
Abstract
This study validated a Swedish translation of the Aging Semantic Differential Scale (ASD, 32-items) distributed online. Translation and back-translation were conducted. A convenience sample of nursing students completed the online questionnaire (N = 292) in spring 2020. Confirmatory factor analysis tested a validated four-factor structure consisting of 26 items, and the reliability and validity of the scale were tested. The Swedish version of the ASD was found to be reliable and valid. Model fit indices, internal reliability, and scale validity were acceptable. Construct validity was verified, and mean differences were observed, in accord with previous research regarding participants’ age, sex, clinical experience, and personal relationships with older individuals. The findings provide cross-cultural validation of the ASD by extending its international use. The validation of an online version expands data collection flexibility. As this modified instrument required only 26 items, it may be beneficial for use in future studies and practical settings.
Introduction
Globally, the proportion of older people is predicted to continue to increase over time. The World Health Organization (WHO) estimates that there is currently a population of 125 million people aged 80 years and older, and, by 2050, this age group is predicted to include 434 million people (World Health Organization, 2015). Similar age-distribution proportions are currently also observed in Sweden (Statistics Sweden, 2020a, 2020b). Older people are often assumed to be dependent and a burden to society (Ayalon, 2019), exemplified in current public discourse surrounding the Covid-19 pandemic, with older individuals being blamed for societal restrictions by some individuals (Fraser et al., 2020).
Negative perceptions toward older individuals can translate into ageism and negative behaviors (Burnes et al., 2019), and there are several relationships between ageist perceptions and negative health outcomes affecting older people (Chang et al., 2020). For example, negative perceptions among health care providers such as nurses and physicians can result in reduced patient involvement in treatment and care (Chang et al., 2020). A study in Sweden of more than 34 000 patients revealed that high patient age was correlated with subjectively-rated poor health care experiences (Wolf et al., 2012). A priority area highlighted by the WHO (2017) is combatting negative perceptions toward older individuals. By assessing perceptions toward older people, it may be possible to develop educational interventions targeting specific populations or domains of perceptions, and, in turn, reduce ageism (Burnes et al., 2019; Gallo, 2019).
Aging Semantic Differential
The Aging Semantic Differential (ASD) is one of the most widely used instruments for assessing perceptions toward older people (Ayalon et al., 2019). The scale was originally developed in 1969 to estimate individuals’ perceptions toward older individuals (Rosencranz & McNevin, 1969). Unlike a Likert scale measuring agreement and disagreement, in semantic scales, an adjective is paired with its antonym and two opposite adjectives are assigned numbers on a scale (Tullis & Albert, 2008). The original instrument contains 32 bipolar adjectives and their antonyms, which participants rate on a scale from 1 to 7. For example, one of the paired adjectives in the ASD is the item “Generous—Selfish.” Participants report, via a 7-point scale, on which pole of generous or selfish they generally perceive people over 80 to be. A summary score between 32 and 224 can thus be produced. Lower scores indicate more positive perceptions.
The original version of the ASD had a three-factor structure (Rosencranz & McNevin, 1969). However, attempts to verify the original three-factor model were unsuccessful (Gonzales et al., 2010; Holtzman et al., 1979; Underwood et al., 1985). Instead, a four-factor structure, containing 28 items, was successfully verified (Holtzman et al., 1979). Versions of the scale in English and German using a modified four-factor structure with 26 items were later validated (Gluth et al., 2010; Intrieri et al., 1995).
The first factor pertains to perceptions about older individuals’ autonomy and independence (Autonomy). The second factor entails perceptions regarding older individuals’ health, vitality, and activity (Instrumentality). The third factor captures perceptions about older individuals’ friendliness and engagement in social situations (Acceptability). The fourth factor pertains to older individuals’ optimism and life satisfaction (Integrity) (Intrieri et al., 1995; Rosencranz & McNevin, 1969).
There are currently no published translations or validations of the ASD in Swedish. Most Swedish studies of perceptions toward older people have used the Kogan’s Attitudes toward Older People Scale (KOAP) (Engström & Fagerberg, 2011; Runkawatt et al., 2013; Söderhamn et al., 2001). A comparison between the KOAP and ASD reported that the ASD was more psychometrically robust (Iwasaki & Jones, 2008). In addition, a recent systematic review reported that most ageism scale validation studies have been conducted in English-speaking countries, highlighting the need for cross-cultural validation (Ayalon et al., 2019). Besides English, the ASD has previously only been validated in German and Mandarin-Chinese (Gluth et al., 2010; Gonzales et al., 2010, 2017).
