
Abstract
This article examines how a group of microbiologists organized their practices for the governance of hospital infections, positioning the clinical microbiology laboratory as an obligatory passage point for such interventions and for a new, modern vision of the hospital as an institution cognizant of its infectious risks. Drawing on fieldwork, archival research and oral histories with former members of the laboratory at the Clínica Puerta de Hierro in Madrid, Spain, during the late 1960s, I argue that these microbiologists employed epidemiological tools to claim their authority over antibiotic governance and hospital infections. Particularly relevant was the epidemiological map, a blueprint of the hospital where lab staff pinpointed hospital infections of clinical concern. By describing and showing these paper technologies in symposia, published papers, and conference discussions, the maps both materialized the professional and disciplinary authority of the microbiology lab and assisted in enrolling clinical colleagues into new interventions for managing antibiotic use and containing in-hospital infections. Most significantly, the maps were able to transform the vision of the hospital architecture as infectious landscape, replacing the traditional idea of a space void of infectious risk with a modernized account of an institution capable of effectively controlling and governing the hospital's infectiousness.
Introduction
On a sunny morning of November 2023, I arrived at the café of a hotel in one of the coastal neighborhoods of Valencia, in the Mediterranean seaside of Spain. I had agreed to meet up with microbiologist María Santos, after e-mails and WhatsApp messages with her eldest daughter, whose details I had found on the internet. I wanted to ask her more about how they had begun their intervention to control antibiotic use and (resistant) infections at the Hospital La Fe in Valencia, and her memories of her time as one of the first trainee clinical microbiologists in Madrid during the 1960s. After an endearing conversation, we waved good-bye outside the hotel, both struggling to keep still in the heavy wind. There, we agreed that they would e-mail me some photos, documents and references of interest. Later that day, her daughter sent me a few e-mails full of attachments on behalf of María Santos, including photos, book chapter titles, and publications. Included was a PowerPoint that Santos had prepared to celebrate her and her husband's retirement in 2011 (see Figure 3). Little did I know that one of those slides contained copies of the map, forms, and graphs that they used at Hospital La Fe during the 1970s. The sight of those colored pins on the epidemiological map made me jump off my office chair; up until that point, these pins had existed only in my imagination. Visible on my PC monitor, they brought it home that the epidemiological map that this article focuses on was truly a “paper technology” (Hess and Mendelsohn 2010), to be tinkered with by design. It demonstrated how the map and its pins have circulated through several professional generations, embodying a way of understanding the hospital and the task of overseeing its infections that has carried on in the years since María Santos first drew on the map of La Fe.
In the 1960s, the epidemiological map and the colored pins embodied a new mode of expertise and authority in the hospital. Recent scholarship on science and technology studies (STS) has explored the performative capacity and epistemic authority of epidemiology, revealing how mapping and modeling practices have become entrenched in narratives about risk and appropriate intervention (Bauer 2014; Engelmann et al. 2023; Engelmann 2021; Rhodes and Lancaster 2020). The practice of mapping infections in the hospital emerging from Manuel Moreno López's and María Santos's papers belongs to a longer genealogy of epidemiological “generative machines” (Bauer 2014), one which could be grasped with hands (de Chadarevian and Hopwood 2004) by clinical microbiologists. The map, as I will show, assisted microbiologists in making their own claims to authority and illustrates the persuasive and generative power of epidemiological media.
This article examines how the mapa epidemiológico (epidemiological map), served as an authoritative instrument in the emerging setting of hospital epidemiology in Spain during the 1960s and 1970s. This account reveals how the epidemiological map was leveraged by microbiologists to claim authority over antibiotic use and hospital infection management at the Clínica Puerta de Hierro (hereafter Clínica) in Madrid, Spain, including through the creation of a new intervention, the Política de antibióticos (antibiotics policy). As I show, these microbiologists used epidemiological tools and tropes to gain legitimacy within the Clínica as well as among their professional colleagues in Spanish medicine, leaning on the authority of the epidemiological map to promote an understanding of hospitals as spaces of infection and entities responsible for microbial oversight. These tools provided the material, professional, and disciplinary means for the clinical microbiology laboratory to emerge as an obligatory passage point (Callon 1984; see also Latour 1983; 1988) for (anti)microbial management, and for microbiologists to gain authority and new roles in governing antibiotic interventions, to advance the vision of a new, self-observing hospital attuned to the infective risks it harbors.
The analysis also demonstrates how the reorganization of clinical microbiology in medical expertise took place in the context of broader social and economic changes in 1960s Spain. The years between 1964 and 1970 are often characterized as the period when the Francoist regime began to open up politically and economically. During this time, Spain became integrated into international markets and institutions such as the United Nations Educational, Scientific and Cultural Organization (UNESCO). International tourism became a central feature of Spanish economic growth, increasing from 7.5 million tourists visiting Spain in 1961 to an astonishing 17 million just 5 years later, in 1966 (Fernández-Cebrián 2023, 7). This social and economic transformation played a direct role in the creation of hospitals like the Clínica, whose architecture, technological accoutrements, and clinical services were advertised as emblems of Spanish modernity (No-Do 1964). This description of one of the first cases of an antibiotic-resistant infection in a hospital in London offers a glimpse into Spain's changing place in international economics: “Early in 1964 a single infection focused our attention upon an entirely different but equally alarming aspect of the problem of antibiotic resistance.…The patient was infected while on holiday in Spain and was admitted to hospital severely ill on his return” (Ridley and Phillips 1966, 5). Such opening of Spain to international trade and mass tourism would also have microbiological consequences.
The discussion proceeds in four sections. A first section situates the epidemiological map in the larger literature on the history of hospital infections, epidemiological tools and performativity, and paper technologies. I argue that the map's malleability as a paper technology that could be tinkered with provided the means for these actors to claim their authority over antibiotic governance and hospital infection oversight. The second section introduces the Clínica and its microbiology lab, and characterizes how the epidemiological map figured in their strategies for managing hospital infections. The third section describes the work of the lab's chief of service, Manuel Moreno López, to demonstrate how epidemiological expertise was utilized to depict the hospital as a space for epidemiological events, and to position microbiology as the authoritative caretaker of in-hospital antibiotic use. Fourth, I situate how this discourse influenced Spanish medicine within and beyond the Clínica through the example of the presentation of the Clínica's infection control and antibiotic policies at the “I Symposium on Antibiotic use and Hospital medicine,” celebrated in Madrid in the Autumn of 1968.
