
Abstract
A growing understanding of twice-exceptional (2e) students has caused many to consider the possibility of misdiagnosis and missed diagnoses in the gifted student. Despite this, auditory processing disorders (APD) and vision processing disorders (VPD) are seldom examined in the 2e research literature, yet are not uncommon in the 2e population. Because both auditory and vision processing are foundational to the human experience, challenges in these areas may significantly impact higher-order skills such as attention and executive function, as well as academic performance. This article explores what is currently known about these processing disorders, examines potential co-occurring conditions, such as dyslexia and Attention Deficit/Hyperactivity Disorder (ADHD), and presents clinical case file data suggesting how these sensory disorders may appear in the 2e population. Proper identification, management, and support of APD and VPD in 2e students could improve our ability to address student needs at the foundational level.
Keywords
Introduction
A substantial literature base has developed around twice-exceptional (2e) students who have mainstream diagnoses such as Attention Deficit/Hyperactivity Disorder (ADHD), autism spectrum disorder (ASD), anxiety, dyslexia, and dysgraphia (Baldwin et al., 2015; Baum et al., 2017; Gomez et al., 2020; Reis et al., 2014). There is also the possibility of misdiagnosis as well as under-diagnosis in the gifted student who can compensate and mask symptoms (Baum et al., 2017; Webb et al., 2016). For example, the recognition of stealth dyslexia as a gifted manifestation of dyslexia has opened the door to better understanding and support for many previously overlooked dyslexic students (Boris, 2022; Eide & Eide, 2012). Data from functional magnetic resonance imaging (fMRI) has confirmed the same brain differences in stealth dyslexic students that are also seen in classically dyslexic students (Hancock et al., 2016; Tanaka et al., 2011).
Identifying the correct diagnoses as early as possible is paramount for 2e students. Misdiagnosis or under-diagnosis can lead to frustration and missed opportunities to support and intervene. There is risk to applying inappropriate supports, accommodations, or interventions that prove to be ineffective, which may cause frustration and confusion for students as well as clinicians, teachers, and parents (Baum et al., 2017). When an intervention is indicated, confidence in the intervention to address a student’s specific challenge area is important.
Additionally, the brain is neuroplastic, or able to change, and especially so in early childhood (Kelvington et al., 2022). The earlier that challenges can be identified, the greater the possibility of providing interventions that can meaningfully improve functioning and long-term outcomes. For example, Lovett et al. (2017) demonstrated that dyslexia intervention in first or second grade was nearly twice as effective as intervention in third grade, and first graders who received intervention retained a faster rate of reading skill growth after the intervention stopped when compared older students.
This article raises the possibility of foundational sensory processing disorders that may be missed when evaluating 2e students. While not unique to 2e students, these processing disorders may be more easily overlooked in the context of 2e students who have strong compensatory skills and ability to mask difficulties. Auditory processing disorders (APD) and vision processing disorders (VPD) are seldom mentioned in 2e research literature, yet several practitioners have noted these challenges in the 2e population (Gilman, 2020; Kircher-Morris, 2021; Rosen, 2016; Webb et al., 2016). APD is not hearing loss, but rather processing asymmetries in the brain that can make it difficult for individuals to understand words, concentrate, and interact socially in the context of background noise. Similarly, VPD concerns how well both eyes work together, affecting binocular vision, smooth saccades when reading, and overall visual stamina. Both disorders share the characteristic of impaired integration at the neurological level. Because auditory processing and vision processing are foundational to the human experience, challenges in these areas may significantly impact higher-order skills such as attention and executive function, along with academic skills. These challenges may appear similar to learning disabilities, behavioral/emotional regulation challenges, ADHD, or other neurodiversity, raising the possibility for misdiagnosis or missed diagnosis. However, these sensory disorders require specialists to diagnose, and are not often considered on a neuropsychological evaluation, or suggested for referral to a specialist.
This paper’s co-authors include educational consultant who has seen a high incidence of APD and VPD in her 2e client base; two developmental optometrists with expertise in VPD, two audiologists with expertise in APD, and a neuropsychologist. This paper presents an overview of APD and VPD foundational research and a literature review of recent research that has demonstrated possible co-occurrence between auditory and vision processing disorders and common diagnoses such as ADHD, anxiety, autism, and dyslexia (Brenner et al., 2007; Ghanizadeh, 2009; Granet et al., 2005; Hatch, 2020; Kritsi et al., 2008; Raghuram et al., 2018). Articles were selected within the past 15 years, except where newer research on a topic was not available. An exhaustive search was conducted across multiple databases including PubMed, VDR Journal, ERIC, ProQuest, Academia.edu, Google Scholar, and Research Gate using combinations of the search terms “auditory processing,” “APD,” “CAPD,” “central auditory nervous system,” “synchrony,” “vision processing,” “VPD,” “convergence insufficiency,” “ocular motor dysfunction,” “dyslexia,” “ADHD,” “autism,” “anxiety,” “comorbid,” “gifted,” and “twice-exceptional”; any peer-reviewed article in English that mentioned possible co-occurring conditions with APD or VPD was included. Clinician co-authors further added clinical data and case reports to illustrate how these sensory disorders may manifest in gifted students, the pervasive impacts they may have, and how intervention may make a significant difference in both quality of life and academic success.
Auditory Processing Disorders
The ability to hear and understand an auditory message is critical for communication, learning, and social relationships. What is less well known is that being able to hear and process sounds requires tasks to be completed by different areas of the auditory system. The ability to perceive or detect the presence of sound is the role of the peripheral hearing mechanism consisting of the outer, middle, and inner ear. However, the ability to understand and prioritize this auditory information is completed by the brain’s central auditory nervous system (CANS), which includes cortical and brainstem areas of function (Burleigh et al., 2002). In other words, the ears collect and send auditory information to the brain and the CANS then converts that sound to something meaningful while also simultaneously filtering background noise. When an individual has normal hearing acuity but difficulty understanding auditory information and concentrating in the presence of background noise, the cause may be an inefficient CANS and they may have APD, sometimes also referred to as central auditory processing disorder (CAPD).
