
Abstract
The accident at Fukushima Daiichi nuclear power plant contaminated the soil of densely populated regions in Fukushima Prefecture with radiocaesium, which poses risks of internal and external exposure to the residents. However, extensive whole-body-count surveys have shown that internal exposure levels of residents are negligible. In addition, data from personal dosimeters have shown that external exposure levels have decreased, so the estimated annual external dose of the majority of people is <1 mSv in most areas of Fukushima. Despite these reassuring data, many problems remain in Fukushima, many of which are psychosocial rather than radiological. This article will discuss the roles of measurement and communication in the postaccident phase based on 5 years of experience.
1. INTERNAL EXPOSURES
After the accident at Fukushima Daiichi nuclear power plant (FDNPP), there was considerable confusion in the assessment of internal radiation exposures of Fukushima residents. Nowadays, it is known that the internal exposure risks of Fukushima residents are negligible (Hayano et al., 2013; Sato et al., 2013; Miyazaki et al., 2014; Hayano, 2015a). However, this does not mean that the problems are over; in particular, families with children remain unconvinced.
1.1. Initial confusion: are the numbers correct?
The author started to collaborate with medical doctors in Fukushima in Summer 2011, when Dr Tsubokura of Minamisoma Municipal General Hospital (MMGH) and Dr Miyazaki of Fukushima Medical University made contact on Twitter (@hayano), and asked for help with the evaluation of data they had obtained using a chair-type whole-body counter (WBC) in July 2011. This WBC was brought to MMGH, located 23 km north of FDNPP, at the end of June 2011. This was the first WBC unit installed in Fukushima Prefecture after the accident, and was provided on loan for 3 months from Ningyo-toge Environmental Engineering Centre of the Japan Atomic Energy Agency.
Fig. 1 (left) compares gamma-ray spectra obtained with no one sitting on the WBC chair (black) and with a high-risk subject sitting on the WBC chair (red). The radiocaesium peaks are lower when a subject is sitting in the chair compared with background radiation alone. This is because this type of WBC does not have sufficient shielding, and the human body partially