
Abstract
Older adults are often exposed to elderspeak, a specialized speech register linked with negative outcomes. However, previous research has mainly been conducted in nursing homes without considering multiple contextual conditions. Based on a novel contextually-driven framework, we examined elderspeak in an acute general versus geriatric German hospital setting. Individual-level information such as cognitive impairment (CI) and audio-recorded data from care interactions between 105 older patients (M = 83.2 years; 49% with severe CI) and 34 registered nurses (M = 38.9 years) were assessed. Psycholinguistic analyses were based on manual coding (κ = .85 to κ = .97) and computer-assisted procedures. First, diminutives (61%), collective pronouns (70%), and tag questions (97%) were detected. Second, patients’ functional impairment emerged as an important factor for elderspeak. Our study suggests that functional impairment may be a more salient trigger of stereotype activation than CI and that elderspeak deserves more attention in acute hospital settings.
Keywords
Acutely ill older patients represent a substantial and steadily increasing subgroup of the hospital population in many countries (Mukadam & Sampson, 2011). In Germany, around 45% of inpatients were estimated to be aged 65 years or older of whom 40% had comorbid cognitive impairment (CI; Bickel et al., 2018). Systematic reviews have shown that CI significantly increases the length of hospital stay in older inpatients and the risk of adverse outcomes such as functional decline (Möllers et al., 2019; Mukadam & Sampson, 2011).
In this context, elderspeak has been considered as a crucial factor contributing to neuropsychiatric symptoms (NPS) such as aggression (Herman & Williams, 2009) and finally to poorer treatment outcomes in older inpatients with CI (George et al., 2013). Elderspeak describes a specialized speech register that occurs in intergenerational interactions. Typical markers are the inappropriate use of diminutives, collective pronouns, and tag questions as well as exaggerated prosody, reduced fluency, lower grammatical complexity, and simplified vocabulary (Kemper, 1994; Samuelsson et al., 2013; Schroyen et al., 2018). Despite its potential relevance in the acute hospital setting, the bulk of previous research on elderspeak has been conducted in nursing home settings (Kemper, 1994; Williams, 2006; Williams et al., 2009). In general, only a few studies have dealt with this issue in German populations (Sachweh, 1998).
The current study addresses these gaps by examining elderspeak in two German acute hospital settings. We also strive to add more complexity to previous elderspeak literature by considering different types of elderspeak outcomes and their contextual embeddedness.
Previous Research on Elderspeak
Elderspeak can be seen as a substantial part of views on aging (VoA) research including work on age stereotypes (Kornadt & Rothermund, 2011) as well as ageism research (Chang et al., 2020; Gendron et al., 2016; Schroyen et al., 2018; Voss, Bodner, et al., 2018). A robust finding is that more negative VoA are significantly linked with undesired developmental outcomes such as impaired functional health, lower well-being, and higher mortality (Westerhof et al., 2014). Elderspeak research adds an important facet to VoA work because it concentrates on naturally occurring behavior and offers a high degree of ecological validity (Chang et al., 2020; Samuelsson et al., 2013).
Research from a variety of settings has demonstrated that older adults are often recipients of elderspeak (Kemper, 1994; Kemper et al., 1998; Sachweh, 1998; Samuelsson et al., 2013; Williams et al., 2009). Although elderspeak is mostly seen as a negative speech register, ambiguous findings exist on the consequences of some components of elderspeak (Kemper & Harden, 1999; Lowery, 2013; Schroyen et al., 2018). Importantly, elderspeak should not be confused with the concept of comfort talk, which includes techniques of rapid rapport, patient-centered communication styles, and hypnotic language to reduce patients’ stress, anxiety, and pain (Lang, 2012). Whereas there is robust evidence on the effectiveness of comfort talk (Lang, 2012), results on the effects of elderspeak are more mixed. Therefore, we differentiate between (1) likely harmful and (2) hybrid features of elderspeak incorporating beneficial and harmful aspects depending on contextual characteristics.
In terms of likely harmful features of elderspeak, tag questions, diminutives, and collective pronoun substitution deserve particular attention. First, tag questions such as “right?” (German example: “gell?”) have been described as rhetorical questions to politely push older adults’ answers and behaviors in a desired direction (Herman & Williams, 2009; Kemper, 1994; Williams, Shaw, et al., 2017). Hence, tag questions undermine meaningful conversations and self-determined behaviors of older adults. Second, diminutives refer to the use of intimate forms of address such as first names, nicknames, and terms of endearment as well as oversimplified words and exaggerated praise (Sachweh, 1998; Williams, Shaw, et al., 2017). Diminutives were judged as inappropriate because they suggest an intimate relationship such as between children and parents (Edwards & Noller, 1993; Williams, 2006). Furthermore, diminutives may reinforce power differentials between patients and healthcare professionals inherent in institutional settings (Ryan et al., 2008; Williams, Shaw, et al., 2017). Third, collective pronoun substitutions (CPS) characterize nurses’ use of plural (“we/our”) instead of singular pronouns (“you”/your”) during care activities, which are either performed by the patient or the nurse alone, but not together (Sachweh, 1998; Williams, Shaw, et al., 2017). In line with research on overprotective behaviors toward older adults (Baltes & Wahl, 1992; Ryan et al., 2006) and work on elderspeak (Williams, 2006; Williams, Shaw, et al., 2017), CPS can be considered as patronizing because the autonomy of an older person is ignored.
With respect to hybrid features of elderspeak, simple vocabulary as well as a reduced fluency in terms of a slower speech rate, a reduced sentence length, and more sentence fragments were observed in interactions with older adults when compared to younger adults (Kemper, 1994; Kemper & Harden, 1999; Kemper et al., 1996). Some studies found improvements in sentence comprehension and better recall of medical instructions (Kemper et al., 1995; McGuire et al., 2000), but it was nevertheless judged as patronizing by older adults (Gould et al., 2002). Other work even reported an increase in communication problems (Kemper, 1994; Kemper et al., 1996). Finally, reduced grammatical complexity can be seen as a likely beneficial feature of elderspeak that improved older adults’ communication performance (Kemper & Harden, 1999; Kemper et al., 1996).
A Contextual Approach to Elderspeak
Elderspeak has mostly been embedded into the Communication Predicament of Aging Model (CPA; Ryan et al., 1995). The CPA model assumes an adverse feedback loop based on negative age stereotypes. It puts strong emphasis on disability-related cues of elderspeak receivers at the proximal level such as cognitive and functional deficits. The Age Stereotypes in Interactions Model (ASI; Hummert, 1994) extended the CPA model by addressing contextual characteristics at the distal level, e.g. non-institutional versus institutional environments as well as perceiver’s characteristics such as VoA. Nevertheless, the integrative consideration of multiple contextual conditions at the proximal and distal level has remained limited in previous conceptualizations of elderspeak.
