
Abstract
As chronic conditions dominate mortality trends, the place of death has emerged as a key marker of end-of-life (EoL) care quality. Although many older adults wish to die at home, structural barriers often lead to institutional deaths, especially among socioeconomically disadvantaged groups. This study investigates how housing types, defined by economic status, affordability, and congregate features, affect place of death in older adults. Drawing on National Health and Aging Trends Study data (N = 3,145), we examine links between housing type, EoL resource access, unmet needs, and death location. Residents of Subsidized Senior Housing (SSH) report more formal support yet still face unmet functional assistance needs, while traditional home residents depend on informal caregivers. SSH residents more often die in nursing homes or hospitals, whereas higher-income peers more frequently die at home. These findings indicate housing environments shape EoL resource availability, underscoring the need for targeted policy to reduce housing-related EoL disparities.
The relationship between housing and place of death has gained growing attention as a marker of end-of-life (EoL) care quality and equity. Over recent decades, deaths have gradually shifted from hospitals to homes and community settings, reflecting changes in health systems and population aging (Houttekier et al., 2010). Because many older adults wish to die in familiar surroundings, understanding how residential environments shape EoL experiences is increasingly important (Boucaud-Maitre et al., 2023; Ervik et al., 2023). Although hospitals remain the most common site of death, recent trends show modest increases in home or community-based deaths (Broad et al., 2013; Nyblom et al., 2024). The location of death influences not only health-care utilization but also dignity, caregiver burden, and the alignment of care with personal preferences (Gao et al., 2019).
Housing is more than physical shelter; it determines the resources and social supports that structure late-life care. Differences between subsidized senior housing (SSH), market-rate congregate housing, and traditional private homes influence both formal and informal care availability. These settings are tightly linked to socioeconomic status (SES), support systems, and access to medical resources, all of which shape dying trajectories. While prior research has explored place of death in relation to disease or care utilization, few studies have centered housing itself as an analytic framework for EoL planning.
Two critical gaps remain. First, although disparities in EoL care and in place of death have been studied separately, little is known about how unmet EoL resource needs, such as functional support or caregiving, affect place of death. Much existing work emphasizes hospice enrollment or symptom control (Gomes et al., 2013b; Teno et al., 2013), overlooking broader support systems. Second, the idea of “home” as a preferred death setting has been narrowly confined to private residences. Yet many older adults now live in congregate environments such as senior housing, an expanding segment of the care continuum (Hansford et al., 2022). Research still focuses largely on medical institutions or private homes, leaving EoL outcomes in alternative housing types understudied (Sørstrøm et al., 2024).
This study addresses these gaps by examining how housing type, defined by economic conditions and support availability, influence place of death among older adults. It investigates how unmet needs and access to formal and informal EoL resources interact with housing contexts to shape dying trajectories. By integrating housing and SES, this research provides a structural perspective on barriers to preference-aligned, equitable end-of-life experiences.
Conceptual Background
Guided by the person–environment (P–E) fit framework (Chaudhury & Oswald, 2019; Lawton & Nahemow, 1973), this study conceptualizes housing as a meso-level environment that structures access to end-of-life (EoL) resources. Rooted in Lawton’s ecological model of aging, the P–E fit perspective posits that well-being results from the dynamic alignment between individuals’ competencies and the demands or supports embedded in their environments, which operate across multiple levels—from the physical home to broader social and community contexts (Lawton, 1999).
While the framework itself is inherently multilevel, early empirical applications tended to focus on micro-level environments such as home design, accessibility, and interpersonal adaptation. Subsequent research has expanded this focus toward organizational and community settings—for example, care facilities, r housing, and neighborhood —where structural and social factors shape the extent to which older adults can achieve environmental congruence (cf. Oswald et al., 2024; van Hoof et al., 2021).
Building on this broader perspective, the present study treats housing type as a meso-level environment that enables or constrains access to EoL resources. Subsidized and market-rate senior housing represent distinct ecological contexts that differ in affordability, service coordination, and the integration of formal and informal care. Within this framework, the place of death is interpreted as an outcome of person–environment alignment: when environmental supports adequately meet residents’ EoL needs and preferences, dying in place becomes feasible; when misfit—manifested as unmet needs or fragmented services—occurs, transitions to institutional deaths become more likely.
End-of-Life Resources and Place of Death
End-of-life (EoL) care provides comprehensive support for people with terminal illness, typically during the final year of life. Although often conflated with palliative care, it focuses specifically on improving quality of life and alleviating suffering in the last stage. Services include pain control, emotional support, and spiritual care, usually delivered at home or in residential settings (Marcus, 2009).
