
Abstract
International Commission on Radiological Protection (ICRP) Publication 103 provided a detailed explanation of the purpose and use of effective dose and equivalent dose to individual organs and tissues. Effective dose has proven to be a valuable and robust quantity for use in the implementation of protection principles. However, questions have arisen regarding practical applications, and a Task Group has been set up to consider issues of concern. This paper focusses on two key proposals developed by the Task Group that are under consideration by ICRP: (1) confusion will be avoided if equivalent dose is no longer used as a protection quantity, but regarded as an intermediate step in the calculation of effective dose. It would be more appropriate for limits for the avoidance of deterministic effects to the hands and feet, lens of the eye, and skin, to be set in terms of the quantity, absorbed dose (Gy) rather than equivalent dose (Sv). (2) Effective dose is in widespread use in medical practice as a measure of risk, thereby going beyond its intended purpose. While doses incurred at low levels of exposure may be measured or assessed with reasonable reliability, health effects have not been demonstrated reliably at such levels but are inferred. However, bearing in mind the uncertainties associated with risk projection to low doses or low dose rates, it may be considered reasonable to use effective dose as a rough indicator of possible risk, with the additional consideration of variation in risk with age, sex and population group.
1. INTRODUCTION
The concept of effective dose was introduced originally in the 1977 Recommendations of the International Commission on Radiological Protection (ICRP) for the control of occupational and public exposures to external and internal sources of radiation, considering moderate and low levels of exposure in relation to stochastic health effects (ICRP, 1977). While the concept has remained essentially unchanged through the 1990 Recommendations (ICRP, 1991) to the 2007 Recommendations (ICRP, 2007), its use has been extended to members of the public of all ages, including in-utero exposures of the embryo and fetus (ICRP, 2001, 2004, 2006). Effective dose is accepted and applied internationally as the central radiological protection quantity, and has proven to be a valuable and robust quantity for use in the optimisation of protection and setting of control criteria: limits, constraints, and reference levels. However, confusion has arisen in its practical application, particularly in the communication of dose information to non-experts (e.g. Gonzalez et al., 2013). In addition, effective dose is increasingly used in medical applications, including a problematic and growing application to the assessment of risks to individuals (Martin, 2007; Brenner, 2008, 2012; Balonov and Shrimpton, 2012; Harrison and Ortiz-Lopez, 2015).
The calculation of effective dose can be seen as a three-step process, starting with the determination of mean absorbed doses to organs and tissues, in gray (Gy; J kg−1), with the intermediate stage of converting absorbed doses to equivalent doses, in sievert (Sv), using radiation weighting factors (wR). The summing of organ/tissue equivalent doses, each weighted by the appropriate tissue weighting factor (wT), gives the effective dose, in Sv. Confusion can occur between equivalent dose (in Sv) and effective dose (also in Sv) when they are not distinguished carefully, particularly when considering doses from internal emitters that concentrate in specific organs, such as iodine-131 (Gonzalez et al., 2013). There is also the potential for confusion between equivalent dose and the operational quantity, dose equivalent (Sv), used to measure exposures to external sources, and in which monitoring equipment is calibrated (ICRP, 2007).
Effective dose has proven to be a useful tool in controlling exposures received by patients undergoing medical diagnostic and interventional procedures. However, its use to provide estimates of risk to individual patients goes beyond its intended use (ICRP, 2007; Menzel and Harrison, 2012). Brenner (2008, 2012) suggested that effective dose should be replaced by ‘effective risk’ as a more scientifically based quantity. This approach ignores the large uncertainties associated with risk inference at low doses based on epidemiological observations of populations exposed to higher doses (UNSCEAR, 2012). While doses can be measured or estimated with reasonable reliability down to very low levels, the inferred risk that may be associated with the dose is increasingly uncertain as dose decreases (Dietze et al., 2009; UNSCEAR, 2012).
An ICRP Task Group is currently preparing a report to provide guidance on the use of effective dose as a risk-related protection quantity. This paper focusses on Task Group proposals relating to: (1) discontinuation of the use of equivalent dose as a separate protection quantity; and (2) the use of effective dose as a rough indicator of possible risk from particular medical diagnostic procedures.