In addition, to the best of our knowledge, previously published ASD validation studies have all distributed the instrument as a paper-based questionnaire (Ayalon et al., 2019; Gluth et al., 2010; Gonzales et al., 2010, 2017). Internet-based survey methods are useful for facilitating larger scale studies by simplifying data collection and data transfer. Thus, psychometrically validating online versions of established scales is an important task (Evans & Mathur, 2018).
For the ASD, there is no consensus regarding whether older individuals should be viewed as a group, or if age ranges should be applied. Rosencranz and McNevin’s original study (1969) used three age ranges (20–30, 40–55, and 70–85 years) as did a study by Gekoski et al. (1991) (mid-20s, mid-40s, or early 70s). However, other studies have used a general construct of “old persons” (Gluth et al., 2010; Intrieri et al., 1995; Underwood et al., 1985).
We focused on individuals aged 80 years and older, because current research has revealed age group differences in experiences of ageist stereotypes among adults over 50 years old (Giasson et al., 2017). For example, research show that some people in the “fourth age” (80+ years) face societal stereotypes from those in the “third age” (people 60–79 years old) (Kydd & Fleming, 2017).
Thus, the aim of the current study was to validate a Swedish translation of the ASD distributed online, to examine perceptions about people aged 80 years and older.
Research Design
Data Collection and Sampling
Data were collected between February-June 2020, using an online questionnaire distributed to all enrolled Bachelor’s and Master’s level nursing students at the University of Gothenburg, Sweden.
A convenience sample of students was recruited by course leaders and lecturers who invited voluntary participation in the research project via the completion of the questionnaire during the courses. The responsible lecturers informed the students about the study verbally and in writing during the course introduction.
The intention was to enable all enrolled nursing students in spring 2020 to participate in the study. For Bachelor’s level students, this included semesters 1–6, and for Master’s level student’s, semesters 1–3 were included. For each semester, a specific course was chosen to target individual students and the questionnaire was distributed via the course’s online platform.
Measurements
A study-specific questionnaire was created, consisting of the ASD with all 32 items and background variables. The questionnaire was created using Microsoft Forms©, which was familiar to students because it was also used for course evaluations.
Background Information
The questionnaire contained demographic questions regarding participants’ age (in years), sex (male, female, other, do not want to disclose), and study level (which semester they were currently enrolled in and whether they were enrolled at the BSc or MSc level).
The questionnaire also included questions about participants’ experiences of caring for persons 80 years and older (yes/no) and having family or relatives 80 years and older (yes/no). If participants did have family/relatives that were 80 years and older, they were asked to rate how much they felt they could share with them (1 = all personal matters, 6 = no personal matters). Participants were asked whether they had heard the concept “ageism” before (yes/no).
Translation of the ASD
We translated the 32-item ASD from English to Swedish. See Supplementary file 1 for the original 32 items and the Swedish translation. We first conducted a forward translation by having a panel of multilingual nursing researchers and lecturers translate the items to Swedish. We then conducted a back-translation using a native speaker of English who also spoke Swedish, to independently translate the Swedish items back, verifying the initial translation. The focus of the translations was on the conceptual equivalent of the items (adjectives). We assessed face validity by piloting the questionnaires with nine nursing students in their first semester. The results indicated that the translation was comprehensible, and no changes were made.
Ethical Considerations
The study plan was submitted to the Swedish Ethical Review Authority. However, the study did not fall under the scope of the Ethical Review Act and thus a full application and ethical review was not required (registration ID nr: 2019-06152). Oral and written information was given to the study participants, and submission of the online questionnaires was considered to constitute consent. The participating researchers also took part in inviting students to participate in the study. This might have consciously or unconsciously influenced the recruitment procedure. We tried to mitigate potential impact by providing information about the study and participation in a systematic way to all students. This was done using a standardized power point presentation for the oral presentation and a template for the written information. All responses were anonymous, and the server did not register the IP addresses or link responses to the user accounts on the student platform. Because of anonymity, students could not withdraw from the study after submitting their data.
Data Analyses
Descriptive and inferential data analyses were performed using IBM SPSS Statistics (v.26) and SAS (v.9.4). P-values lower than 0.05 were considered statistically significant.
Confirmatory Factor Analysis
Confirmatory factor analysis (CFA) is an established procedure for identifying relationships between latent and observed variables in theory-derived models (Harrington, 2009). CFA was thus conducted to test whether the previously developed four-factor structure of the ASD (Gluth et al., 2010) was valid and reliable in this sample. This model was chosen as it only uses 26 items (unlike the original 32), and short scales and brevity in constructs are beneficial for achieving greater parsimony and increased response rates (Netemeyer et al., 2003). In addition, the current study was conducted in collaboration with an Austrian research team, who used the German four-factor model for their validation study.
