
Abstract
Day-to-day social life and mental health are intertwined. Yet, no study to date has assessed how the quantity and quality of social interactions in daily life are associated with changes in depressive symptoms. This study examines these links using multiple-timescale data (iSHAIB data set; N = 133), where the level of depressive symptoms was measured before and after three 21-day periods of event-contingent experience sampling of individuals’ interpersonal interactions (T = 64,112). We find weak between-person effects for interaction quantity and perceiving interpersonal warmth of others on changes in depressive symptoms over the 21-day period, but strong and robust evidence for overwarming—a novel construct representing the self-perceived difference between one’s own and interaction partner’s level of interpersonal warmth. The findings highlight the important role qualitative aspects of social interactions may play in the progression of individuals’ depressive symptoms.
Keywords
Introduction
Bowlby (1978) argued that people have an inherent motivation to bond with others and that a disruption of social ties can lead to emotional distress (also see Baumeister & Leary, 1995). Others similarly suggest that interpersonal factors contribute to the development and treatment success of depressive symptomatology (Gunlicks-Stoessel & Weissman, 2012). Therapists and laypersons might thus strategically encourage individuals with higher levels of depressive symptoms to frequently engage in social interactions as means to reduce social isolation, social anhedonia, and feelings of loneliness (Nezlek, 2001). This recommendation aligns with the theoretical underpinnings of various psychotherapies for depression, spanning from psychodynamic theory to interpersonal psychotherapy and behavior activation, all of which emphasize the importance of addressing social interactions and withdrawal. However, there is considerable agreement that the quality, rather than the sheer quantity, of social interactions contributes to depression (Nezlek et al., 2000; Santini et al., 2015; Sun et al., 2019). In particular, having negative social interactions perceived as conflictive and lacking in social support may instead further contribute to depressive symptoms (Rook, 1984; Schuster et al., 1990; Vranceanu et al., 2009). At the same time, emerging research suggests that fostering positive social perceptions could play a crucial role in buffering against depressive symptoms (e.g., Chaves et al., 2019). Similarly, the perception of available social support has been shown to provide a buffer against the development and progression of depressive symptoms (Lakey & Cronin, 2008) as well as providing support to others (e.g., Block et al., 2022; Gloster et al., 2023). Integrating dimensions of social perceptions of social interaction into our understanding of the interplay between social interactions and depressive symptoms offers a more comprehensive perspective of the role of social interaction in the development of depressive symptoms.
Given the significance of social interactions in the etiology and treatment of depressive symptoms (e.g., Klerman et al., 1994), fostering (positive social) behavior activation has emerged as a prominent strategy (Manos et al., 2010). By engaging in behaviors, such as physical activity and social interaction, individuals with depressive symptoms can experience positive reinforcement, leading to a restoration of self-efficacy and self-worth (Manos et al., 2010; McCusker et al., 2016). While behavior activation encompasses various forms, the scientific literature has primarily focused on studying the quantity rather than the quality of social interactions (Manos et al., 2010; Santini et al., 2015). Consequently, limited knowledge exists regarding how the quality and quantity of day-to-day social interactions contribute to changes in depressive symptoms—in particular within non-clinical populations. In non-clinical populations, a regular engagement in social interactions may constitute a protective and sub-therapeutic factor regarding depressive symptoms through the feeling of belongingness and social support processes (Baumeister & Leary, 1995; Lakey & Cronin, 2008). Despite considerable theoretical debate on the importance of both the quantity and perceived quality of social interactions (Santini et al., 2015), the underlying mechanisms through which they relate to changes in depressive symptoms remain unclear. In particular methodological hurdles, such as the absence of longitudinal studies, have impeded progress in understanding the interplay between social interactions and the development of depressive symptoms.
