
Abstract
This systematic review provides an overview of the unique challenges allied health professions face in the translation and implementation of evidence into practice, which remain relatively under reported and uninformed by a theoretical basis of behaviour change. MEDLINE, EMBASE, CINAHL and Scopus databases from 2010 to 2022 were searched for primary study designs resulting in 21 articles included in this review (PROSPERO: 2022 CRD42022314996). Allied health disciplines reported in the review were mainly from occupational therapy, physiotherapy, dietetics, and speech pathology. The most frequently reported implementation determinants across the Theoretical Domains Framework were identified as ‘environmental context and resources’, and ‘knowledge’. The results also identified a greater influence of ‘social influences’ and ‘beliefs about consequences’ in implementation. Implementing evidence into clinical practice is a multifaceted, complex process, and the use of the Theoretical Domains Framework provided a systematic approach to understanding the drivers behind the target behaviours. However, there is a paucity of studies across the allied health professions that describe implementation strategies used and their impact. Many of the studies focused on implementation by the individual clinician rather than the role organizations can play in the translation of evidence into practice.
Translating evidence into practice remains challenging across the health professions. Evidence is costly to generate and slow to reach clinicians at point of care. It is often quoted that it takes an average of 17 years for research evidence to be translated into routine clinical practice (Morris et al., 2011).
Evidence-based practice (EBP) ensures that clinical practice is informed by the best available scientific evidence and incorporates professional experience. It has evolved from the evidence-based medicine movement, originally defined as “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients” (Sackett et al., 1996). The implication of this definition, is that the evidence-based process prioritises the selection of interventions by critical appraisal of research evidence as applicable to the characteristics of the patient (Parrish, 2018). Evidence-based medicine was historically focused on medical and surgical interventions (Djulbegovic & Guyatt, 2017). However, EBP is now an expectation of contemporary clinical practice for medicine, nursing and allied health professionals, and is described by the World Health Organization as one of the most important global public health challenges in the 21st century (Haines et al., 2004).
While EBP and education has been well reported as part of medical training, there is little evidence available to support the consistency of this education in the allied health professions (Dizon et al., 2012). Allied health professionals are usually university-level qualified practitioners, with a specialised expertise in specific areas of health (Allied Health Professions Australia, 2019). They often work within a multidisciplinary team, grouped into therapeutic and technical professions. The allied health workforce is diverse and can include dietetics, occupational therapy, physiotherapy, social work, speech pathology and podiatry, within the hospital setting. Allied health professionals frequently work within complex interprofessional teams, often practicing their professional discipline across multiple medical specialties where evidence must compete with several factors that influence decision making. This unique professional dynamic can lead to tensions, as allied health professionals are required to keep up to date with evidence within their professional discipline as well as across the medical specialties where they practice (Smith & Johnson, 2023).
The practice of translating evidence into clinical practice among allied health professionals remains under reported (Sarkies et al., 2018, 2019). Allied health has faced challenges in the translation and implementation of EBP, including reported lack of time and resources and a lack of understanding on how to translate research into practice. It is also suggested that barriers to EBP are complex, especially within the public hospital setting (Smith & Johnson, 2023). For example, allied health professionals often provide support for medical and nursing care, which can lead to referrals and requests for services that could be considered low value like chest physiotherapy as an adjunctive treatment for adults with pneumonia (Elshaug et al., 2012) Implementation strategies are frequently educationally based, where non-educational strategies could be more suited to contextual barriers to research translation in allied health. The gap of getting evidence into practice remains, despite the enthusiasm of allied health professional (Hitch et al., 2019). Implementing EBP frequently encounters resistance to change within the healthcare community. Smith and Johnson (2023), reported three overarching themes in their systematic review of embedding translational research into the public hospital system: leadership, capabilities, and organisational culture (Smith & Johnson, 2023). However, they did not examine issues specific to allied health professionals.
Existing interventions used to reduce the evidence-to-practice gap for allied health professionals do not appear to have been informed using a theoretical basis of behaviour change (Michie et al., 2011; Rycroft-Malone, 2004). Behaviour change theories have been used to support the use of research evidence to inform policy and management decision making as well as in clinical practice (Atkins et al., 2017; Sarkies et al., 2017). Implementation science researchers propose that the identification of the theoretical domains of the implementation problem and then linking this to relevant behaviour change techniques is an effective approach for the implementation of evidence-based practices. The Theoretical Domains Framework (TDF) provides a validated tool that was specifically designed to facilitate and identify the influences of health professional behaviour in relation to implementing EBP (Atkins et al., 2017). The TDF enables an understanding of implementation problems and therefore facilitating the most effective interventions, which can be used to understand complex, multifaceted behaviours. There is a paucity of information on translating evidence into practice within the public health system and still less focusing on the allied health professions (Smith & Johnson, 2023). The aim of this systematic review is to determine what is known about the perceived barriers and enablers to allied health professionals translating evidence into clinical practice in the hospital setting.
Methods
Design
This systematic review has been registered with in PROSPERO (2022 CRD42022314996) and reported according to PRISMA reporting methods. The structure of the research question was based on the JBI mixed methods review methodology: PICo: Population, (Phenomenon of) Interest and Core Concepts (Stern et al., 2021).
Study Selection and Inclusion Criteria
All primary study designs looking at translation of evidence into clinical practice were included with studies reporting on the following allied health professions working in the public hospital setting: dietetics, occupational therapy, physiotherapy, social work, speech pathology, radiation therapy, orthotist, exercise physiology, and podiatry; Organization for Economic Cooperation and Development (OECD) countries’ health systems; adults over 18 years old.
The phenomenon of interest included the translation of evidence by allied health professionals into ‘usual care’ clinical practice. Evidence translation can be defined as the use research evidence to inform health and healthcare decision-making by health professionals. Evidence translation can also be described under different terms but for the purpose of this review it will be referred to as evidence translation. This review focuses on the factors that represent the barriers or enablers to allied health professionals translating evidence into clinical practice.
Search Strategy
The lead author consulted with a librarian in the field of medicine and healthcare to design the search strategy. Key words, synonyms and subject headings were searched relating to the concepts of allied health professionals and translating evidence into clinical practice. Publications were limited to English language and those published from the year 2010 to 23/3/2022. The search strategy was applied to the following electronic databases: MEDLINE, EMBASE, CINAHL and Scopus (Appendix A). Electronic databases were supplemented by reviewing reference lists of included articles relevant to the field of allied health professions to ensure data saturation. An electronic alert was put in place to identify potentially relevant articles published after completion of the search to date.
Study Screening and Selection
Covidence software was used as a screening and data extraction tool (Harrison et al., 2020). Duplicates were automatically removed using Covidence. Three reviewers (JB, IM, CT) independently read each title and abstract using this software and voted to include or exclude according to pre-determined inclusion and exclusion criteria. Those included, progressed to full text screening by two independent reviewers (JB, CH). Any conflicts were resolved with discussion and a third reviewer (MS) was brought in if consensus could not be ensured.