As suggested by West et al., (1995), we used maximum likelihood estimation because the data did not show any significant tendency for non-normality, as shown in Table 2. Values of multiple indices of goodness-of-fit were computed and used for model evaluation: χ2, goodness-of-fit-index (GFI values of > 0.90), root mean square error of approximation (RMSEA < 0.10), and standardized root mean square residual (SRMR < 0.08) (Hu & Bentler, 1999). Low chi-values are preferred (no established value ranges), but because the χ2 value is strongly affected by sample size, normed χ2 (NC) values were also calculated by dividing the χ2 values by degrees of freedom. An NC value of less than 5 is considered acceptable (Schumacker & Lomax, 2004).
Internal Reliability
Internal reliability was investigated in terms of Cronbach’s α. For instruments of typical length, Cronbach’s α ≥.9 is usually regarded as excellent, ≥.8 as good, and ≥.7 as acceptable (Butts & Michels, 2006). We also assessed item convergent and discriminant validity. Convergent validity implies that items are correlated with their own scales, and correlations should ideally be above 0.5, while discriminant validity implies that items are correlated with other scales, which ideally should be below 0.85 (Kline, 2011). Evidence of convergent and discriminant validity is best interpreted relative to each other (Kline, 2011). Thus, a composite measure of discriminant and convergent validity was also calculated, i.e. “scaling success.” If the correlation between an item and its own scale were significantly larger than the correlation coefficients between that item and another scale, then a “scaling success” was concluded.
We also analyzed item distribution scores to assess whether individual items exhibited signs of skewness, kurtosis, and ceiling/floor effects. Cut-off values were set at: kurtosis <7.00, skewness <2.00, ceiling and floor effects; if more than 15% of respondents rated the lowest (=1) or highest (=7) possible score, respectively (McHorney & Tarlov, 1995; West et al., 1995).
Construct Validity
Construct validity refers to the extent to which scores on a scale relate to other measures in a way that is consistent with theoretically derived assumptions. For comparing mean differences between groups, Fisher’s non-parametric permutation test was used for continuous variables. We tested mean differences between younger and older participants (≤25, >25), females and males, participants with previous experience with care of older people (yes/no), MSc vs BSc level students, as these aspects have previously been shown to influence perceptions toward older people (Engström & Fagerberg, 2011; Runkawatt et al., 2013; Söderhamn et al., 2001).
Results
Of 859 students registered in courses examined for data collection, 292 surveys were submitted (34%). The median time to complete the survey was 4 minutes. Missing values per ASD-item ranged from 1 to 6 (0.3%–2%).
Sample Characteristics
The students’ ages ranged from 18 to 61 years (mean = 29.1; standard deviation = 8.5), 67% of students were 30 years old or younger. Of participants, 244 (85%) were female and 42 (15%) were male. There were 222 (77%) BSc level nursing students and 67 (23%) MSc level students.
Factor Structure
The four-factor structure with 26 items showed acceptable model fit (χ2 = 784.90; df = 293; NC = 2.83; p-value = 0.001; GFI = 0.92; NNFI = 0.82; SRMR = 0.07; RMSEA = 0.07). See Figure 1.
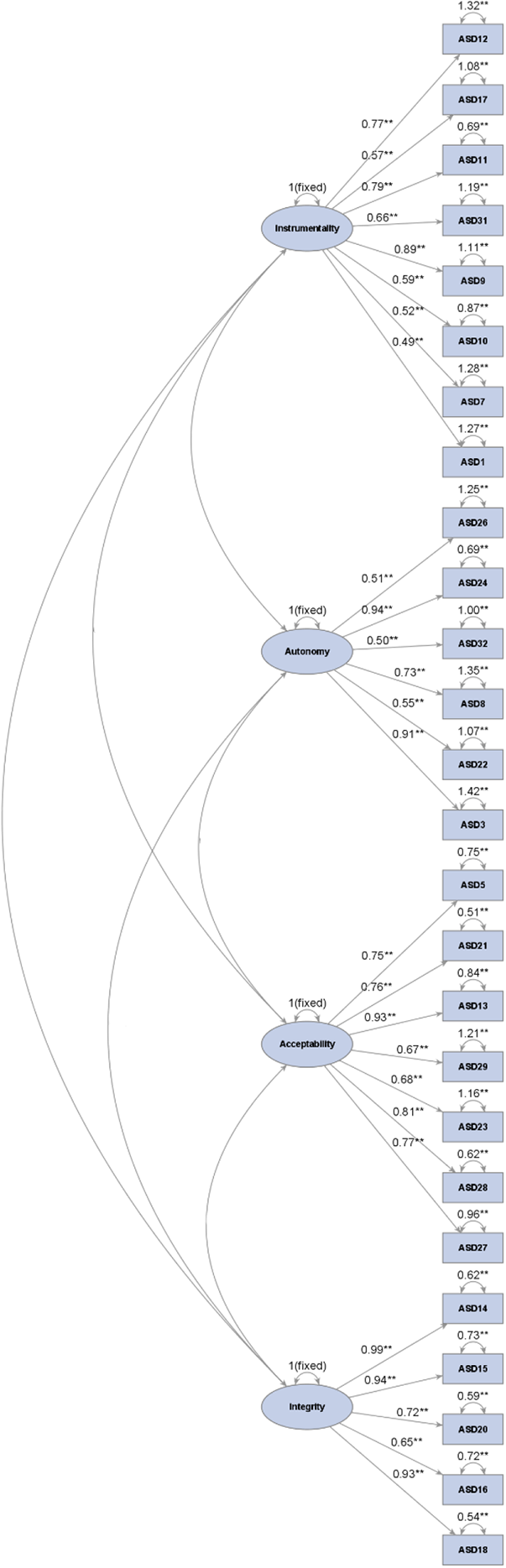
Factor structure of the Swedish ASD (26 items).
