
Abstract
Introduction
Diabetes mellitus is a chronic metabolic disease associated with impaired quality of life, premature mortality, and significant economic costs (Davis et al., 2022; Erdem & Korda, 2014; Wu et al., 2019). Its prevalence has been increasing steadily over the years and is expected to continue to grow, with an estimated 422 million adults with diabetes worldwide in 2014 and approximately 1.5 million deaths per year caused directly by diabetes worldwide (WHO, 2021). Nearly 14% of the population in Canada live with type 1 or type 2 diabetes (Diabetes Canada, 2022a). In Ontario, 15% of the population (2,346,000 individuals) lives with type 1 or type 2 diabetes, and this is expected to increase to 17% (2,953,000 individuals) by 2032 (Diabetes Canada, 2019). Ontario has more people living with diabetes than anywhere else in Canada (Diabetes Canada, 2022b). While diabetes affects all age groups, one in five older adults (≥65 years of age) are diagnosed with diabetes every year compared to one in 10 for younger people (Diabetes Canada, 2019). Older adults living with diabetes experience additional challenges, such as mobility issues, comorbidities and polypharmacy, changing socioeconomic status, increased likelihood of lonelinesss and lack of social support (Diabetes Canada, 2019).
The care provided to someone with diabetes must be comprehensive, addressing the effects of this chronic condition on all aspects of their life (Erdem & Korda, 2014; Pitchalard et al., 2022; Sherifali et al., 2015; Wallace et al., 2019). Health-care providers are a source of health information and coping skills that help individuals with diabetes to understand their condition, change their lifestyle and deal with negative emotions and symptoms (Sherifali et al., 2015). Therefore, strategies to enhance confidence or self-efficacy are essential in supporting individuals to implement changes to improve their well-being, health and quality of life.
Diabetes is a demanding condition with a wide range of physical and psychosocial consequences (Knox et al., 2015; Simmons et al., 2013). Self-management is the ability to manage symptoms, lifestyle changes, treatments, and psychosocial, cultural, and spiritual effects of chronic diseases with the support of family, health providers and community members (Simmons et al., 2013; Wallace et al., 2019). Self-management is an essential skill that becomes more important as age increases (Beck et al., 2017; Byrne et al., 2022). Effective self-management for older adults entails learning about self-care behaviours, including adherence to treatment, monitoring symptoms and modifying behaviours to maintain their well-being and independence for as long as possible (Akhter et al., 2017; Wallace et al., 2019).
To improve the health, well-being, and quality of life of people with diabetes, diabetes self-management education (DSME) and support interventions have been developed in Canada (Meneilly et al., 2018; Sherifali et al., 2018). Diabetes self-management education is an ongoing educational process that facilitates the knowledge, skills, and abilities an individual needs to complete diabetes self-care (Akhter et al., 2017; Sanchez, 2011). Diabetes self-management education is about delivering information and skills, motivating individuals and facilitating behavioural change (Akhter et al., 2017). The rationale is that increasing knowledge, skills, and confidence in managing diabetes will lead to improvement in health-related behaviours and health outcomes. Diabetes self-management education is regarded as an essential element in the model of diabetes management adopted by the Canadian Diabetes Guidelines (Sherifali et al., 2018).
Through DSME, individuals with diabetes learn to manage their condition to avoid complications (Akhter et al., 2017; Sanchez, 2011). Multiple modalities of DSME are offered to people living with diabetes (e.g., didactic, empowerment-based), in a variety of formats (e.g., individual vs. group sessions, in-person vs. virtual), led by a variety of professionals or peers (e.g., nurse educators, community workers, pharmacists), and with varying timelines (e.g., upon diagnosis) (Beck et al., 2017). Older adults with diabetes learn self-management skills through education and support programs (Beck et al., 2017). This is critical step toward achieving optimal glycemic control, minimizing comorbidities and mortality, and improving quality of life (Davis et al., 2022; Wu et al., 2019).
There is an extensive body of literature strongly supporting the use of DSME (Akhter et al., 2017; Knox et al., 2015; Simmons et al., 2013) to improve diabetes self-care for older adults in rural areas (Akhter et al., 2017) to reduce diabetes and associated costs (Li et al., 2020), mitigate future complications and improve overall health. However, older adults are underrepresented in DSME research (Miklavcic et al., 2020; Petrovsky et al., 2022). The exclusion of older adults from research is highly problematic, as they experience the greatest burden of chronic illness. Furthermore, a primary focus on the DSME experiences of older adults is negligible in the literature (Levy, 2022; Weinger et al., 2014). The purpose of this study was to explore the DSME experiences of older adults in a rural Ontario setting. The findings from the study will provide a framework for the design of self-management education material and delivery methods for older adults living in a rural setting.
