
Abstract
Transforming nursing homes (NHs) from restrictive institutions to person-centered homes, referred to as NH culture change, is complex and multifaceted. This study, based on a survey of administrators in Minnesota NHs (n = 102), tested the domain-specific relationships of culture change practices with resident quality of life (QOL) and family satisfaction, and examined the moderating effect of small-home or household models on these relationships. The findings revealed that culture change operationalized through physical environment transformation, staff empowerment, staff leadership, and end-of-life care was positively associated with at least one domain of resident QOL and family satisfaction, while staff empowerment had the most extensive effects. Implementing small-home and household models had a buffering effect on the positive relationships between staff empowerment and the outcomes. The findings provide meaningful implications for designing and implementing NH culture change practices that best benefit residents’ QOL and improve family satisfaction.
Keywords
Background
Nursing home (NH) culture change is generally viewed as a philosophy and a process seeking to transform NHs from restrictive institutions to living communities where residents can continue their lives according to their preference and with dignity (Koren, 2010; Mitty, 2005; Zimmerman et al., 2014). Culture change in NHs has become a national campaign in the United States with about 88% of NHs at least partially engaging in and 16% completely implementing culture change practices (Miller et al., 2018), and it also has gained growing recognition in the NH industry worldwide (Caspar et al., 2009; de Rooij et al., 2011; Sjogren et al., 2017).
While some NHs implement culture change through adopting established models such as the Green House Project (Rabig et al., 2006), others develop their culture change initiatives based on the organization’s budget, mission, leadership, workforce, resident case mix, or external policies (Zimmerman et al., 2014). Culture change is inherently complex (Sterns et al., 2010) and typically involves reforms of three major domains: care practices, workplace practices, and the physical environment according to the Holistic Approach to Transformational Change (HATCh) model (Healthcentric Advisors, 2020) and the Nursing Home Integrated Model for Producing and Assessing Cultural Transformation (Hartmann et al., 2013). Culture change in care practices involves prioritizing resident preferences and promoting resident autonomy and engagement. Culture change in workplace practices embraces staff empowerment, interdisciplinary collaboration, and nonhierarchical management. The environment domain of culture change involves modifying the physical environment to feature a home-like atmosphere and a supportive design that promotes residents’ independence and engagement (Hartmann et al., 2013).
Literature Review
The number of studies examining the effects of culture change practices on quality outcomes is accumulating. However, prior studies focused on quality of care indicators derived from clinical data or administrative data, and few statistically significant correlations between culture change and clinical quality outcomes have been found (Hill et al., 2011; Shier et al., 2014). Although the ultimate goal of NH culture change is to improve resident quality of life (QOL) and family satisfaction, these two important outcomes have not been adequately examined (Hill et al., 2011; Shier et al., 2014; Duan, Mueller, Yu, & Talley, 2020). Measures of QOL for NH residents should reflect an individual’s multidimensional appraisal of important aspects of life including physical, psychological, social, and environmental well-being (Kane et al., 2003). Prior studies examining QOL-related outcomes tended to use unidimensional measures that only tapped single domains of QOL, such as functional ability, satisfaction with services, perceptions of choice over basic everyday activities (Burack et al., 2012; Molony et al., 2011; Poey et al., 2017), or use measures that were not reported by residents themselves, such as survey deficiencies (Lepore et al., 2020). Only a few used multidimensional and self-reported measures of QOL (Kane et al., 2007). Moreover, family satisfaction has been rarely studied as an outcome of culture change implementation. However, family members provide important information about quality of care as they continue their involvement in caring for their loved ones after NH placement (Shippee, Henning-Smith, Gaugler, Held, & Kane, 2017).
While previous studies tended to examine culture change as a whole “package” (such as a binary measure of whether or not a certain culture change model is implemented; Burack, et al., 2012; Kane et al., 2007), it is important to recognize the complexity of culture change and the variations in depth and scope of culture change implementation across NHs (Miller et al., 2014, 2018). As shown in a national survey of culture change practices in U.S. NHs, culture change practices associated with resident-centered care and physical environment association were more prevalent than practices associated with staff empowerment and family and community engagement (Miller et al., 2014, 2018). With the development of comprehensive domain-specific culture change assessment tools, deconstructing the complex culture change into its domains and evaluated domain-sensitive outcomes has become possible (Miller et al., 2014, 2018). Examining domain-specific relationships will better inform the development of outcome-oriented culture change initiatives and maximize the efficacy and cost-effectiveness of culture change interventions (Miller et al., 2014, 2018). This is particularly important given the outcome variables—resident QOL and family satisfaction—are multidimensional and complex in themselves (Kane et al., 2003).
The moderating effect of architectural renovation on the relationships between culture change practices and quality outcomes has not been examined in the literature. Physical environment transformation is one of the components of NH culture change and has been realized in various forms (Miller et al., 2018). Some NHs may engage in radical changes in architectural structure by building self-contained units or small-scale homes (often referred to as small-home or household models), while others may only implement small and financially manageable changes in the physical environment, such as eliminating overhead pages and encouraging home-like decorations (Shield et al., 2014). Investigating if culture change practices yield different effects in NHs implementing small-home or household models versus NHs maintaining the traditional architectural structure will provide practical implications for NH providers as they design cost-effectiveness culture change interventions (Shield, Tyler, et al., 2014).
To address those knowledge gaps, this study aims to (1) test the domain-specific relationships of culture change practices with resident QOL and family satisfaction, (2) examine the moderating effect of small-home or household models on these relationships. We hypothesized that culture change practices are positively associated with various resident QOL domains or family satisfaction domains, and the positive relationships between culture change practices and resident QOL or family satisfaction are more pronounced in NHs implementing small-home or household models than in traditional NHs.
Method
Sample and Data Sources
This study applied a cross-sectional design, and the target population was all Medicare and/or Medicaid certified NHs in Minnesota (n = 363). This study used a total population sampling method and NH administrators from all Medicare and/or Medicaid certified NHs in Minnesota were invited to participate in an online survey about the implementation of culture change practices in their facility. The survey was conducted between August 2018 and January 2019, and 102 NH administrators completed the survey with a response rate of 28.1%. Administrative data (i.e., NH characteristics and quality measures) obtained from the Minnesota Department of Human Services was linked to the survey data. This study was exempt from human subject research by the Institutional Review Board of University of Minnesota because no personal questions of respondents were involved in the survey and only facility-level data were used.
