
Abstract
The paper presents a novel framework for the prediction of the raised Intracranial Pressure (ICP) from ocular ultrasound images of traumatic patients through automated measurement of Optic Nerve Sheath Diameter (ONSD) and Eyeball Transverse Diameter (ETD). The measurement of ONSD using an ocular ultrasound scan is non-invasive and correlates with the raised ICP. However, the existing studies suggested that the ONSD value alone is insufficient to indicate the ICP condition. Since the ONSD and ETD values may vary among patients belonging to different ethnicity/origins, there is a need for developing an independent global biomarker for predicting raised ICP condition. The proposed work develops an automated framework for the prediction of raised ICP by developing algorithms for the automated measurement of ONSD and ETD values. It is established that the ONSD and ETD ratio (OER) is a potential biomarker for ICP prediction independent of ethnicity and origin. The OER threshold value is determined by performing statistical analysis on the data of 57 trauma patients obtained from the AIIMS, New Delhi. The automated OER is computed and compared with the conventionally measured ICP by determining suitable correlation coefficients. It is found that there is a significant correlation of OER with ICP (r = .81, p ≤ .01), whereas the correlation of ONSD alone with ICP is relatively less (r = .69, p = .004). These correlation values indicate that OER is a better parameter for the prediction of ICP. Further, the threshold value of OER is found to be 0.21 for predicting raised ICP conditions in this study. Scatter plot and Heat map analysis of OER and corresponding ICP reveal that patients with OER ≥ 0.21, have ICP in the range of 17 to 35 mm Hg. In the data available for this research work, OER ranges from 0.17 to 0.35.
Keywords
Introduction
Intracranial pressure (ICP) is an assessment parameter for patients suffering from traumatic brain injury. The normal ICP range in healthy patients is 5 to 15 mm of Hg.1 -4 Regular monitoring of ICP is needed in case of accidental damage to the brain, as it causes ICP to rise; this raised ICP in the brain reduces cerebral perfusion pressure (CPP), which results in brain damage.5 -7 The measurement of intracranial pressure can be performed through invasive and non-invasive methods, but the invasive techniques are complex and harmful to patients; they include ventriculostomy and micro transducers for continuous ICP monitoring.5,8 -10 Ventriculostomy is considered a standard invasive technique for ICP monitoring. However, such a method needs regular monitoring in the presence of a neurosurgeon; if a