
Abstract
Widowhood often leads to increased depressive symptoms, yet the gendered role of adult-child support in moderating these consequences is understudied. We used eight waves of the Survey of Health, Ageing and Retirement in Europe and fixed-effects panel regression to assess how three forms of support from adult children – contact frequency, instrumental support, and geographic proximity – affect depressive symptoms in 2,600 widowed women and 896 widowed men. Results show that weekly contact with at least one adult child buffered the increase in depressive symptoms after widowhood, whereas the receipt of instrumental support was associated with larger increases. Additionally, those living within 25 km of the nearest child experienced smaller increases in depressive symptoms compared to those with cohabiting children. No gender differences emerged. The findings emphasize that the effectiveness of adult children’s support depends on the specific type; there’s no universal solution to helping bereaved parents adapt to widowhood.
Keywords
Introduction
Europe’s population is aging rapidly, with those aged 65 and older rising from 19% in 2014 to 22% in 2024 (Eurostat, 2025). Consequently, more individuals face periods of vulnerability associated with health decline, retirement, or the loss of close social ties (Charles & Carstensen, 2010). Spousal loss is among the most stressful life events and linked to increased depressive symptoms (Schmitz, 2021). While social support can promote well-being during stressful life events (Pearlin et al., 1990), its impact during widowhood is not clear: Some studies suggest a positive effect on depressive symptoms (Ha, 2008; Hewitt et al., 2012), while others report no significant or even negative effects (Anusic & Lucas, 2013; Monserud & Markides, 2017), probably due to diminished personal autonomy (Jessee et al., 2025; Silverstein et al., 1996).
These inconsistent findings may reflect two key measurement issues: First, many studies merge distinct sources of support – such as family members and friends – rather than analyzing them separately (e.g., Anusic & Lucas, 2013; Cohen & Wills, 1985; Gumà & Fernández-Carro, 2019; Monserud & Markides, 2017), potentially concealing source-specific effects (Dean et al., 1990). Following marital dissolution in later life, close relationships with children can protect mental health (Jessee & Carr, 2025b). For widowed older adults, children often become the primary source of support, stepping into the void left by the deceased partner (Guiaux et al., 2007). Second, many studies examine only one type of support (e.g., Hewitt et al., 2012; Tosi & Grundy, 2019), yet social support is multifaceted, and its various dimensions can affect widowed individual’s well-being differently (Tambellini et al., 2025). For instance, frequent contact with an adult child can provide emotional support, companionship, and feelings of security (Buber & Engelhardt, 2008), whereas (unwanted) household assistance may lead them to feel redundant and overly dependent on their children (Silverstein et al., 1996).
The effect of social support from adult children may also differ by gender. Longitudinal studies indicate that widowers often experience more persistent depressive effects than widows in the years following spousal loss (G. R. Lee et al., 2001; Williams & Umberson, 2004). Moreover, women tend to adjust (more) successfully (Streeter, 2020), likely due to their higher social connectedness (Kapelle & Monden, 2024). Additionally, the nature of the parent–child relationship and the types of support exchanged after widowhood differ between widows and widowers (Jiao et al., 2021; Kalmijn, 2007).
These considerations underscore the need for a comprehensive, gender-sensitive analysis that maps a larger spectrum of support from adult children who emerge as the go-to source of help for many older people who have lost their spouse. Using longitudinal data from eight waves of the Survey of Health, Ageing and Retirement in Europe (SHARE) this study investigates how social support from adult children affects the increase of depressive symptoms after widowhood, with a specific focus on gender differences. We focus on three distinct dimensions of intergenerational solidarity (Bengtson & Roberts, 1991): a) contact frequency (associational dimension), b) instrumental support (functional dimension), and c) geographic proximity (structural dimension). Understanding the interrelations between gender and social support from adult children after widowhood offers insights for scientific debates on the buffering effect of social support and informs interventions to reduce the mental distress of widowed individuals.
Gendered Effects of Widowhood on Mental Health
The transition to widowhood is associated with poor mental health including increased depression (G. R. Lee et al., 2001; Schmitz, 2021). The Attachment Theory argues that losing a spouse triggers a mental health decline, in particular because it severs one of the strongest bonds individuals have throughout their life courses (Bowlby, 1980). From this perspective, widowhood can be seen as a primary stressor. The Social Production Function Theory additionally highlights secondary stressors that can emerge after a spouse’s death, such as limited social contacts and reduced financial resources (Ormel et al., 1999). However, the extent to which individuals experience a loss of these resources often differs between men and women (Perrig-Chiello et al., 2016; Schmitz, 2021). Men are often believed to suffer more from spousal loss than women because their social networks tend to be smaller, less diverse and they may depend on their spouse as “kin-keepers” to maintain ties with family and friends – factors that can leave them feeling especially lonely after widowhood (Kapelle & Monden, 2024). Additionally, women are generally more likely to seek help (Thoits, 1995), while social norms pressure men to be independent and self-reliant. Widowers often face additional psychological stress from taking on household chores previously managed by their spouse (Tiedt et al., 2015; Umberson et al., 1992).
In contrast, widows often face greater financial strain because women are more likely than men to leave paid work for unpaid caregiving and, on average, have lower earnings (Rowold et al., 2024), which contributes to an increased poverty risks among widowed women (Gillen & Kim, 2009; Hungerford, 2001), albeit the specific strains and mental health implications of widowhood differ across different cohorts and national contexts (Perrig-Chiello et al., 2016; Schmitz, 2021).
Despite the distinct challenges faced by widows and widowers, most studies report no immediate gender differences in the mental health consequences (H. J. Lee et al., 2016; Sasson & Umberson, 2014; Schaan, 2013; Schmitz, 2021). However, when viewed over a longer period, men appear to recover more slowly than women (Streeter, 2020).
