
Abstract
This article draws insights from a case study examining unanswered health questions of residents in two polluted towns in an industrial region in southern France. A participatory health study, as conducted by the author, is presented as a way to address undone science by providing the residents with relevant data supporting their illness claims. Local residents were included in the health survey process, from the formulation of the questions to the final data analysis. Through this strongly participatory science (SPS) process, the townspeople offered many creative ideas in the final report for how the data could be used to assist in improving their health and environment and policy work is already in evidence, resulting from the study. Drawing from the literature on participatory science and expertise as well as from the initial outcomes of the local health study, I propose that SPS produces a form of knowledge justice. Understanding knowledge and its making as part of a social justice agenda aligns well with environmental justice frames. Through SPS, local residents have a hermeneutical resource to make sense of their embodied lives and augment their claims with strong data supporting actions for improving their health and environment.
The role of science in contested environments has been highlighted over the last several decades, providing a powerful lens for making visible “knowledge inequities” in vulnerable communities. These struggles have been well documented in the Environmental Justice (EJ) movement in the form of case studies that have looked at specific instances where residents have formed alliances, especially with scientists and experts, and spoken out against their exposure to toxins such as industrial and agricultural chemicals (Allen 2003; Liévanos, London, and Sze 2011; Ottinger 2013; McCormick 2009; Harrison 2011; Brown and Mikkelsen 1990). In a number of cases, such as the Etang de Berre industrial region in France, a key component in the controversy was the debate over scientific knowledge, specifically the lack of credible health science used for guiding policy.
Local residents can have concerns about regulatory reliance on corporate science or the lack of citizen-relevant science in government decision-making. Often science or the content of science—the questions asked, the methods used, and the answers it does or does not provide—is a “weak link” in environmental injustice claims. In the Etang de Berre, for example, though there have been numerous state-sponsored health studies, none support the residents’ claims of excessive illnesses. Instead, the studies tend to show that there are few, if any, elevated illnesses and that more studies should be done (Allen, Ferrier, and Cohen 2017). In frustration, the residents collected over 4,000 signatures requesting health data and, in 2007, several dozen participated in a protest, occupying the terraces of the regional health service in Marseille demanding, unsuccessfully, to know their health status. 1
Activists and academics have proposed lay participation as a possible remedy for the dearth of clear guidance from data and from science. Lay participation could mean anything from asking people what their questions are (to form the basis of scientific research) to including them in the collection and analysis of data. This article proposes that a strongly participatory process for making science in environmental controversies can lead to greater knowledge justice (Egert and Allen 2017) and potentially provide resources for environmentally polluted communities to have a voice in policy-making and other allied positive changes. Such a strategy would provide an alternative to the current knowledge aporia that many EJ struggles fall into, often ceding authority to experts or political elite-driven science that does not serve the public’s interest, as they define it, or answer the public’s questions.
In the current activist environmental knowledge economy, calls for greater local stakeholder inclusion in knowledge making coincide with a turn toward “citizen science”: lay participation in scientific endeavors, popular epidemiology, and other kinds of democratic embodiments of science. Through such engagement, local residents push for their experiences and embodied knowledge to influence government decision-making (Corburn 2005; Fischer 2000). Sometimes residents can look to counter-experts who they perceive as representing an alternative scientific viewpoint more closely aligned with their own experiences and not in service to industrial interests (Allen 2003; Frickel and Moore 2006; Hess 2016). There are other examples whereby lay citizens become experts themselves, familiarizing themselves with the language and protocols of science (Epstein 1996) or the tools of technology for data collection (Ottinger 2013). Popular epidemiology, community-based participatory research, and other forms of including residents in the actual framing of questions and hypotheses are ways to include the public in making knowledge to inform decisions (Allen 2003; Brown 2007; Corburn 2005; Minkler and Wallerstein 2008).
I begin by discussing current literature on participatory science with a focus on processes that include laypeople. Next, I present an argument for producing stronger knowledge through more strongly participatory science (SPS), which is illustrated by a case study in an industrial region of France. While the area had been the subject of numerous health studies, none provided evidence of the illnesses that the residents, including local doctors, believed were elevated. With my research team, and in concert with the townspeople, we designed and executed a health survey revealing many of the elevated illnesses observed by the inhabitants. The study’s results included a list of ideas developed by the residents for improving environmental health outcomes. This new study is already doing “work” for the town by challenging repermitting applications and arguing for expanded health clinics, among other actions. In conclusion, I present an argument for knowledge justice, meaning both an inclusive approach to making science, such as SPS, and the increased potential for policy uptake of resident-relevant scientific knowledge, necessary for socially just outcomes in science-based controversies.
Making Science with Citizens
Interest in participatory science has increased among government agencies, nongovernmental organizations, environmental groups, and the public. This term functions as an umbrella concept for a wide range of activities and modes of engagement, including “citizen science” (Irwin 1995, 2015), “street science” (Corburn 2005), “popular epidemiology” (Brown 2007; Allen 2003), “consensus conferences”(Guston 1999), “citizen juries,” and “crowdsourcing” (Haklay 2013), to name a few. These cover an array of different practices and understandings about what laypeople’s contribution to science is or could be, ranging from citizens functioning as a collection apparatus for carefully circumscribed projects, to the collaborative shaping of research questions and methods.