Internal Reliability
We assessed scale reliability and item convergent and discriminant validity. Scaling was successful and all Cronbach’s α scores were acceptable.
Several items showed weak correlations with their own scales indicating unsatisfactory convergent validity. All item correlations with other scales were lower than 0.85 indicated good discriminant validity. Item correlations with their own scales were consistently higher than item correlations with other scales, as indicated by high proportions of scaling successes (83%−100%). Taken together, these findings indicated acceptable scale validity for the instrument (Table 1).
Internal Reliability and Scale Validity.
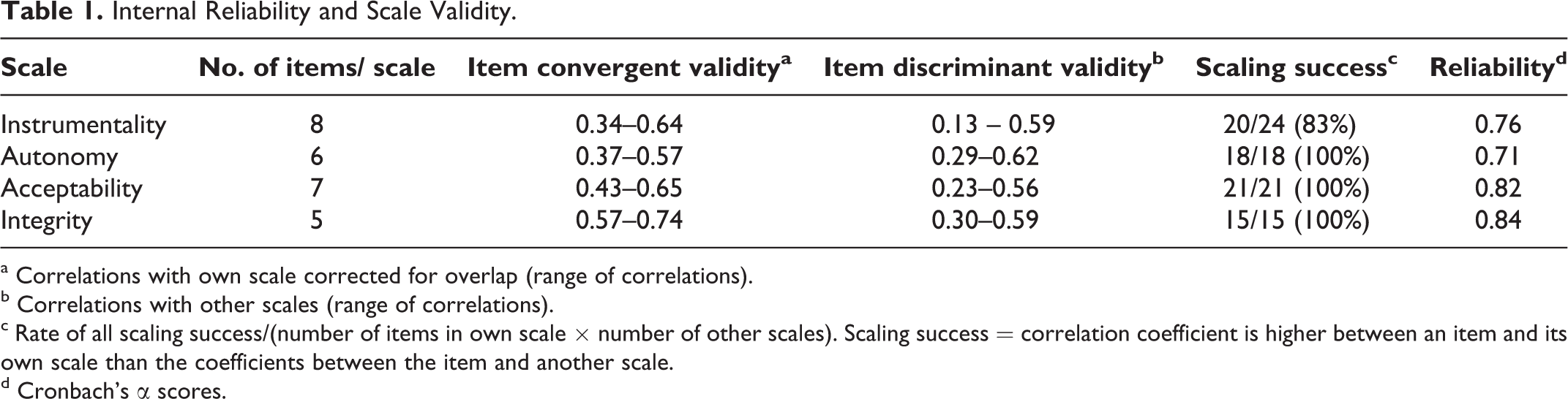
a Correlations with own scale corrected for overlap (range of correlations).
b Correlations with other scales (range of correlations).
c Rate of all scaling success/(number of items in own scale × number of other scales). Scaling success = correlation coefficient is higher between an item and its own scale than the coefficients between the item and another scale.
d Cronbach’s α scores.
Item Score Distributions
Parameters related to item score distributions are presented in Table 2. Lowest mean scores (more positive perceptions) were as follows: ASD21 (Friendly-Unfriendly), ASD29 (Ordinary-Eccentric), and ASD12 (Handsome-Ugly). Highest mean scores (more negative perceptions) were: ASD7 (Busy-Idle), ASD17 (Flexible-Inflexible), and ASD18 (Hopeful-Dejected).
Item Distribution Scores for the Validated Four-Factor Structure (26 Items).
