
Abstract
Whereas scientific evidence is the basis for recommendations and guidance on radiological protection, professional ethics is critically important and should always guide professional behaviour. The International Commission on Radiological Protection (ICRP) established Task Group 109 to advise medical professionals, patients, families, carers, the public, and authorities about the ethical aspects of radiological protection of patients in the diagnostic and therapeutic use of radiation in medicine. Occupational exposures and research-related exposures are not within the scope of this task group. Task Group 109 will produce a report that will be available to the different interested parties for consultation before publication. Presently, the report is at the stage of a working document that has benefitted from an international workshop organised on the topic by the World Health Organization. It presents the history of ethics in medicine in ICRP, and explains why this subject is important, and the benefits it can bring to the standard biomedical ethics. As risk is an essential part in decision-making and communication, a summary is included on what is known about the dose–effect relationship, with emphasis on the associated uncertainties. Once this theoretical framework has been presented, the report becomes resolutely more practical. First, it proposes an evaluation method to analyse specific situations from an ethical point of view. This method allows stakeholders to review a set of six ethical values and provides hints on how they could be balanced. Next, various situations (e.g. pregnancy, elderly, paediatric, end of life) are considered in two steps: first within a realistic, ethically challenging scenario on which the evaluation method is applied; and second within a more general context. Scenarios are presented and discussed with attention to specific patient circumstances, and on how and which reflections on ethical values can be of help in the decision-making process. Finally, two important related aspects are considered: how should we communicate with patients, family, and other stakeholders; and how should we incorporate ethics into the education and training of medical professionals?
1. Introduction
In many developed countries, medicine has become one of the greatest areas of government expenditure. This level of investment can only occur when the community regards it as important and in line with ethical expectations (Malone et al., 2018). Fuelled by an increased aversion of medical paternalistic attitudes, healthcare providers are pressured to provide more openness, accountability, transparency, and honesty. Likewise, there is now a high level of consensus in most political, social, and legal systems to respect the dignity of individuals, their autonomy, and their rights in general. All this, and other obligations including prudence, imposes new burdens on healthcare professions and practices, including radiological protection, which have not been accustomed to this type of expectation and related oversight (Malone and Zolzer, 2016; Parsa-Parsi, 2017).
1.1. Ethical values in radiological protection
The International Commission on Radiological Protection (ICRP) was founded at the second International Congress of Radiology held in 1928, in response to increasing concerns about the need for guidance to address health effects from ionising radiation in the medical community. For more than 90 years, ICRP has continued to provide recommendations and guidance to protect patients, workers, and the public. In this context, ICRP recently published Publication 138 which defines the ethical foundations of the system of radiological protection (ICRP, 2018). It proposes a set of values that are similar, but not identical, to the principles of biomedical ethics established by Beauchamp and Childress (1979). Publication 138 (ICRP, 2018) presents four core values: beneficence/non-maleficence, prudence, justice, and dignity. In addition, three procedural values that play a role in the practical implementation of the core values are also discussed: accountability, transparency, and inclusivity (i.e. stakeholder participation). For readers unfamiliar with these values, a definition of the main ethical values is given below (ICRP, 2018).
‘Beneficence’ means promoting or doing good, and ‘non-maleficence’ means avoiding causation of harm. Beneficence includes consideration of direct benefits, both for individuals and communities. The planned use of radiation, although coupled with known and unknown risks, can undoubtedly have desirable outcomes. These potential benefits have to be weighed against the potential harms. This is achieved in practice by: (i) ensuring that the use is justified; and (ii) ensuring that acute tissue effects are avoided or minimised, and stochastic effects are reduced as far as reasonably achievable while still providing the desired outcome given the prevailing circumstances (i.e. optimisation). From the viewpoint of evidence-based medicine and public health, the application of beneficence and non-maleficence requires an evaluation of the benefits, harms, and risks. This is neither straightforward nor sufficient. A variety of social, psychological, and cultural aspects also need to be considered. Furthermore, there may be disagreement on what matters most or on how to value or weigh these factors. In this respect, it is worth recalling the World Health Organization’s (WHO) definition of health: ‘Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’ (WHO, 1948).
