
Abstract
The Brief COPE Inventory is a widely used scale that measures how a person copes with a specific situation. Despite its widespread use, the factor structure of this scale is somewhat unclear and has not been tested among patients pursuing bariatric surgery. We tested competing factor analytic models of the Brief COPE Inventory among patients pursuing bariatric surgery to identify the best fitting factor model for use in pre-surgical psychological evaluations. We also examined reliability and validity of the subscales from the best fitting model of coping. Participants included 1984 patients pursuing bariatric surgery (Mage = 42.58 years, SD = 10.89, 81.39% female). The best fitting model of the Brief COPE Inventory among patients pursuing bariatric surgery was a three-factor model including interpersonal, intrapersonal, and maladaptive coping strategies. These results were replicated in a subset of the original sample and demonstrated appropriate convergent and discriminant validity with several key outcomes. The Brief COPE Inventory can be conceptualized as a multidimensional scale assessing interpersonal coping, intrapersonal coping, and maladaptive coping among patients pursuing bariatric surgery. Future work should examine how these subscales are related to surgical outcomes among people receiving treatment for excess weight.
Introduction
The Brief COPE Inventory is one of the most commonly used self-report assessment tools to measure how people tend to cope with stressful situations (Solberg et al., 2022). The Brief COPE Inventory was developed as a brief alternative to the original 60-item version to improve its utility in clinical and research settings. The original 60-item version of the COPE Inventory measured 15 distinct aspects of coping, including planning, restraint, and venting among several other methods (Carver et al., 1989). The Brief COPE Inventory consists of 28 statements regarding how people may cope with stress, and it is broken down into 14 2-item factors (Carver, 1997). Several studies have examined the factor structure of the Brief COPE Inventory among specific health psychology populations, including women with postpartum depression (Azale et al., 2018), patients with breast cancer (Fletcher et al., 2006), patients pursuing liver transplant (Amoyal et al., 2016), and several other populations. However, individual studies often modify the scale to suit their needs or sample characteristics; thus, a clear factor structure of the Brief COPE Inventory is difficult to determine (Solberg et al., 2022). Because sample characteristics may be critical in determining appropriate use of the scale, testing the factor structure of the scale is essential in ensuring its appropriate use in clinical practice.
Previous research has found several possible factor structures of the Brief COPE Inventory. Numerous studies found adequate fit of the original 14-factor conceptualization (Ashktorab et al., 2017; Dias et al., 2009; Garcia et al., 2018), but few studies have conducted confirmatory factor analyses to determine if a different model provides better fit to the data. In a sample of pregnant women, a higher-order model was identified as the best fitting model, which collapsed the 14 factors into three higher-order factors (active, social support, and disengaged coping; Peters et al., 2020). In a sample of females with postpartum depression, the 14-factor structure was collapsed into three factors (problem-focused, emotion-focused, and dysfunctional/avoidant coping; Azale et al., 2018). In addition to confirmatory approaches, numerous studies employed exploratory approaches, with the most commonly identified factor structure including two opposing methods: approach and avoidant coping styles (see Solberg et al., 2022 for a review). In addition to the two-factor structures identified, three-factor structures identified across studies generally include active coping, social support, and disengaged coping.
In addition to the relatively unclear factor structure of the Brief COPE Inventory within health psychology, external validity of the subscales remains unclear. Prior research shows that the 14 subscales of the Brief COPE are generally weakly correlated, with substance use and religion subscales having the lowest correlation, while active coping and planning correlating more strongly (Nahlen Bose et al., 2015). Adaptive coping strategies (e.g., positive reframing, planning) tend to be positively correlated to social functioning and well-being and negative correlated to schizophrenia symptoms (Meyer, 2001) while maladaptive coping strategies (e.g., denial, self-blame) tend to be positively associated with depression symptoms and negatively associated with well-being among people in psychiatric inpatient units. Avoidant coping styles, generally defined as a composite of behavioral disengagement items, substance use items, and denial items, was negatively related to physical health among patients with coronary heart disease (Nahlen Bose et al., 2015). However, other coping styles did not correlate to health status. Among a sample of women with breast cancer, eight-week test-retest reliability was highly variable among the subscales of the Brief COPE Index, with correlations ranging from zero to 1, with a median correlation of .445 (Yusoff et al., 2010). Internal consistency was also highly variable, with Cronbach alpha ranging from .25 to 1.00. Overall, the Brief COPE Index has questionable psychometric properties, which suggests the need for additional studies further exploring this measure.
Despite its widespread use in health psychology, psychometric properties of the Brief COPE Inventory have not been examined among patients pursuing bariatric surgery. Identifying statistically supported models of coping that include theoretically based coping themes among these patients is important for several reasons. First, most of the research examining coping among patients pursuing bariatric surgery or patients who have undergone bariatric surgery has focused on how people would cope with a hypothetical situation (e.g., limiting overeating when watching television) rather than focusing on using psychometrically sound measures of coping (Bergh et al., 2016; Latner et al., 2013). Hypothetical coping can be especially concerning as it may be influenced by socially desirable responding or responding in a way a person believes they should respond to stress. Second, psychometrically sound models of coping allow researchers and clinicians to identify empirically based themes in how a person copes with stress that may be more meaningful than specific strategies. For example, knowing that a person tends to cope with stress by reaching out to others may be more important for clinicians to know since clinicians can directly translate this coping theme into practice by helping the patient expand their social support network. Identification of these themes may be especially important in examining health-related outcomes among smaller samples or harder to access populations. Third, despite the lack of psychometric evidence of the Brief COPE Inventory in patients pursuing bariatric surgery, this scale is frequently used in clinical practice. The goal of the current study is to identify the best fitting factor structure of the Brief COPE Inventory among patients pursuing bariatric surgery and examine external validity of the coping subscales from the best fitting model. By pinpointing a psychometrically sound model of coping among patients pursuing bariatric surgery, clinicians can employ use of such a model into their clinical practice to better understand how their patients tend to cope with stress and recognize areas for potential intervention with patients who tend to engage in unhelpful coping mechanisms.