Adult Children’s Social Support following Widowhood
According to the Stress Buffering Hypothesis, adult children’s social support can reduce the perceived burden of critical life events such as widowhood, making individuals more resilient during difficult times by offering companionship, assistance with household chores, and even financial support (Cohen & Wills, 1985). On the other side, the Social Breakdown Hypothesis suggests that receiving ‘too much’ support from a child can ‘backfire’, producing unintended negative effects (Silverstein et al., 1996). These negative effects of support are usually attributed to an individual’s reduced self-esteem and increased feelings of dependency (Jessee et al., 2025).
In their framework of intergenerational solidarity, Bengtson and Roberts (1991) spell out six dimensions of support among parents and their adult children: associational (e.g., frequency of interactions), affectual (e.g., emotional closeness), consensual (e.g., similarity in values and beliefs), functional (e.g., intergenerational exchanges), normative (e.g., adherence to family obligations) and structural (e.g., geographical proximity or the number of family members available to provide support). In this paper, we focus on the three dimensions most commonly examined and consistently available in longitudinal aging studies, including SHARE: associational (contact frequency), functional (instrumental help), and structural (geographic proximity). These dimensions reflect key challenges faced by widowed individuals, including increased loneliness (Kapelle & Monden, 2024) and a greater need for practical assistance, as spouses commonly serve as the primary source of care in later life (Agree & Glaser, 2009). Moreover, structural solidarity captures the opportunities for maintaining contact and exchanging support (Heylen et al., 2012). Whether support buffers or heightens distress after widowhood may depend on which of these forms is considered and may be further influenced by the gender-specific support needs and preferences of widows and widowers.
Contact Frequency
Frequent contact with children can provide parents with emotional support, companionship and feelings of security. Such contact can reduce depression (Buber & Engelhardt, 2008) and lead to eventual assistance from children as it provides opportunity structures for support exchange (Grundy & Read, 2012), creating a “kinship reservoir” that can be tapped for practical assistance in times of need (Hünteler & Hank, 2025). Regular contact with adult children also protects mental health decline during later-life marital dissolution, whereas lack of contact with at least one child is associated with mental well-being decreases (Jessee & Carr, 2025b).
However, in the context of widowhood, Ha and Ingersoll-Dayton (2011) found that contact frequency with friends or relatives does not significantly affect levels of depression or grief. Nonetheless, gender differences may play a role. Widowers often experience higher loneliness (Kapelle & Monden, 2024) and infrequent contact with adult children increases depressive symptoms in widowed fathers but not widowed mothers (Tosi & Grundy, 2019). Again, the evidence is inconclusive and a recent study suggests that lacking contact to at least one child affects both widows and widowers to a similar extent (Jessee & Carr, 2025a).
Instrumental Support
Instrumental support from adult children is another key aspect of social support, but research on its health effects is mixed (for an overview, see Jessee, 2023). Some studies show positive outcomes, as instrumental support can positively shape behavioral and psychological processes, thereby enhancing both mental and physical health of older adults (Berkman et al., 2000). However, other scholars indicate that instrumental support can harm older adults’ well-being, especially if the support is excessive (Silverstein et al., 1996).
Among the widowed, greater instrumental support from children is linked to fewer depressive symptoms, though this effect may decrease over time (Ha, 2010; Li et al., 2005). Instrumental support tends to be especially beneficial for widowed men, wo often face new household roles (Umberson et al., 1992), given wives traditionally managed these responsibilities in the current older generations. In turn, when widows receive help with tasks they previously managed themselves, instrumental support may signify a notable loss of autonomy, potentially contributing to adverse mental health consequences (Tiedt et al., 2015).
Geographic Proximity
Living near children can shape older adults’ mental health through regular support and engagement (Cohen & Wills, 1985), fostering feeling of security and belonging (Van Der Pers et al., 2014), and increasing perceived social support (Fiori et al., 2006). However, living ‘too close’ to children may heighten depressive symptoms, especially if parents and children share a household (Caputo & Cagney, 2023; Jessee et al., 2025), though co-residence can offer emotional support, practical assistance, and financial benefits (Compton & Pollak, 2015).
For widowed individuals, the impact of geographical proximity is mixed: while it can be protective, it may also cause distress if it threatens parents’ autonomy, resulting in ambivalent feelings (Ha & Carr, 2006). In Europe, co-residence appears beneficial for widows well-being (Grundy & Murphy, 2018). Again, from a gender perspective, close proximity may be particularly important for men, given that they experience higher levels of loneliness following widowhood (Kapelle & Monden, 2024). Other studies report conflicting results, with one study finding greater benefits for widowers (J. A. Lee & Schafer, 2025; Liu et al., 2020), and others for widows (Van Der Pers et al., 2014), underscoring the need for further research on gendered effects of intergenerational proximity in widowhood.
Given mixed evidence on how adult children’s support shapes mental health well-being after spousal loss, we examine three key dimensions of support – contact frequency, instrumental support, and geographic proximity – and their associations with changes in depressive symptoms following widowhood. Given the lack of clear predictions, our approach is explicitly exploratory rather than hypothesis-driven. We also assess potential gender differences in these moderating effects. Understanding these dynamics is crucial, as it can inform the design of targeted social and health services that better support widowed individuals, particularly in aging societies where informal family networks play a central role. Insights from this study may also guide policy development around bereavement support, caregiving structures, and mental health interventions tailored to gender-specific needs.