Many individuals wish to die at home, but this preference is often unmet. Factors such as age, marital status, available services, caregiving capacity, and symptom management influence discrepancies between preferred and actual place of death (Gerber et al., 2019). Access to home-based palliative care increases the likelihood of dying outside hospitals, while unmanaged symptoms raise the probability of hospital deaths (Okamoto et al., 2016). The availability of EoL resources, informal caregivers and formal services like paid aides or hospice, is among the most consistent predictors of home death (Morioka et al., 2018). Unmet needs in daily functioning are more common among those who die in hospitals (Ercin Swearinger & Lapham, 2023), underscoring the importance of caregiving networks.
However, the adequacy of these resources is unevenly distributed and closely tied to housing environments (McCune et al., 2025). Whether an older adult lives in a traditional home, congregate senior housing, or a subsidized setting shapes access to both formal and informal care. Housing context is therefore a critical factor mediating resource availability at the end of life.
Senior Housing and Place of Death
The interplay between EoL resources and place of death is especially salient in senior housing. Such housing spans a continuum—from subsidized senior housing (SSH) and age-restricted apartments to independent and assisted living or continuing care retirement communities (CCRCs) (American Seniors Housing Association et al., 2020). These models differ in medical capacity and supportive services: CCRCs provide full care transitions, whereas age-restricted or independent living offer limited supports such as meals or personal assistance (AARP, 2022; Kisling-Rundgren et al., 2016).
While extensive research addresses institutional settings like nursing homes, much less is known about outcomes in non-medicalized senior housing. Qualitative studies reveal the social and symbolic importance of these environments. Rainsford et al. (2018) found that residents in rural aged care facilities came to regard the facility as “home,” shaping their wish to die there. Parker (2011) showed how relationships and identity in aged care influence dying experiences. Conversely, Wolff et al. (2007)demonstrated that the absence of chronic illness, rather than formal care access, predicted home deaths among disabled older adults, highlighting individual health and informal support. Recent work also shows that death is often marginalized in senior housing, limiting open discussion and proactive planning (Vandenberg et al., 2024).
Together, these studies suggest that congregate housing can facilitate meaningful EoL experiences but that this potential varies by housing type. SSH, in particular, reflects economic vulnerability and limited institutional resources. Although SSH supports aging in place for low-income older adults, its role in shaping dying outcomes remains underexamined. SSH occupies a middle ground, neither fully institutional nor entirely independent, yet is rarely integrated into formal palliative systems. This makes it a critical site for examining how structural conditions of housing shape the final stage of life.
EoL Resources and Place of Death by Economic Status
Socioeconomic status (SES) strongly shapes both end-of-life (EoL) care and place of death. Lower-SES individuals are more likely to die in hospitals, even when home-based options exist (Davies et al., 2019; Wales et al., 2020). In contrast, higher SES is associated with stronger support networks, better health literacy, and greater ability to mobilize resources for home care, increasing the likelihood of dying at home (Wales et al., 2018). Education, income, and neighborhood deprivation each influence access to EoL resources and death location.
SES also intersects with race and ethnicity to compound disparities. Black and Hispanic patients are more likely to die in hospitals and less likely to receive high-quality hospice care (Cole et al., 2019; Estrada et al., 2021; Gruneir et al., 2007), despite evidence that hospice improves symptom control and family preparedness (Howick et al., 2024).
These inequities are further magnified by housing. Residents of subsidized senior housing (SSH) tend to show higher functional impairment and healthcare use than peers in other settings (Kler et al., 2024). Unmet care needs, including skipped meals, medication errors, and inadequate assistance with daily activities, are more frequent in such environments and often lead to avoidable hospitalizations (Morales & Robert, 2022). Although SSH has gained attention as a supportive model for aging in place, few studies have examined its implications for dying. Understanding how SSH mediates access to EoL resources and structures dying experiences is crucial for designing equitable, preference-aligned care systems.
Study Objective and Hypotheses
Guided by the person–environment (P–E) fit framework, this study investigates how housing contexts influence end-of-life (EoL) resources and are associated with the place of death among older adults. Within this framework, housing type is conceptualized as a meso-level environment that structures the alignment, or misalignment, between individual care needs and available supports. A good fit occurs when environmental resources (e.g., formal and informal care, service coordination) meet residents’ EoL needs, whereas misfit is manifested as unmet needs, resource fragmentation, or lack of continuity in care.
Housing type is operationalized to reflect key socioeconomic and structural characteristics, including senior housing status, low-income designation, and housing cost burden. EoL resources are measured through living arrangements, the presence of formal and informal caregivers, and reported unmet needs related to EoL care and functional limitations in the final year of life.
This study addresses two main research questions.
First, how does the availability of and unmet need for EoL resources vary across different housing types?
Second, how do housing type and EoL resources relate to the place of death?
Drawing on the P–E fit perspective, the following hypotheses were tested:
The availability of and unmet need for EoL resources differ significantly by housing type, reflecting variation in the degree of person–environment fit.
Housing type and EoL resources are associated with the place of death such that environments characterized by better fit—manifested as adequate formal and informal supports and fewer unmet needs—are more likely to enable dying in place.