To address this gap, we refer to the conceptual framework for
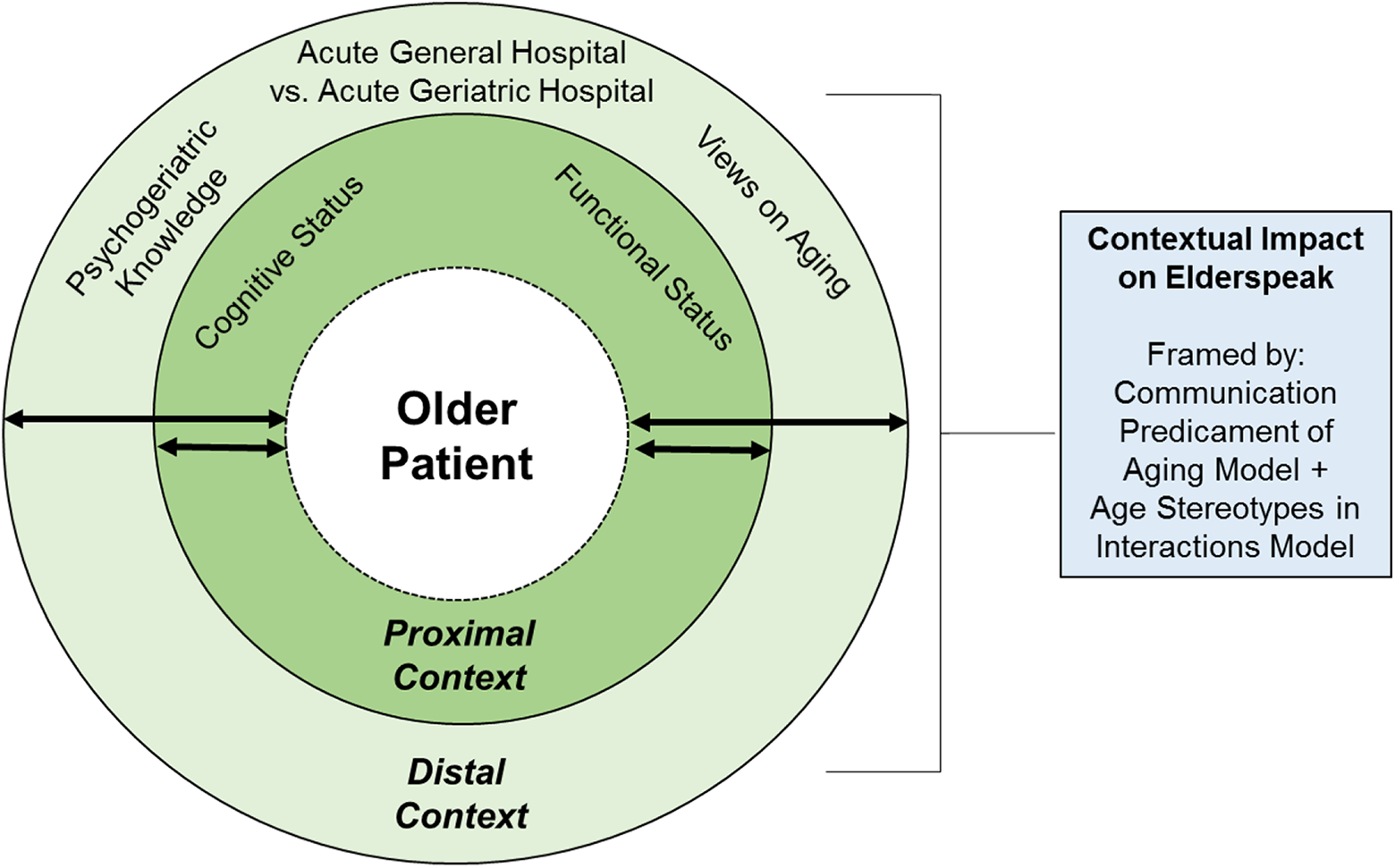
Extended conceptual framework of elderspeak communication integrating parts of the
At the proximal contextual level, we concentrate on everyday care interactions between older patients and nurses in acute hospitals (see Figure 1, inner circle). We consider patients’ cognitive and functional status as two central individual-level variables by which immediate care conditions may be shaped. First, studies indicated that cognitively impaired older adults are more exposed to likely harmful features of elderspeak when compared to cognitively unimpaired older adults (Kemper, 1994; Williams, 2006; Williams et al., 2009). However, inconsistent findings have been reported for most of the hybrid features of elderspeak (Kemper, 1994; Kemper et al., 1998; Williams, 2006). Second, the role of functional impairment as a risk factor of elderspeak has only been considered by a few studies (Caporael & Culbertson, 1986; Lombardi et al., 2014; Sachweh, 1998), although nursing home residents typically require help in basic activities of daily living (ADLs). In our previous study, functional impairment turned out as even more important for explaining likely harmful controlling tones of nurses’ voice toward older patients in the acute hospital setting when compared to CI (Schnabel et al., 2019).
Given previous research on the role of care settings (Baltes & Wahl, 1992), it can be expected that distal contextual factors such as different acute hospital environments, nurses’ psychogeriatric knowledge (Schnabel et al., 2019), and VoA (Schroyen et al., 2018) are also important predictors of elderspeak but produce lower effect sizes when compared to proximal contextual factors. We are to the best of our knowledge the first differentiating between an acute general versus acute geriatric hospital environment (see Figure 1, outer circle). Acute general hospital settings in Germany provide standard care for younger and older patients. Typically, length of stay is limited to a few days (Schnabel et al., 2019). In contrast, acute geriatric hospital settings employ hospital staff who received psychogeriatric training and provide specialized treatment for vulnerable older patients with CI and NPS (Schnabel et al., 2019; Zieschang et al., 2010). Patients of acute geriatric hospital settings usually have a longer length of stay compared to patients of acute general hospital settings due to severe cognitive and functional impairments and the need for early complex geriatric rehabilitation therapy (Kolb et al., 2014; Zieschang et al., 2010).
Objectives and Hypotheses
Our study aimed to examine to what extent nurses use likely harmful as well as hybrid features of elderspeak in the acute hospital setting. At the proximal level of contextual embeddedness of elderspeak, we consider the role of older patients’ cognitive and functional status. We expect lower levels of cognitive and functional status to be significantly associated with a higher use of likely harmful as well as hybrid features of elderspeak (Hypothesis 1).
