
Abstract
This paper aims to address the research questions of whether individual’s oral health status is associated with subjective well-being, as well as if there is possible moderating role of self-rated oral health among two groups of Chinese older adults (≥55 years old) in Honolulu, Hawaiʻi and Taichung, Taiwan. Using survey data collected in 2018 (N = 430, Honolulu) and in 2017 (N = 645, Taichung), ordinary least square regressions were applied. Results showed that, for both samples, oral health status was negatively and significantly associated with subjective well-being, and both associations were moderated by self-rated oral health. In addition, the moderating effects were more salient for the Honolulu sample, who enjoyed higher levels of self-rated oral health and life satisfaction. These results suggest the significant associations of both oral health status and self-rated oral health on individual health and well-being for Chinese older adults residing in different cultural contexts.
Introduction
Oral health is essential to the general health and well-being of older adults. Tooth loss and periodontitis are common among adults over 55 years old and have been considered as part of normal aging (Chan et al., 2021; Shimazaki et al., 2001). However, oral health problems such as dental caries and oral diseases are also prevalent among older adults and these problems appear to be linked to physical and mental decline in older adults (Petersen & Ogawa, 2018). Researchers have developed self-reported oral health outcomes such as “oral-health-related quality of life” to assess the extent to which oral health problems affect functioning and overall well-being of individuals (Slade, 1997). For instance, these problems affect chewing and communication ability, thus, not only diminish the pleasure of eating but also lead to other health problems such as nutritional inadequacy and psychological distress (Griffin et al., 2012). Severe tooth loss may also reduce social engagement, which in turn, could limit social interactions and reduce levels of self-esteem of older adults (Starr & Hall, 2010). Untreated oral health problems and diseases can profoundly impact quality of life and disturb sleep. Failure to prevent or control oral diseases may increase the risk of adverse health outcomes including type-2 diabetes, ischemic stroke and myocardial infarctions (Minassian et al., 2010; Simpson et al., 2015). On the other hand, studies found positive associations between good oral hygiene and health outcomes, showing that enhanced oral hygiene may prevent respiratory infection and death from pneumonia among older adults (Pace & McCullough, 2010). Good oral health was also important for social interactions and general well-being of older adults (Gerritsen et al., 2010; Gülcan et al., 2014).
Although not very well-studied, oral health problems, such as tooth loss and edentulism, were found to be related to individual’s subjective well-being (Rouxel et al., 2018). Subjective well-being (often indicated by life satisfaction and happiness) has been studied and used as a valid indicator of individual quality of life (Piqueras et al., 2011). Studies have documented the significant independent effect of oral health status on poor individual well-being, indicating the direct relationship (Gülcan et al., 2014; Kandelman et al., 2008; Tsakos et al., 2001). However, this negative pathway linking oral health status and subjective well-being among older adults is not conclusive and could be moderated by self-rated oral health. Perception of one’s own oral health has also been found to affect individual well-being, and studies revealed that poor self-rated oral health and poor quality of life co-existed in the same group of older adults, and self-rated oral health was also found to be significantly associated with self-esteem, psychological well-being, and life satisfaction (Chen et al., 2013; Jones et al., 2001; Kotha et al., 2017; Locker et al., 2000). Based on the process of social comparison, individuals carry out self-evaluations by comparing with others (Festinger, 1954): Some individuals tended to compare themselves with those who were better than them with the desire to improve current status or level of ability, while others would prefer comparing to those who were worse off, in an effort to make themselves feel better about their abilities or traits (Collins, 1996; Wills, 1981). These different approaches may lead to diverse health perceptions and studies revealed that social comparison especially influenced subjective age and self-rated health among older adults (Sayag & Kavé, 2022). Previous studies have also suggested that individual health perception could be considered as an important moderator in linking physical health and subjective well-being (Jahn & Cukrowicz, 2012; Su et al., 2019). Based on these findings, it would be reasonable to hypothesize that older adults may have similar degrees of oral health status but positive/negative perceptions of their oral health, thus may result in different levels of well-being. In this sense, the subjective perception of oral health (i.e., self-rated oral health) could represent an important intervening factor between objective oral health status and individual well-being.
While self-reported oral health is strongly associated with self-reported general health, it has its distinctive feature (Wong et al., 2019). Studies revealed that self-rated oral health has a unique role in individual overall health which is not fully captured by self-rated health. It was found that the influence of self-rated oral health on individual well-being, for instance, self-esteem and life satisfaction, is independent of the effect of self-rated health (Benyamini et al., 2004). Self-rated oral health was also seldomly used as a moderator when studying individual health behaviors and well-being, despite its independent contribution to individual health (Jahn & Cukrowicz, 2012; Vigu & Stanciu, 2019; Vigu et al., 2018). Therefore, this paper hypothesizes that self-rated oral health could have a unique moderating role on the relationship between oral health status and individual well-being. For instance, among older adults with the same level of oral health status, those rating themselves as in better oral health may report higher levels of well-being compared to others.