Variables and Measures
Culture change practices
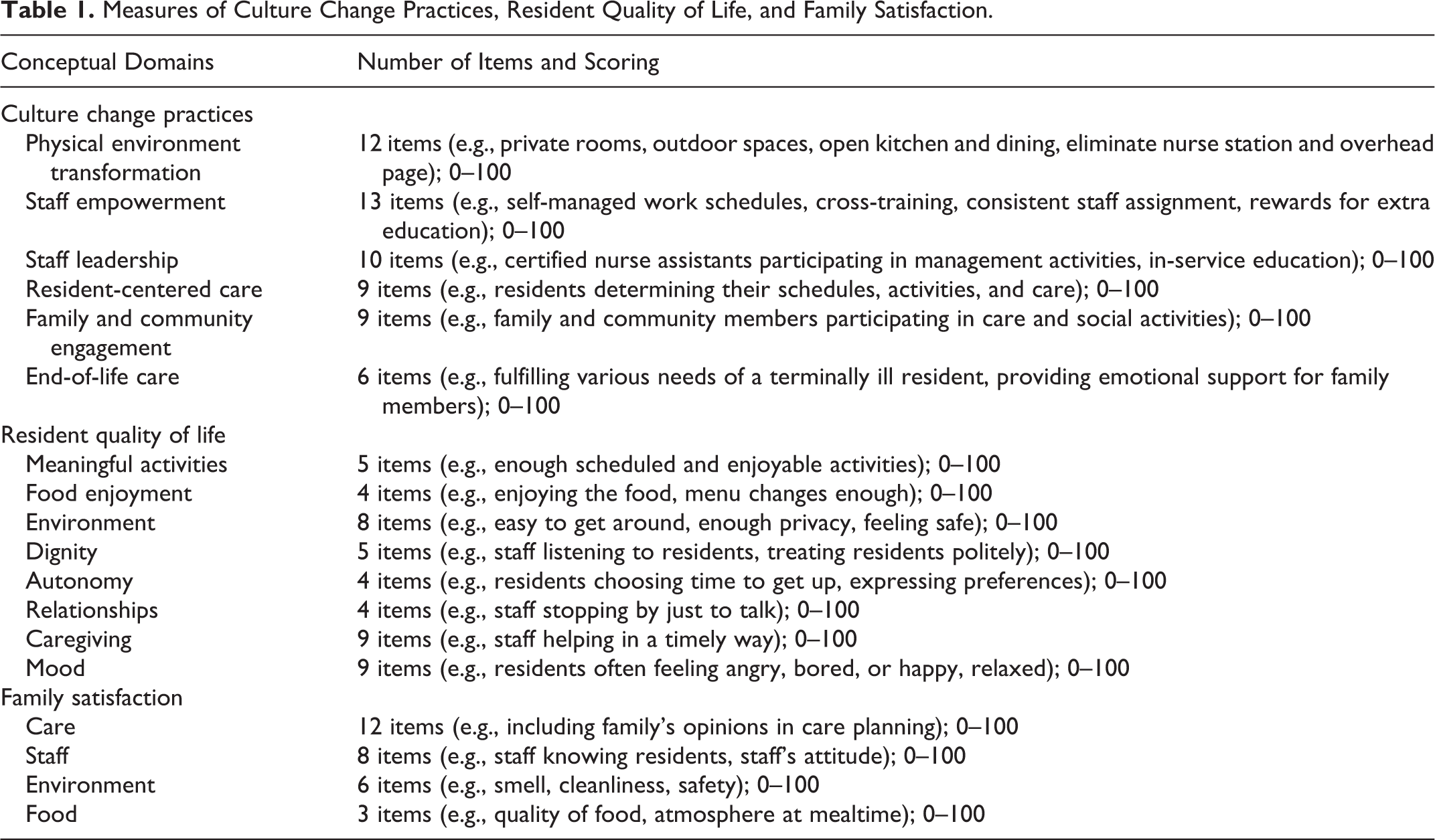
The key independent variables are culture change practices collected through the online survey of NH administrators. The survey instrument was adapted from a culture change assessment tool developed by researchers at Brown University (Miller et al., 2014). The tool measures six domains of culture change practices including physical environment transformation, staff empowerment, staff leadership, resident-centered care, family and community engagement, and end-of-life care. Table 1 lists examples of survey items in each domain. As suggested by the previous use of the tool (Miller et al., 2018), a composite score was obtained for each domain by summing the raw item scores, and then rescaled to 0–100. The missing value of an item was imputed using the mean of completed items in a given domain if one or two items were missing for that domain (imputations were performed for 1–11 NHs per domain). The domain score was reported as incomplete if over two items were missing (missing domain scores were reported for 5–9 NHs per domain). This instrument has demonstrated good internal consistency as reported by previous studies (omega coefficients 0.81–0.91 for six domains; Miller et al., 2018; Tyler et al., 2011). The instrument has satisfactory face and content validity, as it has undergone a rigorous process of item development and scale validation (Miller et al., 2018; Tyler et al., 2011). Cronbach’s α of each domain based on the current sample ranged from 0.43 for physical environment transformation to 0.79 for family and community engagement.
Measures of Culture Change Practices, Resident Quality of Life, and Family Satisfaction.
The moderating variable is the implementation of small-home or household models. The culture change survey contains questions asking whether the facility has redesigned or built some sections of their facility into small-homes or households that house no more than 8–10 or 14–20 residents respectively that include kitchens, dining facilities, and common living areas. The answer was coded as 1 = implementing small-home or household models and 0 = not implementing.