To identify the best fitting model of the Brief COPE Inventory among patients pursuing bariatric surgery, we identified four possible models to examine based on theoretical conceptualizations in the literature. Model 1 is the widely used 14-factor model with two items per factor, as described by Carver (Carver, 1997; Figure S1a). Despite its widely accepted use, model one has not been tested in a sample of patients pursuing bariatric surgery. Model 2 collapses the data into two higher-order factors, measuring adaptive and maladaptive coping (see Figure S1b), which is often informally used in clinical practice to identify whether patients tend to manage their stress well. Model 3 collapses the data into three higher-order factors (emotion-focused, problem-focused, avoidant coping; Azale et al., 2018; Figure S1c). Model 4 collapses the data into three higher-order factors (interpersonal, intrapersonal, and maladaptive coping; Solberg et al., 2022; Figure S1d). We hypothesized that model 2 would fit the data better than model 1, due to the vast body of literature supporting a two-factor model of coping (Solberg et al., 2022). We also hypothesized that models 3 and 4 would fit the data better than model 2 due to their emphasis on differences within approach or adaptive coping styles, such as recognizing differences in whether people focus on emotional or active aspects of coping or whether people prefer to be self-reliant or reach out to others when dealing with stress. The final aim of this study was to examine reliability and validity of the subscales from the best-fitting model.
Method
Procedure and Measurements
Patients enrolled in the bariatric surgery program at [Masked for review] Academic Medical Center between April 2018 and October 2022 completed a brief psychological questionnaire prior to their mandatory pre-surgical psychological evaluation appointment. Patients provided self-report information on their race, ethnicity, gender, age, height, weight, education, and patients completed several self-report measures on anxiety, depression, coping, eating habits, and several other psychological constructs. This study was approved by the [masked for review] institutional review board.
Brief COPE Inventory
The Brief COPE Inventory is a 28-item self-report scale that measures a person’s engagement in different ways to cope with a stressful situation. Items on this scale are rated from 1, I haven’t been doing this at all, to 4, I’ve been doing this a lot. The dispositional version of the Brief COPE Inventory, where items are rated based on how a person generally copes with stress was used in the current study. While the factor structure of the Brief COPE Inventory is somewhat mixed, the scale in general is considered a valid and reliable tool to measure coping. Regarding the factor structure, numerous studies have found adequate fit of Carver’s 14-factor model using traditional fit indices (Dias et al., 2009; Garcia et al., 2018; Monzani et al., 2015). However, several studies have found alternative factor structures that fit data well (see introduction for a review). The subscales of the Brief COPE Inventory have good internal consistency, with item correlations ranging from r = .50 to .90 across subscales (Carver, 1997). Test-retest reliability for the Brief COPE Inventory is widely variable (Yusoff et al., 2010). Validity evidence, while somewhat limited, suggests that maladaptive coping strategies tend to positively correlate with psychopathology symptoms (Meyer, 2001) and adaptive strategies correlate with well-being. Avoidant coping strategies have also correlated with negative health outcomes (Nahlen Bose et al., 2015).
Three Factor Eating Questionnaire
The three-factor eating questionnaire (TFEQ; Stunkard & Messick, 1985) is a 51-item self-report scale measuring cognitive restraint of eating, disinhibited eating, and hunger. Items 1–36 are rated in a true/false format and 15 items that are recoded into a 0/1 format. The subscales have fair to excellent internal consistency across samples of patients with overweight/obesity (Karlsson et al., 2000; Stunkard & Messick, 1985). Internal consistency in the current sample was good for restraint and hunger, αs = .81 and .82, respectively, and adequate for disinhibition, α = .65.
Beck Anxiety Inventory
The BAI, (Beck & Steer, 1993) is a 21-item self-report tool to measure anxiety symptoms. Items are rated from zero to 3, with higher scores indicating higher levels of anxiety over the past two weeks. Scores from zero to 7 indicate minimal anxiety, 8 to 15 indicate mild anxiety, 16–25 indicate moderate anxiety, and 26 to 63 indicate severe anxiety. The BAI has excellent internal consistency among patients pursuing bariatric surgery (Marek et al., 2016). Internal consistency in the current sample was excellent, α = .92.
Beck Depression Inventory-II
The BDI-II (Beck et al., 1996) is a 21-item self-report measure of depression. Items are rated from zero to 3, with higher scores indicating higher levels of depression over the past two weeks. Scores of 13 or less indicate minimal depression, 14–19, mild depression, 20–28 indicating moderate depression, and 29–63 suggesting severe depression. The BDI-II has excellent internal consistency in a sample of patients pursuing bariatric surgery (Hall et al., 2013). Internal consistency in the current sample was excellent, α = .93.
