
Abstract
Background:Jejunostomy feeding tubes (JFTs) can be used to provide nutrition support to patients who have had surgery for esophagogastric cancer. Although previous research reports how patients cope with a gastrostomy tube, little is known about the impact of having a JFT. The aim of this qualitative study was to explore how patients and their informal caregivers experience living with a JFT in the first months following surgery. Methods: Participants were purposively sampled from a cohort of patients recruited to a trial investigating home enteral nutrition vs standard care after esophagogastric surgery for cancer. The sampling framework considered age, sex, and marital status. Informal caregivers were also invited to participate. Interviews were audio recorded, transcribed verbatim, and anonymized. Inductive thematic analysis was used to identify key themes related to living with a JFT. Results: Fifteen patient interviews were conducted; 8 also included a family caregiver. Analysis of the data resulted in 2 main themes: “challenges” and “facilitators” when living with a JFT. While “physical effects,” “worries” and “impact on routine” were the main challenges, “support,” “adaptation” and “perceived benefit” were what motivated continuation of the intervention. Conclusion: Findings suggest that participants coped well with a JFT, describing high levels of compliance with stoma care and the feeding regimen. Nonetheless, disturbed sleep patterns and stoma-related problems proved troublesome. A better understanding of these practical challenges, from the patient and family caregiver perspective, should guide healthcare teams in providing proactive support to avoid preventable problems.
Keywords
Clinical Relevancy Statement
Jejunostomy feeding tubes are often placed as a short-term adjunct in patients having surgery for esophagogastric cancer. This study provides an in-depth exploration of how patients and their family caregivers experience living with a feeding tube. The findings, which highlight the practical and emotional challenges that this intervention brings, along with an explanation of how people cope and adapt, can be used by healthcare teams to proactively support this group of patients.
Background
Major esophagogastric surgery as a treatment for cancer can lead to nutrition-related complications such as a reduced oral intake and malnutrition.1,2 During the immediate postoperative recovery for this type of surgery, patients are likely to be nil by mouth, progressing to oral fluids and diet, for the majority, within 8 days. 3 For some patients, the transition to eating and drinking sufficient to meet nutrition requirements can take much longer. Side effects of the surgery, along with the need to develop altered eating habits due to change in anatomical structure, can lead to prolonged periods of suboptimal nutrition,2,4 with >10% weight loss at 6 months reported for the majority of patients postesophagectomy. 5
Enteral feeding via a jejunostomy tube can be used to provide nutrition support to patients following esophagogastric surgery.4,6,7 In UK hospitals, practice varies, with figures suggesting that just over two-thirds of patients undergoing esophagectomy have a jejunostomy feeding tube (JFT) placed. 8 While major complications following placement of a JFT are rare, 4 the procedure is not without risk, with the findings from some studies suggesting an increased risk of postoperative complications such as infection and tube blockage.9,10
For those who struggle to maintain their nutrition status via the oral route, home enteral feeding via a JFT can be initiated. While minor complications such as stomal discharge, pain, and mechanical tube-related problems have been reported in patients fitted with longer term enteral feeding tubes, 11 less is known about the duration of feeding in the population of patients who have a JFT. Whether this intervention improves nutrition-related outcomes postoperatively is also not clear.
Previous research has begun to explore home enteral tube feeding from the patient’s perspective. Qualitative findings from studies of adult patients with gastrostomy tubes describe the physical and psychosocial impact of tube feeding.12–15 Quantitative survey data provide further evidence of the consequences of gastrostomy tube feeding, in terms of health-related quality of life, including the side effects that are experienced.16–18 No studies to date have identified how patients manage a JFT postdischarge from the hospital. Furthermore, although the impact of home enteral nutrition (EN) on informal caregivers is reported to be burdensome,19–21 how this is experienced by those caring for someone with a JFT remains largely unknown. The aim of this qualitative study was to explore how patients and their informal caregivers experience living with a JFT after surgery for esophagogastric cancer.