Making Antibiotic Authority: Paper Technologies of Epidemiological Expertise
This research builds on scholarship on the history of infections in Western hospital institutions. Historians of medicine have observed how debates around hospital infections, antibiotics, and antimicrobial resistance in the second half of the 20th century became a fertile ground for hospital microbiologists to legitimate their authority and role within the hospital workforce. To this end, microbiologists made use of a variety of tropes, practices and concepts from other sciences, such as evolutionary biology (Gradmann forthcoming; 2017), ecology (Condrau and Kirk 2011), or as in this case, epidemiology, with the aim of transforming the enterprise of the clinical laboratory and the role of the microbiologist in the hospital. While epidemiological methods and tools had the power of boosting the authority of clinical microbiology in some instances (e.g., Hillier 2006), in other cases, bacteriological theories or concepts became integrated into modes of reasoning characteristic of epidemiology; demonstrating how the relation between microbiology and epidemiology could at times be one of both fields competing for authority over the question of epidemics and infection dynamics while at other times their instrumental relationship could turn more ambiguous (Amsterdamska 2004; 2005). Focusing on the rise in use and circulation of the so-called “phage typing” technique as a tool to control staphylococcal outbreaks in hospitals across the world during the 1950s, Hillier (2006) problematized how these epidemiological events became crucial for hospital microbiologists to claim authority and expertise in hospital medicine and ownership of infection control strategies. I build on this scholarship to show how another technique—the epidemiological map—was used by microbiologists to legitimate their role in relation to the governance of hospital infections.
This research also directly contributes to a body of STS scholarship that has historicized and problematized the science of epidemiology (e.g., Amsterdamska 2005; Bauer 2014; Engelmann 2021; Rhodes and Lancaster 2020). I focus on a material object—the mapa epidemiológico (epidemiological map)—to demonstrate that it is the malleability of epidemiological media that facilitates its performative capacity and professional authority. Epidemiological maps, as Tom Koch (2011) has argued, can work as experimental systems to explore epidemiological challenges and act as tools to reason with. Here, the map's significance as an epidemiological tool lies on how it demonstrates that it is through people's fingertips, and their tinkering with paper copies, colored pins, and diagnostic and clinical information files, that epidemiological knowledge is generated. Consequently, such epidemiological reasoning saliently persuades and makes a case for these actors to exert their authority within the Clínica and beyond.
Analytically, I draw inspiration from historiographies of science and medicine that have studied how paper tools and paper technologies have played a role in the management of information in experimental scientific practice and processes of knowledge production. The notion of “paper technologies” (coined by Te Heesen's [2005] study of the scientific notebook) facilitates an exploration of the experimental and pragmatic uses of material and paper-based fact-keeping techniques (e.g., list making, pasting notes, filing cabinet) in a variety of aspects of science, technology and medicine. Hess and Mendelsohn (2010; see also Hess 2018) suggest that the notion of paper technologies permits an analysis of humanist text-based practices as applied to medicine—practices which made possible the drawing of generalizations from specific case studies. Building on this research in the history of science and STS, my framing of the mapa epidemiológico as a generative “paper technology” permits an analysis not just of the socio-material practices or debates that occurred, but most crucially, of the knowledge-making process, and the expert authority and legitimization that derived from tinkering with a model of the hospital's infection on paper.
Firstly, I show that the map acted as an object that was tinkered with and grasped with hands (Engelmann 2021; de Chadarevian and Hopwood 2004), pinned and unpinned. Furthermore, such mapping was accompanied by a constellation of practices (including microbiological culturing and typing, antibiotic sensitivity testing, collection of clinical and administrative information, collection of statistical data) that made possible the confirmation of an infection case that preceded the pin on the paper map. Secondly, the map also acted as a discursive object—included as a figure in medical and scientific presentations and publications—contributing to showcasing and legitimizing the intervention when these microbiologists presented their work to a diversity of audiences. Crucially, I suggest that in the space of the modern hospital, the epidemiological map acted as a generative epidemiological machine, capable of intervening in the very phenomena that it was responding to. Or to say it differently, the map, and its constellation of practices and processes, visually translated the hospital into a space of infection. Not dissimilar to how other epidemiological maps or models would visualize “population” or “geography” (Koch 2011), the mapa epidemiológico at the Clínica literally turned the hospital space into an infectious landscape or environment (ambiente in Spanish). By acquiring a performative role, the map did not merely assist microbiologists in reporting hospital infections; with staff literally placing colored pins on a piece of paper representing the hospital, the map also helped create a vantage point, a “vision” or gaze that transformed the literal architecture of the hospital into a geography of (hospital) infection readied for (anti)microbial governance.
The Clínica Puerta de Hierro: A Model of Microbiological Modernity
The Clínica Puerta de Hierro 1 opened its doors in July 1964, in a wealthy villa of the same name in northeastern Madrid (see Figure 1). Francoist Spain was then undergoing a series of social and healthcare reforms that included a revamped social security system, the Seguridad Social, and the passage of legislation such as the Ley de Hospitales (Hospital Act, Boletín Oficial del Estado 1962). Alongside exponential increases in state investment in hospital care, which prompted the construction of a number of new hospitals, these 1960 reforms demonstrated the growing valorization of healthcare institutions within the technocratic Francoist regime (Pieltáin Álvarez-Arenas 2003). The Seguridad Social system favored and provided the means for accessing treatment for illnesses (instead of disease prevention), and paved the way for a healthcare system designed to have hospital care at the center, and public health and community care at the fringes (Perdiguero-Gil and Comelles 2019a; see also 2019b; Comelles, Agís and Prats 2017; Barceló i Prats, Comelles and Gil 2019; Barceló i Prats and Comelles 2020; Barceló-Prats 2021). For reformers, medical professionals, and the general population, hospital-based healthcare was becoming a desirable, powerful and authoritative element of a new, modern Spain.
