
Abstract
Objectives
To examine associations between physical activity (PA) and prospectively assessed memory in a cohort of cognitively healthy adults, after accounting for understudied social determinants.
Methods
We used data from the Canadian Longitudinal Study on Aging (CLSA). PA (exposure) and memory (outcome) were assessed using validated measures in 2013–2015 and 2015–2018, respectively. Respondents reported their daily number of hours spent engaging in five different PAs. We conducted multiple imputation and used linear regression (n = 41,394), adjusting for five categories of covariates: demographics, sensory health characteristics, health behaviors, health status, and social determinants (sex/gender, education, income, social support, perceived social standing, race, and sexual orientation).
Results
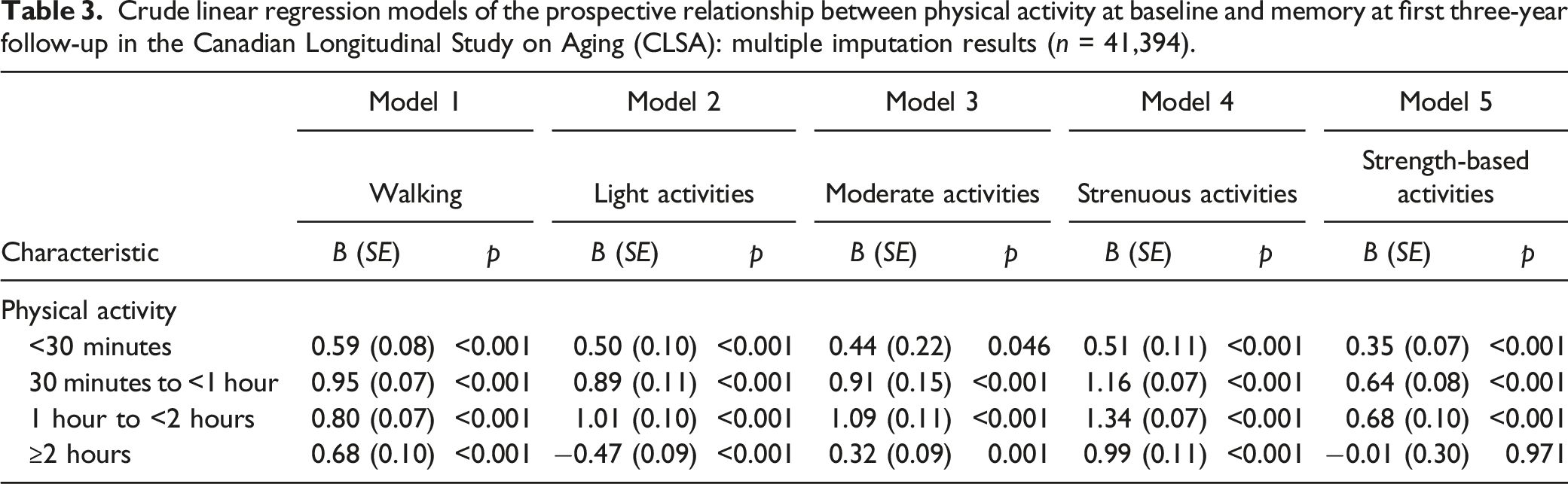
In crude models, nearly every intensity and duration of PA was associated with better memory. In fully adjusted models, protective associations were attenuated; however, some associations held: all durations of walking, most durations of light activities, moderate activities for ≥1 hour, and strenuous activities for 1 to <2 hours.
Discussion
Some forms of PA may be associated with better memory. The benefits of higher intensity PA may only be realized after social determinants are addressed.
Introduction
Identifying modifiable lifestyle activities which may reduce or slow memory decline among older adults is important to promoting healthy aging and cognitive function. Recent observational research suggests that a greater number of weekly steps may be protective against cognitive decline (Rabin et al., 2019). In systematic reviews and meta-analyses of randomized controlled trials (RCTs), the protective effects of physical activity on cognitive function in older adults have also been identified (Falck et al., 2019; Northey et al., 2018). In these trial reviews, clinical samples (Northey et al., 2018) and participants with clinical disorders (Falck et al., 2019), including depression (i.e., a risk factor for cognitive decline), were excluded to meet the study aims but reduce the generalizability of the findings. Other reviews of interventional research have mixed findings and cite short follow-up periods (Hoffmann et al., 2021; Young et al., 2015). However, Hoffman and colleagues (2021) observed that aerobic exercise had a large effect on memory (g = 0.80). In a review of RCTs with at least 6 months of follow-up, a protective effect of physical activity against cognitive decline or dementia was not consistently demonstrated (Brasure et al., 2018). The authors summarized the evidence as insufficient or of low-strength, potentially attributable to between-study heterogeneity and common methodological challenges, including sample size issues and short follow-up (Brasure et al., 2018).
Regular physical activity is recognized for its potential to improve cognitive function and reduce dementia risk, including Alzheimer’s disease (Piercy et al., 2018). Participation in physical activity may protect against dementia through cardiovascular, neurogenesis, or anti-inflammatory mechanisms (Valenzuela et al., 2020). For example, physical activity has cardiovascular benefits and may affect cognitive health by promoting cerebral blood flow (Valenzuela et al., 2020). Exercise may also increase neurogenesis, production of brain-derived neurotrophic factor in the hippocampus, and circulation of anti-inflammatory cytokines (IL-10β and IL-4β), actions that may improve cognitive function (Valenzuela et al., 2020). Long-term memory has specifically been identified for its potential to be modified by engagement in physical activity (Pontifex et al., 2016).
