
Abstract
This paper discusses the rights of people with young onset dementia in their everyday lives. It does this by collaborating with co-author Petri, who was diagnosed with dementia whilst of working age. Petri shares his story of navigating the system to find resources for living a good and valuable life with dementia, starting with the challenges he faced in getting a diagnosis and accessing services, through to advocating for people living with dementia to defend their rights. The narrative form of Petri’s overall story is progressive; it reveals a range of challenges yet portrays a person living as well as possible with dementia. Key themes in Petri’s story are accompanied by a dialogue of Finnish laws and regulations, as well as literature on dementia. Besides increasing awareness and fostering change, Petri sees opportunities such as advocacy work as a rehabilitative activity for himself and as a way to show that it is possible to live an active life with dementia. From a practical and ethical point of view, it is crucial that academic researchers carefully consider how to remain sensitive to the lived experience of realizing one’s rights and maintain a regular dialogue and transparency during the co-authoring process.
Personal Reflexive Statement
Petri is living with dementia and is a core member of our team. He was diagnosed with dementia when he was working age, which led him to become an expert by experience as well as advocate trained by the Alzheimer Society of Finland. He is also a member of the Alzheimer Europe working group of people with dementia (EWGPWD). The rest of our team is made up of researchers from a wide range of disciplines, united by an interest in increasing knowledge and understanding of the lived experience of dementia. Petri has shared his first-hand experiences of young onset dementia as a member of the Finnish project steering group that we assembled to support our research focusing on working-aged people’s experiences of mild cognitive impairment or dementia. Working with Petri to understand lived experiences from first-hand perspectives is how we got the idea of writing together.
Introduction
This paper discusses the rights of people with young onset dementia in their everyday lives. To do this, Petri (author 2), who was diagnosed with dementia whilst of working age, shares his story to further understanding of this situation. A growing number of studies looking at the experience of receiving a diagnosis of dementia at a young age, with symptoms beginning before the age of 65 (Hendriks et al. 2021), are shedding light on people’s daily lives. This includes the different kinds of support needed relative to older people living with dementia plus the harmful impact of stigma associated with dementia (e.g., Busted, Nielsen, and Birkelund 2020; Greenwood and Smith 2016; O’Malley et al. 2021; Stamou et al. 2021). Other research has increased our specific understanding of receiving a dementia diagnosis whilst in employment (e.g., Chaplin and Davidson 2016; Nygård et al. 2023; Ritchie, Tolson, and Danson 2018). These studies highlight how the voices, needs and rights of people living with young onset dementia are not always considered, and different ways in which their position in society must be improved. People with dementia have also called for a rights-based approach to ensure their equal rights, such as access to the UN Convention on the Rights of Persons with Disabilities (CRPD; Dementia Alliance International 2016).
Most research involves people with dementia as research participants rather than as collaborators. To engage people living with dementia in meaningful ways, academic researchers must not only be open to challenging traditional views of research (Di Lorito et al. 2020), but also abandon preconceptions, largely based on stigma, about what experts in lived experience of dementia have to offer to the research process (Mann and Hung 2019; McConnell et al. 2019). Patient and public involvement (PPI), including co-research (Di Lorito et al. 2020) with people living with dementia is slowly becoming more common. As co-researchers, people living with dementia have developed new research projects (e.g., Thoft, Ward, and Youell 2021), implemented research by designing methods, conducting interviews, contributing to data analysis (Stevenson and Taylor 2019; Tanner 2012). While co-authoring where an individual with lived experience is also part of the writing team is becoming more common (see, e.g., Astell et al. 2014; Oliver et al. 2020; Williams, Richardson, and Draper 2018), the experiences of people living with dementia are most often reported by someone else, such as re-told by a researcher or by proxy through a family member.
Following the principle of “Nothing about us without us” (e.g., Oldfield 2021; Rahman et al. 2022) this paper explores the first-hand experiences of the second author, Petri, in navigating the system in Finland to find resources for living a good and valuable life with dementia. In this context, we use “system” mainly to refer to social and health care, but also touch on the knowledge and understanding of dementia (or lack of it) that circulates in society that people face and have to manage when they develop dementia.
Petri’s own story of young onset dementia provides insights into the different challenges—and successes—people face in realizing their rights. His story starts with the common problem among people with young onset dementia of getting a diagnosis, continues with challenges he faced accessing services, through to his work advocating for people living with dementia in Finland and abroad to defend their rights. Adopting a storytelling approach delivers insights into the meaning an individual gives to their lived experience, providing new ways of understanding illness or other adversity challenging counterproductive cultural perceptions and stereotypes (Frank 2013). Narrative research on dementia can illuminate the challenges and resilience of people with dementia and their loved ones (e.g., Buggins, Clarke, and Wolverson 2021; Li, Keady, and Ward 2021; Rossi-Harries et al. 2024), but also the collaborative and embodied aspects of storytelling (Hydén 2013).
Approach and Methods
A case study approach was adopted to explore the rights of people living with young onset dementia. Case studies can be based on one, two, or multiple cases, to gain an in-depth, detailed and complex understanding of the phenomenon of interest (e.g., Harris 2008; Harrison et al. 2017). Our single case study explores Petri’s accounts of his experiences, including articles and speeches he produced at different times, analyzed through narrative and thematic means.
