
Abstract
The International Commission on Radiological Protection (ICRP) publishes guidance on protection from radon in homes and workplaces, and dose coefficients for use in assessments of exposure for protection purposes. ICRP Publication 126 recommends an upper reference level for exposures in homes and workplaces of 300 Bq m−3. In general, protection can be optimised using measurements of air concentrations directly, without considering radiation doses. However, dose estimates are required for workers when radon is considered as an occupational exposure (e.g. in mines), and for higher exposures in other workplaces (e.g. offices) when the reference level is exceeded persistently. ICRP Publication 137 recommends a dose coefficient of 3 mSv per mJ h m−3 (approximately 10 mSv per working level month) for most circumstances of exposure in workplaces, equivalent to 6.7 nSv per Bq h m−3 using an equilibrium factor of 0.4. Using this dose coefficient, annual exposure of workers to 300 Bq m−3 corresponds to 4 mSv. For comparison, using the same coefficient for exposures in homes, 300 Bq m−3 corresponds to 14 mSv. If circumstances of occupational exposure warrant more detailed consideration and reliable alternative data are available, site-specific doses can be assessed using methodology provided in ICRP Publication 137.
1. Introduction
For the first symposium of the International Commission on Radiological Protection (ICRP), Harrison and Marsh (2012) reviewed developments in the calculation of dose coefficients for isotopes of radon. Since that time, ICRP has issued Publication 126 (ICRP, 2014) giving guidance on protection, and Publication 137 (ICRP, 2017) which includes dose coefficients for the inhalation of 222Rn (radon), 220Rn (thoron), and 219Rn (actinon), together with their radioactive progeny. This article reviews the progression of ICRP recommendations from Publication 65 (ICRP, 1993), through Publications 103 and 115 (ICRP, 2007, 2010), to the most recent publications.
Radon, thoron, and actinon gases decay into a series of solid progeny that include alpha-particle-emitting radionuclides. It is these progeny that deliver the majority (>95%) of the dose received by the epithelial lining of the lung airways. For example, radon decays with a half-life of 3.8 days to progeny that include the alpha emitters 218Po (half-life 3.1 days) and 214Po (half-life 164 µs). As they are formed, progeny aggregate into clusters of approximately 1nm diameter, referred to as the ‘unattached fraction’, and also associate with existing aerosol particles in the air to form the ‘attached fraction’ with larger particle sizes of 10 nm to >1 µm (ICRP, 2017). In most circumstances, the concentration of progeny in inhaled air is less than that of the parent nuclide because of plate-out of particles on to surfaces and the effects of ventilation. This concentration difference between the gas and its solid progeny is quantified by the ‘equilibrium factor’ with typical values for radon and progeny in buildings of approximately 0.4. Air concentrations are measured in terms of the gas (Bq m−3) or of the alpha particle energy emitted by progeny [mJ m−3 or working level (WL)], related by the equilibrium factor. Measurements of exposure introduce time, as Bq h m−3, mJ h m−3, and working level month (WLM; 1 WL for 1 working month).
The inhalation of radon and progeny has been unique among internal exposures in that there is strong quantitative evidence of the relationship between exposures and the induction of lung cancer from studies of underground miners and people in their homes (UNSCEAR, 2009, 2019; ICRP, 2010; Laurier et al., 2020). In general, control of radon exposures can be based directly on measurements of air concentrations and the setting of reference levels for homes and workplaces (ICRP, 2007, 2014). However, dose estimates and dose coefficients are required for circumstances where, from the outset, the exposure is considered to be occupational, and in circumstances where exposures in workplaces remain persistently above the reference level despite remediation. Dose estimates may also be required in assessing public exposures in some circumstances; for example, when considering doses resulting from past contamination of buildings with radium isotopes.
Exposures to thoron, and particularly actinon, are substantially less important in most cases but can be significant in particular circumstances (ICRP, 2017). This article focuses on radon but also mentions thoron; information on actinon can be found in Publication 137 (ICRP, 2017).