The 1996 American Speech-Language-Hearing Association task force defined the central auditory processes as: …the auditory system mechanisms and processes responsible for the following behavioral phenomena: sound localization and lateralization; auditory discrimination; auditory pattern recognition; temporal aspects of audition, including-temporal resolution, temporal masking, temporal integration, temporal ordering; auditory performance decrements with competing acoustic signals; and auditory performance decrements with degraded acoustic signals. (Task Force on Central Auditory Processing Consensus Development, 1996, 41, 41)
The importance of identifying and understanding APD initially stemmed from teachers and parents who discovered that some children experienced more difficulty understanding auditory messages compared to their peers (Jerger et al., 1991). These challenges occurred despite hearing evaluations demonstrating that these students had hearing capabilities within the range of normal limits, indicating no issue with the peripheral hearing mechanism. Jerger et al. noted, “The construct that such problems may be related to dysfunction in the central auditory system follows from the rich literature on the behavioral manifestations of documented brain lesions affecting the central auditory pathways and centers” (1991, p. 36).
While debate continues in the literature about the precise cause of APD (Moore et al., 2013), an increasing amount of research found objective brain-based differences in individuals with APD. Recent research suggested that a central issue in APD consisted of a timing difference in the processing of sound coming from each ear (Abdollahi et al., 2019), slower or atypical auditory brainstem responses were reported in suspected APD individuals (Ankmnal-Veeranna et al., 2019), and functional magnetic resonance imaging (fMRI) research also noted differences in auditory cortical brain networks associated with APD (Alvand et al., 2022).
When an individual has APD, the presence of sound (e.g., pencils tapping, papers shuffling, birds chirping, background conversations, fans) may degrade their ability to understand speech and/or to maintain focus in their home, academic, work, and/or social environments. Individuals with APD often reported having super-hearing because their CANS becomes overloaded by a variety of sounds throughout their day, which may lead to fatigue and/or overwhelm. These individuals may have difficulty performing to their full potential and may not be aware of the impact of environmental sounds on their functioning, instead attributing their challenges to distractibility, trouble focusing, fatigue, or anxiety. Individuals with APD may also experience a delay in understanding speech which can interfere with the typical cadence of social conversations. All of these factors may impact self-esteem, relationships, and overall well-being.
Diagnosis
Diagnosing APD requires an audiologist with experience in APD to administer a comprehensive battery of standardized tests with available normative data of the CANS in a sound booth. There are various test batteries available for diagnosing APD (Chermak et al., 2017), and there is ongoing debate about the most effective diagnostic tools (Domitz & Schow, 2000; Tabone et al., 2020; Wilson & Arnott, 2013). An individual with APD may easily pass some tests of CANS function but not others (Ahmmed et al., 2014). Some APD test batteries focus on cortical functions, such as hearing competing sentences in each ear, whereas others are sensitive to brainstem functionality, such as understanding isolated words in background noise. Hence, a comprehensive test battery must incorporate age-normed measures that are sensitive to both cortical and brainstem levels of the CANS (Felix et al., 2018). The American Academy of Audiology Clinical Guidelines state that: These procedures may include, but are not limited to, assessment of the following auditory processes: sound localization and lateralization, auditory discrimination, auditory temporal processing, auditory pattern processing, dichotic listening, auditory performance in competing acoustic signals, and auditory performance with degraded acoustic signals. (Musiek et al., 2010, p. 16–17)
It is vital for test batteries to incorporate sufficiently challenging input to effectively assess the CANS. For example, speech-in-noise tests are commonly used tests that can yield very different results depending on the signal-to-noise (S/N) ratio used. S/N is defined as the “difference between the overall level of the signal and the overall level of the background noise… For example, if a speech signal is presented at 70 dB SPL and a noise of 60 dB SPL, the S/N is + 10 dB” (Smaldino et al., 2009, 746). The larger the S/N, the easier the task is for the CANS. Therefore, it is important to administer more sensitive APD tasks, including speech-in-noise tests, such as the NU-6 word lists with a 0 dB S/N, using white noise at the same volume as the target words. Utilizing less sensitive versions of speech-in-noise testing, such as the CID W-22 word lists with a +5 dB S/N or the Auditory-Figure Ground Subtest of the SCAN with a +8 or +12 S/N may miss central auditory processing challenges and may result in false negatives.
An individual is a candidate for APD testing if they have a receptive language age of three years or above, have normal to near-normal hearing in the speech frequency range, have the compliance needed to complete the listening tasks, and are able to wear headphones in the sound booth. Early identification of APD is essential to allow supports to be put into place to reduce the impacts on learning, academic performance, social development, and self-confidence (Guzek & Iwanicka-Pronicka, 2022).
Intervention
There are several management options available to individuals who have been diagnosed with APD (Bellis & Anzalone, 2008). Interventions include compensatory strategies, listening therapies, FM systems, passive ear filters, and low-gain hearing aids. APD management provides accommodations as well as supports to help an individual with APD manage their auditory environment and give them improved access to auditory information during their day. Compensatory strategies that aim to reduce listening demands are common sense approaches such as receiving preferential seating, written instructions, permission to take auditory breaks throughout the day, and permission to take tests in a quiet environment. The use of earplugs or sound attenuating headphones when concentrating, previewing essential information, and incorporating a multi-sensory approach to learning can also be helpful (Bellis & Anzalone, 2008).