Co-authoring
Our writing team consisted of Petri (the second author) and six academic researchers. Petri and his wife have been members of our Finnish project steering group where Petri has shared his first-hand experiences of young onset dementia during our research projects focusing on working-aged people’s experiences of mild cognitive impairment or dementia. Petri, who also works as an advocate for people living with dementia, has knowledge of their rights and has personally had to fight for them. Thus, we started to think about the possibility of writing together.
Roberts et al. (2020) point out various key areas that should be considered when involving people with dementia in research, highlighting the following ones which have received less attention. First, it is important to recognize and acknowledge the contribution made by experts by experience. Second, promoting and protecting their rights and well-being is essential; among other things, this enables direct contributions in a way that is appropriate and meaningful to them. Given Petri’s background as a person who speaks openly about his own experiences on the topic, it was most meaningful to write together to share these experiences. For this paper we drew inspiration from a co-authored article by Williams et al. (2018) exploring how continuing work is possible despite a dementia diagnosis. We also learnt from O’Connor and Mann’s (2019) article in which they pull together their insights on collaboration between a researcher and a dementia advocate.
Data, Analysis, and Writing Process
Early in our collaboration Petri shared his experiences with the health and social services, including a folder containing all the documents he had collected. This information and the ideas exchanged as we discussed them served as the starting point and basis for this paper. Mervi, Petri, and Anna (the first, second, and last author) discussed initial topics and decided Petri would draft his story covering the main issues he wanted to share. Petri also agreed to share the speeches that he had given in Finnish or English between 2017 and 2021 while working as an advocate. Additional material included a concise timeline starting from his sick leave to receiving a dementia diagnosis. Later, we included his writing about his experiences during the COVID-19 pandemic. Television programs and podcasts that had interviewed Petri were also viewed or listened to as complementary material. These were not analyzed, but rather served as a source and support for building a holistic and in-depth understanding of Petri’s experiences alongside the documented information and discussions with him.
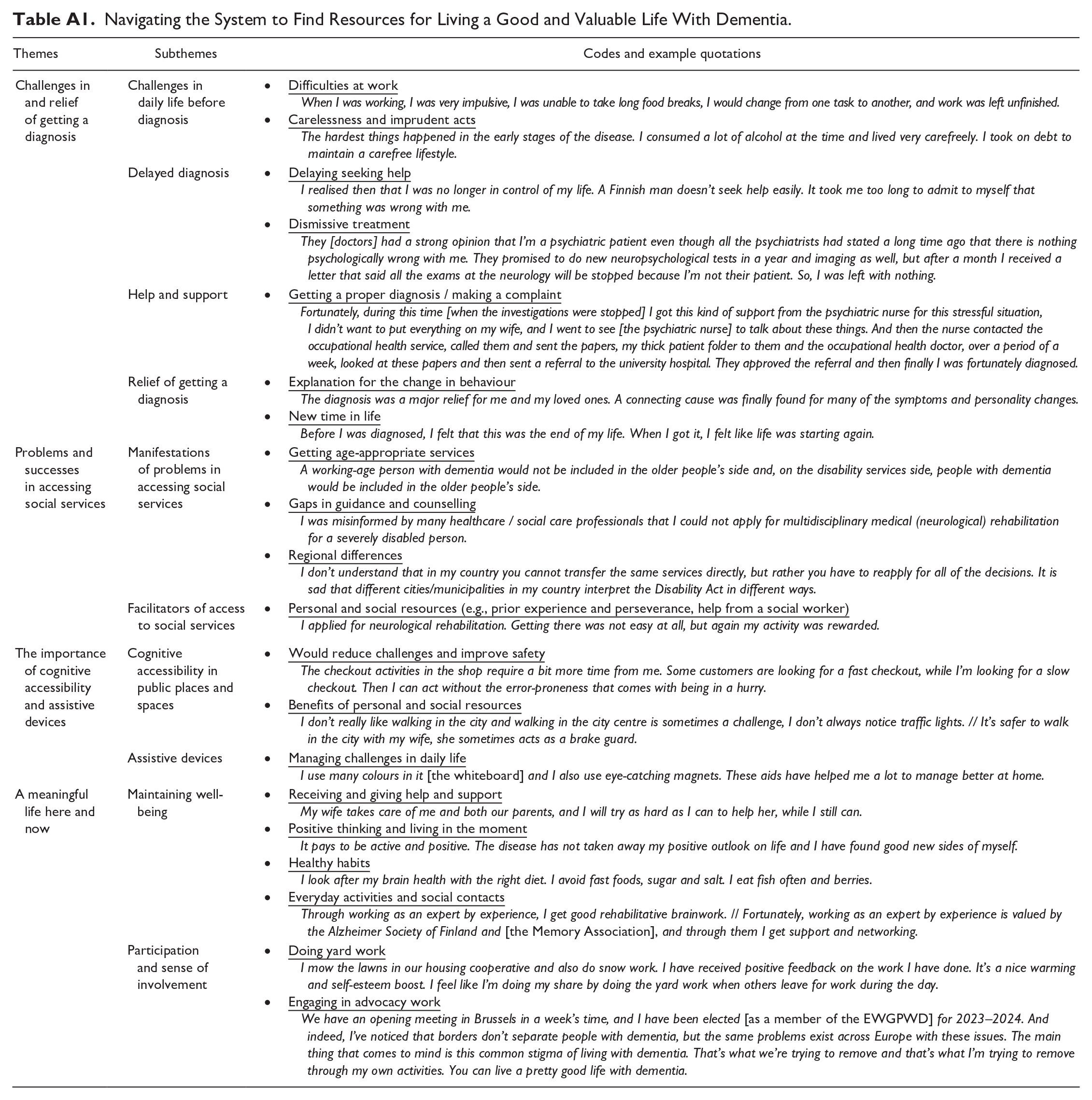
Data analysis and writing took place in 2022 and 2023, focusing mainly on the content of Petri’s writings; however, we also paid attention to the structure of his narrative (Josselson and Hammack 2021; Riessman 2008). Based on the different materials and discussions, we organized the key events and experiences in chronological order to form an overall “plot” of his story, which was then used to identify the prototypical form of his narrative. Gergen and Gergen (1986) suggested that a narrative can be progressive, regressive or one in which there appears no change in terms of achieving a particular goal. This framing helped us to understand Petri’s story as a progressive one in terms of living as well as possible with dementia. Facing challenges with accessing adequate and appropriate services that change shape over time, makes his story more complex. Close examination of the key events, turning points, and characters in Petri’s story showed that his experience was more than events and experiences explicitly related to rights. There were also his own actions, to find different resources to live well with dementia, such as maintaining wellbeing by seeking social contacts with others (the coding framework with themes, sub-themes, codes and example quotations are in an Appendix Table A1).
As we sought to place Petri’s experiences in dialogue with previous literature, the thematic part of our analysis can best be described as combining inductive and deductive techniques (Hsieh and Shannon 2005). Based on Petri’s draft, Mervi (disciplinary background in social psychology) and Anna (disciplinary background in law) created the first version of the paper. Petri and four other co-authors read and discussed the first draft, after which Mervi, Anna, and Petri met on Teams to discuss amendments based on Petri’s ideas and to clarify some issues raised by the co-authors. The paper was revised based on all authors’ comments and circulated again for further review by the whole group.