Method
Sample
We draw on eight waves (1, 2, 4, 5, 6, 7, 8 and 9) of SHARE, a longitudinal, cross-national, and multidisciplinary survey of middle-aged and older adults (50+) in Europe and Israel (Börsch-Supan et al., 2013). SHARE is especially valuable for our study because it offers a range of social support measures linked to adult children and provides a large enough sample size to analyze widowhood effects for both men and women. Waves 3 and 7 include the SHARELIFE retrospective life-course questions. In wave 3, all respondents complete SHARELIFE, but in wave 7 only those who missed wave 3 do so. Accordingly, we dropped wave 3 entirely and limited our sample to respondents who took the standard SHARE interview, excluding anyone who participated in the SHARELIFE module in wave 7.
We included 26 European countries that participated in at least two waves, namely Austria, Belgium, Bulgaria, Croatia, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden, and Switzerland. Ireland was excluded as it only participated in one wave; Israel was excluded as the only non-European country.
For our baseline sample, we only selected individuals that were married at baseline and experienced spousal loss throughout the observation period. Our estimation strategy focuses exclusively on the respondents experiencing widowhood, introducing interaction terms to capture heterogeneity within this group – specifically, whether widowed individuals receive instrumental support from adult children, how frequently they’re in contact with them, and how close they live to their nearest adult child. While this approach yields rich insights into heterogeneity across those dimensions, it also prevents us from constructing a parallel control group of constantly married individuals, since we cannot replicate those same subgroup definitions outside the treated sample. The baseline sample therefore comprises 25,861 observations from 5,430 individuals who experienced spousal loss during the observation period. Our sample was further limited to respondents with at least one adult child, as adult children usually possess the autonomy and resources to provide instrumental support, like grocery shopping or household maintenance, that minors are generally unable to deliver. Therefore, we excluded individuals without adult children (i.e., 18 years or older; N = 470 individuals). We excluded respondents with missing values on our dependent and independent variables (N = 643 individuals). Missing data were particularly high for our moderator variable, contact frequency, because information on relationships with children was collected only from the designated household respondent. However, since contact frequency can vary between parents within the same home (whereas, for instance, proximity remains constant for all household members), we did not carry this information over to other members of the household. Moreover, we excluded respondents with only one wave of information (N = 485 individuals) and again, continuously married respondents (N = 336 individuals). As a result, we obtained a total analytical sample of 11,636 observations from 3,496 individuals. Among them, 896 men and 2,600 women experienced widowhood over the observation period.
Measures
Dependent Variable
Our main dependent variable, the number of depressive symptoms, was measured using the EURO-D scale, a validated scale for the cross-national measurement of depressive symptoms in older adults. Twelve items are used to measure depressive symptoms, among them pessimism, death wish and feelings of guilt. Respondents indicate whether they have experienced each symptom in the past year, with responses scored as 1 (yes) or 0 (no). The items are summed to create a scale from 0 (no symptoms) to 12 (all symptoms). A higher score reflects greater depression, with a score of four or more symptoms indicating a high likelihood of clinical depression (Prince et al., 1999). Due to our analytical approach (see description on fixed effects models below), the estimated effects should be interpreted as within-individual changes in depressive symptoms. When we repeated the analyses with a binary depression measure (1 = depressed, 0 = not depressed), the results followed the same patterns as when focusing on the number of depression as a continuous variable.
Independent Variable
The main explanatory variable was the shift in marital status: respondents are classified as widowed once their self-reported marital status changes from “married” (=0) to “widowed.” (=1).
Moderator Variables
We measured social support from adult children using three variables: (a) Contact frequency, (b) instrumental support, and (c) geographic proximity. We measured social support from adult children in the wave of partner loss, as this study focuses on the immediate resources for coping with widowhood rather than on changing support patterns in the years following partner loss. Opting for a time-invariant moderator is further justified by recent simulations demonstrating that interactions between two time-varying variables in a fixed-effects model may yield spurious findings (Giesselmann & Schmidt-Catran, 2022).
Contact frequency was measured by the question: “During the past 12 months, how often have you been in contact with your child – whether in person, by telephone, or by mail?” Response categories are: daily, several times a week, about once a week, about every two weeks, about once a month, less than once a month, and never. Following Tosi & Grundy (2019), participants were classified as (1) in weekly contact with all children, (2) in weekly contact with one child and less than weekly with the others, and (3) in less than weekly contact with all their children. Parents with one child were classified as having either frequent (1) or infrequent (3) contact with their child.
Instrumental support was measured by asking respondents if, in the last twelve months, they received personal care, help with household work, or help with paperwork from anyone not living in the household, and second, from whom. SHARE allows respondents to list up to three primary helpers, but we only included support provisions from adult children. A binary variable indicated whether respondents received such support (1 = yes). Unfortunately, SHARE does not consistently record how often help is received across all waves, limiting our ability to analyse support frequency in more detail. We also recognise that ‘help’ and ‘care’ represent conceptually distinct forms of functional support (Brandt et al., 2009). Unfortunately, sample sizes become too small to model these categories separately.
Finally, to account for the structural availability of support from adult children, we included a measure of the geographic proximity of the bereaved parent to their closest living child. Although the nearest child may not always be the first to help in times of need, simply having one child nearby creates opportunities for support and contact, giving parents a sense of security and belonging. SHARE records proximity in nine categories: (1) same household; (2) same building; (3) <1 km; (4) 1–5 km; (5) 5–25 km; (6) 25–100 km; (7) 100–500 km; (8) >500 km; and (9) >500 km in another country. For analysis, we condensed these into three groups: (1) co-residence (i.e., living in the same household or the same building), (2) living less than 25 km from the closest living child, and (3) living more than 25 km away from the closest living child.