routine procedure is not followed, it may cause complications for the patients. The non-invasive techniques are considered safe and secure compared to the invasive methods. It is well established that ICP correlates with the optic nerve sheath diameter (ONSD); therefore, accurate measurement of ONSD can be potentially used for the diagnosis of the raised ICP.11 -13 ONSD can be measured using various medical imaging modalities such as Magnetic Resonance Imaging (MRI), Computed Tomography (CT), and Ultrasonography. Ultrasonography has several advantages compared to other modalities, as it is reliable, cost-effective, and has a bedside availability.14 -19 It does not emit harmful radiation, unlike CT scan imaging, for the monitoring of ICP. The measured optic nerve sheath diameter (ONSD) using ocular ultrasound is a biomarker for predicting intracranial pressure (ICP).20,21 The optic nerve sheath diameter is measured at a distance of 3 to 8 mm below the retinal globe using a 6 to 13 MHz linear transducer probe, as shown in Figure 1.
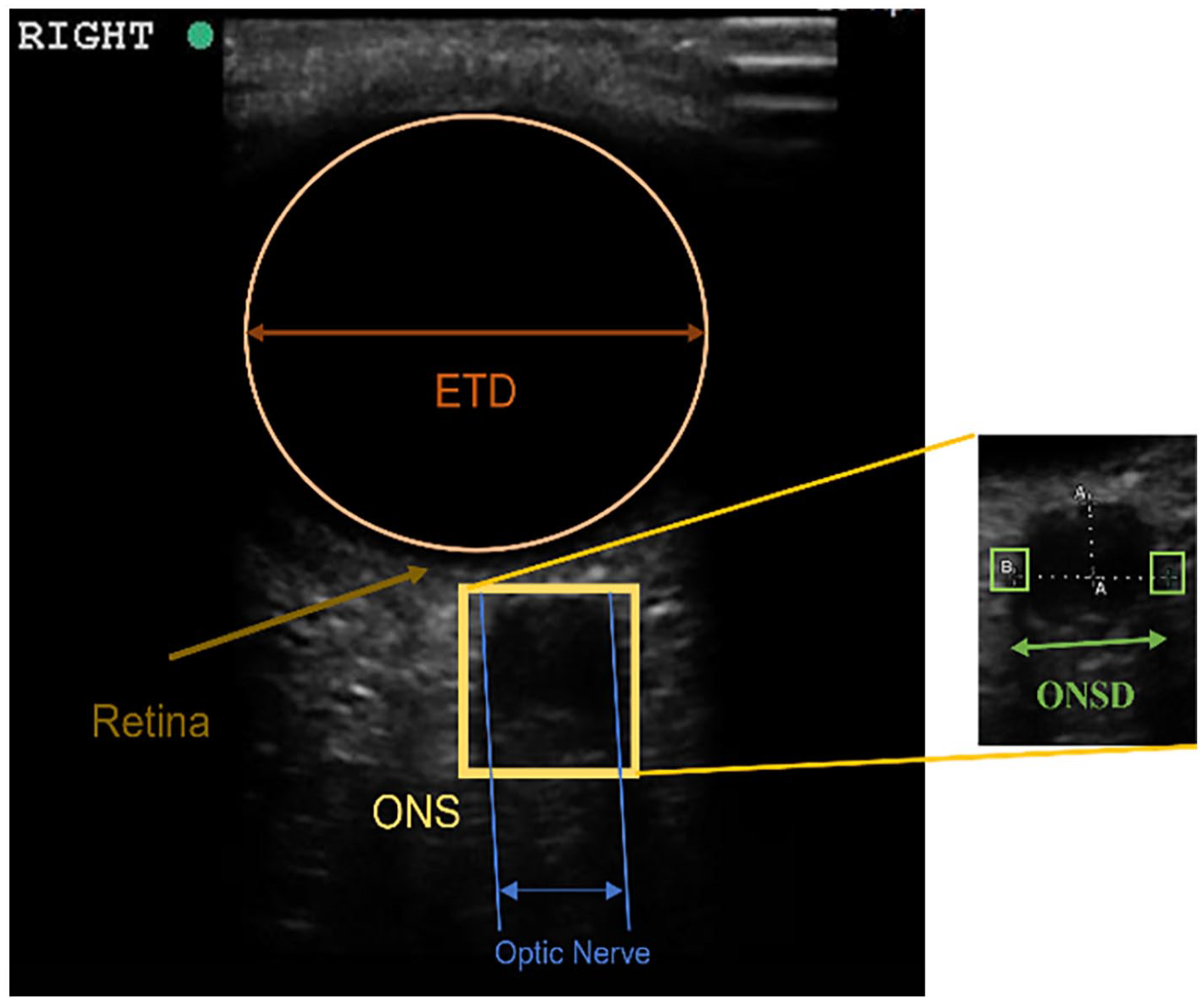
Estimated ONSD (measured by electronic caliper, 3 mm below the retinal globe) and ETD.
Some reported literature has revealed that the ONSD value ranges from 0.46 to 0.77 cm, but it varies according to the patient’s origin and ethnicity.21 -26 The major drawback in assessing intracranial pressure using the ONSD value is the absence of an accurate correlation between ONSD and ICP. Further, there is no established standard threshold value of ONSD indicative of raised ICP condition. Another diagnostic biomarker is eyeball transverse diameter (ETD), which could be a reliable indicator along with the ONSD to predict a raised ICP. The changes in the eyeball can affect the optic nerve sheath diameter (ONSD), which is the thickness of the protective covering around the optic nerve. Recently, few researchers have reported work related to the measurement of ONSD and ETD ratio (OER) for the accurate prediction of intracranial pressure. Some of the studies highlighting the findings and limitations of raised ICP prediction using ONSD measurement in trauma patients are presented in Table 1.
Studies Highlighting the Findings and Limitations of Raised ICP Prediction.
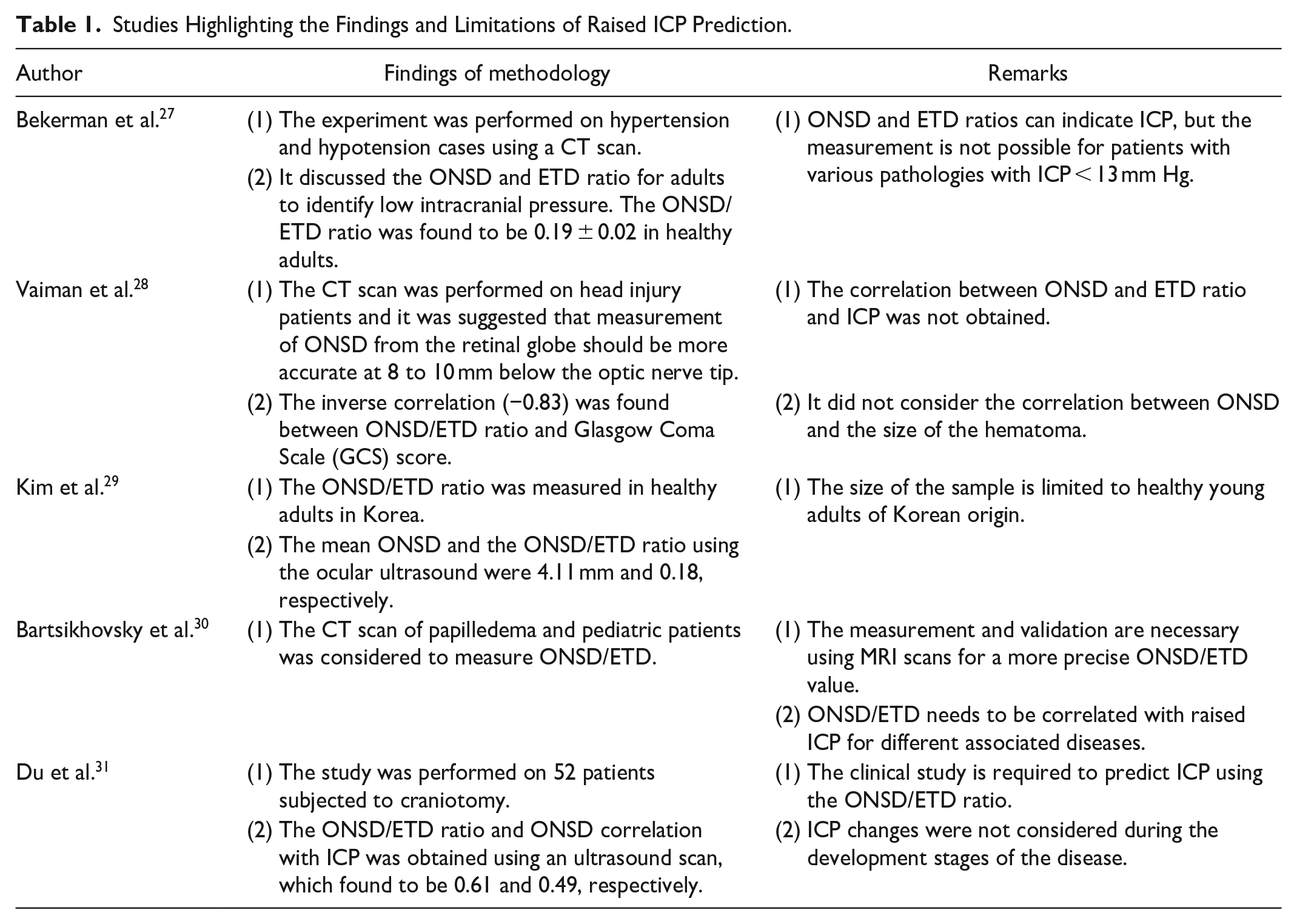
Some literatures27 -31 attempted to determine the threshold value of the OER for predicting intracranial pressure. However, there are certain limitations, which are listed as follows:
The accurate threshold value of ONSD for predicting raised ICP condition is still not very clear due to the small sample size of patients of different origins/ethnicities reported in various studies.