Guidance on partnering with people with dementia in research, highlight the importance of providing adequate training and support, for example, by making “reasonable adjustments” (Roberts et al. 2020). Our approach to involving Petri at every stage of preparing this paper, was to discuss and take his views on both the writing process and the content of the text into account throughout. We worked to establish Petri’s wishes in terms of communication (Williams et al. 2018); for example, he was asked whether the best way for him to contribute would be by meeting and discussing the paper or by writing comments—either directly on the text or, for example, by email. He was asked whether he wanted to read the paper in Finnish or in English, as well as whether there was anything we might do to make the text be easier to read in some other way.
For Petri, things that make co-authoring possible for him were the following: (1) his awareness that academic researchers do not expect him to write scientifically; (2) having several pieces of writing he can draw on; (3) his earlier experience as a dementia advocate; (4) his experience of using different applications such as a translator app; (5) maintaining mutual trust and confidentiality (this is particularly important as the authors may talk about all sorts of things outside of writing the paper, but you only write about the things you agree to write about); and (6) giving enough time for thought, input, and review. From an ethical point of view, fostering cooperation based on trust, respect, and reciprocity is not only crucial to collaborative success, but also a fundamental aspect in respecting another person’s individualism, agency, and dignity (Mann and Hung 2019; Riches, Ridgway, and Edwards 2023).
Collaborative writing required the researchers to always be sensitive to Petri’s personal story, updating information on changes made to the text as well as the status of plans and schedule for publication, thereby also supporting the management of being in the “in-between” period. The uncertainty related to the possibility and timing of scientific publication is indeed one of the key challenges of co-authoring, which further underlines the importance of regular dialogue and transparency.
The following sections contain key themes identified in Petri’s narratives and writings accompanied by a dialogue of Finnish laws and regulations, as well as previous literature on dementia.
Findings: Petri’s Story
We begin by describing the challenges Petri experienced in his daily life before receiving a dementia diagnosis, the problems he faced in getting the diagnosis itself, what help and support he received along the way, and how he responded to the diagnosis. We then go further by highlighting the problems he has encountered in getting appropriate and adequate social services, including describing his efforts and successes in managing these problems. After considering the importance of cognitive accessibility and the benefits of assistive devices, we shed light on how Petri strives to maintain well-being and can experience a sense of participation and inclusion to live a meaningful life here and now.
Challenges and Relief of Getting a Diagnosis
Petri realized that something was not right when he no longer recognized himself as the Petri he had been before. He couldn’t stand still and was always on the move. He says that his work as a parish gardener was interrupted when he hastily moved on to other tasks, and he forgot appointments and deliveries. Previous studies have documented that it is often at work that changes first appear (e.g., Shastri et al. 2022). Petri knew and felt that something was very wrong and wanted to contact the occupational health service but was worried about losing his job and also about his finances. According to Petri, difficulties with control of alcohol consumption and managing money (carelessness and imprudent acts) began to interfere more and more with his daily activities, and incidents started to occur at home. At the end of the summer holidays, Petri dared to seek help because he felt that he would not be able to cope at work for another day.
