
Abstract
This study aimed to translate the ACL Donor Site Morbidity (ACL-DSM) questionnaire into Turkish and assess the reliability and validity of the Turkish version of the ACL-DSM questionnaire (ACL-DSM-Tr) among individuals following anterior cruciate ligament (ACL) reconstruction. The process involved forward and back-translation, cultural adaptation, and validation of the ACL-DSM-Tr questionnaire on ninety-nine patients (mean age 30.73 ± 8.55 years). Participants completed ACL-DSM-Tr, International Knee Documentary Committee (IKDC) subjective form, ACL Return to Sport (ACL-RSI), and Forgotten Joint Scale (FJS) questionnaires. The internal consistency, reliability, and validity of the ACL-DSM-Tr were analyzed. The ACL-DSM-Tr demonstrated a high internal consistency (Cronbach’s alpha .755) and excellent test-retest reliability (Spearman correlation r = .811, p < .001; Cronbach’s alpha .890). The ACL-DSM-Tr score exhibited a strong positive correlation with the IKDC score (r = .690, p < .001) and a moderate positive correlation with the FJS score (r = .535, p < .001). Despite a fair correlation between ACL-DSM-Tr and ACL- RSI subgroup scores, no significant correlation was observed with the ACL-RSI total score (p = .297). In conclusion, the ACL-DSM-Tr demonstrated internal consistency, reliability, and validity in patients with ACL reconstruction. This questionnaire has the potential to yield significant benefits in monitoring patient satisfaction and evaluating the level of comfort experienced at the donor site following ACL reconstruction.
Keywords
Introduction
Anterior cruciate ligament (ACL) injuries are approximately 50% of all sports-related knee injuries, and ACL reconstruction is among the most frequently performed orthopedic procedures (Sanders et al., 2017; Shelton & Fagan, 2011). Reconstruction is performed to restore stability to the knee and decrease the risk of subsequent injury since ACL deficiency is associated with a high risk of mechanical instability, subchondral and bone marrow lesions, inflammatory responses, and the development of osteoarthritis (Kaeding et al., 2015).
Reconstructions often result in donor-site-related problems such as difficulties in kneeling, anterior knee pain, quadriceps or hamstring strength deficits, and impairment in anterior knee sensitivity (Aufwerber et al., 2012). Some studies reported that some of these common donor site complications could impact the quality of life and may result in significant impairment in daily living activities, according to patients’ reports (Mouarbes et al., 2020; Sabat & Kumar, 2013). Donor site morbidity is related to various factors, such as graft selection, patient characteristics, surgical technique, and post-op rehabilitation protocol (Kartus et al., 1997). Subjective assessment of patient-perspective regarding donor site problems is essential. It should be included in the outcome measurement (Aufwerber et al., 2012) since current gold-standard outcome measurements do not fully fulfill donor-site-related complaints. However, they capture the patient’s overall symptoms (Ahmad et al., 2017).
There are several patient-reported outcome measures (PROMs) for ACL patients in the literature, and they are widely used to collect patients’ perceptions of the symptoms after injuries and surgeries (Ahmad et al., 2017). PROMs are valuable since they collect information on health-related outcomes directly from patients. Initially developed for research purposes, they are valuable in clinical decision-making and following changes over time (Churruca et al., 2021). Therefore, due to the abovementioned needs, Hacken et al. developed a 10-question donor site morbidity patient-reported questionnaire to evaluate donor site morbidity after ACL reconstruction. This score - ACL Donor Site Morbidity (ACL-DSM) - was created based on surgeon experience without utilizing patient input, and the final score was created by giving equal weight to all questions. They reported that the ACL-DSM questionnaire might provide a more accurate evaluation for donor-site-related problems than the available self-reported questionnaires for ACL (Hacken et al., 2020).