Validation of the ONSD and ICP relation using well-established standard methods, reported in the various studies, is not sufficient.
No automated module is available for measuring the ratio of ONSD and ETD using ocular ultrasound.
Early detection of change in intracranial pressure and its continuous monitoring is needed for traumatic patients.
This paper proposes an automated framework for predicting raised ICP conditions; this is achieved by developing image processing based algorithms for the automated measurement of ONSD and ETD using ocular ultrasound images. An attempt has been made to determine a threshold value of OER through statistical analysis of the relevant patient data obtained from AIIMS, New Delhi. The developed ICP prediction framework will be helpful in the early detection and continuous bedside monitoring of trauma patients. Further, the proposed framework will minimize the dependency on medical experts for ICP measurement; this will allow technology-driven betterment in the management of trauma conditions in remotely located and specialized manpower-constrained trauma centers. The performance and the accuracy of the proposed framework for predicting ICP conditions are validated by comparing the system-generated ICP prediction results with the actual ICP value (measured by the medical experts) available in the obtained patient data. The main contributions of the proposed work are as follows:
Algorithms are proposed for automated ONSD and ETD ratio measurements by analyzing ocular ultrasound images using image-processing techniques.
Automated measurements of the ONSD and ETD have been compared with manual measurements.
The threshold value of the OER is determined for predicting raised ICP conditions; this is achieved through statistical analysis of the available patient data.
The proposed ICP prediction framework is validated by comparing the system-generated predicted ICP results with the ICP values measured on patients of Indian origin using the conventional invasive method.
The rest of the paper is organized into four sections. Section II provides the details of the proposed algorithms for the automated measurement of ONSD and ETD using ocular ultrasound images. Section III has discussed the obtained results along with the statistical analysis for obtaining the threshold value of the ONSD and ETD ratio. The discussion and overall conclusion of the research work are presented in Sections IV and V, respectively.
Methodology
This section presents a detailed description of the proposed framework for the raised ICP prediction using an ocular ultrasound image. It involves automated algorithms for ONSD and ETD measurement, computation of threshold value of OER for predicting raised ICP condition and validation of the overall raised ICP prediction framework. Figure 2 depicts the important steps involved in the proposed raised ICP prediction framework.
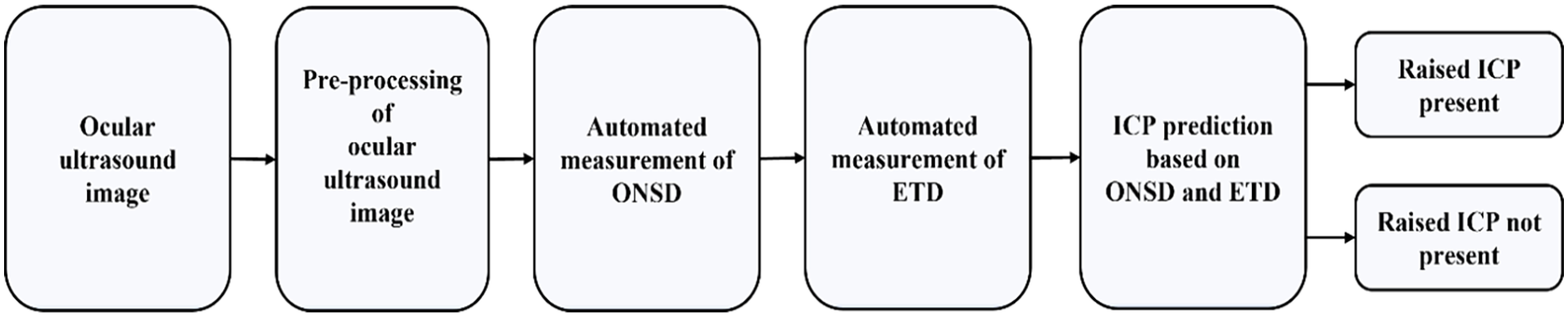
Block diagram of proposed raised ICP prediction framework.