Observational studies of cohorts often demonstrate positive associations between physical activity and cognitive function. For example, physical activity (vs. non-activity) (Beckett et al., 2015) and high (vs. low) physical activity (Beydoun et al., 2014) were associated with a reduced risk of dementia in reviews published in the past decade. Blondell et al. (2014) demonstrated a longitudinal relationship between greater physical activity and a reduced risk of cognitive decline and dementia. More recently, Erickson and colleagues (2019) published a review of the physical activity literature and found strong observational evidence for beneficial, prospective associations between greater physical activity and cognitive decline and dementia. However, the individual prospective cohort studies available for inclusion in the review differed markedly in their range of adjustment for potential confounders (Beckett et al., 2015; Sofi et al., 2011).
Sofi and colleagues (2011) found that their meta-analyzed studies included differing numbers of confounders, with some including two or less. Similarly, Beckett et al. (2015) reported that studies in their review usually included a selection of certain confounders, a list that omitted race, sexual orientation, income, and baseline cognitive function. In an earlier cited review (Blondell et al., 2014), the authors conducted a sensitivity analysis of studies (n = 9) that controlled for 10 or more confounders, finding evidence of attenuation of the strength of the associations between physical activity and cognition. Two of the sensitivity analysis studies adjusted for race, one accounted for social support, none considered sexual orientation, and some considered certain social determinants (Blondell et al., 2014). Race and sexual orientation have both been excluded by studies (Laurin et al., 2001; Rovio et al., 2005) in other review work (Beydoun et al., 2014), or sometimes race but not sexual orientation is captured (Larson et al., 2006; Podewils et al., 2005). Of interest, Podewils et al. (2005) included race and adjusted for several health characteristics and behaviors (e.g., apolipoprotein E genotype, hormone replacement therapy, and alcohol use), and the lesser-studied social support. While some longitudinal associations between physical activity and dementia risk persisted after their extensive multivariable adjustment, the statistical associations were reduced in magnitude as the number of adjustment factors increased, and some statistical relationships disappeared (Podewils et al., 2005). The extent to which social determinants of cognitive aging (e.g., race, social standing, and social support) may attenuate the prospective relationships between health behaviors such as physical activity and memory remains largely understudied.
Existing evidence recognizes race and gender as important social determinants associated with disparities in physical activity. Race and gender are also related to the risk of dementia (Ferretti et al., 2018; Steenland et al., 2015). Sturman et al. (2005) found that in a biracial community in Chicago, physical activity was no longer associated with a slower rate of cognitive change after accounting for demographics and often excluded covariates of race, baseline cognitive function, and cognitive stimulation. Thus, the additional factors (e.g., race) entirely explained their associations. The authors concluded that there was no evidence to suggest that physical activity solely protects against cognitive decline in adults ≥65 years (Sturman et al., 2005). In the same study, older women were documented to engage in 2 hours less of physical activity, on average, per week, when compared to older men (Sturman et al., 2005). Forrester and colleagues’ (2019) biopsychosocial model of minority cognitive aging delineates the relationship between minority stress and cognitive aging outcomes. The authors suggest that the accumulation of social disadvantage and stressors stemming from minoritized identities (e.g., racism) are associated with cognitive aging and increased risk of dementia (Forrester et al., 2019). The model further posits that psychosocial factors (e.g., discrimination, education, and socioeconomic status) lead to unhealthy behavioral determinants such as poor diet and physical inactivity, which in turn lead to manifestations of physical/biological conditions, ultimately increasing risk for cognitive decline (Forrester et al., 2019).
Physical activity disparities by sexual orientation are evident as early as adolescence (Mereish & Poteat, 2015). This is of concern as physical activity is associated with numerous health benefits (Piercy et al., 2018), and among lesbian, gay, and bisexual (LGB) adults has been linked to better mental health (Pharr et al., 2021). Although Nelson and Andel (2020) found little evidence to support a relationship between sexual orientation and physical activity, and there were no observed differences between heterosexual persons and sexual minorities on self-reported memory. The authors concluded their work by calling for more representative, longitudinal, and cognitive research on sexual orientation to address the dearth of literature in the area (Nelson & Andel, 2020). Systemic and structural issues may prevent engagement in sufficient amounts of physical activity (Bantham et al., 2021), a positive health behavior that may help prevent or slow dementia (Valenzuela et al., 2020). However, with sufficient knowledge and resources, these barriers may be addressed and surmounted (Bantham et al., 2021). In short, there is a large literature base tying physical activity to better cognitive health; however, the extent to which a range of social determinants influence findings has not been comprehensively explored. Prospective research with adequate sample sizes which permit adjustment for a range of potential confounders and with a broad spectrum of studied ages is needed to determine whether physical activity may confer a protective memory benefit across time.