Prudence is the ability to make informed and carefully considered choices without full knowledge of the scope and consequences of actions. It is also the ability to choose and act on what is in our power to do and not do. The system of radiological protection is based on solid scientific evidence, but the remaining uncertainties at low levels of exposure necessitate value judgements. Decision-making requires prudence as a central value, but policy makers generally refer to the precautionary principle instead. This principle, which states that lack of full scientific certainty shall not be used to justify postponing appropriate preventive measures ‘where there are threats of serious or irreversible damage’, has been much debated in connection with the ethics of decision-making in recent years. This is also at stake in the domain of radiological protection (Streffer et al., 2004). Neither prudence nor the precautionary principle should be interpreted as demanding zero risk, choosing the least risky option, or requiring action just for the sake of action. Instead, potential risk should always be considered in the context of benefit, either directly to the exposed individual or to the community at large. The experience of over half a century of applying the optimisation radiation protection principle can be considered as a reasoned and pragmatic application of prudence and/or the precautionary principle.
Justice is usually defined as fairness in the distribution of advantages and disadvantages among groups of people (distributive justice), fairness in compensation for losses (restorative justice), and fairness in the rules and procedures in the processes of decision-making (procedural justice). The system of radiological protection aims to ensure that the distribution of individual exposures meets two principles of distributive justice. First, the principle of equity reflects the personal circumstances in which individuals are involved. It is the role of dose constraints and reference levels to reduce the range of exposures to individuals subject to the same exposure situation. Second, the principle of equal rights guarantees equal treatment for all individuals belonging to the same exposure category in planned exposure situations. It is the role of dose limits to ensure that all members of the public, and all occupationally exposed workers, do not exceed the level of risk deemed tolerable by society and recognised in law (Hansson, 2007). Note that dose limits do not apply for patients because the method of choice for diagnosis or treatment may result in higher exposures, and therefore such limits would do more harm than good (ICRP, 2007). Equality is therefore not deemed a prime consideration. Reference levels are intended to at least reduce the variations between patients with similar size and conditions.
Dignity is an attribute of the human condition; the idea that something is due to a person because she/he is human. This means that every individual deserves unconditional respect, irrespective of personal attributes or circumstances such as age, sex, health, disability, social condition, ethnic origin and/or religion, etc. This idea has a prominent place in the Universal Declaration of Human Rights which states that ‘All human beings are born free and equal in dignity and rights’ (United Nations, 1948). Personal autonomy is a corollary of human dignity. This is the idea that individuals have the capacity to act freely (i.e. to make uncoerced and informed decisions). Respect for human dignity was first promoted in radiological protection as ‘informed consent’ in biomedical research, which means that a person has ‘the right to accept the risk voluntarily’ and ‘an equal right to refuse to accept’ such risks (ICRP, 1992). In a number of different ways, the system of radiological protection actively respects dignity and promotion of the autonomy of people facing ionising radiation in their daily lives.
In addition to the core ethical values, Publication 138 (ICRP, 2018) sets out a number of requirements relating to the procedural values and organisational aspects of radiological protection: accountability, transparency, and inclusivity. All are inter-related and have strong ethical aspects.
Accountability can be defined as the procedural ethical value that people who are in charge of decision-making must answer for their actions to all those who are likely to be affected by these actions. Transparency is also part of implementing the value of procedural justice. It concerns the fairness of the process through which information is intentionally shared between individuals and/or organisations. Transparency does not simply mean communication or consultation. It relates to the accessibility of information about the activities, deliberations, and decisions at stake, and also to the clarity, practicality, and honesty with which this information is transmitted.