shields the environmental background radiation. In 2011, it was very difficult to assess the degree of internal contamination of Minamisoma residents correctly using such data. Later, the data were analysed successfully, and the committed effective dose to adult high-risk residents of Minamisoma was estimated to be 0.35 mSv at most (Hayano et al., 2014b; UNSCEAR, 2015).
(left) Typical gamma-ray spectra measured at Minamisoma Municipal General Hospital in July 2011. Black points represent the background spectrum, and red points represent the data for subjects. Source: Hayano et al. (2014b). (right) Distribution of radiocaesium body burden (Bq kg−1) vs age among residents of Fukushima city in December 2011. The average appears to be approximately 20 Bq kg−1, but this was subsequently found to be due to incorrect background calibration.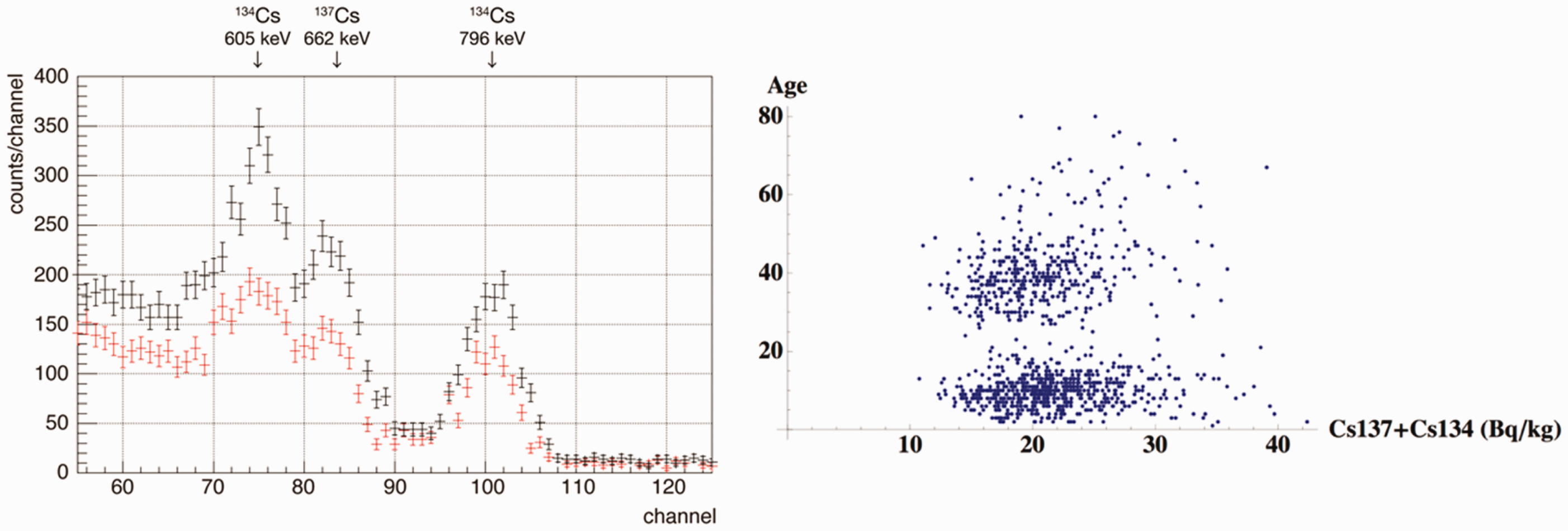
Fig. 1 (right) also shows a problem with a chair-type WBC encountered in Fukushima city in late 2011. A non-governmental organisation measured approximately 1000 residents of Fukushima city, and data suggested an average body burden of approximately 20 Bq kg−1. However, this was due to improper subtraction of background radiation.
As these examples show, when the whole environment is contaminated, chair-type WBCs with insufficient shielding are difficult to operate. This situation was much improved using the FASTSCAN (Canberra Industries Inc., Meriden, CT, USA) with 4 tons of shielding. The FASTSCAN measures a subject in a standing position in 2 min and became a de-facto standard; the first unit was installed at MMGH in September 2011, the second was installed at Hirata Central Hospital (45 km southwest of FDNPP) in October 2011, and there are now more than 50 units throughout Fukushima.
However, the data shown in Fig. 2 from the FASTSCAN at Hirata Central Hospital reveal a further problem. There was a sharp decrease in the percentage of radiocaesium detected in March 2012, when all subjects were asked to change into hospital gowns for scanning; this suggests that the radiocaesium detected before March 2012 must have been mainly due to contamination on clothing.
Percentage of radiocaesium detected at Hirata Central Hospital. After March 2012, when all subjects changed into hospital gowns, the percentage decreased considerably. Source: Hayano et al. (2013).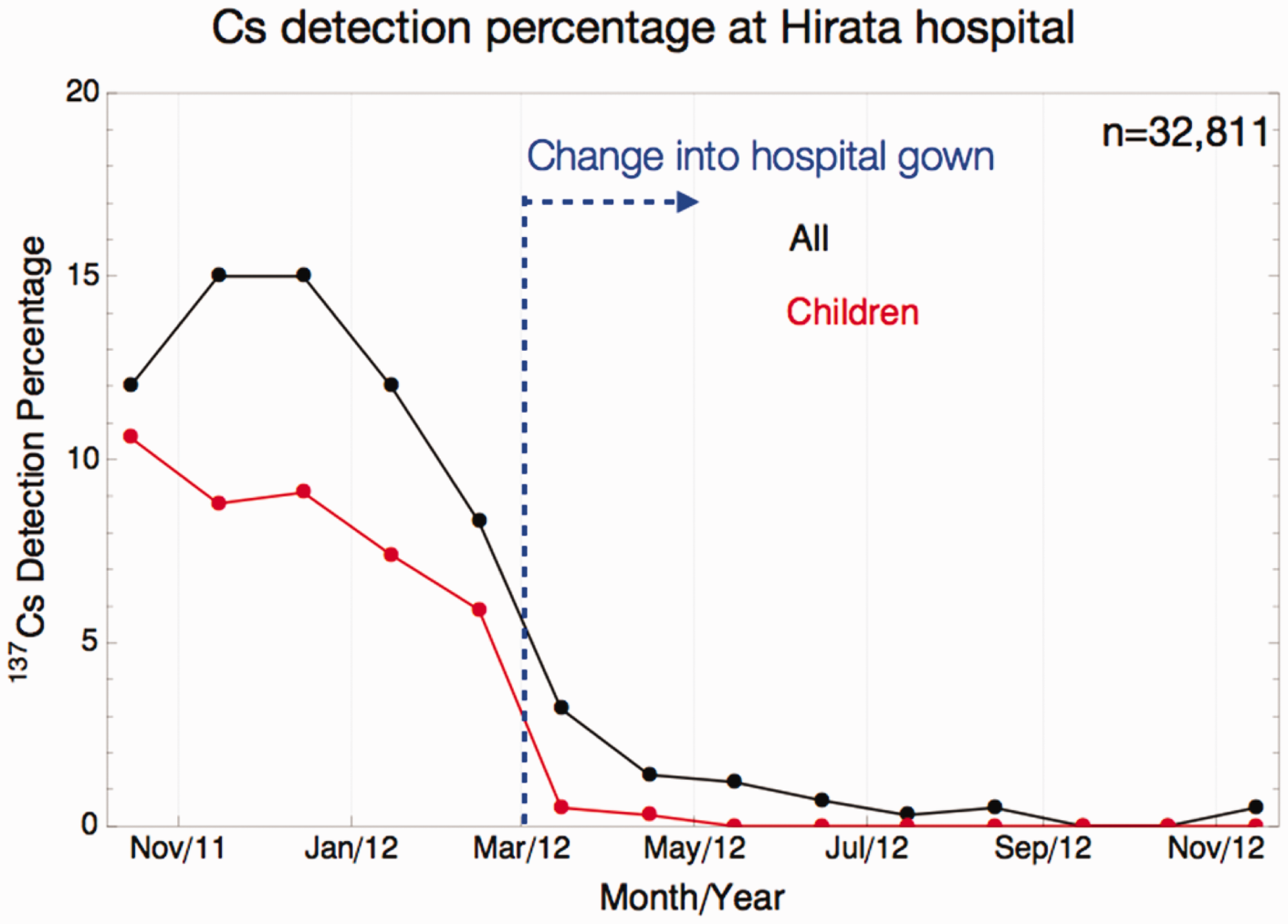