Methods
Study design
This qualitative study used a combination of participatory, art-based and hermeneutic phenomenological approaches to understand DSME for older adults. Using a participatory approach, we engaged with community members, health-care providers and decision-makers as members of our Advisory Committee (AC), to formulate the best research process to investigate DSME for older adults in a rural community in Ontario. Participatory research is a dynamic process rather than a set of specific methods and places importance on the knowledge and views of the community (Kidd et al., 2018). The art-based research method was a creative way to help older adults communicate their feelings, thoughts, and reflections on their experiences. Art-based research adds value when addressing research questions that cannot be answered with traditional research methods (Fraser & al Sayah, 2011). Hermeneutic phenomenology, which is a human science that attempts to unravel the meaning of individual experiences, guided the thematic analysis of the data (van Manen, 2016).
Setting and participants
Participant Demographic Information.
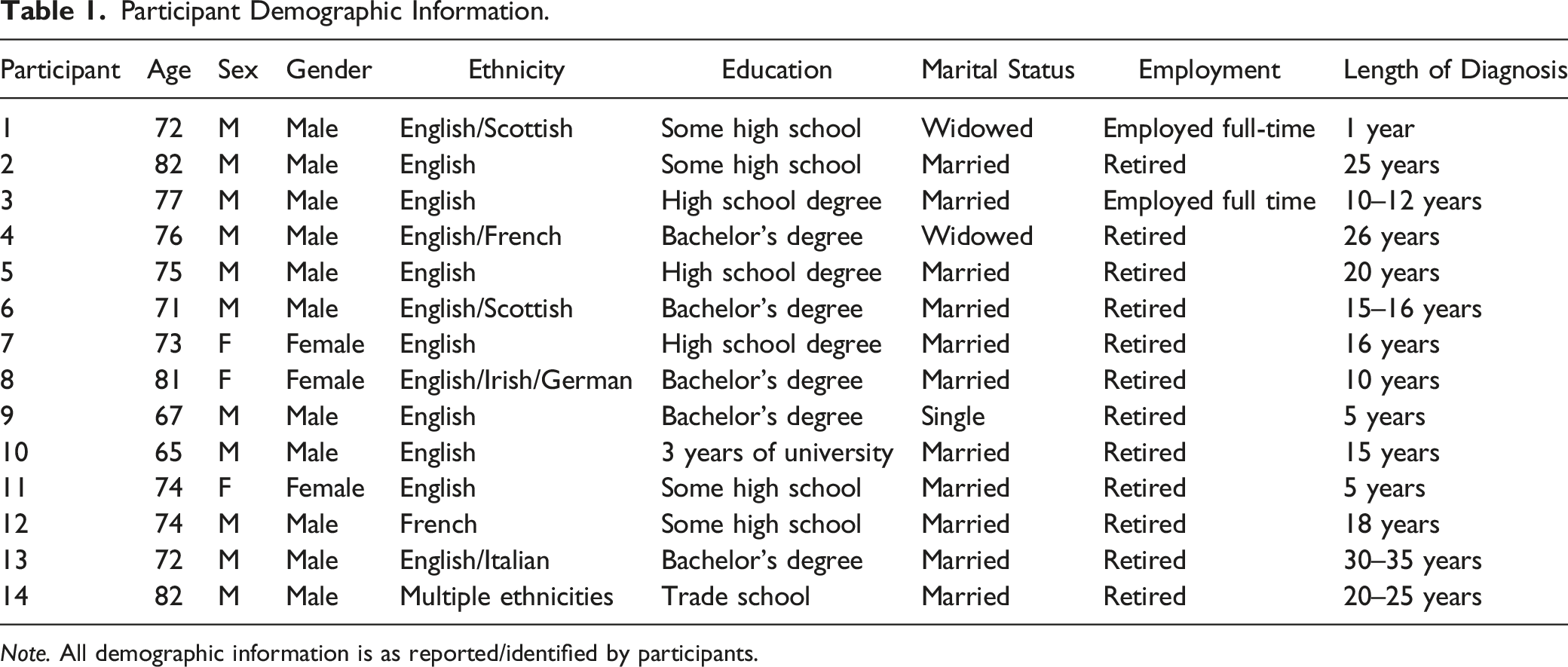
Note. All demographic information is as reported/identified by participants.