At the distal level of contextual embeddedness of elderspeak, we predict that acute hospital setting, nurses’ psychogeriatric knowledge and age stereotypes account for significant amounts of explained variance in likely harmful as well as hybrid elderspeak features over and above proximal contextual variables (Hypothesis 2).
In accordance with the CODA model, we expect stronger effect sizes for proximal than distal contextual variables when predicting likely harmful as well as hybrid features of elderspeak (Hypothesis 3).
At the exploratory level, we also examine whether social-contextual features such as time of the day (morning versus evening care) and interaction type (dyadic versus triadic) play a role.
Research Design
Recruitment and Sample
Data collection took place in two academic acute hospitals (n = 114 and 105 beds, respectively) located in a medium-sized southwestern city in Germany. From September 2017 to March 2018, data were gathered within an acute general, internal medicine ward specialized in cardiology, angiology, and pulmonology (n = 36 beds; mean length of stay = 4.9 days) and an acute geriatric ward (n = 35 beds; mean length of stay = 16.5 days). The first author spent 2 months as an intern in both hospitals to analyze the daily routines and to reduce participant reactivity (Herman & Williams, 2009). For detailed information on the study design and recruitment, please see Schnabel et al., 2019.
All patients who were younger than 65 years, terminally ill, isolated, not sufficiently proficient in the German language, or planned for discharge were excluded from the study. According to our research design, patients with severe CI were planned to account for around 50% of the patient sample in both hospital settings. Patients were allocated to the CI group based on the 10/11 cut-off of the 6-Item Cognitive Impairment Test (6CIT; Hessler et al., 2017) showing the best sensitivity-specificity ratio (88% and 95%, respectively). Lower error scores indicate a better cognitive status (possible range: 0–28). A German validation study pointed to its higher sensitivity in the acute hospital setting when compared to medical records (Hessler et al., 2017). Medical records were only used in 10% of cases in which screenings were entirely not feasible due to CI (4/11 with diagnosed dementia).
Patients’ functional impairment was rated by nurses using the Barthel Index (Mahoney & Barthel, 1965). Lower sum scores represent a higher degree of dependency in ADLs (possible range: 0–100). Patients’ perceptions of age discrimination related to the care interaction as well as the hospital stay as a whole were examined by use of a dichotomous (yes/no) single-item (modified from Hudelson et al., 2010).
All registered nurses were eligible for inclusion. Written informed consent was obtained from all participants or the legal representatives of CI patients as well as from all individuals in the audio-recorded rooms. Approximately 27% of the screened patients finally participated in the study leading to the precalculated sample size of 106 patients (49% with CI; for more details, see Schnabel et al., 2019). 34 registered nurses took part in the study.
Following the rule of Williams (2006), one patient was excluded because the interaction was shorter than one minute. Sample characteristics are displayed in Tables S1 and S2 in the Online Supplemental Material. As can be seen in Supplementary Table S1, CI patients were characterized by stronger cognitive, functional, and communication impairments. Besides, patients of the acute geriatric hospital showed a significantly lower functional status, a slower speech rate as well as a longer hospital stay (see Supplementary Table S1). In general, our interview data pointed to low percentages of patients having experienced age discrimination during the care interaction (4%) or the hospital stay (2%). At the social-contextual level, interactions in the geriatric hospital more commonly took place in the bathroom. Furthermore, the number of other patients in the room was higher in the geriatric hospital, whereas the number of nursing aides was higher in the general hospital. As can be seen in Supplementary Table S2, nurses in the geriatric hospital reported better psychogeriatric knowledge of whom 50% were geriatric-trained nurses. The study was approved by the ethics commission of the Faculty of Behavioral and Cultural Studies at Heidelberg University in July 2017 as well as by hospital staff leadership and staff councils.
General Procedure
Our approach was based on three data sources: (a) audio-recordings during the morning or evening care; (b) standardized interviews with the patients and nurses after the observed care interaction; and (c) patient data from the medical information system.
Audio-recordings
The first author took the role of a non-participant observer to gain full control over the audio recording process. PCM digital audio recorders (48 kHz, 16 bits) placed in the patient rooms were immediately activated before the nurse entered the room and stopped as soon as the care was finished in the room. Mostly, there was one morning round in the geriatric hospital, whereas care in the general hospital was divided into two morning rounds. The first round (7.00–8.00 am) served to manage the most essential care tasks such as monitoring vital signs. The second round (9.00–11.00 am) comprised the assistance in ADLs. When possible, both morning rounds were recorded to increase the comparability between both hospital settings. There was only one assessment day for each patient being observed during a maximum of two care encounters (i.e., morning rounds). The majority of nurses were measured on more than 1 day during multiple care encounters (24% once, 47% 2–4 times, 29% 5–6 times).
Standardized interviews
Patients were interviewed by trained students to examine sociodemographic, health-and hospital-related variables (see Supplementary Table S1). Interviewers underwent a communication training conveying evidence-based strategies for interactions with CI patients (Harwood et al., 2012). Further, they were instructed to code doubtful answers as missing. Standardized interviews with nurses were conducted by the first author and focused on nurses’ sociodemographic and professional background, the number of previous care interactions with the patient, and nurses’ perceptions of changes in their own behavior because of being observed (see Supplementary Tables S1 and S2). Nurses’ evaluative age stereotypes in the life domains friends, leisure, lifestyle, and health were operationalized by 8-point bipolar items ranging from a negative to a positive pole (Kornadt & Rothermund, 2011). Values ≤ 4 indicate a tendency toward negative age stereotypes. The internal consistency of subscales was acceptable to good (Cronbach’s α = .76 to .83) in our study. However, the item “physical appearance” had to be removed from its subscale to increase internal consistency (Cronbach’s α > .60). The assessment of nurses’ psychogeriatric knowledge was based on a self-rated single item ranging from 1 (very low) to 5 (very high; Tropea et al., 2017).
Data preparation
Using the software Audacity (Version 2.1.3; https://www.audacityteam.org/), target speakers were identified by the first author. For example, audio-recorded utterances of other patients and nursing aides were qualified as “non-relevant.” Speech pauses longer than one minute as well as time slots where the nurse left the room or interacted with non-relevant individuals were subtracted from interaction times. Following these rules, we roughly divided care interactions (n = 105) into three categories: (a) 0–10 min (56%), (b) 11–20 min (28%), and (c) >20 min (16%). In the case of longer interaction times, the first 5 minutes (category b) or first 10 minutes (category c) were considered as habituation phases with a higher risk of participant reactivity (Williams, 2006; Williams et al., 2009) and excluded from further analyses. This procedure also allowed us to test for potential effects of participant reactivity by examining differences in the occurrence of elderspeak between category a (56%) and categories b/c (44%). Due to a higher number of utterances for categories b/c, relative frequencies were computed. The occurrence of elderspeak features did not significantly differ between categories (all Bonferroni-Holm corrected p values > .05).