Data Extraction
Study details included were design, setting, population, intervention, barriers, and enablers. Study details were extracted using specifically designed templates by investigators and piloted for use. Data extracted was recorded using a Microsoft Excel spreadsheet. Any disagreements were resolved by discussion. If agreement could not be resolved, MS was consulted.
Study Quality Appraisal
QuADS Appraisal Tool
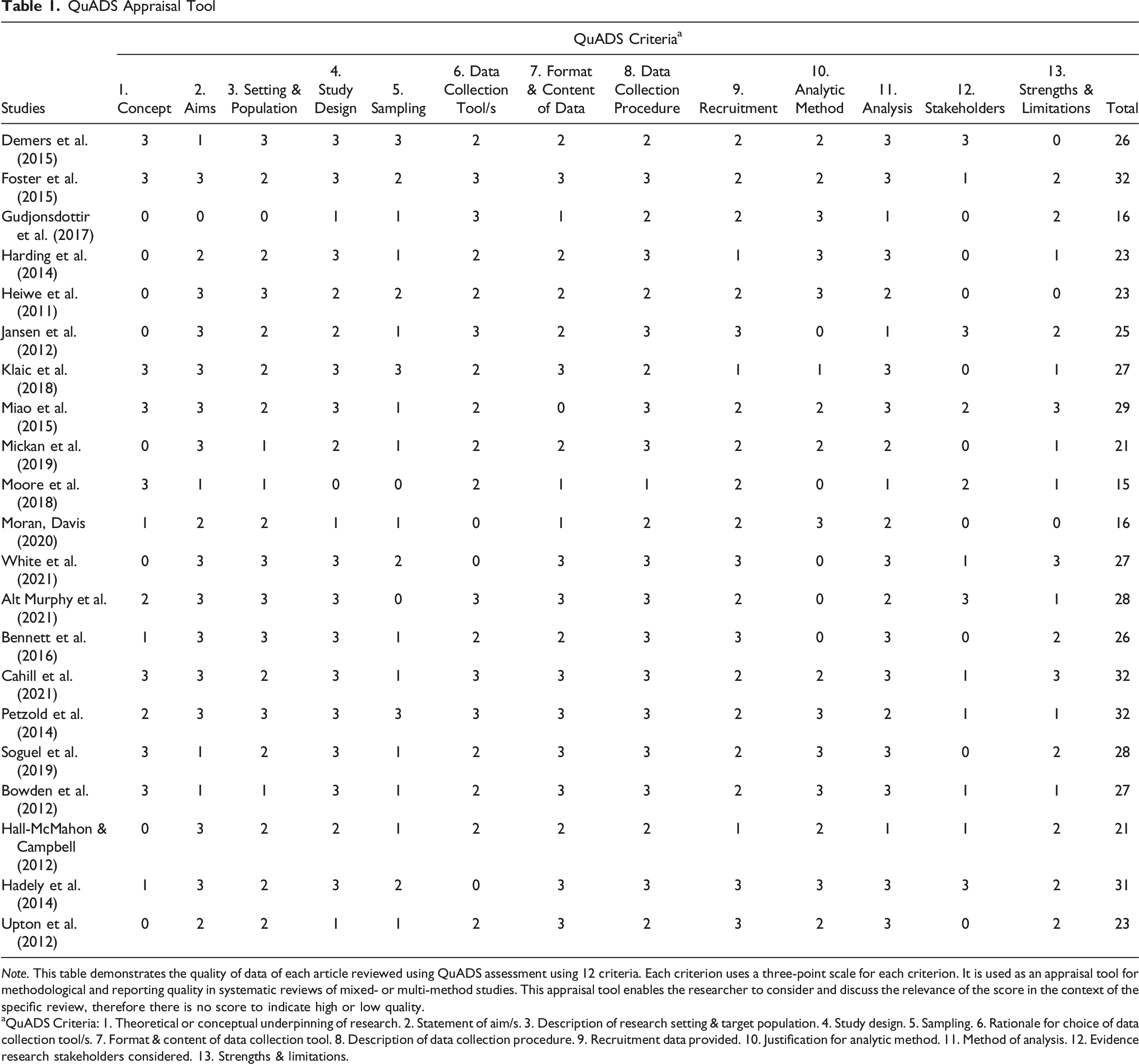
Note. This table demonstrates the quality of data of each article reviewed using QuADS assessment using 12 criteria. Each criterion uses a three-point scale for each criterion. It is used as an appraisal tool for methodological and reporting quality in systematic reviews of mixed- or multi-method studies. This appraisal tool enables the researcher to consider and discuss the relevance of the score in the context of the specific review, therefore there is no score to indicate high or low quality.
aQuADS Criteria: 1. Theoretical or conceptual underpinning of research. 2. Statement of aim/s. 3. Description of research setting & target population. 4. Study design. 5. Sampling. 6. Rationale for choice of data collection tool/s. 7. Format & content of data collection tool. 8. Description of data collection procedure. 9. Recruitment data provided. 10. Justification for analytic method. 11. Method of analysis. 12. Evidence research stakeholders considered. 13. Strengths & limitations.
Data Synthesis and Presentation
A convergent integrated approach to synthesis was taken. Any quantitative data was qualitized by using textual descriptions, then aggregated to produce overall integrated findings and thus providing a richer narrative synthesis for the review, using themes guided by the Theoretical Domains Framework. A narrative synthesis was undertaken due to the variability of studies that were reviewed, to determine any barriers and enablers perceived to impact on the translation of evidence in clinical practice (Popay et al., 2006). Framework analysis using the TDF was applied to facilitate the exploration of the determinants of behaviour to understand and give an insight into drivers behind the target behaviours and its applicability to the area under review (Dixon-Woods, 2011). The lead author coded barriers and enablers in the results sections of the included studies line by line into the TDF domains and constructs using NVivo software v14 (Dhakal, 2022). The codes were checked with MS and the robustness of the synthesis reviewed using critical reflection with the lead author.