Recruitment strategy
The health-care providers and members of our AC identified potential participants from their practice. They presented the invitation letter to potential participants, with the research team subsequently contacting individuals who expressed an interest in the study. During a phone conversation with a team member, interested older adults received detailed study information and were asked to provide verbal informed consent. Following this, consenting participants were mailed iPads® to use as cameras. Participants received mailed step-by-step printed instructions about the photo-assignment, and a follow-up email or phone call from a member of the research team to answer any questions. Participants were asked to return the iPads© within 2–3 weeks, however extra time was given if the participants needed. Study material, including consent forms, a guide to photovoice, an iPad© to take photos and watch a welcome video, instructions on the use of the iPad©, as well as contact information for a local technical support resource, was mailed directly to participants with a return envelope. Upon receipt of the iPad© and digital photos, a team member printed and sent back the photos to the participants. All follow-up communications and interviews were completed over the phone.
Data collection
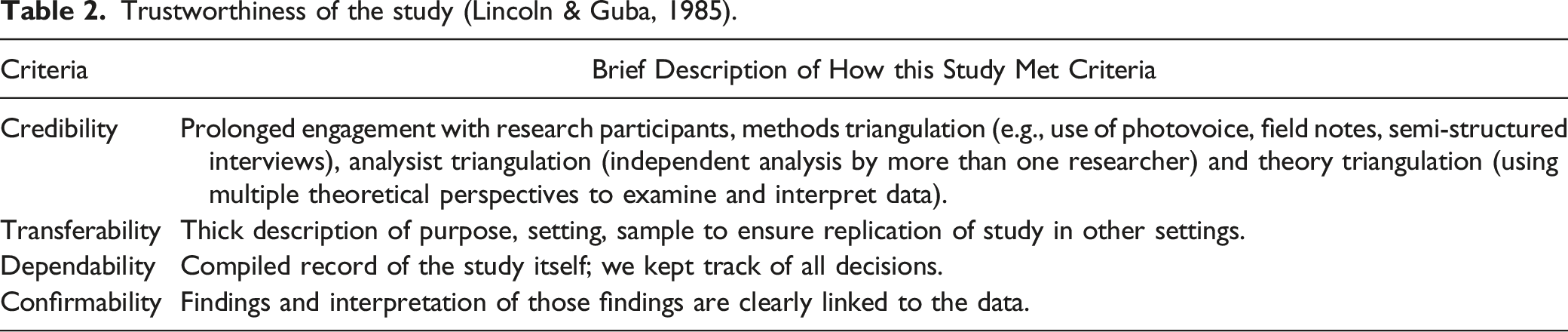
Trustworthiness of the study (Lincoln & Guba, 1985).
Data analysis
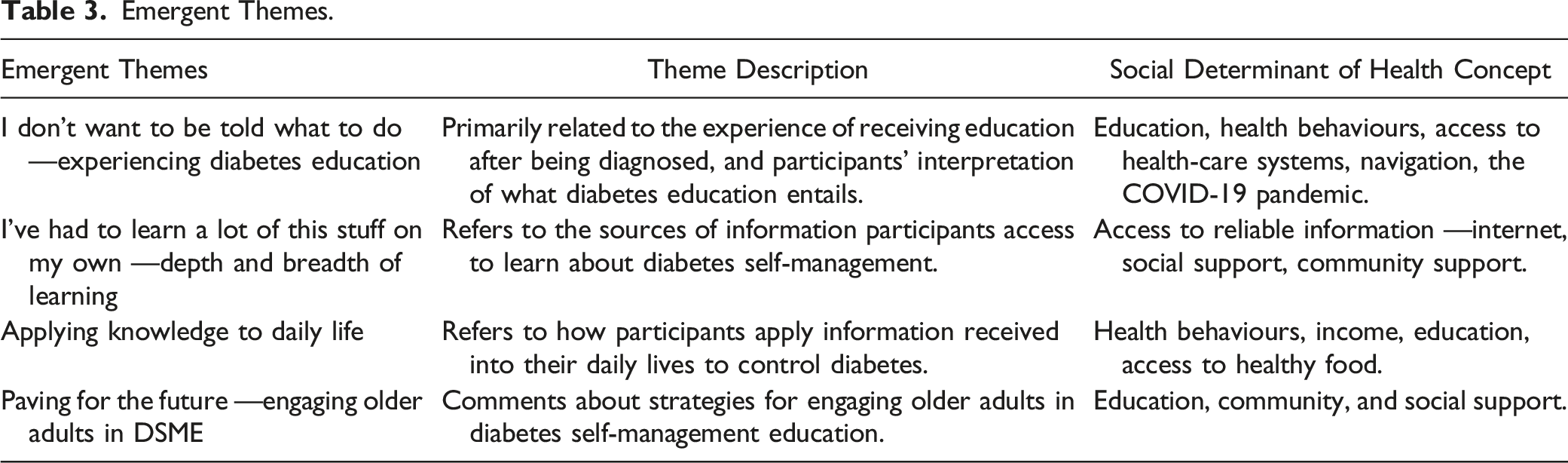
Emergent Themes.