That summer, I had been working in the same job for 25 years in a cemetery. By spring, I had celebrated my fiftieth birthday. I took a summer holiday as planned, but the plan was not to never go back to work. (Petri’s writing)
Petri sought help from health services, but as is often the case with people of working age, it took time to get a diagnosis (O’Malley et al. 2021; Roach, Drummond, and Keady 2016; van Vliet et al. 2013). In Petri’s case, it took two years. Thus, it seems to take a lot of perseverance not to give up on getting help if the diagnosis is delayed even though it is the patient’s right to be diagnosed. Petri would have liked to see multidisciplinary collaboration during the diagnostic process: I would think that a diagnosis would be made more quickly by a multidisciplinary team, with many doctors who are familiar with a particular disease, as well as other health professionals. This would help in avoiding gaps in information and also reduce the number of patient visits. There would also be savings for society and the patient through this approach. (Petri’s writing)
The Charter of Fundamental Rights of the European Union states that everyone has the right to receive medical treatment in accordance with national law and practice (Article 35). According to the Finnish Health Care Act (1326/2010, HCA), a patient who has received a referral from a doctor based on an examination must have access to specialist care within a time limit. If assessment of the need for treatment requires a specialist assessment or special screening or laboratory tests, the assessment and the necessary tests must be carried out within three months of the date of receipt of the referral. Treatment and counseling that are deemed necessary based on an assessment of the need for treatment must be provided and started within a reasonable period, but within six months of the need for treatment being established (HCA § 52). However, the problem for Petri was that his diagnosis was delayed; there seemed to be no explanation for his symptoms, and he was discharged without a diagnosis. Petri recalls that in the end his situation was dismissed: The hardest day of those two years was when I was discharged from the psychiatry and neurology outpatient clinics within the same week. I was left without a treating and investigating body. (Petri’s writing)
However, Petri was lucky. While he no longer had anyone investigating his condition, he received psychosocial support from a psychiatric nurse, who took charge of the situation and referred him back to occupational health care. There, an occupational health physician interested in Petri’s symptoms carefully examined his medical records, interviewed him clinically, and then made a referral to the neurology outpatient clinic at the University Hospital.
While for some people, diagnosis of dementia comes as a shock, for others like Petri, it is a relief (Clemerson, Walsh, and Isaac 2014; Johannessen et al. 2019). Petri notes that the time before receiving the diagnosis had been very stressful for his whole family. According to him, the diagnosis helped them to understand the reasons behind his changes in behavior.
Petri says that although he was eventually diagnosed, he was still bothered by the dismissive treatment he faced in health care. For the first time in his life, he felt mistreated. The Finnish Patient Act (785/1992) lays down general principles for the treatment of patients. According to the Act, patients have the right to good quality health and medical care and must be treated in such a way that their dignity is not violated and that their personal convictions and privacy are respected (Article 3.2). According to the travaux prèparatoires of the Act, patient treatment refers to the way in which a patient is treated during treatment or investigations.
Petri made a complaint about his treatment to the hospital’s chief physician based on section 10 of the Patient Act. According to Petri, many of his friends encouraged him to complain. He also saw the importance of addressing the issue (i.e., dismissive treatment and terminated investigations) so that those in a similar situation would be treated more fairly in the future. The patient ombudsman gave advice and helped Petri with the complaint. In the end, he received a decision that the neurology outpatient clinic should not have stopped the investigations. This unit later called and apologized for the mistake they had made. Petri answered them positively: “Nothing is won by bitterness and anger.” However, Petri hopes that no one else endures the same experience.
Problems and Successes in Accessing Social Services
People diagnosed with young onset dementia value access to age-appropriate services suitable for their specific needs and, for example, support with applying for benefits after the end of employment (Stamou et al. 2021). Petri’s case highlights a key issue for people living with young onset dementia, regarding whether they receive their services as part of disability services or as part of older people services. The question of whose client Petri was in the first place, was debated between the different services. Petri says: A working-age person with dementia would not be included in the older people’s side and, on the disability services side, people with dementia would be included in the older people’s side. (Petri’s writing)
Petri knew that he might be eligible for rehabilitative day activities under the Disability Services Act (380/1987) and contacted the city’s disability services. In response, Petri, 52 years old at the time, was told that he was on the side of older people services. However, through home care, he had already been informed that there were no other activities that could be organized on the older people’s side, other than occasional visits to the older people’s strength and balance group. According to Petri, this was not meaningful for a person of working age. As noted by Clemerson et al. (2014), the lack of tailored services for younger people living with dementia is problematic and can reinforce their isolation.