2. DOSE QUANTITIES
The procedure for the assessment of effective dose adopted by ICRP is to use absorbed dose as the fundamental physical quantity; to average it over specified organs and tissues; to apply suitably chosen wR to take account of differences in biological effectiveness of different radiations to generate stochastic health effects to give equivalent dose; and to consider differences in sensitivities of organs and tissues to radiation-induced stochastic health effects and their contribution to total detriment (ICRP, 1991, 2007). Absorbed doses are calculated for reference persons using reference phantoms with specified organ and tissues masses (ICRP, 2009). Values of the equivalent dose to organs and tissues are weighted using wT providing a simplified representation of relative detriment, and the weighted equivalent doses are then summed to give the effective dose. This quantity is used to sum exposures to radiation from incorporated radionuclides and to external radiation fields. Exposure limits, constraints, and reference levels in relation to stochastic health effects are set in terms of effective dose.
Equivalent dose can be seen as an intermediate step in the calculation of effective dose. Currently, equivalent dose is only used as a separate quantity in specifying limits for the avoidance of deterministic effects/tissue reactions in the cases of irradiation of the hands and feet, lens of the eye, and skin; that is, limits set below thresholds for the occurrence of damage to organs and tissues (ICRP, 2007). However, wR values relate specifically to stochastic effects, and available data on the relative biological effectiveness (RBE) of different radiation types (e.g. α particles and neutrons, cf. γ rays) show that values are generally greater for cancer induction than for deterministic effects (ICRP, 2003). It is arguably more appropriate, therefore, to use absorbed dose to set these deterministic limits, either relying on conservatism in the limits to allow for differences in RBE or using appropriate values of RBE relating to deterministic effects. In practice, such differences between radiations may not be of great practical concern in relation to limits for the lens of the eye, skin, and hands and feet as these are mainly relevant to circumstances of exposure to penetrating low-linear-energy-transfer (LET) radiations.
Communication difficulties have arisen in situations where equivalent dose (Sv) and effective dose (Sv) have not been distinguished adequately; for example, in explaining doses for intakes of iodine-131 for which the equivalent dose to the thyroid (wT = 0.04) is more than 20 times greater than the effective dose (Gonzalez et al., 2013). There is also scope for confusion between equivalent dose and the operational quantity, dose equivalent (Sv). As effective dose is not a directly measurable quantity, operational quantities for the measurement of external exposures and calibration of instruments have been defined in terms of dose equivalent (ICRU, 1985, 1988; ICRP, 2007). Confusion between quantities would be avoided if organ and tissue doses were referred to in terms of absorbed dose, specifying low- and high-LET components if necessary. For example, an intake of iodine-131 might result in an effective dose of 10 mSv, with a thyroid dose of 240 mGy (low LET). For ingestion of plutonium-239 by an adult member of the public, the committed effective dose is 2.5 × 10−7 Sv Bq−1, dominated (>99.9%) by α particles and contributions of 8.6 × 10−8 Gy Bq−1 to the liver, 4.1 × 10−7 Gy Bq−1 to bone surfaces, and 2.0 × 10−8 Gy Bq−1 to red bone marrow.
It is proposed that consideration should be given to discontinuation of the use of equivalent dose as a distinct protection quantity, leaving effective dose as the primary protection quantity relating to stochastic health effects, and dose equivalent as the operational quantity used in measurements. Deterministic limits would be set in terms of absorbed dose.
3. DOSES AND RISKS FROM MEDICAL PROCEDURES
The radiation doses received in diagnostic and interventional procedures are recorded in terms of quantities that can be measured for each technique. Suitable quantities are entrance surface air kinetic energy released per unit mass (kerma) and kerma-area product for radiography and fluoroscopy, and volume averaged computed tomography (CT) dose index and dose length product for CT. These measured quantities provide straightforward methods for assessment, and are used for comparison of doses for particular types of examination among different healthcare facilities and even different countries. Surveys are made to establish diagnostic reference levels in terms of these measurable quantities (Martin, 2008, 2011; ICRP, 2016), and dose comparisons are made against them to judge whether protection is optimised. Measured dose quantities are suitable for making comparisons between techniques that deliver exposures with similar relative distributions of absorbed dose inside the body, and should always form the first approach when considering patient dose. However, as organs and tissues vary in their sensitivity to radiation and associated risk of development of cancer, measurable dose quantities are unable to convey a meaningful comparison of the possible health detriment associated with techniques that result in different distributions of dose within the body. Effective dose has provided a valuable tool to fulfil this requirement.