Testing the validation and reliability of the scales to exploit their potential benefits is crucial to improve the quality of studies and clinical outcome follow-ups. Thus, the high incidence of donor site symptoms and the lack of any tool to evaluate these symptoms led us to conduct this study. A Turkish version of the ACL-DSM (ACL-DSM-Tr) questionnaire would be essential for evaluating the donor site comfort of the patients with ACL reconstruction. Therefore, the aim of the study was to translate the ACL-DSM questionnaire into Turkish to use this questionnaire in Turkish-speaking populations. The first hypothesis of the study was to translate the ACL-DSM questionnaire into the Turkish language and the second hypothesis was to examine and evaluate the psychometric properties of the Turkish version of this scale in individuals who have undergone ACL reconstruction.
Materials and Methods
The data was collected from May 2022 to November 2022 in the Orthopedic Rehabilitation Unit of the Faculty of Physical Therapy and Rehabilitation at Hacettepe University. The number of items utilized in the scale was multiplied by 4–10 to establish the sample size for the study (Terwee et al., 2018). Hacettepe University Ethics Committee approved the study (GO 22/469). All participants were provided an informed consent form prior to participation.
Participants
Participants who were aged between 18–45 years; had unilateral ACL reconstruction using hamstring tendon autograft; had a pre-injury Tegner Activity Score of at least 5; were able to read and write Turkish were included in the present study. The patients were excluded if they had additional meniscus or cartilage repair to ACL reconstruction, had ACL reconstruction revision, or had a history of previous knee surgery.
The patients received all questionnaires by email with a shared online survey link. The study was carried out via online surveys using https://freeonlinesurveys.com. For test-retest evaluation, the ACL-DSM-Tr was administered 7–14 days after their initial attempt.
Patient-Reported Outcomes Measures
The ACL-DSM questionnaire is a new 10-item patient-focused questionnaire developed to assess morbidity in the harvest area adequately. The questionnaire measures subjective outcomes, including donor site pain, numbness, function, strength, and physical appearance at the surgical site. There are four possible answers to the questions in the questionnaire, each representing increasing symptom severity and patient dissatisfaction. Response options are scored from 0 to 10, depending on the symptom severity or functional limitation. A perfect score of 100 represented no complaints whatsoever. Total scores are divided into four subcategories representing overall post-surgical morbidity: excellent (≥93.3 points), good (80.0–93.2 points), moderate (50.0–79.9 points), and poor (≤49.9 points) (Hacken et al., 2020).
The International Knee Documentation Committee (IKDC) subjective knee form is used to assess the signs, symptoms, function, and sports participation of individuals with knee diseases, including patellofemoral dysfunction, ligamentous and meniscal injuries, and osteoarthritis. This form has 18 items specifically chosen to measure symptoms, allowing clinicians to evaluate pain, stiffness, edema, joint locking, and joint instability. Other items are specifically chosen to test knee function and assess the capacity to carry out daily activities. The total IKDC score runs from 0 to 100, with 100 representing a knee with better levels of function and no symptoms (Irrgang et al., 2001).
ACL Return to Sports after Injury (ACL-RSI), including three subscales under emotions, performance confidence, and risk assessment evaluation, were used. The scale consists of 12 questions that are scored using a visual analog scale (VAS) in increments of 10 points from 0 to 100 (Webster et al., 2008). A percentage of the combined scores for each of the 12 questions is used to compute the overall score. A high score was a sign of a satisfying psychological response (Webster et al., 2008).
The Forgotten Joint Score (FJS) was created to detect the consciousness of an artificial joint (such as the hip or knee) during daily activities. It uses a 5-point Likert response scale (0, never; 1, almost; 2, seldom; 3, sometimes; and 4, mostly) with 12 items to measure a patient’s capacity to forget an artificial joint while performing activities of daily living such as lying in bed at night, sitting for an extended period of time in a chair, walking for an extended period of time, taking a bath, driving, climbing stairs, walking on uneven ground, rising from a low seated position, standing for an extended period of time, and performing housework or gardening. The raw scores are converted to a scale of 0 to 100. High scores suggest a successful outcome, implying a high degree of “forgetting” the joint (Behrend et al., 2012; Lee et al., 2020).