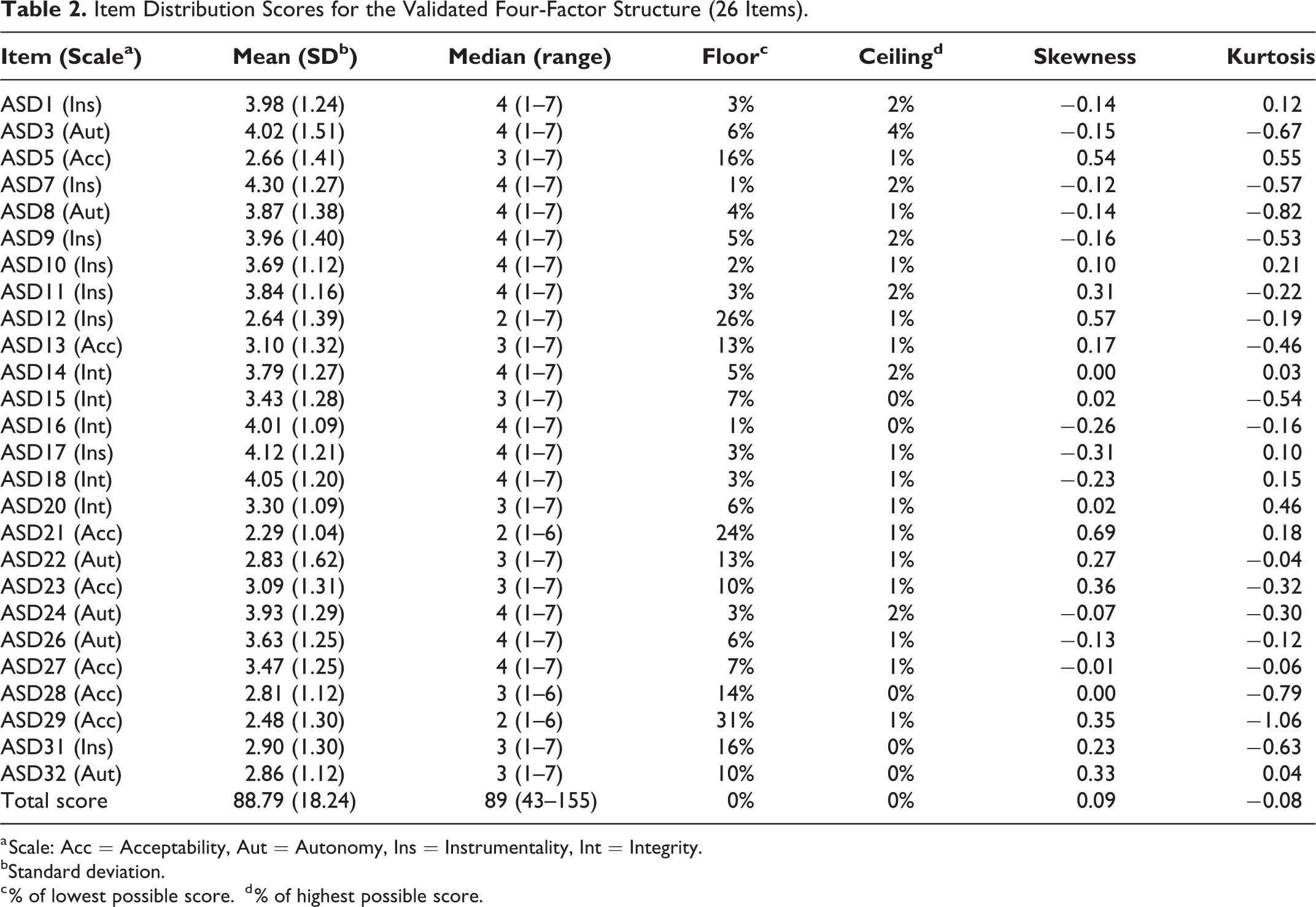
a Scale: Acc = Acceptability, Aut = Autonomy, Ins = Instrumentality, Int = Integrity.
bStandard deviation.
c % of lowest possible score.
d % of highest possible score.
Skewness and kurtosis were acceptable. Unlike the summary score, there was evidence of a slight floor effect (items: ASD5, ASD12, ASD21, ASD29, and ASD31).
Construct Validity
By testing mean differences between subgroups for the four identified scales (instrumentality, autonomy, acceptability, and integrity) we found trends that were consistent with previous studies, indicating that younger participants, females, participants with previous experience caring for older people, MSc level students, and participants with a personal relationship with an older person, generally exhibited lower ratings (i.e., more positive perceptions). However, several differences were not statistically significant. Table 3. We did not observe any consistent trends in mean differences for the variable familiarity with the concept of ageism.