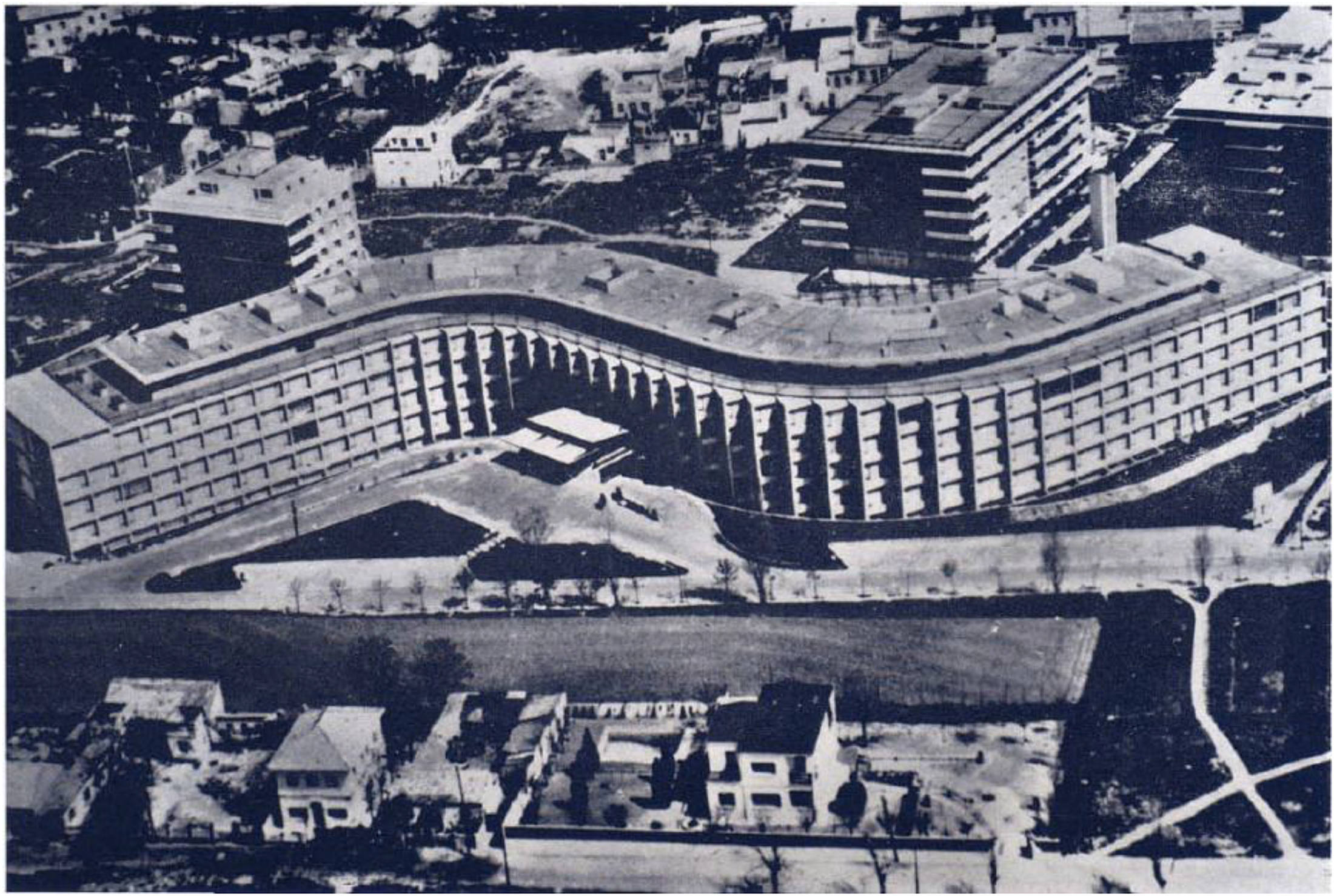
The S-shaped Clínica Puerta de Hierro, Madrid. Image reproduced from the original in Cuadernos de Arquitectura 1969, 73 (3 trim.), 34, with permission from the Col·legi d'Arquitectes de Catalunya (COAC).
The intertwining of hospital care with imaginations of Spanish modernity is made clear in the regime's propagandistic newsreel Noticiario y Documentales (No-Do 1964) produced to publicize the opening of the Clínica. In the footage, the Clínica is described as a “model” institution, served with materials of the highest scientific and technological standards. The film claims that the Clínica will have a cobalt unit, swimming pools for the rehabilitation of poliomyelitis patients, a radiodiagnostic service, and a TV-radiocontrol circuit surrounding the hospital. As the narrator, well-known journalist Matías Prats, describes the technological marvels of this new clinic, dictator Francisco Franco is shown walking through the hospital facilities, with doctor Segovia de Arana, the Clínica's medical director, guiding the tour (No-Do 1964).
The building that accommodated the Clínica had been constructed as a private clinic five years earlier, funded by the Dominican fathers of the Philippines.
2
The Instituto Nacional de Previsión (INP, Institute for National Provision) bought it at the start of the decade, with the purpose of adding it to the growing Seguridad Social network of clinics. It immediately underwent refurbishments to adapt its premises to its new clinical purpose.
3
With a unique S-shaped design resulting from the limited land space available in this affluent neighborhood, the Clínica was architecturally suited to become a vanguard institution of Spanish hospital care. For their part, the Clínica's co-directors, Segovia de Arana and Diego Figuera, dreamed of creating a truly modern hospital. Diego Figuera Aymerich (2002, 195–96), co-director and chief of surgery, recalls this dream in his memoirs: we agreed to call it ‘Centro Nacional de Especialidades Medicoquirúrgicas of the Seguridad Social’ [Social Security Center for Medico-Surgical Specialties]. We chose this pretentious name deliberately, to signal from the very beginning that it was going to be something different.…In that spring of 1964, a unique opportunity was opening before us. Finally, we could build in Spain the hospital that we had always dreamt of; modern in its organization and function, in the style of the best [medical] centers that we had got to know in other parts of the world.