2. ICRP Publications
2.1. Publications 65 and 103
Risks of lung cancer mortality from prolonged exposures to radon were estimated in Publication 65 (ICRP, 1993) from studies of cohorts of underground miners. The nominal ‘fatality and detriment’ coefficient obtained was 8 × 10−5 per mJ h m−3, which corresponds to a rounded value of 3 × 10−4 per WLM. A dose conversion convention was used in which this risk coefficient was divided by the detriment coefficients for all stochastic effects from Publication 60 (ICRP, 1991) of 5.6 × 10−5 per mSv for workers and 7.3 × 10−5 per mSv for members of the public. The conversion coefficients obtained were 1.4 mSv per mJ h m−3 for workers and 1.1 mSv per mJ h m−3 for members of the public (5 mSv per WLM and 4 mSv per WLM, respectively).
It was recommended that an action level for initiating intervention should be set nationally, corresponding to an effective dose of between 3 and 10 mSv year−1 for both homes and workplaces. The annual occupancy of homes is taken to be 7000 h and the working year as 2000 h; with the assumption of an equilibrium factor of 0.4, this range of action levels was calculated to correspond to radon concentrations of 200–600 Bq m−3 in homes and 500–1500 Bq m−3 in workplaces.
The 2007 Recommendations (Publication 103; ICRP, 2007) repeated the guidance provided in Publication 65 (ICRP, 1993), and referred to upper values of reference levels of 600 Bq m−3 for domestic dwellings and 1500 Bq m−3 for workplaces, corresponding to an effective dose of 10 mSv year−1. In addition, Publication 103 (ICRP, 2007) noted that an action level of 1000 Bq m−3 had been established in the International Atomic Energy Agency’s Basic Safety Standards (IAEA, 1996), and concurred that this could be used globally as the agreed entry point for occupational protection requirements. However, the existence of more recent epidemiological data was recognised, including results from cohort studies of miners and case–control studies of residential exposures. A task group started work in 2007 to review these data and provide the basis for updated recommendations.
2.2. Publication 115
The review of epidemiological studies of cohorts of underground miners provided in Publication 65 (ICRP, 1993) was updated in Publication 115 (ICRP, 2010), focusing on more recent studies with lower levels of radon exposure (see Laurier et al., 2020). Estimates of lifetime risks of lung cancer fatality based on the newer data were greater than those from earlier studies, and an increase in the lifetime risk coefficient was proposed from 8 × 10−5 per mJ h m−3 to 1.4 × 10−4 per mJ h m−3 (5 × 10−4 per WLM). Comparisons of studies of the risk of lung cancer in mines and in homes are not straightforward, mainly because of the different epidemiological designs of studies. However, comparisons were made with the results of a European pooling of studies of domestic exposures (Darby et al., 2005, 2006) and showed good consistency. The residential studies show a clear difference between smokers and non-smokers, with the risk of radon-induced lung cancer being increased substantially by smoking. The risk coefficient derived on the basis of the miner studies applies to a mixed population of smokers and non-smokers.
Publication 115 (ICRP, 2010) also included a statement on radon from ICRP, which adopted the revised risk coefficient proposed in the same publication, and made changes to reference levels from those recommended in Publication 103 (ICRP, 2007), confirming that an annual effective dose of approximately 10 mSv would almost certainly warrant action to reduce exposures. The upper reference level for radon exposures in homes was revised from 600 Bq m−3 to 300 Bq m−3. For protection of workers, the statement referred only to the level of 1000 Bq m−3 to be set as the entry point for applying occupational protection requirements.
No revisions of dose conversion coefficients for radon were provided in Publication 115 (ICRP, 2010), but instead the statement on radon signalled the intention that, in future, ICRP would provide dose coefficients for radon isotopes calculated using biokinetic and dosimetric models as for all other radionuclides.
2.3. Publication 126
Following the changes recommended in Publication 115 (ICRP, 2010), Publication 126 (ICRP, 2014) updated ICRP advice on protection of the public and workers against radon exposures. As in Publication 103 (ICRP, 2007), the advice centres around the optimisation of protection to maintain or reduce exposures to levels that are as low as reasonably achievable, taking economic and social circumstances into account. The objective is to reduce both the overall risk of lung cancer in the general population and the individual risk to the most highly exposed individuals. Radon exposures are classified as an existing exposure situation, as defined in Publication 103 (ICRP, 2007), and can only be controlled by actions on exposure pathways. Consequently, the appropriate reference level should correspond to an annual effective dose in the range of 1–20 mSv, and Publication 126 (ICRP, 2014) reaffirmed previous advice that a dose of the order of 10 mSv should be regarded as a benchmark for setting a reference level.