Moreover, older adults’ perceptions of health, both general health and oral health, could be contingent on the sociocultural context in which they were embedded (Falk et al., 2017). It was reported that older adults in Asian countries often showed relatively poorer self-rated health compared to their higher life expectancy. Conversely, self-rated health in the U.S. and Canada tended to lean toward the positive side and on average scored higher (Choi & Miyamoto, 2022; Lee & Shinkai, 2003). One explanation would be that older adults in Asia were more influenced by the traditional Confucius “golden mean” and humility thinking and tend to rate themselves as in the middle between extremes (Kim et al., 2001). But under the Western cultural context, humility might be considered as a sign of weakness (Xu et al., 2019). Such cultural differences indicate that, Chinese older adults, under the influence of mixed cultures (i.e., both Chinese and American cultures), might show more positive psychological outlooks and higher levels of self-evaluation of health than their counterparts who were largely only immersed in the traditional Chinese culture (Zhang et al., 2018). Therefore, it would be interesting and meaningful to examine the similarities and differences in the focal relationship among Chinese older adults residing in different cultural contexts, and in this study, we aim to examine the moderating role of self-rated oral health among two groups of Chinese older adults living in Honolulu, Hawaiʻi and Taichung, Taiwan.
Statistics from U.S. Census Bureau (2018) showed that the Chinese comprised 14.82% of the Honolulu population and constituted about 4.7% of the state population. Data from Hawaiʻi Department of Health showed that the life expectancy at birth of Chinese Americans were 90 and 85.3 for females and males in 2010 (Wu et al., 2017). Meanwhile, Taichung is the second largest city in Taiwan, located in the middle of the west coast. According to Taichung City statistics, the average life expectancy climbed from 78.98 in 2010 to 81.11 in 2020, and the percentage of older population ascended from 8.69% to 13.63% in the same period (Taichung City Government, 2021). The two samples were included not only because of their similar long-life expectancy but also due to the different health care systems, cultural values, access to care and environment that the two groups had access to, enabling the comparison (Ridic et al., 2012; Wu et al., 2010).
Taken together, this study aims to investigate the association between oral health status and subjective well-being, as well as how self-rated oral health moderates the relationship under different cultural backgrounds. The conceptual framework is summarized in Figure 1. Conceptual framework.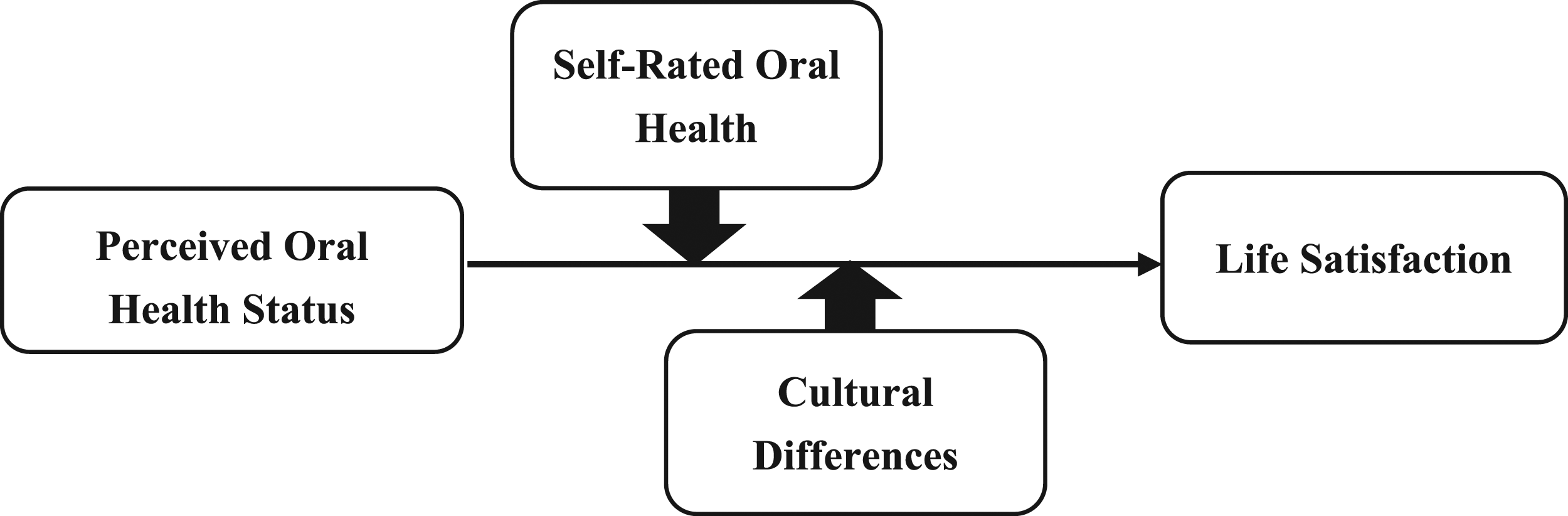
Methods
Data
Sampling
The survey data used in this study were collected in Honolulu, Hawaiʻi in 2018 and Taichung, Taiwan in 2017. Data from Honolulu were primarily collected from local Chinese communities, for instance, clubs based on kinship or village of origin, professional associations and social or religious societies using snowball and convenience sampling strategies.