4
Aspirations for the Clínica to serve as a truly modern hospital were not limited to its architectural ingenuity or its novel service organization. The vision of the modern, organized and forward-looking hospital also encompassed a new role for the hospital's microbiology laboratory, and a shift toward thinking of the hospital as a place of infection. The risk of contracting and spreading infections among hospitalized patients was a growing concern internationally. At the time, medical practitioners increasingly understood the hospital as a risky, dangerous environment (Gradmann forthcoming; 2017). Staff at the Clínica shared these concerns, as demonstrated by director Segovia de Arana's (1968, 45) speech: More than ever, it is of interest to know the predisposing and triggering causes of hospital-acquired infections in order to overcome, or at least reduce, their severity. For scientific, administrative and economic reasons, a hospital must make every effort to control infections. This can only be achieved when all members of a hospital are aware of the problem and contribute to solving it through coordinated, intelligent and sustained teamwork. There is no better index of hospital quality than the effectiveness of hospital-acquired infection control. The contrary is also true, since the most alarming infectious situation is always found in poorly organized hospitals.
Moreno López and his trainees established structures and practices to control hospital infections and antibiotic use shortly after the inauguration of the clinic. As co-director Figuera recounted in his memoirs, these practices emerged from the vision of the Clínica as a model modern hospital, where in-hospital risks of infection were managed by microbiological expertise. But a key element of these practices, as Figuera Aymerich (2002, 196–97) also recalled, was the creation of an epidemiological map of the hospital space itself: We set up a block of ten operation theatres, with their pre-operation theatre rooms and anesthetic rooms. We established ‘clean’ and ‘dirty’ zones, and rules for circulation across them to avoid contamination. Doctor Manuel Moreno established an efficient and to a great extent original system of control of surgical infections, with diffusion maps and treatment guidelines.
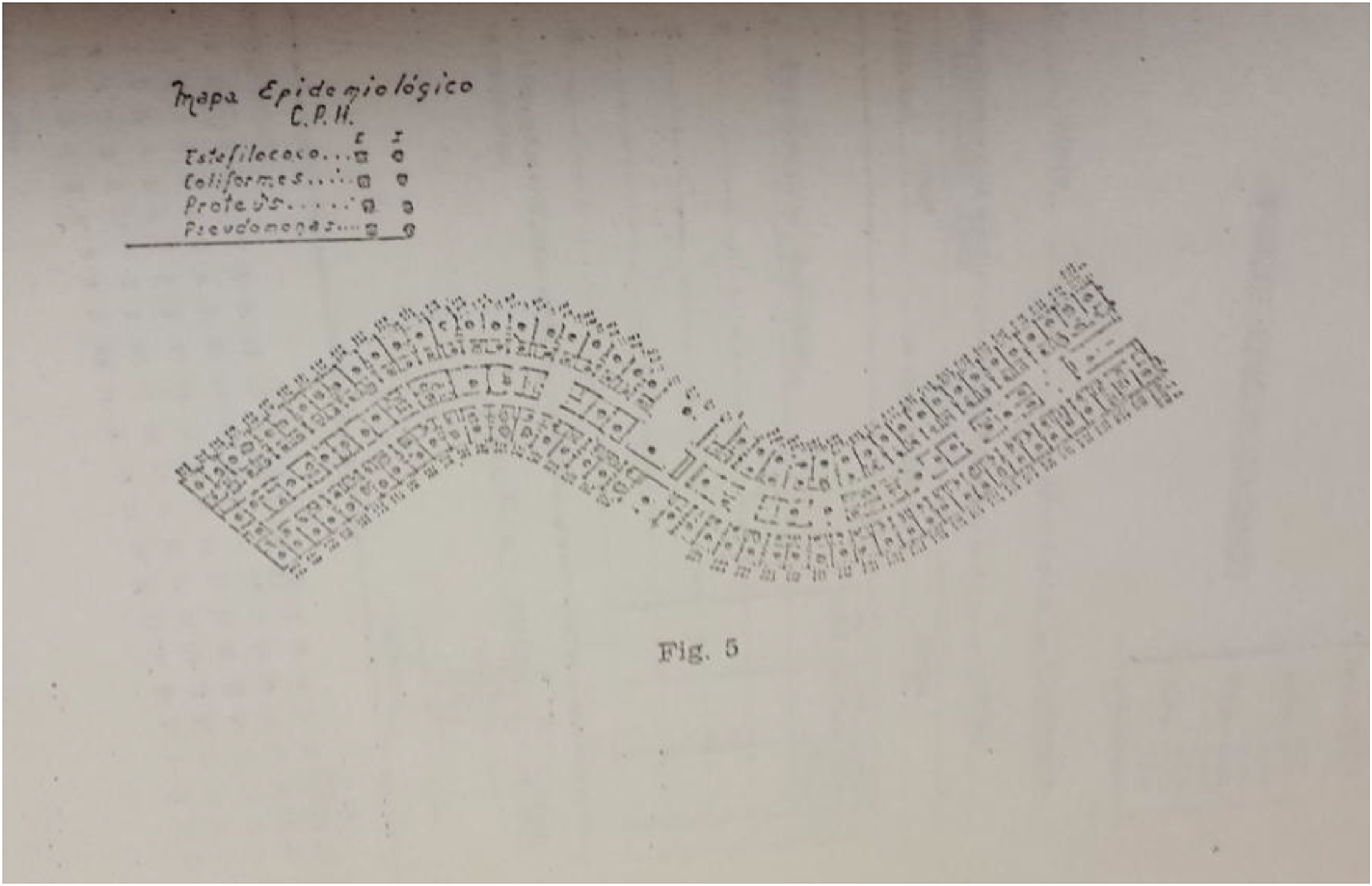
The mapa epidemiológico, in Moreno López (1970, 121). It shows the schema of the hospital rooms and a legend on the upper right-hand side with the list of the four pathogenic microorganisms overseen by the Servicio de epidemiología: Staphylococcus (Estafilococo), Escherichia coli (Coliformes), Proteus, and Pseudomonas. Image reproduced from the original in the journal Anales del Instituto Médico de Beneficiencia, with permission from the Department of Health, Gobierno de Navarra.
The Política de antibióticos (antibiotics policy), as the intervention became known at the Clínica, established that the use of non-essential antibiotics should be suppressed; the prophylactic use of antibiotics in surgery reduced to a minimum; and antibiotic treatments given in the correct dosage and time intervals only. Unanimously accepted at an all-staff general meeting, the Política de antibióticos also required the hospital to reinforce aseptic techniques in surgical procedures; design a containment area with increased transmission control measures; and carry out carrier control surveys among hospital staff to monitor hospital infections (Moreno López 1966). Finally, it was agreed that the Clínica would create a Comité de Infecciones (infections committee) to lead the design and implementation of hygiene measures, antibiotic use control, and hospital infection monitoring, as well as organizing regular training sessions.