In a second step, minimal transcripts were created by four trained students and the first author following the cGAT conventions (Schmidt et al., 2015). Using the FOLK EditoR (FOLKER; Schmidt, 2012), words were transcribed in modified orthography providing full information on typical features of spoken language. Conformance with the cGAT conventions was automatically checked by FOLKER. Additionally, the content of all transcripts was rechecked by the first author.
In a third step, transcripts were segmented into utterances, i.e. maximal syntactic units based on recommendations suggested by Westpfahl et al. (2019). Four types of segments were annotated: (a) simple sentential units, (b) complex sentential units with dependent structures, (c) non-sentential units without a finite verb, and (d) abandoned units with a syntactically and/or pragmatically incomplete structure. We made two minor adjustments to align the German guideline with the English guideline used in previous studies (Kemper et al., 1989). Segmentation was performed by the first author and a linguistic expert. Interrater reliability was determined by the
In a fourth step, nurses’ utterances were manually coded for likely harmful features of elderspeak using the
Measures
Likely harmful features of elderspeak
First, tag questions were coded, which typically occur in the right outer field of an imperative or declarative utterance characterized by a rising intonation (Kemper, 1994; Kemper et al., 1995; Westpfahl et al., 2019). With respect to diminutives, intimate forms of address (first names, nicknames, and terms of endearment) and baby-talk like terms (oversimplified terms, exaggerated praise, and diminutive suffixes) were differentiated. Finally, nurses’ use of CPS was coded as inappropriate for activities, which were independently performed by the patient or the nurse. To avoid ambiguity in the case of plural pronouns referring to several involved nurses, only dyadic care interactions were analyzed (n = 76).
Hybrid features of elderspeak
Two general measures of fluency were extracted via FOLKER: (a) mean length of utterance in words per utterance and (b) speech rate in words per minute. As a more specific measure of fluency, sentence fragments were derived from non-sentential and abandoned units. As a semantic indicator of lexical diversity, type-token ratios (TTR), i.e. the number of different word forms related to the total number of words were calculated using FOLKER. Grammatical complexity was operationalized by complex sentential units.
Data Analyses
Data analyses were performed using IBM SPSS version 25 (Armonk, NY, USA). Due to varying length of interactions (Kemper, 1994; Williams et al., 2009), relative frequencies were computed for descriptive and correlational analyses by dividing the absolute number of annotated features by the total number of nurses’ utterances (M = 129.54, SD = 66.21, range = 25–346). The different types of diminutives were analyzed together given the low mean percentages of intimate forms of address (≤1%). For examining cross-domain associations between the psycholinguistic variables, Spearman’s correlations were computed due to positively skewed distributions and outliers. Two extreme outliers (>3 SDs above the mean) were excluded from further analyses because they may have biased test results (Osborne & Overbay, 2004). A series of blockwise hierarchical regression analyses were conducted to predict elderspeak outcomes by groups of proximal and distal contextual variables. To reduce the number of variables, mean ratings of evaluative age stereotypes across different life domains were calculated. Squared semipartial correlations (sr2) will be reported to indicate the unique contribution of a single predictor variable.
Results
Descriptive Findings
Descriptive information as well as bivariate correlations between the psycholinguistic variables are displayed in Supplementary Table S3. Overall, the mean relative frequencies of likely harmful elderspeak features were between 2% and 8%. We also analyzed the occurrence of at least one example within the whole care interaction. In the majority of interactions (97%), at least one tag question was used. CPS occurred at least once in 70% of the interactions. Baby-talk like terms were found in 57% and intimate forms of address in 16% of interactions.
Likely harmful features were not linked to each other (see Supplementary Table S3). Hybrid measures of fluency and syntax showed low to moderate correlations. Mean length of utterance was strongly associated with most of the other hybrid features and thus not considered as a dependent variable for further analyses. An increasing number of nurses’ tokens was associated with a decreasing lexical diversity, which is known as a general phenomenon of TTR (Richards, 1987).
As expected, patients’ cognitive and functional status were both significantly related to elderspeak features (see the upper half of Supplementary Table S4). A lower functional status was linked with a higher use of diminutives, a slower speech rate, a reduced grammatical complexity, and a lower lexical diversity, whereas a lower cognitive status was only associated with a reduced grammatical complexity and a lower lexical diversity. Patients’ sociodemographic variables were unrelated to most of the elderspeak features.
Nurses’ variables revealed limited associations with elderspeak features (see the lower half of Supplementary Table S4). CPS increased with the negativity of age stereotype ratings. Nurses’ gender was associated with speech rate, sentence fragments, and complex units, whereas age did not matter at all. Nurses’ mother tongue was highly correlated with their speech rate. The number of previous care interactions with the patient was only linked with sentence fragments.
Examining the Role of Proximal Context for Elderspeak
In order to sequentially examine the role of proximal contextual predictors at the multivariate level, seven hierarchical regression analyses were conducted for the three likely harmful and four hybrid elderspeak outcomes. The sample size varied in these analyses between n = 71 (CPS), n = 98 (diminutives, tag questions) and n = 99 (sentence fragments, complex units, TTR, speech rate) due to refused interviews of nurses (n = 2) or omitted items. Because sample sizes were relatively small, only theoretically meaningful predictor variables and significantly correlated control variables were included (see Supplementary Table S4). There was no indication of multicollinearity problems (all variance inflation factors < 2, r ≤ .50).
In the first step, we considered gender as well as nurses’ number of utterances as control variables because all regression analyses were consistently performed with the absolute numbers of elderspeak outcomes depending on the length of interactions. Due to substantial correlations between nurses’ mother tongue and speech rate, we also controlled for this variable when predicting speech rate. In a second step, we entered patients’ cognitive group and functional status as proximal contextual predictors of elderspeak.
As can be seen in Table 1, control variables already explained a considerable amount of variance in likely harmful features of elderspeak ranging between 17% and 50% of explained variance (Adjusted R2). However, only nurses’ number of utterances significantly contributed to the prediction of likely harmful features of elderspeak, whereas gender of patients and nurses did not. Proximal contextual factors significantly increased the amount of explained variance in only one of the three likely harmful features of elderspeak, i.e. in diminutives (ΔR2 = 11%). In particular, functional status played an important role for diminutives (p = .001, sr2 = .10), whereas cognitive group did not (p = .615, sr2 = .00).
