
Abstract
Veterinary use of radiation in the diagnosis, management, and treatment of disease has expanded and diversified, as have the corresponding radiological protection concerns. Radiological exposure of personnel involved in veterinary procedures and, where applicable, members of the public providing assistance (e.g. owners or handlers) has always been included within the system of radiological protection. Veterinary practice is now addressed explicitly as the modern complexities associated with this practice warrant dedicated consideration, and there is a need to clarify and strengthen the application of radiological protection principles in this area. The Commission recommends that the system of radiological protection should be applied in veterinary practice principally for the protection of humans, but with explicit attention to the protection of exposed animals. Additionally, consideration should be given to the risk of potential contamination of the environment associated with applications of nuclear medicine in veterinary practice. This publication focuses primarily on justification and optimisation in veterinary practice, and sets the scene for more detailed guidance to follow in future Recommendations. It is intended for a wide-ranging audience, including radiological protection professionals, veterinary staff, students, education and training providers, and members of the public, as an introduction to radiological protection in veterinary practice.
© 2022 ICRP. Published by SAGE.
MAIN POINTS
The objective of this publication is to provide an initial set of relevant observations, considerations, and general recommendations related to radiological protection in veterinary practice, intended for a wide-ranging audience. Radiological protection challenges specific to veterinary practice arise from the different combinations of personnel and members of the public who may be involved, and from operational environments required when dealing with animals. The priority of radiological protection in veterinary practice is that of the humans involved, but the exposure of animals should also be the object of explicit attention because, like humans, animals are subject to potential tissue reactions or stochastic effects resulting from exposure to radiation. In veterinary practice, the core and procedural ethical values of the system of radiological protection are elaborated on with discussion of additional interpretations of these values, including animal welfare, sustainable development, solidarity, reverence for life, stewardship, respect for autonomy, and empathy. Veterinary applications of ionising radiation, and their ensuing protection challenges, are, to a large extent, comparable to situations in human medical applications, and could benefit from similar approaches, such as the three levels of justification, and optimisation as a process to ensure that the likelihood and magnitude of exposures and the number of individuals exposed are reasonable and appropriate for the situation at hand, considering economic, societal, and environmental factors.
1. WHY THIS PUBLICATION?
(1) Why this publication on radiological protection in veterinary practice? Modern medical imaging techniques often have a pivotal role to play in the diagnosis of injury and disease in animals, and have therefore become an essential tool in the provision of high-quality veterinary care. The same holds true in providing the best possible advice to owners, breeders, or potential purchasers on the suitability of an animal for a specific purpose. On the treatment side, different radiotherapeutic modalities, including nuclear medicine techniques, are now increasingly available and will contribute to providing the quality of care that owners want for their animals. (2) Factors such as the digitalisation of radiology, high availability of second-hand equipment from human medicine, and manufacturing of dedicated veterinary equipment have made radiological procedures more widely attainable. Under the rising pressure of public demand, the number of radiological procedures has therefore increased substantially in recent years. (3) Although this evolution can be applauded from the veterinary services side, practitioners need to be aware of the radiation risks present. Digitalisation of imaging does not just increase the mean number of procedures, but may also increase the mean number of views per procedure, resulting in an increase in radiation dose per procedure for both the animal being examined or treated and the humans involved in undertaking the procedure. Practitioners need to be aware that the radiation dose from a computed tomography (CT) scan, a nuclear medicine diagnostic procedure, or a fluoroscopically guided intervention can be substantially higher compared with that encountered in general radiography procedures (NCRP, 2009). (4) Radiological risks have increased in veterinary practice as a result of these evolutions, and they can affect both the animals examined or treated as well as the humans assisting in these procedures – professionals and owners alike. When working with radioactive materials in applications such as nuclear medicine, persons who are not actually present during the procedures could also be exposed or become radioactively contaminated, as could the environment, for example as a consequence of inadequate management of waste (i.e. urine, faeces) passed by an animal following a nuclear medicine procedure. (5) The objective of the current publication is not to discourage veterinarians or animal owners from the beneficial uses of ionising radiation in veterinary practice. Far from it, the benefits of radiological techniques in veterinary practice are more than convincing; such techniques enable the provision of the best possible animal care, as well as solid advice to owners, breeders, and purchasers. The Commission recommends the inclusion of radiological protection considerations in veterinary clinical practice, so that procedures can be performed safely from that perspective. (6) The implementation of radiological protection measures does not need to be overly complex or difficult. Although some of the terminology may be unfamiliar at first, such measures are consistent with other approaches to workplace and patient safety. The approach to radiation protection is completely in line with what can be expected from other aspects of day-to-day quality veterinary services. The first principle of radiation protection for instance, ‘justification’, transposes the ‘primum non nocere’ or ‘first do not harm’ concept of the Hippocratic Oath; it tells us to perform only those radiological procedures that are appropriate in the context at hand, and to refrain from superfluous procedures. The second principle, ‘optimisation’, tells us to adapt the procedural settings in such a way that the diagnostic or therapeutic objective is met while optimising protection and safety, resulting in a radiation dose to the animal itself and the humans involved which is as low as reasonably achievable; just as one would adapt the dose of a pharmaceutical product to an animal’s weight. In standard radiology for instance, limiting the exposure zone strictly to the region of clinical interest leads to better image quality with a lower dose. In interventional procedures, as well as restricting the radiation beam to the region of interest, the skilful use of pulsed fluoroscopy mode can make a tremendous difference. (7) However, unfortunately, working correctly and safely with complex techniques and advanced equipment is not always that simple. For such applications, particularly therapeutic applications, additional – and continued – education and training efforts are undoubtedly required. (8) Finally, the constant and safe provision of quality diagnostic and therapeutic services when using ionising radiation demands that radiation protection considerations are integrated in the quality management of the undertaking, be it a small one-person private practice or a large veterinary hospital. This quality system should oversee the facility and its dedicated rooms; equipment and quality control; qualifications of staff and ongoing education and training; procedural rules; records, which should include dose indicators; incident and accident management, etc.
2. INTRODUCTION
2.1. Objective
(9) Veterinary practice has changed considerably over the last few decades, and along with it, applications using ionising radiation have increased in type and variety (McEntee, 2004; Farrelly and McEntee, 2014; Pentreath et al., 2020). More specifically, such applications have diversified greatly and now comprise interventional radiology and CT scanning, nuclear medicine applications including unsealed source therapy, and mixed modality imaging, as well as brachy- and teletherapy (Johnson, 2013; LaRue and Custis, 2014; Kent et al., 2018; Scansen and Drees, 2020) with a wide variety of animals beyond cats, dogs, and horses being treated (e.g. Adkesson and Ivančić, 2019; Schilliger et al., 2020). Historically, radiological protection and its application in veterinary practice have not received the same level of dedicated attention as other areas. However, with the aforementioned advances in technology and the availability of said technology, there is a need to describe the radiological protection challenges in veterinary practice more fully, together with how these challenges can be managed by application of the International Commission on Radiological Protection’s (ICRP) framework. This publication seeks to do just that, and is intended for a wide-ranging audience, including radiological protection professionals, veterinary staff, students, education and training providers, and interested members of the public, as an introduction to the issues surrounding radiological protection in veterinary practice.
2.2. Scope and context
(10) Radiological protection in the field of human medicine has been the subject of many ICRP publications, both at a general level (ICRP, 2007b) and in relation to specific aspects (e.g. ICRP,
2000, 2013a,b, 2014c, 2017a, 2018b). These publications may provide inspiration for developing specific guidance and advice that can be applied in veterinary practice, keeping in mind that although veterinary practice has many similarities to human medicine in terms of radiological protection considerations, it also has many differences. Both practices involve the need to protect professional workers, plus the need to protect the general public and the environment, and of course to protect the patient. However, in the case of veterinary practice, the patient is an animal. (11) The protection of humans in veterinary practice raises a number of challenges because of the different combinations of personnel involved, and the different operational environments required when dealing with animals. The exposure of animals also raises specific issues, as individual animals have not been considered previously within the context of the system of radiological protection. (12) Following on from the latest extension of the Commission’s mandate beyond that of the protection of humans to one that encompasses the protection of non-human species (i.e. biota) in an environmental context (ICRP, 2003b), the Commission has now determined, through detailed consideration of protection of the animal in many aspects of veterinary practice and based on a report from a task group set up to examine the issue, that it is both appropriate and timely to include consideration of exposed animals in its Recommendations (Pentreath et al., 2020). The first step, as set out in the current publication, is that of considering how this subject may be accommodated within the existing overall framework of radiological protection. (13) The Commission has always acknowledged that its guidance with regard to all medical practices has necessarily been somewhat different from that relating to other categories of radiation exposure. Thus, for example, human patients are exceptions from the principle of the application of dose limits because generic dose limits might reduce the effectiveness of the diagnosis or treatment, thereby doing more harm than good. Emphasis is therefore placed on the justification of the procedures in the first place, on the optimisation of protection in relation to the source, and, for diagnostic procedures, on the use of diagnostic reference levels (DRLs). Even the justification principle in the radiological protection of human patients is somewhat different from other human exposure situations in that, generally, both the benefits and risks relate uniquely to the same person (although other aspects may apply – such as doses to medical staff). Also, any specific method or procedure that can be regarded as justified in general does not necessarily imply that its application to a specific patient is fully justified in itself (ICRP, 2007b). (14) In the case of veterinary practice, fundamental issues also arise with regard to the principles of justification and optimisation, and these inevitably spill over into morals and ethics relating to the health and well-being of the exposed animal. This publication therefore dwells upon these topics – ethics, justification, and optimisation in veterinary practice – at some length, and sets the scene for more detailed guidance to follow in the future.
2.3. Background and motivation
(15) After Röntgen’s discovery of x rays, veterinarians were among the first to perceive the potential benefits of radiology for animal health care (Beamer, 1939; Schnelle, 1968; Kealy, 2002). In January 1896, post-mortem animal radiographs [fish, frogs, a snake, a lizard, a rabbit, a chameleon (Fig. 2.1, left), and a rat (Fig. 2.1, right)] were published, with the first veterinary radiograph of an equine foot published in March of the same year (Eder and Valenta, 1896; Johnson, 2013). Diagnostic radiography (or ‘roentgenology’) was widely used by military medical departments by World War I, including in veterinary medicine (Fig. 2.2). (16) Starting with the rise of small animal practice in the 1930s, plain film radiography (Fig. 2.3) was virtually the only veterinary application of ionising radiation for many decades. Moreover, the number of procedures was limited and the doses to human bystanders were low to trivial, provided that some simple rules were followed (Wantz and Frick, 1937). Consequently, veterinary use of ionising radiation was not a high priority for veterinarians or radiological protection professionals (Wood et al., 1974), although there were some relevant publications that provided guidance or otherwise stressed the importance of radiological protection in veterinary practice (NCRP, 1970; NHMRC,
1982
,
1984; NEB, 1989). Even just over 15 years ago, the prevalence of veterinary radiology was acknowledged to be low (NCRP, 2004). However, since then, veterinary procedures making use of ionising radiation have increased substantially and are now as diverse as in human health care, although not necessarily universally available (Johnson, 2013; LaRue and Custis, 2014). (17) Veterinary diagnostic radiology has become more popular for a number of reasons, including digitalisation and the wider availability of sophisticated applications such as CT scanning and cone beam CT scanning throughout the world (McEvoy, 2015). Digitalisation, which enables images to be processed, stored, and shared electronically, has made radiologic imaging much more convenient compared with traditional film-screen radiography. Images can be viewed immediately, and digital detectors enable images to be interpretable over a wide range of exposure parameters. Although this feature diminishes the need for retakes, the ease of the digital imaging process often leads to an increase in the mean number of exposures per study. At the same time, there will be a tendency to choose exposure parameters at the high end of what is compatible with interpretable images, often referred to as ‘exposure creep’ (Gibson and Davidson, 2012). Both these tendencies will result in higher doses to the animal and to all human bystanders. Interventional radiology procedures have entered the practice field, as have nuclear medicine applications, both diagnostic and therapeutic. Lastly, brachytherapy and external beam radiotherapy have become available in multiple centres around the world, although there are large differences in local availability. (18) Although there is currently no centralised global database describing veterinary facilities with specific radiological services offered, at the time of writing, the American College of Veterinary Radiology’s ‘Find a Specialist’ database
1
indicates the type of services offered (and number of specialists) as CT (n = 412), fluoroscopy (n = 243), interventional radiology (n = 98), nuclear scintigraphy (n = 123), radiation therapy (n = 140), radioiodine therapy (n = 101), and radiology (n = 486). The European Board of Veterinary Specialisation lists
2
308 specialists certified in veterinary diagnostic imaging, with 11 additional specialists certified in veterinary diagnostic imaging and radiation oncology. (19) Radiation-related risks have also expanded because of these important practice changes. For example, in addition to the external exposure associated with nuclear medicine procedures, relevant veterinary clinics need to consider the risk of contamination by radioactive substances to staff, owners, handlers, and the environment. Lessons learned from human medicine inform us that radiation exposure of veterinary staff involved in interventional procedures also needs to be monitored closely as doses could be significant (e.g. Klein et al., 2009; Duran et al., 2013; Ko et al., 2018), as could the doses to the animal patients themselves (e.g. Wagner, 2007; Balter and Miller, 2014; Arkans et al., 2017). Here, ‘animal patient’ refers to an animal receiving veterinary medical care or assessment. Unique issues associated with animal patients may result in higher occupational doses associated with certain procedures. For example, it has been shown that veterinary positron emission tomography (PET) procedures often result in higher doses to staff than comparative PET procedures with human patients. This increase in dose is associated with the need for additional care associated with animal anaesthesia, which is necessary in a number of radiological procedures to ease patient handling and positioning, and to reduce motion artefacts (Martinez et al., 2012). (20) Societal changes also play a role in the increasing number and diversity of procedures performed on animals. Many companion animals are considered by their owners as ‘part of the family’ (Walsh, 2009; Shir-Vertesh, 2012; Bouma et al., 2021) and therefore entitled to the best care available. The same may hold true for working animals, endangered species, and exotic and sports animals, and also when the monetary value of an animal may further stimulate owner interest in their animal’s welfare. More and more owners are ensuring that their animals are covered by specific health insurance (NAPHIA, 2020), which may require radiological examinations as part of insurability checks, and also removes financial barriers that would otherwise restrict the use of these more expensive imaging or treatment options (Kipperman et al., 2017). In addition, the imaging of animals now has a prominent place in a wide variety of suitability checks, such as suitability for breeding or for a career in sports. These procedures, which may not primarily be performed for the benefit of the animal exposed, can become a radiological protection challenge in terms of the high number of exposures, and the fact that a limited number of staff and other assisting persons may be involved. (21) The impact of these changes in veterinary practice on radiological protection needs and challenges have not gone unnoticed, and some authorities and organisations have produced guidance accordingly. For example, the National Council on Radiation Protection and Measurements revised the relevant 1970 report in 2004, and succinctly summarised the goal of radiological protection in veterinary practice (NCRP, 2004): The reasons for using radiation in veterinary medicine are to either obtain optimum diagnostic information or to achieve a specific therapeutic effect while maintaining the radiation dose to the radiological personnel and the general public as low as reasonably achievable (the ALARA principle). Similarly, it is also important to avoid all unnecessary irradiation of the animal patient. (22) The Radiological Protection Institute of Ireland and the Australian Radiation Protection and Nuclear Safety Agency both published relevant guidance in the 2002 ‘Code of Practice for Radiation Protection in Veterinary Medicine’ and the 2009 ‘Code of Practice & Safety Guide for Radiation Protection in Veterinary Medicine’, respectively; each an update of similar reports from the 1980s (RPII, 2002; ARPANSA, 2009). More recently, the International Atomic Energy Agency (IAEA) has prepared a safety guide related to radiological protection and safety in veterinary medicine (IAEA, 2021), and various activities have been developed by a dedicated working group within the Heads of the European Radiological Protection Competent Authorities (HERCA), a voluntary organisation of Europe’s radiological protection regulatory authorities (HERCA,
2012, 2017). The British Veterinary Association has also published practical guidance for the safe use of ionising radiation in veterinary practice (BVA,
2002, 2019). (23) The Commission, now recognising that the complexities of veterinary practice warrant dedicated clarification within the system of radiological protection, has decided that there is a need to strengthen the application of its protection principles in this area (Martinez and Van Bladel, 2020). As mentioned above, the objective of the current publication is not to provide direct, practice-oriented advice, but rather to provide an initial set of relevant recommendations and considerations. The priority of radiological protection in veterinary practice is that of the humans involved in or affected by the procedures, both professionals and members of the public, although the protection of the animal patient from nuclear medicine applications should also be considered explicitly, as well as protection of the environment.