Methods
This qualitative study followed the principles of an inductive thematic inquiry. 22 Semi-structured interviews were conducted with patients who had recently undergone surgery for esophagogastric cancer at a university teaching hospital in the United Kingdom, serving a regional population of approximately 1.75 million. Participants were purposively sampled from a cohort of patients recruited to a pilot randomized controlled trial (RCT). The study compared 6 weeks of home EN with treatment as usual (discontinuation of enteral feeding at the point of discharge from the hospital) after esophagectomy or total gastrectomy for cancer. 23 To maximize variation in the cases interviewed, the purposeful sampling framework considered age, sex, and marital status. To add to the depth of data collected, we were also interested in interviewing patients with diverse informal care arrangements. As such, informal caregivers (eg, spouses or children of those recruited) were also invited to participate. Demographic information, including age and marital status, diagnosis, and preoperative body mass index, was recorded from the trial database. Information relating to which group the participant had been randomized to and the duration of feeding were also recorded. Ethical approval was granted by the Nottingham Research Ethics Committee (protocol 11/EM/0383). All participants, including informal caregivers, gave written informed consent prior to taking part in the interviews.
Face-to-face interviews were conducted by one of the research team (V.H.). Where an informal caregiver had been identified and recruited, a dyadic interview technique was used. All interviews took place between September 2012 and May 2014 at a time and location convenient for each of the participants. The interview schedule consisted of semi-structured questions and prompts that had been developed from the existing literature and agreed to by the study steering group, including service user representation. Although the questions posed were focused on the study aim, a flexible approach was taken to encourage participants to discuss what was important to them with regard to their experience of having a JFT or caring for someone who had one. Interviews were audio recorded, transcribed verbatim, and anonymized. Immediately, following each interview, handwritten notes were made by the researcher to capture impressions and observations that had been made during the interview process. Sampling continued until no new information was contributing to the analysis.
Interview Analysis
Inductive thematic data analysis 22 involved familiarization of the data through reading and rereading the transcripts and field notes. This was followed by initial coding and cross-checking where a code represented a word, phrase, or point of interest or relevance to the study aim. To enhance the reliability and validity of the analysis, the first 3 interview transcripts were analyzed by 3 of the research team (V.H., M.B., and D.B.), following which interpretation of the findings was discussed. Rather than quantifying interrater reliability, the aim of this initial stage of the analysis was to encourage consideration of themes within the wider context, avoiding single profession-centric interpretation of the transcripts. The remaining interviews were analyzed independently with the identification of patterns (ie, themes and subthemes at a semantic level) within and across the interview data by one of the authors (V.H.). Interpretation and summarization of the themes was undertaken collaboratively (V.H. and M.B.) and discussed by the study steering group. Data organization and retrieval were managed using NVivo 10 (QSR International Pty Ltd., Victoria, Australia).
Results
Interviews were conducted with 15 patients, 12 males and 3 females (Table 1). Interviews lasted on average 43 minutes (range, 21–75 minutes), and all but 3 took place at the patient’s home. One of the male patients chose to be interviewed at the hospital, one at work, and one on the local university premises. The median age of the patients was 67 years (range, 52–74 years). Most (67%) were married or cohabiting. All participants were of white British ethnicity. The diagnoses were cancer of the esophagus in 12 participants and proximal gastric cancer in 3 participants. All participants were interviewed within 4 months of having surgery (range, 7–15 weeks). The study population was deemed to be largely representative of the cohort of patients treated for esophagogastric cancer at the recruiting National Health Service (NHS) center.
Characteristics of Study Patient Participants (n = 15).