Early in 1967, Moreno López received approval from the Clínica's co-directors to establish the Servicio de Epidemiología Hospitalaria (hospital epidemiology service) within the microbiology lab (Moreno López 1970). The laboratory was divided into two sections or services, Microbiología and Epidemiología, with distinct daily responsibilities and tasks. Namely, the Microbiology section was tasked with carrying out contamination and sterilization control studies, as well as typological studies of clinical samples (bacteriotipia) and producing antibiogramas (antibiotic sensitivity testing in English) to inform patients’ diagnostic results. Antibiograms generated in the Microbiology section would in turn inform antibiotic policing (literally, policía de antibióticos) and surveillance or computing of the diverse mechanisms of antimicrobial resistance sampled (computación de resistencias). These last two tasks were the jurisdiction of the Epidemiology section in the lab, along with carrier control studies (control de portadores), and recording of infection statistics (estadística de infecciones). Infection statistics were to be inferred from information collected through an epidemiological form (parte epidemiológico) for each patient's case of infection and pinned into the mapa epidemiológico (epidemiological map) (see Moreno López 1970, 118, Figure 4).
Trainee clinical microbiologists Evelio Perea and María Santos were heavily involved in the tasks of the Servicio de Epidemiología Hospitalaria. Under the direction of Moreno López, Perea, Santos and others took responsibility for collecting clinical and microbiological information by completing the epidemiological form for each individual patient of interest and updating the mapa epidemiológico. In an interview, Evelio Perea remembered how they set up the map in the hospital: (We) set up a (process for) monitoring rooms. In fact, informatics didn’t exist back then. So, we hanged a blueprint (with detail of the hospital) rooms on the wall. And on each room, we would put pins for the different bacteria we sampled. And this at least offered a global vision of the hospital. (Interview, 9 June 2021)
The reproduction of the blueprint of the S-shaped hospital, marked with pins indicating rooms occupied by patients with an active relevant infection provided these microbiologists with a practice for extracting and organizing knowledge, and a pragmatic form of surveillance of hospital infections. The practice of mapping the hospital fit smoothly with the modern hospital the Clínica's co-directors dreamt of. As Perea described, the map evoked a “global vision” of infections in the hospital, visualizing the invisible structures and risks of hospital infections and thus strengthening the Clínica as a space of governance and a model of microbiological modernity. Yet, as I address in the next section, the epidemiological map also acted as a performative technology for the Clinica's microbiologists, providing them with a tangible authority over hospital infections and centering the microbiology lab as an obligatory passage point for managing the hospital's (infectious) environment.
The Hospital as a Space of Epidemiological Explanation
In his writing, Moreno López repeatedly framed the hospital epidemiologically: as a space where epidemiological events occur, where sources of contagion could be found, where patients could be considered receptors and vectors of infection, and where chains of transmission, though inexorable, could be potentially tamed and controlled. For example, when he presented the intervention to his colleagues at the Clínica in a seminar for the first time, he did so as follows: For an infection to propagate, logically, three factors are necessary: a source, in this case the patient carrying the original strain; a transmission vehicle, in this case the contaminated material or carrier member of the hospital workforce and, a third factor, the subject susceptible of contracting the disease. All these phases exist in all hospitals. (Moreno López 1966, 3)
Epidemiological reasoning permitted a compelling and dynamic understanding of the sociotechnical, microbial and biological conditions of hospital infection, human disease, and hospital care. In his writing (see e.g., Moreno López 1970, 100, Table 1), sick hospitalized patients were categorized as either “vectors” (passing on the infection) or “receptors” (receiving infections, either from the hospital or from other causes beyond the hospital). Following this logic, a sick patient transferred from another hospital, a trauma patient hospitalized due to a serious accident, or a sick patient arriving infected from their own home could all be “infecting vectors,” with an “infectivity” considered as “extrinsic” to hospital practice. Similarly, a hospitalized patient with a digestive tract flora affected by the consumption of antibiotics, or one with low defense mechanisms due to a blood disorder, a tumor or a chronic debilitating illness, were categorized as “receptors” due to causes external to hospital practice. And a patient hospitalized for a long period of time due to surgery preparations or with a longer stay resulting from surgical wounds or radiation therapy was categorized as a “hospitalized receptor” (receptor hospitalario).