Hierarchical Regression Analysis Predicting Likely Harmful Features of Elderspeak.
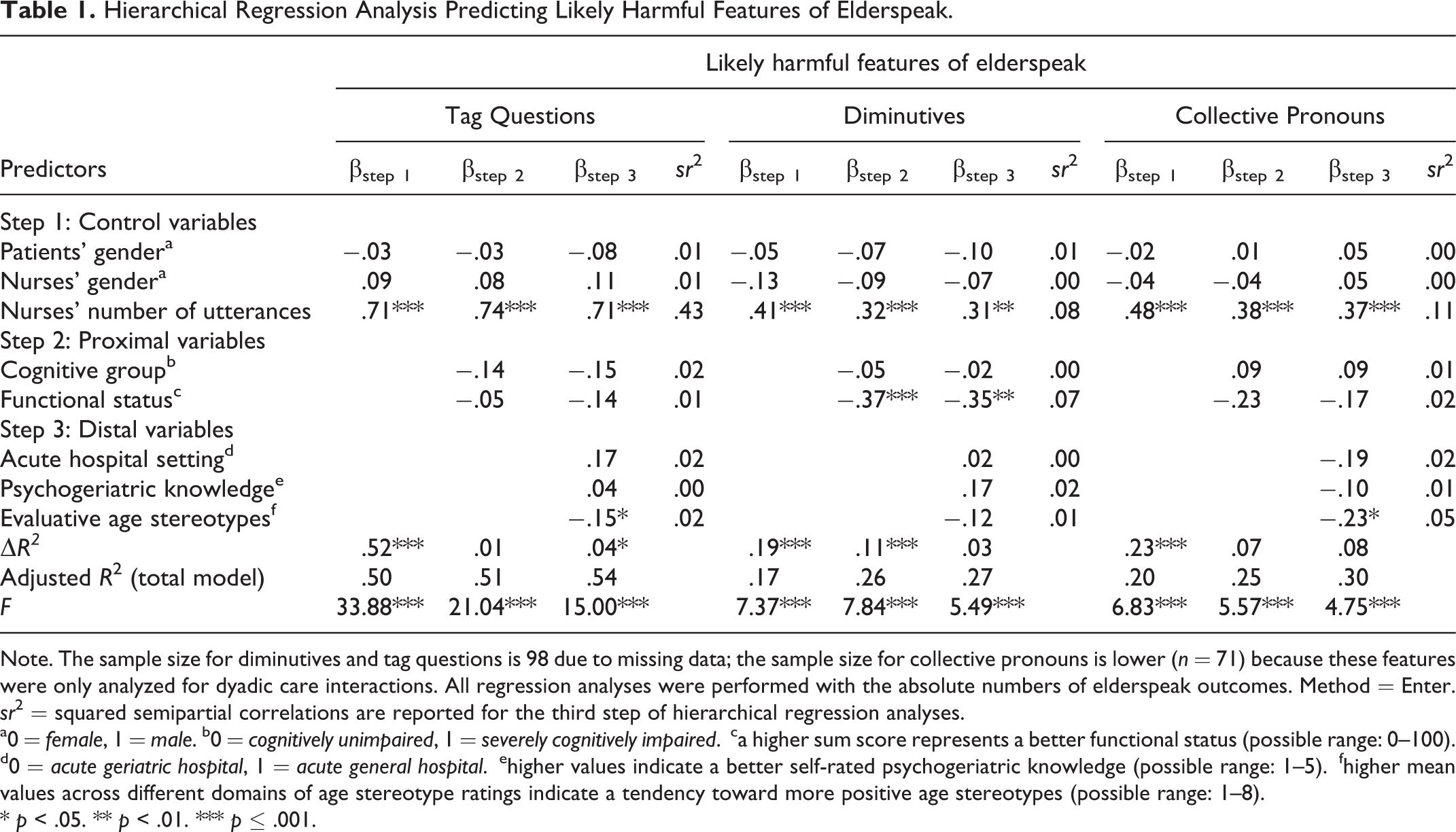
Note. The sample size for diminutives and tag questions is 98 due to missing data; the sample size for collective pronouns is lower (n = 71) because these features were only analyzed for dyadic care interactions. All regression analyses were performed with the absolute numbers of elderspeak outcomes. Method = Enter.
sr2 = squared semipartial correlations are reported for the third step of hierarchical regression analyses.
a0 = female, 1 = male. b0 = cognitively unimpaired, 1 = severely cognitively impaired.
ca higher sum score represents a better functional status (possible range: 0–100). d0 = acute geriatric hospital, 1 = acute general hospital.
ehigher values indicate a better self-rated psychogeriatric knowledge (possible range: 1–5).
fhigher mean values across different domains of age stereotype ratings indicate a tendency toward more positive age stereotypes (possible range: 1–8).
* p < .05. ** p < .01. *** p ≤ .001.
With respect to hybrid features of elderspeak (see Tables 2 and 3), control variables accounted for high amounts of variance ranging between 43% and 91% of explained variance (Adjusted R2). Being a male nurse was associated with a lower number of sentence fragments, a higher number of complex units, and a faster speech rate. Speaking a non-German mother tongue was significantly associated with a slower speech rate. Patients’ gender was not significantly related to any of the hybrid features. Adding proximal factors significantly increased the amounts of variance in two of the four hybrid features of elderspeak, namely in complex units by 7% and in speech rate by 5%. Again, the additional amounts of variance in complex units and speech rate were fully explained by functional status (p = .035 and p = .005, respectively), albeit its contribution was relatively low for both complex units (sr2 = .02) and speech rate (sr2 = .04).
Hierarchical Regression Analysis Predicting Hybrid Features of Elderspeak.