Data of Taichung in this study were from the 2017 Taichung Good Elderly Life Survey, which was supported by the Taiwan Ministry of Science and Technology and conducted by Tunghai University from April to August 2017. The sampling scheme targeted a population between the ages of 56 and 85 based on the household registration information provided by the Taichung Civil Affairs Bureau in December 2016, and four-stage (i.e., cities/counties, districts, administrative neighborhoods, and individuals) stratified random sampling was applied
Collection Procedure
For data from Honolulu, survey inclusion criteria were: 55 years of age and older, self-identified as Chinese, and able to give informed consent. The data collection in Honolulu were conducted in Mandarin, Cantonese or English, and detailed data collection strategies have been reported in previous studies (Zhang et al., 2020). From January to September 2018, a total of 430 respondents completed the survey questionnaire.
Data collection procedure in Taichung adopted the same screening criteria. A total of 645 questionnaires were collected from 1600 potential older adults using four-stage stratified random sampling with the “probability proportional to their size” method and face-to-face interviews in Mandarin or Taiwanese.
Measurement
Dependent Variable
Survey questions and responses used in this study were mostly similar across two study sites, except for a few areas (as explained in the following subsection on moderator). Subjective well-being is a self-reported measure of well-being and was indicated by life satisfaction in this study. Life satisfaction was measured using the Satisfaction with Life Scale (SWLS) developed by Diener et al. (1985), and has been widely used as a valid assessment of individual’s judgement of their satisfaction with their life as a whole (Cheung & Lucas, 2014; López-Ortega et al., 2016; Pavot & Diener, 2009). Life satisfaction was a composite index across five statements: “In most ways my life is close to ideal,” “The status of my life are very good,” “I am satisfied with my life,” “So far, I have gotten the important things I want in my life,” and “If I could live my life again, I would change nothing.” Answers ranged from “1 = strongly disagree” to “5 = strongly agree,” and an average index was computed, with higher scores reflecting higher levels of life satisfaction. The Cronbach’s Alphas for the Honolulu and Taichung samples were 0.928 and 0.862, respectively.
Focal Independent Variable
Oral health status was measured using the following three questions: “In the last year, have you avoided particular foods because of problems with your teeth, mouth, or dentures?” “In the last year, have your teeth or gums been sensitive to hot, cold, or sweets?” and “In the last year, have your gums bled when you brushed your teeth?” Responses to the three questions ranged from “1 = very often” to “5 = never.” We reversely coded the responses and the summary scale ranged from 3 to 15, with higher scores reflecting worse oral health status. This aggregated measure has been used and was found to be a valid measure in previous studies (Wu et al., 2020). The Cronbach’s Alphas for the summary scales were 0.803 and 0.734 for the Honolulu and Taichung samples respectively.
Moderator
Self-rated oral health was measured by asking respondents, “How would you describe the condition of your mouth and teeth?” Responses in the questionnaire used in Honolulu ranged from “1 = very poor,” “2 = poor,” “3 = fair” to “4 = good,” “5 = very good”; while responses in the questionnaire used in Taichung only had four options: “1 = very good, 2 = good, 3 = fair, 4 = not good.” We carried out the following operationalizations: firstly, in the Honolulu coding, we combined 1 and 2 as “not good” to keep in line with the coding in the Taichung coding, and after that, we reversely coded the responses such that higher scores indicate higher levels of self-rated oral health.
The moderator is different from the independent variable in that oral health status consists of comparative objective reports of whether certain oral health problems (chewing, sensitivity, and gum bleeding) exist, while the moderator, self-rated oral health is a more subjective judgement, and the outcome might be influenced by social comparison.
Covariates
Covariates included demographic characteristics such as age (in years), gender (male = 1), marital status (married/partnered = 1), education (≥high school = 1), and annual family income. For annual family income, currency exchange rates and commodity prices were taken into consideration and the options were unified ranging from “1 = under 18,000 USD” to “5 = more than 150,000 USD.” Individual health behaviors such as smoking (“current smoker,” “past smoker,” and “never”), drinking (yes = 1) and frequency of physical exercises (from “1 = never” to “5 = everyday”) were also included. Lastly, we controlled individual health status: self-rated health (from “1 = very poor” to “5 = very good”) and number of chronic conditions (0–10).