Data Analysis
All analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC). Descriptive statistics were reported using means and standard deviations for continuous variables, and frequencies and valid percentages for categorical variables. Data were randomly divided into two samples using a 65%/35% split (Development subsample N = 1290, Validation subsample N = 694) to allow confirmation of the identified best fitting model since there were no concerns for reduced statistical power given the large sample size. Data were then transformed into polychoric correlation matrices for analysis due to the ordinal items of the scale. Transforming Pearson correlations to polychoric correlation allows researchers to use traditional model estimation methods while accounting for the ordinal nature of individual scale items (Kline, 2016). A series of structural equation models using the original subscales, subscales using the higher-order models, and then correlated errors in place of subscales, and finally the models on the correlated errors instead of subscales were run and reported on the development sample using Full Information Maximum Likelihood (FIML) estimation. We standardized each model to have each latent factor with a mean of zero and a standard deviation of 1 for model identification. Using Kline’s (2016) method for evaluating model fit for confirmatory factor analysis, we ran several competing models. We conducted chi-square difference tests between nested models to identify which models best fit the data. We examined global fit by examining the Chi-square statistics for each model. However, as Chi-square statistics tend to be overpowered, models failing this test are tentatively rejected, pending review of residual fit indices and comparison to alternate models (Kline, 2016). Next, we examined the local fit of each model by reviewing residual statistics for any correlational residuals exceeding an absolute value of .10 accompanied by a statistically significant standardized residual statistic. Finally, we reported traditional model fit indices of each model examined. Importantly, the values of traditional fit indices should be interpreted with caution, as the value of traditional fit indices are a function of the parameter estimates in the models (Kline, 2016). The following are generally used as guidelines/cutoffs indicating good model fit for traditional fit indices: RMSEA < .08, SRMR < .05, CFI > .90, and AGFI > .90. The final model was then run on the validation sample to verify fit.
In addition to identifying the best fitting model of coping among patients pursuing bariatric surgery, we examined reliability and validity of the identified subscales. Specifically, we examined Cronbach’s alpha levels of each subscale to determine whether subscales had adequate internal consistency. We then ran a structural equation model with the Brief COPE subscales as predictor latent variables and observed anxiety, depression, and eating habits as outcome variables to examine convergent and discriminant validity of the coping subscales.
Results
Participants
Demographic Characteristics
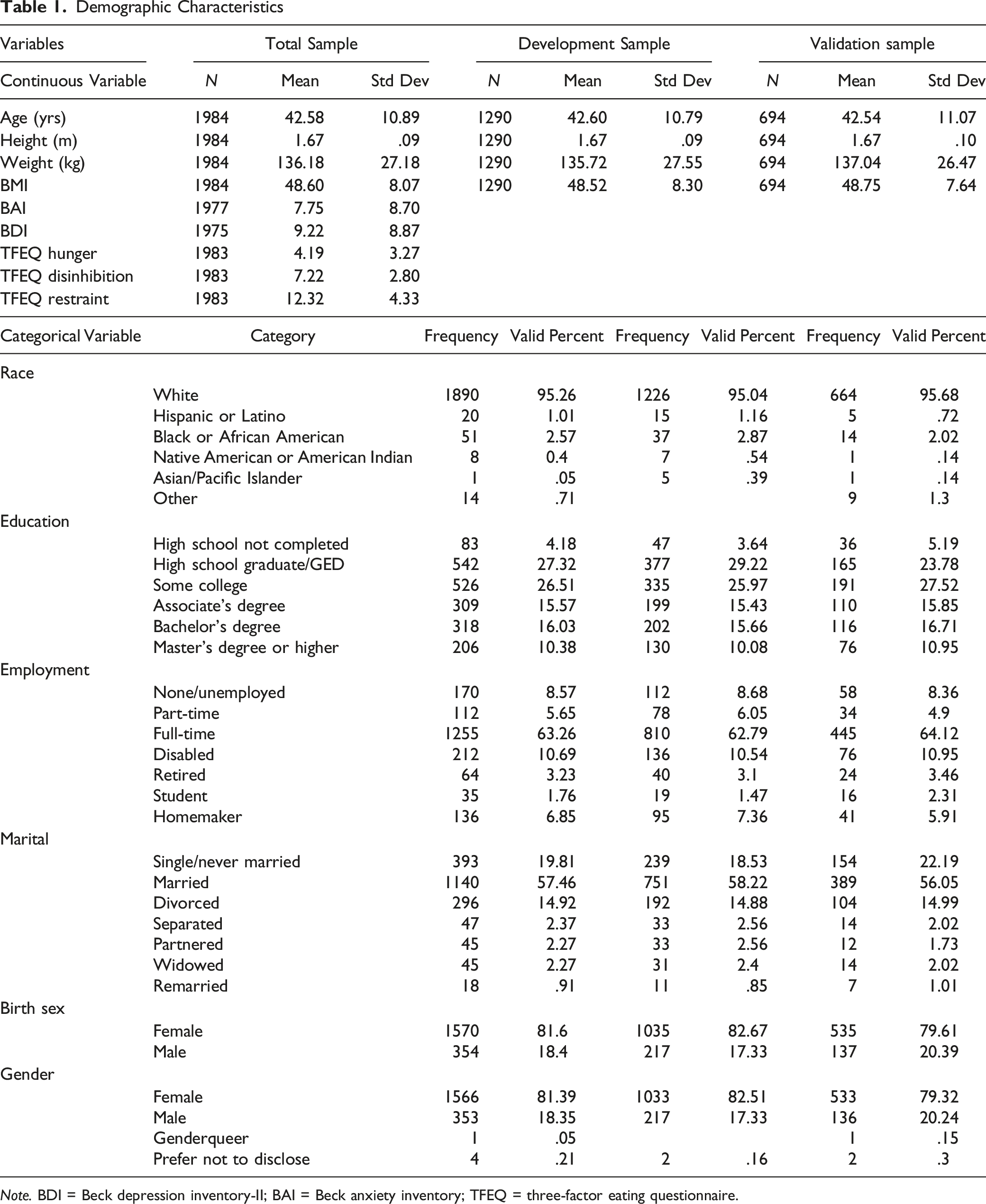
Note. BDI = Beck depression inventory-II; BAI = Beck anxiety inventory; TFEQ = three-factor eating questionnaire.