For building a frame for knowledge justice, a mechanism for a fully participative citizen/resident/stakeholder is helpful. To simply advance an ongoing science project is one thing—but “generating whole new knowledge structures and cognitive frameworks is quite another” (Irwin 2005, 3). Relevant and meaningful civic participation in science making requires more than the public lending approval to an already decided project or choosing between several preselected options. Thus, a strongly participative science that supports a more socially just shaping of knowledge must address three questions: (1) Is it deeply participatory at all levels—from the formation of questions to the final analyses of data? (2) Is the kind of knowledge that is produced reflective of this inclusion and relevant to the lives it impacts and represents? (3) How is participation enabled or enacted?
Dividing citizen science into a four-level classification scheme, Irwin (2015, citing Haklay 2013) has linked participation to depth of engagement in making scientific knowledge. Level 1 citizen science covers crowdsourcing and similar activities that engage citizens in gathering specific kinds of information, such as wildlife counting and other kinds of empirical data gathering for expert-devised projects. “Distributed intelligence” defines level 2 citizen science, where laypeople are interpreting scientific issues prepackaged by experts, such as citizen juries and consensus conferences. The third level of citizen science is termed “participatory science,” defined as lay inclusion in both problem definition and data collection, such as resident-initiated water and air sampling. The final level of citizen science, referred to as “extreme” participation, is defined as collaborative science, whereby lay stakeholders, such as residents, are included in the process from problem definition to data analysis. I call this “strongly participatory” science following Harding’s concept of “strong objectivity” (Harding 1991, 2015). 2
So how is the knowledge produced by SPS different? First, laypeople, particularly those affected by the negative “externalities” of technologies, can suggest new hypotheses and methodological ideas for scientific investigations. Prominent examples of lay expertise abound in the Science and Technology Studies literature, such as Wynne’s (1996) Cumbrian sheep farmers and the lack of local input before devising a herd contamination experiment or Epstein’s (1996) work on AIDS activists and their resistance to “clean test subjects” and the use of placebos. What “demarcates [strong] citizen science activities (of whatever sort) from more conventional science is that they build not only on the active participation of citizens but, also, and explicitly, on their expertise” (Irwin 2015, 35, italics in original). In concert with this must come a realization on the part of science, allied agencies, and institutions, of their own cultural limits; they need to be structurally and cognitively open to new forms of knowledge and participation (Leach, Scoones, and Wynne 2005). SPS illuminates the limitations of traditional science meant to “serve” the public and promisingly points the way forward for more relevant research and, hopefully, better citizen-inflected policy outcomes.
In SPS, laypeople and others with local or contextual knowledge are able to be fully included as having a relevant expertise. In communities facing toxic exposures, for example, it is helpful to translate SPS into policy-relevant science in order to inform future decision-making and correct past failures. However, the translation of collaboratively derived science back into “disciplinary science speak” runs the risk of reintroducing decontextualized data. For this reason, SPS demands that the final stage—data analyses—or other forms of making meaning from empirical information be done with the laypersons who were invested in the project.
Research Methods
The participatory study was conceived following an earlier project funded by the National Science Foundation (NSF) to understand how policy-relevant science was made in chemical regions in several countries. For the French case study, which would develop into the health study for this article, I conducted more than forty-five semi-structured interviews, assisted by a translator.
I interviewed health and environmental agency officials, environmental leaders, journalists, local medical professionals, city risk managers, current and retired industrial workers, and town residents. The interviews focused on how policy-relevant science was made in the region, including questions regarding resident participation and/or exclusion in these processes. Written consent was obtained from interviewees who are identified by name. The interview was recorded, transcribed, and then translated into English.
I described community-based participatory environmental health (CBPEH) research to many local informants, explaining that it had been used successfully in the United States to obtain relevant and rigorous health outcomes data in polluted regions (Balazs and Morello-Frosch 2013; Cohen et al. 2012). Local doctors and residents who are active in local environmental organizations expressed interest, but past state-sponsored studies showing no health problems made them reluctant to lend their group’s name to the CBPEH idea. However, all agreed to participate as individuals and offered us space for resident meetings, should we move forward. I successfully applied to a new French health agency for environmental and occupational health, the Agence Nationale de Sécurité Sanitaire de l’alimentation, de l’environnement et du travail (ANSES), for funds to conduct a health survey. The study was called Fos EPSEAL which stood for Etude participative en santé environnement ancrée localement sur le front industriel de Fos-sur-Mer et Port-Saint-Louis-du-Rhône (trans. Locally based participatory environmental health study in the fence-line towns of Fos-sur-Mer and Port-Saint-Louis-du-Rhône.) I hired my translator, Yolaine Ferrier, from the previous NSF-funded project as the project manager and main point of contact for the residents. An anthropology PhD student and native of the industrial region, she had grown up seeing the stacks of the Shell Chemical plant from her home.