Data Processing
Data analysis was conducted using R software (version 1.3.1093). Missing data were minimal, ranging from 0% to 5% for variables of interest. Multiple imputations were performed to account for the missing values of independent variables using chained equations imputation, also known as Markov chain Monte Carlo algorithm. Five integrated datasets were generated, using linear regression for continuous variables and logistic regression for categorical variables. The datasets were then analyzed separately, and the estimates obtained from each dataset were combined using Rubin’s rules (Rubin, 1987) to obtain one overall multiple imputation estimate.
Confirmatory Factor Analysis (CFA) was carried out to provide solid grounds for the use of our key measures.
Sample Characteristics for Chinese Older Adults in Honolulu and Taichung.
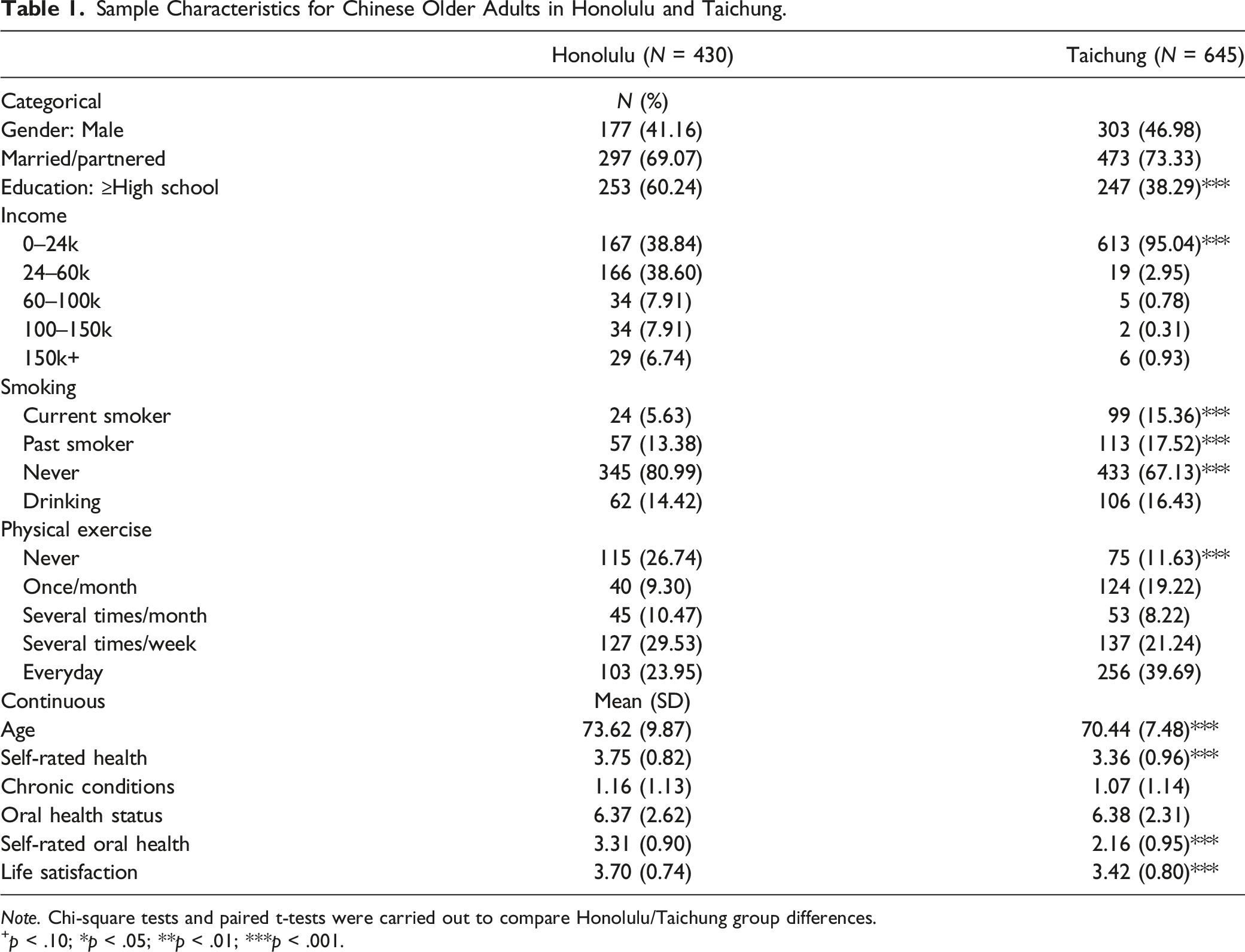
Note. Chi-square tests and paired t-tests were carried out to compare Honolulu/Taichung group differences.