We expand the previous body of work by investigating several understudied determinants of health in a prospective examination of the relationship between physical activity and memory. To do so, we used a large Canadian cohort study of community-dwelling older adults between the ages of 45–85 years at baseline. Using the Canadian Longitudinal Study on Aging (CLSA) we sought to: (1) confirm a prospective, protective association between physical activity and objectively assessed memory, and (2) determine whether a protective association between physical activity and memory persists after adjusting for known confounders and understudied social determinants.
Methods
Study Sample
The CLSA is extensively described elsewhere (Raina et al., 2009, 2019). The CLSA is a longitudinal study of aging and general well-being. Over 50,000 community-dwelling adults between the ages of 45–85 were recruited at baseline. Prospective measurements will be collected every 3-years until 2033 or participant death (Raina et al., 2019). Baseline data collection was completed in 2015 and first follow-up in 2018 (Raina et al., 2019). The CLSA is comprised of two study cohorts that required differing amounts of participation. Participants recruited into the comprehensive cohort (n = 30,097) were required to live within a certain radius (25–50 km) of one of 11 national data collection sites (Raina et al., 2019). In-person participation for the comprehensive cohort was required for some samples not used here (e.g., blood). The tracking cohort (n = 21,241) was interviewed using a computer-assisted telephone interview (CATI) system, but both cohorts share overlapping core CLSA content, including measures of health determinants and memory (Raina et al., 2019). The cohorts were designed to be complementary so that they can be combined for researchers to have access to a larger national population-based sample (Raina et al., 2019).
Participants of the tracking cohort were recruited via the Canadian Community Health Survey (CCHS) – Healthy Aging Component (Raina et al., 2008). The eligibility criteria for the CCHS then defined the characteristics of the Canadian population eligible for participation in the CLSA, a process that enables merging of the two cohort’s data (Raina et al., 2008). Provincial health care registration databases and random digit dialing were used to recruit the comprehensive cohort and supplement recruitment into the tracking cohort (Raina et al., 2008). In accord with the sampling frame of the CCHS, certain persons or groups of persons were not eligible for CLSA survey participation: Canadian persons living in the territories or select remote regions, persons living on First Nations reserves and settlements, full-time members of the Canadian Armed Forces, and incarcerated or institutionalized persons (Raina et al., 2008). Long-term care residents are included in the definition of institutionalized persons, and more information is available in the CLSA Study Protocol (Raina et al., 2008). CLSA participants voluntarily provided written informed consent (Raina et al., 2009). These analyses received ethical clearance from the University of Ottawa Research Ethics Board (REB).
Measures
Statistical Analyses
Basic descriptive statistics were used to describe respondent characteristics at baseline (percentage [%], mean [M] and standard deviation [SD]). Respondents lost to follow-up and those with missing data were compared with retained respondents and those without missing data, respectively. To do so, we used chi-square tests of independence (χ2) and independent sample t-tests. For our primary analyses, we ran crude (unadjusted) linear regression models between physical activity and memory at follow-up, followed by multivariable linear regression models adjusted for covariates and social determinants. Therefore, there is a crude and multivariable model for each physical activity-memory relationship. Physical activity, covariates, and social determinants were all measured at baseline. We conducted multiple imputation using multivariate imputation by chained equations (MICE) (van Buuren et al., 1999) with an augmented approach (White et al., 2010) and m = 28 imputations. Unimputed (complete case) results are presented as a supplementary. Missing on the exposures (measures of PA) ranged from 0.07 to 0.40%, missing on the outcome (memory at first follow-up) was 6.98%, and missing on the covariates was in most cases ≤3% (range: 0.03–3.21%) except for income (6.12%), language of test administration (5.95%), and baseline memory (6.73%). There was no missing data for cohort status, age, and sex/gender. We did not use CLSA-derived survey weights. Others in the field have found that when using CLSA data, unweighted and weighted regression models are highly similar when measures of cognition, including memory measured by the RAVLT, are the outcome (O’Connell et al., 2019). Findings were considered statistically significant at p <0.05. All analyses were conducted using Stata (release 15: College Station, TX: StataCorp LLC).
