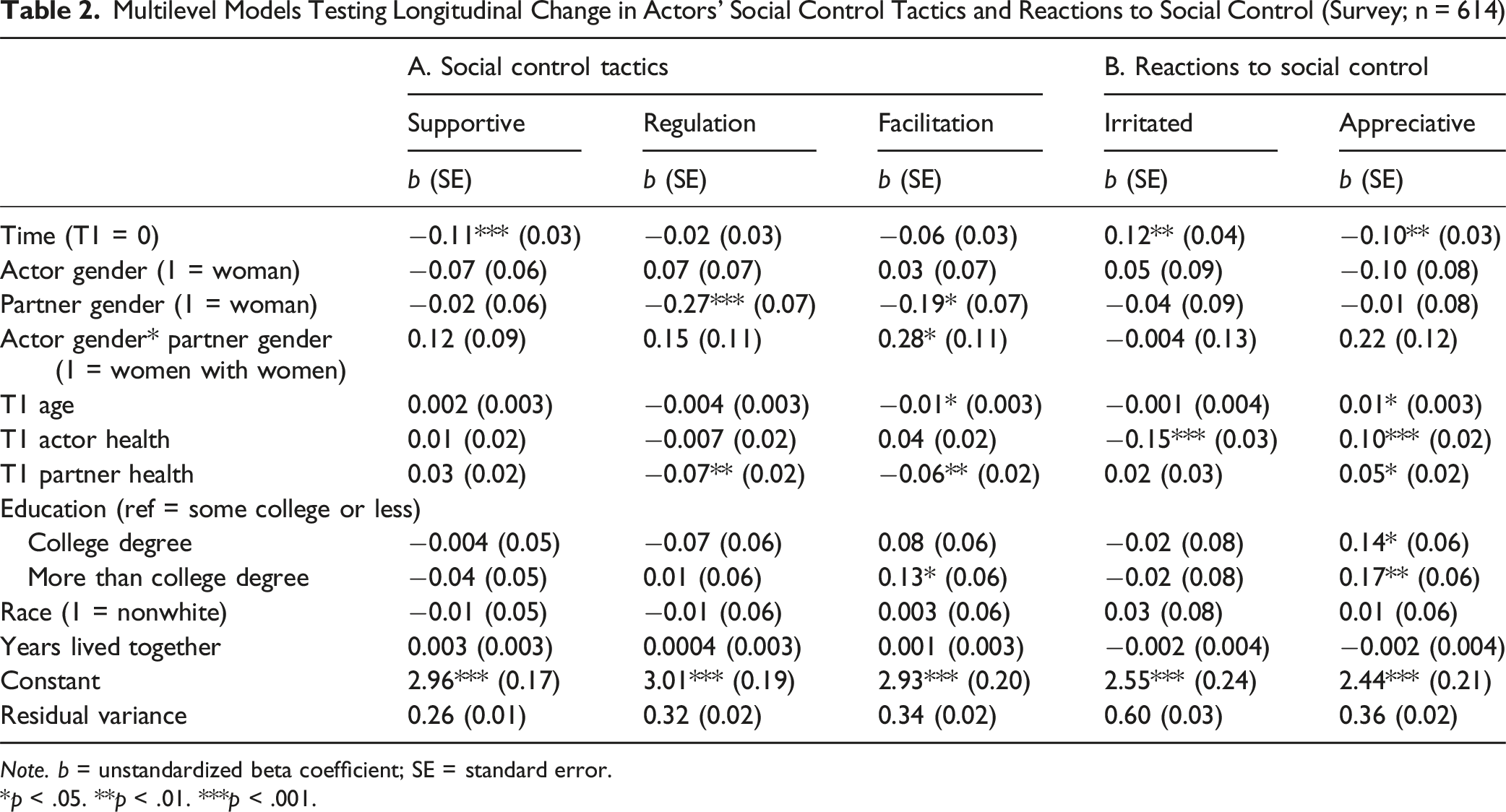
Note. b = unstandardized beta coefficient; SE = standard error.
*p < .05. **p < .01. ***p < .001.