Mean Differences Between Subgroups (Age, Sex, Previous Experience Caring for An Older Person, Education Level, and Personal Relationship With an Older Person).
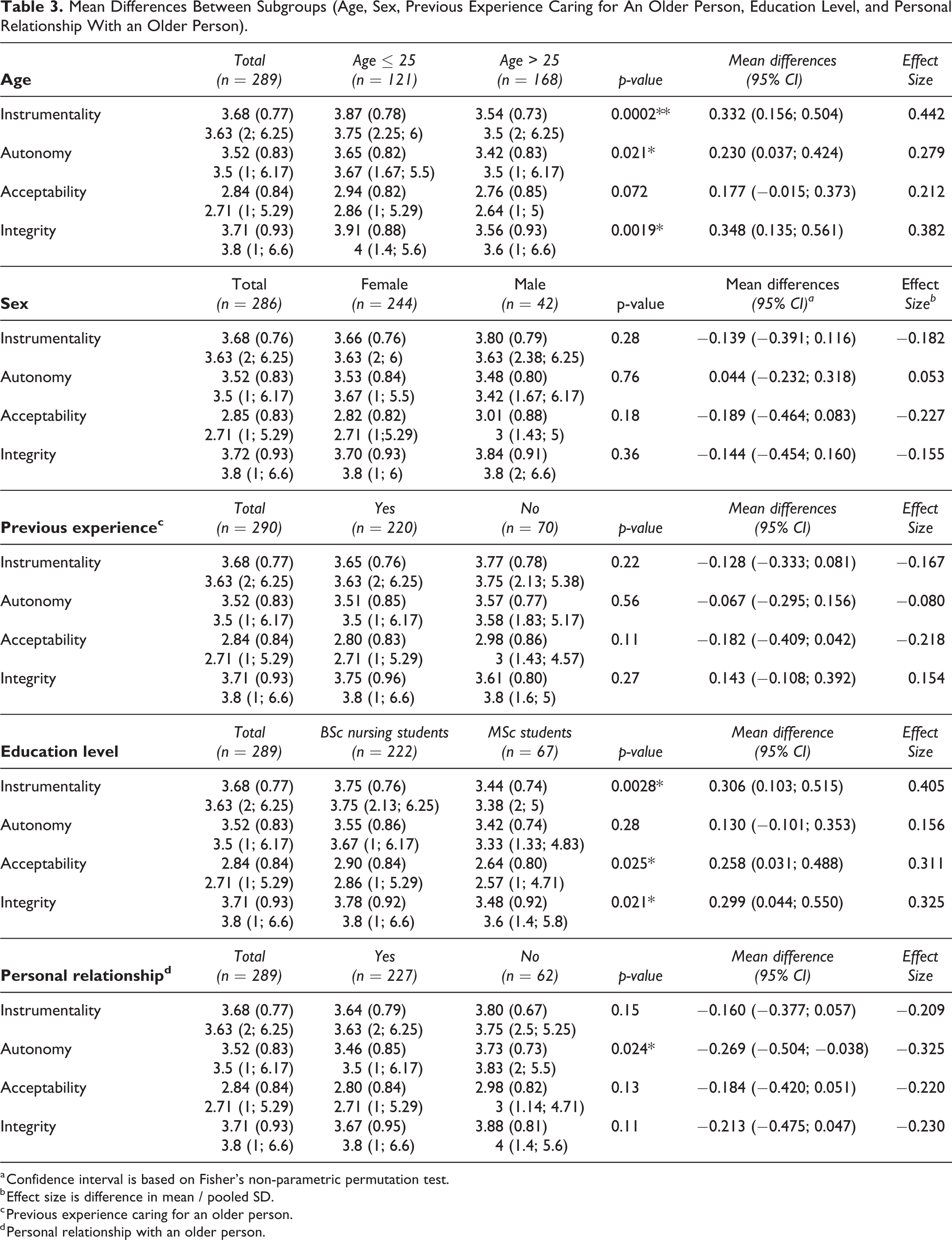
a Confidence interval is based on Fisher’s non-parametric permutation test.
b Effect size is difference in mean / pooled SD.
c Previous experience caring for an older person.
d Personal relationship with an older person.
Discussion
This study aimed to validate a Swedish translation of the ASD scale. We tested our model against a previously reported four-factor model and obtained an acceptable model fit. The Swedish ASD also exhibited acceptable internal reliability, scale validity, and construct validity.