While presenting the Política de antibióticos to his colleagues at the Clínica in 1966, Moreno López explained that the sociotechnical, microbial, and biological conditions of hospital medicine had a detrimental impact on the health of their patients, particularly those undergoing surgery. Here again, he used explicit epidemiological terminology (e.g., host, reservoir, source of infection) to make his point. Somewhat poetically he noted that the microorganisms Proteus and Pseudomonas were sporadically appearing “en las heridas de nuestro hospital” (in the wounds of our hospital) (Moreno López 1966, 6), conveying an image of a hospital with fissures, susceptible to being affected by epidemiological events, involving infectious “vectors” and “receptors” intrinsic and extrinsic to the hospital. In his writings, Moreno López expressed a persistent anxiety. Hospitals were constrained in their ability to control the susceptibility of health structures to infection, and the iatrogenic effects of hospital infections on patients’ health and care. In an article, he lamented the limited utility of “the possibilities and techniques of antibiotherapy within present hospitals, where an inadequate construction, which has not taken into account infectious diseases, have made possible that both cross-infections and hospital infections have taken the form of nature (haya tomado carta de naturaleza)” (Moreno López 1968, 459). He became increasingly outspoken about the issue of hospital design and planning, as the following illustrates: The problem today is difficult to resolve. Avoiding a cross-infection is very easy if the source of endemic or epidemic infection is cut. However, without adequate confinement or triaging areas, patients are admitted to hospital already carrying strains that are multirresistant to antibiotics…. Preventing infections from spreading and stabilizing within the hospital under these conditions is impossible. Without adequate planning for the new hospitals that are being built, bacteriologists will have a lot of work. An adequate internal antibiotic policy will only serve to alleviate the problem, preventing antibiotics from becoming useless within the hospital premises. (Moreno López 1968, 459)
Legitimacy by Symposium: Carving a Space for Clinical Microbiology in Healthcare
Moreno López and his trainees presented this vision of the hospital and its infections, with the map at the center, in a symposium on antibiotics and hospital medicine. Held on Thursday 21 November 1968, the “I Symposium Internacional sobre Antibióticos y Medicina Hospitalaria” (hereafter Symposium) took place at the Clínica. The event provided an opportunity for Moreno López and his students to expand their sphere of influence: while their colleagues at the Clínica had welcomed the microbiology lab's interventions, the goal of hospital infection management required that others be convinced of the authority and value of microbiological expertise. The Symposium therefore served a twofold aim. Firstly, it offered an opportunity to publicly bring forward the image of the model hospital, and for the microbiologists to attach their program to that wider vision. For the Clínica to serve as the modern, efficient, scientific and technological hospital that its co-directors imagined, it could not afford to be dismissive about infections, the microbiologists argued. It had to be alert to the potential risk of disease transmission and resistance, and organized to monitor and know its microbes accordingly. Secondly, the event offered these microbiologists a space to showcase their approach to such an intervention, and legitimize their work among an audience formed by representatives of the state, clinical medicine, microbiology, and the pharmaceutical industry. The late 1960s and early 1970s were formative years for the discipline of microbiology in Spain. At this time, the career of clinical microbiology was nascent within the emerging healthcare systems and professions. As such, professional competencies, roles and authority in the governing of antibiotic interventions and hospital infections were there for the taking. Besides, the industrial economy of the laboratory and the antibiotic pharmaceutical industry were proliferating, and even academic microbiology was in a moment of change. Against this background, the Symposium at the Clínica turned into a crucial setting where the profession of clinical microbiology could legitimize its position in the future of healthcare.
The Symposium brought together a wide range of stakeholders. It was sponsored by Beecham Laboratories, a British pharmaceutical company with long-term industrial and corporate interests in antibiotic therapy research, production, and commercialization. Approximately 400 attendees from all regions of Spain came together to discuss the science of antibiotics, practices for testing antimicrobial resistance, and interventions to control antibiotic use and hospital infections. Several dozen physicians based at Puerta de Hierro also attended the event. Another many dozens came from diverse healthcare institutions of the Seguridad Social network, as well as private clinics and clinical laboratories across the country. Full professors and senior scientists (microbiologists, virologists, pharmacologists) based at major universities and research institutions joined these clinicians and clinical microbiologists to talk about antibiotics and hospital medicine too. Representatives from several pharmaceutical companies were present both as speakers and as part of the audience, including pharmaceutical company representatives of Beecham Laboratories, Eli Lilly, Pfizzer (sic), and the Spanish subsidiary of Bristol Myers. 6 The latter had strong corporate connections with the Spanish pharmaceutical company Antibióticos S.A. 7 (also present at the event), which distributed the great majority of antibiotic drugs in Spain during the 1950s and 1960s (see Santesmases 2018). International guests traveled to Madrid for the event, including clinical microbiologist Yves A. Chabbert (Institut Pasteur, Paris), clinicians D.H. Lawson and A.L. Linton (Western Infirmary, University of Glasgow, Scotland), as well as industrial researchers from Beecham Laboratories (England), and the Research Division at Lilly (United States).
Before this audience, Moreno López and his trainee collaborators presented the rationale behind the Política de antibióticos and the work, structure and practices of the lab service, including the epidemiological map. Evelio Perea, trainee microbiologist, speaker, and co-organizer of the Symposium, recalled how the event highlighted the influential standing of the Clínica and the role of its microbiology laboratory. Perea described an audience member confronting director Figuera about infections within the Clínica: The (Symposium) was a surprise in Spain. Some people stood up. I remember a surgeon, as they say, “de provincias” [i.e., from smaller urban nodes in Spain], who told Figuera—who was young at the time, but held a Chair (in surgery) and had studied cardiovascular surgery abroad in England: “Doctor Figuera, how is it that you have so many infections, and I don’t have any?” And Figuera responded, “it is not that you don’t have any, but that you don’t know that you have them!”… Then, after this Symposium, many people came to learn about the Infections Committee and hospital hygiene. (Interview, 9 June 2021)
The 1970s indeed saw many of these professional debates and power struggles for legitimacy and authority regarding antibiotic management and the knowledge of hospital infections proliferate and endure (see more in Moreno Lozano 2025). The prolific set of actors continued to discuss the role of microbiology in the management of hospital infections, extending to the interventions needed to control the use of antibiotics and the commercial ventures (namely antibiotic drug research and laboratory products) that would be required for clinical microbiology to take on its new role. Further symposia included the I Symposium Internacional de Antibiogramas (Madrid, 1969), the Symposium Internacional sobre Mecanismos de acción y espectro antimicrobiano de los antibióticos (International Symposium on Mechanisms of action and antibiotics’ antimicrobial spectrum, Zaragoza, 1970), and the II Symposium Internacional sobre los Antibióticos (Valencia, 1970). The latter was organized by microbiologist María Santos (with Miguel Gobernado), who I mention at the beginning of this article. Santos and Gobernado were both employed to run the microbiology lab at Hospital La Fe from its inauguration in 1969—another hospital constructed with the purpose of including it into the Seguridad Social network of clinics. The II Symposium hosted in Valencia, subtitled “El Hospital ante la Antibioticoterapia Extrahospitalaria” (The hospital in the face of antibiotic therapy beyond the hospital), brought together a similar confluence of international and national actors concerned with antibiotic management in healthcare.
I return to the slide on the PowerPoint file that María Santos and her daughter sent me as an e-mail attachment mentioned in the Introduction (see Figure 3). The presentation slide depicts the epidemiological map of Hospital La Fe, including: two blueprints of the hospital (the 10th floor of the main building on the top left-hand side, and the rehabilitation center on the top right-hand side), a sample of an epidemiological form on the bottom left-hand side dated February 1976, and a graph showing the progressive incidence of the main infections that affected the maternity ward (the legend reads: “Coli, Pseudomonas, Proteus, Staph. aureus, Mixed”). Marked with colored pins, in the fingertips of microbiologists Santos and Gobernado and their team, such a “vision” of a hospital in which (resistant) hospital infections could be mapped out and pinpointed, materially promoting this gaze that transformed the literal hospital blueprint into an (infectious) hospital environment. Moreno López's efforts had been successful, insofar as the map became a standard tool to establish this vision of the hospital, with many early-career clinical microbiologists populating hospital laboratories across the country in the 1970s.