To date, existing research on how social interaction quantity and quality are linked to depressive symptoms is primarily based on cross-sectional research designs (Santini et al., 2015; Vranceanu et al., 2009). Yet, accurate and robust inference about whether and how social interactions contribute to depressive symptoms requires examination of social processes in individuals’ daily lives with intensive longitudinal data (Trull & Ebner-Priemer, 2013). Pushing beyond prior work where characteristics of social relations were measured retrospectively and statically (e.g., Leigh-Hunt et al., 2017; Santini et al., 2015), ambulatory assessment methods where short surveys (experience sampling methods [ESM]) are delivered and completed via mobile devices (Elmer et al., 2019; Mehl et al., 2001; Trull & Ebner-Priemer, 2013) open opportunity to obtain dense and accurate information about how individuals experience everyday social life (Rinner et al., 2019). In particular, multiple-timescale longitudinal study designs (Ram & Diehl, 2015) where slow-changing outcomes (e.g., depression) are measured alongside ambulatory assessments support new understanding of whether and how social interactions contribute to changes in depression. This study uses data from a multiple-timescale study to investigate how the quantity and quality of social interactions in daily life are associated with month-to-month changes in depressive symptoms. Such a longitudinal investigation may help to (re)inform theories on how quality and quantity of social interactions play together in depression development. In the remainder of this introduction, we discuss how the quantity and perceptions of the quality of social interactions are theoretically associated with changes in depressive symptoms and which research gaps remain unresolved that this study aims to address.
Quantity of Social Interactions
Having fewer social interactions may go hand-in-hand with perceiving a threat of social exclusion and loneliness (Cacioppo et al., 2014). In line with behavior activation theories for treating depressive symptoms (Manos et al., 2010), individuals who have fewer social interactions in their day-to-day life have fewer opportunities to receive social support, which may be a protective factor against the development of depressive symptoms (Lakey & Cronin, 2008).
Despite these theoretical stands, empirical results on the relationship between interaction quantity and depressive symptoms are mixed. On one hand, some studies find that a lower quantity of social interactions is associated with higher levels of depressive symptoms (Brown et al., 2011; Elmer & Stadtfeld, 2020; Nezlek et al., 1994; Sun et al., 2019; Villanueva et al., 2020). For instance, Villanueva et al.’s (2020) analysis of experience sampling data obtained from individuals with and without a depression diagnosis found that depressed individuals reported fewer face-to-face interaction than non-depressed individuals. Similar results have emerged from studies of sub-clinical populations, with individuals with higher levels of depression reporting that they were alone more frequently than individuals with fewer depressive symptoms (Brown et al., 2011). On the other hand, some studies find no or only limited evidence of an association between the quantity of social interactions and depression markers (Baddeley et al., 2012; Nezlek et al., 2000). For example, Nezlek and colleagues (2000) found that clinically depressed individuals did not report fewer social interactions than non-depressed individuals.
It is important to note that the studies described above are studies where depressive symptoms were only measured once before the day-to-day social interactions were measured with ESM (i.e., contemporaneous study designs). Such a study design does not allow to make conclusions about the directionality of effects. Notably, neither set of findings indicates whether the (lack of) associations between the quantity of social interactions and depression markers emerges because (a) individuals with depression are withdrawing from social life or (b) because reduced social life is leading to elevated depressive symptoms (Elmer, 2019). Disentangling these possibilities requires that depression be measured multiple times. This study uses data from a multiple-timescale longitudinal data collection where changes in depression were measured repeatedly over three measurement periods (Ram et al., 2014) to examine the relation between quantity of social interactions and monthly changes in depressive symptoms: Is a higher quantity of social interaction associated with changes—specifically a reduction of—depressive symptoms (RQ1)?
Quality of Social Interactions
There is a clear theoretical consensus that a mere quantification of social interactions may not be sufficient to describe changes in depressive symptoms; rather, the nature and quality of these interactions may be of greater significance (Nezlek et al., 2000; Santini et al., 2015; Sun et al., 2019). Yet, to date, no study has examined how the quality of social interactions over a period of multiple weeks is associated with subsequent changes in depressive symptoms. Such a longitudinal examination of the quality of social interactions and depressive symptoms would contribute to a more nuanced theoretical discussion on social factors contributing to changes in depressive symptoms and what factors of social interactions behavior activation interventions may target.
In comparison with research on how the quantity of social interactions is related to depressive symptoms, research on how the quality of social interactions in daily life with depressive symptoms is even more scarce (Pemberton & Fuller Tyszkiewicz, 2016). A few results, obtained from contemporaneous study designs wherein depression was only assessed once prior to social behavior observations, indicate that individuals with clinical and high sub-clinical levels of depressive symptoms report having less intimate and less pleasant social interactions, having less influence over those social interactions (Gloster et al., 2021; Nezlek et al., 1994, 2000), while perceiving the social interactions as equally meaningful than individuals without a depression diagnosis (Villanueva et al., 2021). To our knowledge, none of the existing studies of interaction quality analyzed repeated measures of depression in a longitudinal study design or assessed how characteristics of these interactions are related to changes in depressive symptoms.