Panel B of Table 2 shows results for reactions to social control. Over time, for the full sample, spouses reported more irritation (b = 0.12, p < .05) and less appreciation (b = −0.10, p < .05). Tests of interactions between time and actor gender, partner gender, or couple type were not significant, indicating that changes in tactics and reactions were similar by gender, and across same- and different-sex couples (Full set of results are provided in Supplemental Tables 1 and 2).
These results are net of respondent age, both partners’ self-rated health, and other covariates (education, race, years lived together). Yet, older respondents reported using fewer facilitation tactics and feeling more appreciation at T1. Partner’s better health is associated with less use of regulation and facilitation and greater appreciation, while actor’s better health predicted less irritation and more appreciation at T1. As prior research shows that health behaviors can influence social control (Umberson et al., 2018), we performed additional analyses that included partner health behaviors (BMI, physical activity) as covariates. Inclusion of these covariates did not alter the patterns of results (results are provided in Supplemental Table 3).
Daily Diary Data
Multilevel Models Testing Longitudinal Change in the Daily Association of Actors’ Positive Influence and Joint Health Habits With Partners’ Health Behaviors (Diary; n = 524)
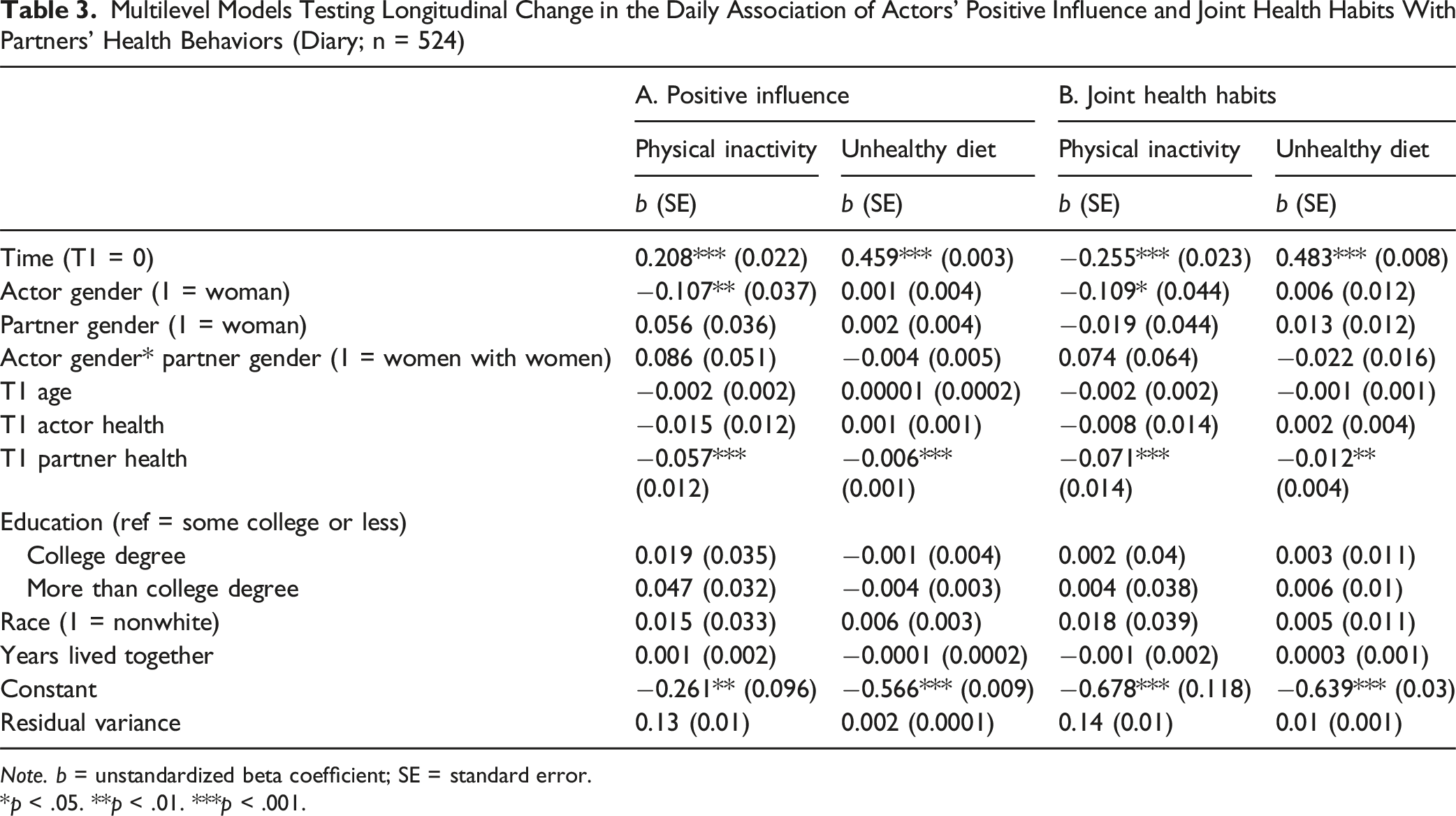
Note. b = unstandardized beta coefficient; SE = standard error.