Analytic Sample
While participants were free of cognitive impairment at the time of recruitment into the CLSA (Raina et al., 2009), some respondents self-reported a health-professional diagnosis of dementia or Alzheimer’s type dementia (n = 111), or memory problems (n = 893), at baseline. We removed these participants (Figure 1) to ensure that our analytic sample was cognitively healthy at baseline. After removal of respondents who did not participate in the initial maintaining contact questionnaire, when baseline physical activity was captured, exclusion of respondents lost to follow-up and those with missing data, the final analytic sample size was n = 30,173 before multiple imputation. Baseline data were collected between September 2011 and May 2015. The maintaining contact questionnaire was administered between baseline and follow-up (September 2013 to December 2015). First follow-up data were collected between December 2015 and July 2018. Flow diagram of respondents participating in the Canadian Longitudinal Study on Aging (CLSA) and followed from baseline to first follow-up.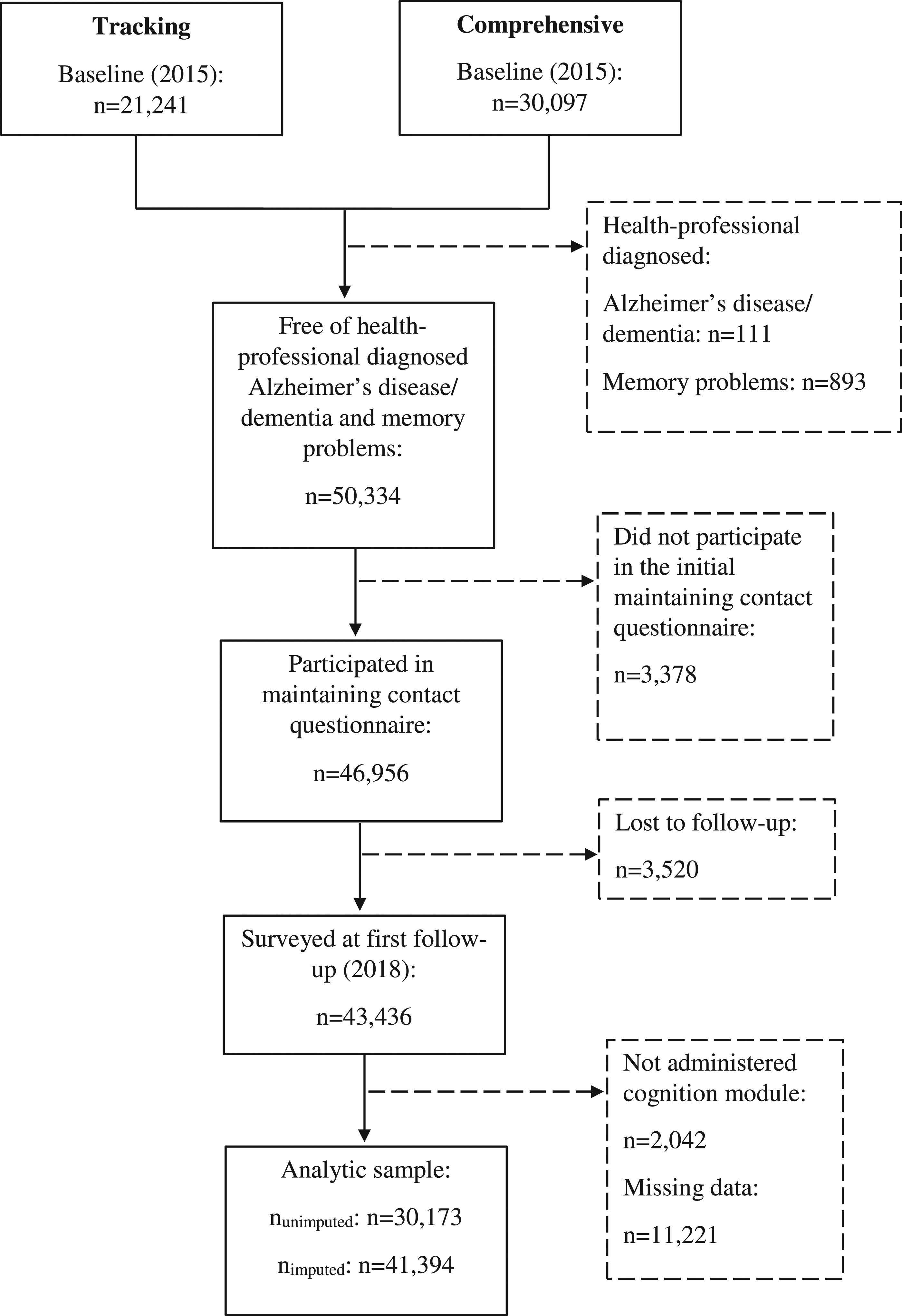
Results
Respondents Lost to Follow-Up
A comparison of respondents lost to follow-up versus retained in the CLSA at first follow-up revealed that those lost to follow-up were more likely to be members of the tracking cohort (62.2%) (χ2 = 801.57, p<0.001), men (51.9%) (χ2 = 12.91, p<0.001), and of older age (M = 66.35, SD = 11.48) (t = −20.57, p <0.001).
Respondents with Missing Data
Respondents with missing data were more likely to be part of the comprehensive cohort (55.7%) (χ2 = 173.88, p <0.001), women (54.7%) (χ2 = 88.91, p <0.001), and of older age (M = 65.22, SD = 10.52) (t = −32.20, p <0.001).