By integrating the P–E fit framework with an analysis of housing structure and resource availability, this study contributes a housing-centered perspective to understanding disparities in place of death among older adults.
Methods
Data and Study Population
Data for this study came from the National Health and Aging Trends Study (NHATS), a nationally representative longitudinal survey of older Americans aged 65 and above enrolled in Medicare. Data were collected annually through in-person interviews, guided by a conceptual framework examining the interplay between physical and cognitive abilities and the environment in which activities occur (Freedman & Freedman, 2024). Detailed sampling methods are available elsewhere (DeMatteis et al., 2016). To explore experiences in the final stage of life, we focused on individuals who died between 2010 and 2022 (waves 1 through 12), with analytic data centered on the last year of life. The initial sample included older adults who passed away during the study period and who provided information on EoL care supports through last-month-of-life interviews (N = 4,358). These interviews covered a range of validated measures related to EoL experiences (Freedman & Kasper, 2019). Prior research has demonstrated that proxy respondents can reliably report on the dying experience, making them suitable substitutes for direct respondents (Ercin Swearinger & Lapham, 2023). Residents of nursing homes and assisted living facilities were excluded, reducing the sample size to 3,582. Further exclusions, including cases with missing place of death or housing information and deaths that occurred in transit, resulted in a final analytical sample of 3,145.
Measures
Place of Death
The dependent variable in this study was place of death, derived from the NHATS last-month-of-life interview. Proxy respondents were asked where the decedent died, with response options including: own home, hospital, nursing home, hospice facility, someone else’s home, in transit, or other. Following previous research using NHATS data (Kim et al., 2024; Lei et al., 2021; Regier et al., 2021), place of death was classified into four categories for analysis: (1) Own home, (2) Hospital, (3) Nursing home, and (4) Hospice. Cases with missing data or unclassifiable responses (e.g., in transit or other) were excluded.
This categorization reflects meaningful differences in the quality and context of EoL care settings. Hospital deaths are frequently associated with more aggressive interventions, including ICU admissions, mechanical ventilation, and repeated hospitalizations, which may signal a lack of preparedness or misalignment with patients’ care preferences. (Earle et al., 2008; Teno et al., 2013; Zhang et al., 2009). In contrast, deaths occurring at home or in hospice facilities are generally more consistent with person-centered goals and are associated with greater satisfaction among family members and caregivers (Kim et al., 2024; Regier et al., 2021; Teno et al., 2013). Importantly, dying at home often reflects a preference to remain in a familiar and emotionally meaningful setting, but may also indicate reliance on family caregivers and limited access to formal care services. In contrast, dying in a hospice facility usually signals access to specialized EoL care with professional support for pain management, symptom control, and emotional needs (Wright et al., 2008). While both settings are associated with less aggressive care at the end of life, they differ in the level and type of support provided, as well as the caregiving burden involved.
In this study, nursing home deaths reflect individuals who were not long-term residents but who were admitted for short-term or transitional care prior to death. These settings can offer continuity of care, but quality varies substantially depending on staffing levels and availability of hospice or palliative services (Miller et al., 2025; Mor et al., 2004).
Housing Types
Housing type was categorized into five groups based on factors such as congregate senior housing versus traditional community-based home, rent-subsidized status, housing cost burden (HCB), and income status. The five categories were: (1) subsidized senior housing (SSH), (2) senior housing with a low-income (LI) status or HCB (SH-LI or HCB), (3) senior housing with non-low-income status and non-HCB (SH-non LI & non-HCB), (4) traditional home with low-income status or HCB (TH-LI or HCB), and (5) traditional home with non-low-income status and non-HCB (TH-non LI & non-HCB).
The housing types were classified into congregate housing and traditional homes, following Freedman and Spillman’s (2014) study and industry standards (American Seniors Housing Association et al., 2020). Freedman and Spillman (2014) identified five settings: traditional community housing, retirement/senior housing, independent living, assisted living, and nursing homes. In this study, congregate housing includes retirement/senior housing and independent living due to their similar environments, though independent living typically offers additional services like meals. Congregate housing refers to age-restricted communities offering supportive services but not licensed for healthcare, unlike assisted living or nursing homes, which were excluded. Congregate housing was further divided based on subsidization, income status, and HCB, following Jenkins Morales and Robert (2022). Subsidized housing status was determined using a question from the NHATS: “Is your home Section 8 or public housing or housing for low-income seniors?” Respondents who answered “yes” were classified as living in subsidized senior housing. Non-subsidized congregate housing was split into those with low-income or high HCB and those without. Traditional home residents were similarly categorized into low-income or high HCB and non-low-income groups.