Time-Varying Covariates
Our fixed effects models account for time-varying covariates related to widowhood and depressive symptoms, while time-constant variables like education, personality traits, relationship duration and country are already controlled for (see description on fixed effects models below). Our model controlled for respondents’ age (in years), a dichotomous variable on current employment status (1 = employed or self-employed vs. 0 = retired, unemployed, constantly sick or disabled, homemaker), financial hardship, and self-rated health. Financial hardship was measured by the question “Thinking of your household’s total monthly income, would you say that your household can make ends meet … a) with great difficulties, b) with some difficulties, c) fairly easy, or d) easy?”. Financial hardship was dichotomized, contrasting respondents with great or some hardship (1) and those with no hardship (fairly easy or easy, (0)). Respondents’ overall health was measured using self-rated health (1 = excellent to 5 = very poor).
Analytical Approach
We first compared unadjusted depressive symptoms levels among the widowed by gender and social support by adult children. To test for significant differences between groups, we used analysis of variance (ANOVA) with post-hoc comparisons and t-test.
Next, we turn to fixed-effects panel regression models (FEM) to examine how social support from adult children moderates the association between widowhood and depressive symptoms. FEM estimate how within-individual changes in the explanatory variable (i.e., the transition to widowhood) relates to within-individual changes in the outcome variable (i.e., depressive symptoms) over time. FEM uses each individual as his or her own control, comparing an individual’s level of depressive symptoms before and after widowhood. FEM (unlike cross-sectional analyses) capture unobserved heterogeneity across individuals that is fixed over time (Wooldridge, 2002).
To capture whether the change in depressive symptoms differs depending on social support from adult children, we estimated Ordinary Least Squares (OLS) linear regression models using the following equation:

Results
Descriptive Results
Descriptive Sample Statistics (Unweighted)
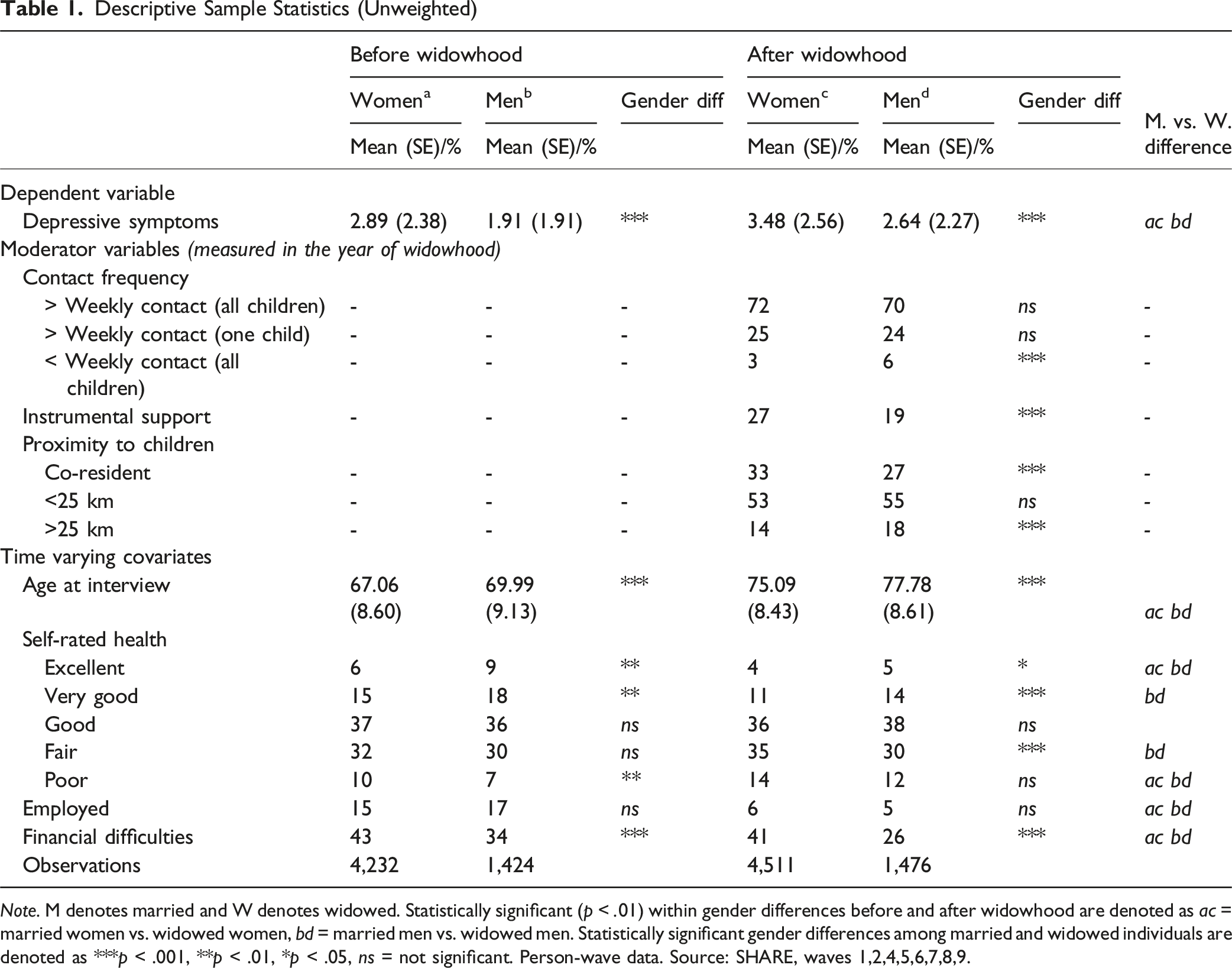
Note. M denotes married and W denotes widowed. Statistically significant (p < .01) within gender differences before and after widowhood are denoted as ac = married women vs. widowed women, bd = married men vs. widowed men. Statistically significant gender differences among married and widowed individuals are denoted as ***p < .001, **p < .01, *p < .05, ns = not significant. Person-wave data. Source: SHARE, waves 1,2,4,5,6,7,8,9.