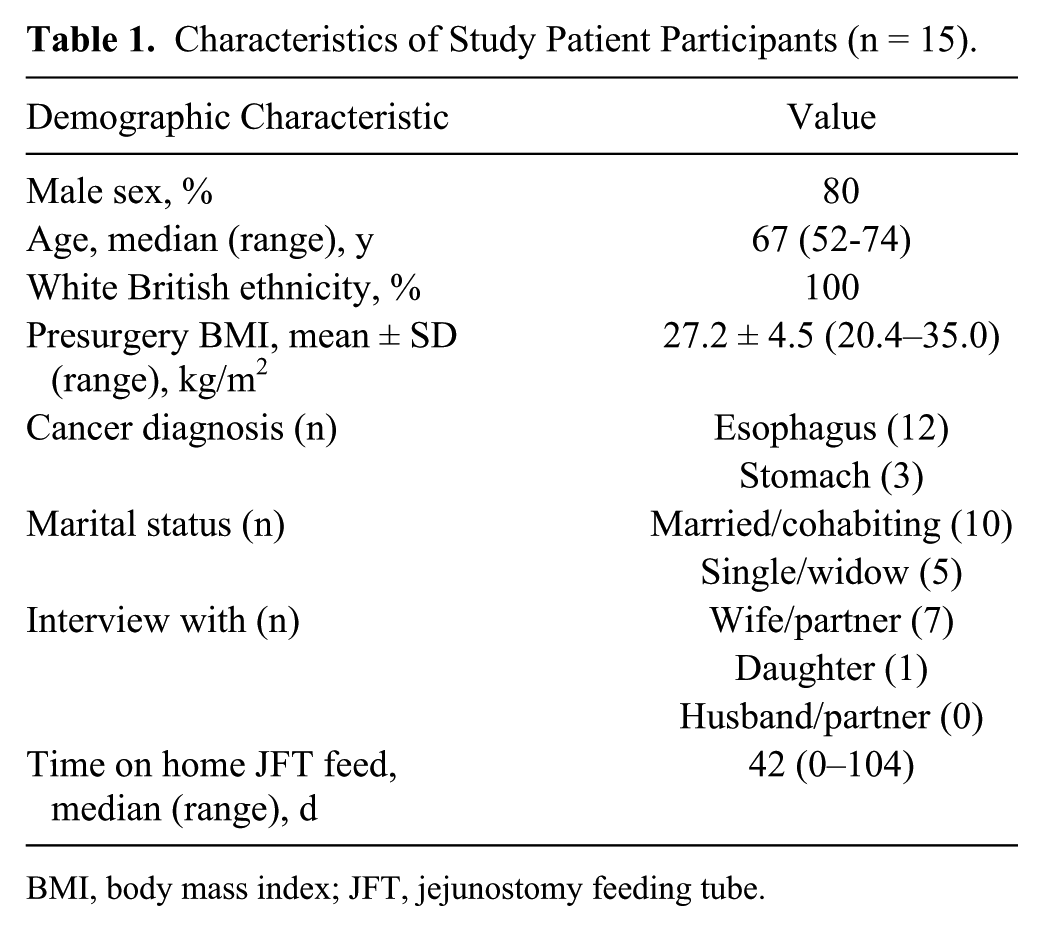
BMI, body mass index; JFT, jejunostomy feeding tube.
All patients had a JFT (Freka , Fresenius Kabi Ltd, Cheshire, UK; Ch/Fr 9) placed at the time of surgery, which had been used in the hospital during the immediate postoperative recovery period. Overall, 11 patients received artificial feeding at home with a median duration of 42 days (range, 0–104 days). For all patients, feed was delivered overnight through an enteral feeding pump. The other participants (n = 4) maintained patency of their JFT through regular flushing with water.
Eight of the interviews also involved a family member who was an informal caregiver, all of whom were female (6 wives, 1 partner, and 1 daughter) and lived in the same house as the patient. Of the 5 men who were interviewed alone, 1 had a wife who was in a care home and 2 of the wives were not able to attend the interview due to other commitments. The remaining 2 men lived alone, and while one talked about a friend who helped out, the other did not refer to any informal support. Both of the 2 women who were interviewed alone referred to children who had provided some, albeit, in one case, limited support.
Analysis of the interview data identified 2 key themes: “challenges” and “facilitators” when living with a JFT. Within these themes, “physical effects,” “worries,” and impact on routine” were the main challenges. “Adaptation,” support,” and “perceived benefit” were what helped patients and their caregivers to cope and what ultimately facilitated compliance.
Challenges of Living With a JFT
Without exception, all participants talked about the challenges of living with a JFT (Table 2). Physical problems that were described often related to the stoma site, with participants describing it as “swollen,” “sore,” “leaking,” and “infected.” It is usual practice in the United Kingdom for the external retention device of the JFT to be sutured in place. It was these stitches that caused patients the most discomfort, being described as “painful” and in one case of having a “cheese wire and cutting” effect. In some cases, the infected stoma site or suture area had warranted oral or topical antibiotic treatment. Also related to the presence of the JFT was the problem that 2 participants had with the tape that was used to hold it in place. One couple explained at length how the tape had caused a rash. They also talked of “so many trips up to the surgery and to loads of pharmacists” in their exploits to try and obtain the correct hypoallergenic tape. Gastrointestinal (GI) symptoms of “fast and loose bowel upset” and “heaving and retching” were experienced by 2 of the male participants who had been fed at home. Other GI side effects that were mentioned, related to the feed, were associated with reflux and bloating.