1.2. Body burdens of Fukushima residents are lower now than in the 1960s
After correcting for this (and other minor problems), more than 30,000 people were scanned at Hirata Central Hospital in 2012; 100% of children and 99% of adults were below FASTSCAN’s detection limit of 300 Bq per body (Hayano et al., 2013). For comparison, the body burden of an adult male in Japan in 1964 was 535 Bq per body (Uchiyama et al., 1996).
When measuring a large number of people for internal contamination, data show a log-normal-like distribution, i.e. a long tail (Hayano, 2015a). However, the percentage of people with a body burden exceeding a few thousand Bq per body in 2012 was very small (approximately 0.01%) at Hirata Central Hospital. In these cases, a germanium semiconductor detector was used to measure the foodstuffs they consumed, and these individuals reported that they regularly ate items for which contamination advisories have been issued (e.g. wild mushrooms, wild boar, freshwater fish, etc.). They were advised to avoid consuming such foodstuffs, whereupon their body burdens decreased at rates consistent with the biological half-life. In this sense, measurement and communication did reduce the internal radiation exposures of those people. However, in retrospect, as the committed effective doses of these individuals were below 1 mSv year−1, strict control may not have been necessary.
1.3. The BABYSCAN story
Data show that internal doses have always been lower than external doses in Fukushima since the FDNPP accident. However, this does not match the risk perceptions of a large proportion of Fukushima residents, especially parents raising children. The geometry of FASTSCAN is not suitable for measuring small children, who cannot stand for 2 min, and this made the situation more difficult as parents wished to have their children (babies) scanned directly.
This situation prevailed until early 2013, when the author decided to develop a WBC that was optimised for measuring small children (BABYSCAN). This was designed not just as a high-sensitivity WBC for small children, but also as a communication device; it was expected to play an important role as a communication tool to facilitate interactions between medical staff and residents.