In order to make judgements regarding justification and optimisation of examinations, and for communication with patients, clinicians need language that reflects a broad perspective of possible risks to health from the procedures being applied. However, the widespread use of effective dose as a measure of risk goes beyond its intended applications (ICRP, 2007). Recognising that there is a role for effective dose in medical practice, it is important that guidance is provided so that uncertainties associated with inferred risks are appreciated, and distinctions are drawn between scientific observations, inferred risks at lower doses, and assumptions applied for protection purposes.
In general, epidemiological data show a linear dose–response relationship between cancer rates and a briefly received absorbed dose from γ rays from a few Gy to around 100 mGy. The data show age- and sex-related differences in cancer rates Gy−1 that also differ between cancer types and populations, depending on the modelling assumptions applied in transferring risks between populations (ICRP, 2007). Attempts are being made to extend observations to lower levels of exposure, notably studies on large worker cohorts exposed over a protracted period (Muirhead et al., 2009; Boice, 2015) and studies of children receiving CT scans (Pearce et al., 2012; Mathews et al., 2013; Huang et al., 2014). The CT studies reported significant elevation of cancer rates at doses of a few tens of mSv. However, caution has been advised in the interpretation of these studies (Boice, 2015). A number of problems were identified, including lack of information on the reasons for the scans, and lack of individual dose reconstruction. It is considered that the patients may well have had underlying conditions that prompted their CT examinations, an example of so-called ‘reverse causation’ or confounding by indication (UNSCEAR, 2013; Mathews et al., 2013; Walsh et al., 2014). It is important that future studies are controlled rigorously to avoid confounding.
Stochastic risks in the range from a few tens of mGy and below are inferred on the basis of observations applying at higher doses and the application of dose–response models, including the assumption of a linear-non-threshold (LNT) dose–response relationship at low doses and dose rates (UNSCEAR, 2013). Unless such models substantially underestimate risks at low doses, epidemiological studies are unlikely to be able to demonstrate health effects at the mGy level. While an LNT dose–response relationship is mechanistically plausible for most cancer types, estimates of risk at low doses or dose rates are subject to substantial uncertainties that are only partly quantifiable at present. Other models are being developed that apply more sophisticated mechanistic considerations (Kaiser et al., 2014). The assumption of an LNT dose–response relationship is explicit in the application of the ICRP protection system, and implicit in the use of effective dose calculated to reference persons. Protection is optimised on the assumption that risks are proportional to dose over a wide range of doses down to fractions of a mSv and even below.
In discussion of the appropriate use of effective dose in medical applications, Publication 103 (ICRP, 2007) states that: ‘… risk assessment for medical diagnosis and treatment… is best evaluated using appropriate risk values for the individual tissues at risk and for the age and sex distribution of the individuals undergoing the medical procedures.’ With respect to diagnostic procedures, these are inferred risks as discussed above, assuming that epidemiological observations of cancer rates Gy−1 can be applied, with suitable adjustments, at lower doses.
Wall et al. (2011), and Balonov and Shrimpton (2012) estimated radiation risks from a range of medical x-ray examinations (radiography, fluoroscopy and CT) as a function of the age and sex of the patient, applying the risk models of UNSCEAR (2006) and ICRP (2007). Risk estimates were based on typical organ/tissue doses and age- and sex-specific risk factors for individual cancer types. Effective dose was also calculated for each procedure so that values of risk per unit effective dose (Sv) could be compared. Fig. 1 shows the results presented by Wall et al. (2011), calculated using risk data for an ICRP Euro-American composite population (Publication 103 analyses use three Euro-American and four Asian populations). While lifetime risks of radiation-induced cancer decrease with patient age for all examinations, the pattern of changes differs markedly between examinations and between sexes, reflecting differences in the changing radiosensitivity of organs and tissues.