The existing literature does, however, note that a specific quality of social interactions, interpersonal warmth, may be particularly related to depressive symptoms (also see Downie et al., 2008; Reis & Wheeler, 1991). Unexpectedly, Zuroff et al. (2007), in a study where depressive symptoms were measured prior to an event-contingent experience sampling phase, found no relation between higher levels of depression and individuals’ self-reported interpersonal warmth (defined specifically as “attempts to create or maintain affiliative social bonds,” Zuroff et al., 2007, p. 765). 1 Although the studied sample was relatively small (N= 113), the null finding suggests some reconsideration of how one’s own display of interpersonal warmth may contribute to dyadic interpersonal processes.
Interpersonal theories (Pincus & Ansell, 2012) suggest that mental health is manifested through the interplay of one’s own and other’s behavior. This view suggests further consideration of how the interplay between respondents’ perceptions of their own and their interaction partners’ interpersonal warmth is related to changes in depressive symptoms. In this study, we thus examine both (a) other’s warmth, 2 specifically the level of interpersonal warmth displayed by others as rated by the focal person and (b) correspondence, specifically the perceived relative difference between focal person’s and other’s warmth.
It is important to emphasize that our study does not investigate interpersonal warmth through a traditional dyadic lens, where all participants involved in a social interaction share their individual perceptions. Instead, our approach delves into participants’ perceptions of their own behavior as well as their perception of others’ behavior. In the context of studying depressive symptom trajectories, this subjective viewpoint is predicated on the assumption that internal perceptions are at least—if not more important—in its contribution to the maintenance of depression as the external view of the interaction partner. Indeed, theorization and clinical training focus nearly exclusively on intrapsychic processes (Hu et al., 2015; Sweeney et al., 1986; Weary et al., 1987). Hence, including an individual’s subjective view about their own and others’ social behavior provides information of the intricate interplay between social dynamics and depressive experiences because one’s own behavior can be put into relation with one’s perception of others’ behavior.
Other’s Warmth
“Expressions of warmth and openness are suited for safe environments, not threatening ones” (Zuroff et al., 2007, p. 771). This statement suggests that there is a relationship between how safe one feels and how one perceives the expression of interpersonal warmth from others. Individuals’ positive perception of others’ social behavior might thus reflect the extent to which they feel accepted as a person (Zuroff et al., 2007).
Indeed, there is empirical evidence that the lack of acceptance and the presence of interpersonal rejection (Marcus & Nardone, 1992) and conflict (Vranceanu et al., 2009) are predictors of depression. It may not be the actual behavior of interaction partners that contribute to changes in depressive symptoms, but how the interaction partners’ behaviors are perceived by the focal individual, as subjective perceptions govern emotional reactions. A heightened sensitivity to negative (social) stimuli of individuals with depressive symptoms (i.e., the social behavior of others) may lead to increased rumination, avoidance behaviors, and withdrawal from rewarding activities, contributing to the persistence of depressive symptoms (Katz et al., 2020).
At the same time, it is plausible that positive perceptions of interpersonal warmth in social interactions might play a pivotal role in contributing to a remission of depressive symptoms. The experience of genuine warmth, acceptance, and belongingness could foster a positive shift in emotional responses (Leary, 2015). This, in turn, may facilitate a reduction in rumination and avoidance tendencies, potentially leading to a more favorable trajectory in managing and alleviating depressive symptoms (e.g., Chaves et al., 2019).
Following from this view, we examine the relation between perceived quality of social interactions, specifically perceived other’s warmth, and monthly changes in depressive symptoms: Are higher levels of perceived interpersonal warmth displayed by interaction partners associated with changes—specifically a reduction of—depressive symptoms (RQ2)?