We examined two dimensions of EoL resource access: (1) the availability of informal and formal support, and (2) unmet needs related to EoL care and functional limitations. To assess the availability of EoL resources, we included two variables. First, living arrangement was coded as a binary indicator (living alone = 1; living with someone else = 0). Second, type of caregiving support was categorized into four groups: (1) no helper, (2) only informal helper, (3) only formal helper, and (4) both informal and formal helpers. To assess unmet needs, we compared respondents’ reported care needs with the services they actually received and categorized them into three groups: (1) no reported needs, (2) needs that were met, and (3) unmet needs. EoL care needs included assistance with pain management, breathing difficulties, anxiety, and personal care. Functional limitation needs were identified based on whether the respondent experienced any difficulties with ADLs or IADLs. For both types of need—EoL care and functional limitations—we created dichotomous variables indicating whether the respondent had at least one unmet need (coded as 1) versus no unmet needs, which included both respondents with fully met needs and those who reported no needs at all (coded as 0).
Covariates
A series of covariates that could influence place of death were controlled for in our analyses. Age was grouped into three categories: young-old (65–74), middle-old (75–84), and oldest-old (85+). Gender included male, female, and not reported. Race/ethnicity was categorized into Non-Hispanic White, Non-Hispanic Black, Hispanic, and other/not reported. Education was binary, indicating whether the participant completed high school. Self-rated health ranged from 1 (very poor) to 5 (very good). The number of chronic conditions were measured continuously, including eight conditions (e.g., cancer, stroke, diabetes). Cognitive status was categorized into cognitively normal, mild cognitive impairment (MCI), and dementia, based on physician diagnosis, the AD8 Dementia Screening Interview, and cognitive tests for memory, orientation, and executive function (Kasper et al., 2013). Dementia was defined by a diagnosis, an AD8 score of 2 or higher (Galvin et al., 2005), or cognitive test scores 1.5 SD below the mean in two or more domains. MCI was defined by scores 1.5 SD below the mean in a single domain.
Data Analysis
Descriptive statistics were used to characterize the study sample. Differences between groups were assessed through bivariate analyses by housing type using Chi-square tests and ANOVA. Multinomial logistic regressions were conducted to examine the associations between housing types, EoL care resources, and places of death. Specifically, Model 1 included a series of EoL care resource variables—such as the availability of formal and informal support (e.g., living alone, presence of unpaid or paid helpers), unmet needs related to EOL care and functional limitations—along with covariates including socio-demographic attributes and health conditions. In Model 2, housing type was added to the model. All analyses were conducted using STATA version 16.1.