Respondent Characteristics
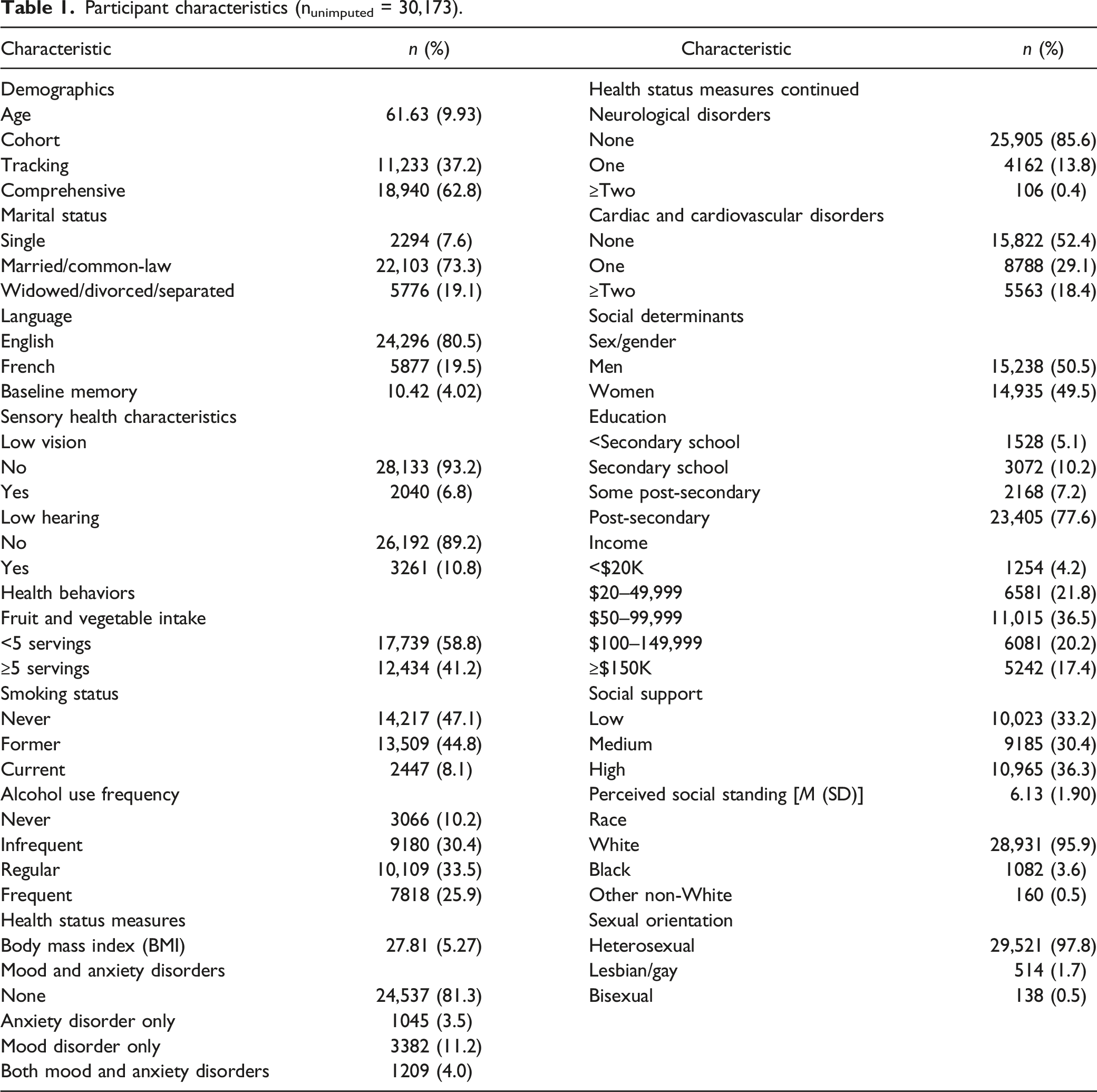
Participant characteristics (nunimputed = 30,173).
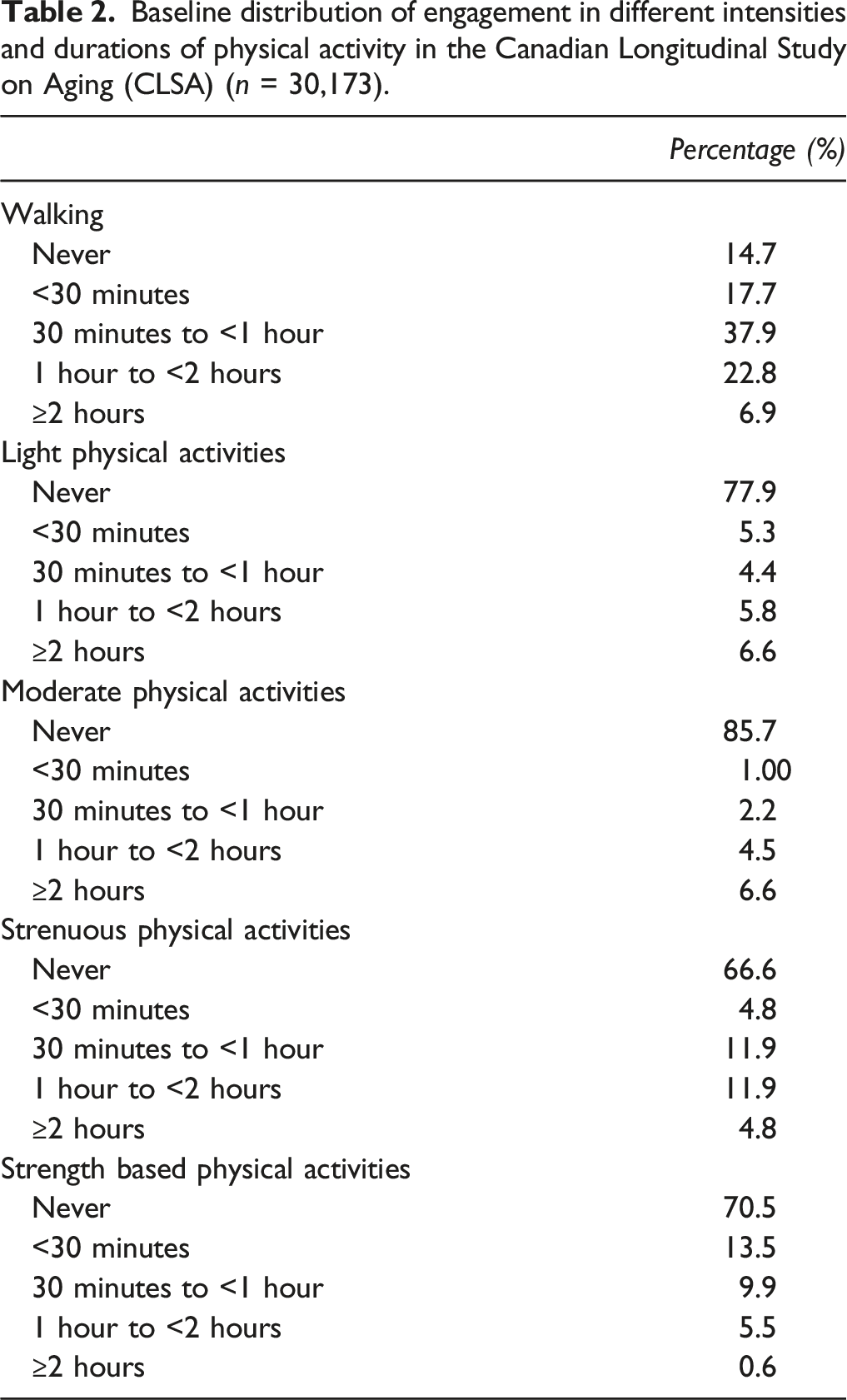
Baseline distribution of engagement in different intensities and durations of physical activity in the Canadian Longitudinal Study on Aging (CLSA) (n = 30,173).
Linear Regression Models
Crude linear regression models of the prospective relationship between physical activity at baseline and memory at first three-year follow-up in the Canadian Longitudinal Study on Aging (CLSA): multiple imputation results (n = 41,394).
Multivariable linear regression models of the prospective relationship between physical activity at baseline and memory at first three-year follow-up in the Canadian Longitudinal Study on Aging (CLSA): multiple imputation results (n = 41,394).