Development Subsample
Model 1
Traditional Fit Statistics for all Models
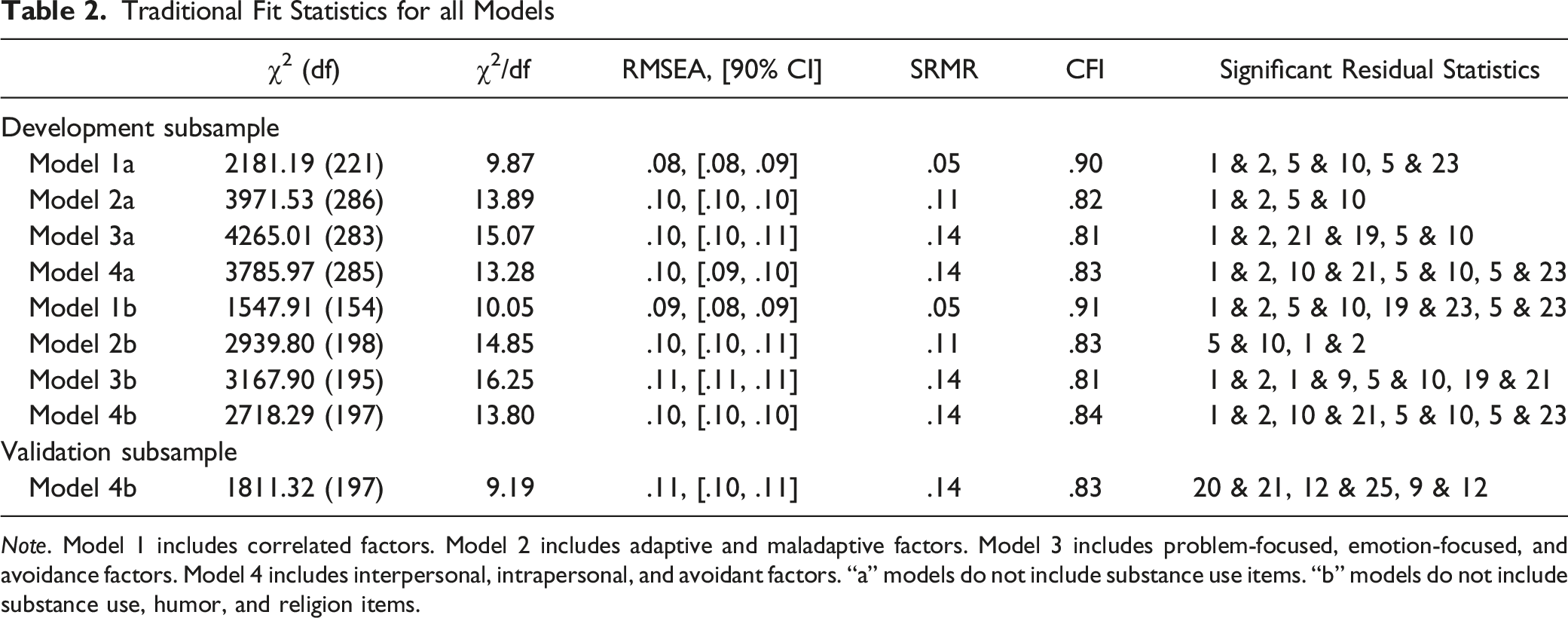
Note. Model 1 includes correlated factors. Model 2 includes adaptive and maladaptive factors. Model 3 includes problem-focused, emotion-focused, and avoidance factors. Model 4 includes interpersonal, intrapersonal, and avoidant factors. “a” models do not include substance use items. “b” models do not include substance use, humor, and religion items.
This model was also run with 11 factors (dropping substance use, humor, and religion items; model 1b). The humor and religion items (items 18, 28, 22, and 27) were dropped from analysis due to participants generally rating items as either high or low, which impacted variability. Similar to the 13-factor model, this model converged with error messages. The model failed the exact fit test, χ2 (154) = 1547.91, p < .0001. Furthermore, this model had four out of 231 (1.73%) correlational residuals associated with statistically significant standardized residual statistics, AIC = 1745.91, AGFI = .84, RMSEA = .09, CFI = .91. Again, due to the error messages and significant chi-square value, this model yielded poor fit to the data (see Table 2 for additional fit indices).
Cronbach’s alphas across the various subscales yielded generally good internal consistency. Values for each subscale are as follows: active coping = .71, planning = .73, positive reframing = .67, acceptance = .62, humor = .76, religion = .88, self-distraction = .52, using emotional support = .81, using instrumental support = .77, venting = .61, denial = .67, substance use = .80, behavioral disengagement = .57, and self-blame = .74. These values indicate that, while most subscales have good internal consistency, six of fourteen subscales have acceptable or poor internal consistency.
Model 2
To address issues with models having non-positive definite covariance matrices, we ran each of the remaining models with errors among subscale items allowed to correlate rather than modeling subscales. 1 Model two, the two-factor model, included adaptive and maladaptive coping. Model 2a (dropping substance use items) failed the exact fit test, χ2 (286) = 3971.53, p < .001, AIC = 4100.53, AGFI = .76, RMSEA = .10, CFI = .82. However, this model only had two statistically significant correlational residuals out of 325 (.62%), suggesting that the model has good local fit. Model 2b (dropping substance use, humor, and religion items) also failed the exact fit test, χ2 (198) = 2939.80, p < .001, AIC = 3049.80, AGFI = .78, RMSEA = .10, CFI = .83. Similarly, this model also had only two statistically significant correlational residuals out of 231 (.87%), suggesting good local fit (see Table 2 for traditional fit indices). Because models 1a and 1b converged with numerous error messages, we were unable to test our hypothesis that model 2 provided better fit to the data than model 1. Internal consistency for the subscales in this sample was adequate to good. Cronbach’s alphas for the subscales are as follows: adaptive = .89, adaptive (without humor and religion items) = .89, and maladaptive = .72.