The value of inclusivity is usually presented with the phrase ‘stakeholder participation’, which is the way the value is applied in practice. Stakeholder participation, also noted as stakeholder involvement or engagement, means ‘involving all relevant parties in the decision-making processes related to radiological protection’ (IRPA, 2008). Empathy was not proposed explicitly as a procedural value in Publication 138 (ICRP, 2018), but it deserves to be introduced here because it is linked to the concept of inclusivity. Empathy can be defined as the capacity to understand what another person is experiencing from within the other person’s frame of reference, or, more prosaically, the capacity to place oneself in another’s shoes. So far, empathy has not been widely accepted as an ethical value, yet it plays an essential role in situations where perceived and factual risks often diverge.
1.2. Application of ethics in radiation medicine
Once the ethical framework of radiological protection had been established, ICRP mandated Task Group 109 (TG109) to advise medical professionals, patients, families, carers, the public, and authorities about the ethical aspects of radiological protection of patients in the diagnostic and therapeutic use of radiation in medicine. Occupational exposures and research-related exposures are not within the scope of this task group.
TG109 is composed of a group of medical professionals and academics, a patient advocate, and an ethicist. It has held two face-to-face meetings and benefitted from an international stakeholders’ workshop organised on the topic by WHO in Geneva in September 2019.
The goal of this article is to report on the approach proposed by TG109. Although this is a work in progress, TG109 has already identified that the presence of guidelines is not in itself sufficient to ensure that practice will be ethically acceptable. Ethical values together with critical thinking need to be deeply rooted in health professionals in order to be effective. Thus, the task of TG109 includes not just identifying the guidelines, but also suggesting related supportive actions, including education, ongoing training, and audit to ensure that an ethics curriculum becomes a widely accepted part of practice and professional culture. The outline of the current version of the working document is presented in Fig. 1.
Present outline of the working document of the International Commission on Radiological Protections’s Task Group 109.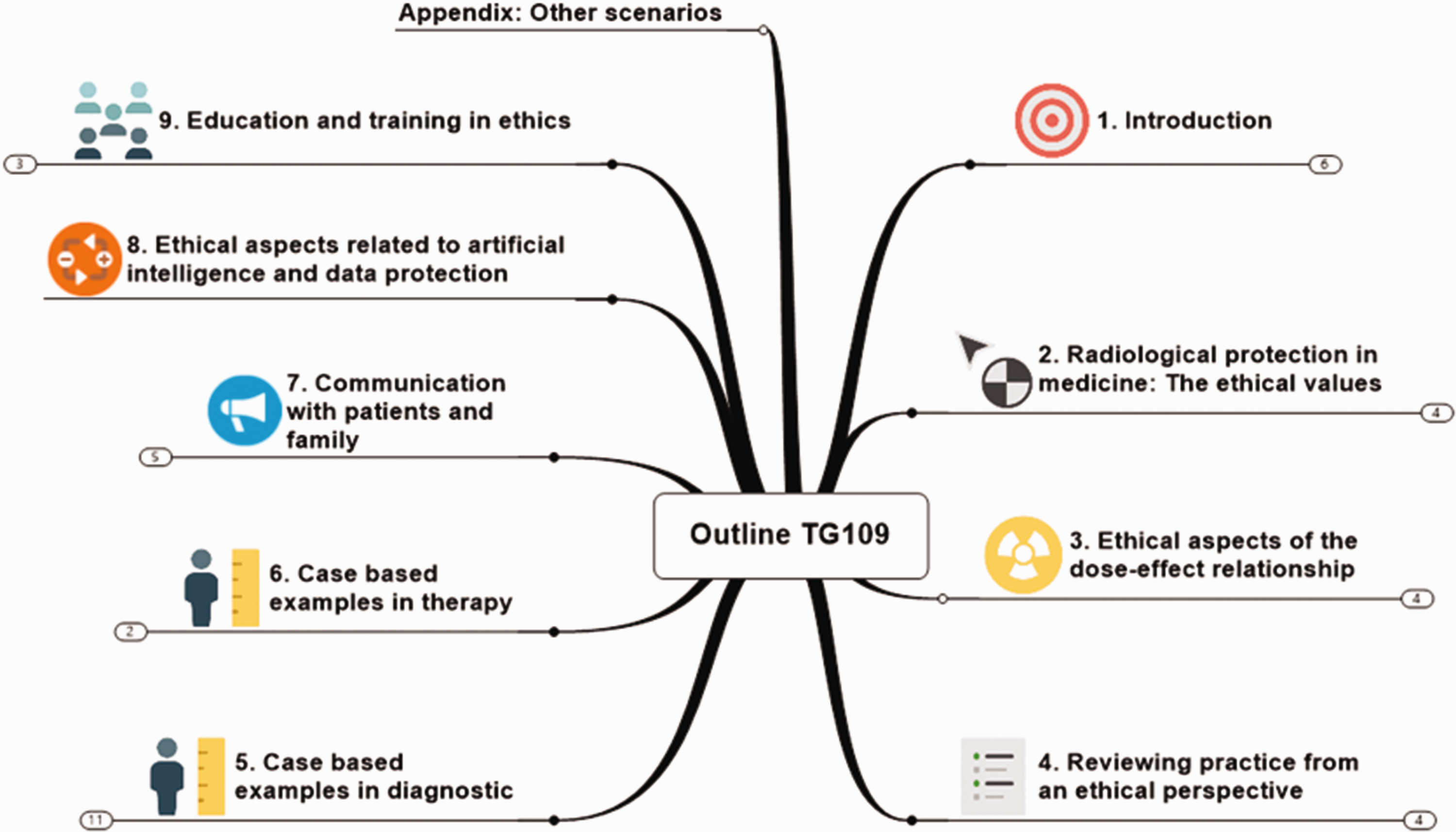
2. Status of the working document
2.1. Ethical aspects of the dose–effect relationship