*p < .05. **p < .01. ***p < .001.
Panel A shows that, at T1, more daily positive influence attempts were associated with less physical inactivity and fewer unhealthy dietary practices by the spouse. However, these associations weakened over six years. Interaction models indicated that the decline in effectiveness differed by partner gender (b = 0.14, p < .01; Supplemental Table 4). To visualize the interaction effect, we graphed partner’s inactivity scores by actor’s levels of positive influence at T1 and T2 for those married to women and those married to men. As illustrated in Figure 1, the association between positive influence and reduced inactivity became weaker over time, and this apparent weakening of influence was greater for those married to women than those married to men. Change in the daily association of actors’ positive influence tactics with partners’ physical inactivity by couple type (Longitudinal diary sample)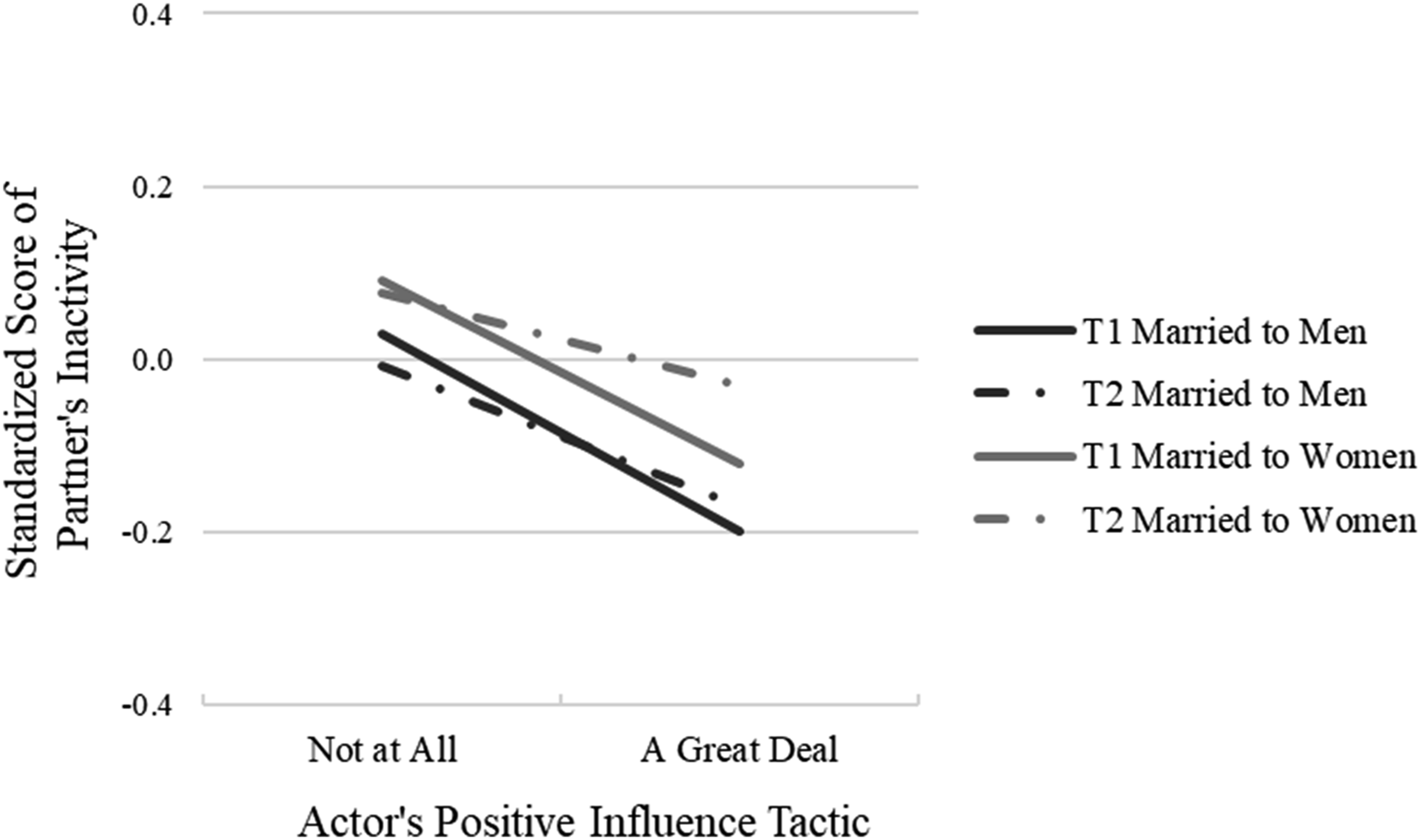
Panel B shows that at T1, joint participation in health habits was associated with less inactivity and fewer unhealthy eating behaviors by the spouse. Over time, the daily association with unhealthy eating weakened, while the association with physical activity strengthened. A three-way interaction of time × actor gender × partner gender (b = 0.068, p < .05; Supplemental Table 5) indicated that the association between joint participation in health habits and spouses’ diet behaviors differed by couple type. To visualize the interaction effect, we graphed partner’s diet behaviors by actor’s levels of joint health habits at T1 and T2 for men married to women and women married to women. Figure 2 illustrates that the association between joint participation in health habits and spouses’ diet behaviors becomes