Correspondence and Overwarming
Given that interpersonal behavior is, by definition, a dyadic phenomenon, interaction quality likely depends on the interplay between one’s own and other’s behavior according to interpersonal theories of social behavior (Pincus & Ansell, 2012). A correspondence in interpersonal warmth, that is, displaying a similar level of warmth, has been theorized to sustain interpersonal functioning and interpersonal bonds (Carson, 1969; Sadler et al., 2011). Correspondence is conceptualized by the absolute difference between the self- and other’s ratings. Specifically, the Theory of Interpersonal Complementarity postulates that individuals have a healthy interaction style when oneself and others correspond in their display of warmth (Sadler et al., 2011). Perceiving the interaction to be in correspondence with regard to interpersonal warmth, could help individuals reduce depressive symptoms through increasing self-esteem (Sowislo & Orth, 2013; Zuroff et al., 2007) by perceiving the environment to be in balance with oneself and by perceiving to be able to adapt to the warmth displayed by others.
As a derivation of the correspondence of interpersonal warmth, we further explore the concept of overwarming—representing the tendency of individuals (to perceive) displaying more interpersonal warmth than their interaction partner. Overwarming is conceptualized as the perceived difference between the self- and the other’s ratings. Compared with the correspondence construct, these values are not absolutized. Analogously, a tendency of individuals (to perceive) to show less interpersonal warmth than their interaction partner is conceptualized as underwarming.
The level of perceived overwarming could potentially be associated with better depression trajectories for two reasons. First, individuals who perceive themselves as showing more interpersonal warmth may have higher self-esteem, which could protect against depressive symptoms (Sowislo & Orth, 2013; Zuroff et al., 2007). Second, overwarming may facilitate the formation of strong social connections and support networks, which have been shown to be important for mental health and well-being (Lakey & Cronin, 2008). On a methodological level, Johns (1981) outlines that taking the absolute of a difference score may lead to loss of information regarding the directionality of the difference. By not taking the absolute value of the difference between self- and other’s ratings, the overwarming construct accounts for this methodological limitation.
Propelling forward the dyadic nature of interpersonal interaction, we examine how correspondence of interpersonal warmth and level of overwarming are related to monthly changes in depressive symptoms: Are higher levels of correspondence in interpersonal warmth associated with a reduction of depressive symptoms (RQ3a)? Are higher levels of overwarming associated with changes in depressive symptoms (RQ3b)?
Interpersonal Turbulence
In addition to an individual’s general level of other’s warmth perceptions, correspondence, and warming, the level of variability in these measures could indicate a destabilized interplay between the individual and the social environment (Knobloch & Theiss, 2011; Solomon, 2015). Individuals who experience more interpersonal turbulence, for example, through reoccurring conflicts will have more “dells” of negative interactions in their day-to-day social life and thus a higher variability in interaction quality measures. Such a destabilization of personal relationships through lower levels of safety could contribute to an increase in depressive symptoms (Rook, 1984). On the other hand, a flattening or lack of variance might signal depressive behavior too—as reduced feelings of joy might prevent “peaks” of positive interactions. Following previous work on destabilization (Jeronimus, 2019) and the relations between intraindividual variability and change (Ram & Gerstorf, 2009), we explore in Research Question 4 (RQ4): Is interpersonal turbulence in interpersonal warmth associated with changes in depressive symptoms?
Methods
Data for our analysis were drawn from the Intraindividual Study of Affect, Health, and Interpersonal Behavior (iSAHIB; Ram et al., 2014), a multiple-timescale longitudinal study of adults that supports investigation of the interplay between (mental) health and everyday affective and social experiences. The R-code for estimating the reported models, a codebook, and additional stimulus materials can be found on OSF https://osf.io/hq48z.
Procedure
During three 21-day experience sampling phases (bursts) spaced at about 4.5-month intervals, participants were instructed to complete a short survey after every social interaction that lasted longer than 5 minutes (i.e., event-contingent experience sampling). At the start and the end of each experience sampling phase, a series of questionnaires were administered assessing a variety of constructs, including depressive symptoms.