Translation and Cross-Cultural Adaptation
First, permission to investigate the validity and reliability of the ACL-DSM scale in the Turkish population was obtained from the developer of the ACL-DSM scale. The ACL-DSM scale was translated by two native Turkish speakers with good English command. Two independent native English speakers who are also proficient in Turkish and had not studied the first translation process performed retranslation (from Turkish to English). A standard version was formed with the synthesis of the two translations. The expert committee compared and reviewed the original and re-translated versions of the ACL-DSM scale, consisting of three physiotherapists, and the final version was created.
As a lack of knowledge of the term ‘donor site’ could affect understanding the questionnaire/questions, translators added an explanation of what the donor site means as information before the questionnaire. Also, in the last question, the word ‘quadriceps’ was not used to make the question easier to understand. Instead of quadriceps, translators used only tight muscles. For a precise understanding, see supplementary material 1.
After completing the translation and cross-cultural adaptation processes, content validity was approved by the expert committee, who are experienced in the area and fluent in English and Turkish.
Statistical Analysis
Descriptive analyses are reported as means and standard deviations for continuous data and percentages for non-continuous/categorical data. Internal consistency was estimated using Cronbach’s alpha test, which indicates homogeneity between items within a questionnaire. A Cronbach’s alpha value of .60 ≤ α ≤ .79 was considered quite reliable, and α ≥ .80 is considered highly reliable (McGraw & Wong, 1996; Terwee et al., 2007). In order to determine the test-retest reliability of the ACL-DSM-Tr, we calculated the intraclass correlation coefficient (ICC) with corresponding 95% confidence intervals (CIs) between the first and second administration of the ACL-DSM-Tr. Values were considered as little or no (0–.25), weak (.26–.49), moderate (.50 and .69), strong (.70 and .89), very strong (.90 and 1.00) (Plichta et al., 2013). Also, standard error of measurement and Reliable Change Index (RC) scores are calculated for each item, and the total score is used to test the reliability and interpretability of scores (Crosby et al., 2003; Mokkink et al., 2010; Wyrwich et al., 1999). A lower score of RC than 1.96 is considered a change in the score that reflects the real change and preciseness of the instrument (Jacobson & Truax, 1992).
Criterion validity was evaluated by correlating ACL-DSM-Tr with IKDC, ACL-RSI, and the FJS scores. Analysis was carried out with the Spearman correlation test, and results were expressed as ‘strong’ (r > .5), ‘medium’ (.5 < r < .3), or ‘small’ (r < .3) (Terwee et al., 2007). In addition, the floor-ceiling effect was investigated following the quality criteria for measurement properties of health status questionnaires (Terwee et al., 2007). The proportion (%) of patients who obtained the lowest (0) or the highest (100) score for each question and the total score was calculated. If more than 15% of participants achieved the lowest or highest possible score, floor or ceiling effects are considered (Terwee et al., 2007). Statistical significance was set at p < 0.05. All analyses were performed using IBM SPSS Statistics software (Version 23.0, IBM Inc, Armonk, NY, USA).