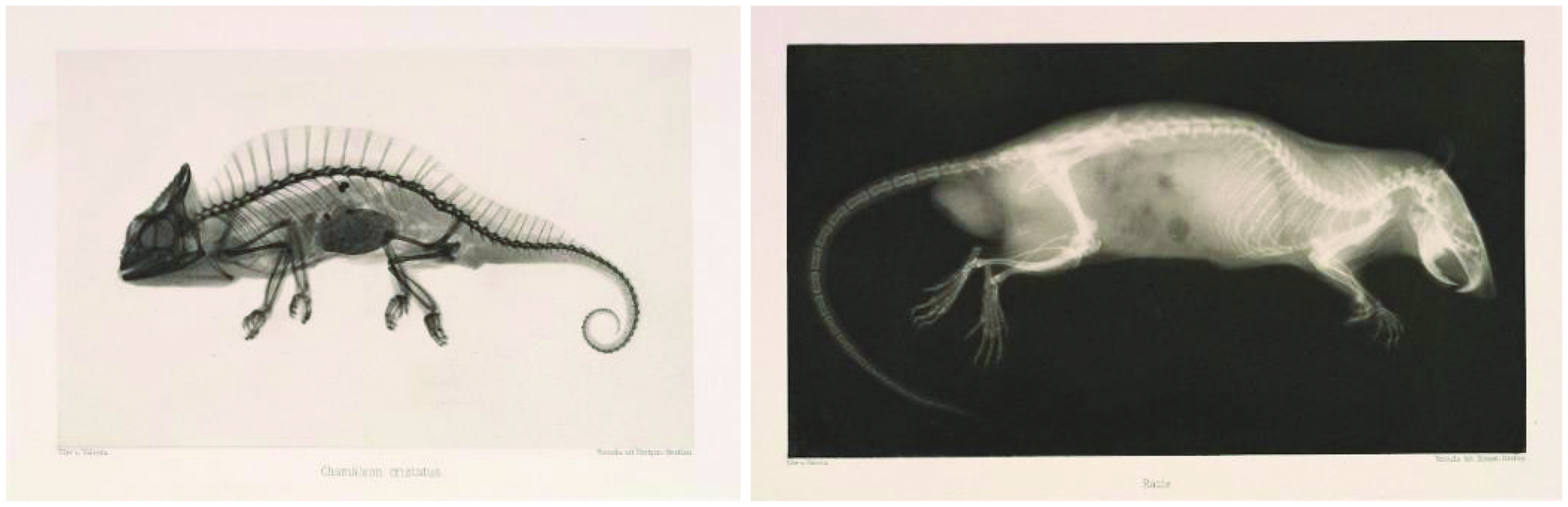
Crested chameleon (left) and rat (right). Source: Eder, J.M., Valenta, E., 1896. Versuche über Photographie mittelst der Röntgen'schen Strahlen. R. Lechner, Wien. Available at: https://www.metmuseum.org/art/collection/search/660046 (last accessed 15 August 2022).
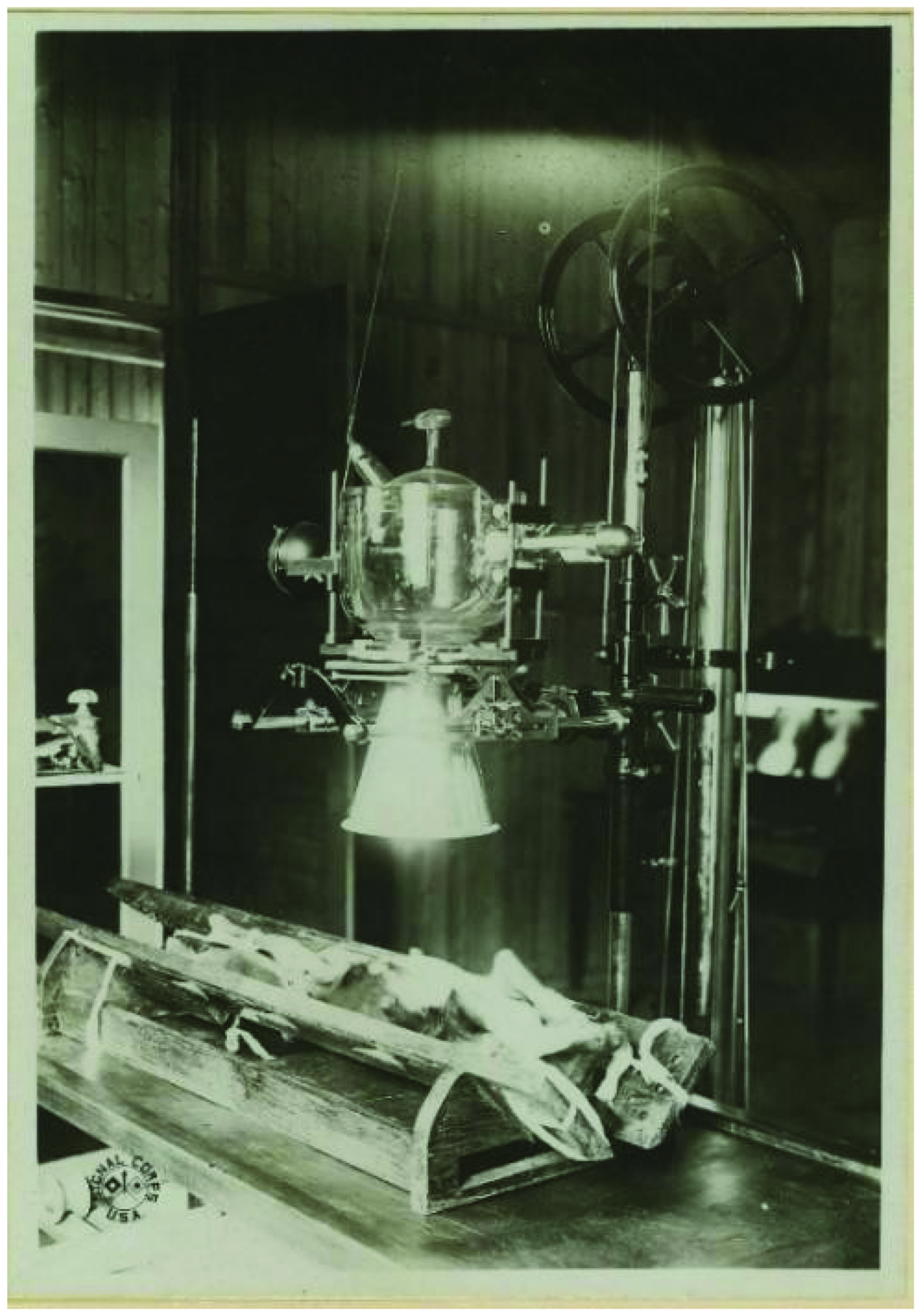
Operating upon a dog, for instruction, at Central Medical Department Laboratory, Dijon, France, 6 September 1918 (Reeve 10216). Source: OHA 80: Reeve Photograph Collection. National Museum of Health and Medicine, Silver Spring, MD, USA.
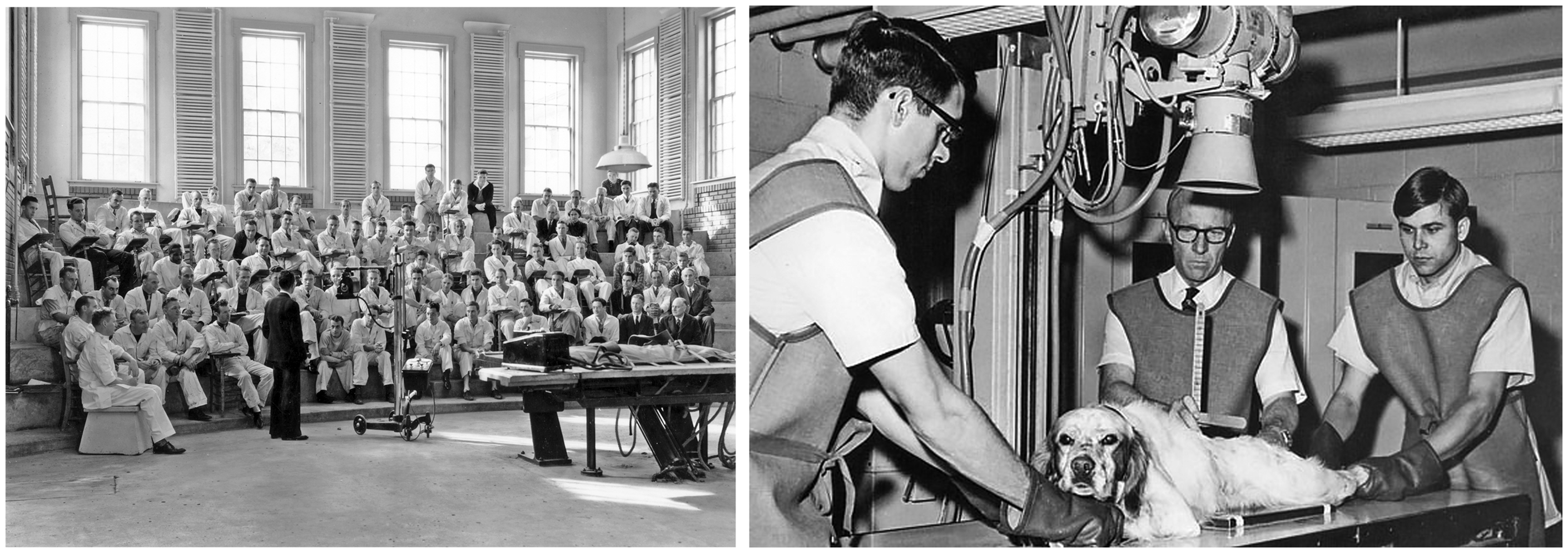
Veterinary lecture on radiography, 1936 (left) and students x raying a dog, 1969 (right), both at Kansas State University. Source: College of Veterinary Medicine, Kansas State University, Manhattan, KS, USA.
3. BASIC CONCEPTS OF RADIOLOGICAL PROTECTION
3.1. Dosimetric quantities
(24) Quantities and units used in the system of radiological protection are covered in Annex B of the 2007 Recommendations (ICRP, 2007a), as well as the online ICRP Glossary
3
. It should be pointed out, however, that most of these quantities and units have been developed exclusively for the protection of humans exposed to ionising radiation. (25) ‘Absorbed dose’ is the energy imparted by ionising radiation to a mass, per unit mass, and has units of J kg−1 with the special name gray (Gy). Absorbed dose, which is measurable, is the fundamental physical quantity used in radiological protection as it can be related to radiation effects, particularly those associated with tissue reactions. Absorbed dose is the appropriate dosimetric quantity for use in setting limits on organ/tissue doses to prevent tissue reactions (i.e. deterministic effects, see Section 3.2.1) in humans, and it is currently the only appropriate dosimetric quantity for expressing doses to animals (ICRP,
2014a, 2021a). (26) ‘Equivalent dose’ is derived from absorbed dose by accounting for biological effectiveness of the different types of radiation (e.g. alpha, beta, gamma), and generally applies to a specific human organ or tissue. Note that the Commission expects to change from the use of equivalent dose to absorbed dose in setting limits on organ/tissue doses for humans at the time that new General Recommendations are issued (ICRP, 2021a). Equivalent dose serves, then, as an intermediate step in the calculation of ‘effective dose’, which is an additionally weighted quantity that accounts for different tissue radiation sensitivities with respect to the induction of stochastic effects, and applies to the whole (human) body (ICRP, 2021a). Effective dose is a risk-adjusted quantity that enables consolidation of doses received from all radiation types and from internal and external exposures for the purpose of managing protection of humans at low to moderate doses. It is of particular use in the optimisation of protection for workers and members of the public. Effective dose may be considered as an approximate indicator of possible risk in a population of people, recognising that lifetime cancer risks vary with age at exposure, sex, and population group (Harrison et al., 2016; ICRP, 2021a). Equivalent and effective dose have the same SI units as absorbed dose, J kg−1, but are expressed using the special name ‘sievert’ (Sv). Of note, these quantities were developed using methodology and models specific to humans. (27) ‘Activity’ refers to the amount of radioactive substance present, and is typically expressed as the number of nuclear transformations (or disintegrations) per second with the unit ‘becquerel’ (Bq), which is equivalent to s−1. ‘Dose coefficient’ is a generic term that refers to a quantity which expresses dose (or dose rate) per unit intake of activity or other metric of (potential) exposure, such as particle fluence or environmental radioactivity concentration (ICRP,
2009a, 2012a, 2020a). Dose coefficients are also sometimes referred to as ‘dose conversion coefficients’ or ‘dose conversion factors’ (ICRP, 2017b). (28) As the radiation sensitivity of animals, both with respect to tissue reactions and stochastic effects, is known to differ from one species to another (e.g. von Zallinger and Tempel, 1998; ICRP, 2014a; Adam-Guillermin et al., 2018), current radiation and tissue weighting factors (and thus equivalent and effective dose) cannot be used to estimate radiation-induced risk incurred by an animal submitted to a procedure in which ionising radiation is used. It should therefore be emphasised that radiation doses for any animal can only be expressed in terms of absorbed dose (Gy). However, recommendations have recently been made for weighting absorbed dose based on reported relative biological effectiveness (RBE) of specific radiation types for (non-human) biota in an environmental context (ICRP, 2021b). Note that the Commission’s 12 Reference Animals and Plants (RAPs) for relating exposure to dose and dose to biological effect have been described at the taxonomic level of family; nine of the RAPs represent animals, two of which are large and small mammals: Cervidae (deer) and Muridae (rodent) (ICRP, 2008). RAPs are intended to be broadly representative of environmental biota. Dose coefficients for the RAPs are formulated in terms of absorbed dose rate (µGy day−1) per unit activity concentration (Bq kg−1) to which the organism is exposed (ICRP, 2017b). In the development of these dose coefficients, data on biological effects relating to external and internal sources of radiation were drawn from a wide range of relevant literature (ICRP, 2008), which, although not focused specifically on veterinary applications, does provide a useful baseline for information on radiation effects in animals. (29) Although a full suite of veterinary dose coefficients does not exist, some limited experimental research has been done in this area (e.g. Hall, 2011). In addition, a variety of computational anatomical animal models are available that are suitable for dosimetric modelling (Zaidi, 2018), including at least five for canines (Padilla et al., 2008; Kramer et al., 2012; Bell, 2015; Stabin et al., 2015), and many databases exist on the effects of radiation on mammals (e.g. Zander et al., 2019). A discussion of currently available dosimetric data in veterinary diagnostic radiology is included in Section 6.2.2.
3.2. Summary of the biological basis for radiological protection
(30) Adverse biological effects induced by radiation may be divided into two main categories: tissue reactions leading to tissue/organ damage (also called ‘deterministic effects’), and cancer and heritable diseases (also called ‘stochastic effects’) (ICRP, 2020b). These effects, in humans and animals, are summarised in brief here; the biological basis for radiological protection is covered thoroughly in Annex A of the 2007 Recommendations (ICRP, 2007a) and other ICRP publications (e.g. ICRP,
2003a, 2012b). (31) Current knowledge about the detrimental effects of radiation has been developed from a series of sources, to which experiments on animals have contributed. Animal models are frequently used to extrapolate health risk, carcinogenic or otherwise, to humans (Davidson et al., 1986; Khanna et al., 2006; Fjeld et al., 2007). For these reasons, although not specific to veterinary practice, there is a good amount of data on the effects of animal exposure to a variety of radiation types, albeit predominantly at high doses or dose rates. Although large radiobiology studies often focus on murine models, animal species of broader interest in veterinary medicine, such as canines, have also been studied (e.g. ICRP, 2008; UNSCEAR, 2010; Haley et al., 2011; Singh et al., 2015; Tang et al., 2017). Effects observed in exposed animals are of the same nature as those seen in humans, although the dose–effect relationships may be different (NRC, 1991). Exposure of animals (companion, livestock, and wild animals) to clinically significant doses of ionising radiation results in adverse biological effects, as in humans, but to a variable extent (von Zallinger and Tempel, 1998; Fesenko, 2019). Radiation effects vary by species, breed/strain (genetic susceptibility and individual radiosensitivity), sex, age at exposure, dose (cumulative) and dose rate, radiation RBE, and mode of exposure (external or internal) (e.g. Broerse et al., 1985; Hinton et al., 2007; Haley et al., 2011; Tang et al., 2017; Fesenko, 2019; ICRP, 2021b; Spatola et al., 2021).
3.2.1. Tissue reactions (deterministic effects)
(32) Tissue reactions result after exposure to high doses of radiation over a relatively short period of time, and manifest clinically when the radiation dose received is above a given threshold. These effects are seen in companion animals treated with ionising radiation for therapy (e.g. cancer treatment, pain alleviation). Although originally defined as such for humans, effects are often classified as ‘acute’ (manifesting shortly after exposure) or ‘late’ (manifesting months to years after exposure) in animals as well (Collen and Mayer, 2006; ICRP, 2012b). As in humans, as the dose increases the effect is seen with increasing frequency and severity, and specific effects depend on the tissue irradiated (e.g. LaDue and Klein, 2001). (33) In radiotherapy, high radiation doses delivered to the target tissue induce tissue reactions that ultimately prevent cancerous cells from further out-of-control multiplication. That said, effects such as skin burns and ocular effects are potential undesired effects on healthy tissues in some therapeutic procedures and cannot always be avoided (Gillette et al., 1995; Collen and Mayer, 2006; Pinard et al., 2012). Overexposure in radiotherapy, however, can result in severe tissue reactions that are very painful and can also lead to a variety of long-term complications. The specific complication will depend on the technology being used, dose fraction, total dose, and the organ(s) in the target volume. These complications can be benign to severe, and tend to be irreversible (e.g. fibrosis, necrosis, chronic inflammation) and difficult to treat, with detrimental impact on the patient’s quality of life in both animals and humans (Gillette et al., 1995; Collen and Mayer, 2006; Balter and Miller, 2014; Hall and Giaccia, 2019; Mayer et al., 2019a). An interesting (trivial) consequence of radiation exposure associated with radiotherapy can be the change in colour of an animal’s fur (leukotrichia; Fig. 3.1) (Inomata et al., 2009; Gerard et al., 2010; Mayer et al., 2019a; Lee et al., 2020). (34) In interventional procedures, lesions such as radiation-induced skin burns in the area where the primary radiation beam enters the body may appear within weeks (Balter et al., 2010), particularly when complex procedures requiring prolonged fluoroscopy times are performed on larger animals. Most of such injuries can be managed and are self-limiting, but it is important to remember that unnecessary tissue reactions result in needless suffering. (35) Although occupational doses received in veterinary practice are generally too low to observe tissue reactions, some nuclear medicine, interventional, or brachytherapy procedures, combined with poor practice, incidents, or accidents, have the potential to result in skin burns or effects on the lens of the eye based on experience in human medicine (Miller et al., 2010; Dauer, 2014; ICRP, 2018b).

A canine patient before (left) and 3 months after (right) intensity-modulated radiation therapy. In both images, the patient is being prepared for positron emission tomography imaging. Note the lightening of the fur (leukotrichia) in the area of the beam. Source: Jan Rødal, The Norwegian Radium Hospital, Oslo University Hospital, Norway (Rødal et al., 2010).