There are several types of listening therapies which aim to strengthen and/or change the auditory system in order to reduce the impacts of APD (Bellis & Anzalone, 2008). These therapies may take months or years to complete. Burleigh et al. (2002) observed that “although therapeutic programs enhance performance in specific skill areas such as language, phonemic recognition, reading, and spelling, there is a paucity of data demonstrating that they change underlying central auditory abilities” (p. 152). Similarly, clients seen at two of the co-authors’ APD clinic who had previously completed listening therapies reported improved skills in academic performance and other skill-based functions; however, they continued to demonstrate decreased ability to understand speech and concentrate in the presence of background noise.
Another management approach is to give a student access to a frequency modulated (FM) system. This can be accomplished with either a personal FM system, consisting of the student wearing headphones/earbuds, or a soundfield FM system, which incorporates the use of a speaker system and a microphone for the teacher (Burleigh et al., 2002). In a classroom setting, these systems provide improved auditory input to the listener regardless of their location in the room relative to the speaker, making this technology especially beneficial in lecture-type environments; however, FM systems only work where the technology is implemented, which typically leaves out cafeteria, playground, community, and home environments. FM systems improve classroom behaviors and reduce the effort that students expend to understand and focus in their academic environment (Johnston et al., 2009; Purdy et al., 2009). FM systems can also be beneficial in higher education and work environments.
Wearing a passive ear filter is another management option. Colorado State University (CSU) Center for Central Auditory Research collected data on individuals with and without APD to document the benefits of the passive ear filter utilizing speech-in-noise testing in a soundfield setting (Burleigh et al., 2002). The authors found, (1) persons with normal CANS function perform significantly better in noise than individuals with CAPD (2) those without CANS dysfunction discriminate best with two ears in an unfiltered condition (3) when a filter is fit appropriately in persons with defined CAP [Central Auditory Processing] asymmetries, speech discrimination performance is significantly improved. (Burleigh et al., 2002, p. 154)
A passive ear filter worn in only one ear helps to balance timing asynchronies in the CANS and improve the ability to understand speech in the presence of background noise. The passive ear filter does not filter, dampen, or change an individual’s hearing acuity, it merely adjusts the timing of auditory input between both ears. Burleigh et al. (2002) found that for individuals with APD, the “mean improvement increased from 64 percent with no filters to more than 80 percent when using the preferred ear with the custom filter system” (p. 155).
Low-gain hearing aids, another option, are hearing aids that are worn in both ears and are programmed with a low-gain approach, which provides a minimal amount of amplification. The hearing aids can be programmed with different noise reduction algorithms in an effort to isolate target sounds, such as speech, while dampening the sounds deemed by the hearing devices as unimportant in order to improve an individual’s ability to understand auditory information (Serra, 2017).
Possible Co-occurring Conditions
APD may occur as an isolated condition and may also co-occur with other diagnoses. People with strong intellectual abilities, including gifted individuals, have also been identified with APD (Rigo et al., 1998). Obtaining a proper diagnosis is essential for implementing proper treatment and management strategies. What may complicate the task of obtaining an accurate diagnosis is the fact that many of the most commonly reported behaviors of APD are also often reported in individuals diagnosed with ADHD, autism, anxiety, dyslexia, and other learning challenges (Dawes & Bishop, 2009; Lawson et al., 2015). For instance, a systematic review of 13 studies with small sample sizes found significant symptom overlaps between APD, dyslexia, and ADHD that were indistinguishable from one another (de Wit et al., 2018). Using factor analysis, a sample of 110 children ages 6–11, children with suspected APD also had challenges with working memory, executive attention, and processing speed (Ahmmed et al., 2014). These challenges are also indicated in other learning disabilities and ADHD. Studying 104 children and teens with ADHD, Ghanizadeh (2009) found that those who were diagnosed with oppositional defiant disorder (ODD) or separation anxiety disorder (SAD) endorsed many more auditory processing challenges (as indicated on a checklist) than others with only ADHD.
Back et al. (2022) found that differences in intelligence and executive function can affect the results of some test batteries for APD, and called for better methods to disambiguate APD from cognition. A similar result had been found earlier by Rigo et al. (1998) where low-achieving gifted students scored significantly lower on measures of auditory processing than high-achieving gifted students, suggesting that APD may be a cause of the lower achievement. However, only a few of the auditory processing measures for the low-achieving gifted group were significantly lower, whereas for learning disabled non-gifted students, all of the auditory processing measures were significantly lower. These data suggest there may be nuances to detecting APD in gifted children depending on which assessments are used.
ADHD and APD
ADHD and APD present analogously and can be difficult to discriminate. There has long been evidence that individuals with APD were diagnosed instead with ADHD (Riccio et al., 1994). Keller (1992) also noted, A diagnosis of ADHD should not be made without first ruling out the possibility that APD might be mimicking ADHD. I have had the opportunity to evaluate children who I believe were erroneously provided stimulant treatment, who did not benefit from the medication, and who had auditory perceptual disorders without ADHD. When stimulant treatment was stopped there was no change in their behavior functioning or school performance. (p. 113)
Dawes and Bishop (2009) added, Although the clinician needs to be alert to the possibility that poor attention may affect performance on tests of auditory processing, it does not seem reasonable to argue that APD is just another way of describing ADHD. Rather, it seems as though APD and ADHD are frequently co-morbid while being distinct entities. (p. 453)
More recently, researchers have attempted to better delineate ADHD and APD diagnoses. APD has presented in individuals as difficulty focusing, distractibility, and/or inattention when extraneous background noise is present. However, in a quiet environment, these individuals did not exhibit those behaviors (Chermak & Bellis, 2014). Conversely, individuals with ADHD will exhibit these same behaviors regardless of the type of acoustic environment. Gyldenkærne et al. (2014) studied more than 100 children with listening difficulties and confirmed that while 34 children were found to have both APD and ADHD, the remaining children did not. They were indeed received separate diagnoses and could be disambiguated.