For the ANSES-funded project, my team and I interviewed more resident informants until we were sure that we had compiled a complete list of health and related concerns. We designed the health survey tool to address questions that mattered to the public. Over a six-month period in 2015, we went door-to-door, “randomly sampling a cross-section of residents to systematically document health issues in Fos-sur-Mer and Port-Saint-Louis-du-Rhône, two towns in the industrial port area of Marseille, France” (Cohen et al. 2017, 1). We collected voluntary, anonymous information about the health of the residents and other members of their households. If no one was at home, we left a flyer so they could participate online or call us to complete it by phone. We surveyed 816 households representing 2,055 people (8.3 percent of the population), including many children. This represents a 22 percent response rate for all doors knocked on (including those not home or not answering the door) or a 45 percent response rate for those who answered their door and agreed to take the survey. 3 For illnesses (e.g., asthma, cancers, diabetes), we phrased the survey question, “Have you ever been diagnosed by a doctor with _____?” We also asked additional questions about chronic conditions that residents had expressed concern about (i.e., skin conditions, eye irritation, nose and throat irritation, etc.). The data were entered through the survey provider, Qualtrics. Toward the conclusion of the project, community members were invited to participate in small focus groups of five to ten people to assist in analyzing and contextualizing the data. The Virginia Tech Institutional Review Board approved the research protocols.
Etang de Berre: A Case Study in Controversy and Change
The heavily industrialized region of the Etang de Berre in southern France is home to hundreds of chemical, gas, and steel installations, including almost fifty Seveso high-hazard threshold facilities. 4 The area also has about 400,000 inhabitants in thirty-one municipalities. Many environmental problems and accompanying debates have occurred in recent decades, much of the conflict focused on the siting of new facilities as well as the effects of pollution and other industrial externalities on humans and their immediate surroundings. Tensions have been particularly visible in the two towns closest to concentrated industrial facilities: Fos-sur-Mer (Fos) and Port-Saint-Louis-du-Rhône (PSL).
In 1965, in an effort to further develop the region, the area and towns along the water extending from Marseille to the Camargue were declared part of an autonomous district, the Grand Port Maritime de Marseille (GPMM), which was administered by the state in consultation with industry (Garnier 2001). Decisions could be made about expansion and siting within this district, autonomously, without substantive input from the local residents or their elected officials. According to Philippe Chamaret, director of the Institut Ecocitoyen, a local environmental research organization, the local population has not had a voice in siting and permitting decisions for the last fifty years because of GPMM’s special status. He explained that, in the beginning it was not much of an issue as “people came to Fos for jobs, but the oil crisis of the 70s happened” and the area experienced an economic slowdown. 5 Plant automation and more reliance on contract labor furthered economic insecurity in the region. Additionally, after the downturn of the 1970s, some residents felt that economic diversification and alternative development were hampered by the region’s petrochemical status. According to Daniel Moutet, a longshoreman and local environmental leader, several automobile manufacturing opportunities in the 1980s were turned away as the port authorities did not think these kinds of facilities would align well with the petrochemical-based companies currently there. 6
From Siting Controversies to Unanswered Health Questions
The controversies that awoke environmental concerns of the townspeople were the siting of a large Gaz de France liquid natural gas terminal on the Fos public beach (opened 2005) and the construction of an incinerator in Fos designed to burn all the garbage of Marseille, one of the largest cities in France (opened 2010). These were hugely unpopular projects for the residents of Fos and nearby towns and served to catalyze community members to form environmental groups, even though their protests were not able to halt either project. Notably, the main environmental groups in Fos, Association de Défense et de Protection du Littoral du Golfe de Fos, headed by Daniel Moutet, and the Collectif Citoyen Santé Environnement (CCSE), headed by Gérard Casanova in PSL, were formed as a direct response to these two siting decisions by the autonomous port authority (GPMM) who held complete authority over industrial development in the region.
The siting controversies prompted residents to ask what the combination of emissions from all the polluting facilities was doing to their health? The answers they received were both confusing and troubling. According to Fos journalist Véronique Gravier, “the people wondered about health issues and made requests to government agencies—they were told there is no data available.”
7
Daniel Moutet furthered this concern: It seems like our community has more cancer cases than the national average. The prefect for the region is not allowing any data about cancer to be given to the public. They are hiding data. It is a matter of reassuring the public so there is no panic—that is why data is not revealed.
8
On arrival here, it was impossible to miss the difference [in the prevalence of serious illness]. We were both surprised and angry…. My wife treats many children and the number of sick children was too high. We were not prepared for that!
9
The Disconnect between State Health Studies and Local Residents
Resident frustration was also fueled, in part, by the many professionally driven health studies of the area that have been conducted over the past two decades. In comparison to many polluted communities in the United States, where residents often struggle to get a single health study conducted, this region has been host to more than a dozen studies that illustrate some of the continued challenges of using scientific research to answer laypeople’s questions (Allen, Ferrier, and Cohen 2017). While a full accounting of all the studies is outside the scope of this article, a brief summary of two characteristic studies would help to explain the locals’ frustration with experts.