When examining our moderator variables, we find that, during the year of widowhood, the majority of both women and men maintained more than weekly contact with all of their children (72 % vs. 70 %). Men, however, were significantly more likely than women to have less than weekly contact with all of their children. Over one quarter of women (27 %) received instrumental support during the year of widowhood; a significantly higher share than that observed among men (19 %). Finally, more than half of women and men lived within 25 km of their nearest child, and roughly one third reported co-residence with at least one child (33 % of women vs. 27 % of men).
We next investigate how social support from adult children in the year of spousal loss relates to depressive symptoms among widowed men and women. Figure 1 plots average depressive symptoms scores by contact frequency, instrumental help, and geographic proximity measured in the year of spousal loss. To determine which subgroup differences are statistically significant, we employ t-tests and ANOVA followed by post-hoc tests. Unadjusted Depressive Symptoms (Euro-D) by Gender and Social Support From Adult Children (a) Contact frequency, (B) Instrumental help, (c) Geographic proximity. Notes. Results are Based on Unweighted Data From SHARE, Waves 1, 2, 4, 5, 6, 7, 8, 9 Release 9.0.0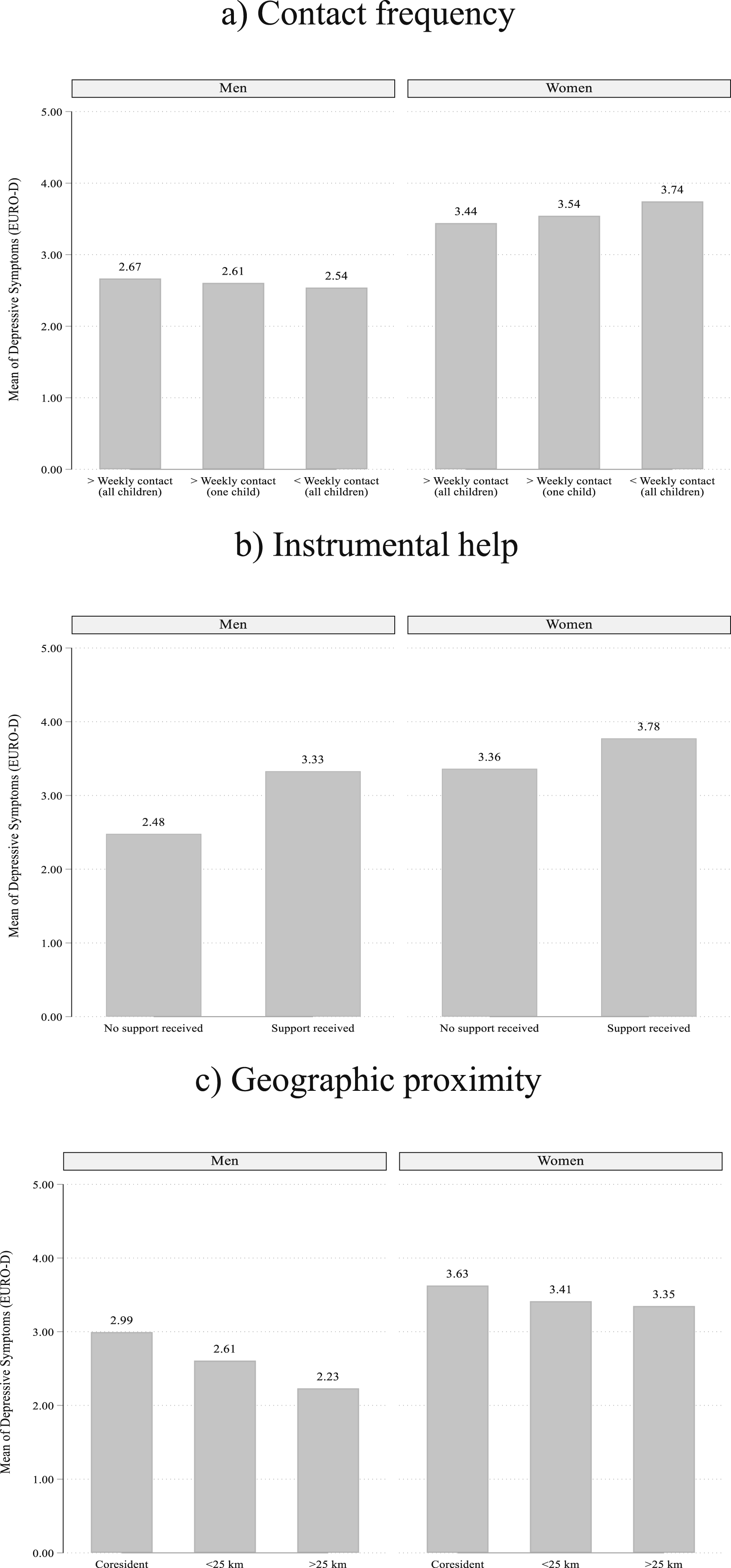
We found no significant difference in the number of depressive symptoms among widowed men and women by contact frequency with children. In contrast, both widowed men and women who received instrumental support reported significantly more symptoms than those who did not. A similar pattern emerged for geographic proximity: widowed men and women co-residing with their children had a significantly higher number of depressive symptoms compared to the other categories. Although the overall patterns were similar for both genders, women consistently exhibited higher depressive symptom scores than men across all levels of support, reflecting established gender disparities in depression.