Quality outcomes
Facility-level risk-adjusted quality measures on resident QOL and family satisfaction came from publicly available data published in the 2018 Minnesota Nursing Home Report Card (Minnesota Department of Health and Human Services, 2019). Resident QOL and family satisfaction are collected through face-to-face interviews or surveys with a random sample of residents or family members in every NH. The Minnesota Department of Human Services contracts with an outside research vendor to complete these standardized interviews and surveys annually.
Both resident QOL and family satisfaction surveys capture multiple domains of quality outcomes. Table 1 shows the outcome measures by domain. The resident QOL survey has eight domains including meaningful activities, food enjoyment, environment, dignity, autonomy, relationships, caregiving, and mood. The family satisfaction survey has four domains including staff, care, environment, and food. Each resident QOL or family satisfaction domain is measured on a 0–100 scale with higher scores indicating better outcomes. A summary score of resident QOL or family satisfaction for an individual was calculated by taking the average of the domain scores. This study used the risk-adjusted facility-level score for each outcome. Risk-adjusted facility-level quality scores created by Minnesota Department of Health and Human Services (2019) were facility-aggregated averages constructed by taking the predicted mean of all interviewed or surveyed individuals in the NH based on linear regression modeling adjusting for facility characteristics and resident or family member characteristics that are generally not a result of provider performance. Hierarchical linear regression modeling is used to account for the variation in the number of surveys per facility (Minnesota Department of Health and Human Services, 2019). The reliability of resident QOL and family satisfaction instruments have been documented with Cronbach’s α ranging from 0.53 to 0.77 across the eight resident QOL domains (Kane et al., 2003) and 0.860.96 across the four family satisfaction domains (Shippee et al., 2017).
NH structural and organizational characteristics
Data on NH structural and organizational characteristics were obtained from cost reports submitted by facilities to the Minnesota Department of Human Services. The variables included proprietary status (for-profit, non-profit, government-owned), chain affiliation (yes/no), geographic location (metropolitan, micropolitan, rural), size (number of active beds), occupancy rate (the number of occupied beds divided by the total number of active beds), payer mix (percentage of resident days paid by Medicaid), and staffing (hours of a given type of staff per resident day). Staffing was calculated for registered nurses (RNs), licensed practical nurses (LPNs), certified nursing assistants (CNAs), mental health and social work staff, and activity staff.
Analysis
Descriptive statistics were used to describe NH characteristics, culture change domain scores, resident QOL scores, and family satisfaction scores. ANOVA or χ2 tests were used to compare sample characteristics between NHs implementing small-home or household models and NHs maintaining the traditional architectural structure. We built a linear regression model separately for the summary scores of resident QOL and family satisfaction, and their domain scores. The independent variable was an individual culture change domain (six culture change domains were introduced separately). We added an interaction between a given culture change domain and small-home or household models to each regression model to test the moderating effect of small-home or household models. Each regression model controlled for covariates that were found associated with QOL and family satisfaction in prior studies (i.e., number of active beds, activity staff hours per resident day, and proportion of Medicaid resident days; Shippee et al., 2017; Shippee, Henning-Smith, Kane, & Lewis, 2015; Shippee, Hong, Henning-Smith, & Kane, 2015). We also a conducted sensitivity analysis by introducing a different set of covariates (including proprietary status, geographic location, chain affiliation, occupancy rates, nurse assistant staffing, number of active beds, activity staff hours per resident day, and proportion of Medicaid resident days). The results (available upon request) were consistent with the initial models. All analyses were conducted in Stata 15.0 (StataCorp, 2017). Sampling weights were applied to ANOVA, χ2 tests, and regression analyses to adjust for the disproportional sampling of NHs of different proprietary status and geographic location. The Stata syntax poststrata and postweight under the syvset command was used to adjust the sample weights and the population size.
When testing the domain-specific association, our statistical hypothesis is that a certain culture change domain is associated with at least one resident QOL domain or family satisfaction domain. As multiple hypothesis tests were performed to test the relationships of a given a certain culture change domain with multiple outcome domains (eight resident QOL domains and four family satisfaction domains), the results may be subjected to increased family-wise error rate (FWER, the probability of making one or more false discoveries or type I errors). Therefore, we applied Šidák correction to each test of individual outcome domains to counteract the multiple comparison problem (Abdi, 2007). Given a family-wise α level of 0.5 for testing eight different null hypotheses on the relationships of a culture change domain with eight resident QOL domains, each null hypothesis was rejected that had a p-value lower than αper test of resident QOL domains =
Results
Table 2 shows the characteristics of participating NHs. No significant differences in NH characteristics and the quality outcomes were observed between participants and non-participants, except that participating NHs were less likely to be affiliated with a chain (49% vs 64%) and had slightly higher CNA hours per resident day (2.42 vs. 2.32; p < .05). Of the surveyed NHs, 34% (n = 35) implemented small-home or household models. As shown in Table 2, NHs implementing small-home or household models were more likely to be non-profit, have a higher number of active beds, a higher occupancy rate, lower staffing of activity staff, and a lower proportion of Medicaid residents (p < .05). They also reported higher culture change scores in physical environmental transformation and staff empowerment (p < .05). Nursing homes that implemented small-home or household models had significantly higher scores on overall resident QOL and three QOL domains (i.e., environment, autonomy, caregiving), and overall family satisfaction and three satisfaction domains (i.e., care, environment, food; p < .05).
Nursing Home (NH) Characteristics, Culture Change Scores, Resident Quality of Life, and Family Satisfaction by Status of NHs That Did and Did Not Implement Small-Home or Household Models.