3.2.2. Stochastic effects (cancer and heritable effects)
(36) Stochastic effects are those effects for which the probability of occurrence, but not severity, is a function of dose with no apparent threshold. Ionising radiation can interact with a cell such that the cell is damaged but can continue through the cell cycle, thus potentially leading to a malignant disease. Stochastic effects resulting from exposure to ionising radiation include cancers, which can result from damage to somatic cells, and heritable effects, which can result from damage to germ cells. Of note, a wide variety of environmental contaminants as well as naturally occurring mutations in somatic and germ cells also contribute, respectively, to cancers and hereditary diseases in humans and animals (Kelsey et al., 1998; NRC, 2006; Fjeld et al., 2007). (37) For humans, although there are indications of an increase in the risk of cancer for exposed children, including after in-utero exposures (Wakeford and Bithell, 2021) at lower doses, an increase of the risk of cancer in exposed members of the public at doses below approximately 100 mSv cannot be firmly demonstrated by epidemiological surveys alone. However, when combined with a deliberately prudent interpretation of radiation physics and radiation biology data, the Commission considers a linear-non-threshold model to be the best practical approach to managing risk from radiation exposure (ICRP, 2007a). This model assumes a linear relationship between dose and stochastic risk, which means that any increase in dose may result in an increase in the stochastic risk, bearing in mind that risks are increasingly uncertain at lower doses (ICRP, 2021a). It is challenging to develop definitive risk predictions for radiogenic stochastic effects at low doses because there are a variety of factors that contribute to overall risk, as well as additional modifying factors that can influence the promotion or progression of the disease (NRC, 2006; McLean et al., 2017). The risk indicator used by the Commission for humans is the ‘radiation detriment’, which is sex- and age-averaged over a composite reference population. It is determined from the lifetime risk of cancer, and considers severity in terms of lethality, quality of life, and years of life lost. It also considers heritable effects based on information from animal studies (ICRP, 2007a; Ban et al., 2022; ICRP, 2022). (38) With respect to exposed animals, a common misconception is that an animal with a shorter life span than a human will not experience radiogenic cancer. However, it has been widely observed since the 1970s that, across species, neither increased body size nor longer life span is associated with an increase in the overall risk of cancer, as expected from the associated increase in the number of cells or cellular divisions, respectively (Abegglen et al., 2015; Vincze et al., 2022). This provided foundational insight for the modern recognition that the physiological factors influencing the responses of organisms to carcinogens are varied and complex. (39) Cancer patterns in mammals are similar and, in general, are relative to life span (Albert et al., 1994; Schiffman and Breen, 2015); in other words, ‘risk of cancer in old age is not vastly different in species with very different life-spans’ (Peto, 2016). Latency periods are less than that in humans for many animals with shorter, physiologically compressed life spans (NRC, 1991; Backer et al., 2001; Cagan et al., 2022). Of interest to veterinary practice is the observation that dogs demonstrate a comparatively greater risk of developing cancers overall (Dobson, 2013; Abegglen et al., 2015; Schiffman and Breen, 2015). For cancer prevention in dogs, it has been stated explicitly in the literature that ‘dogs should be exposed to radiation only when the expected benefits will outweigh the risks’ (Kelsey et al., 1998), consistent with the principle of justification in radiological protection. A large number of studies investigating radiation carcinogenesis (and other morbidities) in experimental animals have been conducted, and dose–response relationships vary (Broerse et al., 1985; Duport et al., 2012; Tang et al., 2017; Spatola et al., 2021). (40) Inheritance of radiation-induced abnormalities was reported by Hermann Muller in 1927 based on studies with x-ray irradiation of Drosophila (fruit flies) (Pontecorvo, 1968). Since then, ample evidence of radiogenic hereditary effects in other animals and plants has been reported (e.g. UNSCEAR, 2001; Russell, 2013). Of note, radiation exposure can only increase the incidence of the same mutations that occur spontaneously in a population (Hall and Giaccia, 2019). This makes potential heritable radiogenic effects in humans difficult to study because of the high natural incidence of the same mutations. Thus, hereditary effects in humans have not been definitively or reliably shown to be induced by ionising radiation exposure (Boice, 2020; NCRP, 2021). Humans are likely also susceptible to these effects, but with risk much lower than that for carcinogenesis (UNSCEAR,
2001, 2014). (41) In humans, the likelihood of developing cancer in response to exposure to a carcinogenic agent depends on a variety of factors including, but not limited to, age; sex; environmental, socio-economic, and lifestyle factors; and genotype (Colditz et al., 1996). Individual variability in radiosensitivity to carcinogenesis is acknowledged but not fully understood (Rajaraman et al., 2018). However, there are some clear, population-level attributes, such as age and sex, that influence susceptibility to radiation-induced carcinogenesis (NRC, 2006; Preston et al., 2007). This risk is higher overall for the fetus, children, and adolescents, due to their longer life ahead and the comparative sensitivity of developing organs and tissues (ICRP, 2013b); and for females, primarily due to the radiosensitivity of the breast (Boice et al., 1991; NRC, 2006). This age and sex dependence of risk should be considered in the process of justification and optimisation, particularly with respect to children. For example, in veterinary practice, children and young adolescents are excluded from assisting in radiological examinations as the exposure is not justified. Similarly, the potential presence of individuals who are or may be pregnant needs careful consideration with respect to justification when radiological procedures are being performed; this has to do with both the radiosensitivity of the unborn child (Section 3.2.3) and the possible sensitivity of the breast tissue in some stages of preparing for lactation (Ronckers et al., 2004). The justification process for any such exposure should bear in mind that the dose limit for the unborn child (1 mSv during pregnancy; see Table 3.1) is not to be exceeded. If the presence of a pregnant or possibly pregnant individual is deemed justified, and informed consent is given, radiological protection measures need to be optimised. This could be achieved by providing instructions on where to stand, how to behave, what protective equipment to use, etc. Strategies for optimisation are discussed further in Section 6. (42) It has been shown in laboratory animals that age at exposure and sex influence the risk of carcinogenesis, although to a varying extent (Benjamin et al., 1991; Shuryak et al., 2010; Haley et al., 2011; Tang et al., 2017). These risk dependencies are thus also relevant considerations for animal patients, as some groups receive exposures from a young age (e.g. dysplasia screening in puppies) (Dziuk, 2007) or presale examinations of performance horses (Judy, 2013). Being mindful of these risks is especially important when determining if such exposures are justified (discussed further in Section 6.2).
Summary of the dose limits* recommended in Publication 103 (ICRP, 2007a).
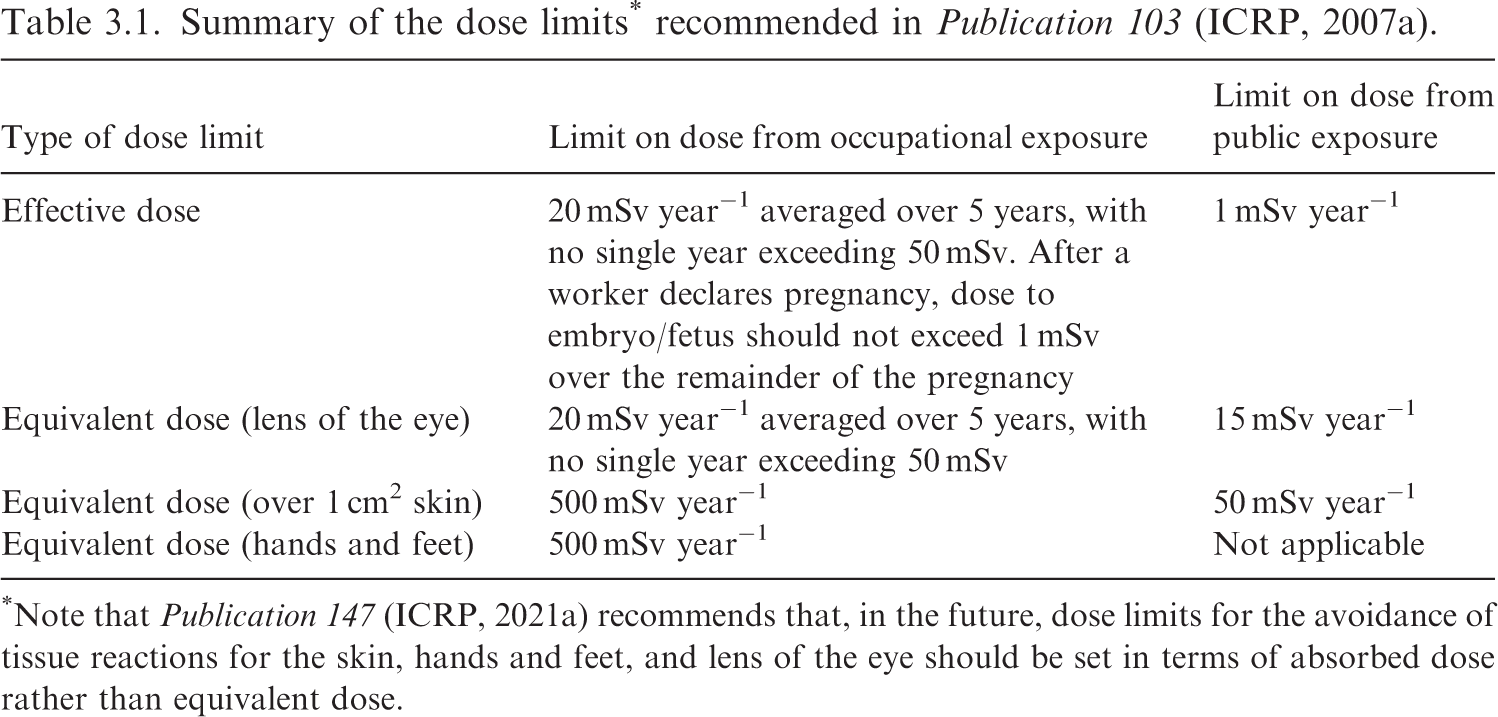
*Note that Publication 147 (ICRP, 2021a) recommends that, in the future, dose limits for the avoidance of tissue reactions for the skin, hands and feet, and lens of the eye should be set in terms of absorbed dose rather than equivalent dose.
3.2.3. Effects of in-utero exposure
(43) Radiation effects on the embryo/fetus during pregnancy (i.e. teratogenic effects) depend on the stage of pregnancy at the time of exposure, the absorbed dose to the embryo/fetus, and the type of radiation (e.g. Benjamin et al., 1998; Russell, 2013; Hall and Giaccia, 2019). At most diagnostic levels, effects in humans include risk of childhood cancer, while at doses in excess of 100–200 mGy during the most radiosensitive fetal time period, there are risks of tissue reactions including nervous system abnormalities, malformations, growth retardation, intellectual disabilities, and fetal death (ICRP,
2000, 2003a). Publication 84 (ICRP, 2000) discusses the management of pregnant patients and pregnant workers in medical facilities where ionising radiation is used. Publication 90 (ICRP, 2003a) critically evaluates and summarises the effects of prenatal irradiation, including evidence from animal studies which are particularly relevant to veterinary practice.
3.3. The Commission’s framework of radiological protection
(44) The primary aim of the system of radiological protection is to contribute to an appropriate level of protection for humans and the environment against the detrimental effects of radiation exposure without unduly limiting the desirable human actions that may be associated with such exposure (ICRP, 2007a). For humans, radiation exposures are managed with the goal of reducing stochastic effects to the extent reasonable, and preventing unnecessary tissue reactions in healthy tissues (e.g. in radiotherapy, a tissue reaction may be unavoidable in order to obtain effective treatment). It should be stressed here that the Commission’s system of protection has been developed with the primary aim to protect humans. More recently, environmental protection has also been addressed, in which the focus is on the protection of populations in the natural environment. Although, in general, population-level environmental protection is based on knowledge of the effects of radiation on representative animals and plants, little concern has been demonstrated for the possible detrimental effects for an individual animal, except for those belonging to endangered species, although it was acknowledged as early as the 1930s that attention to animal patient exposure should not be neglected (Wantz and Frick, 1937). Of note, Publication 146 (ICRP, 2020b) does include explicit consideration of pets and livestock in its discussion of emergency preparedness and response. (45) It is worth re-emphasising that the protection of humans and the environment in the context of veterinary practice is currently included in the system of radiological protection, but is addressed explicitly and elaborated upon here. As such, much of the information herein regarding radiological protection of veterinary staff and members of the public, including animal owners and handlers, and the environment, is drawn from Publications 103 and 105 (ICRP, 2007a,b). The protection of animals in the context of environmental protection addresses only the collective impact (e.g. preservation of species and maintaining biodiversity) (ICRP, 2003b). The Commission now specifies that the system includes protection of the individual animal in special circumstances. Animal patients undergoing radiological veterinary procedures comprise one case among others, including animal research subjects and pets/domestic animals in a radiological emergency [e.g. Publication 146 (ICRP, 2020b)].
3.3.1. Exposure situations and categories
(46) Different exposure situations and categories are defined within the system of radiological protection to take into consideration the specific circumstance under which an exposure occurs. The exposure situations are: planned (situations in which protection can be planned ahead of time), emergency (unexpected situations, such as accidents, that may necessitate urgent intervention), and existing (situations that already exist and may need a decision on management or control). The radiological, nuclear medicine, and radiotherapeutic procedures performed in veterinary practice discussed in this publication are considered to be planned exposure situations. (47) Three exposure categories are identified: occupational exposure (received at work as a result of situations that can reasonably be regarded as being the responsibility of the operating management), medical exposure (received as a patient/research volunteer or from a patient as a non-occupational comforter/carer), and public exposure (received apart from occupational and medical) (ICRP,
2007a, 2014b). As the Recommendations are currently written (ICRP, 2007a,b), the medical exposure category appears to apply solely to human medicine. Veterinary applications of ionising radiation are, to a very large extent, comparable to human medical exposures; in fact, the only distinction is that the exposures are aimed at animals in one case and at humans in the other. In both cases, occupational and public exposures may occur. As veterinary practice involves subjects other than humans, local governments and regulatory agencies manage exposures received in a veterinary setting in different ways. Where veterinary practice is considered – from a regulatory perspective – to be comparable with an industrial application of ionising radiation rather than a medical application, this may lead to an approach whereby the animal is considered a mere object, without consideration of its characteristics as a sentient living creature. (48) Environmental exposure (i.e. exposure to the living environment) is a fourth type of exposure, although it is not defined explicitly as an exposure category in Publication 103 (ICRP, 2007a). Thus far, ICRP has focused on the natural environment, with the goal of maintaining biological diversity, conserving species, and maintaining the health status of associated habitats, communities, and ecosystems (ICRP,
2003b, 2008, 2009c, 2014a, 2017b, 2021b), although there is ongoing discussion on potentially broadening this perspective (Clement et al., 2021).
3.3.2. Principles of protection
(49) The core of the system of radiological protection consists of three fundamental principles: justification, optimisation, and application of dose limits (ICRP, 2007a). The principle of justification (see Section 6.1) specifies that ‘any decision that alters the radiation exposure situation should do more good than harm’. The principle of optimisation of protection (see Section 6.2) specifies that ‘the likelihood of incurring exposure, the number of people exposed, and the magnitude of their individual doses should all be kept as low as reasonably achievable [ALARA], taking into account economic and societal factors’. Environmental factors have also been included explicitly in discussions of optimisation (ICRP, 2020b). Of note, in medical exposures, optimisation involves keeping patient exposures to the minimum required to achieve the desired medical objective, whether diagnostic or therapeutic (ICRP, 2013a). Justification and optimisation are source-related principles, and restrictions on dose from a particular source (e.g. dose constraints) are used to avoid severely inequitable outcomes of the optimisation process. The final principle, application of dose limits (see Section 6.3), indicates that ‘the total dose to any individual from regulated sources in planned exposure situations other than medical exposure of patients should not exceed the appropriate limits specified by the Commission’. In other words, radiation doses should not exceed appropriately established limits for workers and the public (Table 3.1). (50) Dose constraints are prospective, source-related restrictions on individual dose to workers and/or members of the public intended to serve as the upper bound of the optimisation goal for that source (Fig. 3.2). Note that dose constraints are not intended to be hard limits. Rather, consistent with the core value of justice, dose constraints are intended to serve as a mechanism for limiting potential inequity that could result from differences in value judgements when implementing the optimisation process. In fact, interpreting constraints as rigorous limits can distort the outcome of the optimisation process (ICRP, 2007a). Dose constraints are used initially within the optimisation process at the planning stage to establish an appropriate level of protection for a given situation, and develop corresponding protective actions. The numerical value taken for a dose constraint will depend on the situation at hand. (51) After the planning stage, dose constraints can uncover discrepancies between planning and implementation, or reveal potential changes that warrant additional consideration. If set properly, a dose constraint can play a role in revealing a departure from normal situations. For example, if a process or procedure is known to consistently and appropriately result in an effective dose of 0.5 mSv over 3 months, and recently that procedure resulted in 2 mSv over 3 months, a review would be conducted to discern the root cause of the increase. The increase may have been warranted, in which case no further action is necessary, or it may demonstrate a lapse in proper technique, problem with equipment, or other issues that need to be addressed. (52) The principle of optimisation of protection for human patients is unique in the system of radiological protection. In diagnostic procedures, it is the same person who gets the benefit and suffers the risk. The imposition of individual restrictions on patient dose could also be counterproductive to the medical purpose of the procedure. Source-related dose constraints for the individual are therefore not relevant, and thus DRLs for a particular procedure, which apply to groups of similar patients rather than individuals, are used. Radiation therapy is also very different from other situations in that the dose is intentional; cell killing is the purpose of the treatment. In this case, optimisation becomes an exercise in minimising doses (and/or their deleterious effects) to surrounding tissues without compromising the pre-determined and intentionally lethal dose and effect to the target volume. (53) Intuitively, these ideas could also apply to animal patients (Pentreath, 2016), although if and how these patients fit within the principle of optimisation has not been defined explicitly. Thus, management strategies are inconsistent between different countries (HERCA, 2012). In many countries, veterinary medicine is considered to be an industrial rather than a medical practice, the latter of which is considered to include human medicine alone. Unfortunately, this philosophy often neglects considerations associated with unique but necessary aspects of veterinary practice, such as safety of animal patients under sedation or anaesthesia, or situation-dependent risk management consistent with a graded approach (IAEA, 2018) (i.e. the implementation of the system of protection in a way that is proportionate to the associated risk, the complexity of the exposure situation, and the prevailing circumstances). (54) Dose limits do not apply to the patient in medical exposures so as not to interfere with necessary, medically indicated diagnostic or therapeutic procedures; generic dose limits might jeopardise the effectiveness of the diagnosis or treatment, thereby doing more harm than good. Emphasis is therefore placed on the justification of the procedures in the first place, on the optimisation of protection, and, for diagnostic procedures, on the use of DRLs, which are not seen as limits, but instead indicate if a dose received from an imaging procedure is unusually high or low to guide the optimisation process and thus help manage patient exposures (ICRP,
2007b, 2017a). The Commission recommends that a similar, proportionate approach to that applied for human medical exposures should be developed and applied for veterinary practice to include a quality dose management programme that allows for periodic audits, continuous peer learning, and use of incident reporting systems that capture incidents and near-misses [e.g. Safety in Radiation Oncology (SAFRON), Safety in Radiological Procedures (SAFRAD), Radiation Oncology Safety Education and Information System (ROSEIS)]
4
. (55) In environmental radiological protection, derived consideration reference levels (DCRLs), rather than limits, are used to inform the appropriate level of management or control of an exposure. DCRLs are absorbed dose rates above which, for a given taxonomic class, there is the potential for deleterious effects on individuals of a species that may lead to population-level consequences. DCRLs can be used as points of reference to optimise the level of effort expended on environmental protection, dependent upon the overall management objectives and the relevant exposure situation (ICRP, 2014a). As such, although relevant to animals in general, the concepts developed for radiological protection of the environment do not suffice for the adequate protection of individual animals exposed in veterinary settings. (56) Emergency and existing exposure situations utilise reference levels rather than limits, because what defines a reasonable or tolerable exposure is strongly dependent on the prevailing circumstances of the exposure in these situations. The current work on radiological protection in veterinary practice focuses on planned exposure situations, although there may potentially be veterinary concerns in the other exposure situations as well (e.g. emergency exposures following a large-scale nuclear accident).