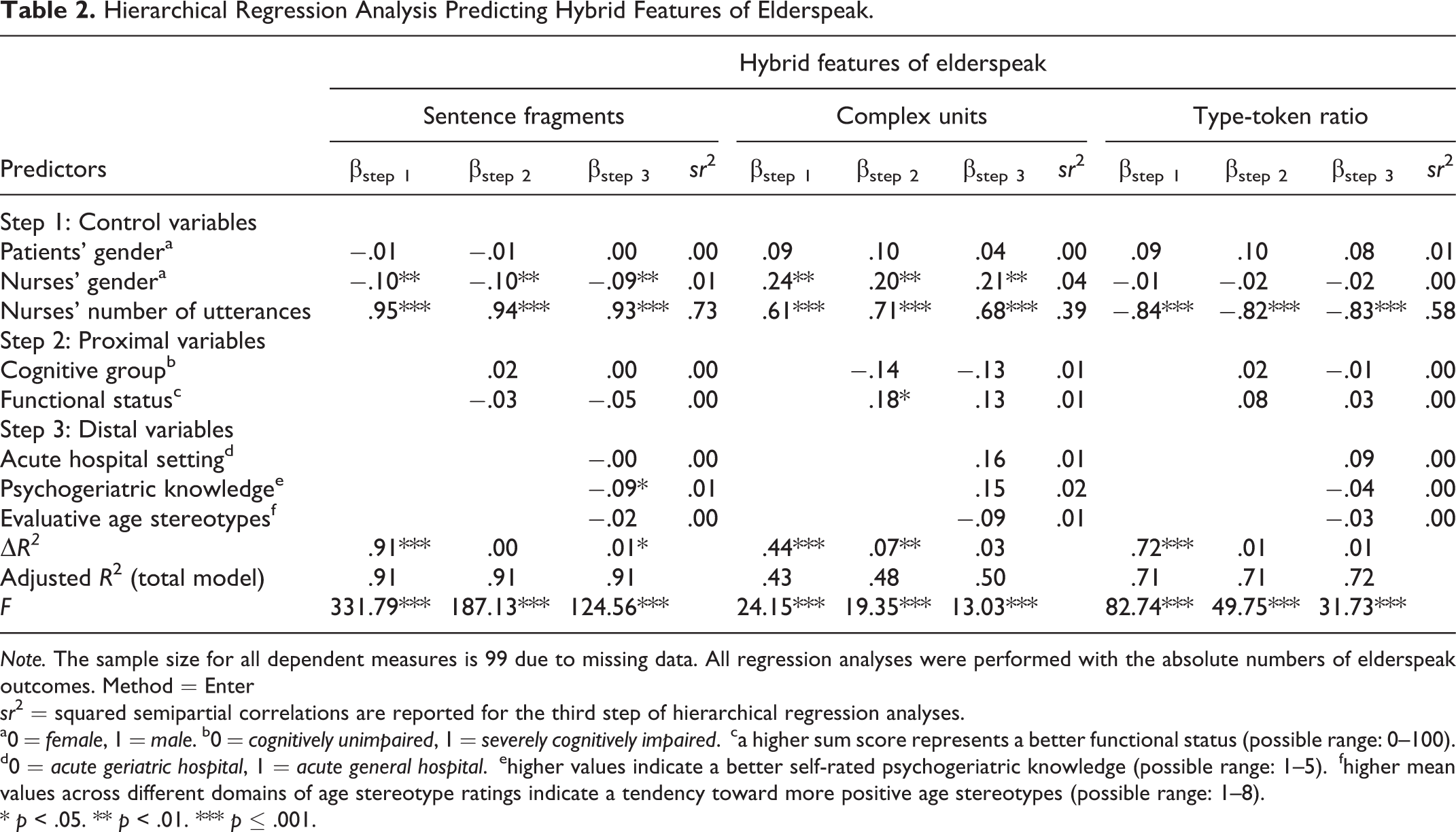
Note. The sample size for all dependent measures is 99 due to missing data. All regression analyses were performed with the absolute numbers of elderspeak outcomes. Method = Enter
sr2 = squared semipartial correlations are reported for the third step of hierarchical regression analyses.
a0 = female, 1 = male. b0 = cognitively unimpaired, 1 = severely cognitively impaired.
ca higher sum score represents a better functional status (possible range: 0–100). d0 = acute geriatric hospital, 1 = acute general hospital.
ehigher values indicate a better self-rated psychogeriatric knowledge (possible range: 1–5).
fhigher mean values across different domains of age stereotype ratings indicate a tendency toward more positive age stereotypes (possible range: 1–8).
* p < .05. ** p < .01. *** p ≤ .001.
Hierarchical Regression Analysis Predicting Speech Rate.
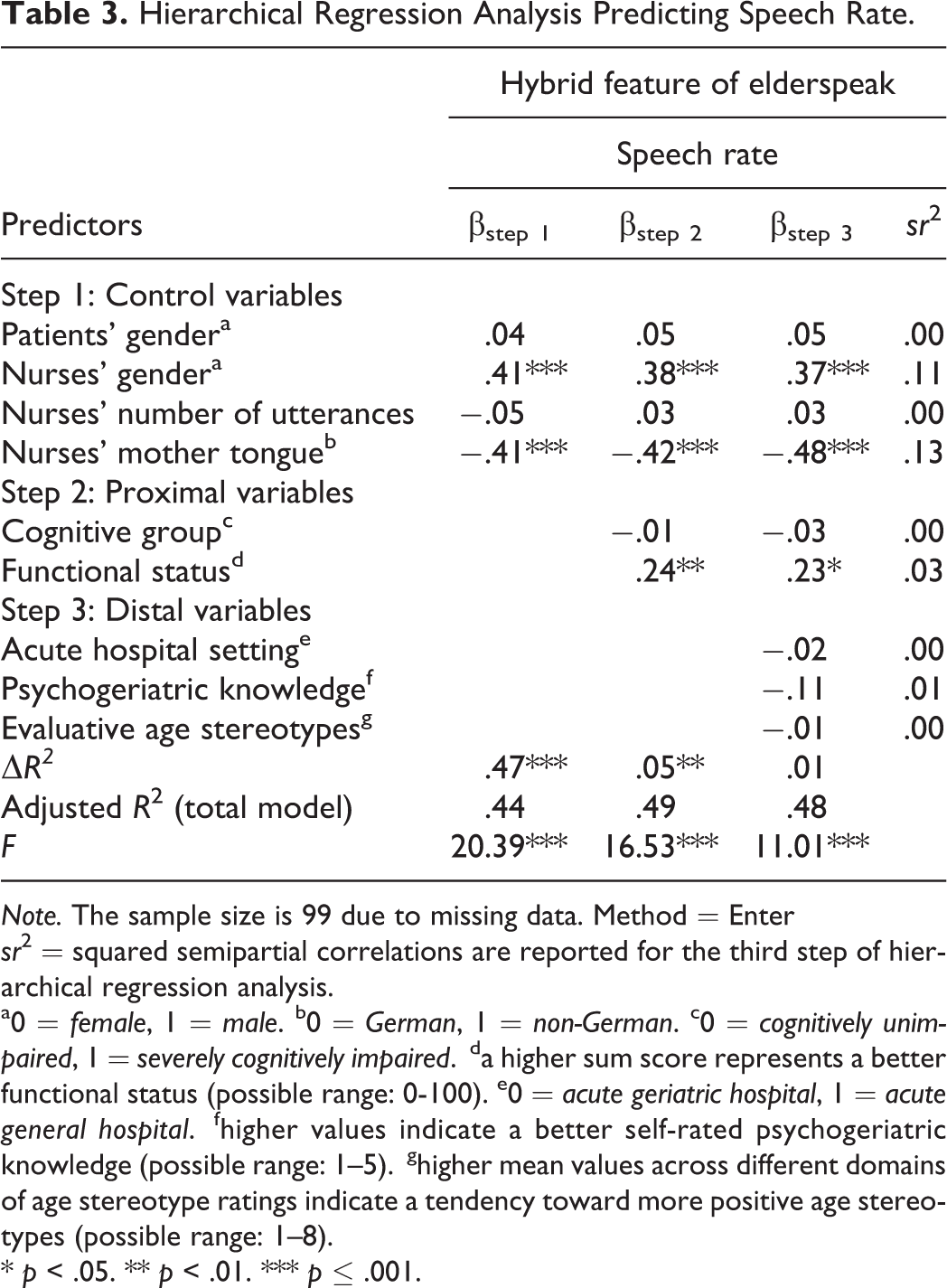
Note. The sample size is 99 due to missing data. Method = Enter
sr2 = squared semipartial correlations are reported for the third step of hierarchical regression analysis.