When using the BABYSCAN, the baby lies on a bed for the 4-min scanning time. The whole unit is heavily shielded with 6 tons of iron, but its exterior is covered with an ergonomically designed plastic cover, giving it a friendly, reassuring look. The detection limit is <50 Bq per body, making it possible to quantify the amount of naturally-occurring potassium-40 in the body of a newborn baby (Hayano et al., 2014a).
The first BABYSCAN was introduced at Hirata Central Hospital in December 2013, the second was introduced at Tokiwakai Hospital in Iwaki city in May 2014, and the third was introduced at MMGH in July 2014. In 2014, more than 2700 children were scanned using these three units, none of whom were found to exceed the detection limit (Hayano et al., 2015b).
This was not at all surprising to the author. However, the large difference in risk perceptions among parents living in different regions of Fukushima, revealed by analysing the pre-scan questionnaire completed by parents, was unexpected. For example, in Minamisoma, 57% of families avoid consumption of tap water, local rice, and local vegetables. In contrast, in Miharu town, some 50 km west of FDNPP, the corresponding figure is 4%, indicating that most families have resumed ‘normal’ life (Hayano et al., 2015b). The protective measures taken by parents in Minamisoma do not visibly contribute to lowering the risks, as all children are below the detection limit. These findings illustrate that the current problems are psychosocial rather than radiological.
2. EXTERNAL EXPOSURES
From Summer 2011, many Fukushima municipalities commenced individual external dose monitoring for members of the public living in existing exposure situations, although such large-scale measurements of the general public have not been considered mandatory in conventional radiation protection schemes. The measurements typically used individual dosimeters (radiophotoluminescence glass dosimeters), and targeted pregnant women and children in most cases. For example, in Fukushima city, the percentage of survey participants whose estimated additional dose was below 1 mSv year−1 (i.e. after subtracting the pre-accident natural background of 0.54 mSv year−1) was 51% in Autumn 2011, 89% in 2012, 93% in 2013, and 96% in 2014. Correspondingly, the estimated average additional exposure for children aged ≤15 years also decreased; 1.04 mSv year−1 in 2011, 0.56 mSv year−1 in 2012, 0.44 mSv year−1 in 2013, and 0.32 mSv year−1 in 2014. 1
The results in other municipalities are similar. External exposure doses are lower than expected by most people, but are slightly higher than internal doses as the latter are almost negligible.
2.1. ‘D-shuttle’ for measurement and communication
These measurements are useful in assessing the overall situation, but are less informative when using the results at individual level. For individual measurements, a badge is typically worn for 3 months to determine the estimated ‘additional’ dose per 3 months. This is not useful when relating the dose received to behaviour.
In Spring 2013, the author, together with Dr Miyazaki, started to use a low-cost electronic personal dosimeter, the ‘D-shuttle’, 2 to measure individual external doses and to communicate the results with the survey participants. This device records integrated hourly Hp(10) dose, and records the data with time stamps. The results can be read out using a computer interface.
2.2. D-shuttle data of French high school students
Fig. 3 shows the D-shuttle data of eight students and four teachers who visited Fukushima from France in Summer 2015. The dosimeters were sent to France before the visit commenced. Time-stamped data from the 12 dosimeters were read out, and are plotted overlaid in Fig. 3. The abscissa range covers 7 days of their visit. The D-shuttle uses a small (2.7 mm × 2.7 mm) silicone sensor for gamma-ray detection; as such, sensitivity is not particularly high (10 counts per 0.1 µSv h−1). This explains the relatively large fluctuations seen in the graphs, but the results of all dosimeters were consistent within statistical errors.