Dyslexia and APD
More than 40 years ago, Welsh et al. (1980) reported a high incidence rate of both dyslexia and APD occurring in the same students with 50% of the dyslexic students they studied also having APD. Researchers continue to see this overlap. Banai and Kraus (2014) observed that individuals diagnosed with APD, dyslexia, and/or specific language impairment often reported the same behavioral manifestations. Hugdahl and Hellend (2014) further observed, “Children with dyslexia show impairment of central auditory processing, with regard to both asymmetry for phonology and speech processing and for cognitive control factors” (p. 181). Lewandowska et al. (2013) reported similarly that auditory processing and dichotic listening predicted reading ability in dyslexic children. Kritsi et al. (2008) found that perception of phonemes was more impaired in students with APD and dyslexia combined than with either disorder alone. Dawes and Bishop (2010) found similar overlaps between dyslexia and APD, and surprisingly found that a third of their sample also scored clinically significant on an autism screener despite not having a formal diagnosis of autism.
Clinical Data
Two of the co-authors conducted two brief case file reviews by drawing random samples from their archive of clinical APD data. All of these individuals included in these file reviews gave written, signed permission for their data to be used for research purposes. Clients travel to the clinic from across the entire United States and internationally, creating a geographically diverse pool of clinical data. These clinical data suggest suitable opportunities for further research. Still, conclusions should not be based on these brief file reviews.
Case File Review of 1000 Individuals with APD
The first case file review looked at the records of 1000 randomly selected children and adults who had been diagnosed with APD between 2007 and 2020. Files were chosen by randomly pulling approximately the same number of client folders out of each of 36 filing cabinets (total pool was approximately 3000 files). The intent of this review was to document the effectiveness of an FM system as compared to the passive ear filter in individuals with APD. Individuals were tested in the sound booth using CSU’s soundfield configuration protocol, presenting single-syllable words in the presence of white noise to determine speech understanding scores (Burleigh et al., 2002). Different mono-syllabic word recognition lists were employed for each test condition. Individuals’ speech understanding scores were obtained first to establish their baseline understanding in a noisy listening environment. Our sample population diagnosed with APD was able to repeat a mean of 58.96% of words correctly without the use of any assistive device (M = 58.96%, SD = 7.83).
When the same individuals were then tested with an FM system in a headphone configuration, utilizing the same listening environment and testing protocol, their speech understanding scores reported a mean of 87.82% words correct (M = 87.82%, SD = 5 .68), an improvement of 28.86% above baseline scores (p < .0001, r = .90).
When testing the passive ear filter, individuals wore a stock ear filter in one ear and repeated back target words in the same noisy listening environment, with both the words and white noise playing on speakers as in the baseline test case. Then the protocol completed with testing the stock ear filter in the other ear. In the passive ear filter condition, our sample population of 1000 individuals was able to repeat a mean of 85.51% of words correctly (M = 85.51%, SD = 5.34) with the passive ear filter in their optimal ear. This was an improvement of 26.55% above baseline scores (p < .0001, r = .89).
Case File Review of 55 Gifted Individuals with APD
The second case file review examined 55 randomly selected files of self-reported gifted individuals ages 4–21 years (64% male, n = 35; 36% female, n = 20) seen at this APD clinic from 2013 to 2021 who were diagnosed with APD. Case history information completed by families reported behaviors and previous diagnoses for each client, and granted permission for their data to be used for research purposes. Files were chosen by randomly pulling client folders out of filing cabinets, rejecting any that did not self-report giftedness.
In this sample, 60% (n = 33) of the gifted individuals with APD had also been diagnosed with visual processing challenges and 20% (n = 11) had been diagnosed with dyslexia. Additionally, 36% (n = 20) of these individuals reported reading difficulties, 40% (n = 22) had been diagnosed with other learning difficulties, and 24% (n = 13) had been diagnosed with ADHD. Of the individuals who had been diagnosed with ADHD in this sample, six individuals reported using an ADHD medication, however, four of those reported no benefit and/or no positive change following the use of medication.
With respect to diagnostic assessment, only 16% (n = 9) of gifted students with APD demonstrated auditory processing difficulties at both the cortical and brainstem levels. Many of the gifted individuals in this sample, 84% (n = 46) evidenced only brainstem inefficiencies with auditory processing, while 100% of this sample showed difficulties at the brainstem level. This clinical data highlights the importance of using auditory processing measures that are sensitive and specific to both the cortical and especially the brainstem areas of the CANS for accurate diagnosis in the 2e population.