Results
The search yielded 888 articles, of which 106 were removed as duplicates. Title and abstract screening was conducted on 57 articles were subjected to a full-text screen. Following this full-text screening, 39 articles did not meet the inclusion criteria, which resulted in the inclusion of 18 articles in this review (Figure 1). In addition, citation searching was also conducted, to which three articles met the inclusion criteria and added to the review and so resulting in a final number of 21 articles included in the review. Characteristics of the articles reviewed can be reviewed in Table 2. PRISMA Flowchart Characteristics of Articles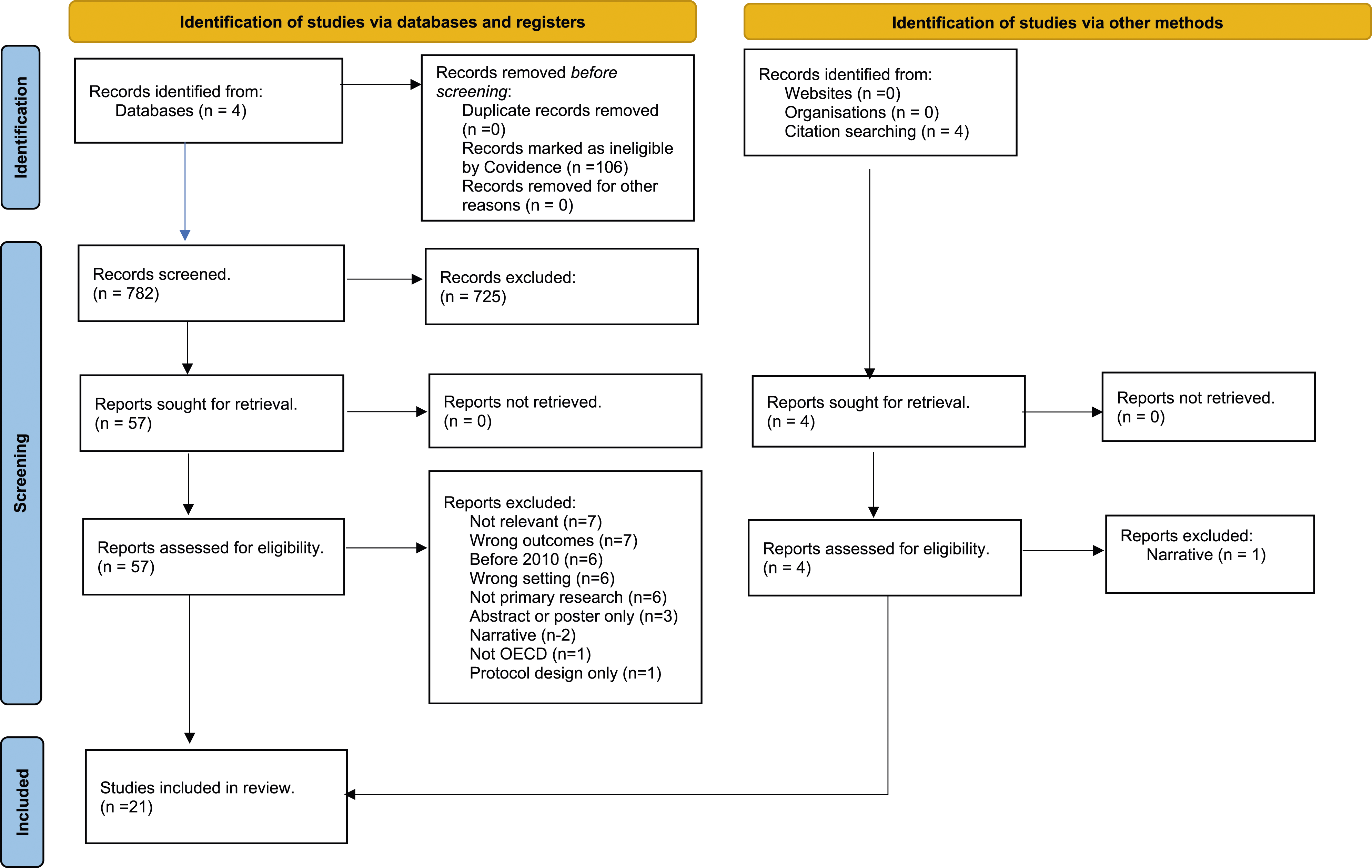
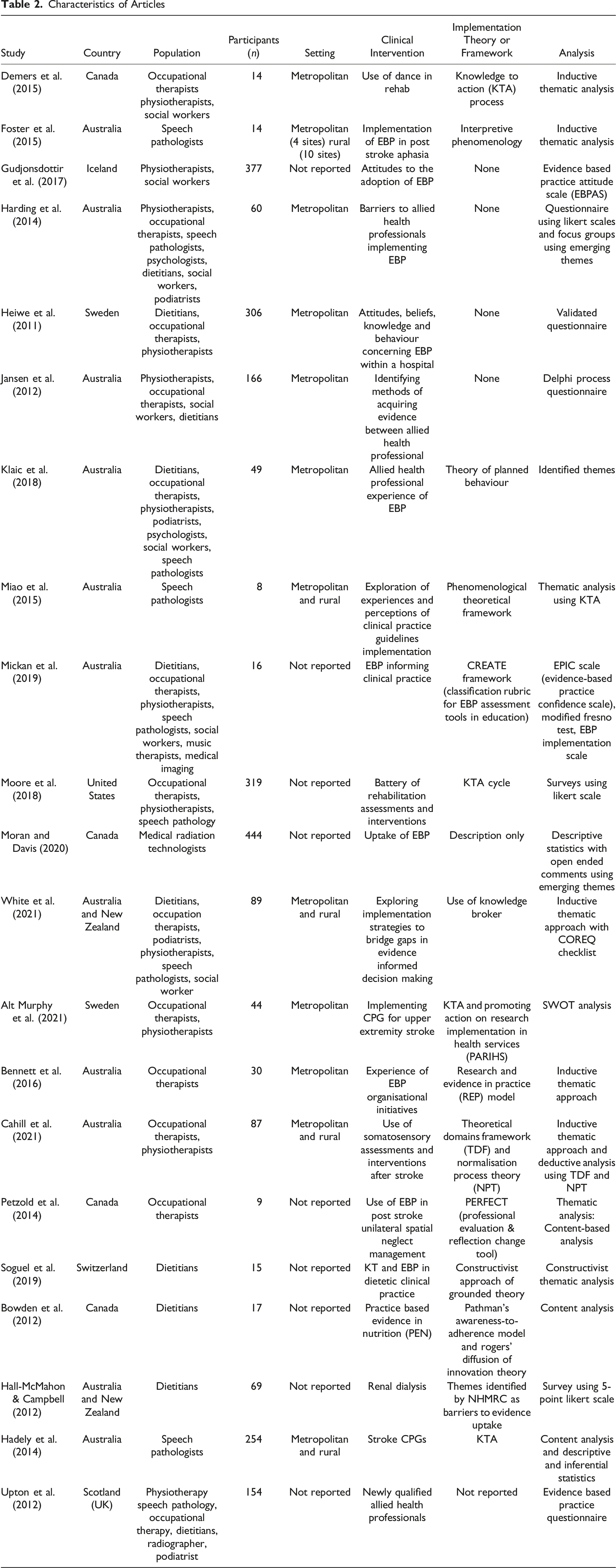
Allied health groups reported in the papers were mainly from occupational therapy, physiotherapy, dietetics, and speech pathology. Participants totalled n = 2541, ranging from eight to 444 participants in each study. Most of the studies were conducted in Australia (n = 11), with other studies from Canada (n = 4), Sweden (n = 2), Iceland (n = 1), United States (n = 1), Switzerland (n = 1) and the United Kingdom (n = 1).