+ p < .10; *p < .05; **p < .01; ***p < .001.
Results
Results from the CFA indicate that, for the Honolulu sample, the Comparative Fit Index (CFI) was 0.988 and Tucker-Lewis Index (TLI) was 0.982, which were quite ideal (>0.95); Root Mean Square Error of Approximation (RMSEA) was 0.059, which was close to ideal (<0.05) and the Standardized Root Mean Square Residual (SRMR) was 0.031, showing that our model was a good fit (<0.08). Overall, in the Honolulu sample, our decision to use the life satisfaction and oral health status scales were comparatively solid. For the Taichung sample, CFI and TLI were 0.982 and 0.974 respectively, while RMSEA was 0.052 and SRMR was 0.027. These results were quite close to those of the Honolulu sample, thus we deem the scales to be solid as well.
Table 1 summarizes the sample characteristics. It shows that differences in age, education, smoking behavior, and physical exercises between two samples were significant. In both samples, there were more females than males, with proportions of 58.84% and 53.02% in Honolulu and Taichung, respectively. Older adults in Honolulu were less likely to be married (69.07%) and enjoyed higher levels of education: More than 60% of older adults had an educational attainment of high school or above, whereas the percentage was only slightly higher than 38% in Taichung. Meanwhile, a greater proportion of older adults in Taichung had the habits of smoking (15.36%) and drinking (16.43%), but they were more likely (60.93%) to do physical exercises several times a week or every day when compared with their Honolulu counterparts (53.48%). On average, the Honolulu sample (73.62) was older than the Taichung sample (70.44), had more chronic conditions (1.16 vs. 1.07), but they rated themselves as in better health, scoring 3.75 out of 5 as compared with 3.36 for their Taichung counterparts. The two samples had similar levels of oral health status (6.37 vs. 6.38). However older adults in Honolulu reported significantly better self-rated oral health (3.31 out of 5) than their Taichung counterparts (2.16 out of 5). Lastly, both samples enjoyed high levels of life satisfaction, but still the Honolulu sample scored a little bit higher than the Taichung sample (3.70 vs. 3.42) and the difference is statistically significant.
Regress Life Satisfaction on Oral Health Status, Self-Rated Oral Health and Control Variables (Honolulu vs. Taichung).
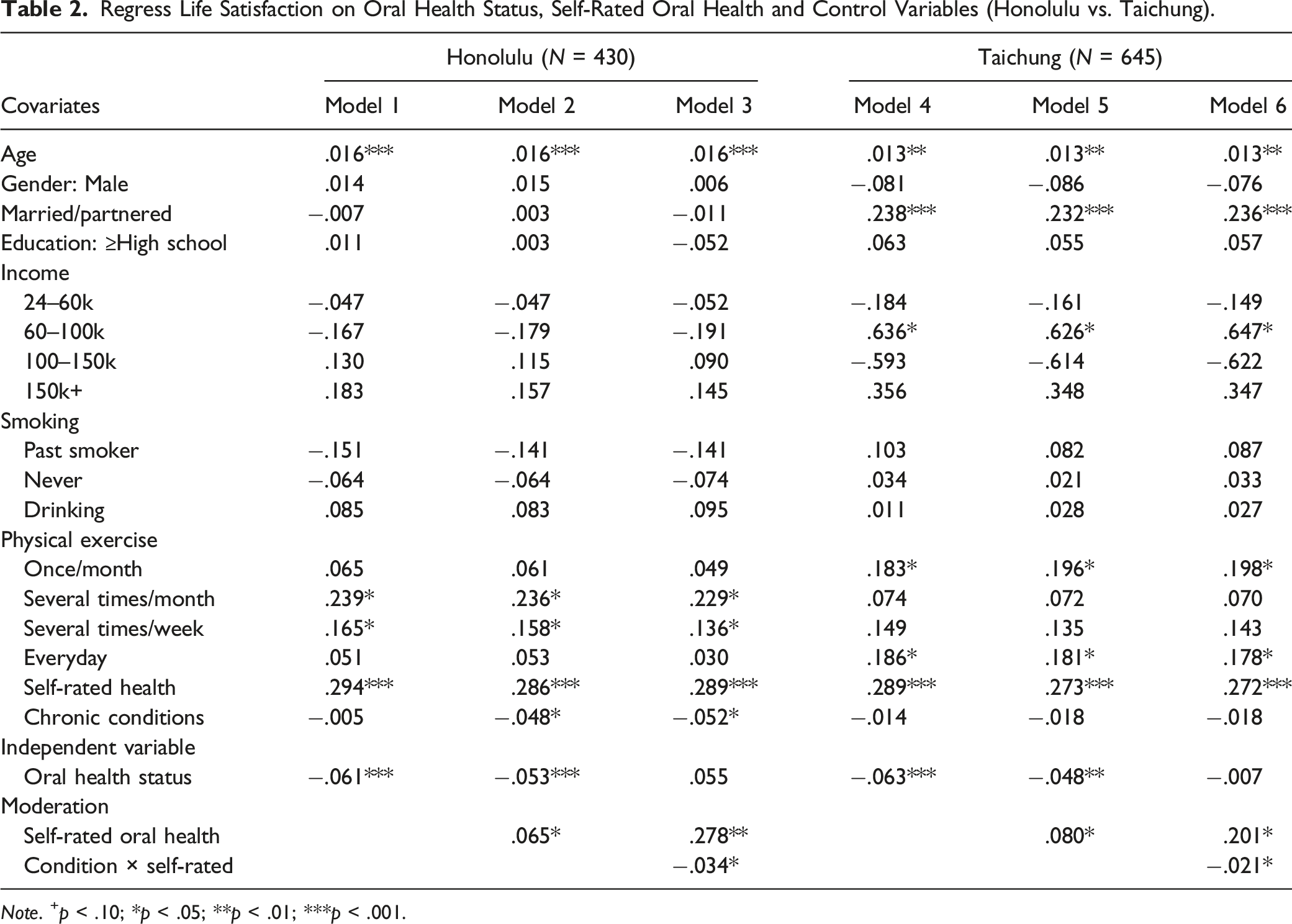
Note. + p < .10; *p < .05; **p < .01; ***p < .001.