Results
Study Sample Characteristics
Sample Characteristics of Samples by Housing Type and Place of Death (N = 3,145)
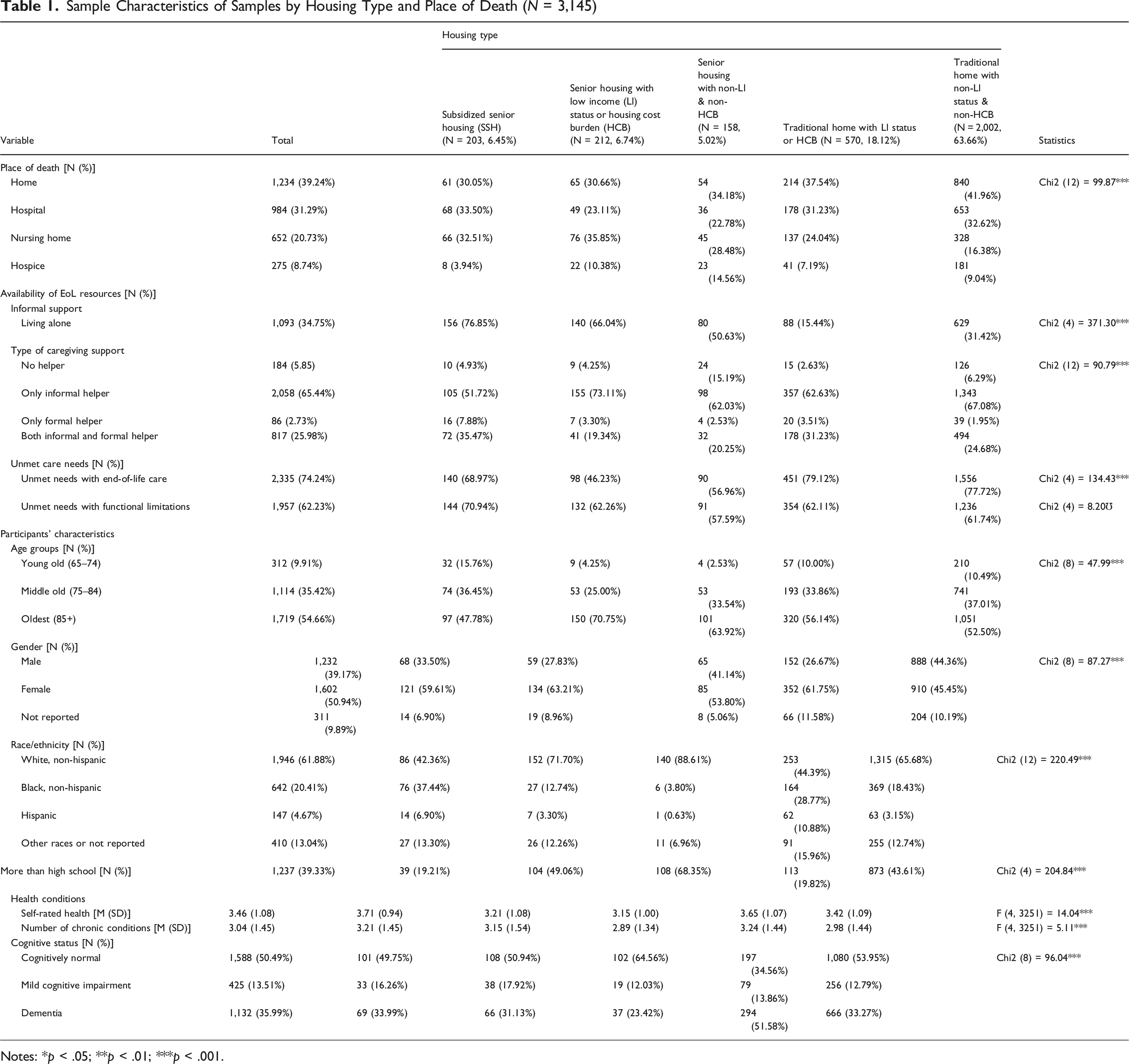
Notes: *p < .05; **p < .01; ***p < .001.
Due to the nature of the sample—comprising individuals who had died—the age distribution skewed older. More than half of the participants were among the oldest-old (age 85 and older), and 35.42% were in the middle-old group (ages 75–84). As a result, the proportion of young-old adults (ages 65–74) was relatively small, accounting for only 9.91% of the sample. The sample was 50.94% female and 39.17% male, with 9.89% not reporting gender. The majority of participants identified as Non-Hispanic White (61.88%), followed by Non-Hispanic Black (20.41%), Hispanic (4.67%), and Other racial/ethnic groups (13.04%). In terms of educational attainment, 39.33% had more than a high school education. Regarding health status, the average self-rated health was 3.45, and participants had an average of 3.04 chronic conditions. About half of the sample were cognitively normal, while 35.99% had dementia.
Differences in Availability and Unmet Needs EoL Resources by Housing Type
The analysis (Table 1) revealed significant differences in the availability of EoL resources and unmet needs across housing types, strongly influenced by individuals’ financial circumstances. One prominent difference was in the proportion of individuals living alone, which varied substantially by housing type. Individuals residing in senior housing communities were significantly more likely to live alone compared to those in traditional homes. Specifically, the rates of living alone were 76.85% in SSH, 66.04% in senior housing with LI or HCB and 50.63% in senior housing with non-LI and non-HCB. In contrast, only 15.44% of individuals in traditional homes with LI or HCB and 31.42% in traditional homes with non-LI and non-HCB lived alone.
Significant differences also emerged in the type of caregiving support across housing types. SSH residents were more likely to have formal caregiving support, either alone (7.88%) or in combination with informal support (35.47%), and had the highest proportion of individuals receiving both informal and formal support. In contrast, they had the lowest proportion of individuals relying solely on informal helpers (51.72%), suggesting a distinct pattern of care availability in service-supported housing settings.
Regarding unmet care needs, residents in traditional homes with LI or HCB reported the highest rate at 79.12%, followed closely by those in traditional homes without LI or HCB at 77.72%. In contrast, residents in SSH reported a lower rate of 68.97%, while the lowest rate was observed among those in senior housing with LI or HCB, at 46.23%. For unmet needs related to functional limitations, the highest rate was again found in SSH at 70.94%. Other housing types showed relatively similar rates, including senior housing with non-LI and non-HCB (57.59%), senior housing with LI or HCB (62.26%), and traditional homes (approximately 62%).