Total lifetime cancer risk per unit effective dose for the International Commission on Radiological Protection’s Euro-American composite population as a function of age at exposure and sex for a range of x-ray examinations and for uniform whole-body exposure (Wall et al., 2011). AP, anteroposterior; IVU, intravenous urography; Lat, lateral; PA, postero-anterior; y, year.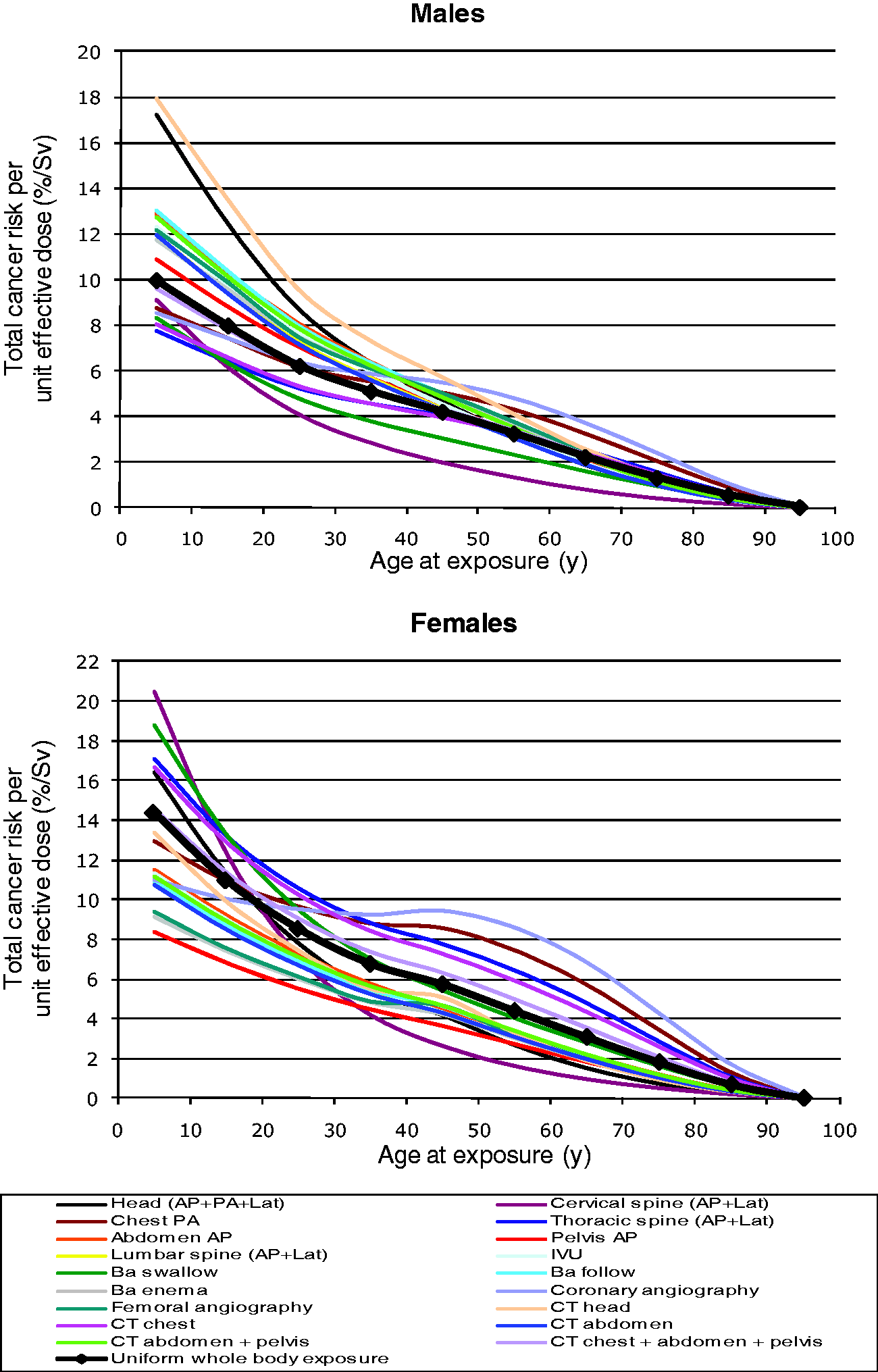
On the basis of the data presented by Wall et al. (2011), and Balonov and Shrimpton (2012), illustrated in Fig. 1, it can be concluded that risks per unit effective dose for most examinations may be around twice as great for the 0–9-y age group than for the 30–39-y age group. For patients in their 60 s, the risk coefficients for most examinations are approximately half those for patients in their 30 s, falling to less than one-third for patients in their 70 s, and about one-tenth for those in their 80 s. Risks for the 30–39-y age group are close to the ICRP sex-averaged nominal detriment-adjusted cancer risk coefficient of 5.5% Sv−1.