Quality Assessment of Studies
Quality assessment was carried out using the QuADS tool (Harrison et al., 2021). Most of the studies had clear statement of aims and study design. Data collection was well described in respect of format and data collection procedure. However, there appeared to be minimal consideration of the research stakeholders and strengths and limitations of the studies were not fully discussed in many cases. Overall, the quality of the studies was considered strong especially with regards study design, description of data collection and appropriateness of analysis but weak in considering stakeholders in the research process. Table 1.
Implementation Determinants
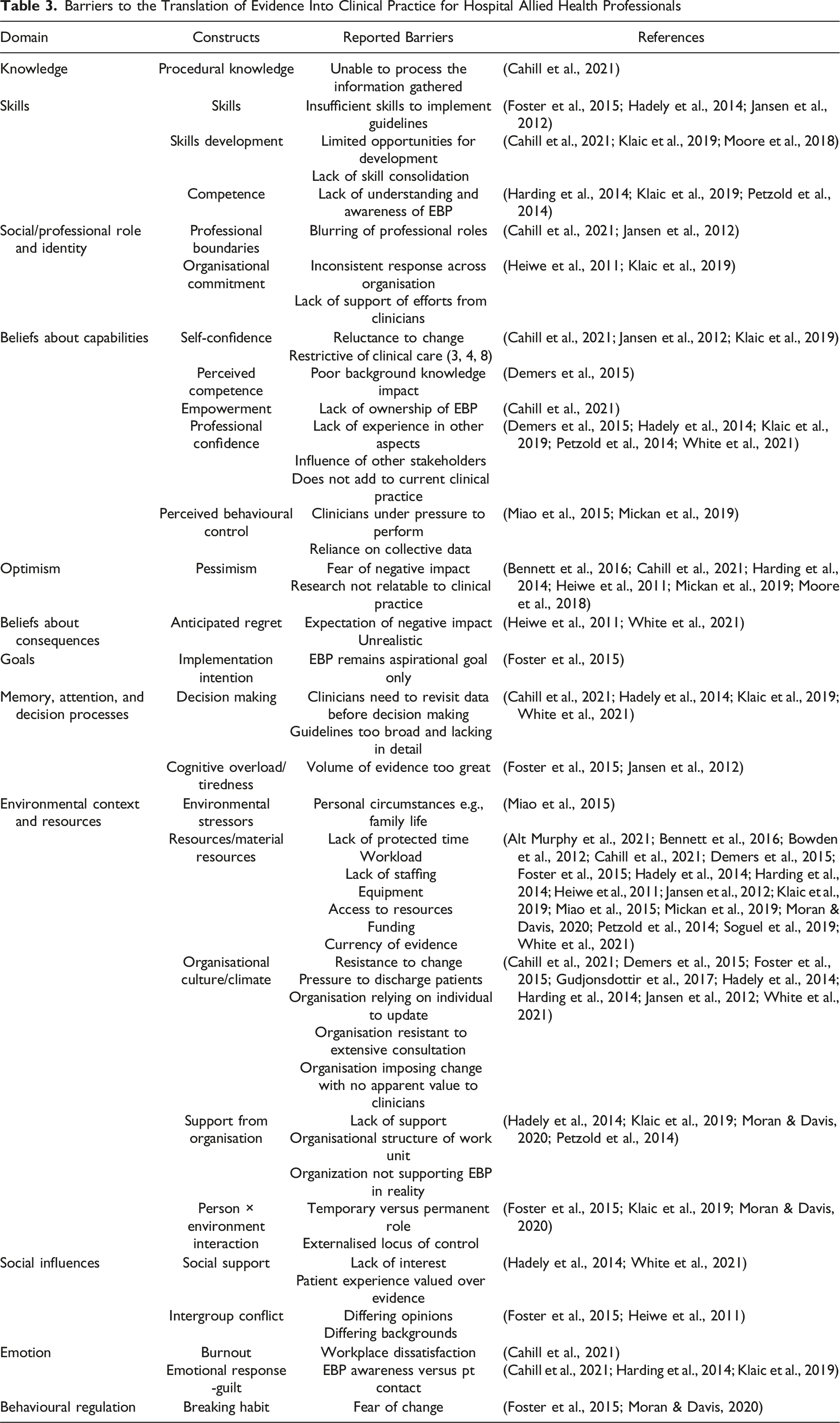
Barriers to the Translation of Evidence Into Clinical Practice for Hospital Allied Health Professionals
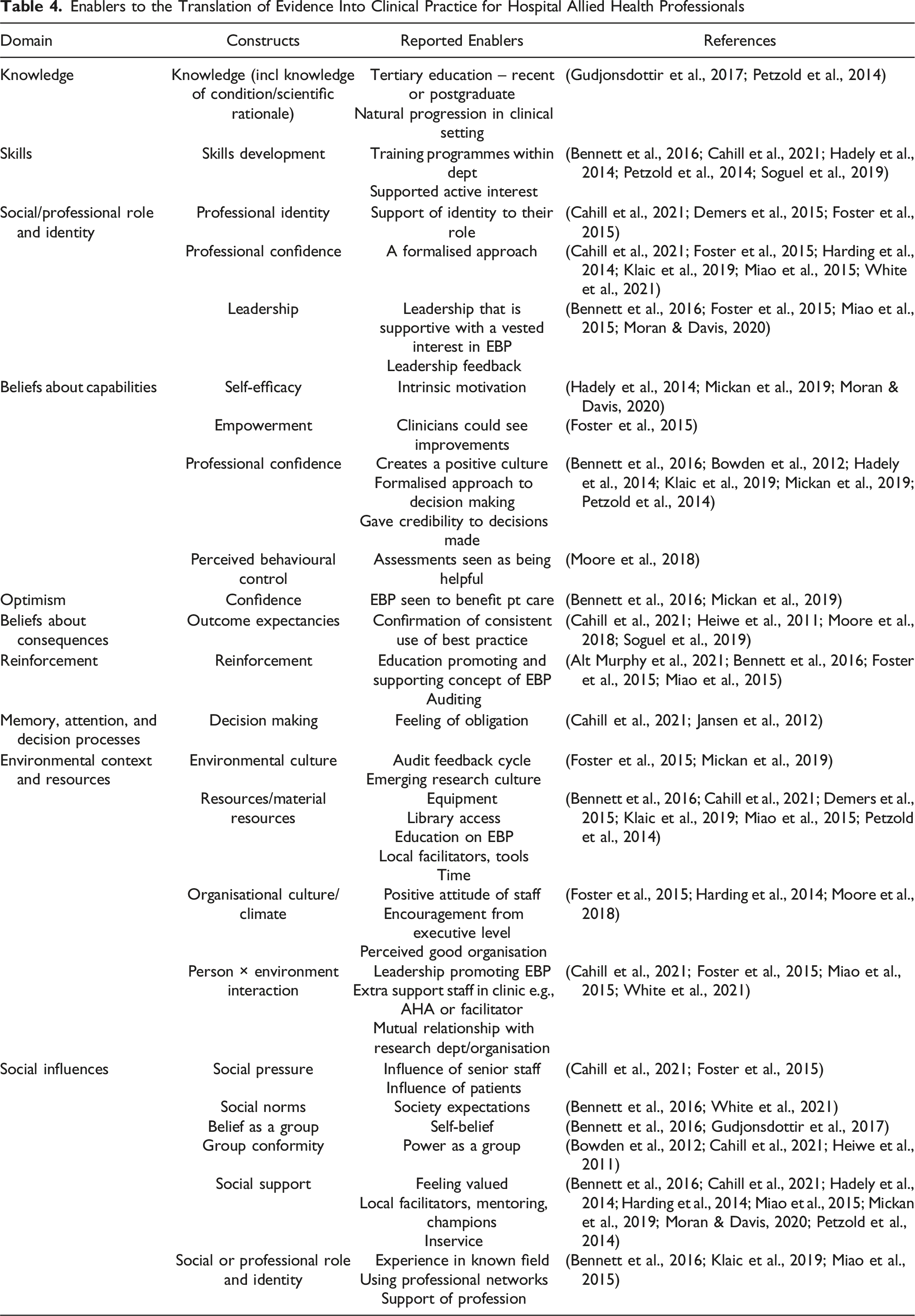
Enablers to the Translation of Evidence Into Clinical Practice for Hospital Allied Health Professionals
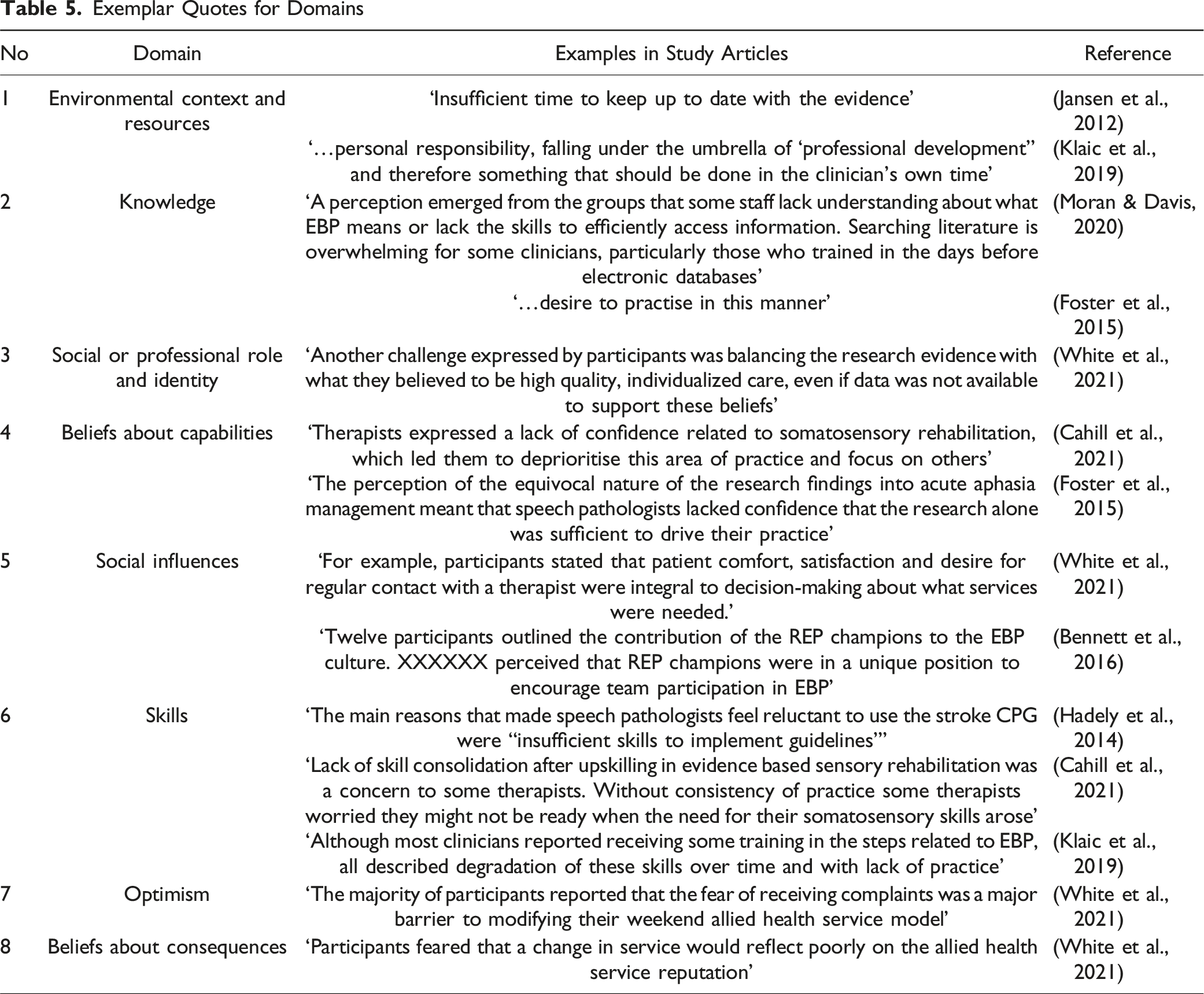
Exemplar Quotes for Domains
Domain: Environmental Context and Resources
Resources were amongst the highest reported obstacles to EBP (n = 17). Time was a commonly reported barrier (n = 14) (Jansen et al., 2012). Clinicians reported the lack of protected non-clinical activity time to prepare and keep up to date with current literature. This was reinforced by an increasing pressure from operational imperatives to treat and discharge patients faster as a greater priority than providing the latest evidence-based care (Bennett et al., 2016; Cahill et al., 2021; Moran & Davis, 2020; Petzold et al., 2014) (n = 4). The lack of protected time was further compounded by the lack of other resources, such as equipment shortfalls and access to electronic resources such as computers in allied health department areas (Harding et al., 2014; Jansen et al., 2012; Moran & Davis, 2020) (n = 9).
EBP was seen as a ‘personal responsibility’, to be completed in clinicians’ own time and, as a result the clinicians felt undervalued by the organisation (Klaic et al., 2019). The organisation, as perceived by some clinicians, created a culture that any change was too hard and required too much effort to make any change worthwhile. As result, clinicians felt disempowered to implement change (Foster et al., 2015; Harding et al., 2014) (n = 8).