One problem with the Finnish social care system is that people living with dementia are bundled into older people services and find it very difficult to access services on the disability side. In Finland social and healthcare services are provided based on different laws. The principle is to provide services based on general legislation, such as the Social Welfare Act (1301/2014) and based on a person’s needs. Nevertheless, there is another law, namely the Act on Disability Services and Assistance (380/1987; hereinafter the “Disability Services Act”), which offers a better legal guarantee for a person in need of services than the Social Welfare Act. The problem is that people with dementia are often regarded as not being entitled to the support provided for under the Disability Services Act because cognitive disabilities, such as those arising from Alzheimer’s disease, are not always viewed as being “disabilities” under the law; rather they are associated with normal aging. The fact that sometimes very similar needs result in access to very different services because of the age or illness of a client can be seen as an ethical and human rights issue (Hoppania, Mäki-Petäjä-Leinonen, and Nikumaa 2017). Thus, it seems that the Finnish approach to the interpretation of the Disability Services Act does not fulfill the requirements set in the UN Convention on the Rights of Persons with Disabilities (UNCRPD), because the assessment of the right to services is based on age and diagnosis more than capabilities.
However, Petri says that he was persistent about the daytime activities and finally the disability services worker said, “put the application in, we have to process it.” Petri submitted the application with a lot of attachments. After a few months, he received a positive decision for day activities, to which he went every two weeks.
In Finland, the obligation to provide information and guidance about social and health care issues is a task that social and health care professionals must carry out (section 5 of the Social Care Customers Act 812/2000 and section 5 of the Patient Act 785/1992). Petri’s story of the progress of his case in relation to the decision on day activities reflects the Finnish culture of guidance and counseling. This is where giving information is sometimes avoided or a negative assessment of the possibility of receiving the service is given in advance before the social care client has even submitted an application. In such cases, some clients leave without formally applying for the service and without receiving a written, appealable decision (Nikumaa and Mäki-Petäjä-Leinonen 2019).
According to Petri, through his perseverance, he received many social welfare benefits and services that he was happy with. For many years he was a client of both disability services and services for older people. Occasionally, home visits were made, and the situation of Petri and his family was assessed. His wife was granted carer’s allowance and Petri was granted the right to a personal assistant under the Disability Services Act, just before the Covid-19 pandemic started in 2020.
Petri characterizes the beginning of the COVID-19 pandemic as an “emotionally difficult time.” The pandemic coincided with Petri’s mother falling seriously ill and Petri did his best in taking care of his aging parents’ affairs. His parents were unable to meet each other due to restrictions in the hospital and according to Petri, getting adequate information and treatment for his mother was challenging. Petri also helped his father a lot during this time. Petri’s personal situation also changed in the midst of the pandemic when he and his family decided, after long consideration, to move to another town for family reasons. He explained that one reason he was not keen to move before, was that it would be “a hassle” to reapply for benefits. He wondered if he would have the energy to prepare the many applications and apply for new medical statements again. This is what happened: I got transport services, but my wife no longer received family caregiver support. We could not understand why family caregiver support was not granted on the same basis as when living in the previous city? Moving to a strange place and creating a new everyday life certainly did not improve our situation. (Petri’s writing)
According to Petri, he got advice from the city’s social worker on how to draft a complaint. He lodged a complaint with the city’s social and health committee, but it was unsuccessful. Petri would very much like to see the Disability Services Act and the Act on Care for the Older People applied in the same way, regardless of where you live.
Petri’s family experience of reapplying for benefits highlights regional and local differences in access to different benefits in Finland. Finland has also received rulings on this from the Council of Europe’s Committee on Social Rights. The revised European Social Charter includes a system of collective bargaining, which Finland ratified in 1998. In this context, the European Committee of Social Rights ruled in 2012 that the right to social protection guaranteed by Article 23 of the Charter had been violated by the differential treatment of caregivers of older people across the country. The complaint further alleged that the differences in the provision of services by municipalities due to inadequate funding, amounted to unequal treatment of older people. In its ruling, the Committee stated that although the Charter does not require that the level of protection should be the same throughout the country, it does require reasonably uniform treatment. The Committee considered it a violation of Article 23 that Finnish legislation allows some older people to remain without family caregiver support or alternative support.
Petri points out that disability services are typically unaware of active, working-age individuals with dementia, which meant he had to work hard to get support from society to be able to advocate for people living with dementia. Recently Petri has been informed that he has been granted a personal assistant, for example for leisure activities and also advocacy work in his home country together with Petri’s wife, who is not always able to take time off work. Petri’s wife will continue to work as his personal assistant when traveling abroad (e.g., to the meetings of the Alzheimer Europe Working Group of People with Dementia, EWGPWD) for which she will be paid a daily allowance. Petri says that earlier he did not have the energy to apply for a personal assistant and hoped that his wife would be granted family caregiver support. Therefore, Petri describes the current situation as a “labour victory.” Petri sees that, with this support, he will be able to continue working as an expert by experience for longer.
The Importance of Cognitive Accessibility and Assistive Devices
Petri considers the ways that dementia affects his ability to carry out activities of daily living and highlights the importance of cognitive accessibility in reducing challenges and improving safety. In other words, the need to pay close attention to characteristics of public places and spaces to make them accessible to people living with cognitive impairments. Petri reports that challenges related to his short-term memory, concentration, attention, and impulsivity may not always show on the surface but can, for example, make activities in public places demanding and sometimes risky.