If radiological imaging and therapy involving ionising radiation had no negative biological effects, their use in medicine would require much less ethical consideration, as is the case with ultrasound imaging for example. Of course, there would still be cost and justification considerations which apply to all medical resources. The type of effects (e.g. erythaema, organ breakdown, cancer, etc.), together with their potential for harm (i.e. severity or likelihood), are directly related to acceptance of the benefit that can be expected from a medical exposure. Appropriate information of the possible unwanted health effects arising from the use of ionising radiation is an essential step in the acceptance of a medical procedure by the patient. This must be complemented with information about the expected benefits of the radiological procedure, as well as the potential consequences of not performing that examination or initiating the proposed treatment. This follows directly from the value of dignity.
Another ethical issue related to the dose–effect relationship comes from the fact that the risk tends to decrease with age, with some exceptions (e.g. pregnancy, breast feeding). This justifies why specific precautions should be applied to children. However, the same reasoning could also have implications for the elderly, where the non-maleficence of an exposure tends to increase with age.
Finally, and despite the fact that scientific knowledge on the effects of ionising radiation is better compared with knowledge on other sources of hazards, there are two large sources of uncertainty. The first concerns the dose–effect relationship at low dose at the population level; it cannot be asserted with certainty that a dose below 50 mSv delivered to each individual of a population will result in a measurable increase in the number of induced cancers. The ethical value of prudence is usually used to justify that any level of dose could be harmful. The second large source of uncertainty concerns the variation of radiosensitivity among individuals. Except for a few specific cases (e.g. patients with ataxia-telangiectasia), it is very difficult to know if a patient is more or less sensitive to ionising radiation than the average population. Here again, one should resort to the value of prudence.
Estimates of radiation-induced harms, including deaths and future cancers, hide notable uncertainty about their origins, significance, and how they might be presented to patients and other health professionals. For example, the importance of a risk of death of a few percent 10 years into the future may be seen very differently by a young mother and an octogenarian man with multiple health conditions. Likewise, there are great differences between the way in which risks are calculated and benefits are estimated; frequently, it is very challenging to make benefit/risk estimates with sound evidence or that gain consensus amongst colleagues. Similar considerations may apply to comparisons with benefits and risks from other treatments/procedures and/or medications.