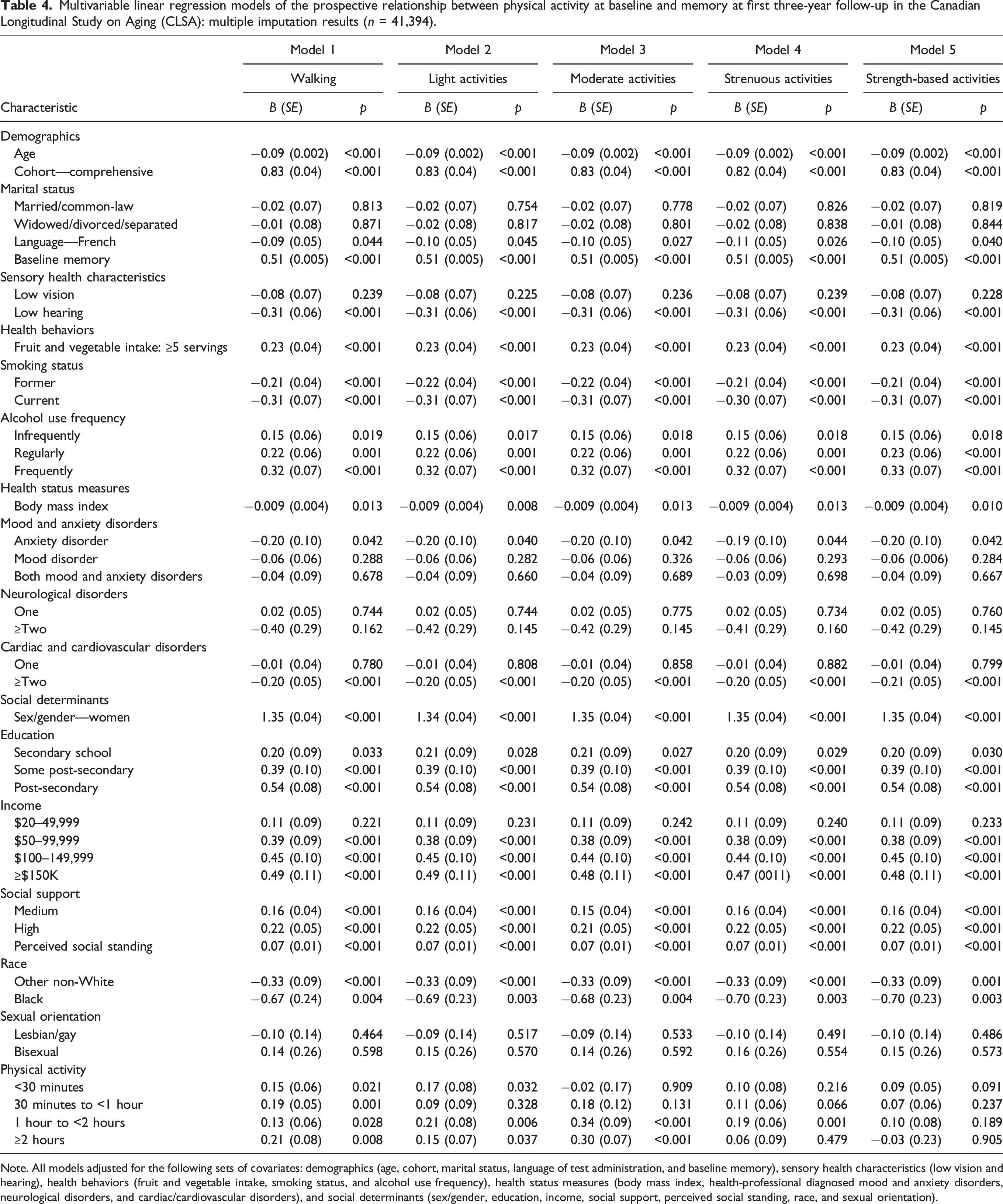
Note. All models adjusted for the following sets of covariates: demographics (age, cohort, marital status, language of test administration, and baseline memory), sensory health characteristics (low vision and hearing), health behaviors (fruit and vegetable intake, smoking status, and alcohol use frequency), health status measures (body mass index, health-professional diagnosed mood and anxiety disorders, neurological disorders, and cardiac/cardiovascular disorders), and social determinants (sex/gender, education, income, social support, perceived social standing, race, and sexual orientation).