weaker over time, particularly for women married to women compared to men married to women. These models adjust for respondent age, both partners’ self-rated health, and other covariates. Actor age and health were not associated with the associations between actors’ social control and spouses’ health behaviors at T1. However, better partner health predicted stronger daily associations of social control with both lower inactivity and healthier diet at T1. Change in the daily association of actors’ joint health habits with partners’ unhealthy diet by couple type (Longitudinal diary sample)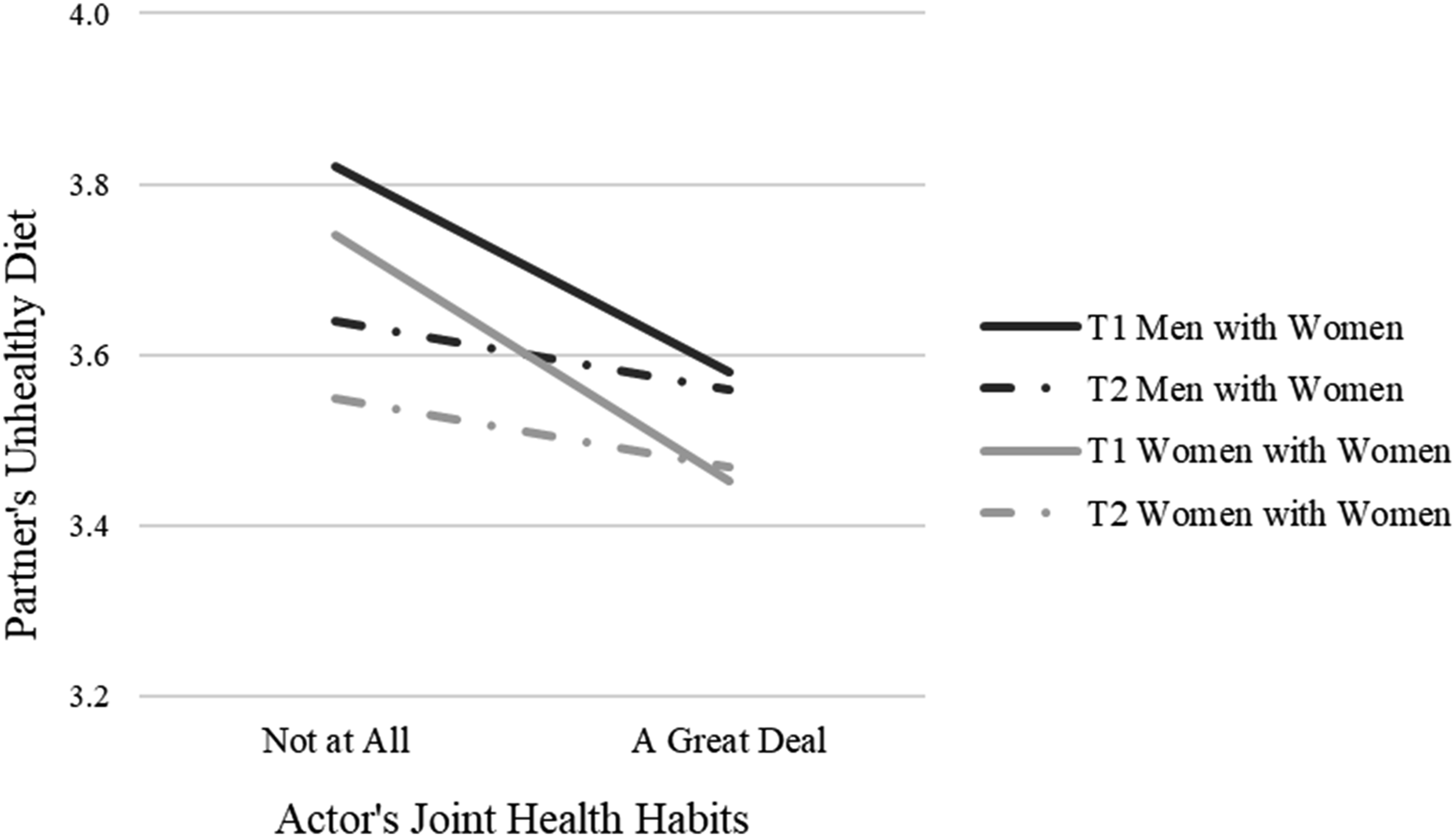
Discussion
This study expands our understanding of sexual minority aging by showing how social control operates and changes over time for married same-sex and different-sex couples. Most longitudinal research on marital dynamics has focused on heterosexual couples, yet spouses’ efforts to influence one another’s health may be especially consequential for aging sexual minority adults who face elevated health risks, greater isolation, and unique caregiving challenges (Fredriksen-Goldsen et al., 2023; Lampe et al., 2024).
Using six years of dyadic survey and diary data, we examined both long-term shifts in control tactics and reactions, and changes in the daily effectiveness of social control for diet and exercise. Three overarching themes emerged: (1) supportive control tactics decline while irritation in response to social control increases, (2) the effectiveness of supportive control tactics generally diminishes over time—especially for women, and particularly women married to women, and (3) collaborative forms of influence, such as joint participation in health activities, may be especially fruitful for sustaining health-promoting behaviors