2.2. Evaluation method
In general, when evidence is lacking from a guideline or the scientific literature, providers often turn to talking with their colleagues and relying on their clinical experience and ethical training. There is very little literature to identify when ethical evaluation is needed for medical applications of radiation. Self-assessment of compliance with the key ethical values would have great benefits in improving sensitivity to ethical issues. A thorough assessment of ethical compliance supported by the advice of an ethical committee would not be practicable nor useful in every single scenario where radiological protection principles have to be applied for the medical use of radiation, and would not be justified. In unusual scenarios, medical providers may consult with ethics committees for help in resolving complex patient care difficulties. More practical, however, is the incorporation into daily practice of an approach to identify the specific situations where ethical dilemmas may arise in order to perform a more comprehensive ethical evaluation.
As such, a relatively simple tabulated evaluation method is proposed to perform a quick self-assessment of the compliance/non-compliance of a given scenario with six key ethical values (Malone and Zölzer, 2016). It is intended to be applied by healthcare providers prescribing and/or performing radiological medical procedures. Based on this initial assessment, further actions can be considered, including evaluation of the particular case by the relevant ethics committee or radiation protection committee.
The method asks the stakeholder to score a given scenario on a six-point scale as compliant (or non-compliant) with the values identified. Compliance with a value is indicated as being strong (☺☺), weak (☺), or neutral (−). Likewise, non-compliance is indicated as strong (☹☹), weak (☹), or neutral (−). Some aspects of scenarios can demonstrate compliance with a value when considered from one perspective, and non-compliance when considered from another. Thus, it is possible to score both ☺☺/☺ and ☹☹/☹ for the same value. The method is open to development in terms of incorporating additional values, or being used serially to assess how situations appear when assessed from different perspectives. It can also be used as a teaching tool; for instance, to illustrate balancing values. It should be noted that there may be no correct answers to this method. Different observers may come to different conclusions for a variety of reasons that are all considered valid.
2.3. Specific situations
2.3.1. General approach
In order to be useful for the day-to-day stakeholders, the report proposes to consider specific situations in radiological diagnostic imaging and therapy involving ionising radiation. Although it is planned to include therapeutic procedures at a later stage, at the time of writing of this article, only the imaging and interventional procedures have been established for 10 situations:
Adult population Pregnant patient Breast feeding Paediatric exposure Elderly exposure End-of-life medical radiation imaging Chronic disease Asymptomatic individual health assessment Organised population screening Carers' and comforters' exposures
For didactic reasons and in order to show how ethics can be addressed in practice, each situation will be discussed in three steps. First, a realistic scenario that contains interesting ethical issues will be presented. Second, a table containing a possible ethical grading of the scenario will be proposed and discussed. Finally, a more general discussion about each situation will be presented.
In this article, a scenario regarding the exposure of an elderly patient is presented as an example. It is important for the reader to realise that this evaluation necessarily contains aspects which are not fully determined. This highlights a level of uncertainty encountered in practice, and the value of having different points of view when ethical issues are complex.
2.3.2. Example of elderly exposure scenario
During his annual health check, Mr Michael, 66 years of age, is given an abdominal ultrasound scan for liver and gallbladder analysis. His doctor prescribes him a computed tomography (CT) scan with contrast agent due to the suspicion of a potential kidney problem. The patient is not given any specific information about the risk and benefit of the CT examination, which is considered as a routine examination to verify the status of his kidney. The CT scan clearly confirms the presence of an early-stage tumour in the right kidney. This is followed, within 3 days, by an interview with the urologic surgeon, who carefully and completely explains the tumour context and suggests that tumour removal surgery should be performed as soon as possible. Thanks to his private insurance, Mr Michael can skip the typical 2-month waiting list, and his operation is performed within 1 week of the meeting with the surgeon. After surgery, the patient is informed that the tumour was small and well located. It is therefore decided not to carry out radiotherapy or other radiological treatments. However, in order to follow the local guidelines, a follow-up CT scan is prescribed every 4 months for 2 years.
Grading of the elderly exposure scenario.