Acquisition of Ocular Ultrasound
The ocular ultrasound image (B-scan) acquisition is an important and portable imaging option for the measurement of ONSD and ETD to assess the raised ICP. In order to protect sensitive structures such as the lens, retina, and vitreous body from potential damage caused by cavitation and thermal effects, it is necessary to adjust the system settings. These adjustments involve setting the mechanical index to 0.23 and the thermal index (TI) to 0.0. As per FDA guidelines for ophthalmic ultrasound, ensuring that the mechanical index (MI) remained below 0.23 and the thermal index (TI) stayed below 1.0. By adjusting the acoustic power while using the small parts preset, we achieved a mechanical index below 0.23. 32 The ultrasound machine (SonoSite M-Turbo) uses the linear probe (frequency of 6–13 MHz), which is held longitudinally to the retinal globe to measure the optic nerve diameter at a distance of 3 mm below the optic nerve tip. The proper contact between the linear probe and the patient’s eye is provided by applying sufficient gel. To obtain a coronal cut through the optic nerve, the ultrasound probe was positioned on the eyelids in a perpendicular orientation (90°) to the coronal plane. The subjects were asked to gaze straight with their eyes closed to align the optic nerve with the probe. The probe was then swept horizontally across the eye from side to side, allowing visualization of the optic nerve region and the surrounding sheath with prominent shape and thickness. The depth of the ultrasound is adjusted so that the image of the eye is filled on the screen. Further, with the help of an electronic caliper, the manual measurement of ONSD is performed on an ultrasound machine display. The gain is adjusted in the machine so that the optic nerve sheath and eyeball can be seen for acceptable imaging. The algorithm-generated measurement performed on the obtained ocular ultrasound data is discussed in Section 2.2.
Patients data collection
The collected data of the patients are in DICOM format, which contains the ocular ultrasound video and image files. Ocular ultrasound images of 57 patients were collected from Jai Prakash Narayan Apex Trauma Center (JPNATC), AIIMS, New Delhi, India, in which 45 patients were males and 12 were females, with ages ranging from 18 to 70 years. The study on patients’ data was done on both the left and right eyes. The obtained data includes the patient’s age, gender, the measured value of the ONSD at a distance of 3 mm from the globe and the corresponding ICP value. The patients admitted to the Trauma Center were having various pathological conditions such as subarachnoid hemorrhage (SAH), diffuse alveolar hemorrhage (DAH), intraventricular hemorrhage (IVH), fracture, epidural hematoma (EDH), diffuse axonal injury (DAI), edema, midline shift (MLS), contusion and brain tumor. A sample of acquired ocular ultrasound image from the trauma center is shown in Figure 3.

Ocular ultrasound image acquired using SonoSite M-Turbo ultrasonography machine.
Automated Measurement of ONSD and ETD Ratio
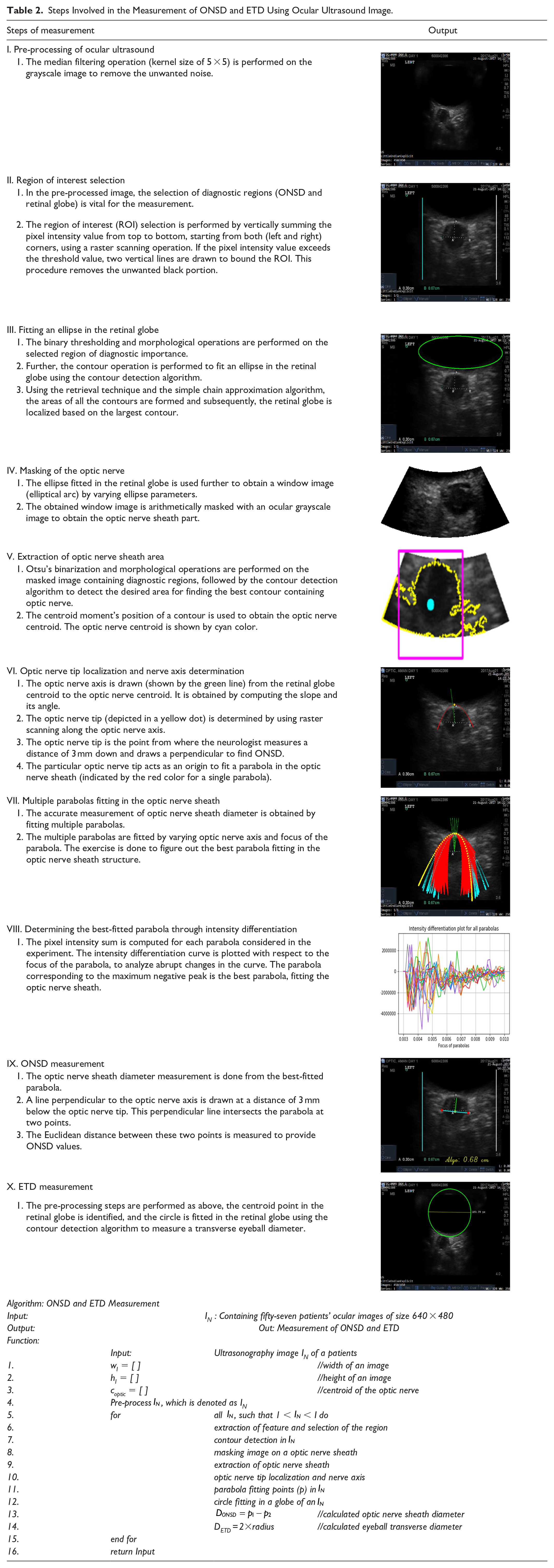
The proposed method discusses the techniques for the automated measurement of optic nerve sheath diameter and eyeball transverse diameter using B-scan ocular ultrasound. The measurement (ONSD and ETD ratio) predicts the ICP presence if the obtained OER is ≥ the OER threshold. Various image processing and computational methods have been involved in the implementation of automated measurement algorithms for the ONSD and ETD. Table 2 provides a detailed description of the involved steps along with their results.