in later life. The survey data trace six-year changes in tactics and reactions, while the diary bursts trace six-year changes in the daily associations between influence attempts and spouses’ diet and exercise. Taken together, the datasets link longitudinal shifts in marital dynamics over years to within-day processes measured at each wave.
Social Control Tactics and Reactions
Survey results show that supportive influence tactics become less common across six years, and spouses grow more irritated and less appreciative in response to their partner’s efforts. This pattern suggests that, over time, spouses may come to see social control as less effective or more intrusive, which could reduce their motivation to engage in this form of health work. Rook and colleagues (2011) caution that control attempts can provoke resistance and distress; our findings indicate that this resistance may intensify with age.
Although most facets of change in social control are similar for same-sex and different-sex couples, the shifts may carry greater health consequences for sexual minority spouses, who have fewer alternative sources of support and caregiving in later life (Reczek & Umberson, 2012), and experience more significant declines in self-rated health over time (Wang, 2022). Gendered baseline differences are evident and some of these differences endure over time: respondents married to women report using less regulation and facilitation than those married to men. Thus, patterns of social control often depend not only on one’s own gender but also on the gender of one’s spouse. This relational dependence of gendered behavior aligns with the gender-as-relational perspective, which emphasizes that the enactment of gender is shaped by the interactional context (Thomeer et al., 2020).