Results
Demographic and Clinical Characteristics of Study Population, and Absolute Values of the Questionnaires
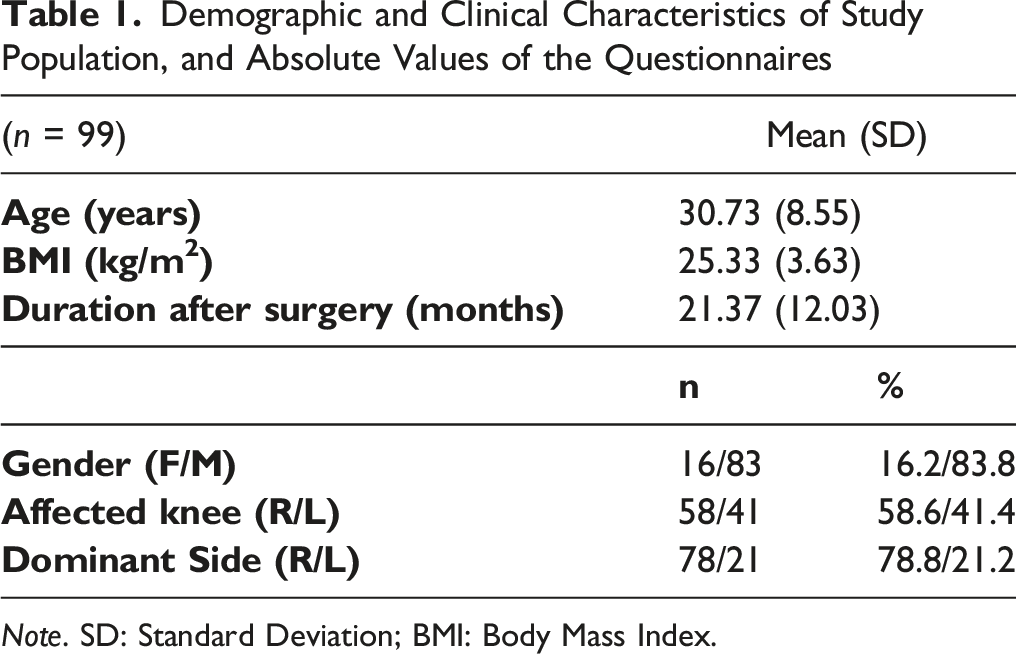
Note. SD: Standard Deviation; BMI: Body Mass Index.
Reliability
Internal Consistency
Internal Consistency and Test-Retest Scores of the Turkish Version of the ACL-DSM
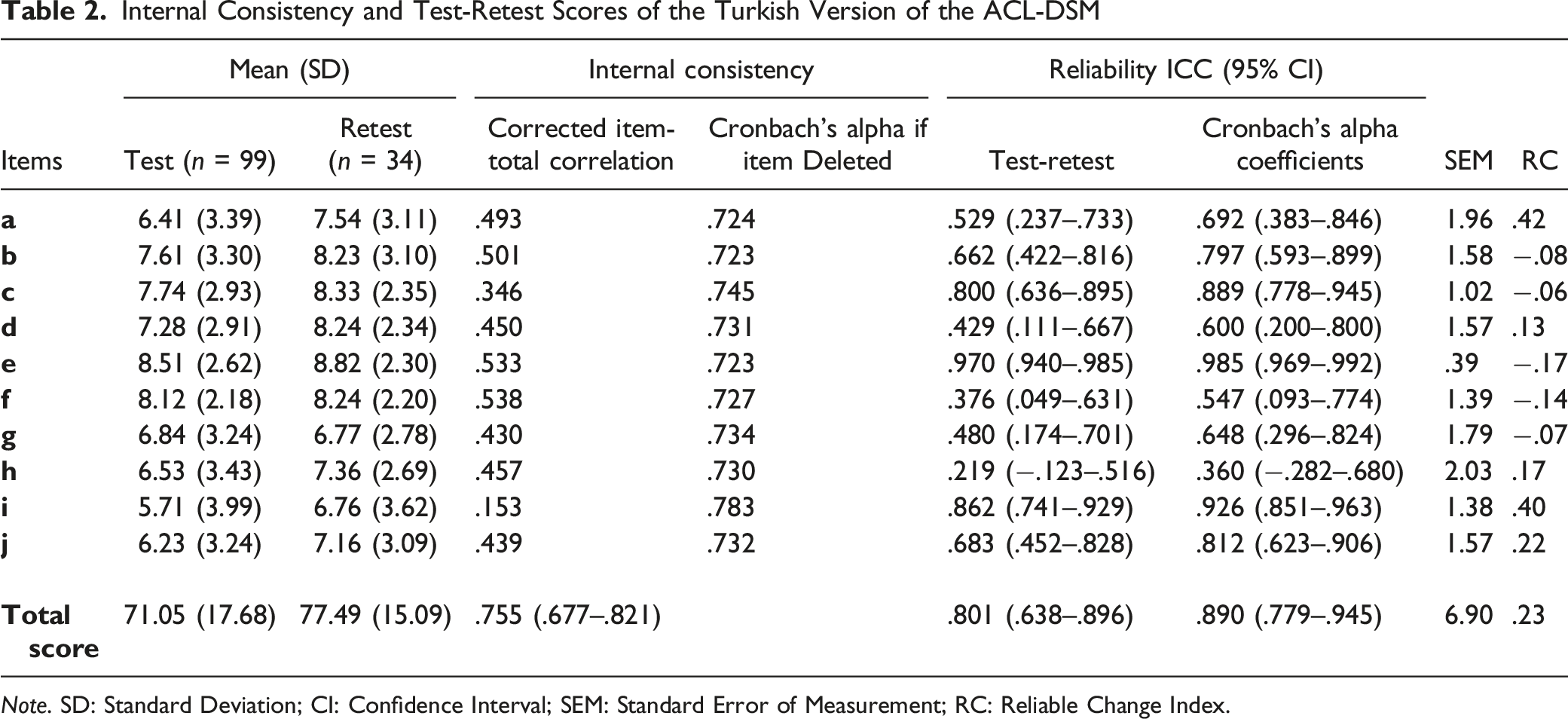
Note. SD: Standard Deviation; CI: Confidence Interval; SEM: Standard Error of Measurement; RC: Reliable Change Index.