Typical doses received in medical x-ray examinations range from a few tens of mSv effective dose for some CT procedures to µSv doses for peripheral x-ray examinations (Mettler et al., 2008; Wall et al., 2011; Smith-Bindman et al., 2015; Shrimpton et al., 2016). As discussed above, risks associated with such doses are inferred and uncertain, and this is particularly the case at the very low doses resulting from peripheral radiographs. Bearing in mind the substantial uncertainties associated with projections of low dose risk, it appears questionable whether detailed calculations of risk using organ/tissue doses and age- and sex-specific risk factors would generally be justified in evaluating medical procedures. It would appear more reasonable to use effective dose and nominal risk coefficients as a rough indicator of possible risk, with the additional consideration of variation in risk with age, sex, and population group. Balonov and Shrimpton (2012) concluded that although effective dose was not intended to provide a measure of risk associated with medical x-ray examinations, simple adjustments to nominal risk coefficients to take account of age and sex differences might make it a useful instrument when considering the justification of examinations.
4. CONCLUSIONS
A cross-Committee Task Group of ICRP is currently developing a report to provide guidance on the practical applications of effective dose. The report will cover a range of issues relating the use of effective dose in the control of occupational, public, and medical exposures. This paper has focussed on two of the central issues being considered by the Task Group, and summarised proposals developed by the Task Group. These proposals are under consideration by ICRP Committees and the Commission.
Confusion can arise in the use of the protection quantities, equivalent and effective dose (both in Sv), when they are not sufficiently well distinguished, and between equivalent dose and the operational quantity, dose equivalent (Sv), used in measurements of exposures to external radiation for the assessment of effective dose (Gonzalez et al., 2013). It is essential to specify which quantity is being used under particular circumstances. Difficulties would be reduced or avoided if organ and tissue doses were referred to in terms of mean absorbed dose (Gy), specifying low- and high-LET components as necessary. The unit Sv would then apply to the protection quantity, effective dose, and the corresponding operational quantity, dose equivalent. Limits to prevent deterministic effects to the lens of the eye, skin, and hands and feet would more appropriately be set in absorbed dose rather than equivalent dose. The Task Group therefore suggests that consideration should be given to discontinuation of the use of equivalent dose as a separate protection quantity.
Effective dose is a risk-adjusted dosimetric quantity for use in the control of exposures to all sources of radiation. However, it is also commonly used as a measure of stochastic risk, particularly in medical applications. While doses can be measured or assessed with reasonable reliability down to very low levels, the associated risk is increasingly uncertain as doses decrease. Risks at doses below around 50–100 mGy are inferred on the basis of epidemiological observations relating to higher doses, usually assuming a linear dose–response relationship at lower doses or dose rates. As discussed in Publication 103 (ICRP, 2007), risks associated with medical procedures are best evaluated using appropriate risk values for the individual tissues at risk, and for the age and sex distribution of the individuals undergoing the medical procedures. However, the analyses of Wall et al. (2011), and Balonov and Shrimpton (2012) showed that the use of effective dose and nominal risk coefficients, rather than best-available data, might underestimate risk for most procedures by approximately a factor of two for young children, and overestimate risk by a factor of two for the 60–69-y age group. Thus, effective dose to a reference person might be used judiciously as a rough indicator of possible risk, with simple adjustments to take account of age and sex differences, without implying greater knowledge of risks at low doses than is justified (Harrison and Ortiz-Lopez, 2015). The overriding consideration in assessing doses received in diagnostic x-ray procedures is arguably the inference that risks demonstrated at higher doses will apply at lower doses.