Results from Fixed Effects Panel Regression
Mean depressive symptoms levels in Figure 1 suggest an association between social support by adult children and depressive symptoms among the widowed. However, these bivariate associations may be misleading, since both observed and unobserved factors may confound the relationship between widowhood, depression, and support. To address this, we next turn to our multivariable fixed effects panel regressions that isolate within-person change in depressive symptoms scores and test whether a change in depressive symptoms is moderated by (a) contact frequency, (b) instrumental support, and (c) geographic proximity to adult children.
Fixed Effects Linear Regression Coefficients Predicting Changes in Depressive Symptoms by Social Support From Children
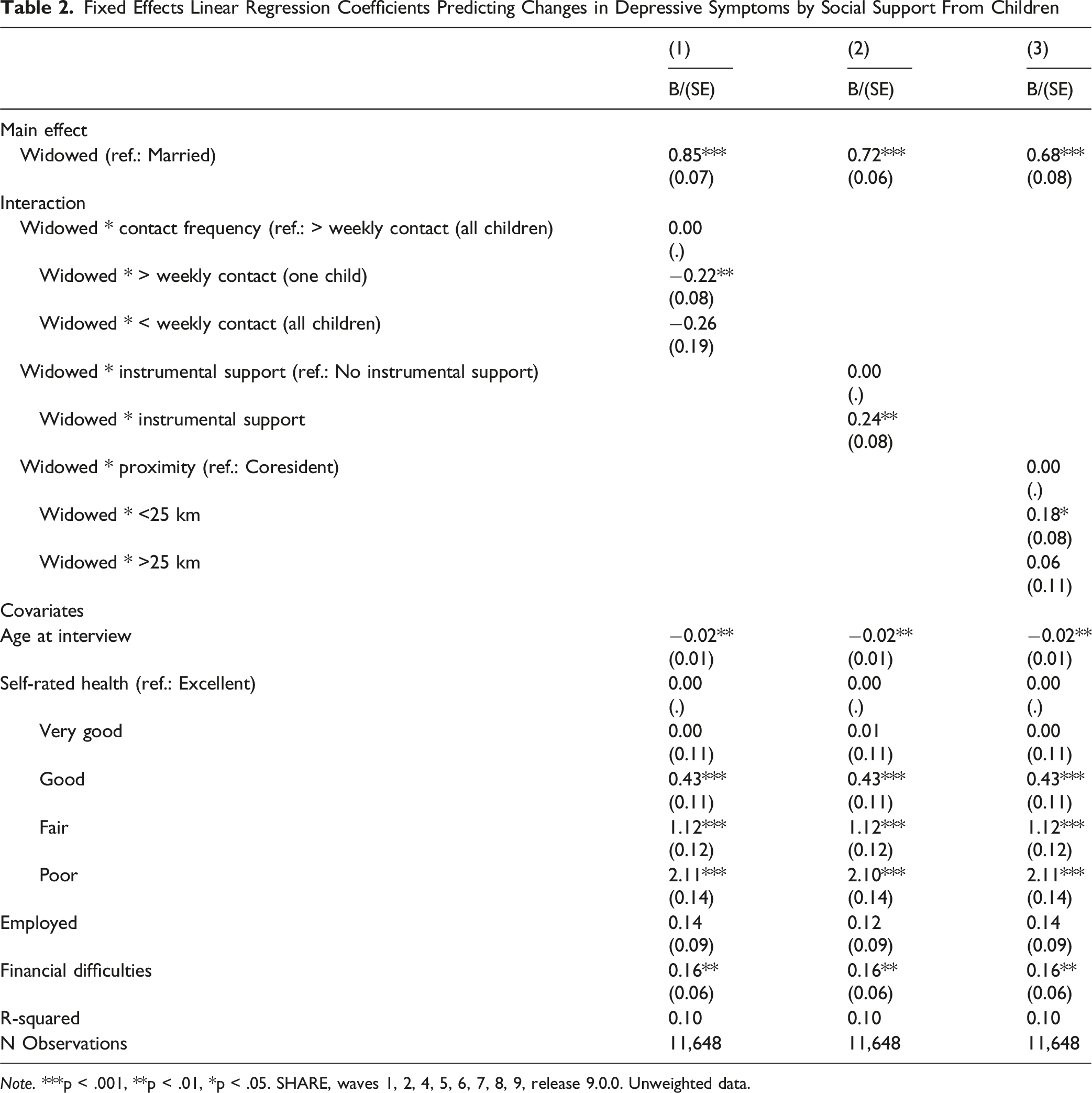
Note. ***p < .001, **p < .01, *p < .05. SHARE, waves 1, 2, 4, 5, 6, 7, 8, 9, release 9.0.0. Unweighted data.
Second, turning to instrumental support from children (Model 2), the model shows that the increase in depressive symptoms following widowhood was 0.24 points larger for respondents who received instrumental support from their children compared to respondents who did not.
Third, we found that increases in individuals depressive symptoms following widowhood were 0.18 points larger when they lived less than 25 km away from their closest living child compared to respondents that cohabited with their children (Model 3). We did not find evidence that living more than 25 km away from a closest living child affected parents’ depressive symptom change following widowhood.