One of the largest and most comprehensive studies done of the region assessed the risk to residents of living with the cumulative exposure to the cocktail of thirty plus chemicals in the air, water, and soil. The study, the Evaluation des Risques Sanitaires dans la Zone industrielle de Fos-sur-Mer dans les Bouches-du-Rhône (ERS-Z), was a risk modeling study conducted by an alliance of government agencies. The final report was hundreds of pages long, filled with technical discussions of “safe chemical thresholds” and a colored map highlighting “quotients of danger” in the region. The report was unhelpful to residents looking for useful information regarding their questions on illness and pollution. The conclusion of the ERS-Z study was that while there were some small areas of concern, overall there was no significant risk for those living in the industrial region.
Jacques Carle, a resident of PSL and member of the local environmental group CCSE, expressed concern with technical risk studies such as ERS-Z: Some health studies have been done but in a very strange manner. We have been told, after the results are consolidated, that, ‘you are OK.’ These studies are only to tell people there is no risk.
10
Due to both budgetary and methodological decisions made by the scientific team, the study used secondary data. Specifically, they used hospital admissions as a way to ascertain rates of asthma, cancer, and cardiac disease, which meant that only the most extreme cases of asthma, and not the total burden of disease, would be captured. The scientists admitted as much explaining that the “lack of significant results for respiratory diseases most probably shows that hospitalization indicators are not the best indicators to evaluate the respiratory health effects of air pollution in adults…” (Pascal et al. 2013, 8). Their study also found no excess risk for cancer due to living in polluted industrial regions, except for acute leukemia in men. However, the study did show a relationship between heart disease and SO2 air pollution. The authors recommended further education of doctors and more surveillance of current and retired workers, but the study concluded that “the health situation of the population exposed to industrial air pollution is generally not a concern for respiratory diseases and cancers” (Pascal et al. 2011, 45).
Many residents were critical of this study and its findings. “It seems impossible not to have been able to establish a link between air pollution and respiratory illness in the Hospitalizations study,” says local activist, Gérard Casanova. He continues: In France, what has not been proven does not exist. As long as there are no studies and we do not know, there is no problem. As long as people do not want us to make this link here, there will not be any targeted studies.
11
Making an SPS Study
In response to the residents’ strong desire for credible health data, in 2014, I applied for, and received, funding from the ANSES to conduct a CBPEH survey in the two heavily polluted industrial towns: Fos and PSL. From an EJ perspective, the two towns have no voice in siting decisions because they are part of the GPMM industrial zone. Both are primarily working class, though, and in PSL, 20 percent of the residents live in poverty and 44 percent live in public housing. Compared with the surrounding region, in both towns, a larger percentage of the population has vocational degrees, and a considerably lower percentage has college degrees (see Table 1). It is unconstitutional to collect statistics on race or religion in France, so only data on first-generation immigrants exist and these data show both towns to have a lower immigrant population than the region as a whole.
Socioeconomic Characteristics of the Towns of Fos-sur-Mer and Port-Saint-Louis-du-Rhône Compared with the Bouches-du-Rhône Region. 18
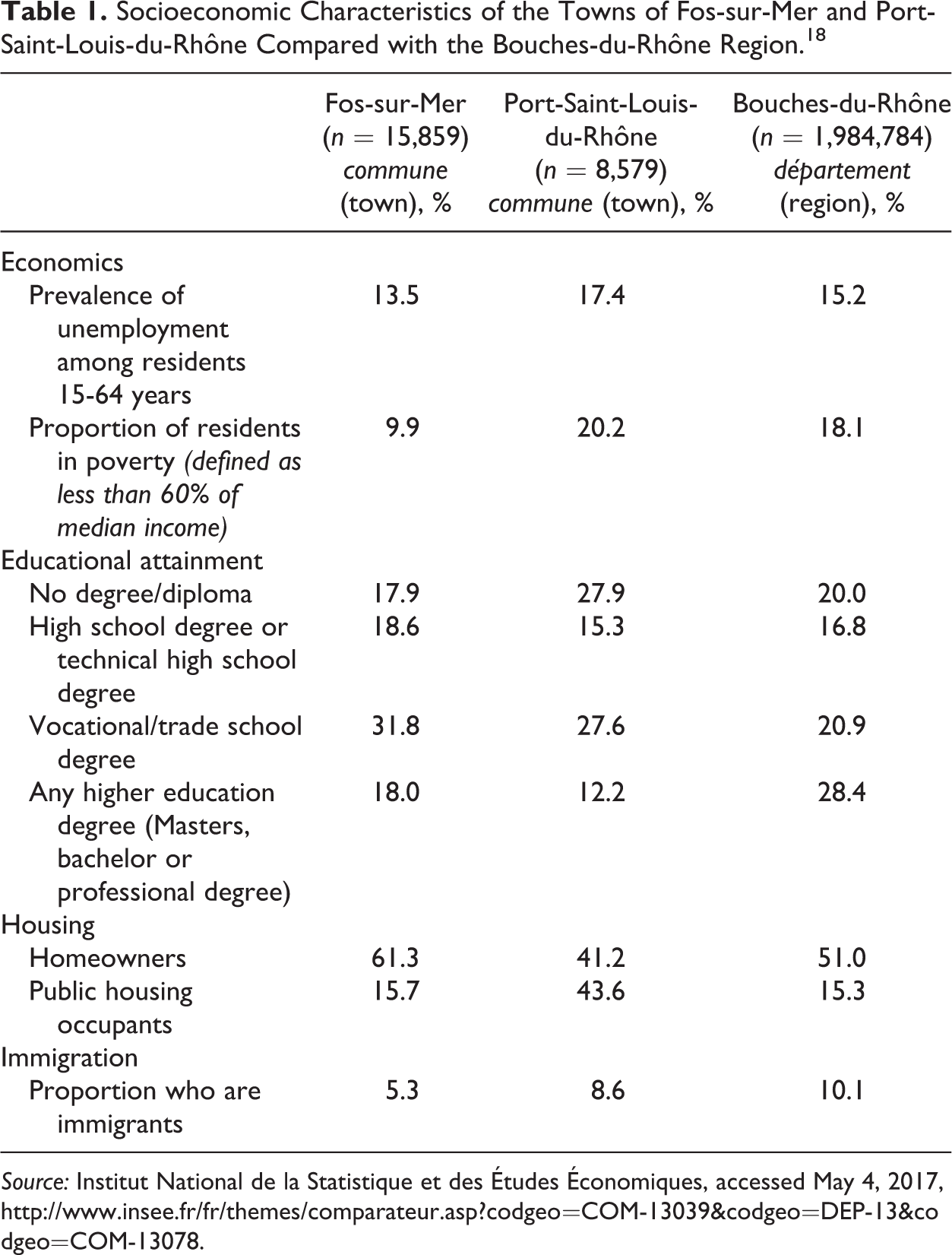
Source: Institut National de la Statistique et des Études Économiques, accessed May 4, 2017, http://www.insee.fr/fr/themes/comparateur.asp?codgeo=COM-13039&codgeo=DEP-13&codgeo=COM-13078.
The idea for the door-to-door study was to work with local people to produce science that answered some of their questions and helped tell, with data, a health story that aligned with what they were observing in their daily lives. My project team consisted of two French social anthropologists, Yolaine Ferrier and Johanna Lees, and an American epidemiologist, Alison Cohen, with experience conducting CBPEH surveys (Allen et al. 2016). 12