Challenges of Living With a Jejunostomy Feeding Tube.
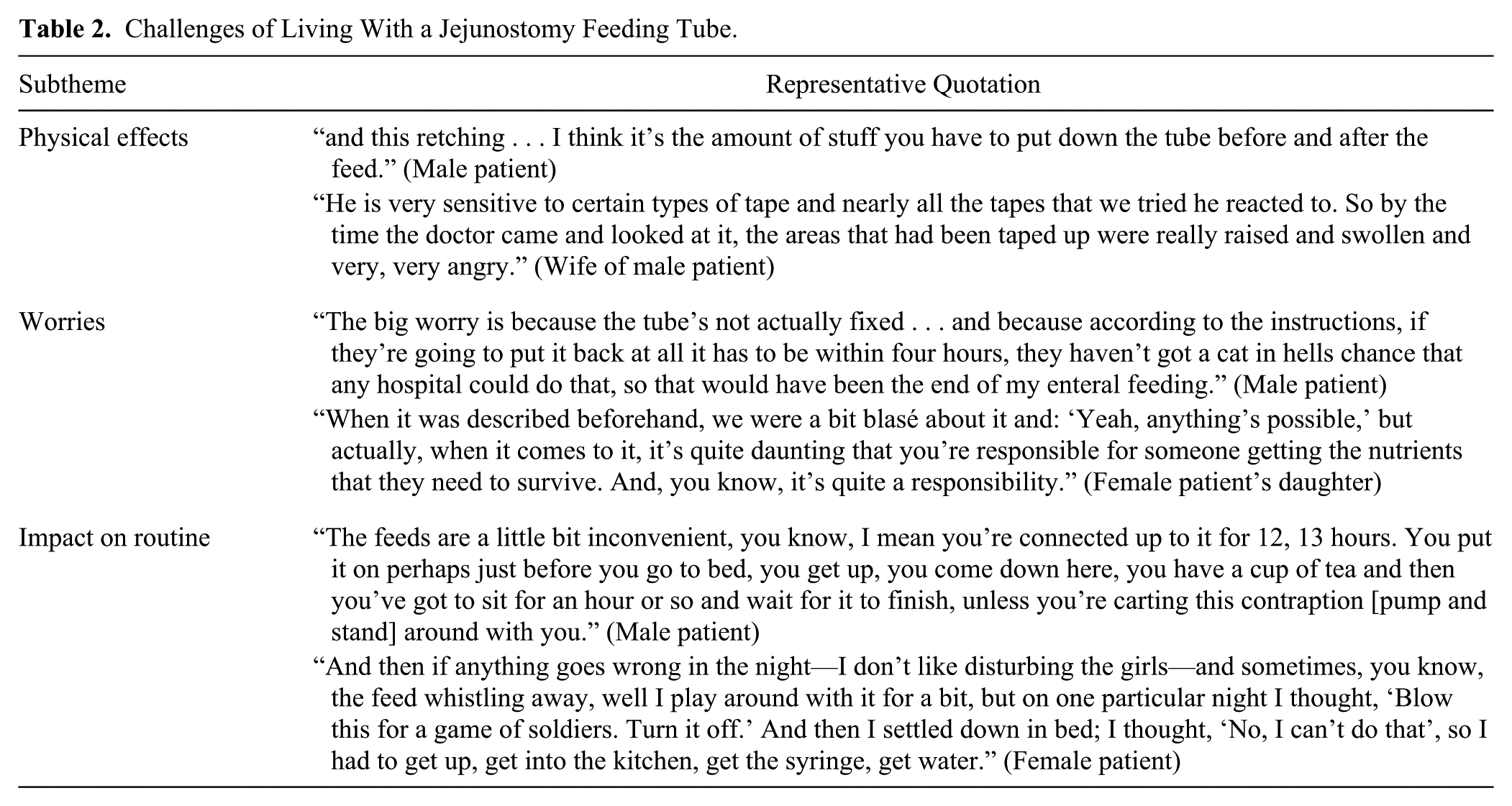
In addition to the physical effects of the JFT being in situ, patients and their caregivers expressed worry. Patients who were being fed reported being worried about the tube falling out. For some, this was more of a concern at nighttime during feeding when they would get up forgetting that they were connected to the pump. The level of worry seemed to be linked with what they had been told by the healthcare team regarding the difficulty of replacing the tube. What would happen when the feed was stopped and the JFT was removed was discussed by several participants. One man, who was worried about weight loss, described how the plan to reduce his feed, instigated by the dietitian, was making him feel “a bit anxious” and “under pressure” to eat. Interestingly, 4 of the other men were more concerned about weight regain, expressing positively how they had lost weight through their treatment. While caregivers echoed some of these concerns, overall they seemed more worried about the general well-being of the patient and the responsibility of looking after them. A wife of one of the patients described the pressure she felt to “make sure that he was getting enough food” and another of how she would wake up in the night worried that her husband might be choking.