D-shuttle data of eight students and four teachers who visited Fukushima from France in Summer 2015.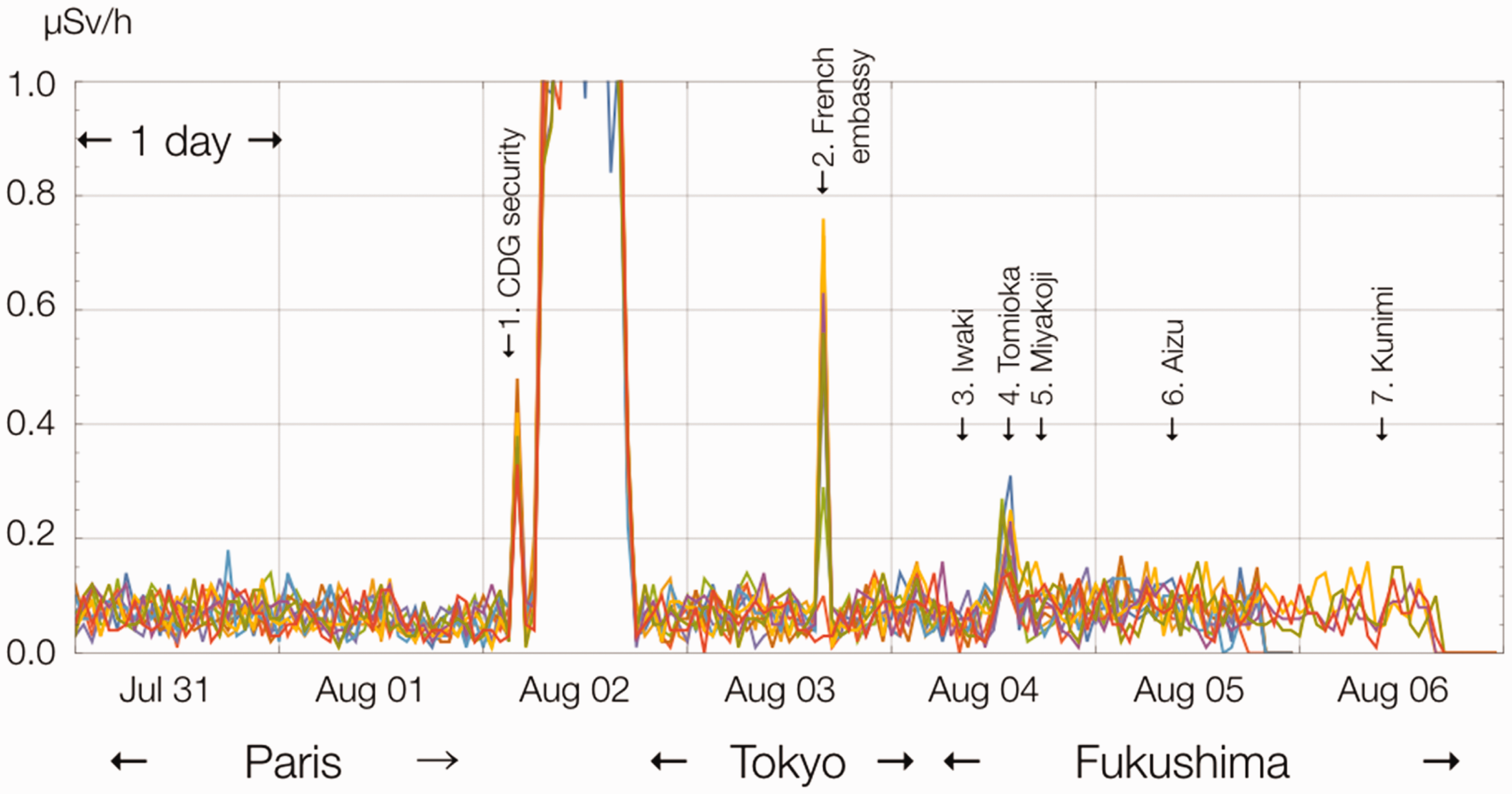
The first peak on 2 August 2015 was due to x-ray screening of hand baggage at Charles de Gaulle airport. During the flight from Paris to Tokyo, the exposure level remained very high due to cosmic rays. On 3 August 2015, the party was invited to the French Embassy in downtown Tokyo, and the dosimeters were x-rayed again (Peak No. 2).
On 4 August 2015, the party drove towards Fukushima along the Pacific coastline, through Iwaki city, and went to the railway station in Tomioka, 10 km south of FDNPP, which was washed away completely by the tsunami (Peak No. 4; note that the evacuation order has not yet been lifted in Tomioka town). Next, they visited the Miyakoji district of Tamura city, within the 20-km zone, which is the first district for which the evacuation order was lifted (April 2014). As shown, there was no visible peak in Miyakoji (Peak. No. 5).