The preliminary findings were notable, and we presented them in open civic meetings in the two towns in 2016 (Cohen et al. 2017). We found that, while the prevalence of cigarette smoking in the towns was similar to the region and to France, the prevalence of asthma was highly elevated in adults. (The rate of cumulative adult asthma in France is 10 percent, the rate is 15.8 percent in the two towns.) We also found that while the prevalence for all cancers in France was 6 percent, in these towns, the prevalence was 10.5 percent. 13 The cancer burden for women in our study was noticeably higher than for men. While the prevalence of cancer in women is 5.4 percent in France, it was 14.5 percent for the women in our study. This was eye-opening, in part, because we likely underrepresented the prevalence of cancer because some cancers (e.g., lung, pancreatic) act rapidly and thus were likely not well represented in our sampling technique. In contrast to our findings, the Hospitalizations study had reported to the residents that there was no evidence of elevated cancer or asthma in the region (except for acute leukemia in men). Endocrine disease was also elevated as was type 1 diabetes, an environmentally triggered autoimmune disease. We also found that many women had sought advice about, and medical treatment for, fertility, though it has been more difficult to find comparative data on fertility and other birth outcome issues.
Interestingly, we found that while 63 percent of our respondents reported at least one chronic disease (in comparison to 39.6 percent of the French population), 72 percent of the respondents self-reported their health as either excellent or good. This “normalization” of chronic illness in these communities reinforces the residents’ attempts to manage their condition with medical treatment or otherwise learn to live with their conditions. “I am artificially healthy,” declared one resident, as she described taking numerous medications to remediate her chronic conditions.
After dissemination of the preliminary data at the town meetings, we ended our presentation with a request that citizens volunteer to participate in a series of focus groups to further analyze the data and suggest “next steps,” given their new health status information. Then we asked the audience whether there were any questions. In the Fos town meeting, the mayor was the first to raise his hand. He stood up, turned to face the audience, his constituents, and said, “This is the health study that we have been waiting for.” He went on to say that our study revealed the many health problems that they had long experienced and encouraged everyone to participate in the focus groups.
Over the next few months, we held over thirty small focus groups (five to ten people) with local residents and locally engaged medical professionals to suggest further analyses and to help make meaning of the survey data, giving context to the numbers. In this way, the data collected were also analyzed with the local people, using socially situated communicative methods from qualitative research, to build a relevant context for the study’s findings (Cashman et al. 2008; Basch 1987; Lunt and Livingstone 1996). The final Fos EPSEAL report was released in January 2016. 14
Emerging Forms of Knowledge Justice: A Constellation of Ideas and Practices
At the center of many local environmental struggles in polluted communities is a debate about science. A typical case is where the polluting corporations, such as steel producers, paper mills, and petrochemical plants, have scientific evidence to make their claim that the externalities from production are benign—to humans and the environment. At times, this is the same science the regulators use to permit the facilities, accepting the data of corporations without question. Alternatively, state agencies may have produced their own science that they use to make decisions about siting, permitting, and regulating noxious facilities. However, local residents can have differing observations regarding the health and environmental impact of these facilities in the communities, but, without science to back them up, they have a difficult time being heard or their observations taken seriously. This lack of relevant science, or “undone science” (Hess 2016), can underlie power differentials between citizens and corporations or government and can be due to institutional norms and disciplinary practices (Allen et al. 2016), but the result is the same—no science answering the citizens’ questions.