In contrast, staff in leadership roles and local facilitators who were supportive of EBP enabled the use of EBP into existing daily routines. This facilitated identification of the benefits of EBP and created an environment that enabled its use within routine care (Bennett et al., 2016; Miao et al., 2015).
Domain: Knowledge
Lack of knowledge of evidence was reported in seven articles, creating a barrier to the use of EBP. The majority of these were because of a lack of understanding of the desired practice change (n = 5). However, the reasons behind the lack of knowledge were, primarily, the lack of training or inability of the clinicians to access relevant research literature (Cahill et al., 2021; Harding et al., 2014) Other reasons included guidelines not being updated to reflect the latest evidence, not enough evidence, or detail, in published studies (Hadely et al., 2014). Clinicians were also reluctant to use evidence due to the inability to match their ‘real world’ clinical practice with research literature (Soguel et al., 2019).
Knowledge of research, the research process and how it relates to EBP was found to be an important facilitator for giving clinicians a better grasp of EBP (Foster et al., 2015; Moran & Davis, 2020) (n = 9). This was further supported by clinicians’ level of education and recency of graduation where they received training on evidence-based practice (Klaic et al., 2019; Petzold et al., 2014). Clinicians strongly expressed the use of evidence as aspirational (n = 6) (Foster et al., 2015).
Domain: Social or Professional Role and Identity
Social or professional role and identity were considered to have some influence on translating knowledge into clinical, which was both an enabler and a barrier (n = 13). Some clinicians described maintaining awareness of the research evidence as a lower priority than high quality individualised care for the patient, regardless of the evidence presented.
Some clinicians were concerned about the use of EBP when this required a change in clinical practice. The clinicians were concerned whether the new knowledge and skills would be used appropriately for their patients (Cahill et al., 2021). Clinicians were reluctant to implement a change when there was a general lack of evidence in their clinical field, favouring patient feedback and extending the scope of practice outside of what was considered within their professional field of expertise (Hadely et al., 2014; Petzold et al., 2014; White et al., 2021).
Clinicians were also concerned about the organisational commitment to EBP. Klaic, McDermott and Haines in 2019 reported that clinicians were concerned about disapproval or ambiguity towards EBP by the organisation and that the effort of clinicians invested in EBP activities were not valued (Klaic et al., 2019). A lack of leadership at service level was also described with a lack of guideline enforcement (Miao et al., 2015)
Organisational commitment and support were considered important for the implementation of new evidence based interventions (Demers et al., 2015). Clinicians reported that organisations which value research and support the attendance of groups that encourage and promote EBP was beneficial (Bennett et al., 2016; Foster et al., 2015). As a result, strategies employed by organisations to improve the use of EBP frequently included educational activities such as small group practical sessions. The use of pocket cards and even learning ‘enforced by management’ was also used as a means of implementing EBP (Petzold et al., 2014).
Knowledge translation also gave the clinician a professional identity and confidence that enabled and encouraged the further seeking out for evidence based changes to their clinical practice (Foster et al., 2015). The action of incorporating evidence into practice was reported to enhance their credibility and increased their confidence in the workplace, which in effect made the clinician more able to seek out evidence-based approaches (Bowden et al., 2012; Foster et al., 2015).
Domain: Beliefs About Capabilities
Some clinicians were reported to lack confidence and default to areas of practice that they were familiar with, placing significant value on their clinical reasoning over newly generated evidence (Cahill et al., 2021; White et al., 2021). For example, Cahill et al. knowledge translation study in 2021 with occupational therapists and physiotherapists implementing upper limb sensory rehabilitation after stroke and Foster et al., in 2015, who provided an understanding of speech pathologists role in EBP for acute post stroke aphasia.
There was also some hesitancy when faced with something new, with clinicians reporting pressures to perform about ‘doing it right’ and allowing research alone to drive their practice. There was a fear of a poor outcome resulting in perceived ramifications if not done right (Foster et al., 2015), and some studies reported a general reluctance to change practice or engage with research (Petzold et al., 2014). Clinicians were concerned that they were fulfilling requirements for EBP rather than using patient centred care (Harding et al., 2014; Klaic et al., 2019). Foster et al. also described a sense of disempowerment and disconnection among speech pathologists with the concept of EBP (Heiwe et al., 2011). Clinicians felt that they were limited in applying EBP due to the influences of others e.g., some patients and other health professionals that influenced allied health service delivery (Petzold et al., 2014; White et al., 2021). In some cases, clinicians felt that EBP did not add anything new or relevant to their current practice (Hadely et al., 2014).
Clinicians that were motivated and had a sense of intrigue of research, were more likely to enthusiastically adopt evidence into practice. Intrinsic motivation was reported to facilitate the use of EBP in clinical practice which gave the clinician more confidence (Mickan et al., 2019; Moran & Davis, 2020; White et al., 2021). This was supported using guidelines that helped increase the use of evidence-based interventions by rationalising and improving clinical practice which was supported and valued by management (Foster et al., 2015; Hadely et al., 2014; Moore et al., 2018).
Domain: Social Influences
Clinicians were reported to have varying levels of indifference towards evidence-based decision-making (Hadely et al., 2014). Participants in the study by White et al., in 2021 cited those participants regarded the patient experience as far more important than published evidence. However, the translation of knowledge into clinical practice was facilitated by the influence of work colleagues and well-informed patients. This was particularly the case if work colleagues were ‘respected’ and supportive of practice change. The use of mentoring, champions and involvement in research or implementation projects was found to have great impact on staff (Bennett et al., 2016; Cahill et al., 2021; Foster et al., 2015; Miao et al., 2015). The use of team-based mentoring on projects and one on one mentoring by research supervisors and the use of Research and Evidence in Practice (REP) Champions was found to enhance the use of EBP by occupational therapists (Bennett et al., 2016; Caldwell et al., 2008).
Clinicians often sought out their professional groups as a significant resource on evidence-based practice (Klaic et al., 2019). Studies reported the importance of group conformity and the need to ensure that sufficient health care professionals were invested in evidence-based practice and generated pride in the department as a group (Bennett et al., 2016; Demers et al., 2015). Clinicians were also influenced by any variances in work practices remaining in keeping with society norms and expectations (White et al., 2021).
Domain: Skills
Skills in the appraisal and application of research were frequently reported in the studies (n = 7). Hadely et al., in 2014 reported a reluctance for the use of evidence based clinical practice guidelines by speech pathologists were that they were not in line with their own practice and had insufficient skills. Occupational therapists and physiotherapists were overwhelmed by the weight of responsibility of getting any new evidence based clinical practice right for the patient, without the development and confidence of practicing the new skill, as reported by Cahill et al., in 2021, in the study across eight different health organisations in Australia. This was reinforced by Klaic et al., in 2018, where seven allied health professional groups were studied to explore the attitudes to EBP using the theory of planned behaviour who reported a loss of EBP skills.