Results
Four themes were identified in our data analysis process: (1) I don’t want to be told what to do — Learning about diabetes education; (2) I’ve had to learn a lot of this stuff on my own —Depth and breadth of learning; (3) It didn’t really get under control till I accepted it — Applying knowledge to daily life; and (4); Paving for the future — Engaging older adults in DSME.
I Don’t Like to be Told What to Do — Learning about Diabetes Education
Participants commonly engaged in diabetes education sessions when they were first diagnosed. In those sessions, they learned about diabetes and its management, including blood glucose monitoring, nutrition, exercise and physical activity, and medication management. As Mike described: [Diabetes] can really affect my life, my longevity, and all of those things. But at the same time, that is manageable. I guess that’s always the thing that I’ve thought about it, you know, I mean, people every day get diagnoses of different things much more serious than others. So, if I had to be diagnosed with something, I think diabetes was something I knew I was taught from the beginning. And I’ve learned to understand that it’s very manageable.
Harold remembered how some of this initial education was in the hospital and lacked detailed information about his condition: Uh, I think looking back, I could have stood a little more education rather than just the: “Hey, you’re diabetic man, make the best out of it…If someone could have told me what it, well I understand that it’s, well Christ I forgotten the body part now that produces the insulin and all that stuff, but what is it in me that suddenly at 50–52 that changed that suddenly it wasn’t controlling the sugar?
Harold described how health-care providers came to his room and gave him some pamphlets on what to eat and what not to eat to control his diabetes, but he did not have much time to ask questions about the information presented or even where to find healthy food in his rural community. As he recalled: Then a series of people came and saw me while I was in the hospital. And one of those was a dietitian she did give me a whole bunch of papers what to eat to maximize my control of diabetes and what not to eat. That I got to admit I did come on when I did read it you know stay away from ice cream or just do this and [buy] this kind of stuff but you know unless you go into a specialty store, you’re not going to find it in a grocery in [rural place].
Unlike Harold, Jane described receiving too much information about the best things to eat, portions, and schedules for eating, and little about other important topics such as food substitutes: “it’d be interesting for a dietitian or diabetes educator to say, you know if you love pasta, here’s an alternative. If you love this, here’s an alternative, you know.” The education participants received when diagnosed with diabetes was primarily focused on diet including what food to eat, what substitutions to use and food proportions.
In the participants’ narratives, their understanding of what diabetes education is varied. Their experiences usually offered a glimpse of the definition learned during their first engagement in diabetes education sessions. Joel explained what diabetes education is: “Knowing what causes diabetes, what to do to prevent it, and you know, how to notice the signs that you need to, and what you need to do if you happen to notice you have a sign and symptom”
Like Joel, Harold explained: [Diabetes education]’s being able to, you know, having your questions answered. It’s even having understanding the questions you want to ask, I think is part of the challenge. You know, I my background is engineering. And as a result, I tend to be quite inquisitive about how things work including, you know, human physiology.
Similar to Harold and Joel, Alex defined diabetes education as, “Making people aware about diabetes, what it can do. Well, make sure they, they know the proper foods that they have to eat and the exercise. Yep, they’re doing stuff like that.” Reaching out to everyone in a group and knowing their needs is essential in the learning process, and particularly crucial when providing education about diabetes for older adults. For these participants, DSME should be about diabetes awareness and knowledge. As Jane explained: When I was first diagnosed, I had a couple of appointments with a diabetic nurse at the [name of hospital]. And it was, they were group sessions, it was like a clinic. And we went there. I think it was a two-hour session that I had to go to once a week for a month. And so, I got a lot of good information from that about, you know, about diabetes, and diet and exercise.
For Jane, diabetes education was a beneficial and valuable process. However, Jane noted some people who attended the session did not seem like they wanted to be there, which may have affected their ability to learn about diabetes. For some individuals, diabetes education was not necessary as they learned about diabetes in their work as frontline providers. Joel stated, “I don’t need to read about it, okay, because I was a volunteer fireman. I was first responder trained. So, I knew all the signs and symptoms of all these diseases.” Similarly, Oscar said, “Pretty much learned to do it myself. I’ve been very remiss of not taking a lot of dietary diabetic education. I don’t like to be told what to do.” Even though education is available in their community, and they recognized the program is accessible to people in rural areas, they felt they did not need diabetes education. This particular experience was also connected to the belief diabetes did not have a large effect on them or their everyday life.
Some participants felt the diabetes education was controlling, “I kind of got turned off by the whole thing because it showed me how much spaghetti is on a plate that you should eat. And I can put that on one fork, you know, so that was probably one of the things that turned me off. Too controlling initially” (Oscar). For Oscar, education about diabetes needs to be about guiding older adults or raising consciousness to avoid complications, instead of controlling them.