Model 3
Model three was a three-factor model, including emotion-focused, problem-focused, and avoidance coping. Model 3a (dropping substance use items) failed the exact fit test, χ2 (283) = 4265.01, p < .001, AIC = 4401.01, AGFI = .76, RMSEA = .10, CFI = 81. This model had three (0.92%) significant correlational residuals, suggesting good local fit. While not nested, model 2a appeared to fit the data better than model 3a, with model 2a having a smaller Chi-square statistic, lower SRMR< and higher CFI values in addition to a lower number of statistically significant correlational residual statistics. Model 3b (dropping substance use, religion, and humor items) also failed the exact fit test, χ2 (195) = 3167.90, p < .001, AIC = 3283.90, AGFI = .76, RMSEA = .11, CFI = .81. This model had four (1.73%) significant correlational residuals, suggesting good local fit. Because models 2 and 3 were not nested, we were unable to hypothesis test to determine the best fitting model. However, model 2b appeared to fit the data better than model 3b, with model 2b having a smaller Chi-square statistic, lower SRMR, and higher CFI values in addition to a lower number of statistically significant correlational residual statistics compared to model 3b. Internal consistency for the subscales was adequate to good. Cronbach’s alphas for the subscales are as follows: emotion-focused = .77, emotion-focused (without humor and religion items) = .76, problem-focused = .83, and avoidance = .74.
Model 4
Model four is a three-factor model including interpersonal, intrapersonal, and maladaptive coping. Model 4a (dropping substance use items) failed the exact fit test, χ2 (285) = 3785.97, p < .001, AIC = 3917.97, AGFI = .77, RMSEA = .10, CFI = .83. This model had four (1.23%) correlational residual statistics exceeding an absolute value of .10 associated with statistically significant standardized residual statistics, which suggests good local fit. Furthermore, this model fit the data significantly better than model 2a, Δχ2 (1) = 185.56, p < .001, thus model 4a was retained as having the best fit to the data (see Table 2 for traditional fit indices), which supports our hypothesis that model 4a produced better fit to the data than model 2a.
Model 4b (dropping substance use, humor, and religion items) also failed the exact fit test, χ2 (197) = 2718.29, p < .001, 2830.29, AGFI = .79, RMSEA = .10, CFI = .84. This model also had four residual statistics of note (1.73%), suggesting good local fit. Similarly, model 4b fit the data significantly better than model 2b, Δχ2 (1) = 221.51, p < .001, thus model 4b is retained as having the best fit to the data (see Table 2 for traditional fit indices), which supports our hypothesis that model 4b produced better fit to the data than model 2b. Internal consistency for the subscales was adequate to good (i.e., higher than .70 and .80 respectively; Cortina, 1993). Cronbach’s alphas for the subscales are as follows: interpersonal = .82, intrapersonal = .83, intrapersonal (without humor and religion items) = .84, and maladaptive = .71.
Validation Subsample
Model 4b was retained as having the best fit to the data among the development subsample, thus we ran this model in the validation subsample to ensure the results were replicated. In the validation sample, model 4b failed the exact fit test, χ2 (197) = 1811.32, p < .001, AIC = 1923.32, AGFI = .76, RMSEA = .11, CFI = .83. However, the model only had three correlational residual statistics exceeding an absolute value of .10 corresponding to statistically significant standardized residual statistics (1.30%), which suggests good local fit. Importantly, the residual statistics of note in the validation sample are not the same as those identified in the development sample. The lack of consistency between the two samples in recommended areas for model improvement suggest that the residual statistics may indicate coincidental relationships among items rather than warranting model modification to address these minor areas of model misfit. Overall, model 4b was retained as having overall good fit to the data in the validation sample (see Table 2 for additional traditional fit indices).