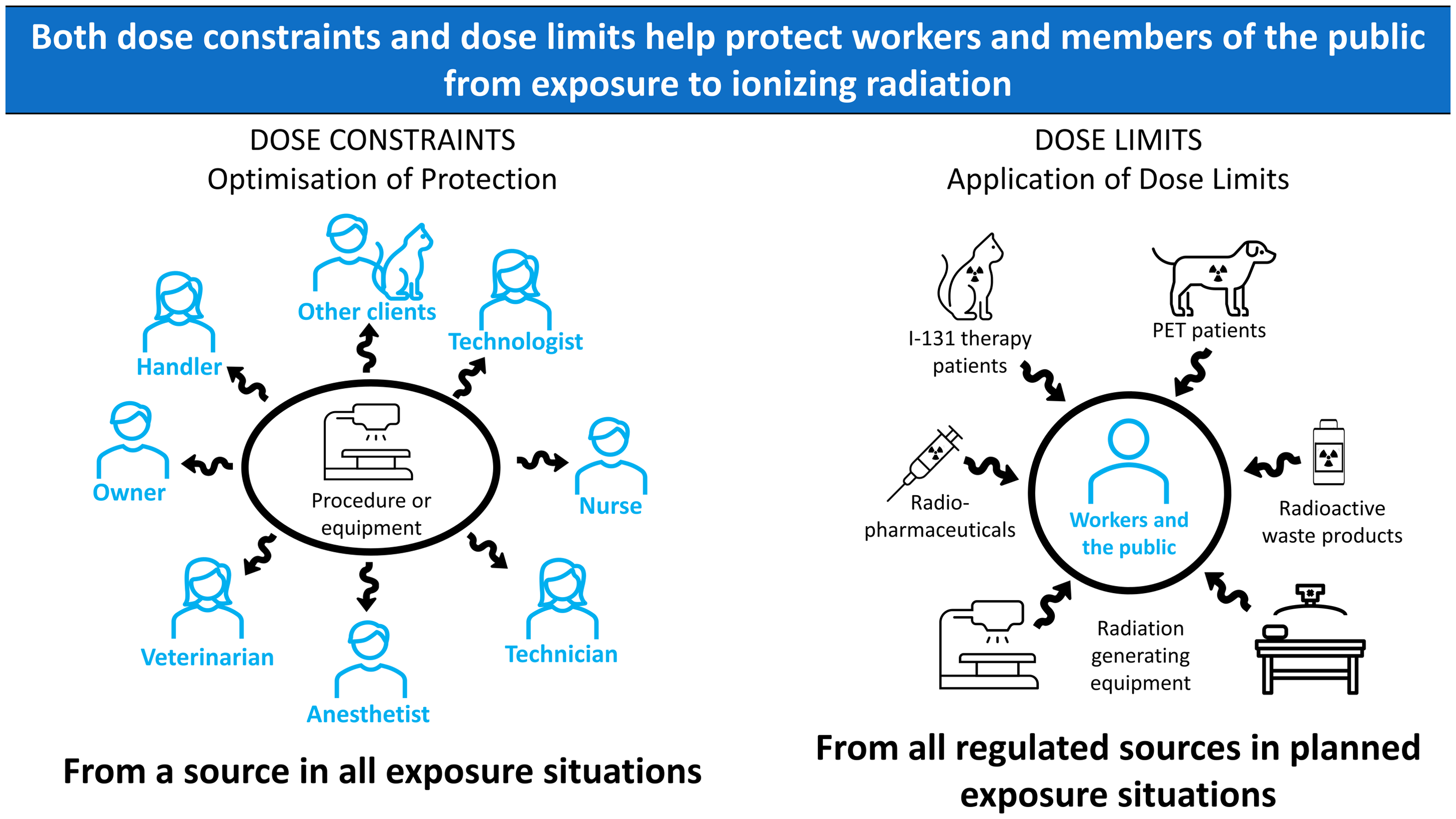
Example comparison of dose constraints (left) to dose limits (right) for protecting workers (occupational exposure) and members of the public (public exposure).
3.4. Potential pathways of exposure and practical protection strategies for veterinary staff and assisting persons
(57) Ionising radiation can be emitted from an unstable atom undergoing radioactive decay, as is the case with radiopharmaceuticals, or from the acceleration of charged particles, as is the case with radiography equipment and linear accelerators. In other words, there are two broad categories of potential sources of exposure to radiation in veterinary practice: radioactive substances and radiation generating equipment. Radiation generating equipment poses a risk of external irradiation for as long as the equipment is ‘on’. Radioactive material poses a risk of both internal and external contamination; for example, if radioiodine is spilled on to uncovered skin, the skin will be externally irradiated, and there will also be the potential for absorption through the skin into the body. Additionally, radioiodine is volatile in its elemental form, and thus is potentially an inhalation hazard as well; in general, working with gaseous, dusty, or volatile radioactive substances poses a risk of internal contamination via inhalation (see Section 3.4.2). (58) The type(s) of radiation emitted by the source will also inform the risk(s) to be considered, as different types of radiation present different exposure pathways of concern. Alpha radiation is unlikely to present an external hazard due to its low penetrating power, but becomes a concern if an alpha-emitting radionuclide (e.g. Ra-223 or other targeted alpha therapies; Gupta et al., 2017; Tafreshi et al., 2019; Rojo et al., 2021) is inhaled, ingested, or gets in the eyes. Depending on the energy, beta radiation may have a range of up to a few metres in air, and can penetrate tissue on the millimetre scale. The primary radiological protection concern for beta radiation is exposure of the skin (i.e. ‘shallow’ dose) and eyes (i.e. ‘lens’ dose). Beta-emitting radionuclides are also a concern if ingested, inhaled, or incorporated through the skin. Gamma and x rays are penetrating radiations, capable of whole-body exposure (i.e. ‘deep’ dose) as well as shallow dose and lens dose. Thus, different strategies are implemented for dose reduction depending on the specific radiation type, but there are some broad generalisations applicable to external and internal radiological protection (ICRP, 2007b; Martin, 2013; Johnson, 2017).
3.4.1. External radiological protection
(59) The three basic rules of external radiological protection are reducing exposure time, increasing distance from the source, and using appropriate shielding. These factors need to be considered together in the design of buildings and rooms for veterinary facilities, in the design of radiological equipment (including sealed and unsealed sources), and in local rules and procedures. Protection strategies will include consideration of engineering controls (e.g. shielding, interlocks), administrative controls (e.g. written procedures), and personal protective equipment (PPE, e.g. gloves, lead aprons), consistent and in conjunction with the management of other workplace hazards (de Castro, 2003). (60) Significantly limiting the duration of an exposure is not always feasible because a certain amount of time is usually required to perform a given task. However, detailed work plans with practice runs beforehand (without the source) can help to reduce overall exposure time. If practical, splitting tasks(s) between personnel or rotating through personnel can also reduce an individual’s exposure time. Another example of optimising time is the use of pulsed fluoroscopy in both fluoroscopy and interventional procedures, in combination with last image hold which can effectively reduce the time of exposure while keeping required image guidance
5
. (61) Where reasonably possible, maximising distance from a radiation source is a simple and practical principle for dose reduction. The use of handling tools (e.g. tweezers, tongs) and hand carts should be considered, along with working at arm’s length and taking one step back where feasible (Fig. 3.3). However, note that these three basic rules should be used in conjunction with each other, as it could be that using a device such as tongs could increase the time spent handling the source (at a greater distance), whereas a short, quick manoeuvre closer to the source may result in less dose. Also, consideration should be given to individuals working for long periods of time in awkward or uncomfortable positions (e.g. working behind shields, etc.), which may create an ergonomic/orthopaedic hazard with potential for fatigue-induced mistakes or, again, an increase in the time to complete the task. Where safely applicable, the use of sedation or anaesthesia may considerably reduce the time that people need to spend in close proximity to an animal; their radiation exposure would then be reduced by the combination of a shorter exposure time and a greater distance from an animal seen as a radiation source. The more fractious an animal, the more personnel will typically have to ‘lean in’ to keep it in position during imaging, and sedation/anaesthesia can make it easier to work at arm’s length or take a step back. Furthermore, sedation/anaesthesia will ease patient positioning, reducing the need for retakes, which will reduce the total exposure time for the personnel involved in restraining animals. (62) The most appropriate type of shielding to employ is dependent on the circumstance as well as the type and energy of the radiation involved. For example, the electrons (i.e. beta particles) produced in beta decay will interact with their surroundings and produce bremsstrahlung (‘braking radiation’). Bremsstrahlung refers to the photons produced when the path of a free electron is decelerated by an atomic nucleus; the more protons in a nearby nucleus, the more bremsstrahlung there will be. It is therefore better to shield beta emitters with low atomic number (Z) material (e.g. plastic or acrylic glass) as this will block the electrons while producing less bremsstrahlung than high Z material. High Z material is good at shielding photons, so lead shielding can be added on the outside of the primary container to shield the resultant photons while storing or transporting. (63) Lead is commonly used to shield gamma- and x-ray radiation; however, in practice, any dense material (e.g. tungsten, steel, concrete, etc.) can attenuate these photons sufficiently if it is thick enough. For example, some high activity sources are housed in basement facilities to make use of the natural, earthen shielding. Photon attenuation is exponential, although for broad beam or poor geometry conditions, scattered radiation can result in ‘build-up’ and an exposure higher than that predicted purely by exponential attenuation. PPE frequently employs lead (e.g. aprons, gloves) or leaded glass (e.g. eyeglasses) to protect radiosensitive organs (Mayer et al., 2018). Care should be given that use of PPE optimises protection and safety (e.g. considering level of transmission, ergonomic issues, influence on the time required to perform a task, etc.). For example, lead aprons are not appropriate for use in PET studies, as the transmission of annihilation photons (511 keV) through a typical apron is >90% (Martinez et al., 2012); the increase in work time associated with wearing an apron negates this fairly trivial reduction in exposure. (64) Shielding should start with assessment of the collective work environment (concrete walls, leaded doors and windows, standing or ceiling-suspended shields, etc.), and should be complemented with appropriate PPE worn by staff and assisting persons.
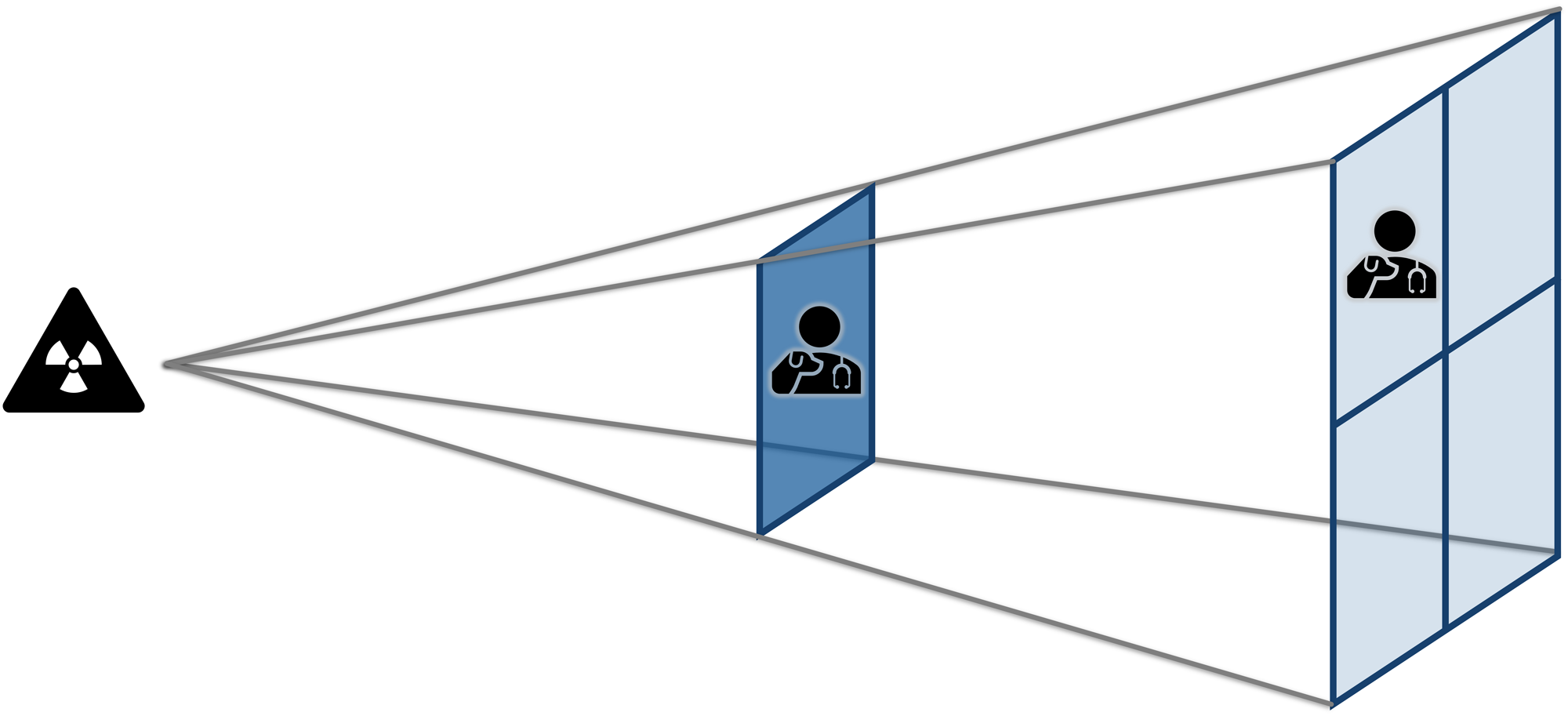
Representation of the inverse-square law. Doubling the distance from a point source of ionising radiation will reduce exposure by a factor of four, as the photons are spread over a larger area.
3.4.2. Protection against contamination
(65) As mentioned above, contamination (the unwanted presence of radioactivity) has the unique potential to be both an internal and external radiation hazard. It is also transferable, so specific precautions relevant to preventing contamination need to be adopted. The potential for contamination is relevant for unsealed sources (i.e. radiopharmaceuticals). (66) Internal exposure to radionuclides is possible through inhalation, ingestion, or absorption through open wounds or even intact skin in the case of a high-mobility radionuclide. Internal radiological protection and contamination prevention measures focus on preventing or minimising the intake of radionuclides into the body and the deposition of radioactive substances on the body. Such protective measures (e.g. confine, contain, enclose) are consistent with general industrial hygiene measures, and generally include strategies for maintaining control of the source and the environment in which the source is handled and used, as well as using PPE when appropriate (see Section 3.4). Additionally, consistent with the justification principle, the amount of radiopharmaceutical administered to a patient should be selected such that no more is used than that needed to achieve the optimal diagnostic or therapeutic result. This optimises protection and safety of the patient, as well as that of workers, the public, and the environment.