Figure 2 visualized the moderating roles of self-rated oral health on the association between oral health problems and life satisfaction for the Honolulu and Taichung samples. There were three lines in both images, and these lines represented the three most populated groups in terms of self-rated oral health, and the percentages were included in the parentheses on the upper left. For the Honolulu sample, they were older adults who rated themselves as in “4. Very good (45%)”, “3. Good (43%)” and “2. Fair (9%)” oral health, while for the Taichung sample, they were the “3. Good (24%)” “2. Fair (38%)” and “1. not good (28%)” groups. On average, the Honolulu sample enjoyed higher levels of life satisfaction. In Figure 2(a), the intersection divided the moderation into two parts: For those whose oral health status scored below 11, higher levels of self-rated oral health could significantly increase the life satisfaction; while for those who had poorer oral health status, which accounted for about 2% of the sample, the moderating effects were negative. For the Taichung sample, the figure showed that for older adults with same oral health status, those rated themselves as in better oral health were more satisfied with life, and the steeper and more divergent lines in Figure 2(b) indicate that the moderating effect was stronger. This suggest that the older adults in Honolulu were more susceptible to the moderating role of self-rated oral health. Visualization of moderating effects of self-rated oral health on subjective well-being by place of residence. Note. “srt” refers to self-rated oral health.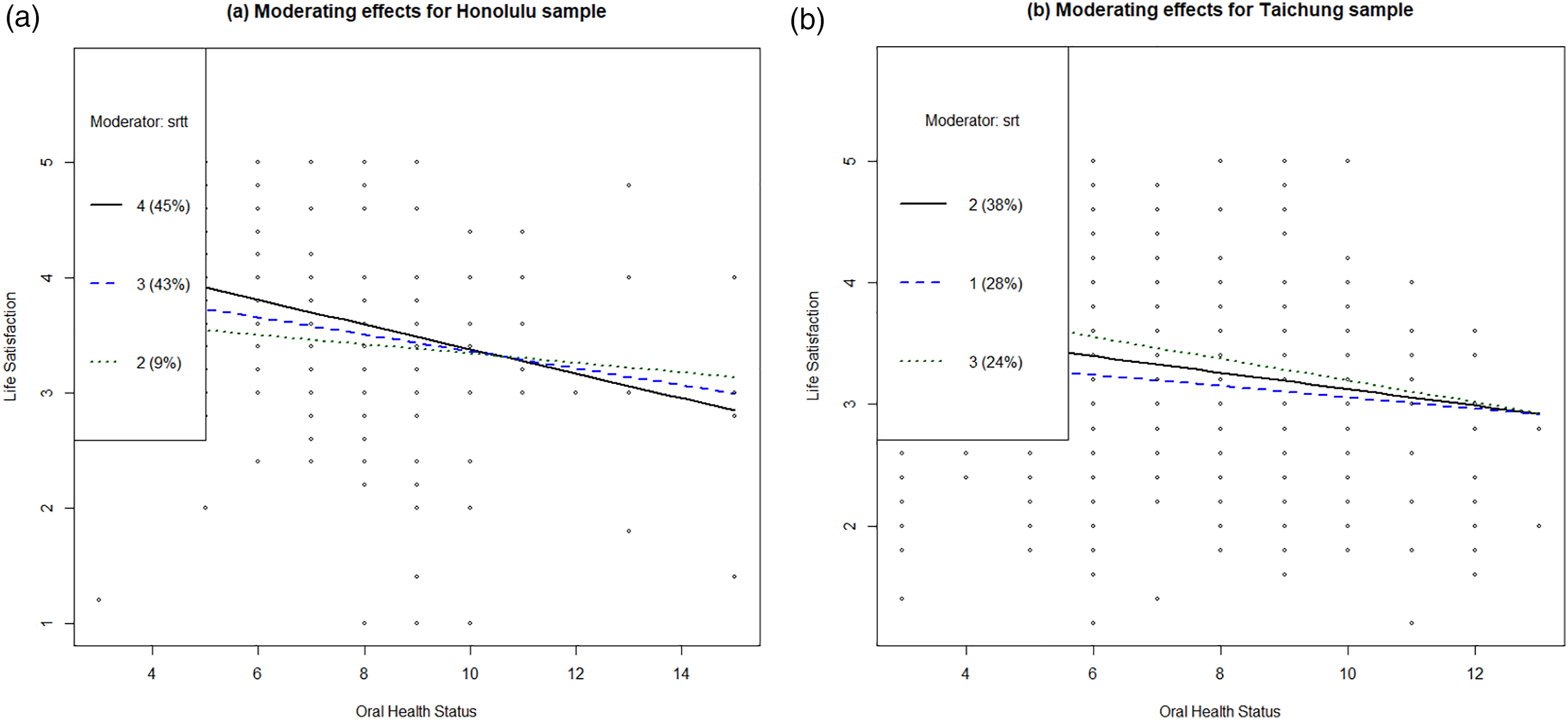
Discussion
This study examined the association between oral health status and individual subjective well-being, and explored the moderating role of self-rated oral health under two cultural backgrounds. Results showed that, for older adults in both Honolulu and Taichung, oral health status was negatively associated with subjective well-being, and this echoed previous studies on how oral health problems were negatively related to individual health (Baiju et al., 2017; Benjamin, 2010). Studies have revealed that oral health included the health of many anatomical structures such as the gums, bones muscles and nerves, and that oral health could affect some of the basic human functions, thereby shaping an individual’s self-image and sense of well-being (Evans, 2009). Originally, the two groups of older adults varied in levels of subjective well-being: Older adults in Taichung reported lower levels of life satisfaction, and they were more susceptible to the influences of oral health status (inferred from the size of coefficients in Models 1 and 4). We speculate at least several reasons that might account for the disparities reported by our Taichung sample: First, medical resources were insufficient for the current Taiwanese older adults during their childhood and youth compared with the younger cohorts in Taiwan. Second, due to insufficient oral health literacy (Ho et al., 2019; Hsu et al., 2013), most of the older adults in Taiwan often reported poor oral hygiene perceptions and behaviors (Hsu et al., 2013; Lin et al., 2016; Wang et al., 2013). As a result, they tended to suffer from serious oral health problems and had poor self-rated oral health. Also, severe oral health problems requiring extensive treatments might have brought them a financial burden as the general insurance does not fully cover those treatments.