Test-Retest Reliability
Correlation Between Total Score of the ACL-DSM-Tr and the IKDC, the ACL-RSI and the FJS
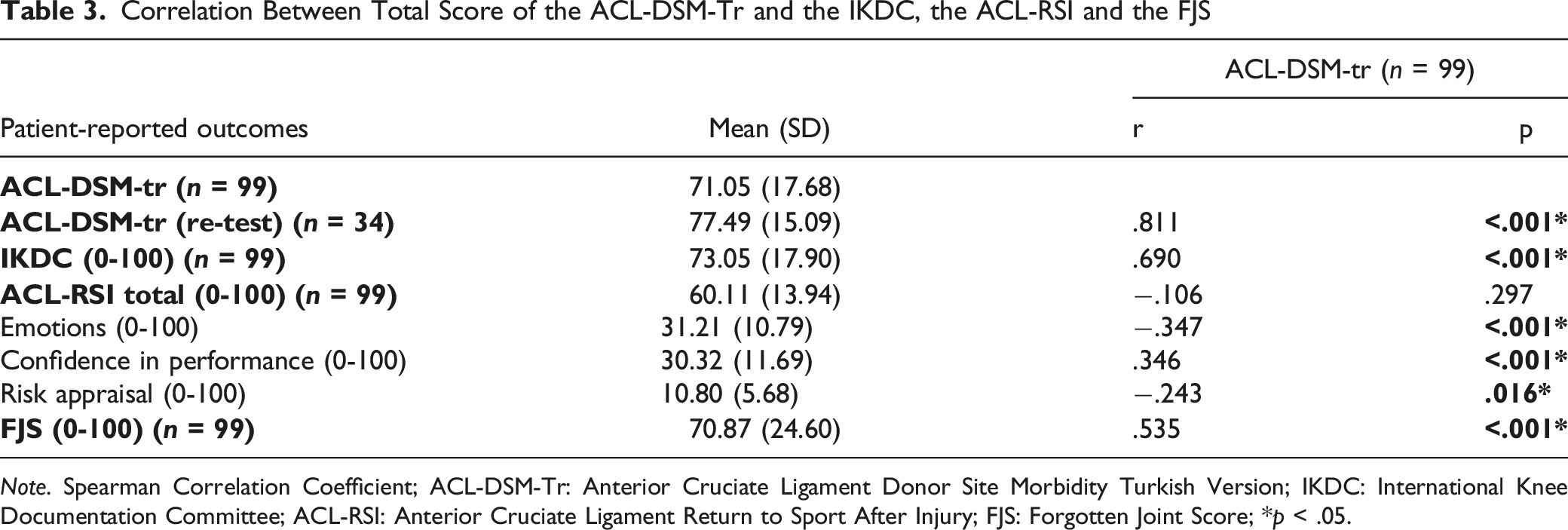
Note. Spearman Correlation Coefficient; ACL-DSM-Tr: Anterior Cruciate Ligament Donor Site Morbidity Turkish Version; IKDC: International Knee Documentation Committee; ACL-RSI: Anterior Cruciate Ligament Return to Sport After Injury; FJS: Forgotten Joint Score; *p < .05.