Walking through areas with a lot of traffic is sometimes a challenge, I don’t notice people walking with me. I may walk across the road at red traffic lights. Fortunately, I’m aware of my symptoms so I was able to voluntarily give up my right to drive. (Petri’s writing)
Petri’s experiences of traffic echo the findings of previous research illuminating how pedestrians with dementia may encounter problems in maintaining focus and staying in control in ongoing and complex traffic situations (Brorsson et al. 2016). Furthermore, challenges can occur in other types of public spaces such as grocery stores where characteristics such as illogical arrangement, overload of products, information and people, visual illusions (e.g., glass walls), or intrusive auditory stimuli can impair the accessibility and usability of the space (Brorsson et al. 2020). In addition to distracting music and unclear signage, Petri points out that he may make the mistake of using the wrong compartment in sex-separated public toilets or for example, confuse very similar-looking medicine packs with each other. However, as detected in a previous study (Brorsson et al. 2020), in addition to characteristics of the space itself, personal capacities such as staying focused contribute to accessibility and usability of the space. Petri mentions humor, giving time for himself, and trying not to get upset, as particularly helpful in such situations, along with his wife’s assistance. Petri also uses a whiteboard at home, which is an important tool for managing challenges in his daily life: I have been using the whiteboard for seven years now. I use different coloured markers and magnets in it. I make a note of upcoming events, medications, dates, and days, where I’ll be, etc. When I go out, I take a photo of the board, so the calendar goes in my pocket. (Petri’s writing)
The whiteboard (and photos of it in Petri’s mobile phone) lead us to reflect on the role of assistive devices and particularly information and communication technology. Assistive technologies can create barriers for a person living with dementia, but they can also extend their daily life opportunities (Kenigsberg et al. 2019). For example, the person living with dementia and those close to them (e.g., family or employer) could use technology to create and track everyday strategies together (Shastri et al. 2022). Above all, assistive technology must meet the needs of people living with young onset dementia and their care partners at the right time to promote independence and self-reliance, making everyday life easier for both (Holthe et al. 2018). An overarching goal is to for mainstream technologies to be more inclusive of people living with dementia, thereby implicitly supporting needs while also fostering inclusion.
A Meaningful Life Here and Now
Working-aged people living with dementia are often diagnosed at a stage in their lives where they still have multiple roles, such as spouse, parent, worker, and child of aging parents (Harris 2004). Petri says that the time before receiving the diagnosis was “a very foggy time” for the whole family and that he even thought his life was “ending.” Previous studies have reported that negative emotions and experiences of stigma and losing one’s sense of self, for example, are possible reactions to receiving a diagnosis (Bannon, Reichman, et al. 2022; Busted et al. 2020). Receiving an explanation for his challenges and careless behavior made Petri feel, in turn, that his life was “starting again.” He emphasizes that he would not have been able to find a new, brighter time without the support and understanding of those close to him. According to Petri, his wife’s support and understanding has been particularly important and helpful. Along with other services, Petri and his family received vital information, advice, and support from their local association of the Alzheimer Society of Finland. According to Petri, this kind of support helps a person living with dementia and their loved ones to cope with change and move on with their lives in a way that suits their situation.
When people with dementia and their loved ones get the support they need, life can go on. I have found my own path after many choices. I don’t want to turn back from this path and go back to the ‘old life’. I have my own thing now and it fills my life like a working life. (Petri’s writing)
Like many younger people living with dementia, Petri has chosen to focus on the positive aspects of his life and the resources he has (Johannessen et al. 2019). Earlier research has shown that the use of adaptive coping strategies such as optimism, problem-solving, seeking acceptance (Bannon, Reichman, et al. 2022) and living in “the here and now” (Johannessen et al. 2019) support living well with dementia. Furthermore, Petri says that he maintains his well-being through a healthy diet, exercise and by seeking social contacts. Petri feels that an active approach and courage have helped him overcome many obstacles. He highlights that he has actively fought against the stigma associated with dementia by being open and “giving dementia a face.” I have given a face to dementia without being ashamed of it. Dementia is a neurological disease and not just a disease of the older people. Over the years I have tried to influence people’s attitudes towards this disease. By doing small things, we can change things in a more memory-friendly direction. (Petri’s writing)
Earlier research has found that dementia often reduces the social networks of people living with young onset dementia and their carers (Harris and Keady 2009). This is despite their wish to stay engaged with others, be included in society (Greenwood and Smith 2016) and take part in meaningful activity that have a positive impact on their quality of life (Roach et al. 2016). Meaningful activity and social engagement can take different forms, as exemplified by the previous Get out of the House (GOOTH) project, where men with young onset dementia were involved in volunteering at a local zoo (Kinney, Kart, and Reddecliff 2011). According to Petri, doing yard work for their housing co-operative while others are at work and receiving positive feedback for it warms his heart, boosts his self-esteem, and makes him feel included. In other words, retaining a positive identity and roles is often very important for younger people living with dementia (Harris and Keady 2009) who may need to leave working life behind and wish to get something to replace it. For Petri this replacement has in many ways been the opportunity to work as an expert by experience.