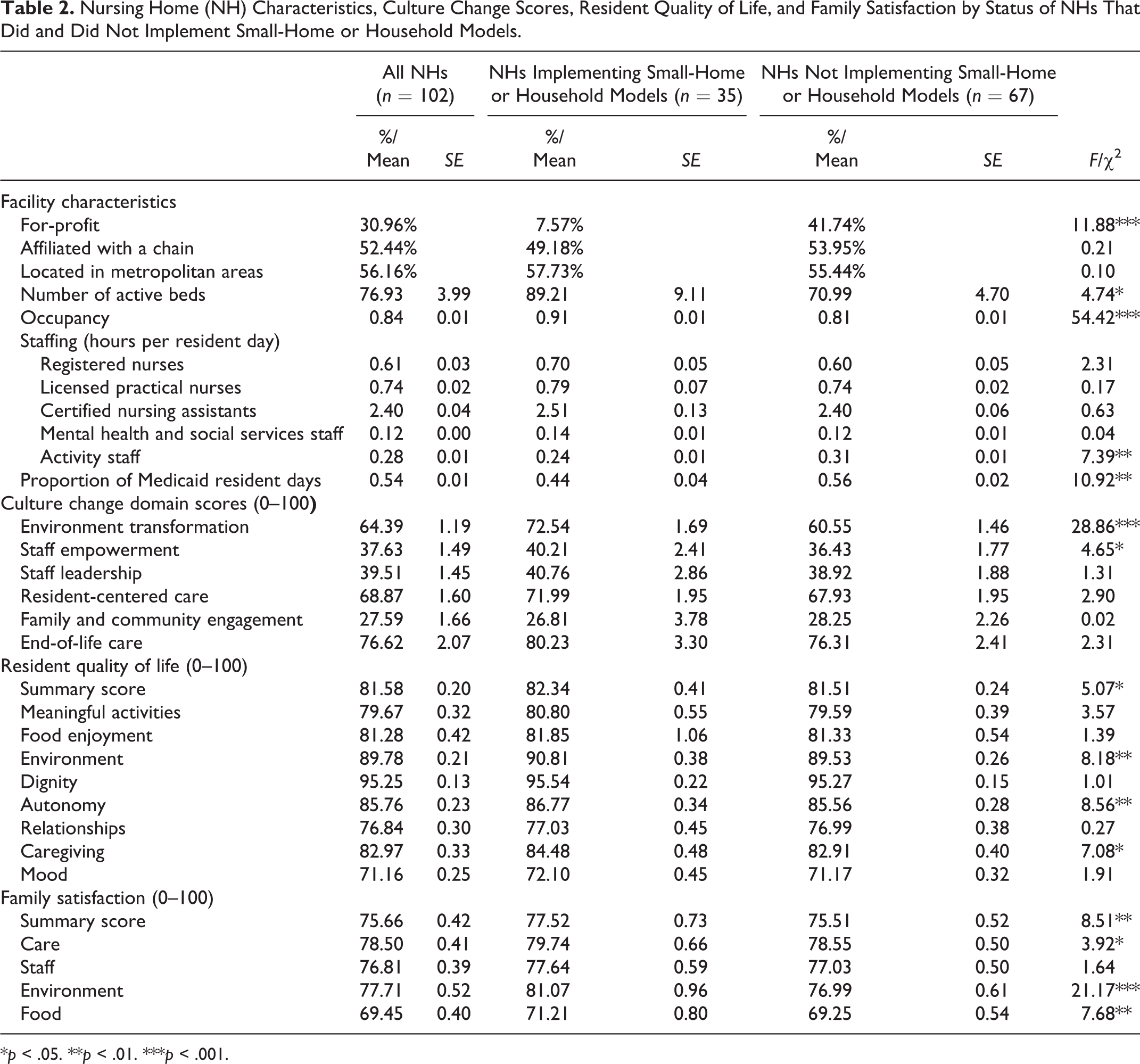
*p < .05. **p < .01. ***p < .001.
Table 3 presents the regression results for the association of each culture change domain with resident QOL, adjusting for the interaction with small-home or household models and covariates (including the number of active beds, activity staff hours per resident day, and proportion of Medicaid resident days). Culture change domains including physical environment transformation, staff empowerment, and staff leadership were significantly associated with the resident QOL summary score (p < .05). At the corrected significance level of (αper test of resident QOL domains = 0.0064) for testing the association with individual resident QOL domains, staff empowerment was found significantly associated with five resident QOL domains including meaningful activities, food enjoyment, dignity, autonomy, and caregiving (p < .006). Staff leadership had a statistically significant association with three resident QOL domains including meaningful activities, dignity, and autonomy (p < .006). End-of-life care had a statistically significant association with meaningful activities (p < .006). In the model testing the association between physical environment transformation and outcome variables, we did not include the interaction term with small-home or household model because of the collinearity between small-home or household models and physical environment transformation. Physical environment transformation was found significantly associated with the environment domain of resident QOL (p < .006).
Unstandardized Coefficients of Individual Culture Change Domains and the Moderating Effect of Small-Home/Household Models in Regression Models for Resident Quality of Life.