a0 = female, 1 = male. b0 = German, 1 = non-German. c0 = cognitively unimpaired, 1 = severely cognitively impaired.
da higher sum score represents a better functional status (possible range: 0-100). e0 = acute geriatric hospital, 1 = acute general hospital.
fhigher values indicate a better self-rated psychogeriatric knowledge (possible range: 1–5).
ghigher mean values across different domains of age stereotype ratings indicate a tendency toward more positive age stereotypes (possible range: 1–8).
* p < .05. ** p < .01. *** p ≤ .001.
Examining the Role of Distal Context for Elderspeak
For examining the additional role of distal contextual variables as predictors of elderspeak over and above control variables and proximal contextual variables, acute hospital setting, psychogeriatric knowledge, and evaluative age stereotypes were entered in the third step of hierarchical regression analyses. Distal contextual factors accounted for significant increments in variance in one of the three likely harmful features of elderspeak (see Table 1), namely in tag questions (ΔR2 = .04). In particular, negative age stereotypes significantly contributed to a higher use of tag questions (p = .037), albeit the uniquely explained variance was relatively low (sr2 = .02). Negative age stereotypes were also significantly related to a higher number of CPS (p = .029; sr2 = .05).
With respect to the four hybrid outcomes of elderspeak, distal contextual factors accounted only for significant amounts of variance in sentence fragments (see Tables 2 and 3). As evident from Table 2, better psychogeriatric knowledge was significantly related to a lower use of sentence fragments (p = .021). However, the uniquely explained variance of psychogeriatric knowledge was relatively low (sr2 = .01).
Comparing the Magnitude of Effect of Proximal Versus Distal Context
For testing the magnitude of effect of proximal versus distal context, we compared the increments in variance of the second (inclusion of proximal variables) versus the third step (inclusion of distal variables) after having controlled for covariates in the first step.
In three of the seven variables, increments in variance were higher for proximal contextual variables when compared to distal contextual variables. First, proximal variables contributed to significant increments in variance in diminutives (ΔR2 = .11, p = .001), whereas distal factors did not (ΔR2 = .03, p = .244). Second, additional amounts of variances in complex units were explained by proximal variables (ΔR2 = .07, p = .003), but not by distal variables (ΔR2 = .03, p = .165). Third, substantial increments of variance were observed for proximal variables (ΔR2 = .05, p = .007) but not for distal variables (ΔR2 = .01, p = .680) when predicting speech rate.
In only two of the seven variables, i.e. tag questions and sentence fragments, distal contextual factors predicted a significantly higher amount of variance. However, the proportion of explained variance was relatively low (ΔR2 = .04, p = .042 and ΔR2 = .01, p = .048, respectively). With respect to CPS and TTR, neither proximal nor distal factors played a substantial role in prediction (see Tables 1 and 2).
Additional Analyses
In order to examine the role of social-contextual distal features, we additionally entered time of the day (morning versus evening care) and interaction type (dyadic versus triadic care interactions), after having included the above-mentioned control variables and proximal variables as predictors of the first block. Adding social-contextual features did not contribute to significant increments in variance for likely harmful features of elderspeak (ΔR2 = .01 to .03; all p-values > .05). With respect to the four hybrid features of elderspeak, social-contextual variables increased the amounts of variance in complex units (ΔR2 = .03, p = .038) and speech rate (ΔR2 = .03, p = .042). Triadic care interactions were marginally associated with a higher number of complex units (β = .13, p = .062, sr2 = .02) as well as with a significantly faster speech rate (β = .19, p = .013, sr2 = .03).
Discussion
To the best of our knowledge, this is the first study that examined the occurrence of likely harmful and hybrid features of elderspeak in acute hospital environments. In order to contribute to a more differentiated understanding of elderspeak and its determinants, conceptually derived proximal and distal contextual predictors were simultaneously considered.
In the majority of care interactions, typical likely harmful features of elderspeak were identified (Sachweh, 1998; Williams, 2006; Williams, Shaw, et al., 2017). Hypothesis 1 assuming that both cognitive and functional impairment play a substantial role in the prediction of likely harmful as well as hybrid features of elderspeak was partly supported. As expected, functional impairment was significantly related to a higher use of diminutives, a reduced grammatical complexity, and a slower speech rate. Surprisingly, none of the elderspeak features was significantly predicted by cognitive status. An explanation for this finding may be that functional impairment is a more salient disability-related feature at the proximal level than CI, which has been shown to remain undetected by hospital staff in nearly 50% of cases (Hessler et al., 2017; Mukadam & Sampson, 2011). This finding is in line with our earlier analysis revealing that functional impairment more strongly contributed to controlling tones of nurses’ voice than CI (Schnabel et al., 2019). Further evidence from research on dependency-supportive behaviors (Baltes & Wahl, 1992; Ryan et al., 2006) and baby talk in German nursing homes (Sachweh, 1998) exists showing that particularly functionally dependent older adults are receivers of patronizing talk.
Distal contextual features played a minor role in the prediction of elderspeak features. Although evaluative age stereotypes only contributed to a small amount of the explained variance, it is interesting to note that this variable played a role in two of the three likely harmful features of elderspeak even after having controlled for several variables. Hence, more negative evaluative age stereotypes were significantly linked with a higher use of tag questions as well as a higher use of CPS. Psychogeriatric knowledge only played a role in sentence fragments. To conclude, support for Hypothesis 2 was given to some extent. The minor role of distal contextual variables strengthens our argument that functional impairment is a strong trigger of negative stereotype activation, which may counteract the positive effects of training programs.