I’ve Had to Learn a Lot of this Stuff on My Own — Depth and Breadth of Learning
In the participants’ conversations, it became evident there are many ways to obtain knowledge about diabetes. Regardless of the diabetes education participants received at diagnosis, there were no major gaps in perceived knowledge about diabetes. Participants’ understanding of diabetes was primarily based on their independent research about the topic, as well as the experiences of family members and friends living with diabetes. Participants also described how taking care of their conditions is necessary to avoid medical complications. Importantly, they also discussed a need and wish for more individualized and specific diabetes education in the early stages of their diagnosis; this stemmed from a perceived lack of explanation about the physiological process of Type 2 diabetes.
Participants emphasized independent research as one of the primary sources to obtain information about diabetes. Wilson said: “You know, and then reading and stuff to just to try…following what works for me.” The internet is one option participants used to access information and answer questions related to diabetes. A similar experience was shared by Jane: “in retrospect, when I look back, I had to educate myself by googling and going online and doing research, really understanding what diabetes is and, and the effects that it can have on your body.” Patrick remembered how the physician who diagnosed him said, “here’s a bunch of pamphlets, here you go.” Patrick did a fair amount of research on the internet to learn more about his condition. By accessing the Internet when it was available, some participants were able to engage in independent research to learn about diabetes. Likewise, Oscar self-managed his diabetes by independently looking for information: “Like, I am not ashamed of having diabetes, I admitted to whoever wants to know, but I’ve never asked for advice or anything like that. I’ll try to make it my own thing.” He continued: “I can go online, they just had a virtual, like more of a psychological or mental approach to what you eat, and how much you eat and all this. So there’s all kinds of programs they have.”
Applying information gained from independent research assisted them in recognizing the effect of diabetes on their bodies and their overall health. This additional knowledge allowed them to accommodate their diabetes self-management to meet their personal preferences and needs. For other participants, books and booklets were the primary sources of information used to learn about the disease and answer their questions. Rose noted, “I bought cookbooks so that I could make meals that were diabetic-friendly. And so really, it was easy for me”. For Rose, the first source of information is her books; if she does not find the information needed, she goes online and searches for information.
Other sources of information for older adults living with diabetes were family members and friends whom they considered experts. Often, these experts were individuals who participants identified as being obsessive about their diabetes, and who had a plethora of knowledge pertaining to diabetes self-management. John explained, “I’m lucky I have a friend who’s a retired nurse who’s done ER and all sorts of other stuff. And she’s also a Type 2…So I learned a lot more about diabetes from her and cheating, you know, from the clinic, but that was fine.” Similarly, Rose said, “I’ve been following along with what Kevin does, ever since he started having diabetes. So, when I was diagnosed, it was really no different than what I was doing before.” Information about diabetes is informally circulated, even if participants attend diabetes education in their community. Those observations assist them in self-managing their condition, as they see how family members or friends face health complications when they do not make the right decisions and learn how to deal with their condition to avoid further complications.
When some participants had questions about their diabetes, health-care providers were identified as the last people they would approach for answers to their questions. Although participants recognized the diabetes nurse educator and diabetes educator as excellent expert sources of information, many participants did independent research instead. Jane said, “So that’s another thing in, probably in, diabetes education, I’ve had to learn a lot of this stuff on my own. Even though the surgeon or the dietitian would give me what, you know, best things to eat and portions and times and everything.” Some participants immediately incorporated the information they received from health-care providers into their daily routine, as Wilson explained: “Well a combination of both but mostly we did, I did go to a session with the dietitian when I was diagnosed, and I’ve tried to follow that advice all along”. Harold’s experience was similar to those of Wilson and Jane: “The dietician here in [place] will remind me of some of the things… make some suggestions and actually she had started a couple of years ago, some cooking monthly sessions in the kitchen with diabetics.” Rose asked for information in the health center when her other sources of information failed: “If I couldn’t get any answers there [books and internet], then I’d probably call the medical center to talk to the dietician or the doctor.” Harold also described how, “The pharmacy in [place] I use, if I’ve got questions, I usually ask the pharmacist and they’ll tell me straight, you know, what’s good for me, what’s bad for me or you know, you shouldn’t try that uh.” Like Harold, Wilson praised the work of the pharmacist in the community: “The pharmacist showed me how to use it. [blood sugar meter].”