Following that, this study also revealed that individual self-rated oral health itself was positively associated with life satisfaction. This finding confirmed the unique role of self-rated oral health in affecting older adult’s well-being and life satisfaction (Benyamini et al., 2004; Locker et al., 2000). It was found that higher levels of self-rated oral health had an independent and positive effect on concurrent and future well-being of older adults while controlling for other measures of health status (Lee et al., 2007, Ng et al., 2011). However, this study also found that, despite two samples shared similar levels of oral health status, they had different evaluations of self-rated oral health with older adults in Taichung rating their overall oral health much lower than their Honolulu counterparts (2.16/5 vs. 3.43/5). Apart from the possible middle mediation and humility cultural differences discussed previously (Xu et al., 2019), we put forward the following speculations: First, self-rated oral health is associated with health-seeking behaviors. Individuals who do not visit dentists or use preventative dental care regularly would be more likely to report poor oral health, while access to oral health care indicates higher socio-economic status and higher levels of oral health (Wamala et al., 2006). Although not shown in Table 1, only 13.5% of older adults in Honolulu reported having no access to oral health care facilities, and 13.1% reported not getting dental care when needed, indicating that more than 85% of the respondents had access to dentists and oral hygienists. This could explain their confidence in rating their overall oral health status. While in Taiwan, most Taiwanese adults practice dental self-care but are less likely to have regular dental visits. According to a nationally representative survey, only 15.6% of adults reported dental check-up every 6 months (Wang et al., 2013) even though general insurance did provide easy access to dentists for the regular checkups since 1994. Thus, further educational efforts are needed to improve the preventive dental care among older adults and the general public in Taiwan (Hsu et al., 2013). Additionally, the Taiwanese dental care system mainly focused on the treatment and ignored the importance of dental hygiene education (Cheng et al., 2007). Second, since self-rated oral health was also related to general health and daily functioning among older adults (Brennan & Singh, 2011; Locker et al., 2005), older adults with more existing health problems and functional limitations would be more likely to rate their oral health poorly and suffer more impacts from oral health problems. This fit the results of this study as well: Older adults in Taichung reported lower scores on self-rated health (3.36/5 vs. 3.75/5), and on average they had more chronic conditions (1.16 vs. 1.07) than the Honolulu sample. Lastly, we conjecture that the difference could also be explained by some other lifestyle-related factors. For instance, both drinking and smoking were found to be strong predictors of worse individual oral health (Jansson, 2008; Millar & Locker, 2007), and there were higher percentages of alcohol drinkers and smokers in our Taichung sample than in our Honolulu sample. Awareness of such health behaviors could also possibly contribute to lower levels of self-rated oral health among the older adults in Taichung.