Providing local people living in polluted communities with science that answers their questions was the purpose of the Fos EPSEAL project. Producing relevant, rigorous science in collaboration with residents is a form of knowledge justice—science that can be used to bolster local claims especially when they are in conflict with what corporate or state agents are saying. Residents, in possession of their own science, which they participated in making, enable knowledge and thus participatory parity at the discussion or negotiation table, wherever that might occur (see Figure 1).
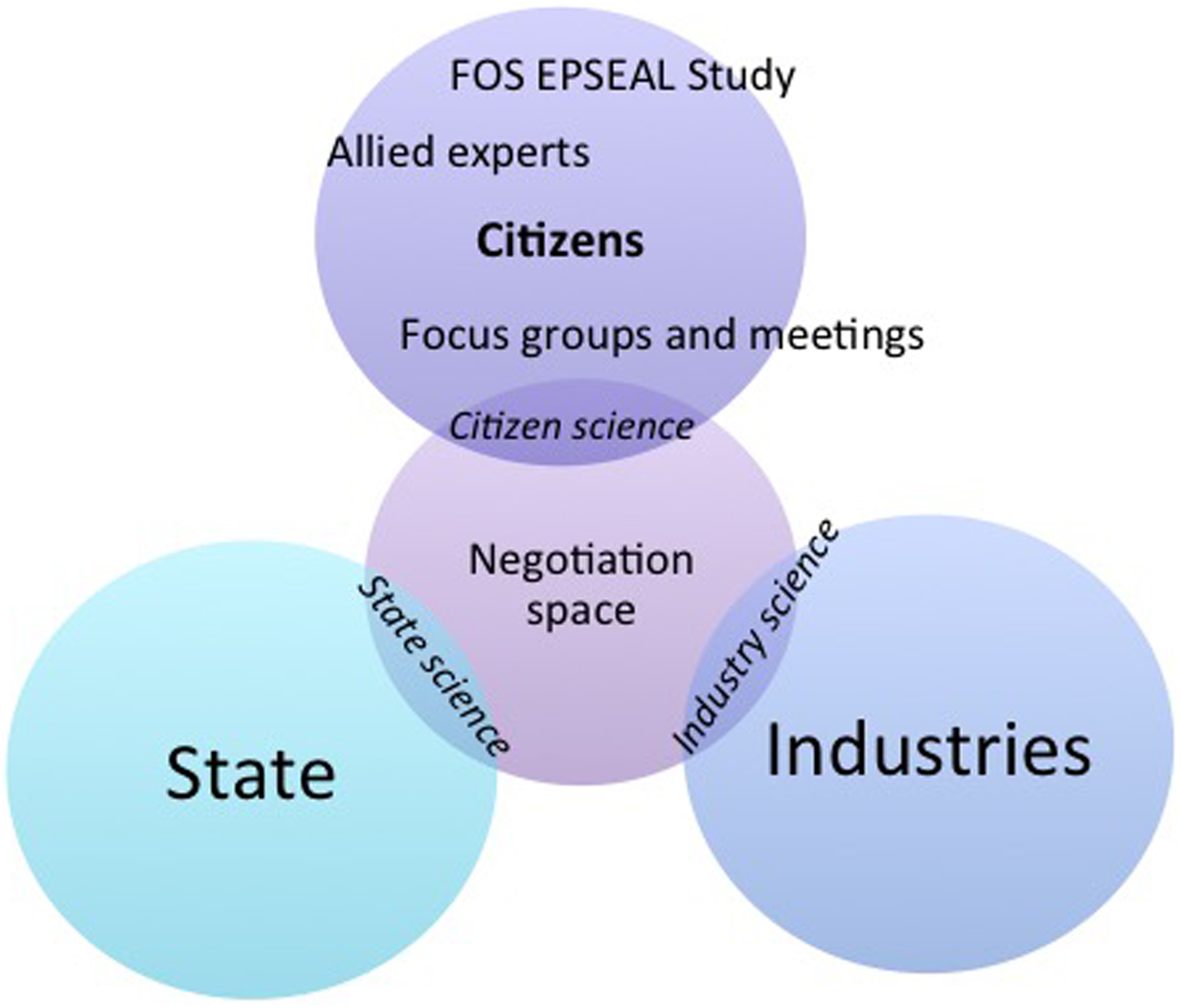
Knowledge justice is each stakeholder having relevant science for decision-making with participatory parity.