4. ETHICS AND VALUES
4.1. Ethics of the system of radiological protection
(67) The system of radiological protection is rooted in, and informed by, the three pillars of science, ethics, and experience, and has evolved over the past several decades (ICRP, 2018a). Ethics, or moral philosophy, seeks to distinguish right from wrong; in other words, it considers the nature of morality and strives to describe and justify how things should be and how we should behave. The system of radiological protection has evolved in parallel with considerations of the morals and ethics relating to it; one has not emerged directly from the other. Thus, the primary aim of radiological protection is met by way of a comprehensive framework underpinned by a set of fundamental scientific principles and ethical considerations. (68) Publication 138 (ICRP, 2018a) has recently clarified the ethical basis of the system for human protection, and identified core ethical principles (referred to as ‘values’ to distinguish from the three principles of radiological protection) as well as procedural ethical values underlying the system. It did not specifically address the ethical aspects of the protection of individual animals in the context of veterinary practice. (69) Three major theories of ethics that underpin the system of radiological protection are utilitarianism, deontology, and virtue ethics, which respectively argue (albeit simplified) for the furthering of the collective interest; the respect for individuals and their rights; and the promotion of integrity, discernment, and wisdom. The core ethical values in relation to humans, considered to be consistent with each of the aforementioned theories and shared across cultures, include beneficence/non-maleficence, prudence, justice, and dignity. Although these values run through the system and are not specific to any one principle, some direct links are clear. Beneficence/non-maleficence, doing good while avoiding harm, relates directly to the principle of justification. Prudence, the ability to make informed and rational decisions in the face of uncertainty, relates to the principle of optimisation of protection. Justice, or equity and fairness, relates directly to the principle of the application of dose limits. Dignity, or respect for all persons, is evident throughout the system and also supports the procedural values, which include accountability, transparency, and inclusiveness. Procedural values emphasise the process for implementation of the core values. Hence, ethics encompasses not only what is done but how it is done. Ethical risk evaluation and management, then, considers factors that go beyond the magnitude of the radiation exposure and the cost associated with reducing the exposure (Oughton, 2013). (70) It is also worth mentioning that although these are the broad values underlying the system of radiological protection, it is not to say that these are the only important values. For example, in environmental protection, additional values such as sustainable development and environmental justice are also emphasised (ICRP, 2003b). Also, since 1979, the seminal principles of biomedical ethics have been beneficence, non-maleficence, justice, and respect for autonomy (Beauchamp and Childress, 2019), which are emphasised in discussions of ethics surrounding the use of radiation in (human) medicine (Malone et al., 2018; Bochud et al., 2020).
4.2. Radiological protection and veterinary ethics
(71) The three ethical theories mentioned above are also taught frequently in veterinary ethics (Fawcett et al., 2018). The core ethical values of the system of radiological protection are consistent with, but of course not the only values important in, veterinary practice. For example, the One Welfare framework (Pinillos et al., 2016; Bourque, 2017; Fawcett et al., 2018) recognises and emphasises the inter-relationships between human health and well-being, animal welfare, socio-economic development, biodiversity, and environmental conservation, and highlights additional ethical principles consistent with a holistic approach to sustainable development, similar to but broader than those presented in Publication 91 (ICRP, 2003b) for protection of the environment (see Annex B for additional discussion). (72) The consideration of ethics applied to veterinary practice can help to inform the application and implementation of the three radiological protection principles. Although there are numerous ethical values that are relevant to veterinary practice, only a few are discussed here in relation to the core and procedural values of Publication 138 (ICRP, 2018a, Table 4.1). These values are consistent with the values of the system of radiological protection, the One Health approach, the One Welfare approach, the World Veterinarian Association Model Veterinarians’ Oath, and veterinary medical ethics in general (ICRP,
2003b
,
2018a; Pinillos et al., 2016; AVMA, 2019; Mackenzie and Jeggo, 2019; WVA, 2019). There are many inter-relationships and applications of the values in Table 4.1 (see Para. 80 for additional examples), extending beyond veterinary practice (Martinez, 2021). Additionally, other ethical values may also come up depending on the circumstances. However, highlighting key values and relationships here is intended to help make the ethical ties between the system of radiological protection, the environment, and veterinary practice clearer, while also offering a more specific framework for considering ethical dilemmas in veterinary practice. Note that, similar to Publication 91 (ICRP, 2003b), some values highlighted are more related to humans, and others to animals and the environment. (73) Animal welfare is, of course, the core of veterinary practice. Many definitions and interpretations exist, but animal welfare refers generally to the well-being of non-human animals (Hewson, 2003). Animal welfare can be linked to beneficence/non-maleficence as the promotion of animal health and welfare, along with avoidance of causing animals unnecessary harm or suffering. For example, beneficence/non-maleficence is evident in determining whether a procedure fits in the clinical pathway; that is, whether it is indicated and appropriate. Regardless of the specific motivation for veterinary intervention, ultimately the general goal is to do more good than harm, with explicit attention given to animal welfare among the various factors considered (e.g. protection of public health and the environment, advancement of knowledge, etc.). (74) Sustainable development is, broadly, development that meets the needs of the present without compromising the ability of future generations to meet their own needs, whether societal, economic, environmental, etc. Sustainable development is highlighted in an environmental context in Publication 91 (ICRP, 2003b), which specifies that sustainable development includes recognition of the need to protect all living resources. Veterinarians care for a variety of species of animals, both domestic and wild; whereas companion and working animals are typically treated for the specific benefit of the animal and/or its owner, a wild animal may be diagnosed and treated as part of broader rehabilitation and conservation efforts. Sustainable development relates to prudence as it involves acting with precaution, particularly when decisions might affect future generations. Note that Publication 122 (ICRP, 2013c) also highlights the protection of future generations as an important ethical consideration, but in the context of radioactive waste management. (75) Solidarity refers to unity arising from shared responsibilities, interests, sympathies, and links to justice through employing the co-expertise process such that outcomes are as fair, equitable, and balanced as possible (ICRP, 2006). The quality and standard of veterinary care should be consistent between patients, regardless of the owner’s background, and solidarity is found through the shared desire for the animal’s well-being; a decision should be made as to the most reasonable course of action in collaboration with the owner. In the instance of unreasonable or irresponsible owners, veterinarians should do their best to ensure what is fair to the animal in the given circumstances. (76) Reverence for life refers to the recognition that both humans and other living things have value and that there is importance in maintaining, assisting, and enhancing life. Similar to human medicine (O’Connor et al., 2019), veterinary practice not only involves treating disease but expressing compassion and respect for the patient as well as the owner. Reverence for life recognises that all living things have a place in the world and deserve to be safe and well, or at the least, to experience life without suffering (Schweitzer and Cicovacki, 2009). (77) Stewardship is the careful and responsible management of something entrusted to one’s care, whether that is pets, livestock, land, resources, or even medical records or other personal information. It is a responsibility that includes conscientious decision-making related to those things for which we have an obligation. This is strongly associated with accountability, a procedural ethical value that refers to the expectation that a person or institution is answerable for their actions or decisions. Accountability could include, for example, the tracking and reporting of misadministration incidents or over-exposures, having a plan for such incidents and accidents, and learning from them to improve care. Annex A provides a summary of roles and responsibilities related to radiological protection. (78) Autonomy is the capacity to make an informed, uncoerced decision, and clearly, one cannot exert their autonomy without transparency, or open and honest communication. For example, available and appropriate diagnostic and treatment options with potential outcomes should be discussed clearly with the owner or responsible party. Owners have the right to know the risks, benefits, alternatives, and financial obligations associated with their animal’s diagnosis and treatment. Similarly, workers have the right to know their occupational risks. Moreover, the responsible veterinarian should ensure that workers are appropriately: (1) informed of relevant risks, radiological and otherwise; (2) trained in the technique or procedure at hand, including radiological protection strategies relevant to themselves, the animal, and bystanders; and (3) protected from unnecessary exposure through practical protection strategies and the provision of proper PPE (see Section 3.4). (79) Empathy is the ability to understand and share the feelings of others, and inclusiveness refers to involving all relevant parties in the decision-making process. Empathy is related to inclusiveness (e.g. ICRP, 2020b) through meaningful engagement with others and appreciation of the needs, challenges, and values of others for mutually agreeable outcomes. Veterinarians and their staff should, of course, advocate for and prioritise the animal’s welfare, but decisions will also necessarily be made based on economic value and financial means of the owner, as well as what the owner is going through (Weil, 1951; Kipperman et al., 2017). (80) Note that there are a variety of inter-relationships between the values in Table 4.1 and other ethical values or principles, and the discussion above is not meant to be exhaustive but rather to provide some additional context for the core and procedural values of the system of radiological protection. For example, transparency is an expression of respect for autonomy, which in turn is strongly related to dignity (ICRP, 2018a; Ban et al., 2022). Solidarity has elements of both justice and inclusiveness, as the co-expertise process involves both fair and genuinely collaborative decision-making (ICRP, 2006). Sustainable development has elements of both justice and prudence in that we want things to be fair, but also have to make decisions without knowing with full certainty what future needs will be. Elements of empathy can help to improve recognition of pain or distress in animals, tying to animal welfare (NRC, 2009; Ellingsen et al., 2010). Reverence for life and sustainable development together support the maintenance of biodiversity, or the variety and variability of life in the world. Although this latter ethical principle is more related to environmental protection (e.g. ICRP, 2003b; UN, 2015), there is overlap in veterinary practice as maintenance of biodiversity is often an active, interdisciplinary effort that may benefit from access to veterinary expertise. (81) Another example of the interplay of several ethical values is the use of animals for research purposes, either in a laboratory or field setting, although this extends beyond radiological protection in veterinary practice, and sometimes beyond veterinary practice as a whole. Such research is recognised as having a societal benefit as it has proven valuable in expanding our fundamental understanding of biology, as well as in improving human health, environmental health, and animal welfare (NRC,
1991, 2009; Friend et al., 1999). However, because this can clearly result in harm to the animals concerned, there is also the public expectation that experiments are scientifically, technically, and humanely appropriate, avoiding doing harm wherever possible (NRC, 2011). In other words, the research community has stewardship over the animals involved, and thus assumes responsibility for the animals’ welfare, which necessitates critical and prudent evaluation of the study design and outcomes (NRC,
2009, 2011; Vasbinder and Locke, 2016). Note, however, that detailed discussion of the use of research animals is beyond the scope of the current publication, and is not elaborated further beyond the brief mention here and Section 6.1.4.
ICRP Publication 138 (ICRP, 2018a) core and procedural ethical values with additional interpretation.

5. UNIQUE ASPECTS OF VETERINARY PRACTICE
(82) As many applications of ionising radiation in veterinary practice may have come about without the active involvement of persons knowledgeable in radiological protection, such as a medical physicist, and often also in the absence of an appropriate radiological protection framework, several issues have arisen. These issues need to be identified and rectified, preferably in close collaboration between the relevant stakeholders (e.g. practising veterinarians, professional societies, radiological protection competent authorities, and radiation protection experts). The issues listed should be seen as illustrative and by no means have the pretension of being exhaustive. (83) If compared with human medicine applications, challenges for radiological protection could be greater in veterinary practice. Many radiological procedures on large animals are performed in environments that have not been designed specifically, or properly fitted out, for these procedures, including in the field. Justification is not currently supported by a veterinary society’s equivalent of the ‘referral guidance’ or ‘appropriateness criteria’ we are familiar with in human medicine. There are no DRLs or similar comparative benchmarks for imaging optimisation. There are important differences with regard to the activities of radiopharmaceuticals administered for therapeutic purposes for the same disease (e.g. hyperthyroidism) in comparable animals (e.g. average-sized house cats). The involvement of a medical physicist is very rare for radiation protection education, training, optimisation, and equipment life cycle issues. Last but not least, not all practitioners performing higher dose diagnostic or even radiotherapeutic procedures have specific or specialist education and training that is accredited and certified. (84) Conventional radiology is available in many small veterinary practices. CT scanners, cone beam CT scanners, C-arms, O-arms, and non-mobile fluoroscopy can be found in an ever-growing number of veterinary clinics, where shielding strategies may require particular attention because of retrofitted equipment. The use of mobile radiographic equipment is standard in dealing with large animals as it is performed on farms, in stables, at auctions, or in the open field. The delimitation of a safe working area and the proper use of the mobile equipment may require extra attention. Nuclear medicine diagnostics and treatments are not so common, but may have been introduced without sufficient consideration of contamination problems, such as in dealing with radioactive waste, particularly urine. Some therapeutic interventions may be performed outside of veterinary clinics, such as when radioactive substances are administered into a horse’s joints at a riding stable, resulting in potential contamination concerns. In nuclear medicine in general, the animal as an ambulatory source with contamination potential deserves specific consideration, particularly when outside the confines of the clinic. Other radiotherapeutic treatments, either teletherapy or brachytherapy, are still rare and restricted to veterinary clinics, but the potential radiological risks to both the animals and people involved in the procedures should not be neglected. As an aside, as such treatment options become more widely available, it is possible that veterinary clinics may face unique nuclear security challenges in addition to the radiation protection and safety aspects described herein. (85) Although more and more dedicated veterinary equipment is becoming available, second-hand equipment coming from human medicine is still very prevalent in veterinary practice. Safety and performance of the equipment should be verified before its first use, and on a regular basis afterwards, by means of radiological protection and quality control programmes, as elaborated on by IAEA (2021). Quality checks need to include all pieces of equipment throughout the imaging or treatment chain (e.g. cameras in nuclear medicine, image monitors, etc.), and should not be restricted to radiation-emitting equipment or sources. There is also a growing influx of speciality veterinary equipment (e.g. FIDEX CT) that falls under industrial rather than medical standards. Although dedicated, fit-for-purpose equipment is certainly welcome in principle, it must still meet appropriate radiation safety standards. Similarly, clinics may not have given due consideration to shielding needs. For example, a room may have been designed with adequate shielding for conventional x-ray applications on a fixed table with the primary beam directed from the ceiling to the floor, but that room may not be adequately shielded for interventional procedures using a C-arm. (86) For historic reasons, most veterinarians learn how to use standard radiologic equipment – fixed, mobile, or both – in their basic curriculum. This should comprise at least the basic notions of radiological protection. More risk-bearing applications, such as the use of CT scanners, interventional radiology, nuclear medicine, and radiotherapy, certainly call for additional education and training, including the corresponding radiological protection. Basic or specialist education and training programmes are on offer in a number of veterinary schools and professional societies, for instance through the American College of Veterinary Radiology and the European College of Veterinary Diagnostic Imaging, but the corresponding curricula do not always include the necessary theoretical radiation science education and practical training on radiological protection topics specifically. Consequently, radiological protection competent authorities may not automatically consider diplomates (board-certified specialists) as sufficiently competent in radiological protection. Practising the more complex and risk-bearing techniques could arguably be restricted to veterinarians who have completed ‘specialist’ programmes successfully, as this would be beneficial for the quality of care or service delivered and the associated radiological protection. Across the world, there are striking differences in the basic and specific education and training requirements related to the application of different imaging and therapy modalities in veterinary applications of ionising radiation. Note that guidance on radiological protection education and training specific to veterinary professionals has been developed by HERCA, inspired by the model developed by the European Commission for Human Medicine (HERCA, 2017; IAEA, 2021). Similarly, Publication 113 (ICRP, 2009b), while focused on human medical care, contains information on education and training that may be useful for informing the development of parallel standards in veterinary practice. (87) These differences can also be observed for the corresponding radiological protection requirements, where some harmonisation of training requirements is necessary (Gregorich et al., 2018). This effort should include the continuous refreshing, updating, and, where needed, extending of theoretical knowledge and practical skills, as well as adapting competencies, attitudes, and behaviours. If other professionals, such as radiographers or radiotherapy technologists, actively intervene or perform radiologic or radiotherapeutic procedures of any sort autonomously, the same principles must apply. They should have completed initial education and training programmes successfully, and continue to refresh and update their knowledge, skills, and competencies regularly throughout their professional life. This should necessarily include radiological protection. It is up to the licensee or otherwise authorised person or entity responsible for the facility to clearly establish the roles and responsibilities of all those involved in the procedures, within the bounds of the appropriate regulatory framework, and ensure that they have, and continue to have, corresponding education and training.
6. APPLICATION OF THE SYSTEM OF RADIOLOGICAL PROTECTION TO VETERINARY PRACTICE
6.1. Justification of radiological procedures in veterinary practice
(88) As mentioned above, the principle of justification is one of the fundamental principles of radiological protection, and states that any decision that alters the radiation exposure situation should do more good than harm (ICRP, 2007a). In addition to the exposure of the animal, veterinary staff are also exposed frequently during veterinary radiological procedures. Sometimes, the animal’s owner or handler, farmworkers, other members of the public, or the environment may also be exposed as a consequence of veterinary use of ionising radiation. Hence, proper justification of veterinary radiological procedures is necessary to avoid unnecessary exposures of people, animals, and the environment. (89) The three levels of justification for radiological practice in medicine, described in Publication 105 (ICRP, 2007b), can also be applied to veterinary practice as recommended herein (Table 6.1). Level 1 justification requires that the proper use of radiation in veterinary practice does more good than harm to society. As radiological procedures are now integral to veterinary practice worldwide, Level 1 justification is taken as a given and is not discussed further in this publication. At Level 2, a specified procedure would be considered generically justified for a specified clinical objective if it does more good than harm by improving the diagnosis or treatment of a defined group of animal patients, or if it will provide necessary information about exposed animals. Level 3 justification requires that the application of a radiological procedure is judged to do more good than harm in the management of the individual animal patient. Level 2 and Level 3 justification in veterinary practice are discussed further in Sections 6.1.1 and 6.1.2. These three levels of justification apply to animal patients, but of course risks to workers, members of the public, and the environment all need to be considered. It is possible that a specific procedure may be justified considering the animal patient, but may nonetheless be unjustified when also considering risks to humans. (90) There has been increasing awareness about the overuse of radiological procedures in human medicine, with a substantial proportion of medical imaging procedures deemed to be unjustified (Picano, 2004; Holmberg et al., 2010; Malone et al., 2012). While similar surveys have not been carried out in veterinary medicine, the challenge of avoiding unjustified use of ionising radiation likely exists here as well, as many of the drivers of overuse in human medicine (Lysdahl and Hofmann, 2009; Hendee et al., 2010) are also present in veterinary medicine. These include, among others, desire for greater confidence in the clinical diagnosis, lack of awareness of doses and associated risks, defensive medicine, lack of access to previously performed examinations at other veterinary practices, and financial conflict of interest, including self-referral and ‘self’-presentation. Self-referral means that the same clinician holds the roles of both referrer and radiological service provider, as ‘ordering physician’ and as ‘imaging services provider’ (they may outsource the interpretation but provide the imaging itself). Self-presentation in human medicine may describe a situation where a person would present at a radiology practice, requesting a procedure for himself or herself, without this request being backed up by a clinician. Similarly, in veterinary medicine, ‘self’-presentation would designate the situation in which an animal owner requests a radiological procedure without the intervention of a veterinary clinician. (91) Unlike in human medicine, where the potential for overuse due to the financial incentives from self-referral is recognised (Kouri et al., 2002), and where regulations and professional codes of ethics in many countries have been put in place to guard against this practice, self-referral is the norm rather than the exception in veterinary medicine. Radiographic equipment is widespread, both in general veterinary practice and in larger veterinary hospitals. Frequently, the veterinary practitioner ordering a radiological procedure will also be the person performing the imaging procedure and interpreting its results. This person may also be the owner of the radiographic equipment, or may be employed by a veterinary practice which explicitly or implicitly expects their staff to ensure return on their investment in radiographic equipment. Hence, financial incentives as drivers for the use of radiological equipment are often present in veterinary medicine, and are considered a risk factor for possible overuse. (92) ‘Self’-presentation, in which the owner/handler of an animal requests a diagnostic imaging or therapeutic procedure without the previous clinical examination of the animal, and hence without a radiology referral from a veterinary practitioner, or where the owner/handler demands a diagnostic or therapeutic procedure that is not considered indicated by their veterinary practitioner, is also a pertinent issue in veterinary practice. As veterinary practice effectively provides services rendered mainly by private practitioners, some veterinarians may feel compelled to comply with such consumer demands (also relevant in presale examinations) to avoid losing business to veterinary practices that oblige such requests.