Despite different levels of self-rated oral health between two groups, substantial moderating effects of self-rated oral health were found: It significantly buffered the detrimental effects of worse oral health status on subjective well-being for both samples. Our findings confirmed the role of self-rated oral health as a powerful resource in coping with oral health problems: For individuals with same or similar oral health status, higher levels self-rated oral health could moderate and reduce the detrimental effects of oral health status on life satisfaction, while at the same time impacting life satisfaction directly. This finding echoed the previous study on how individual view of health could act as a moderator between physical and mental health (Jahn & Cukrowicz, 2012), and even expanded based on that: Instead of the general view of health, we found that specifically self-rated oral health might be influential in promoting individual well-being. These results could significantly impact clinicians’ assessment and treatment of older adults with lower levels of well-being and highlighted the importance of self-assessment in integrated health interventions (Jang et al., 2021).
Our results also indicate that both direct and moderating effects of self-rated oral health were stronger and more effective for older adults in Honolulu. Different resources utilized by older adults under two cultural contexts might help us make sense of these findings. For instance, older adults in Honolulu may be more socially and financially independent, therefore might rely more heavily on internal and individual factors such as self-rated oral health to cope with the detrimental effects of oral health problems (Zhang et al., 2020). On the other hand, older adults in Taichung may be more likely to look outward for support and therefore rely more on social and family resources to cope with oral health status, as indicated by the interdependent and collectivism-oriented Asian culture. Financially, treating severe oral diseases and dental caries, which require dentures or implants, tend to be expensive and often have to rely on support from family members. Besides, due to limited oral health literacy, older adults in Taiwan often lack a sense of self-control over their oral condition and find it hard to evaluate its effects.
Due to the constraints of sampling strategies and data, this study has its limitations. The cross-sectional nature of our data prevents us from making causal inferences with regards to the focal relationships. Also, the brief and self-report measures contain the possibility of underreporting or overreporting, therefore could potentially bias our results. Moreover, some important variables such as the availability as well as types of insurances, especially dental insurance of older adults were missing in the datasets, which limit us from comparing and contrasting the focal relationships more accurately. Lastly, the use of OLS regression, compared with other analysis, might prevent us from making more inferences on the invariance computations and group contrast.
Despite these limitations, this study was one of the first that focused on the relationship between oral health status and subjective well-being, life satisfaction in particular, as well as the moderating role of self-rated oral health under two cultural backgrounds. Our findings suggest that the intervening mechanism of subjective oral heath perceptions was present regardless of place of residence and cultural backgrounds. These findings identified certain important factors that may provide implications for policy makers and aging researchers to develop programs and recommendations and intervention strategies to address the oral health disparities among older adults. Maintenance or enhancement of positive perceptions and optimistic attitudes toward oral health might serve as an important pathway to optimize health outcomes among older adults. Especially for older adults in Taiwan, increasing both oral health awareness and access to preventive dental care will be essential to promote their positive perception of oral health.
Footnotes
Appendix I. Comparison of Focal Scales
Appendix II. Variable Missingness
Honolulu (N = 430)
Taichung (N = 645)
Categorical
N (%)
Gender: Male
0 (0)
0 (0)
Married/partnered
0 (0)
0 (0)
Education: ≥High school
0 (0)
0 (0)
Income
11 (2.6)
0 (0)
Smoking
10 (2.3)
0 (0)
Drinking
19 (4.4)
0 (0)
Physical exercise
10 (2.3)
0 (0)
Continuous
Age
0 (0)
0 (0)
Self-rated health
0 (0)
0 (0)
Chronic conditions
5 (1.2)
0 (0)
Oral health condition
0 (0)
0 (0)
Self-rated oral health
0 (0)
0 (0)
Life satisfaction
0 (0)
0 (0)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Honolulu project was funded by a seed grant from Rory Meyers’ College of Nursing at New York University. Taichung project was supported by the Ministry of Science and Technology, Taiwan.