Social Control Effectiveness
Diary data highlight that the effectiveness of positive influence efforts may wane over time. Daily supportive tactics seem to lose power in shaping diet and exercise, with the sharpest declines among women, especially women married to women. Similarly, joint health activities remain beneficial but show weakening effects for dietary behaviors across six years, again most pronounced for women married to women. These results suggest heightened vulnerability for aging lesbian couples, whose health may be less responsive to spousal influence even as they engage in high levels of caregiving and monitoring.
Collaborative Strategies of Spousal Influence
An important exception to the apparent weakening of social control influence over spouses’ health behaviors occurs for exercise: joint engagement in health activities seems to grow more effective for promoting exercise in both same- and different-sex couples. This finding underscores the promise of collaborative approaches to health behavior change. Because health behavior interventions often involve spouses (Carr et al., 2019), programs that emphasize shared routines may remain effective into later life. This may be an especially effective strategy for same-sex couples who tend to engage in more health care collaboration (Reczek & Umberson, 2012) and health behavior concordance than do different-sex couples (Holway et al., 2018).
Interpreting Change Over Time
Why does effectiveness decline for some forms of social control? Theories of socioemotional reactivity suggest that people become less reactive to relational stressors with age (Blaxton et al., 2020; Carstensen et al., 2011). Reduced responsiveness may blunt the impact of influence attempts, especially when they are direct or regulatory. Joint activities may avoid this problem because they are less coercive and more collaborative. Our combined survey and diary results suggest that increases in irritation and declines in supportive tactics may further erode effectiveness. By contrast, more stable regulatory tactics—often coercive and less effective (Rook et al., 2011)—highlight the persistence of approaches that may not promote long-term health.
Our results also show that declines in the effectiveness of positive influence and joint health habits are more pronounced for spouses married to women in both same-sex and different-sex couples. For example, predicted values from the interaction effects show that the effectiveness of positive influence on spouse’s physical activity declined by about 30% between T1 and T2 for those married to men (i.e., difference in partner’s time spent doing physical activity per a week between those exerted no positive influence and those with highest level of positive influence was 63 minutes at T1 and 42 minutes at T2, an approximately 30% decline), whereas the effectiveness declined by 50% between T1 and T2 for those married to women (i.e., difference in partner’s weekly physical activity by level of positive influence declined from 56 minutes at T1 to 28 minutes at T2, a 50% decline). These findings suggest that women’s decline in responsiveness to their spouse’s control efforts is greater than men’s. Gender is often a strong driver of relationship dynamics in both same-sex and different-sex marriages (Umberson et al., 2018). Women are more relationship-focused than men, and more affected by marital strain (Donoho et al., 2013). It may be that women are more aware of their spouse’s social control efforts and not always pleased with them (Markey et al., 2008; Rook et al., 2011), highlighted by the finding that women report increasing annoyance with their spouse’s control efforts. This interpretation fits with gendered cultural scripts in which women view themselves as the architects, rather than the recipients, of care work (Rook et al., 2011). Future research should distinguish when gender alone drives specific social control dynamics, compared to dynamics that vary more strongly for same-sex compared to different-sex marriages.
Gender and Couple-type Dynamics
Our results advance and add nuance to the literature on gender and marital health influence. At baseline, women married to women reported greater appreciation than other groups, and spouses married to men used more regulation and facilitation. Over time, however, the direction of change was similar across groups—declining appreciation, increasing irritation, and declines in supportive tactics. Despite group differences in starting points, these commonalities remind us that aging couples—regardless of sexual orientation—share challenges in sustaining health-related influence across time. However, it is important to keep in mind that baseline differences in these dynamics also exist; for example, women married to women begin the study period with the highest levels of appreciation for each other’s social control efforts.