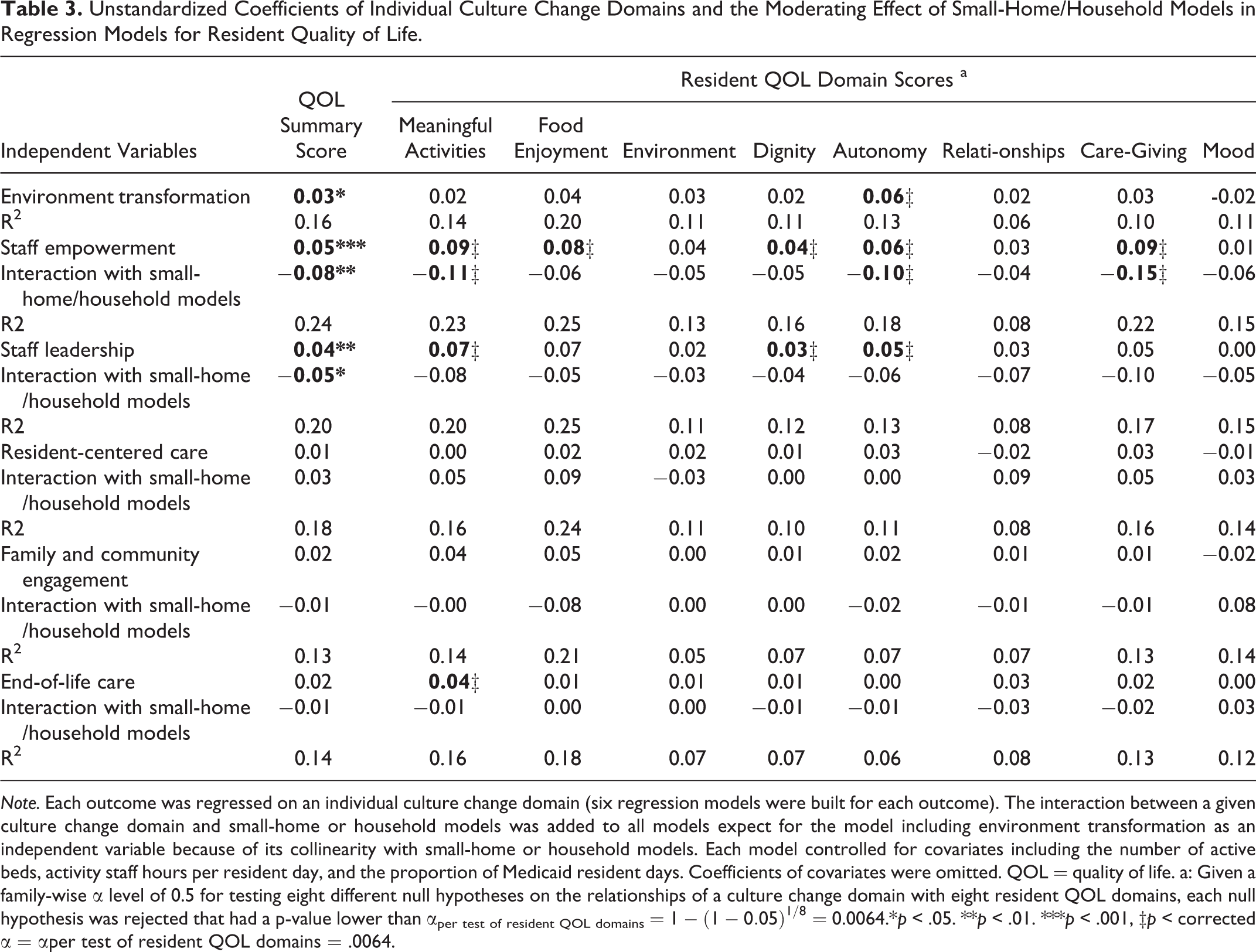
Note. Each outcome was regressed on an individual culture change domain (six regression models were built for each outcome). The interaction between a given culture change domain and small-home or household models was added to all models expect for the model including environment transformation as an independent variable because of its collinearity with small-home or household models. Each model controlled for covariates including the number of active beds, activity staff hours per resident day, and the proportion of Medicaid resident days. Coefficients of covariates were omitted. QOL = quality of life. a: Given a family-wise α level of 0.5 for testing eight different null hypotheses on the relationships of a culture change domain with eight resident QOL domains, each null hypothesis was rejected that had a p-value lower than αper test of resident QOL domains =
Table 3 also demonstrates the moderating effect of small-home and household models on the relationships between culture change and resident QOL. The moderating effect was statistically significant for the relationships of staff empowerment with resident QOL summary score (p < .05) and with three QOL domains including meaningful activities, autonomy, and caregiving (p < .006). A significant moderating effect was also found for the relationship of staff leadership with resident QOL summary score (p < .05). The coefficients of the moderating effects were less than zero and had an absolute value greater than the coefficient of a given culture change domain, indicating that resident QOL declined with the increase of the culture change domain score for NHs implementing small-home or household models. As an example, a 1-point increase in the staff empowerment score resulted in an increase in the QOL summary score of 0.05 (staff empowerment + staff empowerment × small-home or household models = 0.05 × 1 + (−0.08) ×1× 0 = 0.05) for NHs not implementing small-home or household models. However, in NHs implementing small-home or household models, a 1-point increase in staff empowerment score resulted in a decrease in the QOL summary score of 