Criterion Validity
The correlation coefficients between the ACL-DSM-Tr score and the criterion questionnaire scores are presented in Table 3. ACL-DSM-Tr score was strongly correlated with the IKDC score (r = .690, p < .001) and moderately correlated with the FJS score (r = .535, p < .001). ACL-RSI subgroup scores were fairly correlated with ACL-DSM-Tr scores. There was no correlation between the total score of ACL-RSI and ACL-DSM-Tr (p > .05, Table 3).
Floor and Ceiling Effects
None of the participants had a score of 0, and two participants (2.02%) had a score of 100. The floor effect was found to be 0%, and the ceiling effect was 2.02%. Thus, the floor-ceiling effects were in the acceptable range of <15%.
Discussion
The present study aimed to evaluate the reliability and validity of the Turkish version of the ACL-DSM questionnaire, originally developed by Hacken et al. The findings of this study provide compelling evidence supporting the reliability of the questionnaire, as it exhibited a high level of internal consistency. Additionally, the questionnaire demonstrated significant associations with various assessments, including symptoms, sports activity, knee function, joint awareness, and return to sports appraisals. Thus, the ACL-DSM-Tr questionnaire demonstrates validity and reliability in assessing donor site morbidity within the Turkish population.
Reliability refers to the degree of dependability and consistency in scale scores. In this study, we examined the internal consistency of the ACL-DSM-Tr questionnaire, which assesses the extent of random error inherent in item scores by examining their intercorrelations (Cronbach, 1951). The results indicated a favorable level of internal consistency for the overall score, with a Cronbach’s alpha coefficient of .755 (confidence interval: .677–.821). Similarly, the corrected item correlations exhibited consistency with the total score, yielding a Cronbach’s alpha coefficient ranging from .723 to .783. In the literature, a threshold above .90 has generated conflicting interpretations regarding the presence of an excessive number of items in the outcome and the potential narrowness of the attribute under investigation (Fitzpatrick et al., 1998). Consequently, it is recommended that Cronbach’s alpha ideally should be between .70 and .90, indicating a balanced number of items. Consistent with the prevailing perspective, our findings corroborate the established criterion and emphasize the suitability of the questionnaire’s item quality.
The 7–14 days interval was selected to ensure test-retest reliability, although a 2–14 days range is recommended (Marx et al., 2003). The ACL-DSM-Tr exhibited strong test-retest reliability with an ICC of .890 (95% CIs: .779–.945), indicating a high level of internal consistency. These findings suggest that the scores remain stable over time, despite a two-week interval between the test and retest sessions. As for the validity and reliability of the ACL-DSM in different languages, the literature lacks evidence, preventing direct comparisons with other studies regarding reliability. Thus, this study represents the initial endeavor to assess the ACL-DSM-Tr’s reliability and validity in a specific language context. Hacken et al. did not mention reliability testing in the original study as the main focus was on surgery. However, compared to other PROMs reliability ICC scores, the ACL-DSM-Tr showed similar reliability results with the IKDC (ICC: .94; 95% CIs: .88–.97) (Irrgang et al., 2001), with the ACL-RSI (ICC = .92; 95% CIs = .62–.89) (Harput et al., 2017) in the same population.