The Alzheimer Society of Finland trained Petri and his wife to speak for dementia. According to Petri, advocating for people living with dementia in the Alzheimer Society of Finland and its local associations, as well as being a member of the Alzheimer Europe Working Group of People with Dementia, have enabled him to make new social contacts and maintain his ability to function. These opportunities have given him a channel to defend the rights of people living with dementia and, thereby, a sense of involvement and purpose in life. The voices of people living with dementia can be made heard in many ways, such as through consultation or interviews, not to mention research projects led by people with dementia (see Litherland and Hare 2024). Petri sees the appreciation that academic researchers give to people with dementia as important.
I’ve also noticed the same things when I’ve been in the working group [EWGPWD] that I’ve had to fight for my rights in my own country. Unfortunately, these same difficulties in terms of the services received affect people with dementia and their loved ones, regardless of national borders. In one country, some things work better or worse than in another. As a member of the working group, I have been able to share this information with researchers, and also to receive it. (Petri’s writing)
Encouraging feedback has given Petri a sense of contributing to society. Participation in everyday life makes Petri feel that he is living “a good and valuable life.”
Discussion
Through this paper, Petri’s experiences of navigating the system after being diagnosed with dementia at working age, is accompanied by a dialogue of Finnish laws and regulations, as well as previous literature on dementia. In many ways, Petri’s perseverance has enabled him to claim his rights as a person with young onset dementia. According to Petri, several things have helped him along the way, including support and assistance from different professionals (such as psychiatric nurse, patient ombudsman, and social worker), and the local associations of the Alzheimer Society of Finland. Petri sees that in many instances he has received the necessary information unexpectedly or came across it by chance. Furthermore, the fact that he learned to make applications through experience and that he has helped his own parents a lot, has helped him to claim his rights. He feels he has always been “systematic,” for example earlier in working life, and although dementia has had its consequences for him, this skill has not disappeared. Petri wants to be involved in activities to defend his own and others’ rights—through, among other things, writing this paper—so that others do not have to overcome the same hurdles he has. Besides increasing awareness and fostering change, Petri sees opportunities such as activities related to advocating as ways to challenge himself and show that it is possible to live an active life with dementia. Petri sees advocacy work as a rehabilitative activity for himself—“it’s good for the brain.”
This paper is based on a single case study design, which without a doubt limits the conclusions that can be drawn. Despite the uniqueness of Petri’s personal story, it has similarities with the experiences of people living with young onset dementia in different countries reported in existing research literature. In doing so, it reflects common challenges they experience in realizing their rights. First, getting a dementia diagnosis was a complicated path for Petri which seems to be typical in cases of people of working-age (e.g., Roach et al. 2016). Petri’s experience is a striking example of how it may take a lot of perseverance, hope, and good luck in addition to finding people who put effort into helping. Petri felt that he was not treated well in all respects, and he is not alone in this experience (O’Malley et al. 2021). This is a reminder that the right to good quality health and medical care is required to preserve a person’s dignity as well as respecting their personal convictions and autonomy along with their privacy (Mäki-Petäjä-Leinonen 2016).
Second, consistent with previous studies, Petri’s story highlights the need to improve and ensure access to age-appropriate services among people living with young onset dementia, including high-quality guidance, and counseling (e.g., Stamou et al. 2021). The provision of adequate, individually tailored, and comprehensive information is vital for a person’s rights to be secured, particularly in the case of a person with dementia (Nikumaa and Mäki-Petäjä-Leinonen 2019). Overall, a human rights approach to post-diagnostic support would provide people with dementia with “equitable, accessible, affordable, empowering, ethical and dignity-enhancing” services (Cahill 2022). Providing timely resources and psychosocial support to individuals living with young onset dementia and their loved ones is also essential in times of crisis as the COVID-19 pandemic illustrated (Bannon, Wang, et al. 2022). Furthermore, Petri’s experiences during the pandemic illustrate the cumulative burden that can arise for a person with young onset dementia, who may face life changes and responsibilities typical of working age during the restrictive circumstances of a crisis.
Third, Petri’s story underlines the importance of facilitating conditions for living a meaningful life around the social connections and activities that matter to oneself. Younger people living with dementia want to maintain an active social life, continue to participate and remain an active member of their community (Stamou et al. 2024). In relation to this, Petri calls for the necessity to move toward a society in which stigma is a thing of the past and diversity is better considered, including by ensuring cognitive accessibility.
From a practical and ethical perspective, we have learned that if research is to capture authentic experience and perspectives, it is crucial that academic researchers carefully consider how to: (1) remain sensitive to a personal story based on lived experience of realizing one’s rights, as well as (2) maintain a regular dialogue and transparency when engaging in co-authoring to increase socio-legal understanding of the topic at hand. Passing on lived experiences of dementia that sustain a sense of hope and resilience is essential, given that so much of the understanding of the topic circulating in society is to the contrary (Pipon-Young et al. 2011). Petri’s is a good example of a “quest story,” whose teller has learned something of value to share (Frank 2013:118). Petri’s story is indeed progressive (Gergen and Gergen 1986) in the sense that it reframes his identity from a person that he no longer recognized and who could very easily be exposed to stigma, to a person living a valuable and good a life as possible with young onset dementia. This progression occurred through agency in matters over which he can influence himself and with the support of caring others. However, Petri’s story is more complex than that, as it conveys the various challenges a younger person who is diagnosed with dementia and seeks to find different kinds of psychological, social, and material resources for living well, may encounter. In so doing, the story draws attention to equal rights, especially the gaps in their realization in practice, which demonstrate not only the need for coping with challenges and perseverance in pursuit of their rights, but also the need for social justice (Squire 2021).