0.03 (staff empowerment + staff empowerment × small-home or household models = 0.05 × 1 + (−0.08) × 1 × 1 = −0.03). Figure 1 illustrates margins of the outcomes predicted by a given culture change domain at the means of covariates by NHs with or without the implementation of small-home or household models for regression models with a statistically significant interaction term.
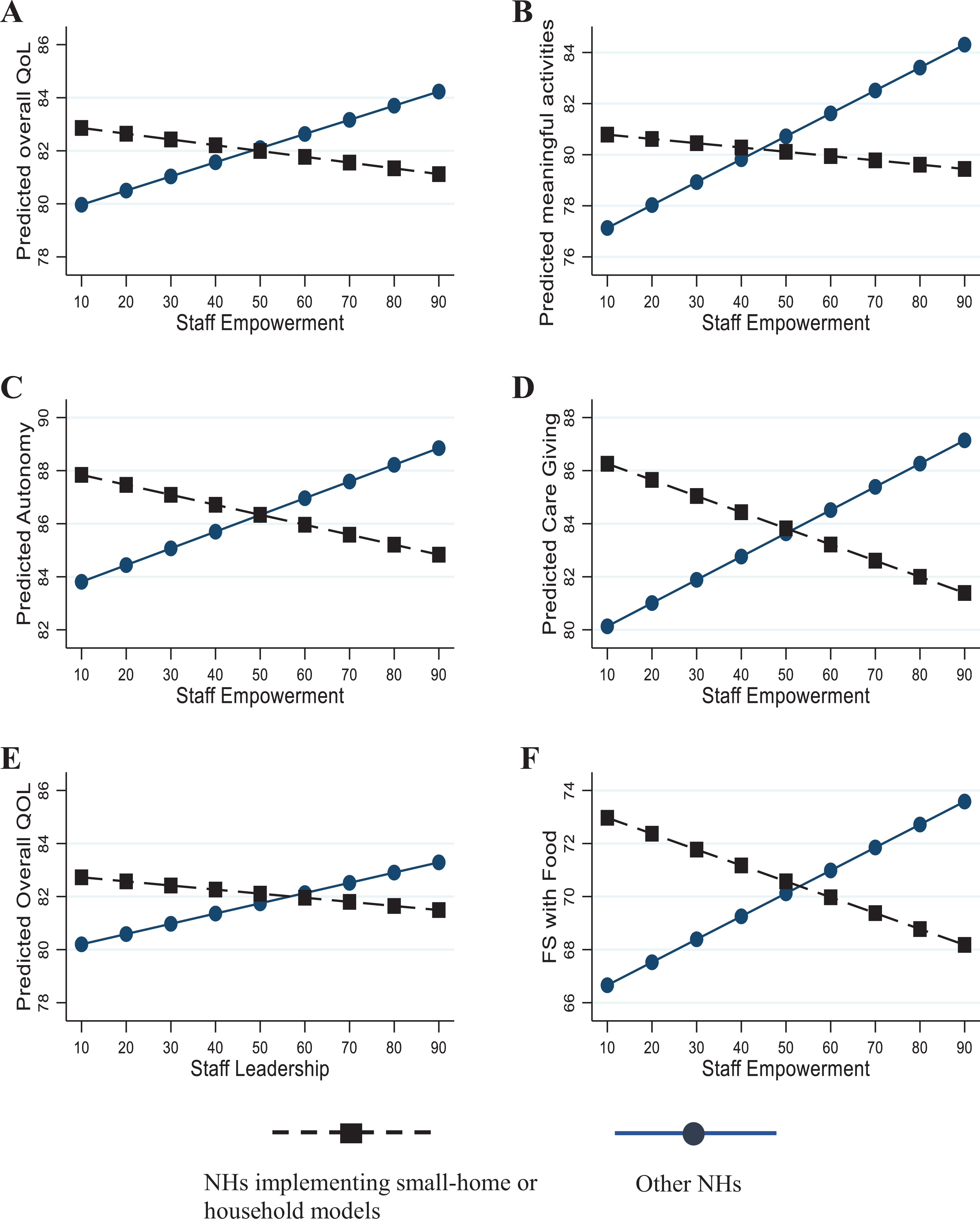
Margins of resident QOL scores and family satisfaction by status of NHS that did and did not implement small-home or household models.
Table 4 presents the regression results for the association of each culture change domain with family satisfaction, adjusting for the interaction with small-home or household models and covariates. Only one culture change domain—end-of-life care—was significantly associated with the family satisfaction summary score (p < .05). At the corrected significance level (αper test of family satisfaction domains = 0.0127) for testing the association with individual family satisfaction domains, three culture change domains, including staff empowerment, staff leadership, and end-of-life care, were significantly associated with the food domain of family satisfaction (p < .013). Physical environment transformation had a statistically significant association with the environment domain of family satisfaction (p < .013).
Unstandardized Coefficients of Individual Culture Change Domains and the Moderating Effect of Small-Home/Household Models in Regression Models for Family Satisfaction.
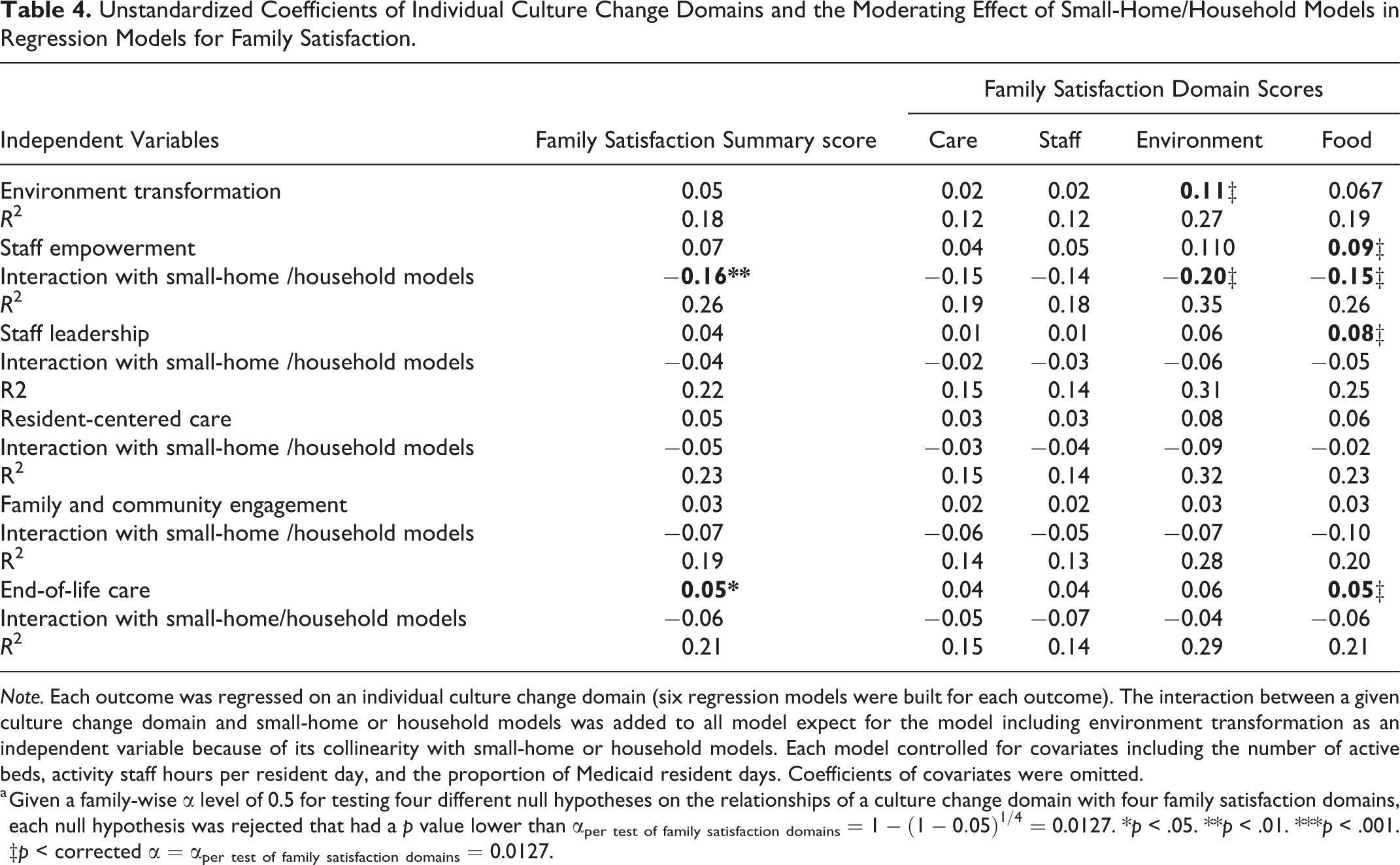
Note. Each outcome was regressed on an individual culture change domain (six regression models were built for each outcome). The interaction between a given culture change domain and small-home or household models was added to all model expect for the model including environment transformation as an independent variable because of its collinearity with small-home or household models. Each model controlled for covariates including the number of active beds, activity staff hours per resident day, and the proportion of Medicaid resident days. Coefficients of covariates were omitted.