Parameter Estimates of the Final Model
In the final model (model 4b) in the development sample, each of the items loaded significantly into the hypothesized factors, with parameter estimates ranging from .17 to .91 (Figure 1(a)). The latent factors of interpersonal and intrapersonal coping are strongly correlated, r = .78, p < .001; however, maladaptive coping was not related to either interpersonal or intrapersonal coping. In the validation sample, each of the items loaded significantly onto the hypothesized factors as well, with parameter estimates ranging from .15 to .93 (Figure 1(b)). Similarly, the latent factors of interpersonal and intrapersonal coping are strongly related, r = .79, p < .001, and maladaptive coping was not related to either interpersonal or intrapersonal coping. Overall, these results suggest that each of the items load significantly onto their proposed factors, which indicates that they are important in understanding themes in coping. Final Model in Development Sub-Sample (a) and Validation Sub-Sample (b). Parameters Statistically Significant, Exception Denoteda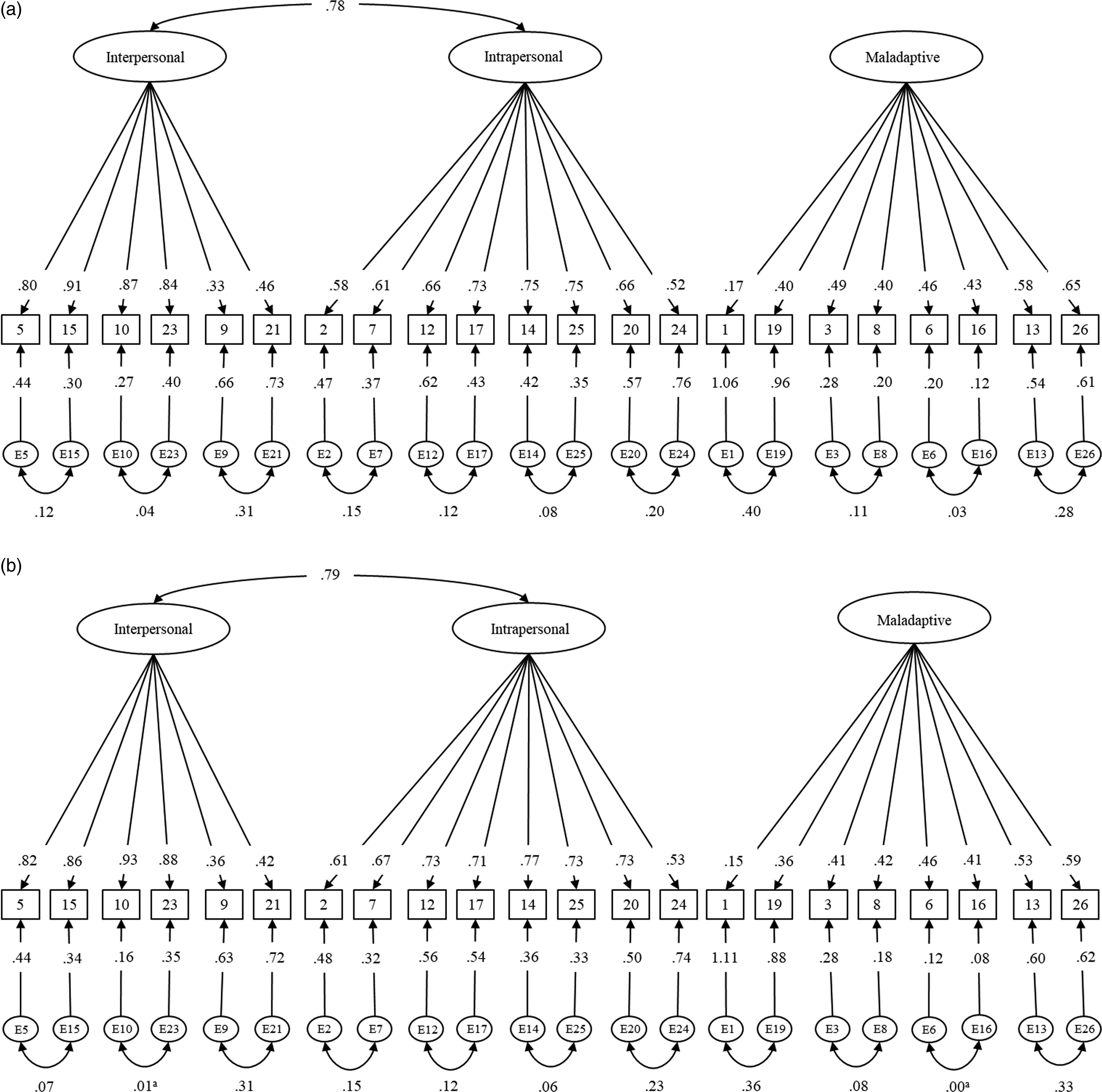
External Validity
To test validity of the subscales, we ran a path analysis with each of the three coping subscales as predictor variables and TFEQ subscales (hunger, disinhibition, and restraint), anxiety, and depression as outcome variables. The average coping scales descriptive statistics for the full sample (n = 1984) included average scores of maladaptive coping of M = 1.69 (SD = .48), range 1–3.75, while interpersonal (M = 2.43 [SD = .73], range 1–4) and intrapersonal coping scales (M = 2.93 [SD = .67], range 1–4) were slightly higher. Outcome descriptive statistics are included in Table 1. The overall model provided good fit to the data, χ2 (302) = 2756.39, p < .0001, AIC = 2908.39, AGFI = .88, RMSEA = .06, 90% CI [.06, .07], CFI = .87 (see Figure 2). Interpersonal coping was weakly related to depression (Standardized B = .08, p < .0001). Interpersonal coping was not statistically significantly related to any other variables. Intrapersonal coping was positively associated with cognitive restraint (B = .31, p < .0001). Intrapersonal coping was not statistically significantly related to anxiety, depression, hunger, or disinhibition. Maladaptive coping was positively associated with anxiety, depression, hunger, and disinhibition (range Bs from .08–.42, all p < .0001). Maladaptive coping was negatively related to cognitive restraint (B = −.08, p < .0001). Overall, these results provide evidence that coping styles converge with and discriminate from measures of anxiety, depression, and eating habits among a sample of patients pursuing bariatric surgery. Structural Equation Model with Coping Subscales Entered as Predictor Variables and Anxiety, Depression, and Eating Habits as Outcome Variables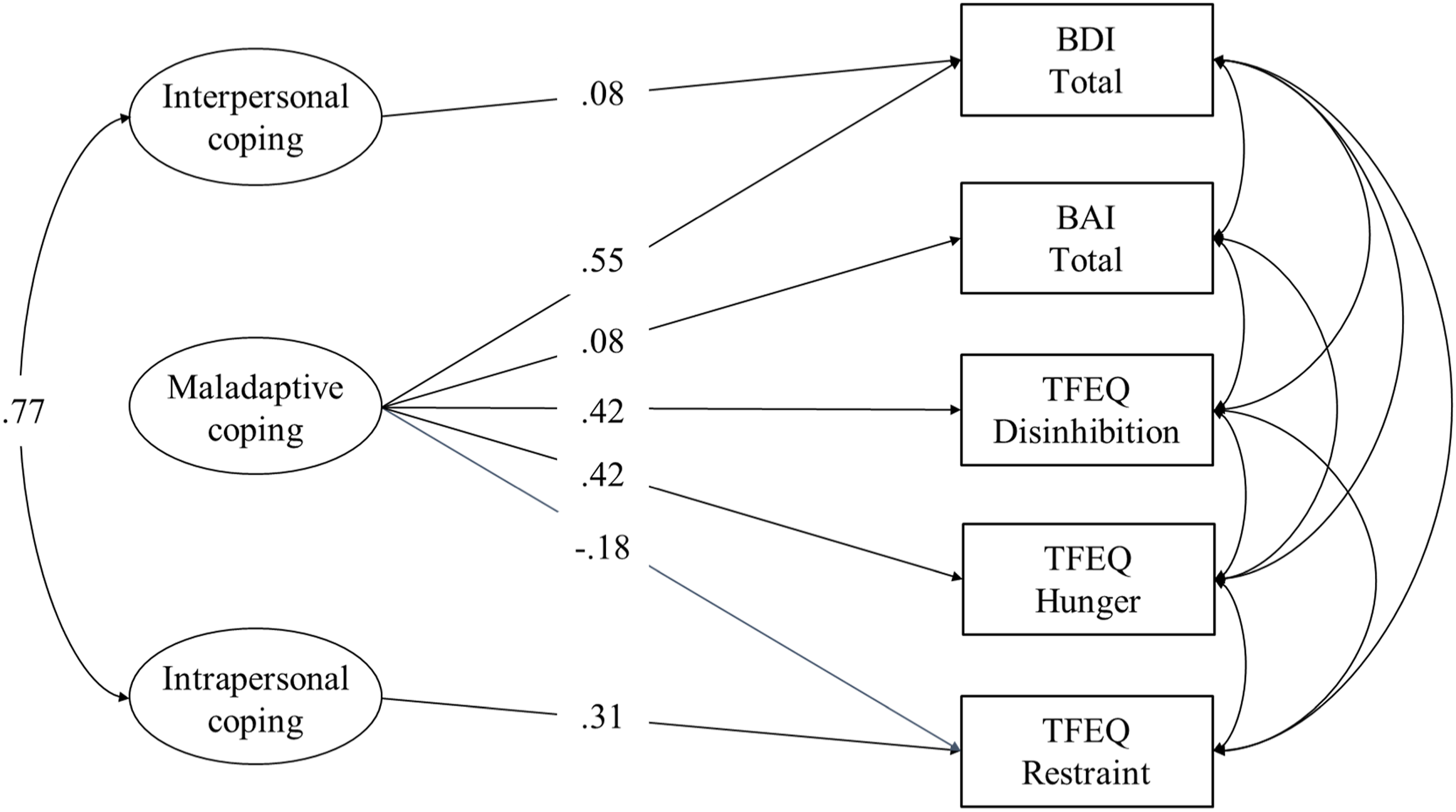
Discussion
Overview