Across all physical activity models, all social determinants of health were statistically associated with memory except for sexual orientation. There were no differences between lesbian/gay and bisexual respondents when compared to heterosexual respondents. However, there was consistent evidence of an inverse association between lesbian/gay sexual orientation identity and memory, suggesting that while not statistically significant, lesbian/gay respondents tended to show poorer memory scores at follow-up. For both education and income, there was a protective relationship with greater educational attainment and higher total household income associated with better memory. As both social support and perceived social standing increased, so too did memory. Across all models, Black and other non-White respondents had lower memory scores at follow-up when compared to White respondents; the strength of associations was noticeably stronger for Black respondents. Specifically, the magnitude of observed associations for Black respondents was more than twice the magnitude for other non-White respondents.
Complete case (unimputed) results can be found in the Supplemental eTables (1, 2) and were mostly similar to those for our previously reported primary findings. In crude models, unimputed results were nearly always weaker, except in some cases. For example, for the two negative associations (light and strength-based activities for ≥2 hours) and some intensities (moderate and strenuous activities) at <30 minutes, the results were somewhat stronger. In adjusted models, there were some differences, including lack of statistical associations between walking and memory at the shortest (<30 minutes) and highest (≥2 hours) durations. The remaining findings for social determinants and physical activity were generally consistent, with some variability in the magnitude of associations.
Discussion
We sought to confirm whether physical activity was prospectively associated with better memory at first follow-up in the CLSA. In unadjusted models and across nearly every intensity and duration of physical activity, there was evidence of a prospective relationship between physical activity and better memory at follow-up. After adjusting for known covariates and lesser-studied social determinants, walking and light activities remained almost always associated with better memory. In contrast, only the highest durations of moderate activities (>1 hour) and engaging in 1 to <2 hours of strenuous activities were associated with better memory. Although in the fully adjusted models, the observed associations were reduced in size. As expected, our observation of some prospective, protective associations between physical activity and memory aligns with existing review evidence from cohort studies suggesting that overall physical activity is beneficial (Beckett et al., 2015; Beydoun et al., 2014; Blondell et al., 2014; Erickson et al., 2019). This study adds to the existing literature base by separating different intensities and durations of physical activity. What physical activity “dose” is best for cognitive health remains unknown, and whether it may vary by population or age remains to be determined (Erickson et al., 2019). Our results suggest that after accounting for numerous health characteristics, behaviors, and social determinants, less intensive physical activities may be of most benefit for memory in this national sample of mid-life and older Canadians.
Our findings support recent advances in 24-hour movement guidelines for Canadian adults (Canadian Society for Exercise Physiology, 2021a; 2021b) and United States (US) recommendations for adults (Piercy et al., 2018). Recent guidelines for both countries recognize the potential health benefits of any physical activity, including light activities, over sedentary behaviors (Canadian Society for Exercise Physiology, 2021b, 2021a; Piercy et al., 2018). Guidelines from the US (Piercy et al., 2018) also address that not all older adults can meet recommended moderate to vigorous activity recommendations due to health considerations but should strive to engage in any amount of physical activity that they are able to. Such advances are relevant because they may be considered more accessibility and equity orientated. However, our findings also share some similarities with those of Sturman and colleagues (2005), who found that after adjustment for covariates often missing from the existing literature (race, baseline cognition, cognitive stimulation), there was no association between physical activity and cognition. Consistent with their work, we did not observe statistical relationships between shorter durations of moderate intensity activities, and almost no associations for strenuous and strength-based activities, in fully adjusted models. There is some evidence to suggest that among older adults, strength-based activities may be better tied to executive function and overall cognition than memory (Li et al., 2018).