The impact of having a JFT on daily routine was described in a number of ways. Most prominent was how having the JFT affected both the patient’s and caregiver’s sleep pattern. For some, presence of the tube, surgical wound site, and the need to sleep propped up directly affected sleeping position and comfort. In addition, for those who were fed overnight, it was common to be kept awake by the whirring noise of the pump. One woman and her daughter described in detail how, particularly in the early days postdischarge, the pump alarmed every other night, resulting in them wanting to “throw the bloody machine out the window.” Another couple explained how they set the feed up at 7 o’clock at night and had to get up at 3 o’clock every morning to disconnect it. They felt that this was the only way that the patient, who was on insulin for type 2 diabetes, could avoid episodes of hyper- and hypoglycemia. One of the other male patients had not been to bed since coming home and preferred to sleep downstairs on the sofa as he found it more comfortable. Another described getting up every hour and a half to “go to the loo.” His wife had moved into another bedroom to avoid being disturbed. In addition to problems with disturbed sleep, the general presence of the tube was described by some as “a rigmarole,” “a nuisance,” and “restrictive.” In contrast, the wife of one of the male patients described how it had not “drastically altered their life” and how it was “all part of every day what we do.”
Facilitators to Living With a JFT
Despite the challenges of living with a JFT, participants explained how consistently well they coped, describing high levels of compliance with stoma care and, where relevant, the feeding regimen (Table 3). In most cases, participants talked about the experience of coming home with a feeding tube being “difficult” but how this was something that they had been able to overcome. Some “got used to it” (eg, the noise of the machine), while others found their own ways of adapting to the challenges. The daughter of one of the female patients described how the “tube was becoming part” of her mother. The same woman went on to describe how a clothes peg (clothes pin) on her pajama top had been used to keep the tube in place overnight and how extra padding had been placed around the JFT to stop it digging in.
Facilitators to Living With a Jejunostomy Feeding Tube.