Fixed Effects Linear Regression Coefficients Predicting Changes in Depressive Symptoms by Social Support From Children, Gender Differences
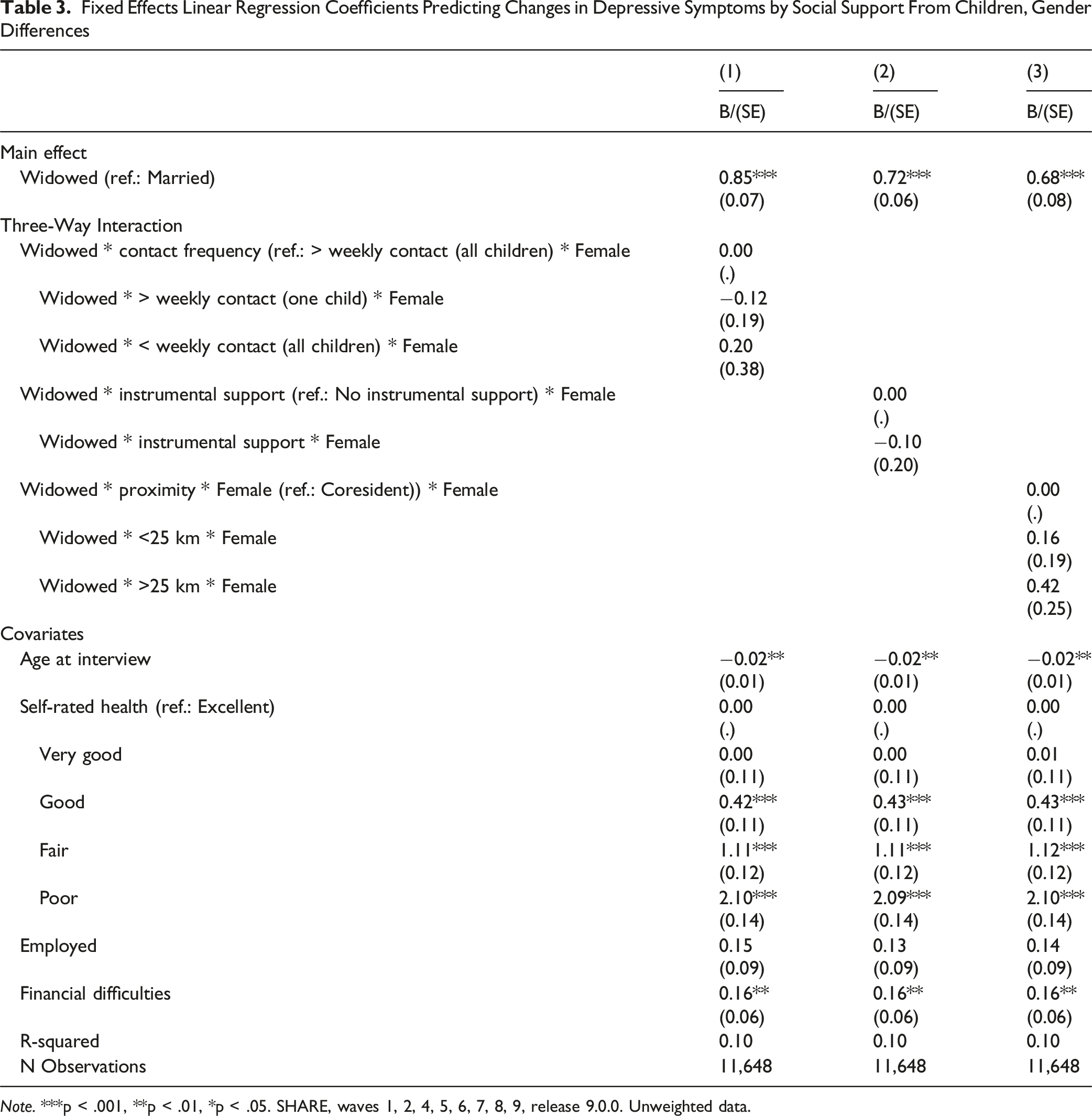
Note. ***p < .001, **p < .01, *p < .05. SHARE, waves 1, 2, 4, 5, 6, 7, 8, 9, release 9.0.0. Unweighted data.
Discussion
Using data from eight waves of SHARE, this study explored how social support (contact frequency, instrumental support, geographic proximity) from adult children moderates depressive symptoms following widowhood, with a specific focus on gender differences.
We find that, first, both widows and widowers benefited from having at least weekly contact with one child rather than having such contact with all children. Based on the social breakdown hypothesis, we assume that ‘too much’ contact with all children may signal an interference with parents’ autonomy (Silverstein et al., 1996). This aligns with prior findings showing that more contact with significant others isn’t always better (Grundy & Read, 2012). These effects may further arise from trade-offs between quantity and quality of relationships, such that it is better to be more selective in regard to which children to maintain frequent contact with. As Ha and Ingersoll-Dayton (2011) have shown the perceived adequacy and quality of support and contact may be more consequential for widowed individuals’ well-being than the quantity itself.
In line with that, our analyses indicate that, second, both widows and widowers who received instrumental support experienced a greater increase in depressive symptoms, compared to those who did not receive such support at the time of widowhood. When adult children take over tasks previously managed by widows, instrumental support may signify a notable loss of autonomy, potentially contributing to the observed adverse mental health consequences for widowed women (Tiedt et al., 2015). Furthermore, because social norms often pressure men to be independent and self-reliant (Thoits, 1995), receiving instrumental support may undermine their sense of independence and autonomy (Silverstein et al., 1996).
Third, widowed women and men showed higher increases in depressive symptoms when living within 25 km of a child compared to those cohabiting with their children. Whereas this contradicts recent findings from the U.S. linking co-residence to poorer parental mental health (Caputo & Cagney, 2023; Jessee et al., 2025), it is in line with European findings that highlight its protective effects (Aranda, 2015; Courtin & Avendano, 2016). In Europe, intergenerational relationships are generally closer, and intergenerational co-residence is a common form of support exchange in many contexts (Albertini & Kohli, 2013). Such living arrangements may buffer against loneliness (Aranda, 2015), which often follows spousal loss (Kapelle & Monden, 2024), and may protect against financial vulnerability through joint household cost-sharing (Compton & Pollak, 2015). Thus, although excessive contact or support can harm well-being, co-residence appears beneficial, likely reflecting emotionally close parent–child relationships. However, as our data cannot capture reasons for or quality of co-residence, qualitative research is needed to clarify why some forms of support help while others hinder.