Influence of EoL Resources and Housing Type on Place of Death
Multinomial Logistic Regression Models of Places of Death (N = 3,145)
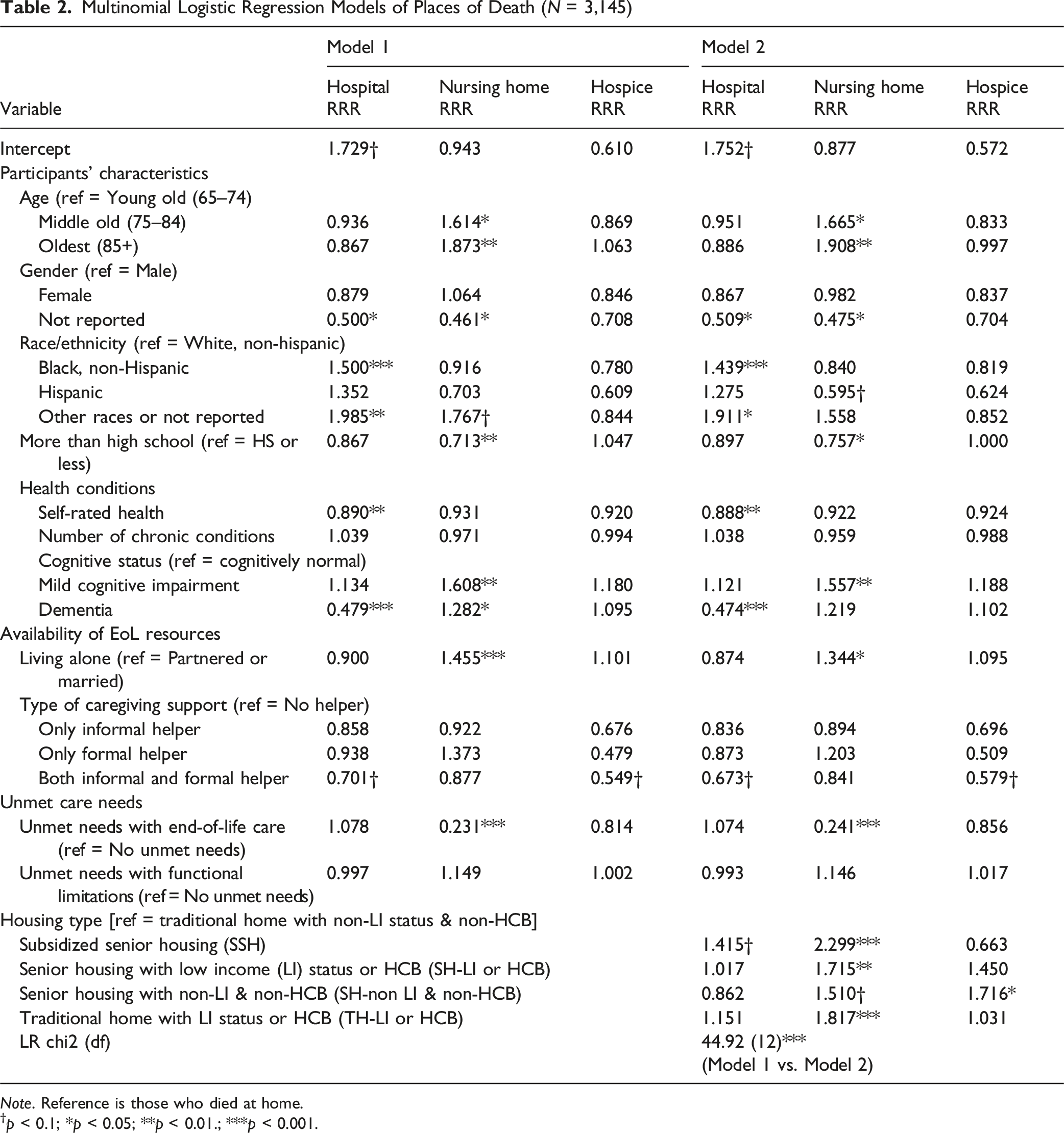
Note. Reference is those who died at home.
†p < 0.1; *p < 0.05; **p < 0.01.; ***p < 0.001.
In Model 2, housing type was added to the analysis, revealing significant associations with place of death. Compared to individuals living in traditional homes with non-LI status and non-HCB, those residing in all other housing types were more likely to die in a nursing home (SSH: RRR = 2.299, p < .001; senior housing with LI or HCB: RRR = 1.715, p < .01; senior housing with non-LI and non-HCB: RRR = 1.510, p < .10; traditional home with LI or HCB: RRR = 1.817, p < .001). Additional analyses using alternative reference categories confirmed this pattern.
Moreover, residents of SSH were also more likely to die in a hospital (RRR = 1.415, p < .10) compared to those in traditional homes with non-LI and non-HCB. Further analyses confirmed that living in SSH was significantly associated with an increased likelihood of hospital death relative to all other housing types. The inclusion of housing type in Model 2 significantly improved model fit (LR χ2 = 44.92, p < .001), indicating that housing type plays a critical role in shaping place of death, particularly in relation to institutional settings such as nursing homes and hospitals.
Discussion
This study examined disparities in end-of-life (EoL) resources by housing type, focusing on how residential environments shaped by social and economic conditions influence access to care and the place of death. Although many older adults prefer to die at home, achieving this is not always possible when support systems are limited. Despite growing attention to EoL equity, the role of housing context in dying outcomes remains underexplored. By highlighting features such as congregate living and housing cost burden, this study reveals how structural conditions shape EoL experiences and contribute to disparities in place of death.