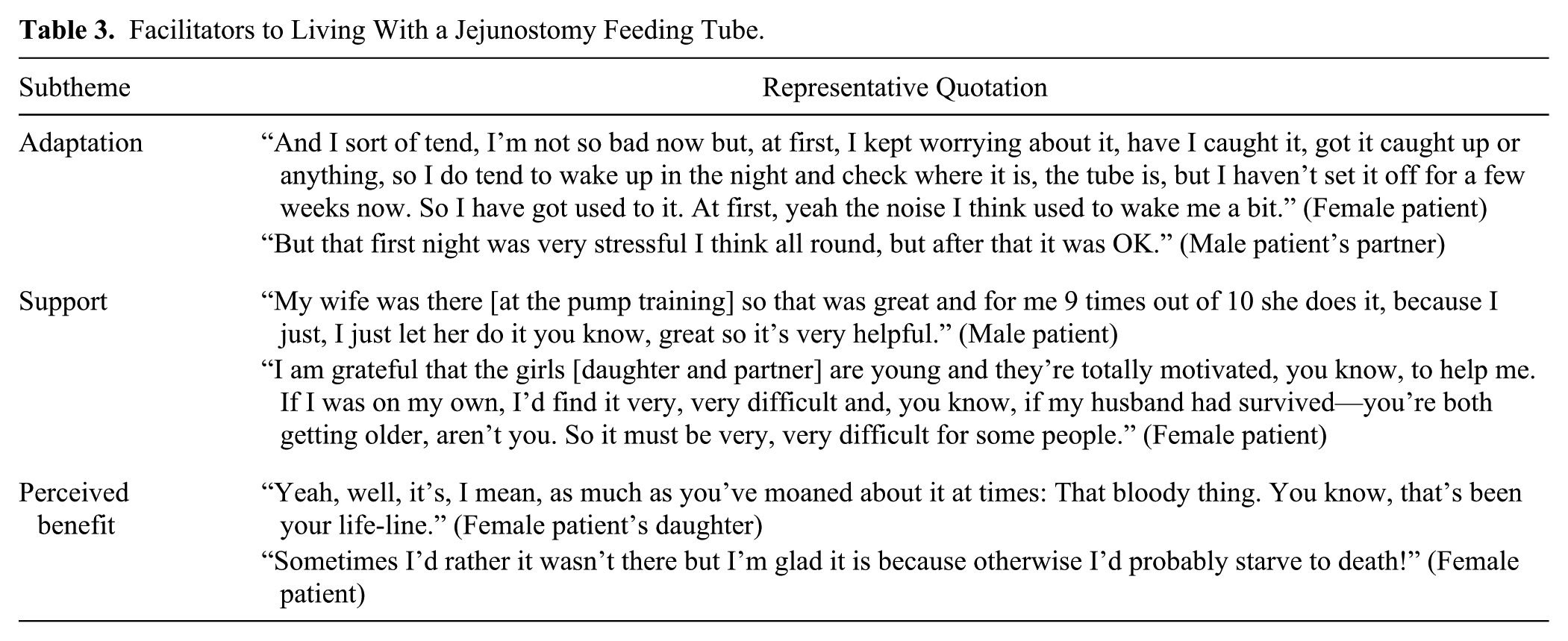
Sources of support included primarily the wives of male participants who, in some cases, took over much of the day-to-day care. Other couples spoke about sharing the tasks and “doing it between us.” Where patients lived alone, sons or daughters were in most cases a great source of support. Indeed, for one woman, her daughter and partner had moved in to help care for her. Interestingly, a number of those who had informal care from loved ones commented on how difficult it would be for others who lived alone to cope with the JFT. One of the single men thought that it would have been made easier if he was married and had a wife to look after him.
Participants talked positively about the level of support that they received from the hospital healthcare team. Most spoke about how much the practical support that the home enteral feeding (HEF) dietitian had provided, particularly around stoma and tube care, was appreciated. One couple voiced their surprise that a dietitian knew about JFTs as well as food. Most described how accessible the HEF team was. In contrast, one of the male participants expressed concern over the lack of support from Friday to Sunday. Likewise, the support from primary care providers was not always seen in such a positive light. The experiences of one couple led them to believe that primary care physicians “weren’t really aware of jejs [JFTs] too much.” Another 2 patients had experienced problems getting an appointment. As local telephone calls in the United Kingdom are charged, phoning the clinic was deemed expensive and “getting past the women on reception” difficult. Training prior to discharge and support from the commercial enteral feeding company were spoken about positively, particularly by one of the female participants who had run into problems with setting up the feed at a weekend.
Both patients and caregivers voiced their perceived benefits of having the tube and feed. For those who had been fed through the JFT, there was an overwhelming sense that the feed had “done them good.” A wife of one of the patients spoke about the feed “making him stronger” and speeding up his recovery time. Another discussed about how the feed had helped the wound to heal quicker. The feed was described as “a Godsend” and a “life-line.” Having the tube was seen as “a backup if you needed it” by one of the women who did not receive feed. In contrast, one of the men thought “it’s daft it being there” and “just useless.” Overall, the male patients spoke more about how the tube motivated them to eat. This was in both the context of “pigheadedness” not wanting to have to use the JFT and also so that it could be removed as quickly possible. These thoughts were both linked to a yearning to “get back to what’s normal” as quickly as possible.