Practice and Policy Implications
Our findings underscore the need for interventions that account for both the vulnerabilities and strengths of aging same-sex and different-sex couples. For sexual minority adults, who often face greater health disparities and unique barriers to accessing caregiving networks (Erosheva et al., 2016), spouses are a critical source of health support. Yet, the declining effectiveness of supportive influence tactics over time suggests that simply encouraging partners to “monitor” each other may be insufficient. Instead, programs should emphasize collaborative approaches—such as joint engagement in health routines—that may remain effective into later life. Because many health behavior interventions already involve spouses (Carr et al., 2019), explicitly structuring shared routines may help sustain benefits as couples age.
Clinicians and policymakers should also recognize that women, especially women married to women, may experience heightened strain from both providing and receiving social control. Tailored supports for these couples could help mitigate health risks and caregiving burdens. More broadly, policies that expand healthcare access, community-based supports, and culturally competent services for sexual minority older adults, with attention to the unique needs of gay and lesbian couples, will enhance the capacity of spouses to sustain one another’s health as they age (Lampe et al., 2024). Future work should also explore how contextual factors such as caregiving, financial strain, having children in the home, and minority stress shape social control dynamics, particularly for sexual minority spouses who often face compounded stressors and fewer sources of support in later life (Lampe et al., 2024).
Limitations
While two waves of data collected six years apart limit our ability to capture fine-grained trajectories of social control, they nonetheless represent a major advance over prior work, which has relied almost entirely on cross-sectional or short-term designs. To our knowledge, this is the first longitudinal dataset to track both same-sex and different-sex spouses across such a time span. Future studies with more waves and shorter intervals will be essential to build on these findings and more fully illuminate long-term patterns of change. Additional limitations should be noted. First, attrition at Time 2 was not trivial; those who remained in the sample were more likely to be women, employed, and highly educated, and less likely to have children. However, attrition was unrelated to baseline levels of social control, health behaviors, or reactions to social control, suggesting it is unlikely to bias conclusions. Second, the relatively smaller number of same-sex couples, particularly when estimating higher-order interactions, may have reduced statistical power to detect more subtle changes. Nonetheless, the consistency of main effects across models and the robustness of results from sensitivity analyses provide confidence in the reliability of our findings. Third, our sample is socioeconomically and geographically selective, though sensitivity checks controlling for SES and region yielded robust results. Fourth, because the study was designed to focus on continuously married spouses, findings may not generalize to those who divorced or separated during the study period. Finally, the historical cohort came of age before the legalization of same-sex marriage, when stigma was more pervasive, and the sample is relatively socioeconomically advantaged, thus limiting generalizability.
Conclusion
Spouses play a central role in shaping each other’s health as they age (Bertogg & Strauss, 2020). Decades of research document this process for heterosexual couples, but longitudinal data on same-sex marriages remain scarce. By integrating two longitudinal components—surveys that track change in tactics and reactions and diary bursts that track change in the day-to-day effectiveness of those tactics across two waves six years apart—this study offers a comprehensive view of how social control evolves in marriage. Our findings show that, over six years, supportive tactics decline and reactivity to control grows more negative, while daily influence becomes less effective—especially for women and most strikingly for women married to women. At the same time, shared participation in health habits may become more effective in promoting physical activity, highlighting a potential pathway for interventions. For aging sexual minority adults, who already face disproportionate stress, isolation, and health disparities (Lampe et al., 2024), these results underscore both vulnerability and opportunity. Declining effectiveness of control highlights risks, particularly for lesbian couples, while the benefits of joint health habits point to promising strategies for supporting resilience. Future work should examine how social control operates across diverse sexual minority populations, including bisexual and transgender spouses and those at intersections of race, ethnicity, and socioeconomic status.
Supplemental Material
Supplemental Material - How Aging Same-Sex and Different-Sex Spouses Influence Each Other’s Health Behaviors: Change Over a Six-Year Period
Supplemental Material for How Aging Same-Sex and Different-Sex Spouses Influence Each Other’s Health Behaviors: Change Over a Six-Year Period by Debra Umberson, Sara Mernitz, Hye Won Chai, Yiwen Wang, Charlotte Perez in Research on Aging.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant, R37AG076057, awarded to Debra Umberson, and P30AG066614, awarded to the Center on Aging and Population Sciences, at The University of Texas at Austin by the National Institute on Aging. Additional funding was provided by grant, P2CHD042849, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Disclaimer
The content is solely the authors’ responsibility and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.