Figure 1 illustrates the behaviors in this clinical sample of gifted students with APD. The top 10 reported behaviors included: (a) easily distracted, (b) difficulty following directions, (c) sensitive to loud sounds, (d) experiences anxiety, (e) easily frustrated, (f) forgetful, (g) difficulty completing assignments, (h) writing difficulties, (i) appears confused in noisy places, and (j) slow to start new tasks. When a gifted individual exhibits any of these commonly reported behaviors of APD, a referral for a comprehensive evaluation by an audiologist specializing in APD should be considered. Behaviors of 55 self-reported gifted individuals later diagnosed with APD.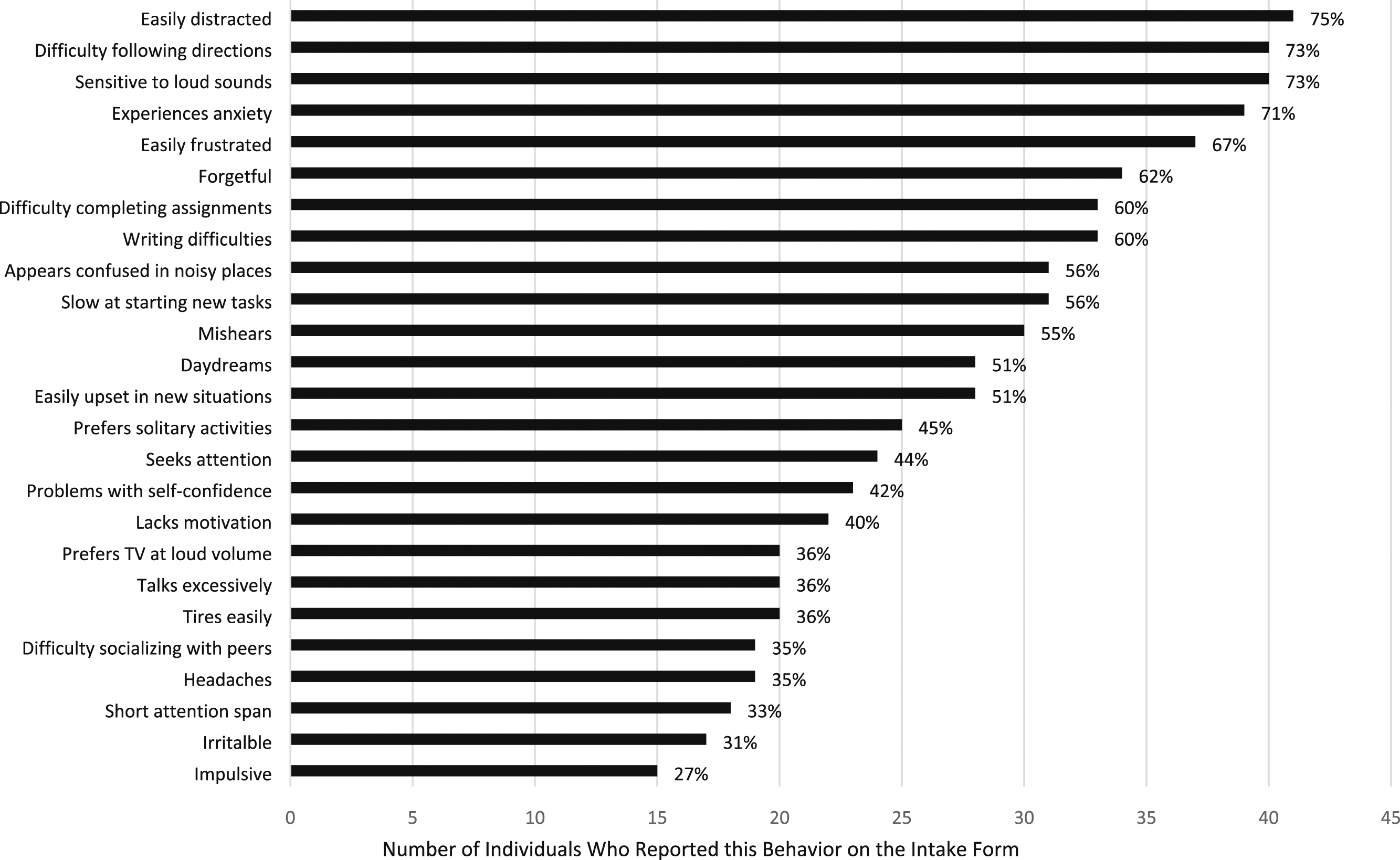
Vision Processing Disorders
Vision encompasses many visual skills, of which eyesight is only one aspect (Scheiman & Wick, 2019). Eyesight, also known as visual acuity, is a measurement of the smallest level of detail one can see from a set distance away. Visual acuity tends to be the most highly emphasized measurement during a vision assessment, and individuals are often informed that their vision is normal if they have a visual acuity of 20/20. Still, visual acuity is just one component in the overall process of vision. Vision also includes understanding how far away things are in space, being able to focus the eyes at that distance accurately over time to maintain targets as single and clear, and deriving meaning and conceptual understanding from those visual details. Visual processing also includes how the brain integrates various pieces of sensory information together, such as visual along with vestibular or auditory input, to plan an appropriate motor or cognitive response.
Consider the example of a student copying from a blackboard in a classroom. The student needs enough visual acuity to be able to discriminate which letters or numbers are on the board. The student must also have adequate eye movement control, or ocular motility, including both pursuits and saccades. Efficient pursuits are the ability to smoothly follow a moving target such as a ball, whereas efficient saccadic jumps enable tracking from one point to another, such as from word to word when reading. Some children’s eye movements are imprecise, and as they attempt to move their eyes from one word to the next, their eyes move too far or too little, and the child loses their place (Scheiman & Wick, 2019). This child may have symptoms such as omitting words or lines of text when reading, re-reading text, or needing a finger or a marker to keep their place.
Accommodation is another visual skill critical to academic success. A crystalline lens inside of each eye either flexes to bring near targets into focus or relaxes to bring distance targets into focus. One should have comfortable flexibility and stamina of this lens control, without accurate accommodation there is difficulty rapidly bringing either far or near targets into focus (Scheiman & Wick, 2019). A student with accommodative dysfunction attempting to copy from the board struggles with either the board or the near page appearing blurry or causing eyestrain.