Summary of the three levels of justification in human medicine and veterinary practice.
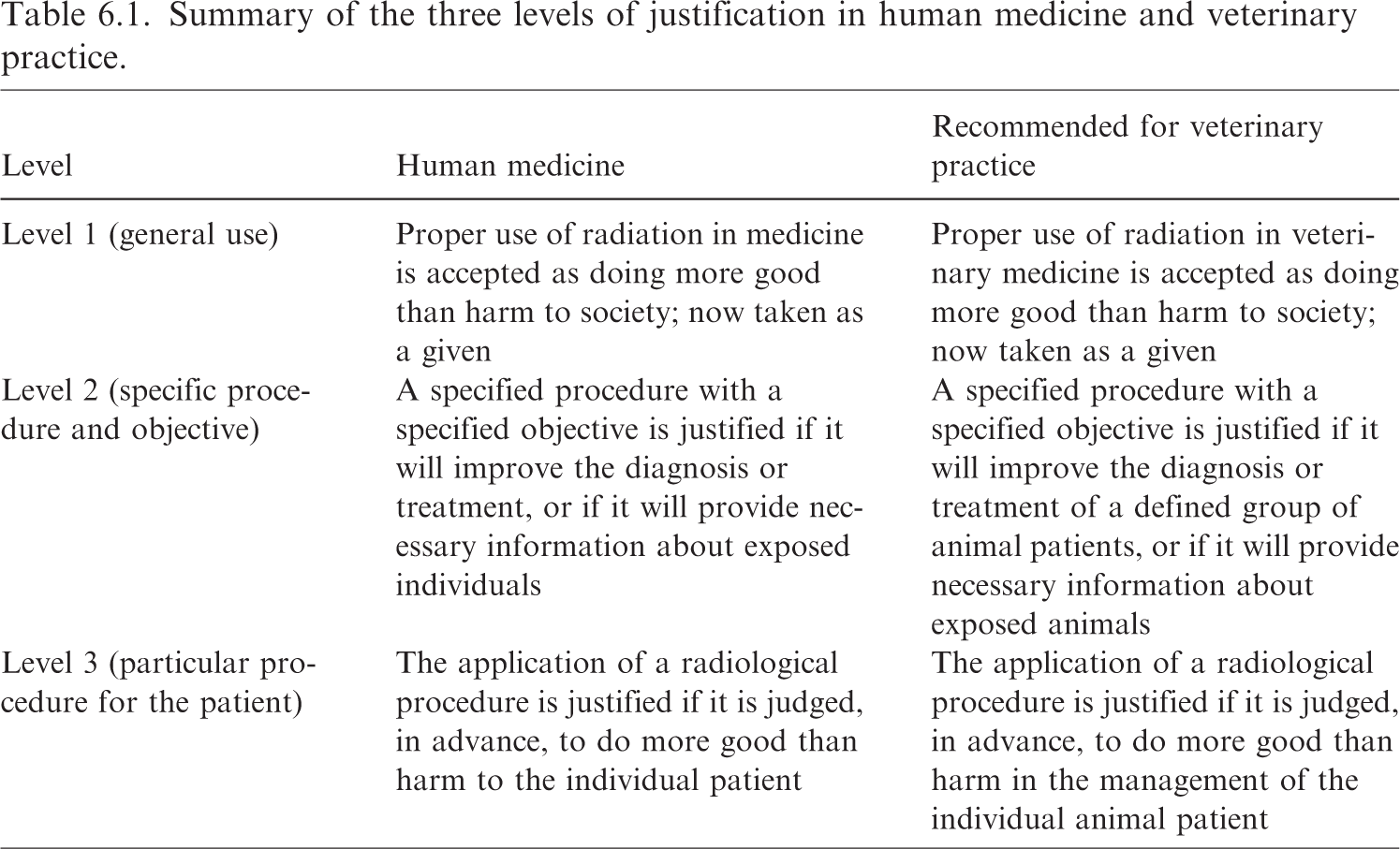
6.1.1. Justification of medical procedures
(93) Specialised veterinary radiologists are limited in number worldwide, and most veterinary practices do not have an in-house veterinary radiologist. Hence, the choice of diagnostic procedure as well as the interpretation of its results are often performed by a general practitioner or a veterinarian of another speciality than radiology, without input from a veterinary radiologist. The radiological procedure is also often performed by someone who has not been trained specifically as a veterinary technologist/radiographer (e.g. a general veterinary practitioner or a veterinary nurse/technician). Appropriate education and training of veterinary staff involved in radiological procedures, either as part of their basic education or as continuing education, is therefore necessary to ensure both the justification and optimisation of such procedures. This training should aim to create awareness about the doses and the associated risks from the various radiological procedures. Those completing the training should be able to perform imaging and quality control on equipment, and engage in effective risk communication with owners and handlers of animals. (94) Decision support tools, such as referral guidelines or appropriateness criteria (EC, 2014; Subramaniam et al., 2019), could also be particularly useful in veterinary medicine to ensure Level 2 justification in the absence of direct veterinary radiologist input. These guidelines should be easily accessible, free of charge, and easy to use (e.g. ideally through integration into the electronic medical record system) to ensure their widespread adoption. Such guidelines, however, need to be developed collaboratively by national or international professional veterinary radiology societies, in conjunction with veterinary professional bodies, and animal health and regulatory authorities, and would require a substantial commitment of time and resources to their creation and periodic update. (95) Of note, referral guidelines or appropriateness criteria not only contain information on different radiological imaging procedures (e.g. plain x ray, CT scanning), but also on imaging modalities that do not make use of ionising radiation – ultrasound and magnetic resonance imaging (MRI) in particular. From the point of view of justification, but only after careful consideration of all other factors (e.g. availability, cost, etc.) that come into play and are judged equal, the imaging method that can provide the required information for the lowest exposure – or no exposure to ionising radiation at all – should be preferred, if available. (96) When new types of radiological equipment are considered and introduced in veterinary practice, an assessment of their potential implications for radiological protection should also be made. Recently, there has been an increase in radiological equipment dedicated to veterinary medicine on the market, and this equipment may not always comply with the imaging quality and/or radiological protection standards required for medical devices. Vigilance, both from potential buyers and regulating authorities, is therefore required to ensure that the adoption of such new equipment can be justified. (97) Level 3 justification requires that the radiological procedure is required for the management of the individual patient. A diagnostic procedure should be able to answer a given clinical question, and have an impact on the patient’s diagnosis, prognosis, or treatment. Consideration should also be given to alternative modalities with less exposure to ionising radiation – or no exposure at all – such as replacing CT with MRI or ultrasound. One part of justification is determination of the most appropriate examination, within the constraints of available modalities. The radiology request should contain sufficient clinical information that a radiologist or an internal or external auditor can assess whether the particular examination is justified.
6.1.2. Justification of non-medically-indicated investigations
(98) Imaging of asymptomatic animals for purposes other than medical diagnosis or treatment is performed frequently in veterinary medicine. Screening programmes for canine hip and elbow dysplasia are in place in many countries (Verhoeven et al., 2012; Hazewinkel, 2018), and large numbers of animals are thus imaged as part of the breeding selection process. Many equine studbooks require that a specified radiographic examination has been performed on their approved stallions (Verwilghen et al., 2009), and presale radiographic examinations of yearling racehorses have become standard practice in many countries (Cohen et al., 2006; RIRDC, 2009; Furniss et al., 2011; Miyakoshi et al., 2017). Other horses, both pleasure and competition horses, also have radiographic examinations frequently as part of the purchase process, and insurance companies may demand a radiographic study of an animal as part of the insurance process. However, in some instances, the radiographic studies performed may not be consistent with current clinical evidence (Barrett et al., 2018; Steel et al., 2019). (99) For non-medically-indicated radiological procedures, Level 2 justification is therefore important. Particular attention should be paid to the clinical evidence for the usefulness of the procedure, ensuring that the chosen imaging procedure is suitable both for the detection of the condition in question, and for screening a potentially large number of animals (Bladon and Main, 2003). Furthermore, there should be a demonstrable relationship between the imaging findings and the goal of the screening. For example, for a breeding suitability examination, the trait in question should have a sufficient degree of heritability, as well as a prevalence in the population that makes it a relevant discriminator between potential breeding animals (e.g. Bruun et al., 2020). For presale examinations, the results of the imaging should be predictive of the animal’s future performance (e.g. Bladon and Main, 2003; RIRDC, 2009). Again, appropriateness criteria could be developed by professional veterinary speciality organisations, in conjunction with professional veterinary societies, regulatory authorities, breed societies, insurance companies, and industry representatives or other stakeholders, as appropriate.
6.1.3. Benefits and risks of radiological procedures
(100) The balance of benefits and risks to the exposed animals, and sometimes more generally to the population to which they belong, veterinary staff, animal owners or handlers, the general public, society at large, and the environment, must all be considered when determining if a given radiological procedure is justified in veterinary practice. This includes full consideration of other modalities that deliver lower or no radiological dose for the indicated need. Along with the beneficence/non-maleficence aspect of justification, finding the appropriate balance will necessarily involve exercising prudence. (101) Benefits for exposed animals include a direct benefit from improved diagnosis and treatment in the case of animal patients, while the results from a presale or breeding suitability examination may help to ensure that the animal is suited for its intended purpose, and will not suffer negative health consequences from its future use. Screening examinations of asymptomatic animals may help to detect subclinical disease, and such early diagnosis may potentially lead to improved treatment results. In addition to welfare benefits for the individual animal, the welfare of animal populations may also be improved through breeding suitability examinations, if undesirable traits or medical conditions can be reduced in the population based on the imaging results. (102) Benefits for veterinary staff from the appropriate use of ionising radiation include the ability to provide the best possible diagnosis and treatment to their patients, customer satisfaction, and financial revenue from the radiological procedures (and any follow-up treatment). Owners and handlers may benefit both emotionally and economically from improved diagnosis and appropriate treatment of their animals. (103) In addition to individual animals, owners, and veterinary staff benefiting directly from the appropriate use of ionising radiation – or its alternatives – in veterinary practice, society at large will also benefit from such use. Animal and human health are interlinked, and radiological procedures that contribute to animal health may also improve public health, particularly when they contribute to the control of zoonotic diseases (Viljoen and Luckins, 2012; see also Annex B). Furthermore, a healthy population of working animals and livestock will also benefit society, both in terms of public health and the economy. Other industries, such as the racing and showing industries, would likely also benefit economically from improved animal health. In the case of rare or endangered species, conservation efforts may also sometimes benefit from the use of radiological procedures to diagnose and/or treat disease in zoo animals or wild animals. Moreover, with increasing societal concern over the ethics of the use of animals for production and entertainment, ensuring good health in these animals could also be seen as a prerequisite for the social acceptance of such use. (104) Radiation risks to exposed animals include both stochastic effects and tissue reactions. While the risk of stochastic effects (compared with tissue reactions) predominates in plain radiography, high-dose diagnostic procedures, such as CT-guided and other interventional procedures, are performed increasingly in veterinary medicine, and could potentially result in tissue reactions, particularly in the skin (Balter et al., 2010; Cléroux et al., 2018). Furthermore, in veterinary radiation therapy, adverse effects associated with tissue reactions are encountered frequently in normal tissues, and the probability of their occurrence must be balanced carefully against the clinical benefits of tumour control or palliation (e.g. Collen and Mayer, 2006; Gieger and Nolan, 2017). On the other hand, lack of access to appropriate diagnostic imaging or therapy, or inappropriate choice of diagnostic or therapeutic modality could lead to adverse health effects for the animal due to misdiagnosis or inappropriate treatment. (105) Veterinary staff receive most of the radiation doses associated with veterinary radiological procedures, either when operating radiological equipment; holding image detectors; restraining animals during diagnostic procedures; performing or assisting in nuclear medicine, interventional, or therapeutic procedures; or caring for animals after nuclear medicine diagnostics or therapy with sealed or unsealed radioactive sources. Most doses to staff will be low (see Section 6.2.2), but over time could potentially contribute to the development of stochastic effects. Additionally, epidemiologic studies of radiation workers in human medicine note a higher incidence of cataracts in both interventional proceduralists and nuclear medicine technologists who receive chronic low-dose exposures (ICRP, 2012b). Higher dose procedures, such as long interventional procedures, potential spills in nuclear medicine, or accidents relating to therapeutic procedures could potentially lead to deterministic effects. Owners or handlers exposed to radiation when assisting in radiological procedures or caring for animals after nuclear medicine procedures may also be at risk, albeit low, mainly for stochastic effects. The assistance of members of the public in radiological procedures is currently a subject of debate, and will be discussed further in Section 6.2.1. (106) Environmental contamination may also occur after diagnostic or therapeutic nuclear medicine procedures, either through releases from the veterinary facility where the procedure is carried out, or through radioactivity eliminated from the animal after its discharge from the veterinary facility. While releases at the veterinary facility are often well controlled and regulated, uncertainty exists after the animal is discharged. These uncertainties will depend on the level of radioactivity in the animal at the time of discharge, the mechanisms of elimination of the radionuclide used, the veterinary practices’ recommendations for isolation of the animal and management of its waste, and the degree of owner or handler compliance with these recommendations. Environmental contamination may lead to radioecological effects, as well as to human exposure through external radiation or internal contamination. The nature and extent of the consequences of environmental contamination will depend on the type, amount, and duration of the contamination event (ICRP, 2014a).
6.1.4. Research animals
(107) There are many contexts in which research might be conducted involving animals and the use or presence of radiation or radioactive substances, in many cases extending beyond veterinary practice; these animals are typically not considered animal patients, and detailed discussion of research animals is beyond the scope of the current publication. Justification in this context should be conducted within the broader scope of research ethics and laboratory/research animal care and use (e.g. replacement, reduction, and refinement; Russell and Burch, 1959) depending on the study, and consistent with local and national guidance or regulations (e.g. Friend et al., 1999; NRC, 2011).
6.2. Optimisation of protection in veterinary practice
(108) In the system of protection, ‘optimisation is always aimed at achieving the best level of protection under the prevailing circumstances through an ongoing, iterative process’ (ICRP, 2007a). Factors to be considered in the optimisation process encompass animal welfare, and whether the motivation for veterinary services is economic (e.g. performance horse) or societal (e.g. companion animals). Note that Publication 101b (ICRP, 2006) provides an elaboration on the history, evolution, and implementation of the optimisation principle, including the need for a graded approach.