Overall, in this study we found that the best fitting model of coping among patients pursuing bariatric surgery was a three-factor model that included interpersonal coping, intrapersonal coping, and maladaptive coping. While a brief analysis of traditional fit indices of the various models may suggest that the models examined in the current study do not generally fit the data well due to the models not meeting typically accepted cutoffs for traditional fit indices, a deeper examination of possible areas of model misfit suggest that the model fits the data well with few areas for improvement. Importantly, traditional fit indices tend to be biased by parameter estimates (Kline, 2016). Furthermore, the exact fit test (i.e., the chi square test) tends to be overpowered, often resulting in researchers rejecting models that otherwise produce good fit. In this study, rather than only relying on a single metric of model fit (e.g., chi-square exact fit test, traditional fit indices such as the CFI or SRMR, and residual statistics), we examined each of these three methods of examining model fit in conjunction. Doing so, we have identified a model that is theoretically justified and yields adequate fit based on the current data.
One major finding is that the traditional 14-factor structure of the Brief COPE Inventory does not fit the data as well for patients pursuing bariatric surgery than the tested best fit model examined in our study. In fact, the 14-factor model would not converge in the current sample, suggesting that the model has critical theoretical errors which prevent the model from running. Even after omitting items with limited variability (i.e., items measuring substance use, humor, and religion), which could be preventing the model from running, the proposed two-item factor models converged but produced error messages, suggesting poor model fit. While the specific reasons for why the model proposed by Carver (1997) did not converge in the current sample remain unclear, it is important that practitioners carefully consider the implications for using subscales that are not empirically supported for use among patients pursuing bariatric surgery.
One critical aspect of examining model fit in the current study included examining residual statistics, including correlational residual statistics and standardized residual statistics. Specifically, we identified correlational statistics that exceeded an absolute value magnitude of .10 that were associated with statistically significant standardized residual statistics. By identifying these statistics, we were able to identify any areas in the model where making modifications would yield a statistically improved model that would correspond to a meaningful improvement in the model. In the development sample, there were relatively few areas for model improvement.
Importantly, the identified areas for model improvement in the development sample were consistent across the majority of the models. For example, items one (from the original distraction subscale) and two (from the original active coping subscale), which both include focusing attention on an activity, were possible areas for model misspecification across all models in the validation sample. Similarly, items five (emotional support subscale) and ten (instrumental support subscale), both of which discuss getting support or advice from others, had correlation residual statistics exceeding |.10| and standardized residual statistics that were statistically significant. Items five and 23, which assess getting emotional support from others and trying to get advice from other people, were significant in models 1 a and b and models 4 a and b.