In contrast to accommodation, vergence eye movements are the ability for both eyes to move in tandem to point to the same location in 3D space. The individual should be able to change their eye alignment to diverge or straighten their eyes to look far away, or similarly, to pull in or converge their eyes together to look at a near target. These eye movements should be simultaneous and accurate, or the student will experience double vision or eye strain. With underdeveloped vergence skills, one eye is misaligned from the other and the two eyes do not point to the same depth or distance from the individual (Scheiman & Wick, 2019). This often is a slight misalignment that is not cosmetically noticeable, though in more severe cases, one eye may be observed to turn inwards or outward. Any amount of misalignment between both eyes may cause symptoms such as double vision, eyestrain, headache, distractibility, or targets such as words to float around or flip. Accurate convergence and divergence are also critical for robust 3D depth perception, and any misalignment between the two eyes will cause a reduction in depth perception and subsequent difficulty with knowing how far away things are in space. Poor convergence or divergence skills prevent a student from being able to move their eyes comfortably from the whiteboard to their near page, and back again. Furthermore, lack of depth perception may provoke anxiety when an individual can’t accurately judge their distance from others, whether in a crowd or on the athletic field (Scheiman & Wick, 2019).
Vision processing skills further include visual perception skills or how a child’s brain makes sense of their incoming visual information (Press, 2017). The child needs to develop strong visual figure-ground skills, the ability to filter out irrelevant information, so that they can focus their attention onto a target without being distracted by surrounding details (e.g., clock on a wall). The child also needs strong visual form constancy, the ability to recognize the same object despite changes in orientation or position, so they can recognize the same material such as a mathematical formula whether it is written in a horizontal or vertical fashion. Visual sequential memory is needed so they can recall letters, numbers, or words in the appropriate order as they copy or write. Visualization, the ability to hold visual images in the mind’s eye, is another skill used in writing, reading, or copying.
Diagnosis
Many of these visual processing skills are not dependent on visual acuity and a simple visual acuity or eyeglasses measurement is not adequate to assess for VPD; hence, VPD is rarely noticed during a routine eye exam. VPD must be diagnosed by a developmental or behavioral optometrist who specializes in functional vision assessments that include measuring ocular motility, vergence control, 3D depth perception, accommodation control, and visual perceptual skills such as visual memory. Common assessments used to diagnose VPD include NSUCO (Nova Southeastern University College of Optometry) Oculomotor Test, Developmental Eye Movement Test, Near Point of Convergence Test, Stereopsis Test, Phorias and Vergences Test, Negative and Positive Relative Accommodation Test, and Test of Visual Perceptual Skills. A deficit in any of these areas, or combined deficits across these various skills, contribute to fatigue and frustration as the individual expends excessive effort to visually interact with their surroundings.
Intervention
VPD can be treated with vision therapy, a series of activities or exercises that guide the student to build their visual processing skills. Vision therapy is conducted under the supervision of a developmental optometrist who structures targeted vision therapy activities based on the child’s specific strengths and weaknesses found during the examination. A vision therapist may work alongside the developmental optometrist to facilitate the vision activities.
Vision therapy emphasizes neurological processing. A common misconception is that vision therapy strengthens the muscles around the eyes, when in fact vision therapy strengthens the neurological pathways that communicate information to and from the eyes (Ciuffreda, 2002). For ocular motility or vergence control, the muscles controlling eye movements do not become stronger or larger, but instead the brain is able to coordinate moving the muscles around both eyes with better fine motor coordination. Additionally, the visual perceptual skills of deriving meaning from visual input are not dependent on musculature, but instead depend on neurological processes such as the ability to select which visual details to pay attention to, process where they are in space, discern what those visual targets represent, and decide how to respond to them.
The Convergence Insufficiency Treatment Trial (CITT), a randomized double-blind study of 221 children, reported that office-based vision therapy in conjunction with daily exercises at home surpassed either home exercises (called pencil pushups) or computer software programs in reducing patient symptoms and improving their clinical measurements of their vergence skills (CITT Study Group, 2008). Additionally, a 2012 study found that parents reported fewer academic concerns after children’s convergence insufficiency was treated with vision therapy, demonstrating a link between VPD and academic performance (Borsting et al., 2012).
Other studies have found that vision therapy was not consistently effective, which led to confusion, even among eye care providers (Rawstron et al., 2005; Rucker & Phillips, 2018; Wang & Kuwera, 2022). Some ophthalmologists and other specialists advised parents not to pursue vision therapy based on these conflicting results. Vision therapy was less effective when activities are assigned with a blanket approach; however, therapy studies tended to have strict protocols in which each patient was assigned the same visual therapy activities regardless of individual differences among patient needs. This continued debate reflects the current state of the field and the need for additional research.
Supplementing vision therapy activities, lenses (such as glasses or contact lenses) may be prescribed to improve visual processing skills. This often includes lenses that enlarge text which may reduce eyestrain, blurry vision or visual clutter, or could include prisms to further help relax the visual system.
Possible Co-occurring Conditions
Vision processing disorders cause symptoms that are also commonly associated with dyslexia, ADHD, or other learning challenges. A team of researchers from Ohio State University linked vision issues with an increased chance of a child having an Individualized Education Plan (IEP) and learning problems (Walline & Carder, 2012). Visual findings, including refractive error, convergence, eye alignment, and accommodation, were compiled for 225 children aged 5–18 years old (M = 9-year-old). Convergence insufficiency was diagnosed in 17.5% of these children with IEPs (compared to 8.4% of the general population), and accommodative deficits were present in 17.3% of the IEP children (compared to 9.4% of the general population). Strikingly, these vision processing diagnoses of convergence or accommodative dysfunction were twice as likely to be diagnosed in a child with an IEP compared to their peers. Similarly, children with IEPs were more likely to have a cosmetic eye turn (strabismus), amblyopia (lazy eye), or blurry vision secondary to refractive error that requires the use of corrective glasses or contact lenses. Walline and Carder concluded, There is considerable association between ocular anomalies and poor school performance. These problems are illustrated by the high prevalence of a variety of eye problems experienced by the patients with IEPs. In fact, only 29.8% of the IEP patients did not require any treatment. Out of the 179 IEP patients who required some form of treatment, 124 (69.3%) would have passed a distance visual acuity screening program. (pp. 91–92)
These data suggested that a substantial number of these children with IEPs and vision challenges did not need glasses for blurry vision or refractive error; rather they had some form of VPD.