For the practical implementation of protection of the public, the upper reference level of 300 Bq m−3 for homes, as recommended in Publication 115 (ICRP, 2010), was confirmed in Publication 126 (ICRP, 2014), with the advice that national authorities should set a reference level in the range of 100–300 Bq m−3 depending on their particular circumstances. This is consistent with advice given by the World Health Organization (WHO, 2009) that the reference level should be set at 100 Bq m−3 if possible, but otherwise at a level not exceeding 300 Bq m−3.
For protection of workers, Publication 126 (ICRP, 2014) goes further than Publication 115 (ICRP, 2010), and recommends that the upper reference level of 300 Bq m−3 should apply generally to all buildings, and hence to workplaces, such as offices, as well as mixed-use settings, such as shops, restaurants, and schools. A graded approach is recommended in which protection is first optimised below the reference level. If remediation is unsuccessful in reducing exposures to below this level, a second step will be a realistic estimation of effective dose. If, despite all reasonable efforts to reduce radon exposures, the doses remain persistently above 10 mSv, the worker should be considered as occupationally exposed. It will only be in a relatively small number of occupations, such as underground mining, that the radon exposure will be considered from the outset to be the responsibility of the operating management, and hence categorised as occupational exposure.
Fig. 1 summarises the Publication 126 (ICRP, 2014) approach to protection from radon in buildings and other locations, applying to homes and workplaces. The intention is that an integrated approach will be taken to measures applied to buildings regardless of their use, and that the national authority will develop a radon protection strategy accordingly.
General approach for the management of radon exposures. ALARA, as low as reasonably achievable, taking economic and societal circumstances into account. *Workplaces where radon exposures are considered by national authorities to be occupational from the outset.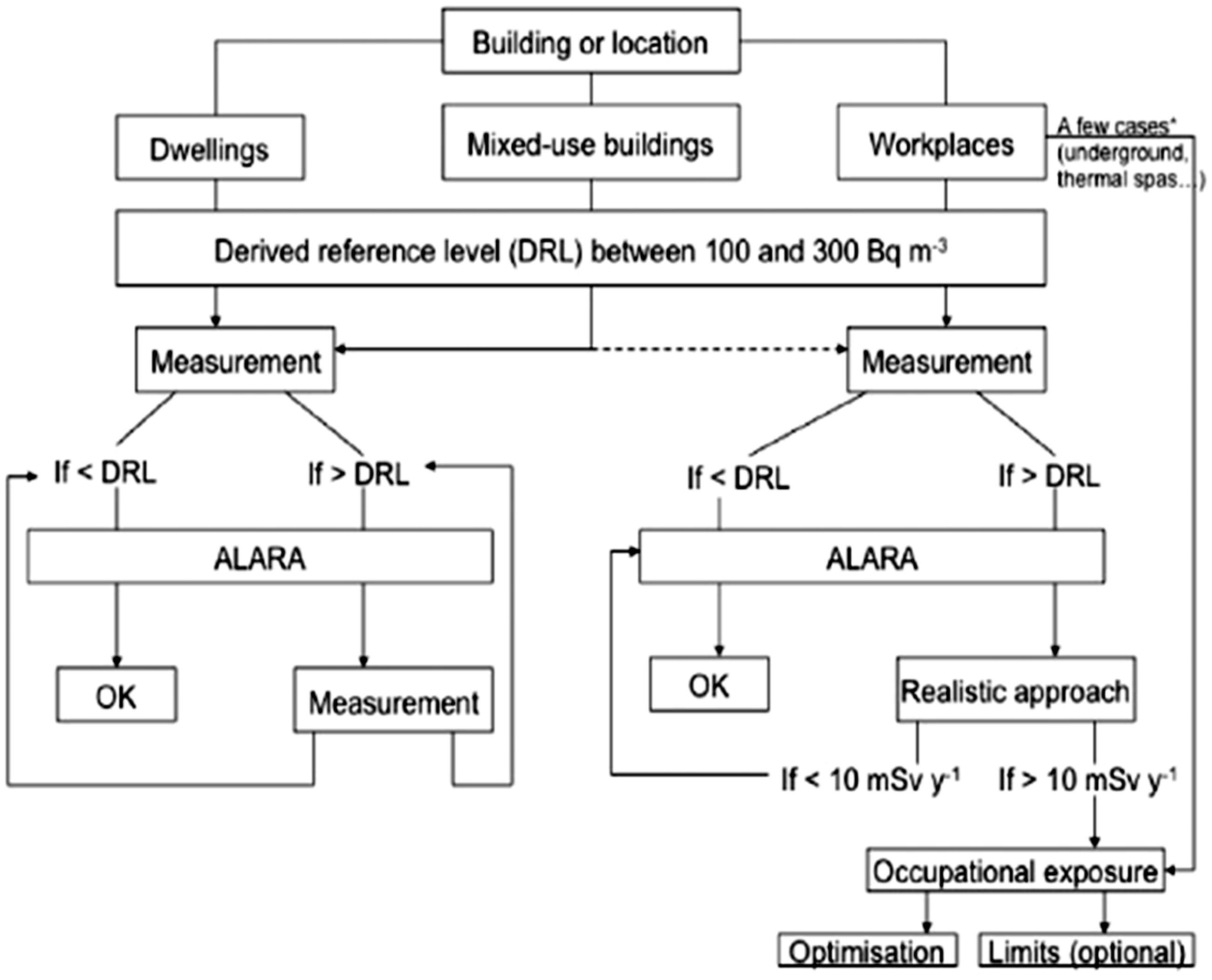
2.4. Publication 137
Publication 115 (ICRP, 2010) signalled the intention to provide dose coefficients for radon isotopes calculated using biokinetic and dosimetric models, and these are provided for occupational exposures in Publication 137 (ICRP, 2017). A publication providing dose coefficients for members of the public is in preparation. Publication 137 (ICRP, 2017) considers the inhalation of radon (222Rn, half-life 3.8 days), thoron (220Rn, half-life 56 s), actinon (219Rn, half-life 4 s), and their progeny; the ingestion of radon gas is also considered because of its solubility in water. Effective dose coefficients are included in the publication; organ and tissue equivalent doses coefficients are available in an electronic annex (www.icrp.org).
Effective doses from the inhalation of radon isotopes are due largely to the equivalent doses received by the lungs, resulting very largely from the deposition of solid progeny aerosol particles in the airways. However, principally for radon because of its longer half-life, absorption of the gas to blood results in smaller doses to other body organs and tissues. The deposition of progeny aerosol particles in the airways is dependent on the particle size distribution, including the unattached fraction which deposits more efficiently than the larger particles of the attached fraction. Breathing rate also determines intake and hence dose.