Clinicians felt that they lacked the opportunities to ‘upskill’ and consolidate training that they had done within the organisation (Cahill et al., 2021; Hadely et al., 2014; Petzold et al., 2014). It was also reported that they lacked the confidence to implement any training which was further confounded by the degradation of their skills due to lack of clinical practice and the feeling of being overwhelmed for those clinicians trained prior to the use of electronic databases (Cahill et al., 2021; Hadely et al., 2014; Harding et al., 2014; Klaic et al., 2019).
In contrast, clinicians reported that training provided through dedicated time and programs enabled the development of the use of EBP (Bennett et al., 2016; Petzold et al., 2014). This was enhanced by incorporating organisational change training, the tailoring of knowledge for different end users and consolidation of skills through exposure to relevant patients (Cahill et al., 2021; Petzold et al., 2014; Soguel et al., 2019).
Domain: Optimism
Some studies reported that there was some pessimism among clinicians using EBP (Bowden et al., 2012; Demers et al., 2015; Foster et al., 2015; Gudjonsdottir et al., 2017; Hadely et al., 2014; White et al., 2021). For example, White et al., in 2021, when aligning weekend allied health resource allocation to evidence-based policy recommendations. Clinicians considered that research was frequently carried out but did not always translate into clinical practice, was not valued and was incompatible with current needs (Bowden et al., 2012; Foster et al., 2015; Hadely et al., 2014). However, studies reported that participants perceived departments that advocate EBP were more beneficial to patient care and were received well by the patients themselves (Bennett et al., 2016; Mickan et al., 2019).
Domain: Beliefs About Consequences
The consequences of evidence translation were reported as burdensome due to the need of continual updating and anticipation of conflicting evidence emerging in the future (Bowden et al., 2012; White et al., 2021). One of the five themes from White et al., in 2021 was a fear of complaints in relation to changing weekend allied health service provision. Complaints were considered time consuming, and participants were wary of changes to a well-established service delivery model reflecting poorly on clinicians. There were also concerns about the evidence not considering the limitations of clinical practice (White et al., 2021). Although, outcome expectancies were favourable. Participants in three studies reported that they were highly motivated to optimize service provision and considered that health outcomes for patients were beneficial and reduce the potential risk (Bowden et al., 2012; Foster et al., 2015; Heiwe et al., 2011).
Other Domains
Other barriers reported in the studies included overload of evidence, much of which was not regarded as relevant to clinicians clinical practice (Hadely et al., 2014). This resulted in clinicians wanting to verify results themselves prior to using new evidence, prioritising clinical care over EBP activities or regarding guidelines as not relevant to their area of work (Hadely et al., 2014; Harding et al., 2014; White et al., 2021). The fear of change was reported if there was a potential to impact on services, or if the clinician had a restricted concept of EBP (Foster et al., 2015; White et al., 2021). Clinicians regarded EBP as ‘an aspirational goal rather than a reality in their practice.’ (Foster et al., 2015).
The use of reinforcement was reported to be a useful facilitator. Tools such as auditing to inform clinicians were found have a positive effect (Bennett et al., 2016; Foster et al., 2015; Miao et al., 2015). Clinical supervision, mentoring and internal or external support promoting EBP were also perceived as enablers to translating evidence into clinical practice (Foster et al., 2015). There was also a general reluctance to change practice or engage with research (Petzold et al., 2014). It was felt that fulfilling requirements was not addressing the needs of the patient or part of the clinical role (Harding et al., 2014; Klaic et al., 2019). Foster et al. described a sense of disempowerment and disconnection among speech pathologists, with the concept of fulfilling requirements (Bowden et al., 2012; Heiwe et al., 2011; White et al., 2021).
Discussion
Summary of Findings
This systematic review reinforces the importance of environment, context, and resources as barriers to implementing EBP for allied health professionals. We also identified the influence of the factors: knowledge, social influences, and beliefs about consequences. Frequently, the expectation was placed upon the individual clinician to implement EBP, which was only enabled when supported by the organisation or staff in leadership roles. This review complements the current research by Smith and Johnson (2023) (Smith & Johnson, 2023), but is differentiated by focusing specifically on allied health disciplines within the public hospital setting and by mapping implementation determinants to a behaviour change framework.
Knowledge
Clinical practice guidelines provide the basis of evidence-based practice. However, allied health professionals frequently find guidelines unrealistic and impractical in the day-to-day workplace. In addition, clinicians were unsure as to how to translate guidelines into practice because of too much information, too many recommendations or lacked specificity (Halls et al., 2021). Several studies reported that clinicians felt EBP lacked relevance to daily practice and that there was a conflict between guidelines and the reasoning of professionals based on experience (Bowden et al., 2012; Foster et al., 2015; Petzold et al., 2014). As a result, the responsibility of adoption of guideline recommendations has fallen on the shoulders of the individual clinician. In most situations, clinicians have taken up the challenge to change practice according to the latest EBP but this reliance on the diligence of clinicians could potentially result in unwarranted variations in clinical care (White et al., 2021). The use of implementation recommendations could improve the uptake of clinical practice guidelines by enabling sufficient change to close the gap between evidence and service delivery and therefore make them more implementable (Sarkies et al., 2022).
Allied health professionals commonly consider EBP as a purely academic exercise that has no effective strategy for their implementation (Goorts et al., 2021). Evidence needs to be tested in the real world to ensure external validity, as well as effectiveness studies to address internal validity. Implementation studies require transportable theory and context to be applied so that dissemination takes into account relevant social, cultural, contextual conditions and thus provide ecological validity to any intervention strategies. (Goorts et al., 2021).
This review confirms that many aspects of the research process and reporting were regarded as a knowledge barrier, e.g., limited understanding in statistical interpretation, and this resulted in the reliance of local internal data and anecdotal staff experiences (Smith & Johnson, 2023; White et al., 2021). Scott et al., in 2012 reported a clear demonstration that education alone has a limited impact on changing clinicians clinical practices and behaviours (Scott et al., 2012). They described the implementation process as a ‘complex and layered factor in embedding translational research’, and later by Goorts et al., in 2021, which called for interventions that are multi-faceted which incorporate the effectiveness of an intervention by measuring changes in patient outcomes (Goorts et al., 2021; Smith & Johnson, 2023). However, it is also imperative to report in this review that local strategies such as working with students was an effective way to keep up to date, and the use of activities of Journal Clubs do have a place (Bennett et al., 2016; Halls et al., 2021). It is also essential, regardless of which implementation strategies are selected, that they are relevant to the local context and ensure that detailed reporting ensues (Harvey & Kitson, 2016).