ADHD and VPD
VPD has also been associated with ADHD. The American Psychological Association’s Diagnostic and Statistical Manual (DSM-5-TR) defines ADHD as a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development (American Psychiatric Association, 2022). A pediatric ophthalmology practice found that convergence insufficiency was three times more likely in a child with ADHD than in the general population (Granet et al., 2005). Another study from the Southern California College of Optometry similarly found that children with convergence insufficiency score higher on the psychosomatic, learning problems, and hyperactive categories of the Connors’ Parent Rating Scales when compared to a group of children with normal binocular vision (Borsting et al., 2005).
Dyslexia and VPD
There is also notable symptom overlap between VPD and dyslexia. A 2018 study found that accommodative, vergence, or ocular motor dysfunctions were more common in a group of dyslexic students when compared to a control group mated by age (Raghuram et al., 2018). Comparing the percentage of these conditions in dyslexics versus their matched peer group: 55% versus 9% had an accommodative diagnosis, 34% versus 15% had a vergence diagnosis, and 62% versus 15% had ocular motor issues. This echoes the findings from the Ohio State University study that explored a general education classroom which included children with IEPs (Walline & Carder, 2012). However, while both disorders can certainly coexist, not all dyslexic students have vision processing challenges. Georgiou et al. (2012) found that only 11 of 21 dyslexic students in their study had vision processing deficits and concluded that these were separate conditions.
Hatch (2020) conducted a meta-analysis of 11 different studies that objectively measured eye-tracking movements while reading with a computerized instrument, such as RightEye or Visagraph. These instruments measured ocular motility via the detection and recording of pupil reflexes to record fixations and regressions (fixations are the eyes’ ability to stop on a target, and regressions are a backwards eye movement as the eyes jump back from right to left when the child is attempting to read text). Hatch found that children with dyslexia or reading disability fixated 2.33 times longer compared to age-matched controls when reading words. Children with dyslexia also had on average 1.58 times more fixations and 1.83 times more regressions during word reading than the control group.
This meta-analysis raised the question of whether eye-tracking ability precedes reading ability, or whether abnormal results in eye tracking are instead due to dyslexia (Hatch, 2020). To address this, let us first explore dyslexia and the skills necessary for good reading. For a child to learn to read the word wig, their auditory processing system must be able to discriminate the sounds/w/-/i/-/g/via phonological awareness while simultaneously perceiving the letters w-i-g (Shaywitz & Shaywitz, 2020). By linking these sounds with the written letters, the child learns the correspondence between phonics sounds and symbols and will learn to decode written text. VPD interferes with this learning process, as poor vergences or accommodation can make the letters double, blur, or float on the page and appear out of order. An oculomotor issue will also interfere with learning to decode, as a child’s eyes may skip over some of the letters present in the word.
As discussed in previous sections, APD is also strongly connected to dyslexia. In a study of 24 dyslexic students, 88% (n = 21) of the students had visual attention deficits, 83% (n = 20) had auditory processing deficits, and 50% (n = 12) of the students had both visual and auditory difficulties (Gokula et al., 2019). Eide and Eide (2006) also reported a variety of presentations of dyslexia, including 20%–30% of dyslexics primarily have deficits in phonics or sound processing issues, 20%–30% primarily have visual memory or sight word issues, and 50%–70% of dyslexics have a mixed profile. For dyslexics with phonics issues, APD may further hamper a child in decoding due to poor sound discrimination, preventing them from linking sounds to written symbols. If so, children may need both auditory supports and explicit phonics instruction to strengthen their decoding skills. Alternatively, visual processing deficits in the child with both VPD and dyslexia may impede the child in visually perceiving the letters as they are attempting to link them to sounds, and these children may need visual processing supports. For dyslexics with sight word issues, orthographic or sight word memory was largely dependent on visual memory; dyslexics who struggled in this area could benefit from visual perceptual memory training (Center et al., 1999). Overall, the mixed profile of the different challenges in those diagnosed with dyslexia has led to some confusion about how to effectively treat dyslexia.
The American Academy of Ophthalmology (2014) stated that vision therapy was not helpful for dyslexia, contradicting others who have argued the opposite (Werth, 2021). This disagreement is likely due to studies that failed to differentiate between VPD and dyslexia, and used one specific treatment approach for a condition that is diverse and required a spectrum of intervention strategies. For the subset of dyslexic children who also have VPD, vision therapy would be helpful alongside traditional phonological and phonics-based dyslexia interventions. However, not all dyslexic children have VPD, and hence vision therapy would not be helpful for them. Thorough assessment by an interdisciplinary team that evaluates for both dyslexia and VPD is essential to ensure that the full diagnostic picture is uncovered.
In the gifted population, a suspicion for stealth dyslexia must be considered for a child who appears to read well enough, but whose reading and writing skills are not congruent with their intellectual abilities. Due to concurrent language strengths and ability to read via sight words, they may be able to mask their phonological reading deficits early on in their academic careers, but, as academic materials become more demanding, the child’s coping strategies may falter. This could indeed be stealth dyslexia, but it could also be a sign of VPD as text becomes denser and writing demands increase, putting more stress on the visual system. Therefore, if a gifted child shows a discrepancy in their written language or reading abilities as compared to their oral language abilities, they should be assessed for VPD as well as stealth dyslexia.