In addition to physical activity, cognitive aging outcomes have been linked to other health behaviors (e.g., fruit and vegetable intake) and sensory health (e.g., hearing) (Stinchcombe & Hammond, 2021), mental health (e.g., depression), as well as social determinants such as social support (Oremus et al., 2020). The strength and direction of associations for our relationships between social determinants and memory correspond with earlier CLSA cross-sectional work, showing disparities in memory by income, education, and race (Stinchcombe & Hammond, 2021). In their review of how to address social inequities in physical activity, Ball and colleagues (2015) draw attention to the social gradient. The authors (Ball et al., 2015) cite Australian work (Australian Bureau of Statistics, 2013) that found that the most socioeconomically privileged adults are more likely to engage in “sufficient physical activity.” Health behavior change is already notoriously difficult at the level of the individual (Samdal et al., 2017) and the population (Kelly & Barker, 2016). Adding to the challenge of general public health promotion of healthy lifestyles, some population groups are more likely to experience barriers to participation in physical activity (Bantham et al., 2021). While our findings support engagement in physical activity for memory benefits in mid-life and older adulthood, particularly the potentially more widely accessible walking and light activities, some persons may be socially obstructed from participating. Members of minority communities often experience disadvantage and barriers to engaging in health promoting behaviors that are linked to cognitive aging (Forrester et al., 2019). Equitable ways to promote physical activity are needed and may be realized through various methods, including community-based approaches and engagement (Ball et al., 2015; Bantham et al., 2021).
In the present study, we did not find a protective relationship for muscle strengthening activities, for engagement in moderate activities <1 hour per day, or most durations of strenuous activities. In terms of memory, the benefits of aerobic activities may outweigh those of muscle strengthening activities when activities are considered in isolation. A combination of aerobic and muscle strengthening activities may be best and is supported by clinical trial evidence (Bossers et al., 2015). Our findings build on previous work by including social determinants of cognitive aging and demonstrate that in a real-world context, where participants may be diverse in their sociodemographic profiles and experience of inequality and disadvantage, the benefits of physical activity may only be observed for some less intense physical activities, or for certain durations. This is also after accounting for other potential daily stressors: medical conditions and loss of a partner (e.g., widowed).
Strengths and Limitations
Our study included the first available follow-up data from the CLSA, yet a limitation is that the follow-up period may still be considered short. While we were able to study how many social determinants are related to cognitive aging, minority stress experiences may be better captured through perceived discrimination or other markers of social disadvantage. We captured multiple minoritized identities in the present study, but these persons comparatively made up a small proportion of the sample. For example, <4.5% of participants in the sample were racialized and <2.5% identified as LGB. These findings require replication, and cognitive aging research that engages members of minoritized communities is needed. Another limitation is our use of a past-week self-report measure of physical activity instead of physical activity data collected via objective means. On average, self-report of physical activity is over-estimated compared to data collected via accelerometer (Prince et al., 2008). Strengths included the population-based survey methodology and our inclusion of several health-professional diagnosed neurological and cardiac/cardiovascular health disorders. In accounting for health disorders, we took a deficit accumulation type approach (Rockwood & Mitnitski, 2007), increasing confidence in the likelihood that frailty may not explain our observed associations. Further, the prospective relationship between physical activity and memory is lesser studied in mid-life adults (Erickson et al., 2019), an age group included here.
Conclusions
From a health equity perspective, population-level benefits of physical activity on memory may only be observed for less intense physical activities, especially walking. Our results suggest that walking and light activities were associated with better memory, and to a lesser extent, moderate physical activity, but only at high levels (>1 hour per day), after accounting for social determinants. Less intensive activities may be more broadly accessible to a wider range of the older adult general population. Therefore, more people may be able to engage in light activities more regularly, increasing their potential long-term cognitive health benefits. The benefit of light exercise may be underestimated.
Supplemental Material
sj-pdf-1-roa-10.1177_01640275211070001 - Supplemental Material for Prospective Associations between Physical Activity and Memory in the Canadian Longitudinal Study on Aging: Examining Social Determinants
Supplemental Material, sj-pdf-1-roa-10.1177_01640275211070001 for Prospective Associations between Physical Activity and Memory in the Canadian Longitudinal Study on Aging: Examining Social Determinants by Nicole G. Hammond and Arne Stinchcombe in Research on Aging
Footnotes
Acknowledgments
The authors would like to thank the participants of the Canadian Longitudinal Study on Aging (CLSA) for their contributions to research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the CLSA is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation. This research has been conducted using the CLSA Baseline Tracking Dataset version 3.6, Baseline Comprehensive Dataset version 4.2, Follow-up 1 Tracking Dataset version 2.1, Follow-up 1 Comprehensive Dataset version 3.0, under Application Number 190238. The CLSA is led by Drs. Parminder Raina, Christina Wolfson, and Susan Kirkland. This work was supported by a grant from the Alzheimer’s Society of Canada Research Program awarded to Dr. Arne Stinchcombe. Ms. Nicole G. Hammond is funded by the Frederick Banting and Charles Best Canada Graduate Scholarship Doctoral Awards (CGS-D) program.
Disclaimer
The opinions expressed in this manuscript are the author’s own and do not reflect the views of the Canadian Longitudinal Study on Aging (CLSA).
Data Availability Statement
Supplementary Material
Supplementary material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.