Effective doses from inhalation of radon and thoron in workplaces by a Reference Worker with an average breathing rate of 1.2 m3 h−1.
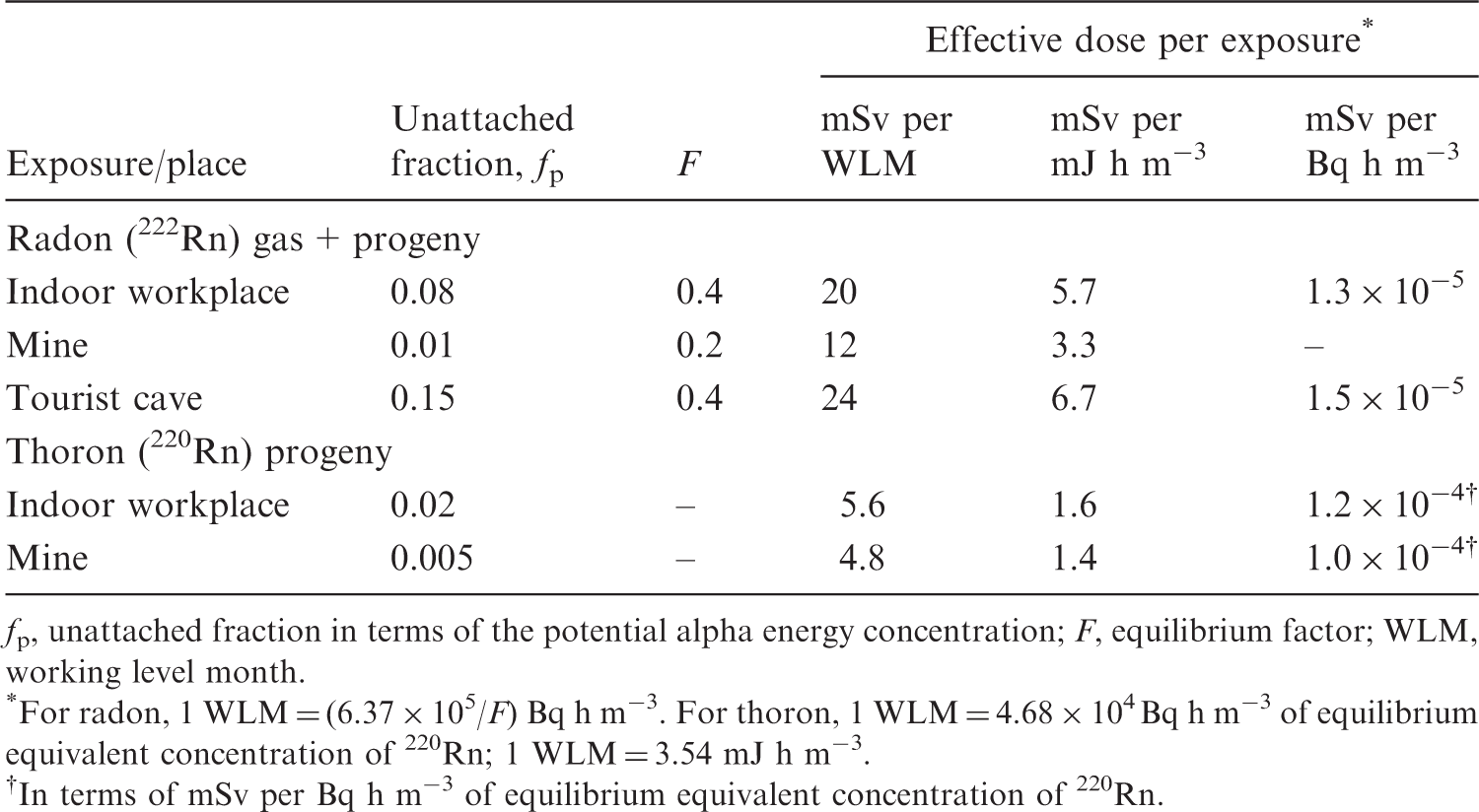
fp, unattached fraction in terms of the potential alpha energy concentration; F, equilibrium factor; WLM, working level month.
*For radon, 1 WLM = (6.37 × 105/F) Bq h m−3. For thoron, 1 WLM = 4.68 × 104 Bq h m−3 of equilibrium equivalent concentration of 220Rn; 1 WLM = 3.54 mJ h m−3.
†In terms of mSv per Bq h m−3 of equilibrium equivalent concentration of 220Rn.
Publication 137 (ICRP, 2017) noted that inhalation of radon and progeny is a special case for which there is good epidemiology on the risk of lung cancer as well as good dosimetric models. Applying the dose conversion convention to the revised risk coefficient of 1.4 × 10−4 per mJ h m−3 (5 × 10−4 per WLM) derived in Publication 115 (ICRP, 2010), and dividing by Publication 103 (ICRP, 2007) stochastic detriment coefficients of 4.2 × 10−5 per mSv for workers and 5.7 × 10−5 per mSv for members of the public, the conversion coefficients are 3.3 mSv per mJ h m−3 (12 mSv per WLM) for workers and 2.5 × 10−4 per mJ h m−3 (9 mSv per WLM) for members of the public. Publication 137 (ICRP, 2017) notes further that a more recent study of a large cohort of German uranium miners showed lower but broadly consistent results for the risk of lung cancer at lower levels of exposure (Kreuzer et al., 2015).