2.3.2.1. Beneficence/non-maleficence
The benefit of performing the first CT scan can be considered as fully justified because the ultrasound examination could not provide adequate information. Furthermore, the skills and high level of professionalism of the medical team cannot be questioned. There is therefore strong compliance with beneficence/non-maleficence (☺☺).
However, some non-compliance with this ethical value can be identified. Mr Michael received no warning about the risk of ionising radiation, and he was not informed about the postoperative CT checks. That made him feel like a passive recipient of health care and may have contributed to induce a persistent state of anxiety. We therefore propose to score non-compliance with beneficence/non-maleficence as weak (☹).
2.3.2.2. Prudence/precaution
At older ages, patients tend to become less sensitive to the effects of ionising radiation. Taking into consideration that the CT scan is recognised to be a highly effective tool for Mr Michael’s health situation, we consider that there was adequate and sufficient prudence to keep any foreseeable possible developments under control. We therefore propose to score compliance with prudence/precaution as strong (☺☺), with a neutral score for non-compliance (−).
2.3.2.3. Justice
From a pure radiological protection point of view, Mr Michael’s examinations were performed in due time, followed the recognised guidelines, and did not differ from what would have been done for other patients in his country. We therefore propose to score compliance with (distributive) justice as strong (☺☺).
The fact that Mr Michael was not considered as a full partner of the decision process shows some non-compliance in terms of procedural justice. Furthermore, the fact that he could skip the waiting list thanks to his private insurance draws some ethical issues regarding distributive justice. However, this latter point is out of the scope of radiological protection, and we propose to score non-compliance with justice as weak (☹).
2.3.2.4. Dignity/autonomy
The fact that Mr Michael was treated quickly and efficiently shows that he was respected as a person by the medical staff. We therefore propose to score compliance with dignity as weak (☺).
On the other hand, there was some serious non-compliance with autonomy. Mr Michael was barely involved in the available therapeutic and follow-up choices, and no spontaneous information about the risk associated with ionising radiation was given to him. This is unfortunate because the patient felt that he was just a receiver of health care and not an actor of his life. This led to notable concern on his part that he might have been exposed to undue risk without his consent. If this had been different, this could have increased his self-esteem, improved his quality of life, and therefore had a good influence on the treatment and his health in general. This is why we propose to score non-compliance with dignity and autonomy as strong (☹☹).
2.3.2.5. Transparency/accountability
Mr Michael was not given a spontaneous, complete, and comprehensible picture of his situation. Presently, many hospitals invite their patients to look at their website or provide printed leaflets to inform them about common procedures and radiation risk. This lack of transparency and accountability towards Mr Michael led us to score non-compliance with transparency and accountability as weak (☹).
2.3.2.6. Inclusivity/empathy
Mr Michael’s strong need for information and desire to be involved could have been anticipated by applying the value of empathy. Indeed, it is reasonable to think that the health professionals considered in their soul and conscience that the proposed treatment was the best and only reasonable decision. However, visibly, Mr Michael had concerns that were not imagined by the professionals. For this reason, we propose to score non-compliance with inclusivity and empathy as strong (☹☹).
3. Conclusion
A set of specific ethical values for radiological protection were proposed in Publication 138 (ICRP, 2018). This article presents the state of work of TG109, which aims to advise medical professionals, patients, families, carers, the public, and authorities about the ethical aspects of radiological protection of patients in the diagnostic and therapeutic use of radiation in medicine. It is proposed to use a relatively simple tabulated evaluation method to perform a series of self-assessments of the compliance/non-compliance of a given patient scenario with six key ethical values. The case of an elderly exposure is presented as an example. In the final report, it is planned to treat a wide range of practical situations typically encountered in medicine using radiological imaging and therapy. Each situation will be initiated by a realistic scenario, where the evaluation method will help the reader to identify the relevant ethical issues. This will serve as an introduction to a more general discussion about each situation. The final report also plans to address other key topics, such as communication with patients and family, artificial intelligence, and education and training of health professionals.
Footnotes
This paper does not necessarily reflect the views of the International Commission on Radiological Protection.