It Didn’t Really Get Under Control Till I Accepted It — Applying Knowledge to Daily Life
A common theme mentioned by participants was the implementation of diabetes education into their daily lives. Some participants were motivated to implement the information they received in their daily lives. Learning to adjust to diabetes in their daily lives emerged as an ongoing process. With changes in life situations (e.g., retirement), and changes in illness (e.g., the pandemic), participants react to and accommodate new experiences. Their ultimate goal is to control their diabetes and avoid complications. Participants described difficulty accepting what diabetes brings to them when they received their diagnosis. As Oscar stated: I was kind of taken aback when I first found out because I never really had any illnesses to deal with. So it was surprising to, to then be diagnosed it took me a while to accept that, like, you know, you got to do this and you got to do that. And I said I don’t want medication, control it, but it didn’t really get under control till I accepted it and started taking the medication and doing the exercise and watching what what I eat and how much I eat, etc.
Something surprising in the participants’ stories was fear of having to take medications when they were first diagnosed with diabetes. The fear was less focused on the symptoms or medical issues that come with diabetes, but instead on having to take medication they do not want to take. This then drove the participant to make changes to their diet right away and stick to it over time. As Jane explained: “I just find having to take a lot of medications is one of the one of the difficult things for me too. I just don’t like taking them and I just, I just, you know, the side effects and drugs and everything.”
It was worse when they were put on insulin, as Kevin explained, “this is, the one thing that I never wanted to have insulin. I almost refused to have it.” Another common discussion point was “guilt”. The participant went back and forth between saying they sometimes feel guilty about not applying their knowledge to their daily lives. Some participants felt guilty when they did not do what they were supposed to, such as test their blood sugar levels every day. For example, Wilson said, “feeling guilty that I don’t do as much as I should. Probably, [I] can’t do everything.” It seemed as though the guilt was about specific tasks or not following diet recommendations, as Mike recalled, “there’s an adapted diabetic Food Guide. So I have all of those things I don’t, I don’t spend a lot of time poring over them, I kind of try to look at what I eat, and maybe look at either the carb content and try to balance things that way.” For other participants, their knowledge about diet was incorporated into their daily lives. As Rose said, “I try to not use as much fats and have a balanced diet”. Similarly, Jonathan explained: I love to eat fresh fruits, and I have to cut back on them first, because of the sugar levels in them and whatnot. My wife is a very good cook and baker and she doesn’t make nearly as much as she used to take those things away from me. Portion sizes for meals are down. Where there used to be a little bit more cooked so that if I wanted seconds, I could have it. There’s not that much anymore.
The Biggest Challenge is Living Rural – DSME in Rural Communities
Participants found that rural living was a barrier to successful diabetes management and education. Travel was a major concern for these participants when accessing physical activity programs, groceries, medical care or diabetes education. As John said, “and I live in a situation where I have to drive 18 to 20 km, just to buy groceries.” Similarly, Wilson explained: “Being in a rural area, of course, I’m a little more limited, but actually that hasn’t been a big limitation.” Many participants live “off the grid” where they face additional challenges to DSME and diabetes self-management, just like Patrick: “So to me, the two are all the challenges of being off the grid and being the challenges of being a diabetic are almost intertwined. So, it’s really hard to sort of separate the two”
Living in a rural area resulted in participants having less opportunities for DSME programs. Wilson explained: “So I think because we’re a small community, and we’re more isolated, it means that they’re more limited in terms of what of what they can offer compared to a larger center, but I think they do their best.” Specifically, travel was the primary concern for participants to access DSME, as Joel expressed, “it’s 45 minutes to an hour to the nearest place where there’s any education”.
Many participants also found diabetes self-management equally difficult to navigate when living in a rural area. Rural living created barriers to access pharmacies, healthy food, and physical activity. Patrick said: “Yeah, I mean, the biggest challenge is more in the winter is exercise. Now, once again, we live in a slightly unusual living situation compared to, I would say, a majority of the members of the study in just the world in general. Because we're in an off the grid situation… So what we find in the winters because we are so incredibly rural, and because I'm living literally in the middle of the woods, in the wintertime, when the snow flies, you know, the nut on the ground here is flat, there is no pavement anywhere.”
Similar to Patrick, John found grocery shopping for diabetic-safe food more difficult. They further stated that “And, you know, clearly the grocer does their very best to, as an example, stock fresh vegetables, but supply, if I want to go to do a what I would consider, quote, a real shop, which we tend to do every couple of weeks or not much more than that, because it’s about by the time all is said and done, it’s a little over 100 km to get from my place to the [name of store] in the outskirts of [city]”
Paving the Way — Engaging Older Adults in DSME
The study participants also shared their suggestions about strategies for organizing a DSME program for older adults in their community. For them, a successful diabetes education program should be organized outside of the health-care setting, in a different space in their community, where refreshments and treats are available during the sessions: “They could hold every couple of months, or once a year, come in and get all the elderly, they all go to the hall, and sit there and have coffee and that in the morning. Go to the coffee club and tell them about it. You know, we have halls all over. You just come in the morning, and you sign up a bunch of older people, and they will listen to you. Give them free coffee and doughnuts; they will come” (Joel).