6.2.1. General considerations
(109) Although the protection and safety of humans may be considered the priority of optimisation efforts, it is important to realise that this can already be largely achieved by limiting the initiating exposure of the animal to what is truly necessary to achieve the clinical objective. Reducing the exposure of the animal will almost invariably be beneficial for the protection of humans involved in whatever way in the veterinary procedure and, where applicable, of the environment. A first step in the optimisation of radiological protection during a veterinary procedure is therefore to adjust the imaging exposure parameters or adapt the activity of radiopharmaceutical administered in such a way that the required clinical effect is obtained with the lowest possible radiation dose, and net benefit is maximised. (110) Radiological examinations are now common practice from a young age (e.g. screening tests) and for the life of certain animals. Pet animals tend to live much longer than they used to due, in part, to robust veterinary care, including earlier diagnosis and specialised medicine (Cozzi et al., 2017). With the increase in prevalence and frequency of radiological examinations, and the increased life span of companion animals, there is a need for more attention to optimisation of protection and safety in veterinary procedures that explicitly include radiological protection considerations with regard to the exposed animals. (111) Optimisation can generally be achieved by: (1) appropriate design and construction of installations, and careful selection of equipment; and (2) day-to-day strategies such as adequate and regularly updated education and training of staff, clarity with regard to their exact roles and responsibilities, routine performance tests of equipment, and systematic application of procedural rules, all embedded in a safety culture at organisational level. The optimisation process may also include dose constraints based on reasonable, good practice, particularly as veterinary staff often perform various services (IAEA, 2021). This approach is consistent with what is advocated for the practice of human medicine (ICRP, 2007b). At present, no guidance is available related to, for instance, animal-specific DRLs or similar imaging guidance parameters. However, considering the societal value of animals, optimisation strategies relevant for human patients should also be valid for animal patients. (112) Optimisation should not be confounded with dose minimisation. Too much focus on dose reduction alone may impede the diagnostic or therapeutic quality of the procedure, and result in suboptimal care or necessitate a repeat procedure. This clear distinction between dose optimisation and dose minimisation is critical in radiotherapy, where underdosage may lead to insufficient tumour control, and even optimal procedures may result in the inevitable appearance of early or late side effects. Moreover, risk induced by radiation exposure is only one of the elements to be taken into consideration, and optimisation of protection and safety therefore needs a holistic view comprising not only broad animal welfare considerations but also general safety aspects for staff members and members of the public. (113) Veterinarians and associated staff face many occupational challenges and hazards, of which exposure to ionising radiation is just one. For example, other hazards such as bites, scratches, or kicks may be more important, and certainly more acute, issues. Thus, the optimisation process for veterinary workers should broadly encompass consideration of risk, benefit, and practicality. In other words, the level of protection should be optimised in a way that most reasonably accounts for the given circumstances, as consistent with other exposure situations. Gloves might be worn when handling a patient prone to biting, but if the patient is afraid of gloves to the extent that an examination cannot be conducted, it may be prudent to leave them off and consider an alternate strategy. (114) Similarly, sedation and anaesthesia are frequently advocated from a radioprotection point of view, but in some cases, the associated detrimental impact on the animal’s health may lead to the conclusion that this may not be the best option for patient restraint. Where permitted, optimisation could then consist of having the owner restrain the animal, even though this might result in some radiation exposure to this person, which, in turn, should be mitigated by providing clear instructions and – where applicable – adapted protective equipment. (115) Optimisation clearly also applies to members of the public, defined in the system of protection as individuals who receive an exposure to ionising radiation that is neither occupational nor medical (ICRP, 2007a). With respect to veterinary practice, the public may include pet owners/handlers, clients in a waiting area, farm hands assisting with an equine examination, etc. In some countries, members of the public will not be allowed to assist in veterinary radiological procedures. In such instances that they can be allowed to assist in some procedures (see Para. 120, for example), the following conditions should be fulfilled: (1) the procedure is justified; (2) the person’s presence is overall beneficial from a ‘holistic’ perspective, as discussed above (see Para. 111); (3) the person, after having received relevant information regarding potential risks, agrees to undergo some limited exposure; and (4) after having been instructed on how to behave (where to stand, where to put their hands, possibly what protective equipment to use, etc.) in order to minimise their exposure. Children and individuals who are pregnant should not be allowed to assist in such radiological procedures. (116) Given the great number and diversity of elements to consider in any specific case, optimisation needs to be tailored to best fit, within the boundaries of what is prudent and reasonable, and the needs of each individual case. This individual approach should first consider the clinical needs, but also the whole environment in which the procedure takes place (e.g. owners’ wishes, location and transport facilities, available equipment, etc.). (117) Prudence is highly relevant to the process of optimisation, consistent with other areas of veterinary practice that use potentially harmful substances or principles; for example, if 50 mg of a drug would suffice to obtain the desired clinical effect, it would not make sense to use 100 mg. Considering the wide variety of risk factors present in a given circumstance and making value judgements as to the most reasonable choice necessarily involves prudence. In situations that are unfamiliar, rare, or without precedent [as may be the case with exotics or zoo animals (e.g. Adkesson and Ivančić, 2019; Schilliger et al., 2020)], it may be prudent to consult a qualified expert (board-certified veterinary radiologist, radiation physicist, safety officer, or other individual with recognised competence in radiation safety) in advance of the procedure for guidance.
6.2.2. Optimisation in veterinary radiology
(118) The main source of veterinary occupational exposure is from diagnostic radiography (UNSCEAR, 2010). Occupational exposures from this modality are mainly due to scattered radiation, so individual effective doses should be low. However, it has long been recognised that poor practice may result in unnecessary exposure (Wantz and Frick, 1937; UNSCEAR, 2010). Additionally, we know from human medicine that doses to staff and patients from more modern, higher dose modalities can be consequential for both patients and staff. This is even more pronounced in interventional procedures (Wagner, 2007; Miller et al., 2010; Balter and Miller, 2014; ICRP, 2018b). Of note, education and training of staff is crucial for optimisation. Guidance material, such as infographics or posted signage, can be very helpful in that respect (Root et al., 2020; Belotta et al., 2021; Freitas et al., 2021). (119) Radiologic procedures should be performed in an adequately safe environment. The room should be spacious enough to allow people to keep sufficient distance from the radiation sources, and it should be equipped with shielding commensurate with the procedures performed. Hazards may arise when a room initially conceived for occasional standard small animal radiographic procedures has become a room in which CT or interventional procedures are performed, or simply when the number of procedures performed rises well beyond that which was taken into consideration when the room was first conceived and constructed. (120) A designated area for radiological examinations or therapeutic procedures should be established and physically demarcated with warning signs (e.g. Fig. 6.1) to limit unnecessary public exposure. As many equine radiography examinations are performed in stables with mobile generators, additional measures should be taken to delineate the exposure area to avoid unforeseen exposure of members of the public who are not involved in the examination. Performing such procedures in stables with solid concrete or brick walls should be preferred where this is possible, because of the shielding offered. Placing signage at the entrance can then suffice. If procedures need to take place in the open field, delineating the designated area with appropriate signage is much more demanding as it needs to consider all risks involved, not just radiological hazards. (121) In general, members of the public should be kept outside areas where radiation activities are performed, and in the small animal veterinary setting, pet owners should typically not be asked to help during radiological procedures. However, there may be some circumstances in which an owner’s presence comforts the animal in a significant way, resulting in a more efficient and, in some cases, physically safer examination. This, in turn, could reduce the overall exposure to the technologist, for instance by reducing the need for repeat exposures. In other instances, it might be inappropriate to include members of the public or owners/handlers due to the nature and frequency of the exposure, and/or the characteristics of the person considered. For example, a young person working at a stable may wish to assist in every horse’s radiograph series, yet this would likely do more overall harm than good. The decision on whether to allow lay-person assistance in an examination results from a balancing exercise of pros and cons, and is similar to that in human paediatrics (i.e. parents and carers, but owners and handlers in the veterinary setting) (ICRP, 2013b), and needs to be made prudently, focused on beneficence and non-maleficence, and considering the prevailing circumstances. Children and individuals who are pregnant need specific consideration and, in some countries, may be legally excluded from participating in such activities. If the presence of members of the public is judged to be required or useful, then rotation of these persons may be considered in order to limit the exposure of any single individual. Similarly, when deciding on where to perform a procedure, it may be that leaving an animal in a familiar environment (e.g. a horse in its stable) may bear more risk of radiation exposure, yet will be beneficial overall, and thus the most reasonable and optimised choice. (122) Any individual involved in a radiological examination should avoid – as much as possible – being exposed where the intensity of the radiation field is highest, such as in the primary radiation beam. Where reasonable, positioning and immobilisation aids and/or patient sedation/anaesthesia should be considered to reduce staff and owner/handler exposures. Similarly, when possible, personnel should stand behind fixed or mobile protective shields; for example, exposure of the head, neck, and upper body of the veterinarian performing an interventional procedure can be reduced considerably by the adequate use of a ceiling-suspended shield. Optimally, neither portable x-ray generators nor the associated cassettes should be handheld. A recent study simulating exposure from scattered radiation in equine radiography to the hands of workers holding the cassette or the x-ray generator found that doses ranged from 0.26 to 2.64 µGy/study−1 and from 0.84 to 12.09 µGy/study−1, respectively, without the use of hand shielding. Hand shielding reduced doses by at least 98%, depending on the type of glove used (Belotta et al., 2022). (123) In some cases, such as with interventional radiology, it is necessary for staff to perform a variety of tasks within the radiation field for varying times and at different distances from the source. Where external radiation exposure is a concern, in addition to the use of protective shields, the use of shielding PPE should be considered, including protective wraparound aprons, hand/forearm protectors, thyroid collars, and eye protection (e.g. lead safety glasses), depending on the specific circumstance. Note that open-palm hand shields or mitts have limited use; in general, fully enclosed leaded gloves should be used rather than open-palm shields during manual restraint of an animal patient, and it should be borne in mind that even fully enclosing gloves only provide limited protection when the hands are positioned in the primary x-ray beam, which should always be avoided (Mayer et al., 2019b). Shielding properties of the PPE selected for a procedure should be balanced against other workplace hazards. For example, the weight of a lead apron can result in orthopaedic issues such as strain on the lower back if worn for long periods of time (Martin and Sutton, 2015; Alexandre et al., 2017). This, along with the restriction of movement, can increase working time as well as result in physical injury; as such, a vest/skirt configuration or the use of lighter aprons, made of so-called ‘lead-equivalent materials’, may be preferred. Similarly, wearing radiation protective gloves while working close to the animal’s irradiated body volume will reduce dose to the extremities and is frequently warranted (Stoeckelhuber et al., 2005). However, use of these gloves will have a negative effect on dexterity and range of motion, which may lead to safety concerns associated with increased muscle fatigue and working time (Martin and Sutton, 2015). (124) With respect to equipment, optimisation of radiological protection involves ensuring that radiological equipment is suitable for the task at hand, and that exposure parameters are adequately tailored to animal patients and veterinary working routines. The use of radiological equipment in a veterinary setting may be off-label (i.e. not used as originally intended or designed) for new or refurbished medical equipment, or dedicated to veterinary practice by design. For all types, it is recommended that the manufacturers should continue to maintain the equipment and that no modification occurs that would decrease image quality and/or radioprotection properties (e.g. inner shielding, collimator). For equipment designed specifically for veterinary use, the manufacturer is often able to alter the components of the equipment for which medical standards are no longer legally ‘needed’ (no established standards of installation and performance). Such changes often have a positive impact on the selling price of the equipment, yet possibly a negative impact on image quality; output stability; and radiological protection of the animal patient, the veterinary professional, and members of the public. For example, reduced inner shielding of portable radiography units results in significantly increased amounts of leakage and scattered radiation. In a number of countries, industrial standards are applied when dealing with veterinary equipment, and this may be insufficient both from a veterinary care perspective and a radiological protection perspective. The Commission therefore recommends that adequate, fit-for-purpose standards should be applied on all equipment marketed and used in veterinary applications of ionising radiation, and suggests that responsible authorities should consider applying appropriate standards for the accreditation of the equipment and the credentialling of staff members. Ideally, these standards would be recognised internationally, as manufacturers often sell equipment in multiple countries. Of note, equipment standards should also include requirements on the device connections that allow installation in a dedicated veterinary room (e.g. light signalling at the room entrances, emergency stops, door switches). (125) Optimisation measures for patient protection in veterinary diagnostic radiology, for the same image quality, should be discussed with the manufacturer and installation engineer, and implemented when possible. This would include considerations such as limitation of views to those necessary for common diagnostic protocols and technique charts for the range of animal sizes relevant to the facility. Similar strategies apply for CT examinations with a special procedure for auditing repeat examinations and requests for systematic whole-body imaging. Standardisation of national referral guidelines for when and what imaging should be done for common situations, and standard protocols that describe how to perform the imaging examination would greatly aid veterinary practice worldwide in caring for animals and increasing radiation safety. Examinations should not be repeated if no clinical benefit would be obtained. In other words, aesthetically pleasing images should not be the preponderant consideration; rather, the image quality needs to be sufficient to confidently make a diagnosis or proceed with an interventional procedure with the lowest possible exposure. The priority for a diagnostic image is that it is interpretable, which relies not just on the physics of the image (e.g. resolution and contrast) but also on factors such as how and where the data are displayed, the ambient environment, and the experience of the person reading the images. Reasonable reduction of the animal dose and improvement of study quality contribute to the optimisation of protection and safety by reducing doses received by both the animal patient and staff. (126) A highly important step in optimisation of radiographic procedures of any kind is to limit the exposed tissue volume to what is relevant for the clinical case at hand. In standard diagnostic radiology and interventional fluoroscopy, this should be achieved by appropriate beam collimation; in CT, this should be achieved by scan length limitation. These simple measures lower patient dose and – by reducing radiation scatter generated in the exposed tissues and materials – improve image quality and reduce the exposure of professionally exposed persons as well as members of the public. (127) A prerequisite for optimisation is a thorough knowledge of the doses associated with a given exposure situation, as well as the factors that influence this dose. Reported doses per image to persons participating in radiographic examinations of small and large animals (Ackerman et al., 1988; Seifert et al., 2007; Hupe and Ankerhold,
2008
,
2011; Barber and McNulty, 2012; Eckert et al., 2015), or per examination for personnel present during standing CT examinations of the equine head (Dakin et al., 2014), fall in the range from 0.1 to 34 µSv. Doses towards the higher end of the range are typically encountered when thicker body parts are being radiographed, such as the abdomen in large dogs, or the equine head, spine (especially thoracic and lumbar regions), and proximal extremities. While several of the above studies state that estimated annual doses will be well below regulatory limits for a given caseload, other studies of occupational doses in veterinary medicine have found that personnel doses may approach annual dose limits recommended by ICRP (Table 4.1) (Hernández-Ruiz et al., 2012; Canato et al., 2014). (128) Recently, dosimetric data have been published for veterinary interventional radiology and intra-operative fluoroscopically guided surgery, where there is close proximity between personnel and animal patients during exposure, often for extended periods (Sung et al., 2018; An et al., 2019; Hersh-Boyle et al., 2019). Reported operator dose levels may approach or even exceed regulatory limits, which emphasises the need for both quantitative radiation monitoring and the use of appropriate protective measures during these procedures. (129) With regards to dose to the animal patient, few dosimetric studies have been published. Primary beam doses or entrance surface skin doses, typically of the order of 1 mGy, have been reported with the aim of assessing their contribution to personnel dose (Veneziani et al., 2010; Barber and McNulty, 2012). However, dosimetric publications aimed at the radiation protection of the animal patient are emerging. Nemanic et al. (2015) addressed the potential of lead shielding to reduce dose to the animal during elbow radiography in dogs, and Hersh-Boyle et al. (2019) reported radiation exposure of dogs and cats undergoing intra-operative fluoroscopic procedures. In the latter study, doses up to 617.5 mGy were reported. However, systematic reporting of dose descriptors such as the dose area product and CT dose index for clinically relevant protocols, both within and between institutions, are lacking in veterinary medicine; hence DRLs or similar do not exist. Furthermore, while the relationship between these dose descriptors and radiation risk in the form of effective dose has been established in human medicine through the use, for example, of anthropomorphic or patient-based voxel phantoms (e.g., ICRP, 2009a) and Monte Carlo simulations, such links still have to be established in veterinary medicine (although, as mentioned earlier, some phantoms such as these have been developed for animals, including canines). The number of different species involved, as well as the range of patient sizes within a species, may be relevant challenges in veterinary medicine. (130) More dosimetric data are needed, both for personnel and animal patients, particularly for potentially high-dose procedures, such as interventional radiology and fluoroscopically guided surgical procedures. Furthermore, as CT interventional procedures become more prevalent in veterinary medicine, dosimetric aspects of these procedures should also be addressed. Systematic reporting of dose descriptors for clinically relevant protocols will be necessary to compare such protocols, both within and between institutions, and thus to optimise such protocols with respect to dose. The relationship between dose descriptors, organ doses, and associated radiation risk must also be determined for veterinary medicine.

The trefoil radiation warning sign.
6.2.3. Nuclear medicine
(131) Nuclear medicine procedures (e.g. Fig. 6.2) involve both external irradiation and contamination hazards. Unsealed sources such as radiopharmaceuticals have the potential to land on the skin or be taken directly into the body, so care should be taken to employ reasonable methods for reducing this risk of contamination. The radiopharmaceutical, the animal to which it has been administered, and all substances then produced by the animal, particularly urine, are also potential contamination sources. All of these should be properly managed, so facilities should be designed and operated (e.g. careful source management, regular checks on possible contamination of the work environment, waste collection and disposal) to reduce the risk of exposure and of unplanned release of any of these into the environment. Practical strategies for reducing time spent nearby, increasing distance, and using appropriate shielding should be applied at the same time to reduce exposure to external irradiation. (132) Safety measures to prevent contamination with radioactive substances can be implemented at the source or the worker, and are consistent with general industrial hygiene practices for protecting workers from other types of contaminants. Example methods for confining or containing a radioactive source include storing radioactive material in a secure, shielded location; limiting the handling of radioactive materials to well-defined areas within a practice (e.g. a secure drawing up area with appropriate mobile shielding); using secondary containment (e.g. trays, buckets) to limit the consequences of possible spills; and using a ventilated hood with sufficient and consistent air flow. Good housekeeping practices (i.e. cleanliness and organisation), regular radiological surveys, and detailed record keeping are also important for the prevention of contamination. (133) External radiation safety measures follow those described in Section 3.4.1. Specific examples in nuclear medicine include using an appropriately shielded syringe, using lead containers and/or hand carts to transport the radiopharmaceutical to the receiving patient, and taking one step back from the injected patient where possible. (134) The PPE used is essentially aimed at preventing contamination risks by the radioactive material involved. For example, when injecting, radiopharmaceutical impermeable gloves, a long-sleeved laboratory coat, and a face mask or shield should be worn to limit skin exposure in the situation of back pressure when injecting into a catheter. (135) With respect to the patient, it is important to be aware of the potential for deterministic effects in patients undergoing certain nuclear medicine procedures. These effects may be unavoidable to some extent (e.g. therapy). In nuclear medicine therapy, there may well be side effects; for example, effects on salivary glands when treated for thyroid cancer with radioiodine. Of course, there are also the potential consequences of extravasation (i.e. when the radiopharmaceutical ends up next to the vein through which it was supposed to enter the body) (van der Pol et al., 2017). (136) It should be kept in mind that the administered activity of a given radioisotope or radiopharmaceutical will, to a large extent, determine the radiation risks to the animal itself, to any humans involved, and to the environment. Prudence can provide insight into whether additional dose (activity) should be used to speed up a nuclear medicine procedure, or whether longer sedation or anaesthesia would be appropriate. Different situations require different approaches, always considering the ALARA principle. For example, there are two standard protocols in PET imaging, based on the timing of radiopharmaceutical injection and induction of anaesthesia. The protocol in which anaesthesia is induced prior to injection has a longer anaesthesia time (up to approximately 2 h) but lower radiation doses to personnel compared with the protocol in which anaesthesia is induced after injection. Reported doses per procedure to personnel participating in veterinary PET studies range from 0 to 30 µSv (Martinez et al., 2012; Hetrick et al., 2015), and estimates of the total annual effective doses to personnel associated with the latter protocol are well within the annual occupational dose limit (maximum approximately 5 mSv assuming 100 animal patients per year) (Martinez et al., 2014). Other considerations beyond anaesthesia time and radiation dose include keeping the animal as still as possible during the radiopharmaceutical uptake period in order to avoid unwanted uptake in active muscles. (137) In order to protect staff, members of the public, and the environment from the consequences of radionuclide administration to an animal, particularly after therapeutic procedures, the animal may need to be hospitalised so that its excrements may be collected and treated as radioactive waste. The risk of contamination from the animal itself usually subsides rather rapidly because of natural elimination, mostly by the kidneys through urine. However, it may take several days or even weeks before the dose rate emitted by the animal has fallen below the threshold values for its release and return home (Davila, 2019). (138) Hospitalisation, particularly for long durations, needs to be considered as a potential welfare issue for both the animal and its owner or carer (Graf, 1999; Boland et al., 2014; Johansson et al., 2014). Again, radiological protection concerns need to be balanced against and considered together with all other values at stake. Hospitalisation creates a stressful situation, especially in small animal pets (dogs, cats), as it has now been shown that animals have feelings, likely evolved to protect primary needs (Hewson, 2003; Lloyd, 2017). With the progressively more prominent place that animals, particularly companion animals, have gained in human society, it can be as stressful for pet owners to have their animal in the hospital for a long duration as it is for the animals themselves (McConnell et al.,
2011
,
2017; Amiot et al., 2016). (139) In view of the complexity of nuclear medicine procedures on animals, resulting, in part, from the need to manage external exposure and contamination risks simultaneously, veterinary nuclear medicine should only be performed by veterinarians and staff members that have completed specialist training programmes successfully. This is even more compelling for therapeutic applications.