Taking account of all the available data, a single effective dose coefficient was recommended of 3 mSv per mJ h m−3 (approximately 10 mSv per WLM), applicable in the majority of circumstances of occupational exposure, with no adjustment for aerosol characteristics. In cases where aerosol characteristics are significantly different from typical conditions, sufficient, reliable aerosol data are available, and estimated doses warrant more detailed consideration, it is possible to calculate site-specific dose coefficients using the data provided in Publication 137 (ICRP, 2017) and the electronic annex. A second higher value of 6 mSv per mJ h m−3 (approximately 20 mSv per WLM) was referred to in Publication 137 (ICRP, 2017), but this may be seen as an example of requirements for more specific calculations when warranted.
Dose coefficients for the inhalation of thoron progeny are given for two situations of exposure: indoor workplaces and mines (Table 1). On the basis of these calculations, it is recommended that a single rounded value of 1.5 mSv per mJ h m−3 (5 mSv WLM−1) should be used for all situations of occupational exposure. This dose coefficient is considered to be applicable to the majority of circumstances with no adjustment for aerosol characteristics. As in the case of inhalation of radon progeny, if sufficient, reliable aerosol data are available and estimated doses warrant more detailed consideration, calculation of site-specific dose coefficients can be carried out using the data provided in Publication 137 (ICRP, 2017).
3. Discussion
Work is in progress to provide updated dose coefficients for members of the public and to include radon isotopes. Effective dose coefficients and organ/tissue equivalent dose coefficients will be calculated for the standard ages considered by ICRP: the 3-month-old infant; 1-year-, 5-year-, 10-year-, and 15-year-old children; and adults. For radon, age at intake has little effect on the dose per exposure because competing effects tend to cancel out, including the opposite effects of lower breathing rates and smaller tissue masses. For example, Marsh et al. (2005) calculated effective dose for different age groups using the ICRP respiratory tract model and reported values of 9.6–12.9 mSv per WLM. ICRP has already indicated in its ICRPaedia notes on radon (www.icrp.org) that the same overall value of the dose coefficient of 3 mSv per mJ h m−3 (approximately 10 mSv per WLM) will apply to members of the public as well as workers. Applying an equilibrium factor of 0.4, this corresponds to 6.7 nSv per Bq h m−3.
The upper reference level of 300 Bq m−3 for radon exposures in homes, as recommended in Publications 115 and 126 (ICRP, 2010, 2014), is established internationally and incorporated into the most recent Basic Safety Standards (IAEA, 2014). Taking the annual occupancy of homes as 7000 h, this corresponds to an effective dose of 14 mSv. The approach recommended in Publication 126 (ICRP, 2014) of also applying this reference level to workers is less firmly established, with the Basic Safety Standards (IAEA, 2016) continuing to advise a reference level of 1000 Bq m−3, although the European Council Directive (2012), for example, requires the use of 300 Bq m−3 (EU, 2014). For a working year of 2000 h, 300 Bq m−3 and 1000 Bq m−3 correspond to effective doses of 4 mSv and 13 mSv, respectively.
A United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) review of radon epidemiology and dosimetry should be published in 2020; a report to the United Nations General Assembly provides a summary of findings (UNSCEAR, 2019). UNSCEAR reviewed epidemiological studies of lung cancer in underground miners, and estimated lifetime risks using similar methodology to that applied in Publication 115 (ICRP, 2010). New data from the large German Wismut cohort were analysed (Kreuzer et al., 2015, 2018), as well as updated studies for other cohorts. The estimates of lifetime excess absolute risk ranged from 2.4 to 7.5 × 10−4 per WLM. Applying the dose conversion convention using Publication 103 (ICRP, 2007) detriment per Sv values, this range corresponds to ranges in dose conversion of 5.7–17.9 mSv per WLM for workers and 4.2–13.2 mSv per WLM for the whole population. The UNSCEAR review of published dosimetric assessments for exposures in homes, indoor workplaces, and mines showed a range of effective dose coefficients which, applying an equilibrium factor of 0.4, corresponds to 3–14 nSv per Bq h m−3, with arithmetic/geometric means of 6–7 nSv per Bq h m−3. UNSCEAR (2019) provides support for the ICRP effective dose coefficient of 3 mSv per mJ h m−3 (approximately 10 mSv per WLM), equivalent to 6.7 nSv per Bq h m−3 with an equilibrium factor of 0.4.