Structural and Economic Drivers of Care Availability and Unmet Needs
This study identified three major patterns in the availability of EoL care resources across housing types. Consistent with H1, the availability of and unmet need for end-of-life (EoL) resources varied significantly by housing type, indicating systematic differences in environmental fit across settings. First, older adults in SSH were far more likely to live alone (76.85%) than those in traditional housing (15–31%), which has important implications for informal caregiving capacity. Second, across all housing types, most older adults relied primarily on only informal caregivers, ranging from 53% to 73%, highlighting the centrality of unpaid care in EoL support. Third, SSH residents were more likely than other groups to receive formal caregiving, either alone (7.88%) or alongside informal support (35.47%). This care pattern may reflect both the congregate structure of SSH and the availability of public support systems targeted toward low-income populations.
Publicly funded long-term care programs might help explain these variations in caregiving arrangements. Medicaid’s Home and Community-Based Services (HCBS) waivers, California’s In-Home Supportive Services (IHSS), and integrated models like the Program of All-Inclusive Care for the Elderly (PACE) all expand access to paid in-home support for eligible older adults (Freedman & Freedman, 2024; Newcomer et al., 2012; Swearinger & Lindhorst, 2025). These mechanisms may help explain why formal support was more prevalent in SSH and among other low-income groups. In contrast, higher-income individuals are often ineligible for these services and may rely more on private or unpaid caregiving networks.
Yet despite these differences in caregiving arrangements, unmet needs for EoL care remained high across all groups. Consistent with H1, these differences indicate systematic variation in environmental fit across housing contexts. The highest levels of unmet EoL care needs were found among those in traditional homes with low income or high housing cost burden (TH–LI or HCB), at 79.12%, suggesting that financial strain combined with structural isolation leaves many older adults without adequate support near the end of life. SSH residents showed somewhat lower EoL care unmet need rates (68.97%), but simultaneously reported the highest rates of unmet needs related to functional limitations (70.94%). These findings suggest partial misfit between care demands and available resources within SSH, whereas residents in financially stable, traditional homes experience comparatively stronger person–environment fit. Together, these results support H1 and illustrate how structural and economic differences across housing environments shape patterns of care availability and unmet need through pathways of environmental fit and misfit.
These patterns reflect systemic constraints across both formal and informal care systems. In SSH, high levels of unmet need may result from staffing limitations or underfunded service models (Christensen et al., 2024). The high proportion of residents living alone in SSH may also reduce access to supplemental informal care (Chen et al., 2022). In low-income traditional housing, even when public programs are available, strict eligibility requirements and geographic inequities in service provision may impede access (Jenkins Morales & Robert, 2022). For higher-income groups in traditional housing, reliance on informal caregivers without professional training may lead to gaps in complex care delivery (Michaels et al., 2022).
Together, these findings underscore that neither economic advantage nor congregate structure alone guarantees adequate EoL support. Persistent unmet needs across all housing types highlight the limitations of current care systems and point to the need for more robust, integrated, and equitable EoL infrastructure (Ercin Swearinger & Lapham, 2023; Wong et al., 2022). Even older adults in financially secure, traditional homes face challenges in navigating fragmented systems, further underscoring the necessity of broad investment in community-based palliative and functional support services.
EoL Resources, Housing Types and Place of Death
Older adults with both informal and formal caregivers were significantly less likely to die in nursing homes or hospice facilities, underscoring the protective effect of dual care networks. Informal caregivers, typically family or friends, provide day-to-day and emotional support, while formal providers add clinical expertise and continuity (Bevans & Sternberg, 2012; McEwen et al., 2018). Integrated care compensates for gaps that arise when relying on either alone, whereas dependence on a single source often leads to fragmented care and unplanned institutionalization. Living alone strongly predicted hospital death, reflecting the vulnerability of those without co-residing advocates or timely symptom recognition (Pimouguet et al., 2017; Threapleton et al., 2017). Expanding access to community-based palliative care, after-hours home support, and caregiver training could reduce these reactive hospitalizations.
In line with H2, housing environments exerted an independent influence on dying outcomes. SSH residents were more likely to die in hospitals or nursing homes than peers in higher-income traditional housing, indicating that affordability and service structure alone cannot offset weak medical integration. SSH often lacks hospice partnerships, staffing, and on-site clinical capacity, making it difficult to manage complex needs (Iyer & Brown, 2022; O’Keeffe et al., 2001). Without proactive care planning, acute symptoms trigger emergency transfers, explaining elevated institutional deaths. By contrast, residents in higher-income homes were more likely to die at home or in hospice, settings of better fit with stronger caregiving networks, accessible services, and lower financial strain. Similarly, resource-rich congregate housing showed higher hospice deaths, suggesting that when organizational environments are financially supported, they can sustain preference-aligned EoL care. These findings support H2 and demonstrate that housing shapes dying outcomes through pathways of environmental fit and misfit, extending the P–E fit framework to EoL contexts.