Finally, we found no gender differences in the moderating effect of social support on the mental health consequences of widowhood. This aligns with evidence that gender differences narrow in later life across various domains (gender gap convergence; e.g., Jessee & Carr, 2025a; Leopold et al., 2018). Our results suggest adult children’s support relates similarly to depressive symptoms in widowed women and men. Although gender differences were absent in our moderation analyses – consistent with prior research on the psychological effects of widowhood (H. J. Lee et al., 2016; Sasson & Umberson, 2014; Schaan, 2013; Schmitz, 2021) – widowed women remain a high-risk group, showing substantially higher depressive symptoms with men. Their average depressive symptom count far exceeds that of widowed men. For instance, women who received instrumental support reported nearly four symptoms on average, close to the threshold for a manifest depression (Prince et al., 1999), highlighting an urgent need for targeted, gender-sensitive mental health support.
Several limitations of our study must be considered: First, our focus on adult-child support at the time of widowhood overlooks later changes in social networks and relationship with children (Ha, 2008). Widowhood can both expand and diminish ties, and losses that may disproportionately affect men, who are generally less proficient than women at sustaining kin ties (Hornstra & Ivanova, 2023) and often report less support than widowed women, especially after repartnering (Jiao et al., 2021; Kalmijn, 2007). Such fluctuations in social support may mediate bereavement-related depression but lie beyond the scope of our current analysis.
Second, due to data constraints, we analyzed only common support dimensions. Although SHARE includes information on financial transfers from children - an important aspect of functional solidarity (Deindl & Brandt, 2011) - such support is relatively uncommon in Europe. Consequently, small cell sizes did not allow gender-sensitive analyses. However, supplementary analyses suggest that financial support does not matter in the association of widowhood and depressive symptoms in the pooled sample (results available from authors). Similarly, we did not differentiate by the child’s gender, although previous research has documented notable differences in intergenerational ties by both parents’ and children’s gender (Fingerman et al., 2020). Moreover, SHARE data do not allow us to examine the perceived adequacy or quality of support or the relationship, which prior research has shown to be more consequential for mental health outcomes following widowhood than contact or support frequency (Ha & Ingersoll-Dayton, 2011).
Third, causality cannot be inferred, as social support and mental health likely influence one another, so that poorer mental health may elicit greater support from children, rather than support affecting mental health (Jessee, 2023; Jessee et al., 2025).
Finally, although we pooled SHARE data, cross-national differences may shape these associations. Depressive symptoms after widowhood are particularly high in Southern Europe, linked to greater loneliness and financial strains (Schmitz, 2021). The mental health effects of children’s support may also depend on cultural norms and national variations in gender roles and welfare systems. Future research should examine these contextual differences to better understand patterns in the post-widowhood support and well-being relationship.
Conclusion
Our findings highlight the need for tailored support strategies, that focus on the type of support by fostering emotionally meaningful ties with at least one child, offering instrumental support that preserves autonomy, and encouraging intergenerational co-residence where feasible. The findings further highlight that the moderating effects of adult children’s support do not differ by gender. This suggests that although baseline mental health varies, the ways in which adult children’s support influences psychological adjustment to widowhood are broadly similar for both women and men. Still, women remain at higher overall risk due to their higher baseline levels of depressive symptoms, underscoring the need for gender-sensitive support strategies that address women’s distinct life course and socioeconomic vulnerabilities.
Footnotes
Acknowledgements
This collaboration was supported by the Minerva Foundation, from which Alina Schmitz and Ella Cohn-Schwartz received funding for the German-Israeli Minerva School „Social networks and health inequalities in ageing societies“. The authors would like to thank Rümeysa Kahraman and Hanna Wilmes for her editorial support.
ORCID iDs
Ethical Approval
This study is a secondary data analysis, and therefore, no new ethics approval was required. The data used in this analysis was obtained from the SHARE (Survey of Health, Ageing and Retirement in Europe) project. SHARE has undergone numerous ethical reviews. Detailed information regarding the ethical guidelines and reviews conducted for SHARE can be found at the following link: ![]() .
.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Minerva Foundation, from which Alina Schmitz and Ella Cohn-Schwartz received funding for the German-Israeli Minerva School “Social networks and health inequalities in ageing societies”.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This paper uses data from SHARE Waves 1, 2, 3, 4, 5, 6, 7, 8 and 9 (DOIs: 10.6103/SHARE.w1.900, 10.6103/SHARE.w2.900, 10.6103/SHARE.w3.900, 10.6103/SHARE.w4.900, 10.6103/SHARE.w5.900, 10.6103/SHARE.w6.900, 10.6103/SHARE.w7.900, 10.6103/SHARE.w8.900, 10.6103/SHARE.w8ca.900, 10.6103/SHARE.w9.900, 10.6103/SHARE.w9ca900); see Börsch-Supan et al. (2013) for methodological details. (1) The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GAN211909, SHARE-LEAP: GA N227822, SHARE M4: GA N261982, DASISH: GA N283646) and Horizon 2020 (SHARE-DEV3: GA N676536, SHARE-COHESION: GA N870628, SERISS: GAN654221, SSHOC: GA N823782, SHARE-COVID19: GA N101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, VS 2020/0313 and SHARE-EUCOV: GA N101052589 and EUCOVII: GA N101102412. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, BSR12-04, R01_AG052527-02, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see ![]() ).
).