According to the participants, DSME programs should be fun, active, and versatile. This was exemplified by Oscar’s statement: “I think there are a lot of fun activities. Especially for seniors, especially through the senior associations and in places like that. We can stay active and have fun.” Participants aspired to see fun educational activities about diabetes, which make them active and provide non-traditional exercise methods. Some participants also highlighted the importance of different learning styles; this is an important consideration when developing a DSME program. Oscar commented: “Now, you know, I did a lot of coaching with my kids. And then later on at the AAA level in hockey. And then I learned early on that people learn in different ways…. Some are tactile; some are visual; some are auditory. So even when you’re teaching these things, I think, you know, you have to be able to hear it, see it, and do it. So, you reach everybody in the group”.
The participants discussed the need for a facilitator who provides an environment in which participants engage in learning about DSME, but also suggested this should not occur for long periods of time. They requested someone with the ability to provide general information and who could adapt content to meet individual needs. Wilson reflected, “A lot of [older adults] are not all that interested in sitting around listening to a lecture speaker for a long time…I don’t feel like my dietary needs would be the same as a lot of other people’s would be, and I know it wouldn’t be, and so, you know, it’s got to be individualized first.”
The participants wanted not only someone with a wealth of knowledge who would assist them in implementing the information into their daily lives and routines, but also someone who was a good communicator and could “put them on the right track” (Harold). Alternatively, some participants suggested learning from another older person or a peer with training and knowledge about diabetes as a strategy for a successful DSME program for older adults. The reason for this was the title of ‘doctor’ or ‘nurse’ may intimidate some, as exemplified by Jonathan’s statement: “Some people are intimidated because of the title doctor or nurse or whatever. They might feel better with their peers.”
Discussion
In this study, we reported the unique DSME experiences of older adults in a rural area of Ontario. Asking older adults to describe their daily experiences of living with diabetes, including experiences in their personal environment and their community, was invaluable to understand how individuals, society and the community influenced their experiences of DSME. Increasing rates of diabetes and its complications among older Canadians highlight the need for studies of DSME needs within this group to inform the development of meaningful interventions. Consistent with the literature, participants described how diabetes management is affected by the availability of, and access to, information (Byrne et al., 2022; Li et al., 2020; Pitchalard et al., 2022; Rachmawati et al., 2019). As an example, participants mentioned how their education was limited to receiving pamphlets on what to eat and how to avoid diabetes complications after diagnosis. Participants said there was either no time to ask questions, or they received too much information about diabetes and not enough about other relevant topics, such as food substitutes and proportions. Participants have a wealth of knowledge and life experiences, but may be overwhelmed by the burden of daily care associated with a new diagnosis of diabetes. Our results support the work by Pitchalard et al. (2022) and Wallace et al. (2019), who found a good level of diabetes self-management is only reached when the necessary information is easy to access and it meets older persons’ needs, including education and cultural values.
Reaching out to everyone in a group and knowing their needs is essential and particularly crucial when providing DSME for older adults. Although some participants recognized the importance of DSME and its availability in their community, they felt they did not need it. For these participants, diabetes does not have a large effect on their everyday lives.
Diabetes self-management education is essential for older adults with diabetes, with the associated benefits including favourable clinical, behavioural and psychosocial outcomes (Knox et al., 2015; Olesen et al., 2020; Simmons et al., 2013). In the Canadian diabetes guidelines, the need for knowledge and skills, problem-solving strategies, peer support and coaching strategies is highlighted (Ivers et al., 2019). In rural settings in Canada, DSME is provided as either an individual session or a group session, in which different healthcare professionals (i.e., diabetes nurse and dietitian) provide information about diabetes self-management (e.g., diet and management of medications). Many of these sessions are based on a pre-determined set of topics (e.g., foot care, nutrition). However, it is suggested adjustments in DSME should be made to prioritize client concerns, making education more accessible and tailored to clients’ needs. The advantages and disadvantages of an individual versus group approach to diabetes education have been investigated in the past, with group meetings often preferred as they provide social support and sharing of experiences between peers, whereas the individual approach allows older adults’ needs and preferences to be better met (Sims Gould et al., 2019). A patient-centered educational approach has been suggested to improve medication adherence, decrease complications and improve health behaviours for individuals with chronic illness (Siddharthan et al., 2016). The participants in this study live in a rural area; they are challenged by limited access to the primary health setting and unreliable communications. Our findings highlight the need for a DSME program that addresses individual concerns and preferences, making education more accessible and tailored to individual needs.