The current study furthers the international development of the ASD by translating it into Swedish. To the best of our knowledge, this is the first time the ASD has been validated in a Scandinavian country. Our findings further corroborated the modified four-factor model of ASD, which used 26 items instead of the original 32 items. This finding is important because short instruments and concise constructs are preferable, imposing less of a burden on respondents and potentially increasing response rates (Netemeyer et al., 2003). As such, the current study contributes by offering cross-cultural validation of the use of a shorter version of the ASD which could be evaluated and used by researchers and practitioners in other disciplines besides nursing.
In accord with previous studies, we found that age, sex, educational qualifications, previous experience of caring for older patients, and personal contact with older people influenced participants’ perceptions toward older individuals (Ridgway et al., 2018). The finding that the age variable showed the most evident mean differences in terms of statistical significance and effect size further suggests that age might be the one of the most consistent demographic variable to predict ageist attitudes, as observed in previous studies (Ridgway et al., 2018; Runkawatt et al., 2013). This reinforces the importance of considering age as a variable to assess construct validity in ageism questionnaires.
No consistent tendencies in mean differences were observed for familiarity with the concept of ageism. This finding was expected because this variable has less support in previous literature compared with age and sex. This finding indicate that this question might not be useful for testing the construct validity of the ASD.
The current study contributes by validating the ASD using a sample including both undergraduate and graduate nursing students, of which many had clinical experience. Previous ASD validation studies have examined medical students (Gonzales et al., 2010; Intrieri et al., 1995), general public samples (Gluth et al., 2010), students not otherwise specified (Gonzales et al., 2017; Iwasaki & Jones, 2008; Rosencranz & McNevin, 1969), and pre-nursing students (Underwood et al., 1985). Thus, the current study demonstrated that the ASD was valid among BSc and MSc level nursing students with and without clinical experience. This finding has important implications because nurses make up a significant proportion of the healthcare sector, which many older people are in contact with. A recent systematic review, including more than 7 million participants, reported that ageist perceptions from health care providers can result in reduced access to health services and a negative influence on care, resulting in negative health outcomes (Chang et al., 2020). Thus, it is important to assess nurses’ perceptions toward older people and potentially work to change their perceptions if negative attitudes are found to be prevalent. This validation study suggests that the ASD can be used in this regard.
Implications
This validation study has several implications for researchers and practitioners in education and healthcare.
Successful validation of the ASD in a Swedish context implies that the instrument might have further international applications. The ASD has now been validated into English, German, and Mandarin-Chinese using different student groups and members of the general public. As such, the current findings suggest that the instrument can assist educators in a range of cultural contexts targeting students of various educational profiles. By assessing perceptions, it is possible to develop educational interventions targeting domains of perceptions. This validated four-factor structure consists of autonomy, instrumentality, acceptability, and integrity. In our sample, integrity had the highest mean scores, whereas acceptability had the lowest scores. This finding indicates that students generally perceived older individuals as somewhat dissatisfied and resigned, while also perceiving them as friendly and generous. This information could thus be used in education to further probe students about these experiences (e.g., to determine whether the perception stems from clinical experiences) and educate students about how they can address these aspects with patients in their professional roles as nurses.
Validation of a four-factor structure requiring only 26 items represents positive progress in terms of the scale’s usability and implications. The median time to complete the study questionnaires was only 4 minutes, indicating that this instrument can be implemented relatively quickly for assessing perceptions toward older individuals. Validation of an Internet-distributed version of the questionnaire provides further flexibility regarding how the ASD can be distributed, making distribution of the questionnaire in classroom and clinical settings feasible. For example, educators could use an online version of the scale to assess students’ attitudes before course enrollment and modify or highlight certain aspects of training in accord with the students’ results. This approach could make the pedagogy more interactive and student oriented. Moreover, in education, as in other sectors, there is a preference for climate-friendly and sustainable solutions, such as using electronic rather than paper-based questionnaires. While digital surveys may be used with improved speed and efficacy of data collection compared with paper or verbal survey modalities, limitations such as low response rates and variations in computer literacy and internet access remain areas of concern (Evans & Mathur, 2018). In our study, participating students had access to computers at university halls and university libraries, which is something to bear in mind and inform students about. An important aspect which we also considered, was the significance of an extra reminder. We posted extra general reminders on the course platforms. Extra reminders have been linked to increased response rates and thereby increased likelihoods of generating a representative sample (Mol, 2017). However, we opted for total anonymity since we used students from our own university, which eliminated the possibility for personalized reminders.