The French students stayed in the homes of students of Fukushima high school on the nights of 4 and 5 August 2015, and visited Aizu on 5 August 2015 (Aizu is distant from FDNPP and is known to be less contaminated than Fukushima city). On 6 August 2015, they visited a peach farmer in Kunimi town, in the northern part of Fukushima Prefecture.
The data clearly show that the individual dose rates were similar in Paris, Tokyo, and various parts of Fukushima (excluding the evacuation zone).
2.3. The D-shuttle project: comparison of individual doses of high school students
The students of Fukushima high school were interested in the capabilities of the D-shuttle, and were motivated to use it to compare the individual doses of high school students living in various parts of Fukushima Prefecture in order to better understand their own exposure situation. This project, termed the ‘D-shuttle project’, was later expanded to include high schools in Japan outside of Fukushima Prefecture, and high schools in France, Poland, and Belarus.
Each participant, 206 in all, wore the D-shuttle for 2 weeks in 2014, and kept a journal of their behaviour (school, home, etc.). Based on the 2-week measurements, the annual exposure of each participant was estimated, and the resultant distributions are compared in Fig. 4 in the form of box-and-whisker diagrams (Adachi et al., 2016). Fig. 4 confirms the results shown in Fig. 3 (i.e. the external doses in Fukushima, including natural background radiations, are not very different from those in other parts of Japan or in Europe).
The 2-week integrated individual dose was converted to annual dose (mSv year−1), presented in box-and-whisker diagrams. Source: Adachi et al. (2016).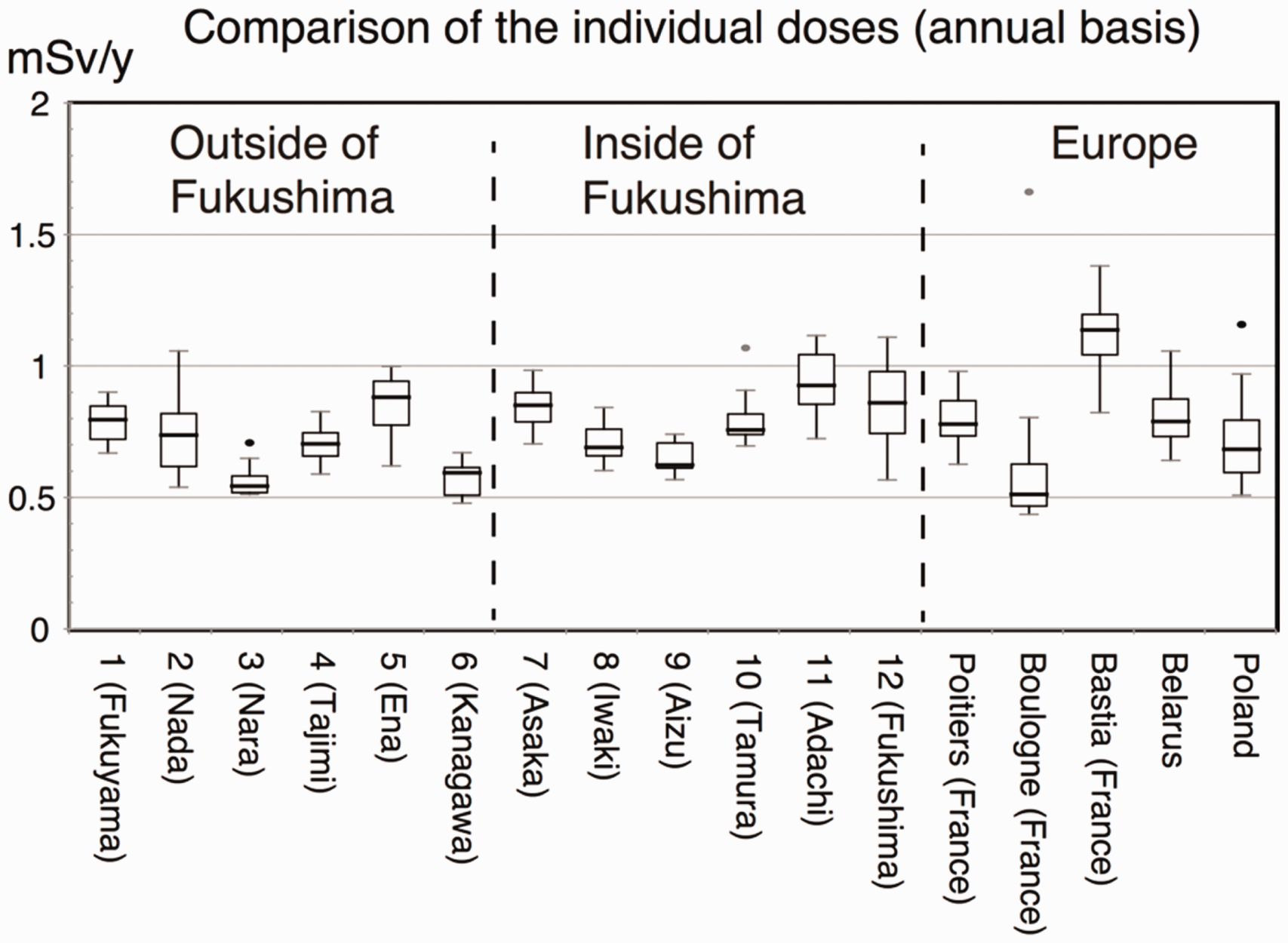
Adachi et al. (2016) published these findings online at the end of November 2015, and attracted considerable media attention in Japan and worldwide; the article had been downloaded more than 65,000 times by Summer 2016.
2.4. ‘Reference level’ in the case of external exposures
When, as in Adachi et al. (2016), the measured dose is low (e.g. additional dose < 1 mSv year−1), measurement and communication work as for internal exposure measurement. Repeated measurements and discussion can result in reassurance, although this may take a long time. However, if the measured external dose is high, the situation is different and more difficult.
In the spirit of ICRP’s reference level (ICRP, 2009), if the measured dose is high, countermeasures need to be taken to reduce the dose below the reference level [within the ‘as low as reasonably achievable’ (ALARA) principle]. In the case of internal exposure, this can be done by advising/deciding not to eat a certain contaminated food, as discussed previously. This can be done at the individual level.