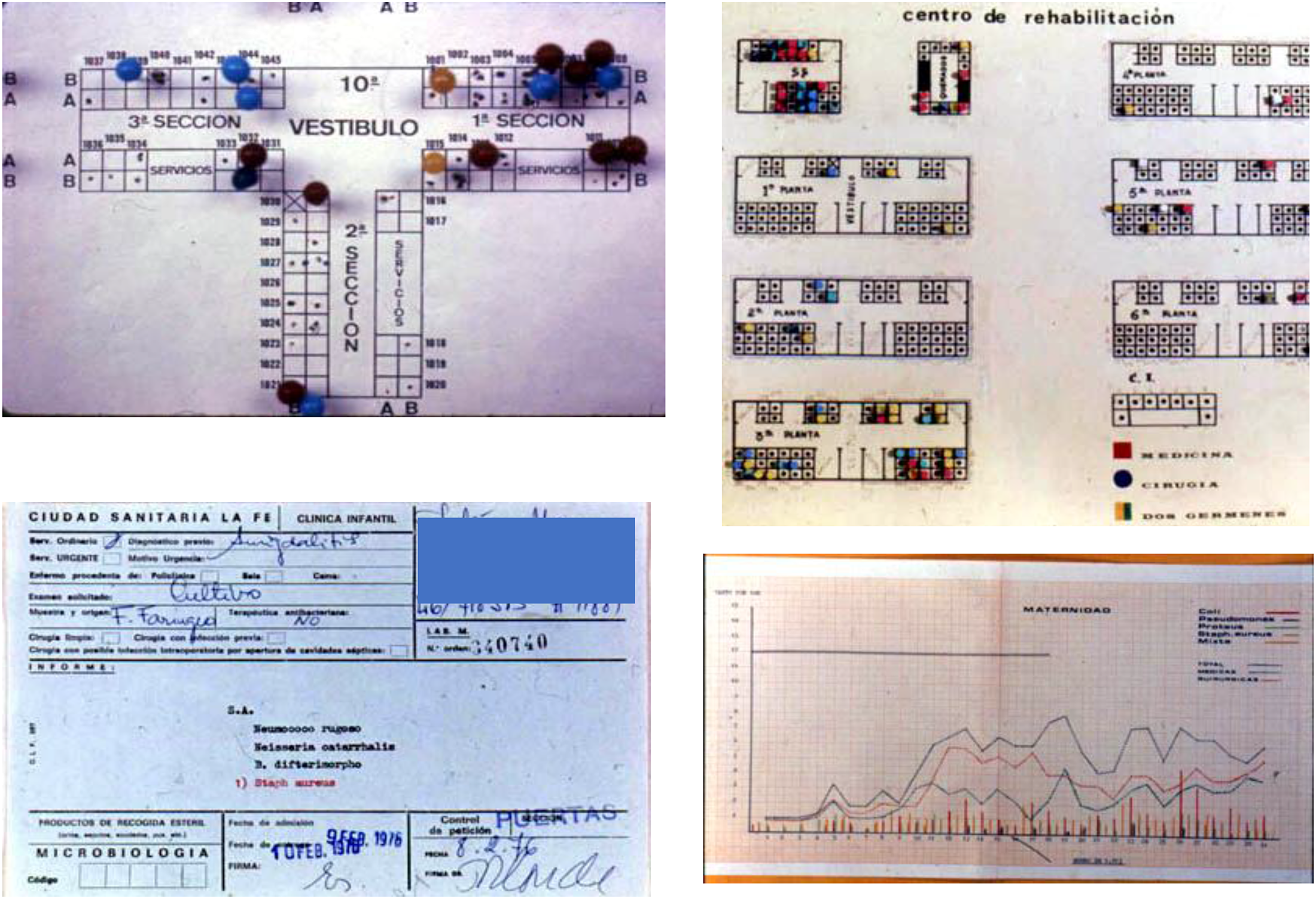
A sample of the materials used in the microbiology lab at Hospital La Fe in Valencia during the 1970s, including two schematic diagrams of the hospital's rooms with colored pins designating infection cases (top left and right), an epidemiological case form (informe) (bottom left) and a graph describing the distribution of infection cases for different pathogens (bottom right). Images reproduced with permission from María Santos and Miguel Gobernado.
The practice of mapping the hospital traveled from the Clínica into La Fe, taking a life of its own in the new setting. Similarly, in the hands of Evelio Perea, these ideas and practices also traveled to Hospital Virgen de la Macarena in Seville. Many of the structures that Moreno López and his trainees trialed in these hospitals in northeastern Madrid, and then Valencia or Seville, have had long-lasting effects on Spanish hospital medicine. For instance, the Comité de Infecciones (infections committee) originated in the context of the Clínica's microbiology lab is a structure de rigueur in any given public hospital in Spain to this day. The Políticas de antibióticos (antibiotic policies), also originated in this context, remained in use in many hospitals across Spain as antibiotic management strategies until the late 2000s and early 2010s, at which time these interventions began to be known as Programas de Optimización del Uso de Antimicrobianos (PROAs, Programs for the Optimization of Antimicrobial Use). During the 1970s and 1980s, papers and pins began to give way to computer-based modes of epidemiological mapping in the hospital (Baquero, Brugués and Jaso 1970; Perea Pérez 1971; Herreros de Tejada 1978; Delgado Gutiérrez 1987; Pérez Gorricho 1985).