Strength and Limitations
One limitation of the current study is related to the current sample, which contained unequally sized subgroups that may have made it challenging to test the statistical significance of differences, such as those between males and females. These subgroup size differences might explain why few mean differences were statistically significant. Another limitation of the current study was the use of convenience sampling, potentially limiting the generalizability of the results due to unforeseen systematic biases. For example, response biases related to participants’ Internet access cannot be ruled out. This might have affected response rates. Although not all previous ASD validation studies provide response rates, some studies using paper-based instruments have reported significantly higher response rates than that in the current study (Gonzales et al., 2017). However, we believe that using an online questionnaire had advantages, allowing students to choose when and where to complete the questionnaire, which may help facilitate participants’ anonymity. Also, by selecting one course per semester for study recruitment, we intended to enable all currently enrolled nursing students to participate. The majority of students complete the semester, and many students are enrolled in several courses simultaneously since they might not complete their courses completely before moving to the next course. Also, courses are not usually archived on the student platform before the start of a new semester, allowing students digital access to the courses throughout a semester. These aspects speak to the likelihood that most students were able to participate in the current study. However, there is a small risk that students that were only registered in certain courses (i.e., that for various reasons did not complete/continue a full semester) were not invited. Nevertheless, we did not get any indications that we systematically missed eligible students.
For the ASD to function effectively, it must be assumed that individuals associate similar connotations with the adjectives, and a challenging aspect of semantic differential techniques is coming up with words that are truly opposites (Tullis & Albert, 2008). In the current study, we observed little evidence of data skewness or kurtosis, indicating that we identified relevant wording that measured opposites in a way that was consistent among participants. Nonetheless, updating the instrument with current adjectives with contemporaneous meanings might contribute by making the scale more relevant. As such, exploratory factor analyses, as well as qualitative approaches, might help reveal other important domains of ageism in the 21st century for future research.
Another limitation of this and previous ASD validation studies was the absence of a standardized definition and use of “older people” across studies that is reliable and valid across cultural and sociolinguistic contexts, samples, and time periods. Because of these methodological variations, it is difficult to compare results across studies. As noted by Gonzales et al. (2017) and Intrieri et al. (1995), the ASD assesses perceptions toward older individuals, and each version of the ASD possesses reliability and validity in its corresponding sociocultural context.
Lastly, while scale validity was acceptable in terms of discriminant validity and internal consistency, convergent validity was generally low. Many items showed weaker correlations than the recommended 0.5 with their own scales. Although convergent validity is best interpreted relative to discriminant validity (proportion of “scaling successes,” which were high in this study), it would have been useful to assess correlations with other related and unrelated questionnaires. Doing so would allow us to get a broader idea of the range of correlations, and thus a more complete picture of the instrument’s internal and external validity.
Conclusions
We extended the international use of the ASD by translating it into Swedish, validating the scale in a Scandinavian country for the first time, and providing cross-cultural validation of a four-factor structure with a reduced number of items compared with the original instrument.
Researchers and practitioners can utilize this instrument to assess perceptions toward older individuals in Sweden. Use of this scale may aid current understanding of perceptions of older individuals and help to inform interventions. This validation of an online version of the scale provides flexibility for researchers depending on their data collection needs and preferences.
Considering the global attention and importance of assessing perception toward older individuals, future studies should test whether a universal ASD instrument can be developed. An international instrument can enable cross-cultural research and provide a deeper understanding of perception toward older individuals in an increasingly globalized and aging world. Using current validated versions of English, German, and Mandarin-Chinese ASD instruments (Gluth et al., 2010; Gonzales et al., 2010, 2017), together with qualitative methods, it may be possible to assess many types of validity and reliability.
Supplemental Material
Supplementary_file - Classic Tool, New Opportunities: A Psychometric Analysis of a Swedish Online Version of the Aging Semantic Differential Scale
Supplementary_file for Classic Tool, New Opportunities: A Psychometric Analysis of a Swedish Online Version of the Aging Semantic Differential Scale by Christopher Holmberg, Axel Wolf, Camilla Eide, Franziska Großschädl, Gerhilde Schüttengruber, Harshida Patel and Birgit Heckemann in Research on Aging
Footnotes
Acknowledgments
Dr Joanne Fuller helped in backtranslation. Dr Helene Berglund and Dr Petra Brembeck helped with data collection. Mr. Brian Knight helped in editing the manuscript.
Author Contributions
CH, AW, CE, FG, GS, and BH contributed to the conception and design of the study. CH, AW, CE, and HP contributed to data acquisition. CH, AW, FG, GS, and BH contributed to the analysis and interpretation of data for the work. All authors contributed to drafting the work and approved of the version to be submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study plan was submitted to the local ethical review board. However, the study did not fall under the scope of the Ethical Review Act and thus a full application and ethical review was not required. (registration ID nr: 2019-06152). Oral and written information was given the study participants and submitting the online questionnaires was considered as their consent. Responses were anonymous and the server did not register the IP addresses nor did it link with user accounts on the student platform. Because of the anonymity, students could not withdraw from the study after their submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.