Steps Involved in the Measurement of ONSD and ETD Using Ocular Ultrasound Image.
Results
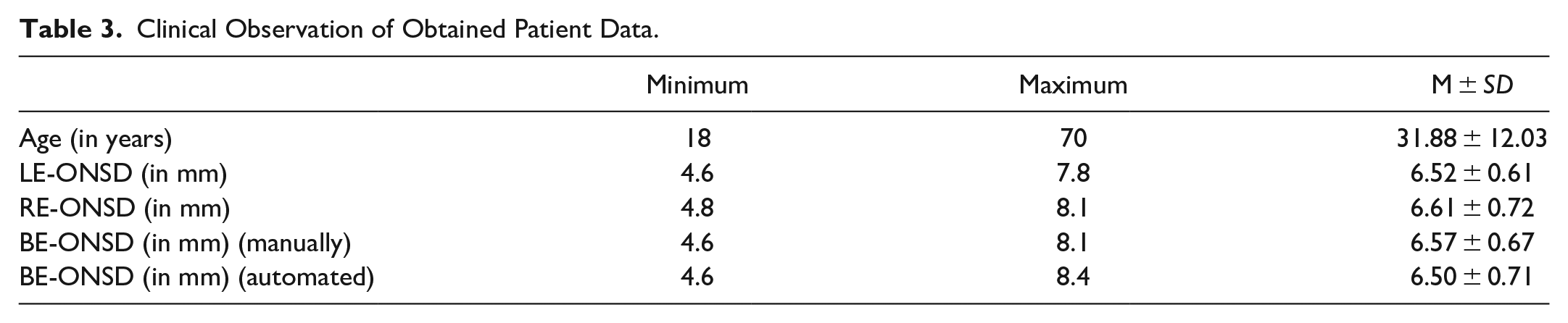
The ocular ultrasound images (both left and right eyes) of 57 trauma patients were collected from the Trauma Center, AIIMS, New Delhi, India. In obtained ocular ultrasound images of the patients, ONSD values were measured by the medical experts using the electronic caliper. The degree of correlation between the ONSD values of the left and right eyes has been found by computing the correlation coefficient between them. Pearson coefficient correlation (r) has been computed to examine the degree of overall closeness between the ONSD values of the left and right eyes of the patient, whereas the p-value indicates the significance of the correlation coefficient for the confidence interval of 95%. A correlation (r) value of .80 (p < .01) has been obtained between the ONSD values measured by the medical experts for the left and right eyes. A strong correlation between the ONSD values of both eyes (BE), establishes that the desired clinical information related to the ICP condition can be obtained by observing ocular ultrasound of one of the eyes of the patients. Based on these findings, it can be suggested that during the acquisition of ocular ultrasound for routine bedside purposes, the ONSD measurement of one eye can be sufficient to save time and avoid discomfort. The mean (M) and standard deviation (SD) of the manually measured ONSD values for the left eye (LE) and right eye (RE) were 6.52 ± 0.61 and 6.61 ± 0.72 mm, respectively. The overall mean and standard deviation of ONSD (manually) for both left and right eyes was 6.57 ± 0.67 mm and ONSD (automated) was 6.50 ± 0.71. Table 3 presents some clinical observations with regard to the patient data used in this study.
Clinical Observation of Obtained Patient Data.
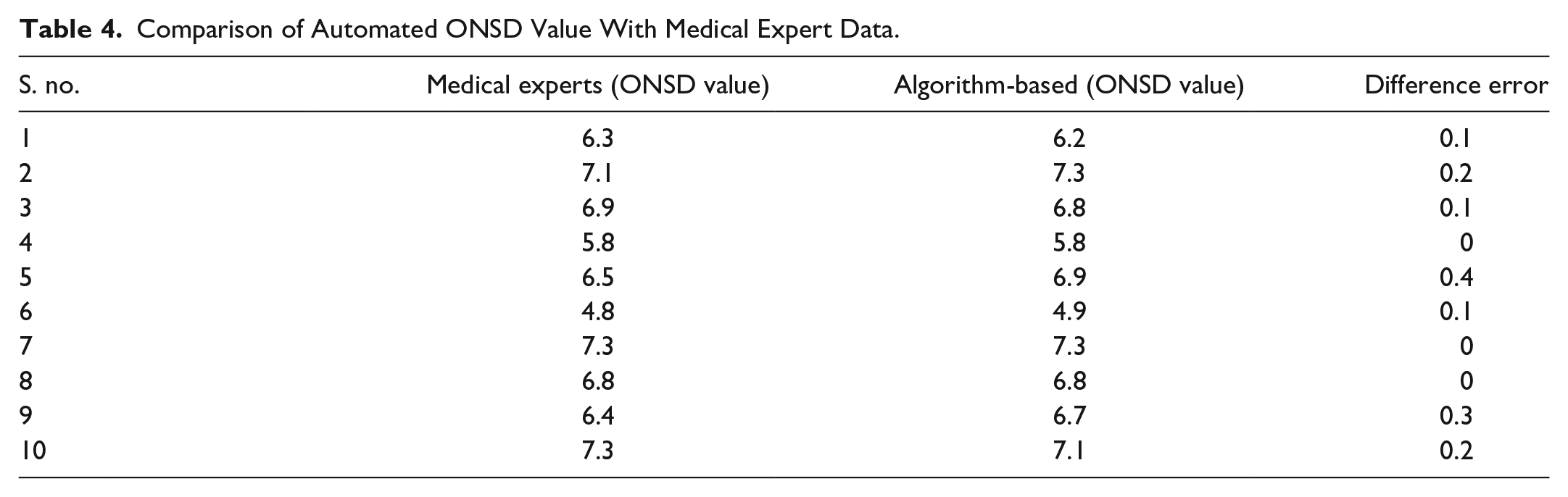
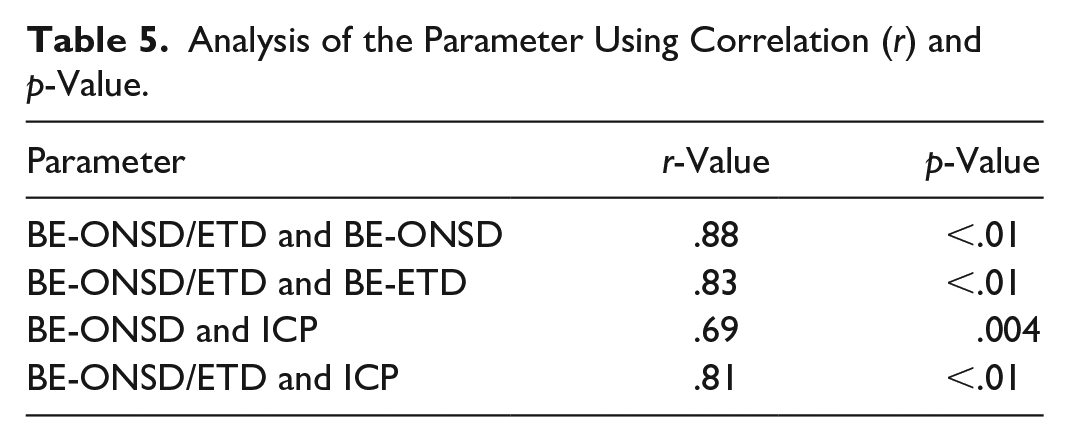