Concepts related to knowledge justice include postcolonial development scholar Shiv Visvanathan’s (2005) idea of “cognitive justice,” meaning “the constitutional right of different systems of knowledge to exist as part of the dialogue and debate” (p. 92). He further explains that for indigenous people in the Global South, “science as development, plan, experiment, and pedagogy determined the life chances of a variety of people…[thus] epistemology is politics” (Visvanathan 2005, 84). In this conception of “knowledge justice,” the power of social movements’ science (McCormick 2009) is not only a protest against a dam, engineered seeds, or a deforestation project, it is a challenge to the dominant narratives of science and the epistemologies that support them. “The idea of cognitive justice suggests that there is a link between survival and forms of knowledge,” explains Visvanathan (2005, 93).
Linking communication and social justice, the concept of testimonial injustice uncovers how those having lay knowledge or empirical evidence are precluded from full participation in fact-collecting venues by institutionalized misrecognition (or nonrecognition) of their credibility (Fricker 2007). This dysfunction in testimonial practices can work both ways: “either the prejudice results in the speaker’s receiving more credibility than she would otherwise have—a credibility excess—or it results in her receiving less credibility than she otherwise would have—credibility deficit” (Fricker 2007, 17). Social gaps in the credibility economy further expand when considering scientists and lay knowers, such as residents, in polluted communities. While environmental data and studies of corporate and/or state scientists are typically accepted by policy makers, the everyday observations and tacit knowledge of local residents about their environment are often held as suspect or simply ignored.
Another form of knowledge injustice, hermeneutical marginalization, is often hidden and can accompany testimonial injustice. The hermeneutically marginalized “participate unequally in the practices through which social meanings are generated” (Fricker 2007, 6). This can mean their social experiences are left inadequately conceptualized or ill-understood—even by themselves—such that they appear to not have an adequate grip on the content they wish to convey. They are heard as irrational or unclear—or they are not heard at all. This knowledge injustice is a social situation whereby a collective hermeneutical gap prevents them from making sense of an experience that is strongly in their interests to render intelligible (Fricker 2007, 7).
One way to consider knowledge justice in light of these epistemic issues is to think of science as an array of “logics of inquiry,” which recognizes the importance of social and political contexts in shaping research agendas and methods. “Starting off research from the questions that arise in the lives of groups that are excluded…permits us to recognize new and valuable …questions and procedures for answering them” (Harding 2015, 38)—questions that probably did not occur to the scientists from a dominant or insular research culture. The practicality and relevance of science depends not only on the context of its making but also on the context of its use: “knowing that vs. knowing how” (Harding 2015, 97). “Knowing that” is science made through professionally constrained questions and methodologies that see the production of knowledge as culturally anonymous with discreet findings shaped as much by “nature” as by the boundedness of the inquiry. Conversely, the science of “knowing how” requires a different logic and a wider contextual frame that includes knowledge about the natural world shaped by those who live its consequences. This conception of knowledge justice aligns with “epistemic modernization,” the inclusion of a broader array of voices in scientific agenda setting, research design, and practice, making science relevant and responsive to those who have been excluded from such processes (Hess 2007; Moore et al. 2011).
Discussion: Residents’ Ownership of Science Leads to Positive Outcomes
SPS as engendered by the Fos EPSEAL project demonstrated that including residents in all aspects of the research, from the questions asked to the analyses conducted, alleviates many of the unjust epistemic problems with science in polluted communities. First, their observations as residents are included as the basis of the questions asked in the health survey. Second, after the random sample is collected and the initial data are generated, we worked in focus groups with the local population, including local doctors, to interpret the data in context and produce further analyses that include their voices as “sense makers” of the numbers. Finally, the focus group participants were asked to think collectively about “next steps”—how might this new report validating their suspicions be used to better their environment. They came up with dozens of ideas including better air quality warning systems, indoor play facilities for schools, local access to medical specialists, better public transportation to discourage auto traffic, and dissemination of recommendations and “best practices” for local food consumption. Other ideas for city administrators were suggested such as ending mechanical blowing for street cleaning, reducing pesticide spraying for mosquitos, and adding charging stations to promote electric cars. They also advocated for regulators to push for cleaner industrial processes, to focus more directly on the most dangerous substances, and to consider cumulative impacts when making siting and repermitting decisions. As of the writing of this article, the mayor of one of the towns has already used the new health study to (1) insist on greater scrutiny in repermitting one nearby industrial incinerator, (2) attempt to stop the expansion of another commercial incinerator, and (3) vocally advocate for stronger air quality regulations from the state.
Soon after the health report was released, one local newspaper reported that “[a]n avalanche of articles, reports and reactions” have appeared, “since a Franco-American team of researchers published the results of its study called [Fos] EPSEAL [and these two towns have become a] symbol of an alarming health situation for those living in the vicinity of factories and also a symbol of the difficulty of the public authorities to answer the questions of the inhabitants…” 15 According to local doctor, Philippe Le Merer, “[t]his study is extremely interesting because it seems to confirm the impression we have as general practitioners in the region: many cancers in our patients, chronic diseases, asthma, and many autoimmune diseases…” 16 The local residents have also taken to the airwaves and given dozens of radio and television interviews about the health study and its findings. One local television reporter told us that she was surprised, following her interviews of people on the street in both towns, that she could not find a single person who did not know about the study. The citizens “owned” the data, understood and were comfortable talking about the science, and the findings aligned with what they knew to be true in their daily lives.