Discussion
The findings from this study suggest that during the first 4 months when patients are recovering from major surgery, having a JFT inserted brings with it additional challenges. Stoma site complications, disrupted sleep patterns, and associated worry contributed to this and occurred, to some extent, in all patients regardless of whether they used the JFT for feeding. Despite feelings of wishing the tube was not there, patients and their family caregivers quickly adapted, becoming experts in tube care and feeding. This, along with their understanding of the benefits of having the JFT and support from healthcare professionals, resulted in an unquestioned level of compliance with care of the JFT and feeding regimen and ultimately a sentiment of positivity around the treatment. The underlying motivation for all involved was an urgency to “get back to normal.”
This is the first study to include a homogeneous population of patients who had a JFT placed after surgery for esophagogastric cancer. Placement of feeding tubes, as a short-term adjunct to treatment, is relatively common in patients diagnosed with upper GI cancer, the aim being to provide support until nutrition requirements can be met orally. Findings from this study provide an original exploration of how patients and their family caregivers experience living with a feeding tube for the first few weeks following discharge from hospital. The timing of the interviews, along with the temporary nature of the JFT placement, may account for some of the differences in findings compared to the existing literature. In addition, other studies have focused predominantly on the experiences of people with gastrostomy tubes, which, although similar in essence, in many cases were placed as a long-term and sometimes permanent intervention. In this study, social concerns reported by others, 13 related to going on holiday or finding a place to feed when away from the home, were not raised. Most participants, up to the point of being interviewed, were more concerned with recovering from major surgery and had not felt well enough to resume their usual social life. In addition, all patients in this study had been on an overnight jejunostomy feed; hence, feeding during the day was not necessary. Despite the difference in type of feeding tube that has previously been reported in the literature, there are clear similarities with the narratives of the participants interviewed in this study. Survey 11 and qualitative data 13 collected from those with gastrostomies have identified commonly occurring minor complications, including stoma site discharge, soreness, GI upset, and disturbed sleep. These types of side effects were also spoken about by patients with a JFT. What has not been identified previously is the problem that suturing of the tube’s external retention device to the surface of the abdomen has in terms of discomfort and infection. The difficulties that patients and their caregivers experience in obtaining ancillary items such as the right tape should also be noted.
The existing evidence base highlights the need for better training and information for patients and their caregivers both in terms of HEF and other healthcare technologies.15,19,24 In contrast, in this study, training about how to care for the JFT and set up the feeding pump was spoken about positively, with participants identifying how quickly they became familiar with the routine. No comments were made about requiring further or better information and training. As part of routine practice, all patients in this study were trained by a registered dietitian before discharge from the hospital, with detailed written information and a 24/7 support line from the homecare company provided. Findings suggest that this is an effective way of ensuring patients and their caregivers can cope with the practical tasks associated with having a JFT at home. Furthermore, the expertise of the HEF specialist dietitian who provided ongoing support to these patients was greatly appreciated and spoken about favorably. Other findings concur with previous work16,25 and suggest that patients do not always have confidence that their primary care practitioner has the expected and required knowledge related to JFTs.
In this study, both patients and caregivers questioned how those living alone could possibly cope with a JFT, giving us some idea of the level of importance that they perceived that this role had. As documented by others,19,21 this came at a cost. Practically, this was in terms of the time taken to provide caring duties. In this study, the emotional burden was wrapped up with feelings of anxiety associated with the level of responsibility felt by the caregiver. Despite these reservations, those living alone coped admirably with having the JFT. Arguably, this was done by drawing more on the community support, including district nursing services and the HEF dietitian.
As identified above, this study differed from others as it focused on the experiences of patients and their informal caregivers in the time period immediately postdischarge from the hospital and before the JFT had become part of “normal life.” Unlike cases of feeding tubes being placed in patients with degenerative neurological conditions, the population in the current study had a realistic hope that their oral intake would improve and that they would “get back to normal.” For them, this was a strong motivation to persevere, with the imminent removal of the tube a sign of progress and the next step to being well again.