Now, the automated measurements of ONSD and ETD values are performed by applying the proposed algorithms using ocular ultrasound images of the patients. The performance of the automated ONSD measurement algorithm has been evaluated and its accuracy has been validated by comparing the manually measured ONSD values with the algorithm-generated ONSD values. Table 4 compares these values for 10 ocular ultrasound images randomly selected, highlighting the difference error. It is quite visible that the difference between the manually measured and algorithm-generated ONSD is negligible. Further, the percent root mean square error (PRD) has been computed between the two sets of ONSD values considering a total of 57 patients, and the obtained PRD value is found to be 9.82. The manually measured ETD is not available for the validation of automated measured ETD. However, through visual inspection by competent medical experts, the automatically measured ETD values were found to be accurate. Further, OER is computed considering the algorithm-generated ONSD and ETD values. The mean value of the OER for both the left and right eye is 0.27 ± 0.03. Now, it becomes significant to investigate the degree of correlation between the OER and the ICP values. The correlation coefficient for the available OER and ICP values has been determined as .81 (p = .004), whereas the correlation coefficient between algorithm-generated ONSD and corresponding ICP values has been found as .69 (p < .01). This clearly establishes that the OER parameter has a greater degree of closeness with ICP. Table 5 depicts the correlation coefficients for some of the diagnostically significant parameters. The next task of this research work is to determine the OER threshold value for predicting raised ICP conditions.
Comparison of Automated ONSD Value With Medical Expert Data.
Analysis of the Parameter Using Correlation (r) and p-Value.