In late 2017, almost a year after the Fos EPSEAL health study was released, Radio France produced a two-part, hour-long podcast on the health issues of the Fos and PSL residents, prompted by the participatory project. At the end of the podcast, the interviewer asks a representative of the French health service why the agency neglected to respond to the residents’ questions about health or their request for data? Their verbal response was “no comment.” 17
We have since been contacted by over a dozen towns and citizen groups in France, all wanting a participatory health study. The French health service, as of the writing of this article, has said when questioned in public meetings, that they have no problem with our data and they see participatory science as a way to augment the kinds of expert studies they conduct. However, they also add that CBPEH studies are too expensive and have not yet agreed to fund them. In our next project, recently funded by the ANSES, we hope to alleviate this problem by conducting a CBPEH training workshop this summer for up to twenty French researchers and townspeople. In the future, it is our hope that strongly participatory health science can be conducted entirely by local residents, in collaboration with local scholars, thus making it more affordable.
Conclusion: Knowledge Justice in Contested Communities
The local populations’ unanswered questions regarding their health provided a useful lens to examine the concept of knowledge justice—or injustice. The residents’ dissatisfaction with the numerous environmental risk and health surveys done in their region cannot be attributed to scientific incompetence. The problem, I argue, is with the research questions asked, the insular methodology followed, and potentially a bias toward economic interests. There was a failure of governmental, institutional, and professional imagination when it came to fully including local residents in shaping the agendas and questions of science, which lead to a maldistribution of the types of science produced toward understanding the health and lived conditions of the townspeople.
How this knowledge inequity gets produced and reproduced is an important question. The exclusion of the residents most impacted by the phenomena being studied misrecognizes a population who could contribute to making rigorous, relevant science. This denial of a group’s knowledge claims, or testimonial injustice, is but one element of the knowledge injustice continuum. There is also the content of knowledge to be addressed. For example, in the ERS-Z study, the unquestioned disciplinary practice of relying on abstract chemical threshold risk data rather than on data drawn from the local residents who have actually experienced illnesses led experts to declare that living in this industrial zone was not harmful to their health. Similarly, the Hospitalizations study focused an analysis of inpatient hospital data rather than the daily respiratory conditions local residents in polluted areas actually experience. Thus, the content of strongly participatory knowledge must also engage with laypeople to alleviate hermeneutical injustice, whereby including the illness hypotheses and embodied understanding of residents within regulatory science.
Local residents can add great value to environmental health science—both in the kinds of questions and ways of knowing—that increases the understanding of population health in polluted communities. Combining disciplinary science “from above” with on-the-ground embodied knowledge creates a more strongly objective and relevant health science. When local residents participate in producing environmental health knowledge—developing questions, collecting evidence, analyzing data, and actively engaged in dissemination strategies—they are producing robust and relevant science or SPS.
In conclusion, SPS advances knowledge justice by providing a strategic framework that can address power inequities through producing relevant science in contested environments (Allen 2017). In this intersecting arena of participatory science and epistemic justice, knowledge shaping is shared among a broader constituency of who can be a knower and is representative of local as well as cosmopolitan voices. Often in environmentally polluted communities, residents’ questions regarding their health are ignored or conversely, they are overwhelmed with science that does not reflect their own observations. While their empirically based knowledge about their lived conditions is discounted, “elite” state-sponsored science or corporate environmental permitting studies are used for policy decisions that negatively impact their neighborhoods (Allen 2003; Brown 2007; Corburn 2005). A justice-oriented frame of scientific knowledge should include, as relevant participants, those most vulnerable and most affected by science and its applications. Knowledge justice through SPS is about providing residents an authoritative voice in the environmental arenas that affect them—as a matter of social equity.
Footnotes
Acknowledgments
First, I want to thank my former doctoral student, Philip Egert, who came up with the term knowledge justice further stimulating my thinking about social justice and science. Additionally, my first foray into designing and conducting a participatory health study would not have been possible without my core team of excellent interdisciplinary scholars: Alison Cohen, Yolaine Ferrier, and Johanna Lees. I am also indebted to Valeria Siniscalchi and the Centre Norbert Elias in Marseille for hosting my project and giving my team a home. Finally, I would like to thank Alice Mah for the opportunity to develop my ideas at her “Toxic Expertise” workshops at the University of Warwick in 2016 and 2017 funded by the European Research Council.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by NSF SBE award 1148586 and was graciously supported by a five-month resident fellowship at the Institut Méditerranéen de Recherches Avancées (IMéRA) in Marseille. The community-based participatory environmental health study was financed by a grant from the Agence Nationale de Sécurité Sanitaire de l’alimentation, de l’environnement et du travail (ANSES), the French agency for food, environment and occupational health & safety (award number: PNREST Anses, Cancer ITMO AVIESAN, 2014/1/023).