a Given a family-wise α level of 0.5 for testing four different null hypotheses on the relationships of a culture change domain with four family satisfaction domains, each null hypothesis was rejected that had a p value lower than αper test of family satisfaction domains =
Table 4 also shows the moderating effect of small-home and household models on the relationships between culture change and family satisfaction. A significant negative moderating effect was found for the relationship between staff empowerment and the food domain of family satisfaction (p < .013). A 1-point increase in the staff empowerment score resulted in an increase of 0.09 in the food domain of family satisfaction for NHs not implementing small-home or household models, but a decrease of 0.06 for NHs implementing small-home or household models.
Discussions
Overall, this study revealed that four out of six domains of culture change practices, including physical environment transformation, staff empowerment, staff leadership, and end-of-life care were positively associated with at least one specific domain of resident QOL and family satisfaction. Staff empowerment had the most extensive benefits on resident QOL as it was significantly associated with five out of eight resident QOL domains. Implementing small-home and household models had a moderating effect on the relationships of staff empowerment with resident QOL and family satisfaction, yet the direction of the moderating effect was opposite to our hypothesis.
The Domain-Specific Relationships Between Culture Change Practices and Resident QOL/Family Satisfaction
Our study revealed that staff empowerment had the most extensive benefits on resident QOL, ranging from promoting residents’ positive experience with meal services and day-to-day care to improving psychosocial well-being (specifically dignity, autonomy, and meaningful activities). Fostering leadership of direct care staff also showed a favorable impact on three QOL domains including dignity, autonomy, and meaningful activities. As posited in Kanter’s theory of structural empowerment (Kanter, 1987), empowering staff relates to providing access to two aspects of organizational structures: power structures (i.e., access to resources, information, and support) and opportunity structures (i.e., advancement in the organization and professional growth). In our survey, the staff empowerment domain measures empowerment in power structures, such as direct care staff’s autonomy toward care activities, self-managed work schedules, and collaborative work, while the staff leadership domains measures empowerment in opportunity structures such as formal opportunities for direct care staff to participate in management activities and professional development activities.
Our findings regarding the positive relationships between a variety of empowerment strategies (including empowerment on both power structures and opportunity structures) and resident QOL are consistent with prior studies. For example, Barry, Brannon, and Mor (2005) indicated that more autonomy over resident care given to nurse assistants was associated with a higher level of social engagement for residents. Empowering nursing staff was associated with family-reported service quality (Hamann, 2014) and the staff’s commitment to providing individualized care (Caspar & O’Rourke, 2008). However, prior studies did not address resident-reported QOL as an outcome of staff empowerment implementation. Some studies provided mechanism-based explanations regarding how staff empowerment influences the care process and care outcomes. Using contingency theory, Zinn et al. (2003) related the value of staff empowerment to the care structure in NH settings. They explained that NH care involves a considerable amount of psychosocial care that is organically structured as opposed to mechanistically structured physical and medical care. A less centralized management structure and a less standardized care process are particularly important for providing psychosocial care. Anderson et al. (2003) also indicated that a working environment with more autonomy may facilitate the information flow among people and the diversity of cognitive schema, which in turn leads to improved quality.
The finding of particular interest is the positive association between resident-and-family-centered end-of-life care and perceived meaningful activities. Death is common in NHs, as one in five of all U.S. deaths and 43% of deaths for individuals over the age of 85 occurred in NHs (Wetle et al., 2004). High-quality end-of-life care has been gaining recognition in long-term care settings (Miller et al., 2018), and it involves various strategic care solutions related to symptom management, pain management, advanced care planning, and palliative/hospice care (Miller & Han, 2008). Although we did not examine these specific care strategies, our finding suggested that person-centered values embedded in end-of-life care that honors various needs of terminally ill residents and their family members/friends are crucial for residents in general to perceive a meaningful life. The finding is supported by prior studies that suggest care culture and value towards end-of-life care is important for the residents, the family, staff, and other residents in NHs (Forbes-Thompson & Gessert, 2005; Wallace et al., 2018).
The positive relationship between physical environment transformation and residents’ perception of autonomy is another finding worthy of note. Regardless of architectural renovations such as redesigning or building some sections of the facility into small-homes or households, those financially manageable actions of eliminating institutional features of the NHs (e.g., removing nurse station and overhead paging, building accessible indoor/outdoor play areas, displaying personal items in common areas, home-like decoration) has shown beneficial effects on resident QOL (Chaudhury et al., 2018; Day et al., 2000). These environmental transformations are generally thought to enhance residents’ experience with the physical aspect of the living environment such as comfort, convenience, safety, and privacy. Our findings further indicated that a non-institutional and homelike environment also had some psychosocial impact as they enhance residents’ perception of autonomy. Prior studies provided a potential explanation for this as they pointed out that a more homelike environment helps engage residents in daily activities and social interaction (Campo & Chaudhury, 2012; Milke et al., 2009; Morgan-Brown et al., 2013; Smit et al., 2012).