There is also considerable discrepancy related to the recency of clinicians’ education. Those clinicians who had less experience but had recency of their education were much more trusting of clinical practice guidelines (Halls et al., 2021). McEvoy et al. also reported in 2010 a variation between allied health professions knowledge in EBP (McEvoy et al., 2010). In some cases, clinicians, namely physiotherapists and occupational therapists, felt they had been unprepared by their university training for implementing EBP (Cahill et al., 2021). For example, Upton (2006) reported a lack of confidence in research skills and their application within the physiotherapists, occupational therapists, podiatrists and radiographers (Upton & Upton, 2006).
Social Influences
Social influences played an important role in the implementation of EBP; both as enabler and barrier. The role of leadership within the team and within the organisation performed an influential role in whether EBP was implemented. Leadership can start from the simple action of junior staff seeking out senior staff to back up initiatives, or when senior staff are regarded as ‘change leaders’ through research experience, leading to a positive impact on implementing EBP (Halls et al., 2021; Smith & Johnson, 2023). The influence of leadership also prevents negative attitudes infiltrating the team by managing workload and providing training opportunities to enable implementation (Halls et al., 2021). As reported in the study by Moran and Davis (2020), success relies on the workplace culture and those around them feeling valued and supported (Moran & Davis, 2020). However, this is reliant on interpersonal processes and whether clinicians supported the proposed practice change, as reported in the study by Cahill in 2021. The ‘knowledge broker’ or knowledge translation (KT) champion, has been reported in studies as an implementation strategy (Sarkies et al., 2021; Smith & Johnson, 2023). The use of KT champions and allied health research positions, where clinicians have been upskilled through mentoring, has resulted in an increased uptake of evidence-based practice, enhanced the research infrastructure, and improved workplace culture and professional development (Smith & Johnson, 2023). Although, Sarkies et al. were unable to determine differences when a knowledge broker was used to align weekend allied health services with currrent evidence using a randomised controlled implementation trial design (Sarkies et al., 2021), reporting that future research should incorporate greater focus on internal organisational relationships with the knowledge broker and encourage more anlytical thinking when confronted with conflicting evidence.
Allied health professionals frequently work within a complex organisational structure especially as members of interprofessional teams. Therefore, behaviour change can be complex and difficult with a number of competing factors (Scott et al., 2012). Group dynamics were often stated as an influence in the implementation of EBP: group conformity was a positive influence with sharing of new knowledge or pride in being part of the department. However, group conflict could also be a potential negative influence occurring with clinicans of difffering health professions opinions creating a barrier to EBP implementation (Bennett et al., 2016; Mickan et al., 2019). A collaborative team was found to result in shared empowerment, adherence to guidelines and clinical decision making, as opposed to siloed disciplines across the multidisciplinary team which can inevitably impact on communication across the team (Halls et al., 2021). However, these collaborative teams are rarely in place due to structural barriers.
Beliefs About Consequences
The TDF domain, beliefs about consequences, describes the ‘acceptance of the truth, reality, or validity about outcomes of behaviour in a given situation’ (Atkins et al., 2017). Bowden et al., in 2012 found that when the EBP was consistent with the values and needs of the clinician, then the EBP was implemented and it was considered, by the clinicians, as validation of their current practice (Bowden et al., 2012). This was also confirmed by Foster and Worrall in 2015, where for ‘passionate clinicians’ it reiterated that they were doing the best they could clinically for their patients (Foster et al., 2015). However, Goorts et al. reported a lack of focus on patient centred outcomes in studies looking at evidence based recommendations and guideline adherence (Goorts et al., 2021). The lack of consequences or outcomes to the use of EBP in the real world or in the clinicians’ clinical practice could potentially create a barrier to its use. Clinicians strongly support EBP when they believe in the benefits for the patients, and express a strong motivation to implement the recommendation (Demers et al., 2015).
White et al. concluded that one of the barriers to implementing EBP is the lack of personal authority to promote change (White et al., 2021). In this study, it was reported that participants were reluctant to change because they anticipated ‘additional, future conflicting evidence’ that supported the change. However, the reasons behind the barriers to beliefs about consequences are multifaceted with clinicians stating concerns as a result of insufficient knowledge, support and ultimately if the implementation fails, then this could ultimately result in the perceived failure of the individual clinician (Heiwe et al., 2011; White et al., 2021). It is important that clinicians have the support of leadership and the organisation, as described by Smith and Johnson (2023), so that leaders are able to demonstrate the value of EBP through patient data outcomes in real terms (Smith & Johnson, 2023).
Allied health professionals are passionate about patient centred care, however, their awareness of EBP is varied across the professions and there is little clarity over the training and processes for EBP across the disciplines (McEvoy et al., 2010). There is also some concern by clinicians that evidence-based knowledge is not relatable to clinical settings and has little relevance to the patient (Heiwe et al., 2011; Scurlock-Evans et al., 2014). Therefore, barriers and enablers to translating evidence into clinical practice should be considered interconnected.
Strengths and Limitations
This review is the first to focus on allied health professionals and the factors that influence translation of evidence into clinical practice using behaviour change theory. The scope of the review was clear with predefined inclusion and exclusion criteria and the search strategy was applied to multiple databases, with a manual search of reference lists of retrieved articles. Data extraction was done independently by separate reviewers and discussed with a third reviewer if there was any disagreement. The use of qualitative narrative synthesis allowed the author to explore the complexity of interventions used while recognizing the heterogeneity of the primary studies included in this review.
The small number of allied health professions represented in the studies reviewed means that it cannot be generalisable to other allied health professions. The main intervention used within many of the studies was focused on educational strategies of the individual clinician with results found to be inconclusive or largely ineffective. However, there was little evidence on alternative intervention strategies and therefore this review was unable to discuss the use of more effective strategies. The studies selected were found to be mainly based in metropolitan areas, as there was limited data reported in rural areas. Therefore, this review is only reflective of allied health working in metropolitan public hospitals.
Future Research and Practice
There is an increasing emphasis on the use of behaviour change theory and further research is required to understand knowledge translation in allied health professions. Behaviour change theory provides a systematic approach to inform interventions in evidence-based practice. It also provides frameworks that are reproducible and will therefore lead to consistency in their use across the allied health professions and settings.
There is a paucity of information on knowledge translation of evidence within the allied health professions as a whole, and specifically, within each discipline. More research is required in investigating the extent to which EBP is used and what are the barriers and enablers to its use in clinical practice. Future research on implementing and sustaining EBP, which involves organisational support should be initiated, and investigating evidence translation in rural areas should be considered a priority.
Conclusions
Research confined to a few allied health professions provides a limited picture of the implementation of EBP. The use of TDF has demonstrated that implementation of EBP is a multifaceted, complex issue, demonstrating that the clinician needs to know about EBP, understand it and know that it will benefit the patient before implementation. Current strategies have focussed on educating the individual, with minimal support from the organisation. This is not getting evidence into practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.