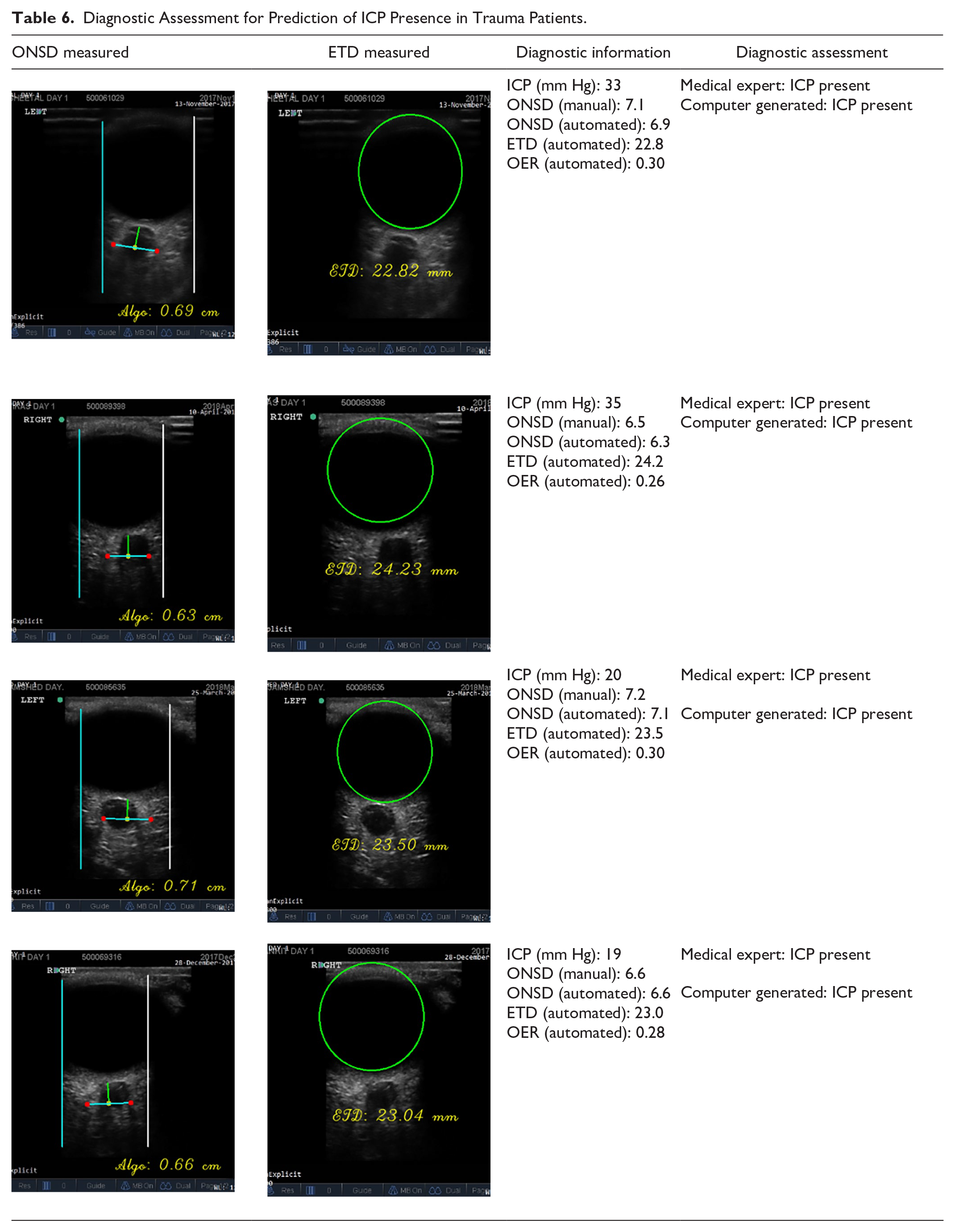
Clinically, ICP values for normal patients range from 5 to 15 mm Hg. For a significantly high-risk patient (hypertension cases), the ICP value lies between 20 and 30 mm Hg or above.20,21 Considering the 114 ocular eye images (57 each for left and right eyes), the computed OER ranges between 0.17 and 0.35. The ICP values obtained through conventional (invasive) ICP measurement ranges between 7 and 35 mm Hg. Based on the reported studies, an ICP value ≤15 mm Hg is considered a “normal” ICP and an ICP value >15 mm Hg is considered a “raised” ICP. An attempt has been made to figure out the threshold value of the OER for predicting raised ICP conditions by analyzing the scatter plot and heat map. Figure 4(a) shows the scatter plot between OER and the corresponding ICP values. It is observed from the figure that for ICP values >15 mm Hg, the minimum OER value is found to be 0.21. Therefore, it is established that the OER value ≥ to 0.21 indicates the raised ICP condition. The conclusion drawn from the scatter plot is further strengthened by the heat map analysis of the OER and ICP values. The heatmap analysis represents the risk assessment of the patients, which is depicted in Figure 4(b). The ICP and the OER significantly indicate high and low risk. The heatmap distribution obtained between ICP and OER indicates that maximum OER values lie in the range of 0.23 to 0.30 for an ICP > 15 mm Hg. Further, it has been observed that 67 eye images have an ICP value well above 20 mm Hg, and in 33 eye images, the ICP value lies between 16 and 20 mm Hg. In all the images of trauma patients, for an ICP above 15 mm Hg, the OER lies well above the threshold value of 0.21. In another case, for an ICP value below 15 mm Hg, its OER lies below the threshold value of 0.21. The patients whose ICP value is below 15 mm Hg suffer from medical conditions such as subarachnoid hemorrhage (SAH) and intraventricular hemorrhage (IVH). Furthermore, the performance of the proposed ICP prediction framework has been validated by comparing the algorithm-generated results with the diagnostic assessment done by competent medical experts. Based on the results presented in Table 6, it can be established that the computer-generated results about the ICP presence closely match the ICP assessment done by the medical experts.

(a) Scatter plot and (b) heatmap between BE-ONSD/ETD and ICP value.
Diagnostic Assessment for Prediction of ICP Presence in Trauma Patients.
Discussion
The study presents a reliable automated framework for the prediction of ICP in trauma patients based on the threshold value of ONSD and ETD ratio (OER). Many literatures have shown a strong correlation between ONSD and ICP. However, there is no established standard threshold value of ONSD to predict ICP. Currently, no reliable method is available for the prediction of ICP with the help of a non-invasive procedure. In the proposed work, novel automated algorithms are developed for the non-invasive measurement of ONSD and ETD in ocular ultrasound images. A threshold value of OER (0.21) has been determined using statistical analysis of the available patient data. An OER value ≥0.21 indicates the ICP presence. The experiment was performed on the data of 57 patients (adults of Indian origin) obtained from the trauma center, JPNATC, AIIMS, New Delhi, India. Obtained results indicate that ICP is strongly correlated with the OER, which gives a more accurate prediction for raised ICP. There was a significant correlation of OER with ICP (r = .81, p ≤ .01), whereas the correlation of ONSD alone with ICP was clearly lesser (r = .69, p = .004). Therefore, results obtained in the proposed work clearly demonstrate that the ratio of ONSD and ETD (OER), automatically measured using an ocular ultrasound is a potential biomarker for ICP prediction, which is independent of ethnicity and origin.