Case Studies
Two of this article’s co-authors selected case studies from their VPD clinic to illustrate some of the ways visual processing disorder can present in the 2e population. All names provided are pseudonyms and parent permission was secured to publish these case profiles.
Mike
Mike, an energetic 6-year-old boy, was brought in for evaluation after he described to his mother that he was seeing double when attempting to read. Mike had not mentioned his double vision prior to age six because he was under the impression that “everyone saw that way.” He had mentioned his double vision offhand to his mother on one occasion when he commented that the second copy was “not real” when he had attempted to touch it and his shocked mother then sought further care. Children with visual difficulties often do not articulate them due to not being aware of how others see and assume that their struggles are a typical experience everyone shares.
Mike had been diagnosed with autism and ADHD prior to his visual processing evaluation. His most recent neuropsychological evaluation had found that he had gifted visuospatial reasoning; he had outstanding ability to reproduce and manipulate complex visual-spatial patterns. The same neuropsychological evaluation had found difficulties with Mike’s sustained attention and fine motor control and had suggested that he be considered twice exceptional. During his vision processing evaluation, Mike was diagnosed with reduced eye-tracking skills, reduced depth perception, and reduced vergence stamina, which was a contrast to his strong visual perceptual skills. Twice exceptional children may have both weaknesses and strengths, and this may also be also reflected in their visual skills. While aspects of Mike’s vision were superior, he needed vision therapy to address other areas. Before treatment, Mike was only able to converge his eyes on a near target up to 4 prism diopters before he saw double vision. Mike was treated with a combination of reading glasses and vision therapy and graduated from the vision therapy program after his tracking, depth perception, and vergence control all improved. He can now converge up to 18 prism diopters while looking at a near target, and can read successfully without double vision.
Samuel
Samuel’s mother brought him to the clinic due to an intermittent red eye. Samuel, a pleasant 6-year-old boy, had been identified as gifted by his neuropsychologist and was enrolled in a specialized school curriculum, accelerating him one to two grade levels ahead of his agemates. He excelled in math and was at an average level of reading among his advanced peers. During the exam, Samuel was diagnosed with a freckle on the front of his eye, and appropriate treatment to minimize irritation of this freckle was recommended to reduce red eye. Samuel was also diagnosed with inaccurate eye tracking, low depth perception, and low vergence stamina. He did not report any visual symptoms to his mother, and his mother was not aware of visual difficulties beyond the occasional red eye. Samuel had become skilled at compensating for his visual struggles and did not display obvious signs of visual processing issues.
During Samuel’s visual processing evaluation and discussion with his mother, she noted that he tended to get bored when reading and wanted to stop after just a couple of pages. He would also mirror and reverse his letters more often than expected given his superior cognitive skills. Samuel also disliked sports and tossing and catching a ball. These were signs indicative of VPD, albeit more subtle ones that can be difficult for parents to relate to a vision processing issue. Samuel continues his treatment with a combination of vision therapy and reading glasses.
Cassie
Cassie, a cheerful 10-year-old, was brought by her mother to assess if she could benefit from vision therapy. She had been diagnosed with ADHD by her neuropsychologist. Neither Cassie nor her mother were aware of signs of a vision processing issue, but she was having difficulty with reading and writing. Her visual processing evaluation showed minimal issues with tracking and vergence control; however, Cassie scored well below average on the Test of Visual Perceptual Skills in the areas of visual discrimination (ability to discern fine differences), visual-spatial relationships (how different objects orient relative to each other), visual form constancy (ability to recognize the same object with differences in orientation), visual sequential memory (recall of visual targets in order), and visual figure ground (ability to focus on select visual details and disregard irrelevant visual stimuli). On the Beery-Buktenica Developmental Tests of Visual-Motor Integration, Cassie also scored low on visual-motor integration, the ability to use her vision to guide fine motor movements, such as tracing accurately through a complex maze.
Cassie began a course of vision therapy. In contrast to the first two cases included here, Cassie’s vision therapy did not emphasize eye tracking, vergences, or depth perception, but instead was largely focused on her perceptual skills. After 12 months of vision therapy, those areas showed improvement, and Cassie’s mother reported better reading and writing performance in school.
Conclusion
While there remain unanswered questions, there is a strong case to call for greater awareness and research considering APD and VPD in the context of a 2e student. Both APD and VPD have substantial symptom overlap with dyslexia and ADHD, which raises the question of whether some 2e students have been misdiagnosed or under-diagnosed when these foundational sensory factors have been overlooked. APD and VPD require a more comprehensive, team-based approach is for an accurate 2e diagnosis and identification of optimal intervention strategies. Neuropsychologists and other clinicians who are evaluating 2e individuals should consider including screening measures, and consider referral to a functional or developmental optometrist for any vision-related concerns, such as fatigue, blurriness, letter reversals, reading challenges, writing challenges, head turn/tilt, attention issues during visual tasks, clumsiness, or difficulty with eye-hand coordination. Similarly, if there are possible auditory-related concerns such as distractibility, difficulty following oral directions, sensitivity to loud sounds, anxiety, easily frustrated, writing difficulties, behavioral dysregulation in noisy environments, or trouble understanding words in background noise, clinicians should consider a referral to an audiologist who specializes in APD who uses an appropriately sensitive test battery to ensure an accurate diagnosis in the context of a gifted individual. Proper identification, management, and support of APD and VPD in 2e students could improve our ability to address student needs at the foundational level.
Footnotes
Acknowledgements
Thank you to Megan Swilley, Sally Krisel, Heidi Lack, Jenn Nee Knoo, Michelle Barmazel, Joy Lawson Davis, Gail Post, and Karen Arnstein for their thoughtful review of drafts of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.