Standard error of measurement (SEM) measures the precision of an outcome instrument and is used in reliability studies to calculate minimal important changes (Crosby et al., 2003). These changes are suggested to be mentioned and discussed in PROM reliability studies (Mokkink et al., 2010). In the present study, the lower SEM values indicate that individual item and total scores are relatively free from errors and facilitate more reliable predictions (Crosby et al., 2003). Moreover, in line with the COSMIN guidelines emphasizing the inclusion of interpretability in reliability studies (Mokkink et al., 2010), we computed Reliability Change Indexes (RC) for both individual items and the total score of the ACL-DSM-Tr. This index, based on SEM, assesses the extent to which observed changes surpass the random fluctuations inherent in an imprecise measurement tool. It represents one of the distribution-based approaches for determining clinically meaningful change (Crosby et al., 2003; Jacobson & Truax, 1992). Our RC analysis revealed that all items within the ACL-DSM-Tr questionnaire, including the total score, demonstrated interpretability (Jacobson & Truax, 1992).
Hacken et al. utilized the IKDC questionnaire for comparison and showed a strong correlation (r = .667) between the two measures, demonstrating the validity of the ACL-DSM questionnaire (Hacken et al., 2020). Similarly, our results also revealed a strong correlation with the IKDC score (r = .690), supporting findings of the original study. While the IKDC questionnaire is widely accepted as a gold standard instrument for assessing ACL reconstructions and excels at capturing symptoms, it does not encompass inquiries regarding incision, numbness, satisfaction, or atrophy-related symptoms (Hambly & Griva, 2010; Irrgang et al., 2001). To address these aspects, we incorporated the ACL-RSI and the FJS outcomes, enabling the assessment of both function-related symptoms and satisfaction/adaptation-related questions. Consequently, significant correlations were observed among the ACL-DSM-Tr, ACL-RSI, and FJS, suggesting that the ACL-DSM-Tr captures patients’ adaptation and satisfaction following reconstruction. However, the study identified a moderate relationship between the subgroups of the ACL-RSI and the ACL-DSM-Tr, indicating relatively weaker validity. This discrepancy may arise from the fact that while the ACL-DSM-Tr includes function-related items, the ACL-RSI primarily comprises belief-oriented questions within the subgroups of emotions, confidence, and risk appraisals.
The strength of the current study is that this is the first cross-culturally adapted questionnaire measuring donor site morbidity in patients with unilateral ACL reconstruction in the Turkish language. Notably, this is the first version study of the ACL-DSM questionnaire; these findings can be regarded as preliminary data, laying the foundation for future research. Additionally, this study provides comprehensive insights into the reliability and interpretability of the ACL-DSM questionnaire. However, despite thoroughly examining the internal consistency, reliability, and validity of the ACL-DSM-Tr, several limitations should be acknowledged. Firstly, the majority of participants in the present study were male (83.8%), resulting in a limited representation of females (16.2%) and thereby restricting the generalizability of the findings to both genders equally. Secondly, all participants in this study had undergone ACL reconstructions exclusively with hamstring tendon grafts, which differs from the original study by Hacken et al., which included only patellar tendon graft reconstructions. This discrepancy is noteworthy as the choice of graft is recognized to influence donor site morbidity (Johnston et al., 2021; Kartus et al., 2001; Magnitskaya et al., 2020; Mouarbes et al., 2020). Moreover, the disparity in the total scores of the ACL-DSM between the present study (71.05) and the previous study (98.3) constitutes a limitation and necessitates further investigation during longer follow-up periods. These limitations and disparities should be appropriately considered in future studies to enhance the comprehensiveness of research findings.
Conclusions
In conclusion, the ACL-DSM-Tr was an internally consistent, reliable, and valid patient-reported outcome in Turkish-speaking patients who had undergone unilateral ACL reconstruction with hamstring tendon autograft. The current study demonstrated that ACL-DSM-Tr offers psychometrically appropriate and useful monitoring of patients with ACL reconstruction representing both objective and subjective parameters related to donor site morbidity. This questionnaire should be considered by clinicians to assess patient satisfaction and donor site comfort following reconstruction surgery.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Hacettepe University Non-Interventional Clinical Research Ethics Committee approved the study on 10.05.2022, with the registration number of GO 22/469.