Communication and advance planning are central to these outcomes. Early conversations about care preferences reduce unnecessary interventions and promote concordant care (Trice & Prigerson, 2009; Wallace, 2015). In SSH, the absence of routine planning increases reactive, institution-based responses. Embedding communication practices and palliative assessments into standard care could mitigate this risk. These findings should not be read as a failure of the SSH model but as evidence that housing-based care platforms need stronger clinical integration and support. With targeted hospice partnerships, caregiver education, and proactive coordination, SSH could become a scalable and equitable infrastructure for dying in place—particularly for low-income older adults who face structural barriers to home death.
Viewed through the person–environment (P–E) fit lens, disparities in place of death mirror the degree of alignment between residents’ needs and environmental supports. SSH provides partial fit—its affordability and social design reduce some stressors, yet limited coordination creates misfit at life’s end. In contrast, higher-income traditional homes show greater congruence, where strong caregiving networks and access to services enable preference-aligned deaths. Thus, place of death reflects not only socioeconomic advantage but the quality of environmental fit between people and the housing contexts in which they live and die.
Implications for Housing-Based EoL Care Policy
Housing environments, particularly subsidized senior housing (SSH), shape end-of-life (EoL) outcomes in ways that extend beyond access to care. Despite affordability and structured services, SSH residents experience higher hospital and nursing home deaths, revealing care delivery gaps that limit dying at home. Although home deaths can improve symptom management and family satisfaction when well supported (Gomes et al., 2013a; Hammer et al., 2023), such outcomes remain difficult to achieve in structurally constrained settings.
Enhancing the feasibility of dying in place requires integrated clinical services, continuity of care, and proactive communication among residents, caregivers, and providers. Strengthening SSH through hospice partnerships, routine advance-care planning, and on-site palliative assessments could reduce avoidable hospitalizations and expand noninstitutional care capacity (Brumley et al., 2003).
Formal support is also critical for those above income-eligibility thresholds. In higher-income households, unpaid caregivers often manage complex tasks alone; broader eligibility or partial subsidies for paid home health aides and respite services such as adult day programs could ease burden and improve outcomes (Estrada et al., 2025; Wylie et al., 2021).
Strengthening advance-care planning and health-literacy infrastructure across housing contexts is equally vital. Interventions such as decision aids, educational workshops, and routine EoL planning increase hospice use and reduce crisis admissions (Durbin et al., 2010; Nouri et al., 2019). Embedding these programs in senior housing and community services would foster earlier preparation and more responsive care.
Reducing disparities in place of death requires policies aligned with the structural realities of each housing environment. SSH and traditional homes face distinct challenges—limited clinical integration versus variable informal support—and thus demand coordinated, housing-sensitive investments rather than one-size-fits-all approaches.
Limitations and Directions for Future Study
This study has several limitations. The cross-sectional design limits the ability to establish causal relationships between housing type, EoL resources, and place of death. Future longitudinal studies tracking older adults’ care transitions, housing changes, and support availability over time would provide valuable insights into how EoL needs evolve and how different housing environments shape these experiences. Additionally, geographic variations in access to healthcare, particularly between urban and rural settings, were not fully addressed in this study. These differences may significantly influence access to EoL resources, and future research should incorporate geographic diversity to understand how location affects care.
Another limitation is the lack of data on individuals’ EoL preferences, particularly regarding their desired place of death. Without this information, we could not assess the concordance between preferred and actual place of death. Some individuals may have died at home due to limited institutional EOL resources rather than personal preference, while others may have preferred hospital-based care. Future research should explore how well actual place of death aligns with individual preferences and the factors that influence this alignment.
Conclusion
This study demonstrates how housing environments intersect with economic status to shape the place of death. Although residents of subsidized senior housing (SSH) are more likely to die in institutional settings, this pattern reflects structural gaps in the integration of end-of-life (EoL) resources rather than a failure of the housing model. SSH provides affordability, communal living, and coordinated social supports, yet limited medical integration constrains its capacity for dying in place. When strengthened through hospice partnerships and proactive care planning, SSH could serve as an equitable platform for reducing EoL disparities among low-income older adults. Economic differences within senior housing, between subsidized and non-subsidized settings, further underscore how financial vulnerability shapes dying experiences. As the population ages, enhancing EoL infrastructure in senior housing may help ensure that affordability does not come at the expense of dignity in dying.
Conceptually, this study extends the person–environment (P–E) fit framework to the end-of-life domain, positioning place of death as an outcome of person–environment alignment. Prior applications focused on adaptation to physical or social surroundings earlier in life; here, dying is framed as a continuation of that adaptive process within organizational environments such as senior housing. By linking environmental gerontology with EoL research, this study shows that inequalities in care and death stem not only from individual differences but from the relational ecology of people and places in which they live and die.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.