Footnotes
Appendix
Navigating the System to Find Resources for Living a Good and Valuable Life With Dementia.
| Themes | Subthemes | Codes and example quotations |
|---|---|---|
| Challenges in and relief of getting a diagnosis | Challenges in daily life before diagnosis | • When I was working, I was very impulsive, I was unable to take long food breaks, I would change from one task to another, and work was left unfinished. • The hardest things happened in the early stages of the disease. I consumed a lot of alcohol at the time and lived very carefreely. I took on debt to maintain a carefree lifestyle. |
| Delayed diagnosis | • I realised then that I was no longer in control of my life. A Finnish man doesn’t seek help easily. It took me too long to admit to myself that something was wrong with me. • They [doctors] had a strong opinion that I’m a psychiatric patient even though all the psychiatrists had stated a long time ago that there is nothing psychologically wrong with me. They promised to do new neuropsychological tests in a year and imaging as well, but after a month I received a letter that said all the exams at the neurology will be stopped because I’m not their patient. So, I was left with nothing. |
|
| Help and support | • Fortunately, during this time [when the investigations were stopped] I got this kind of support from the psychiatric nurse for this stressful situation, I didn’t want to put everything on my wife, and I went to see [the psychiatric nurse] to talk about these things. And then the nurse contacted the occupational health service, called them and sent the papers, my thick patient folder to them and the occupational health doctor, over a period of a week, looked at these papers and then sent a referral to the university hospital. They approved the referral and then finally I was fortunately diagnosed. |
|
| Relief of getting a diagnosis | • The diagnosis was a major relief for me and my loved ones. A connecting cause was finally found for many of the symptoms and personality changes. • Before I was diagnosed, I felt that this was the end of my life. When I got it, I felt like life was starting again. |
|
| Problems and successes in accessing social services | Manifestations of problems in accessing social services | • A working-age person with dementia would not be included in the older people’s side and, on the disability services side, people with dementia would be included in the older people’s side. • I was misinformed by many healthcare / social care professionals that I could not apply for multidisciplinary medical (neurological) rehabilitation for a severely disabled person. • I don’t understand that in my country you cannot transfer the same services directly, but rather you have to reapply for all of the decisions. It is sad that different cities/municipalities in my country interpret the Disability Act in different ways. |
| Facilitators of access to social services | • I applied for neurological rehabilitation. Getting there was not easy at all, but again my activity was rewarded. |
|
| The importance of cognitive accessibility and assistive devices | Cognitive accessibility in public places and spaces | • The checkout activities in the shop require a bit more time from me. Some customers are looking for a fast checkout, while I’m looking for a slow checkout. Then I can act without the error-proneness that comes with being in a hurry. • I don’t really like walking in the city and walking in the city centre is sometimes a challenge, I don’t always notice traffic lights. // It’s safer to walk in the city with my wife, she sometimes acts as a brake guard. |
| Assistive devices | • I use many colours in it [the whiteboard] and I also use eye-catching magnets. These aids have helped me a lot to manage better at home. |
|
| A meaningful life here and now | Maintaining well-being | • My wife takes care of me and both our parents, and I will try as hard as I can to help her, while I still can. • It pays to be active and positive. The disease has not taken away my positive outlook on life and I have found good new sides of myself. • I look after my brain health with the right diet. I avoid fast foods, sugar and salt. I eat fish often and berries. • Through working as an expert by experience, I get good rehabilitative brainwork. // Fortunately, working as an expert by experience is valued by the Alzheimer Society of Finland and [the Memory Association], and through them I get support and networking. |
| Participation and sense of involvement | • I mow the lawns in our housing cooperative and also do snow work. I have received positive feedback on the work I have done. It’s a nice warming and self-esteem boost. I feel like I’m doing my share by doing the yard work when others leave for work during the day. • We have an opening meeting in Brussels in a week’s time, and I have been elected [as a member of the EWGPWD] for 2023–2024. And indeed, I’ve noticed that borders don’t separate people with dementia, but the same problems exist across Europe with these issues. The main thing that comes to mind is this common stigma of living with dementia. That’s what we’re trying to remove and that’s what I’m trying to remove through my own activities. You can live a pretty good life with dementia. |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Research Council of Finland (318848); Swedish Council for Health, Working Life and Welfare, FORTE (2017-02303); and Canadian Institute for Health Research (MYB155683) under the framework of the JPI MYBL; as well as the Research Council of Finland (314749), Ontario Shores Research Chair in Dementia Wellbeing, Schlegel Research Chair in Technology for Independent Living and the Strategic Research Council (SRC) within the Research Council of Finland (345298).