Our participants recognized the importance of gaining knowledge about their condition and following diet and physical activity recommendations. Interestingly, the primary sources of knowledge about diabetes and its management included independent research (e.g., reading online, books, booklets, etc.), as well as learning from family and friends living with diabetes, diabetes nurse educators, diabetes educators and pharmacists in their community. Although the Internet connectivity is not reliable in their rural community, many widely used the Internet an acceptable source of information about diabetes and strategies for self-management. Our participants mentioned the need to improve their digital skills to ensure they can access high quality health information. Similar results were described by du Pon et al. (2020), Stellefson et al. (2013), and Scheffer et al. (2021), who highlighted the importance of investing in developing online skills for older adults to improve their eHealth literacy.
Family and friends were described as a second source of knowledge when participants had questions about their condition or self-management. These findings are consistent with the work of Wallace et al. (2019) and David et al. (2019), who suggested family dynamics have the potential to affect diabetes self-management behaviours in older adults. For our participants, health-care providers were considered a trusted source of health information; despite this, they were the least preferred source of diabetes self-management information. In contrast, Chaudhuri et al. (2013) and Sherifali et al., (2015) found participants ranked health-care providers as the most trusted source of health information. Patient-provider communication has also been important in managing and controlling diabetes in Canada (Ndjaboue et al., 2020). Several researchers have reported a positive rapport between health-care providers and older adults with diabetes leads to better foot care and prevention of diabetic foot ulcer (Ahmad Sharoni et al., 2016). Recent findings from expert patients in Canada (i.e., patient partners recruited via Diabetes Action Canada) emphasize the importance of professional knowledge and communication skills, such as up-to-date information, empathy and cultural competence, when caring for people with diabetes (Ndjaboue et al., 2020).
Our participants understood the importance of information for the management of diabetes and avoidance of complications; however, they found some of the provided information was generic and not structured to meet their needs. The participants suggested more interactive activities, which could be integrated with other activities in the community, as well as the provision of education involving peers. This could be considered for future implementation or adaptation of current DSME programs in Canada. Indeed, participants in other studies had a positive reaction to the possible opportunity for peer support and peer-lead interventions (Akhter et al., 2017; Sanchez, 2011; Simmons et al., 2013). Different community-based models have been developed for DSME that seem to work better for populations in vulnerable circumstances such as living in rural settings (Akhter et al., 2017), or populations suffering inequalities in care for diabetes (Nieblas-Bedolla et al., 2019; Wallace et al., 2019). For example, story-based techniques promoted feelings of empowerment, support and knowledge in older persons with diabetes in Toronto (Gucciardi et al., 2021).
Overall, our findings contribute to the evidence on the complexities of self-management and family support for older adults. For older persons in this rural setting, many elements regarding DSME echo similar elements as reported by other populations; this is an important finding to be illuminated. Uniquely however, the older persons in this study framed DSME as needing to be a fun, social-like activity, in an engaging setting apart from medicalized environments — perhaps as a way to ‘normalize’ a potentially stressful event; this too is equally informative for future program-building. Generally, it is crucial to design DSME that is inclusive of the unique and diverse health information needs and preferences of older adults, their friends and family members; this will help to ensure they remain engaged and knowledgeable about their condition and avoid complications.
Study Limitations
We acknowledge some limitations in this study. First, our goal in this study was to understand the experiences of and thoughts about DSME as described by older persons in their own words. This study approach will not satisfy those wanting generalizable findings based on large samples; importantly however, we believe the tendency to generalize may keep us away from the nuanced uniqueness of the lifeworld (van Manen, 2016). Second, this study was conducted in a rural setting, and the majority of the participants were white males of English descent. As such, different views and perspectives about DSME may be obtained from suburban and urban populations, or cohorts with a more diverse representation of sex, gender and ethnicity. Finally, although phone interviews remain an excellent method of data collection, they prevent the use of visual aids that could be of assistance while interviewing and preclude observation of the participant’s non-verbal communication and body language.
Conclusion
The purpose of this study was to understand the experiences of older adults accessing and engaging with DSME. Diagnosis of diabetes is a life-changing event that requires the development of self-management skills to control the disease and avoid complications. Our findings reaffirm the importance of DSME programs. However, the older adults in our study clearly expressed a preference to seek education from non-healthcare system sources (e.g., independent research, family members and friends); this finding should not be underestimated. By developing programming that builds health literacy for older adults and offering peer support programs, health-care professionals, in collaboration with decision-makers and older adults living with diabetes, can bolster engagement of older adults living with diabetes in rural settings, build and sustain patients’ knowledge of diabetes self-management, and improve clinical and quality of life outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Canadian Institutes of Health Research-Institute of Aging; File #410802 and Research Development Fund - School of Nursing, Queen’s University.