However, in some models, specific pairs of items emerged as areas for model improvement that were not consistent across models. For example, items 10 (instrumental support subscale) and 21 (venting subscale), inquiring about seeking help or advice from people and expressing negative feelings was noted in models 4a and 4b. In models 3a and 3b, items 19 (distraction subscale) and 21 (venting subscale), which assessed thinking about stressors less and expressing negative feelings, were identified as an area for model improvement. Other item pairs, such as items one (distraction subscale) and nine (venting subscale) in model 3b and items 19 and 23 in model 1b, only emerged in a single model.
Interestingly, in the validation sample, none of the previously identified item pairs emerged as potential areas for model improvement. While the validation sample had three item pairs for potential model modification, no theoretical justification exists to justify adding item covariances. Furthermore, the lack of replication would suggest that the areas for model improvement identified in the validation subsample are likely emerging by chance rather than due to genuine relations among specific items.
Regarding convergent and discriminant validity, the cross-sectional structural equation model highlighted important relationships between variables. Specifically, the large associations between maladaptive coping and measures of disinhibited eating and depression provide support for convergent validity. The small to moderate relationships between intrapersonal coping with cognitive restraint and maladaptive coping with hunger, cognitive restraint, and disinhibition provide some evidence for convergent validity as well. The small associations between interpersonal coping with depression and maladaptive coping with anxiety, in conjunction with the lack of relationships among interpersonal coping with eating habits and intrapersonal coping with psychopathology measures provide evidence for discriminant validity in our sample.
Implications and Future Directions
The findings from the current study suggest that, while coping is traditionally considered to consist of numerous, distinct methods, coping can be consolidated into three distinct but related forms, including interpersonal, intrapersonal, and maladaptive coping. The finding that coping can be consolidated into more general methods of coping among bariatric candidates (i.e., reaching out, turning inward, and using unhelpful methods) increases options for identifying and targeting coping related to health outcomes. For example, consolidating coping strategies into a few specific areas allows researchers to identify what types of coping are most closely related to health. Furthermore, this allows clinicians to focus on increasing an area of coping within their clients (e.g., connecting with others) rather than trying to help clients increase on specific strategies (e.g., seeking advice from others). Future work should seek to replicate the findings in the study regarding factor structure and expand on this work by examining how these subscales relate to other established measures of coping. While additional work is needed to determine how these areas of coping are related to different aspects of health and other forms of coping, the current study found that these areas of coping are empirically based.
Limitations
There are several important limitations to consider in the current study. First, the sample consisted of primarily White females from predominantly rural areas pursuing bariatric surgery. As such, it is possible that the results of this study may not replicate among other populations of patients pursuing bariatric surgery. It is critical that these results are replicated among a more racially diverse sample. It would also be important to seek to replicate these findings among a sample with more gender diversity as well. While the majority of people seeking bariatric surgery identify their race as White and their gender as female (Melendez-Araujo et al., 2022), it is possible that the structure of coping is gender specific. Furthermore, social desirability may have played an important part in this study, as patients pursuing bariatric surgery may be motivated to systematically respond to items in a way that increases their chances of being approved for surgery. Social desirability may have influenced the limited variability and low scores in specific areas (e.g., under-reporting alcohol use), as current substance use is a contraindication for surgery.
Another important limitation in this study is that we were not able to replicate these findings with a distinct sample. While the findings of this study are robust and we were able to replicate our findings within the sample, they may be specific to patients pursuing bariatric surgery at our clinic. While we suspect this is not the case, as the models we examined are based on identified model in other health psychology samples (e.g., patients with postpartum depression, patients with coronary heart disease), it is possible that the results of this study would not replicate outside of our sample population. Future work should replicate the factor structure of the Brief COPE Inventory with other health psychology samples, including non-surgical samples of people with excess weight and weight related illnesses.
A third important limitation in this study is that we were not able to test the original models as hypothesized and needed to modify the models in order for them to converge. Specifically, rather than testing higher-order models of coping, which would suggest that the Brief COPE Inventory can be used with both the subscales and the higher-order factors, we needed to covary subscale items rather than modeling the subscales. This modification was a statistical decision in order to allow us to conduct chi-square difference tests among nested models, but it prevented us from being able to compare the proposed higher-order models with the models that only included the subscales. Importantly, while we found a model that fits the data relatively well, this does not rule out the possibility that other models yet to be identified may fit equally well or better. Thus, additional research is required to comprehensively understand the structure of coping among bariatric candidates.
Conclusions
In the current study, we found that a three-factor model of coping, consisting of interpersonal coping (i.e., reaching out to others), intrapersonal coping (i.e., focusing on managing stress on one’s own), and maladaptive coping (i.e., avoiding/ignoring), was the best fitting model of coping. We found that this model fit the data significantly better than a two-factor model of coping (examining adaptive and maladaptive coping), which fit the data better than a three-factor model examining emotion-focused, problem-focused, and avoidant coping. These data suggest that examining themes in coping rather than specific coping strategies may be helpful in studying and understanding how coping is related to health. While the results in the current study are specific to patients pursuing bariatric surgery, it is important that we try to replicate the identified three factor model among other health psychology populations.
Supplemental Material
Supplemental Material - Psychometric Properties of the Brief Coping Orientation to Problems Experienced Inventory Among Patients Pursuing Bariatric Surgery
Supplemental Material for Psychometric Properties of the Brief Coping Orientation to Problems Experienced Inventory Among Patients Pursuing Bariatric Surgery by Emily M. Bartholomay, Christa Lilly, Stephanie Cox, Lawrence Tabone, Nova Szoka, Salim Abunnaja, and Laura Aylward in Evaluation & the Health Professions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nova Szoka is the founder of Endolumik Inc. and is a consultant for CSTATS. The remaining authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.