Embedded in these paper technologies, in these maps, their pins, forms and graphs, a material vision of the hospital as an institution cognizant of its own infections was set up to endure for years to come. During the 1990s, epidemiological data on the most prevalent mechanisms of antimicrobial resistance (AMR) in clinical pathogens became of strategic interest for public health surveillance, for health professionals and national and regional institutions alike. Testament to this is the establishment of the Estudio EPINE in 1990 to monitor the prevalence of hospital-acquired infections among a number of volunteer public hospitals (still active today), and the Red Española para la Vigilancia y el Estudio de la Resistencia a Antibióticos (REVERA) in 1996, which collects data across public hospitals, in turn informing the European Antimicrobial Resistance Surveillance System (EARSS, EARS-Net since 2010). The epidemiological reasoning inherent in the early practice of mapping the Spanish hospital has remained a crucial feature of AMR surveillance and antimicrobial governance interventions to this day.
Conclusion
In this article, I have presented the case of the microbiology laboratory at the Clínica Puerta de Hierro in Madrid, and problematized how epidemiological tools and ideas—particularly embodied in the mapa epidemiológico—assisted a group of clinical microbiologists in making their own claims to authority in the context of the hospital. Building on scholarship on the history of hospital infections and the field of epidemiology, and an analytical approach that leans on historiographical studies of documentary practices in medicine and science, this article frames the epidemiological map as a generative paper technology to problematize the persuasive and generative power of epidemiological media. Crucial to my analysis is an appreciation of epidemiological tools, such as the map presented here, not as a lifeless document, but as an object designed to be tinkered with and grasped with hands, pierced with colored pins over and over again, and in combination with a constellation of other paper-based and documentary practices (e.g., graphs, forms). It is in the tinkering with this paper hanging on the wall of the microbiology lab, through its circulation across scientific events and publications as a figure, and its eventual replication in other Spanish hospitals, that the epidemiological map embodied its generative power. If we take seriously recent problematizations of how paper technologies in science and medicine are entangled in dynamics of gendering knowledge and expert authority (Bittel, Leong and Von Oertzen 2019), future research will necessitate an additional analysis of the gendered dynamics of laboratory structures and medical specialties.
In this article, I have demonstrated that the epidemiological map served as an authoritative instrument in the emergence of clinical microbiology in Spanish hospital medicine during the 1960s and 1970s. Epidemiology provided these clinical microbiologists with the epistemic, practical, and procedural means necessary to build legitimacy within the Clínica as well as with their professional colleagues in Spanish medicine. Leaning on the authority of the epidemiological map, Manuel Moreno López and his trainees turned the microbiology lab into an obligatory point of passage for antibiotic management at the Clínica, in turn assisting the Clínica to become a model of microbiological modernity in the nascent hospital medicine of Francoist Spain at the turn of the 1970s. These epidemiological artifacts and practices arguably elevated the role of the clinical microbiologist at a crucial time. During the early 1970s, the curricula of medical specialty training and specialists’ competencies were debated and negotiated between representatives of healthcare professions and state authorities, culminating in the publication of the 1978 Medical Specialties Act (Ley de Especialidades Médicas, Boletín Oficial del Estado 1978). Further research on the social history of medical specialization in Spain since the 1970s would elucidate how healthcare professionals other than microbiologists (e.g., pharmacists, clinicians, nurses) may have evoked the hospital space as an infectious environment too or legitimated their role in antibiotic governance and infection control in ways that epidemiological reasonings and tools may obscure.
The epidemiological map is illustrative of the significance of material spatiality to the epidemiological management of infectious diseases. The case speaks to historical and contemporary analyses of epidemiological mapping practices and problematizations of its role in creating and performing sociality and enabling or constraining intervention, examined in the case of tobacco control and smoking policies in postcolonial Africa during the 1970s (Reubi 2020) or the Gates-funded HIV initiative Avahan in India during the early 2000s and 2010s (Lorway and Khan 2014). Mapping practices and epidemiological categories play critical roles in mobilizing specific visions of social life, populations, communities and identities, mediating social connections, and generating relations of responsibility, zones of affinity or exclusion, and forms of belonging (Lorway and Khan 2014). Through these maps and categories, epidemiologists tell stories loaded with normative visions of the social that shape health policies and programs. The epidemiological map indeed acted as a generative epidemiological machine, also capable of intervening in the very phenomena that it was responding to, and mobilizing visions of the hospital, patients, professionals, and microbes that shaped antibiotic management policies. The map, the pins, and a constellation of practices and processes literally translated the hospital space into an infectious landscape or environment. The practice of mapping the hospital embodied a vision of the modern hospital as one that was not void of infections, but that could nonetheless be cognizant of its microbes. Enquiring further into the role of spatiality in infection control and antibiotic governance in the hospital also speaks directly to problematizations of AMR and resistant infections in relation to the built environment, and contemporary “aerographic” social practices created to navigate hospital design to avoid cross-infection (Brown et al. 2020; 2021). The pins and paper blueprints on the wall of the microbiology lab at the Clínica, the practice of mapping the hospital, and such a vision of the hospital as an infectious environment (ready for practices of governance and optimization) remains a principle for present-day antibiotic governance and infection control in Spanish hospital medicine.
Footnotes
Acknowledgements
I am grateful to Evelio Perea, María Santos, and Elena Gobernado for their generous engagement with this research and for providing stories and materials that have enriched this account enormously. I am also grateful for invaluable documentation support from Teresa Carretero (Biblioteca Nacional de Ciencias de la Salud, Instituto de Salud Carlos III, Madrid), Ana Abad (Fundació Bosch Aymerich, Barcelona), and Montse Viu (Col·legi d’Arquitectes de Catalunya, Barcelona). I’d also like to thank participants in the “Learning from pandemics before COVID-19” workshop at the Residencia de Estudiantes (CSIC, Madrid, November 2022) for helpful preliminary feedback on this draft, as well as Carolina Mayes, Lukas Engelmann, Miguel García-Sancho, and Ian Harper for careful direction and encouragement in carrying out and writing this research. The study that informs this research received ethics approval by the ethics board of the School of Social and Political Science at the University of Edinburgh.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research for this article has received funding from the European Research Council (ERC) under the European Union's Horizon 2020 Research and Innovation Programme (Grant Agreement No. 947872). This research was also supported by the Royal Society of Edinburgh (RSE) Research Award (Saltire Fellowship, 2022, no. 1921), and the School of Social and Political Science's Alice Brown PhD scholarship (2019-25), University of Edinburgh.
Declaration of Conflicting Interests
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.