Confirming Hypothesis 3, proximal context mostly emerged as more important for the prediction of elderspeak features showing larger effect sizes when compared to distal context. In particular, functional status contributed to the explanation of variance in both likely harmful as well as hybrid features of elderspeak. This underpins the importance of including different contextual levels. The current study also demonstrated that CODA can be a heuristically fruitful extension of the CPA and ASI model. Setting elderspeak into contextual spaces may help to better organize the existing research, which has dealt with a large number of dependent variables in a relatively unstructured manner (Kemper et al., 1998).
In line with previous research (Lombardi et al., 2014), the current study demonstrated that dyadic nurse-patient care interactions were associated with simplifications in terms of a reduced speech rate and a lower grammatical complexity. In general, control variables explained large proportions of variance, in particular in hybrid features. Hence, gender and mother tongue became more important for hybrid compared to likely harmful features of elderspeak indicating that hybrid features are influenced by a myriad of factors.
Although our finding suggest that functional impairment is a more important trigger of harmful and hybrid elements of elderspeak than CI, the consequences of elderspeak may be particularly harmful for patients with CI. Research conducted in the acute hospital setting has demonstrated that NPS more frequently occur in patients with CI (76%) when compared to patients without CI (38%; Hessler et al., 2017). In particular, expansive symptoms such as nighttime disturbances (38%), aberrant motor behavior (28%), aggression (25%), and irritability (25%) were associated with major complications during care and caused the highest caregiver burden. Previous research has clearly shown that elderspeak can increase the likelihood of NPS in patients with CI (Herman & Williams, 2009; Williams et al., 2009).
However, some authors argue that specific simplifications might be beneficial for CI patients by lowering working memory demands (Samuelsson et al., 2013). Nevertheless, speaking too slowly and simply as with young children might rather tax working memory and can be perceived as patronizing (Harwood et al., 2012; Kemper & Harden, 1999). A comparison of our data with German social interactions (Westpfahl & Gorisch, 2018) revealed typical syntactic features for spontaneously spoken German in everyday interactions that are dominated by sentence fragments and not so much by complex units. Furthermore, only a low amount of patients reported perceived age discrimination in our study.
To conclude, the appropriateness of elderspeak depends on several factors such as the level of familiarity, the degree of simplifications, and particular combinations of linguistic features (Kemper & Harden, 1999). For example, first name terms may even be interpreted as a form of person-centered communication if the patients wants to be addressed in that way or in the case of a close relationship with the healthcare professional (O’Connor & St. Pierre, 2004). More research is needed to disentangle beneficial versus harmful effects of elderspeak and to provide target-specific guidelines for older patients who represent a heterogeneous sample with different communication needs.
Limitations
One limitation of our study is that findings are based on relatively small and potentially positively biased subsamples requiring further replication in a broader variety of contexts such as rural hospitals.
Second, although particular emphasis was placed on the differentiation between harmful and hybrid features of elderspeak, the current findings do not allow us to draw conclusions on the positive versus negative valence of elderspeak. As the validity of self-reports is limited in CI patients, timed-event sequential studies focusing on behavioral reactions are needed (Herman & Williams, 2009; Williams et al., 2009).
Third, the present study only focused on three likely harmful features of elderspeak. Future studies should also consider prosodic features of elderspeak such as high pitch, which can also be seen as a likely harmful feature of elderspeak (Kemper & Harden, 1999; Kemper et al., 1996).
Finally, the acceptance of elderspeak likely depends on cultural norms (Voss, Kornadt, et al., 2018) limiting a direct comparison of our study with previous studies that were predominantly conducted in the USA (Lowery, 2013).
Implications
Our findings deserve particular attention with respect to daily interactions in the acute hospital context. Considering the evident discrepancy between lacking resources and the increased need for assistance in ADLs among vulnerable older inpatients (Voss, Bodner, et al., 2018), person-centered communication might be in danger. Importantly, negative age stereotypes are often activated via implicit mechanisms, which have been shown to be pervasive and more negative than explicitly activated ones (Gendron et al., 2016). Some studies even indicated that nurses consciously used elderspeak to improve residents’ well-being, their understanding, and cooperation during care interactions (Grimme et al., 2015). Thus, raising nurses’ awareness of potentially harmful communication styles can be an important step to reduce unmet needs and NPS among older patients with CI (Williams, Perkhounkova, et al., 2017). The implementation of evidence-based communication strategies in nursing education and training programs is of high practical relevance.
Supplemental Material
ROA-20-085_R1_Supplemental_Tables_Elderspeak - Elderspeak in Acute Hospitals? The Role of Context, Cognitive and Functional Impairment
ROA-20-085_R1_Supplemental_Tables_Elderspeak for Elderspeak in Acute Hospitals? The Role of Context, Cognitive and Functional Impairment by Eva-Luisa Schnabel, Hans-Werner Wahl, Christina Streib and Thomas Schmidt in Research on Aging
Footnotes
Authors’ Note
Eva-Luisa Schnabel is now at the Bavarian Care and Nursing Authority, Amberg, Germany.
Acknowledgments
We thank all participating patients and nurses as well as the directors of both acute hospitals involved in this study for their cooperation. Furthermore, we thank Lea Draeger, Larissa Frey, Nora Schädel, and Sandra Schmitt for their help in conducting interviews and processing the data. A special thanks goes to Anton Borlinghaus who acted as an excellent adviser for the syntactic segmentation procedure of our spoken language data. We thank Thomas Spranz-Fogasy, Evi Schedl, and Swantje Westpfahl, Leibniz Institute for the German Language (IDS) in Mannheim, Germany, for their cooperative role and valuable recommendations in collecting, transcribing, and analyzing the linguistic data. Further, we thank Anton Schönstein for statistical recommendations. Finally, we thank Markus Schick, head of the Bavarian Care and Nursing Authority in Amberg, Germany, for stimulating discussions regarding practical implications and future societal directions of this study.
According to the core values of transparency, openness, and reproducibility in science, parts of the research data underlying this study, i.e. audio recordings, transcripts, annotations, and metadata will be archived for long-term use being available for research purposes under specific conditions by the trusted Archive for Spoken German (AGD) at the IDS (![]() ).
).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a doctoral scholarship from the Robert Bosch Foundation Stuttgart within the Graduate Program “People with Dementia in Acute Care Hospitals (GPPDACH)”, located at the Network Aging Research (NAR), Heidelberg University, Germany.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.