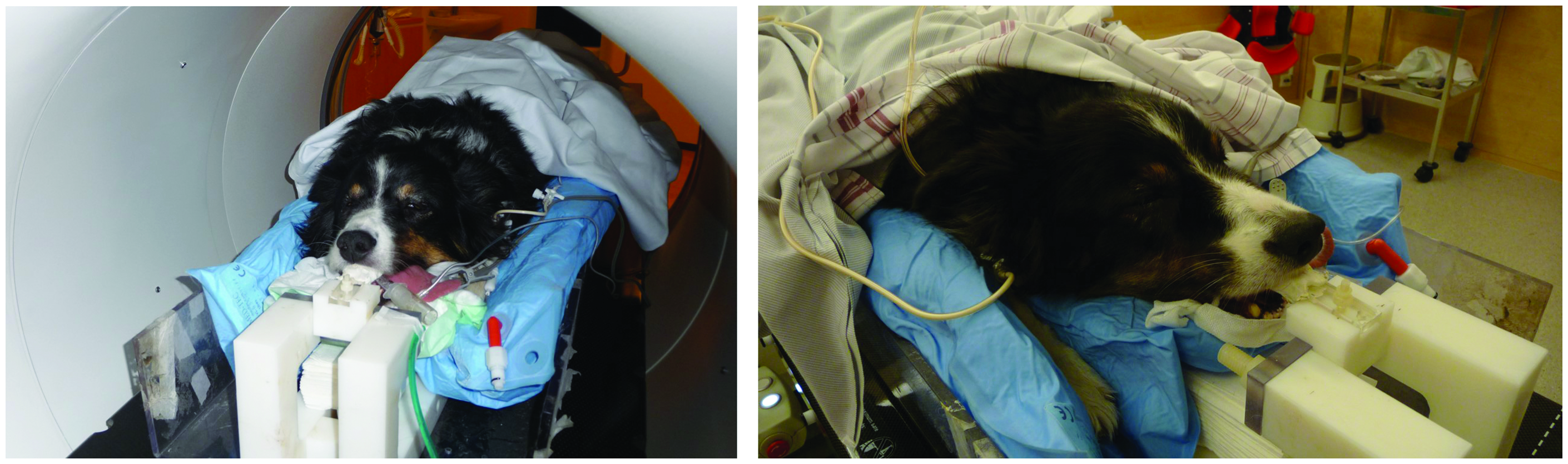
A canine patient being prepared for 18F-FDG positron emission tomography imaging in preparation for radiotherapy. Source: Jan Rødal, The Norwegian Radium Hospital, Oslo University Hospital, Norway (Rødal et al., 2010).

A feline patient exhibiting cutaneous mast cell tumour (left), undergoing brachytherapy (middle) in which a strontium-90 ophthalmic applicator is applied to the surface of the tumour. Six weeks post treatment (right), showing resolution of the mass. Note the hyperpigmentation and hair loss in the irradiated area. Source: Michael R. Broome, Advanced Veterinary Medical Imaging, Tustin, CA, USA (www.avmi.net).
6.2.4. External beam radiotherapy and brachytherapy
(140) Optimisation has a crucial role to play in all therapeutic applications of ionising radiation. As such treatments gain prevalence in veterinary care (Figs 6.3 and 6.4), this importance is increasing from both the perspective of the animals treated and the perspective of the professionals providing this type of care. For the animal patient, optimisation means making sure that, despite the very high doses delivered to the target volume and needed to obtain the desired therapeutic effect, the exposure of other tissues and organs is kept as low as reasonably achievable. The objective is that deterministic side effects are avoided to the extent possible, and that the overall exposure of healthy tissues, particularly radiosensitive tissues, is minimised in order to limit the probability for induction of delayed tissue reactions or second primary cancers. (141) The high doses and dose rates applied also have the potential to cause serious risks to staff members involved in these procedures. Blocked sources in remote after-loading or accidental ‘beam on’ situations in teletherapy could generate these types of risks, whereby other deterministic effects than just skin burns cannot be excluded. Strict procedures must be in place to allow the most optimal and safe use. Such complex and high-risk procedures should only be performed by veterinarians who have completed extensive education and training in radiological protection. From a veterinary care perspective, it may be preferable that the radiological practitioners responsible for these procedures are diplomates of speciality education and training programmes, bearing in mind the current curricula may be insufficient when it comes to addressing the radiation hazards specifically. The Commission therefore recommends that the providers of such education and training programmes better embrace radiological protection as an indispensable and integrated element of quality care.
6.3. Application of dose limits
(142) All individuals working with radiation in a veterinary practice must do so within the applicable legal requirements to ensure that neither occupational nor public radiation dose limits are exceeded. Although dose limits are maximum permitted values (Table 3.1), all doses are to be kept as low as reasonably achievable. Radiation workers should be subject to personal dose monitoring (where deemed appropriate by risk assessment or required by national legislation) to ensure that dose limits are not being exceeded, and working procedures are optimised. Except for pregnancy, the basis for dose limitation is the same for men and women, but once pregnancy is declared, additional controls need to be considered to protect the unborn child, reflected with a recommended fetal dose limit (ICRP, 2000). (143) The concept of ‘carer’ refers to an individual who may be (knowingly) exposed to radiation as a voluntary helper, providing support or care for a patient in a context that is not associated with their occupation (ICRP, 2007a). Carers are susceptible to being exposed to doses exceeding public dose limits (e.g. in some radiotherapeutic applications), which is considered appropriate within reason by the system of radiological protection. Although, to date, animals have not been legally recognised as ‘patients’ in veterinary practice, there is a direct benefit both to the animal patient and the owner in many circumstances. The Commission recommends that the concepts of patient and carer should be tailored to be applicable within reason in veterinary practice (i.e. animal patient and owner/handler). Although additional study is warranted, interest in modelling and/or measuring doses to owners/handlers from veterinary nuclear medicine procedures has seemingly increased over the past few years (e.g. Davila, 2019; Wendt et al., 2020; Arno and Smith, 2021; Smith and Krimins, 2022; Suwannasaeng et al., 2022). (144) If exposure of an owner/handler is deemed justified based on the prevailing circumstances, dose constraints should be used, potentially set above the public dose limit, to guide the associated optimisation of protection in a proportionate, practical way, noting that children and individuals not engaged in direct comforting or care should be treated as members of the public (subject to the public dose limit of 1 mSv year−1), consistent with human medicine (ICRP, 2007a). Of note, the suggested dose constraint, to be used flexibly, for carers of human patients is 5 mSv per episode for an adult (ICRP, 2007b).
6.4. Quality aspects of radiological protection and managerial responsibilities
(145) Radiological protection should be approached with a holistic perspective and graded approach, considering the full range of risks, benefits, and managerial issues associated with veterinary practice. Note that more detailed, practical guidance on general management of occupational health and safety is available elsewhere (e.g. HSE, 2013; IAEA, 2018; ISO, 2018). (146) Quality aspects of a sustainably effective radiation safety programme would include, broadly, consideration of equipment and facilities, education and training, assignment of responsibilities, procedural protocols, follow-up of outcomes, and dose and incident monitoring and reporting, as appropriate. Radiation safety should take a balanced place among all other safety considerations, both in the optimisation process and in general management approaches. These quality aspects should thus be included within the overall quality assurance programme, and are important to ensure and maintain the best attainable veterinary services. (147) When fixed installations are concerned, this starts with design and layout of the facility, considering the architectural requirements of the building and rooms, in particular those where radioactive sources will be stored and/or radiological procedures will be applied. Important considerations would include, for example, accessibility and access control, the optimal positioning of the equipment and animal, and the shielding requirements for the walls and doors. When mobile equipment is used, similar considerations come into play. In nuclear medicine, where unsealed radioactive sources are used and/or stored, specific attention should be devoted to the safe and secure storage of sources, along with the collection and further handling of radioactive waste. Considerations should also be given to minimisation of any spread of contamination (including in ventilation design), ease of decontamination and eventual decommissioning, as well as ease of operation and maintenance. In radiotherapy, room shielding and access control are of crucial importance, as is the safe and secure storage of radioactive sources that may be present (e.g. those used in brachytherapy) (IAEA, 2019). (148) The next step is to consider the applications themselves (i.e. the way in which ionising radiation is used). Tasks and associated responsibilities for each procedure or treatment should be assigned explicitly to staff members, so that they know exactly what is expected from them, and ensuring that all staff have had, and continue to have, adequate and regularly updated education and training commensurate with these tasks and responsibilities. Members of staff should have sufficient theoretical knowledge, practical skills, and the right mindset: the attitude to adopt a radiation safety culture while working with ionising radiation. (149) Equipment should work adequately; this is not limited to radiation emitting devices but should cover the complete imaging or treatment chain (e.g. image displays, planning software, etc.), along with the more obvious items such as shielding equipment, PPE, and dosimeters that serve to protect and monitor staff and, where applicable, members of the public assisting with a procedure. All equipment should be monitored and maintained regularly for adequacy of performance. Making sure that quality services are consistently provided safely makes the application of procedure guidelines or handbooks necessary. (150) In the event of incidents, accidents, or near-misses, a system should be implemented to ensure that these are investigated thoroughly. Any such events should serve as an opportunity for further improvement of radiation and general safety. Reporting of anything unusual should be encouraged, and actions to prevent any possible worsening or repetition should be taken until the situation has been fully understood and, whenever applicable, remediated. Learning from incidents, accidents, or near-misses could be much more profitable than just for the undertaking where such event occurred; they could, in fact, be shared between colleagues – for instance, through a platform offered by professional societies (e.g. ROSEIS) or international organisations such as IAEA (e.g. SAFRON, SAFRAD) – as a means to prevent the same or a similar event from happening in a comparable professional context elsewhere. (151) Systematic follow-up of procedure outcomes should be made in terms of their contribution to the cure pathway or to the adequacy of the suitability guidance delivered. Such follow-up would be a strong help in constructing or enlarging the evidence base for justification of animal exposures. (152) Finally, doses or dose indicators, as appropriate, to animals, staff, members of the public, and the environment should be assessed periodically, and monitored as applicable and needed. The systematic recording and follow-up of dose indicators, and intercomparisons with those registered by others in similar conditions, will contribute to optimisation of procedures, and will allow for the early detection of malfunctioning devices or the systematic performance of insufficiently optimised procedures.
7. SUMMARY OF RECOMMENDATIONS AND CONSIDERATIONS
(153) Veterinary use of radiation in the diagnosis, management, and treatment of disease has expanded and diversified considerably over the last few decades. Diagnostic imaging procedures are performed in an increasing number of situations where the animal’s health care is not necessarily the primary objective of the investigation. These practice changes have come with an increase in exposure-related risks to the veterinary professional staff, owners/handlers, other members of the public, the environment, and animals submitted to these procedures. Radiological protection concerns have therefore increased, and the many unique aspects of veterinary practice compared with human medicine add to these concerns. Radiological protection challenges specific to veterinary practice arise from the different combinations of individuals who may be involved, and from operational environments required when dealing with animals. (154) The priority of radiological protection is that of humans, but the animal’s exposure should also be the object of explicit attention from a radiological protection perspective in veterinary practice because, like humans, animals are subject to potential tissue reactions or stochastic effects resulting from exposure to radiation. Moreover, animals are not just objects, but sentient living beings able to feel and suffer. In veterinary practice, additional interpretation of the core and procedural ethical values of the system of radiological protection described in Publication 138 (ICRP, 2018a) includes animal welfare, sustainable development, solidarity, reverence for life, stewardship, respect for autonomy, and empathy. (155) As in all applications of ionising radiation, radiation safety management needs to be commensurate with the implied risks. As risks in veterinary applications have increased and diversified over the last few decades, radiation protection should get more, and more explicit, attention by the full application of the Commission’s system of radiological protection. Despite some differences, the radiological protection concerns originating from the use of ionising radiation in veterinary practice are, to a large extent, comparable with equivalent human medicine applications and non-medically-indicated human imaging. It is therefore recommended that veterinary applications should be treated in a comparable, proportionate way. This recommendation applies to the radiation safety requirements of the installations, but equipment should also meet the standards set for medical devices rather than just industrial standards. (156) It is recommended that the safe execution of veterinary applications should be guaranteed by the implementation of a quality assurance programme at managerial level with an applied graded approach. The analysis of incidents and accidents should be part of such a programme, as this may contribute to the continuous improvement of safety. International organisations and professional societies could set up and recommend the use of incident/accident reporting tools, particularly useful for interventional radiology, nuclear medicine, and radiotherapeutic applications, which could then provide lessons learned to all professionals in a ‘no shame–no blame’ setting. (157) Veterinarians and their co-workers should be sufficiently educated and trained in the radiation safety aspects of the radiological modalities they use. The Commission recommends that specific applications such as interventional radiology, nuclear medicine, and radiotherapy should be reserved for professionals that can demonstrate successful completion of an education and training programme which provides them with the necessary knowledge, skills, and attitudes to provide adequate care to the animals whilst taking responsibility for the radiation safety aspects of their activities. This responsibility covers staff and possible members of the public present, the individual animal, and the environment, where applicable. (158) The protection principles of justification, optimisation, and dose limits should apply in full to veterinary applications. The three levels of justification for radiological practice in medicine can also be applied to animal patients, while also considering if associated occupational and/or public exposures are justified. Level 1 requires that the proper use of radiation in veterinary practice does more good than harm to society. At Level 2, a specified procedure would be considered generically justified for a specified clinical objective if it will improve the diagnosis or treatment of a defined group of animal patients, or if it will provide necessary information about exposed animals. It is recommended that scientific organisations and specialist professional societies should provide guidelines that could assist clinicians in making appropriate choices; examples can be taken from referral guidelines and appropriateness criteria that have been in use in human medicine for years (ICRP, 2007b). Similar guidance would be particularly welcome when presale and insurability examinations on horses (or other animals, as relevant) are concerned. Level 3 justification requires that the application of a radiological procedure is judged to do more good than harm in the management of the individual animal patient. The balance of benefits and risks to the exposed animals, veterinary staff, animal owners or handlers, general public, society at large, and, where applicable, the environment must all be considered when determining if a given radiological procedure is justified in veterinary medicine. (159) Optimisation in veterinary care should be considered a process for ensuring that the likelihood and magnitude of exposures and the number of individuals exposed are as low as reasonably achievable, considering economic, societal, animal welfare, and environmental factors. Given the great number and diversity of elements to consider in any specific case, optimisation needs to be tailored to best fit, within the boundaries of what is prudent and reasonable, the needs of each case individually. This individual approach should first consider the clinical needs in a healthcare setting or the added value of a given test in the case of non-medical animal imaging procedures, but also the whole environment in which the procedure takes place (e.g. owner’s wishes, location and transport facilities, available equipment, etc.). The Commission acknowledges that managing the exposure of the individual animal as an integrative part of the optimisation process may be challenging, as this type of exposure has not previously been addressed specifically within the context of the system of radiological protection. Dose limits apply to those occupationally exposed and the general public, including the animal’s owner, but not the animal patient. (160) This publication, being meant for a broad audience, provides a general overview of the issues and concerns related to radiological protection in veterinary practice. The intent of the current publication is to acknowledge the importance and unique aspects of radiological protection in veterinary practice explicitly, and to lay the foundations inviting additional guidance in the future, similar to the approach for radiological protection in human medicine. For detailed, practice-oriented guidance, IAEA has developed a thorough report with modality-specific approaches to radiological protection (IAEA, 2021). The Commission hopes that highlighting radiological protection concerns and related knowledge gaps will inspire additional research and development related to the evidence-based use of ionising radiation in veterinary practice in support of the justification process; dedicated facilities and equipment; improved understanding of the radiosensitivity of different types of animals; and practice guidelines in support of exposure management and other relevant areas to promote health and safety of personnel, the general public, and the environment, while further improving the quality of care for the patients and healthy animals submitted to radiological procedures. This is sure to be a collaborative approach between veterinarians and their societies, research institutions, veterinary schools and colleges, radiation protection professionals, regulatory authorities, and other organisations.
Footnotes
4
See https://www.iaea.org/resources/rpop/resources/databases-and-learning-systems/safron, https://www.iaea.org/resources/rpop/resources/databases-and-learning-systems/safrad, and ![]() for SAFRON, SAFRAD, and ROSEIS, respectively.
for SAFRON, SAFRAD, and ROSEIS, respectively.
5
‘Last image hold’ refers to the feature of fluoroscopy systems in which the most recent image continues to be displayed on the monitor when fluoroscopy is stopped. See, for example, the discussion of Mahesh (2001).