Our study also examined multiple domains of family satisfaction that may be associated with culture change practices, considering family members can also provide unique and valuable perspectives regarding the quality of NH care. Three culture change domains, including staff empowerment, staff leadership, and end-of-life care, were positively associated with family satisfaction with food, and physical environment transformation was associated with family satisfaction with the environment. We found no significant relationships of the caregiving and staff domains of family satisfaction with any domains of culture change practices. While family members can directly perceive culture change in the areas of the physical environment, food services and daily routine care without deep involvement and are readily satisfied with those overt aspects of services, satisfaction with caregiving and the relationship with the staff will require deeper interaction and engagement from both the family members and care providers (Gladstone et al., 2006; Zimmerman et al., 2012).
The Moderating Role of Small-Home or Household Models
Promoting staff empowerment largely contributed to improved outcomes (i.e., meaningful activities, dignity, autonomy, caregiving, and family satisfaction with food) for NHs maintaining the traditional architectural structure, but it resulted in unchanged or declined quality outcomes for NHs implementing small-home or household models. This finding contradicted our hypothesis. The unexpected negative interaction may be due to the small sample size of small-home or household NH, which could result in insufficient statistical power to examine the actual interplay among the implementation of small-home or household models, various culture change practices, and quality outcomes related to QOL and family satisfaction. Additionally, the binary measure of small-home or household models was limited as it only captures architectural features. However, those unmeasured features, such as organizational and operational adaptation to the implementation of s small-home or household models likely confounded our analyses. Another possible explanation may be potential challenges in effectively implementing staff empowerment strategies in small-home or household homes. Previous studies indicated NHs implementing small-home or household models strived to fit in staff to both the physical renovations and the accompanying organizational restructuring (Bowers & Nolet, 2011; Shield et al., 2014). As noted by CNAs in the Green House homes, working in a small-scale home requires a wide range of new skills such as sophisticated interpersonal abilities, time-management skills, and ability to manage complexity, skills that most of them had not developed before transitioning to the new model (Bowers & Nolet, 2011). Consequently, challenges to adapt to the new care model might negatively influence the provision of high-quality care. More qualitative research with data source triangulation, such as field observation, in-depth interviews and focus groups with CNAs and other stakeholders, is needed to understand direct care staff’s responses to empowerment strategies and their adaptation to a new care model.
Limitations and Directions for Future Research
Some limitations of this study should be noted. First, the low response rate and potential nonresponse bias may bias the results and limit the generalizability of studying findings. While the two facility characteristics (chain affiliation and CNA staffing) associated with nonresponse in this study has not been reported as predictors of resident QOL in prior studies (Shippee, Henning-Smith, et al., 2015; Shippee, Hong, et al., 2015) and thus may have a minor impact on the parameter estimation, unobservable nonresponse bias suggests the need for caution in interpreting the results. The application of weight adjustment may increase the generalizability of the findings to all NHs in Minnesota. Yet, the findings could not be generalized to all NHs in the US and Veterans Affairs (VA) NHs. Second, the small sample size could reduce statistical power to investigate the complex interplay among various culture change domains and quality outcomes using structural equation modeling. Although this study provides a preliminary examination of domain-specific relationships of culture change practices with resident QOL and family satisfaction, a further examination of the complexity of culture change implementation and its impact on care provision will help build the theoretical base of NH culture change, an area of research that is still underdeveloped.
Moreover, the use of facility-level quality outcomes in our study may be subject to aggregation bias. Given insufficient statistical power caused by potential aggregation bias plus the small sample size, caution is particularly needed when interpreting the negative results as they could be false negative. It is also needed to note that the results based on facility-level analyses could not be inferred to individual residents. This is particularly relevant considering that residents from one facility may reside in care units with different levels of culture change implementation. In measuring the status of the small-home or household implementation, we asked the proportion of residents living in small-home or household care units and replicated our regression analyses excluding NHs where less than 75% of residents residing in small-home or household units from the sample of small-homes or household homes (results were consistent with the initial analyses). However, we were not able to evaluate to what extent culture change practices of various domains differ across care units. In this regard, an examination at the levels of care unit and individual resident is useful to discern how culture change occurring in a resident’s immediate surroundings impacts his or her QOL. Finally, the cross-sectional data did not allow us to establish causal relationships among culture change practices and quality outcomes. While an experimental design with randomization is ideal, a quasi-experimental study with concurrent comparison groups and repeated measures of both culture change practices and self-reported quality outcomes is more feasible in NH settings and should be considered when examining the causal effects of culture change interventions.
Implications for Practice
Despite the limitations, the findings from the present study provide some practical implications for designing and implementing NH culture change practices that best benefit resident QOL and improve family satisfaction. Given the extensive impact on improving resident QOL, culture change in workplace practices that promotes staff empowerment and fosters staff leadership should be emphasized and prioritized in culture change implementation, especially for NHs that are incapable of remodeling the architectural structure. Although building small-homes or households may not be feasible for all NHs, the beneficial effects of minor and manageable physical environment transformation on resident psychosocial well-being support NHs’ strategic plans on eliminating the institutional features of the NH environment and creating a home-like atmosphere. Resident-and-family-centered values embedded in day-to-day care should also be extended to end-of-life care, a vital aspect of NH care, to enhance residents’ perception of living a purposeful and meaningful life. Moving beyond fulfilling those essential needs such as food enjoyment, satisfaction with the environment, and autonomy, NHs should continue to explore culture change initiatives that address comprehensive psychosocial needs of both residents and family members. Those initiatives need to work towards fostering meaningful interpersonal relationships among residents, family, and staff, and nurturing personal growth.
Conclusions
This study examined the domain-specific relationships of culture change domains with resident QOL and family satisfaction. The findings revealed that culture change practices in the physical environment, staff empowerment, staff leadership, and end-of-life care were positively associated with at least one specific domain of resident QOL and family satisfaction, with staff empowerment having the most extensive benefits on resident QOL. Implementing small-home and household models had a buffering effect on the positive relationships between staff empowerment and the outcomes. The findings provided meaningful implications for designing and implementing NH culture change practices that best benefit resident QOL and improve family satisfaction.
Footnotes
Acknowledgments
The authors would like to thank all nursing home administrators for participating in the survey, Teresa M. Lewis from Minnesota Department of Human Services for her assistance in the data collection, Margot Schwartz and Dr. Susan C. Miller from Brown University for their instructions on the use of the culture change assessment tool.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.