In the case of external exposure, there is little that an individual can do to reduce the dose level. For example, asking for additional decontamination may not be easily granted, as massive decontamination works have already been undertaken according to government-defined instructions in most parts of Fukushima. If the dominant contributor to the integrated dose is work undertaken in an orchard, should the individual stop working in the orchard? This would deprive him/her of a source of income and makes little sense.
As such, the concept of reference level does not work in practice when the dominant exposure is external. This is the case in Fukushima.
3. CONCLUSIONS
Despite initial confusion, dose measurements in Fukushima, both internal and external, are now well under control. Huge amounts of data have been collected, and have been disseminated one way or the other 3 (sometimes not easy to find, particularly for those who do not read Japanese). It has been well established that internal radiation exposures due to radiocaesium are negligible, and external exposures (other than in the evacuation zone) are not very different from those in other parts of Japan or other countries. Unfortunately, awareness of these results is poor within Japan, let alone worldwide.
Face-to-face communication of the results is important to regain the trust of residents living in contaminated areas. This is a slow process but seems to be the best way to achieve this goal. When, in rare cases, internal dose is found to be high, this can be lowered by avoiding consumption of the particular contaminated foodstuff.
However, when external exposure is dominant and measurements show that the dose is relatively high, there is little that the stakeholders can do. In this case, communication is of little benefit, unless there is a clear way to reduce the dose without sacrificing the individual’s quality of life. Over the past 5 years, ALAP (as low as possible) has become the norm in Fukushima, and it appears to be difficult to make decisions according to the ALARA principle, both at the level of the individual or at the level of authorities.
Footnotes
2
Codeveloped by the National Institute of Advanced Industrial Science and Technology and Chiyoda Technol Corporation.
3
For example, Fukushima Prefecture website: http://www.pref.fukushima.lg.jp/site/portal/ (in 7 different languages), Fukushima Medical University website: http://fukushima-mimamori.jp (Japanese and English), Nuclear Regulation Authority website: http://radioactivity.nsr.go.jp/ (Japanese and English), Fishery Agency website: http://www.jfa.maff.go.jp/e/inspection/index.html (Japanese and English), and the Extension Site of Distribution Map of Radiation Dose: ![]() (Japanese and English).
(Japanese and English).