Strengths and Limitations
The qualitative methodological approach used in this study, alongside the use of dyadic interviews, resulted in the collection of rich data and a deep understanding of the experiences of patients and their family caregivers. The qualitative nature of the work does mean that the study findings are not generalizable across all people who have had a JFT placed, and although the sample is considered representative of patients who undergo surgery for esophagogastric cancer in the United Kingdom, we were unable to identify any male informal caregivers to interview. Their views and roles as caregivers therefore remain unexplored. It should be considered that the patients who were interviewed were also recruited into an RCT. Being part of this study meant that the patients had received additional visits from the research team. How this influenced their experiences with regard to their JFT is not known. Furthermore, although this study focused on the first few months postdischarge, participants were recruited over a 2-month time frame. This may have had some bearing on what they reported.
It was the intention that conducting dyadic interviews would allow us to gain a deeper insight into the shared experiences of both the patient and their family caregiver. During these interviews, there were examples of where this happened. In particular, the presence of a wife or partner resulted in a discussion that included a much greater level of detail, particularly around the emotional aspects of the experience. Whether the presence of a loved one restricted what was discussed is also possible.
Finally, it is important to acknowledge how the previous clinical experience of the research team, which included 2 dietitians, had the potential to influence the data collection, analysis, and interpretation. In an attempt to encourage participants to be honest, rather than inadvertently reporting what they thought we wanted to hear, the profession of the interviewer was not disclosed. While every attempt was made during the analysis to ensure that what had been said was fully understood, participant validation could have further strengthened study validity.
Recommendations for Practice
If JFTs are to be placed as a short-term adjunct to treatment, understanding the implications of this intervention for both patients and their caregivers is paramount. In addition to the practical aspects, such as care of the tube and stoma site, and training on the feeding system, hospital and community healthcare professionals also need to address the associated sense and burden of responsibility that caregivers experience. Findings from this study suggest that by having a specialist HEF dietetic service that is involved in the training and support of patients, the caregivers, working alongside a commercial homecare company, can address this need. There remains a wider issue of access to community-based practitioners who are confident and knowledgeable about HEF.
What was striking about the findings from this study was how accepting and “matter of fact” participants were when talking about the problems that they experienced. In clinical practice, during routine follow-up, conversations need to identify side effects, including cases where the JFT and/or feed are affecting sleep. Use of an adapted “impact of living with a percutaneous endoscopic gastrostomy” questionnaire 13 could be one approach to this. Importantly, flexible individualized approaches to feeding regimens such as intermittent feeding, rather than overnight feeding for all, should be considered. This needs to be balanced with maximizing appetite during the day to encourage oral intake and not affecting daily routine. With jejunal feeding, this is further complicated by potential limitations on what might be tolerated in terms of rate and volume. Finally, considering the extent of the problems that the stitches caused, how these tubes are anchored in place needs to be evaluated.
Conclusion
The experiences of patients and their family caregivers suggest that placement of a JFT as an adjunct to surgical treatment for esophagogastric cancer is deemed acceptable and worthwhile. It is, however, not without consequence, as disturbed sleep patterns and stoma site–related problems prove troublesome. A better understanding of these practical challenges and worry associated with living with a JFT, from the patient and family caregiver perspective, should help healthcare teams provide proactive support to avoid preventable problems.
Footnotes
Acknowledgements
The authors acknowledge with gratitude the experiences shared by the patients and their family caregivers. Thanks also go to the Leicestershire Partnership NHS Trust Home Enteral Nutrition Service for the support that they provided to the research team and study participants.
Financial disclosure:
This article presents independent research funded by the United Kingdom National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (grant reference number PBPG-0610-22480). The views expressed are those of the authors and not necessarily those of the United Kingdom National Health Service, the NIHR, or the United Kingdom Department of Health. Support for consumables (tube feeds, pumps, and ancillaries) for this trial was provided by Nutricia. This study was supported by the University of Leicester Clinical Trials Unit.
Conflicts of interest:
Dr Bowrey and Professor Thomas have received departmental research grant support from Fresenius-Kabi for work unrelated to this study.
This article originally appeared online on August 28, 2015.
Statement of Authorship
V. Halliday, M. Baker, A. L. Thomas, and D. Bowrey all contributed to the conception and design of the research; V. Halliday and M. Baker contributed to acquisition of the data; V. Halliday, M. Baker, A. L. Thomas, and D. Bowrey all contributed to analysis and interpretation of the data. All authors drafted the manuscript, critically revised the manuscript, agree to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.