The automated measurement of OER and its strong correlation with an ICP can help in predicting raised ICP; this will facilitate trauma patients in early diagnosis and continuous monitoring of the raised ICP condition. Moreover, the presented automated framework for the non-invasive measurement of ONSD, ETD, and subsequent ICP prediction can be potentially useful in efficiently delivering tele-trauma services in remote, rural, semi-urban, and highway-side trauma centers. However, several limitations need to be addressed to overcome the challenges in accurate non-invasive ICP prediction. The present technique employs a B-scan ultrasonography imaging to achieve satisfactory visualization by manually adjusting the ultrasound machine’s gain. This adjustment allows for the optic nerve sheath and eyeball to be clearly observed. In the absence of a standardized gain value in the equipment settings, a limitation, referred to as the “blooming effect” by Vitiello et al. 33 arises due to the equipment’s gain-setting for repeated measurements using B-scan ultrasonography in patients. The gain settings affect the appearance of ocular structures, which can introduce errors in the manual evaluation of the optic nerve sheath diameter (ONSD) and eyeball transverse diameter (ETD), particularly with the B-scan method. Moreover, Vitiello et al. 33 has also discussed issues related to the caliper location, which has been taken care of in the proposed automated algorithm for the measurement of the ONSD by considering the orientation of the optic nerve axis. Furthermore, these issues can be overcome by utilizing the standardized A-scan technique, as suggested by Vitiello et al. 33 and Ossoinig et al. 34 which is more sensitive than the B-scan technique and is considered an accurate method for evaluating the ONSD, particularly when dealing with less than 0.5 mm.
Furthermore, it is crucial to consider the positioning of the ultrasound probe and the significance of evaluating both eyes. Ross et al. 35 demonstrated that placing the probe on the temporal bulbar conjunctiva, after prior anesthesia, with patients lying on their back and their eyes in a primary gaze position, provides potential variation in ONSD measurements. This is caused due to the changes in the position of the eyeball which can lead to variations in the amount of cerebrospinal fluid (CSF) surrounding the optic nerve, resulting in different ONSD values. Another study by Rosa et al. 36 utilized A-scan ultrasonography to assess the relationship between both eyes and found a statistically significant difference (p < .001) in ONSD values between the two eyes, without a clear dominance, in both normal and idiopathic intracranial hypertension (IIH) patients. This indicates that asymmetry exists in both eyes and suggests the importance of evaluating both eyes in ONSD measurements. However, the proposed methodology solely relies on B-scan ultrasonography and demonstrates a strong correlation (.80) in ONSD measurements by medical experts. Based on the recommended suggestions and supported by relevant references, it is necessary to conduct a thorough investigation to evaluate the performance of different ultrasound imaging modes (A-scan and B-scan) under various conditions, including open eyelid, closed eyelid, and the application of anesthesia prior to probe placement.36 –38 This issue is still unresolved and will undoubtedly be addressed in our future research work.
The study further concerns the lack of power analysis in determining the sample size. A larger population in the clinical trial can confirm the accuracy and dependability of the findings. Additionally, it is crucial to create a dependable automated system that can measure ICP value using non-invasive techniques. Furthermore, there is a need for grading criteria, enabling differentiation between different clinical conditions based on diagnostic biomarkers such as ONSD, ETD, and ICP. In developing a strong and reliable ICP prediction tool, a significant collection of relevant open-source clinical data from patients of diverse backgrounds and ethnicities is required. Furthermore, implementing an IoT-enabled hardware module for ICP prediction could enhance the management of tele-trauma conditions.
Conclusion
This paper presented a new non-invasive and automated ICP prediction framework based on ocular ultrasound. The objective was achieved by proposing automated algorithms for ONSD and ETD measurement, determining a threshold of OER using statistical analysis, and realizing an integrated module for predicting ICP presence. The PRD value of 9.82 between the manually measured ONSD and algorithm-generated ONSD validated the accuracy of the proposed automated ONSD measurement algorithm. The study found that the ratio of ONSD and ETD was strongly correlated with the ICP. There was a stronger correlation of OER with ICP (r = .81, p ≤ .01), as compared to a correlation of ONSD alone with ICP (r = .69, p = .004). The threshold value of OER (0.21) was determined statistically using the available patient data for ICP prediction. Finally, it was found that the patients with OER ≥ 0.21 had ICPs ranging between 17 and 35 mm Hg; this range is considered a raised ICP condition.
Footnotes
Acknowledgements
This work is in collaboration with the Jai Prakash Narayan Apex Trauma Center (JPNATC), All India Institute of Medical Sciences, New Delhi, India and partially supported by the Department of Science and Technology (DST), Government of India under BDTD.
Author Contributions
All authors contributed equally to this work. In addition, all authors have read and approved the final manuscript and have given their consent for publication of the article.
Data Availability
All relevant data are within the paper and its supporting files.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
This study was approved by the Ethics Committee “JPNATC, All India Institute of Medical Sciences, New Delhi, India” (Ref. Number: IEC-442/02.07.2021, RP-25/2021; DOA: 19/07/2021).