Participants
Participants, N = 150 (51% female) adults living in the Mid-Atlantic region of the United States, were recruited from the Pennsylvania State University and surrounding community with no particular focus on recruiting a clinical sample. Participants were between the age of 19 and 89 years (MAge = 47.64, SDAge = 18.85) and mostly identified as White (91%). The majority of participants indicated a family income of U.S.$20,000 to U.S.$49,000 (n = 46, 31%) or U.S.$50,000 to U.S.$74,000 (n = 30, 20%). From these 150 participants, we excluded 17 participants that did not report more than 10 social interactions within each experience sampling phase, as this would make average interaction ratings potentially unreliable. In fact, 15 of these 17 individuals did not report any social interactions for at least one experience sampling phase (the other two only had two and eight observations in one experience sampling phase). For these reasons, these outlier observations were removed. These non-completers did not differ on key demographics from those included in the analyses (gender
Measures
Depressive Symptoms
Individuals’ level of depressive symptoms was assessed before (Dpreij) and after (Dpostij) each of the three experience sampling bursts, using the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). At each assessment, participants were asked how frequently they experienced 20 symptoms during the past week. Answers to the 20 items, each given on the 4-point scale (0 = “Rarely or none of the time” to 3 = “Most or all of the time (5-7 days)” were summed to obtain a total score that could range from 0 to 60 (overall Cronbach’s
Social Interaction Measures
From the experience sampling assessments of social interactions, we derive measures of interaction quantity and interaction quality.
Quantity of Social Interactions
The quantity of social interactions experienced during each experience sampling phase was quantified as the total number of interactions reported on during that burst of the study. Although partially related to participant compliance, this measure is commonly used to assess interaction quantity in event-contingent sampling designs (see Reis & Wheeler, 1991). For straightforward interpretation of the statistical model results, the number of interactions
Quality of Social Interaction
After each social interaction, participants were asked to rate the interaction on an interpersonal grid (Moskowitz & Zuroff, 2005). Measures of interaction quality were derived (as described below) from two items assessing interpersonal warmth, where participants were asked to “rate how you acted” (self-perception) and “rate how the other person acted” (perception of others) on a −50 (distant) to +50 (friendly) slider-type response scale.
Covariates
Gender (0 = female, 1 = male, centered) and age (in years, centered at mean 48.11) were measured at the start of the study via baseline questionnaire.
Data Preparation
Depression Change
The change in depressive symptoms during each experience sampling phase was computed by subtracting the pre-burst CES-D score from the post-burst CES-D score, thus representing the degree to which each individuals’ depressive symptoms increased during each experience sampling phase
Correspondence, Overwarming, and Turbulence
The level of correspondence of interpersonal warmth for each social interaction t was computed as the absolute difference between the self and other’s rating of interpersonal warmth
The level of overwarming was computed for each social interaction t as the difference between the ratings of self and other’s interpersonal warmth
Within each of the three experience sampling phases (21 days each), individuals reported on average 111.17 (SD = 39.28) interactions
Data Analysis
The four research questions were examined using multilevel linear regression models (Snijders & Bosker, 1999) that accommodated the nested data structure (up to three experience sampling phases nested within each of 133 participants). Change of depressive symptoms (D∆ij
Our research questions focus on the within- and between-person effects for the number of social interactions reported
To examine these research questions, we first defined a baseline model (M0) with no random slope terms, which looked as follows,
with






where the person-level random intercept is represented as
All the multilevel analyses were conducted in R using the lme4 package (Version 1.1-31; Bates et al., 2015) with missing data treated as missing at random and using restricted maximum likelihood (REML) estimators. Data from the iSAHIB study (Ram et al., 2014) were collected under an institutional review board protocol that has not allowed public posting of deidentified data.
Robustness Analyses
We ran a series of robustness analyses to further examine the associations between social interaction characteristics and changes in depressive symptoms under alternative modeling strategies.
Random Slope Models
As the slopes of within-person effects can vary between individuals, we further estimated a series of models in which we also estimate random slopes. For each research question, we then estimated a separate model, in which the respective slope of the within-person effect was estimated with a random slope term and person-level covariates were added to the baseline model M0. For consistency, we name the extended models M1, M2, M3a, M3b, and M4, in line with the numbering research questions. For more mathematical details on the models M1 to M4 see the “Extended Analysis Strategy” section in the Supplementary Materials.
Alternative Model Specifications
We additionally report (a) a model in which the covariates gender and age were omitted and (b) a residualized change score model. In a residualized change score model, the dependent variable constitutes
Latent Change Score
We further examined the between-person associations between social interaction characteristics and changes in depressive symptoms using a latent change score model (Grimm et al., 2017). In latent change score models, a latent change variable is used to regress predictors on. The advantage of latent change score models over multilevel models is that allow for a more reliable representation of variables (through latent constructs) and that statistical artifacts (such as Lord’s paradox) are reduced (e.g., see Castro-Schilo & Grimm, 2018; Gollwitzer et al., 2014). We estimated such a model using the R software lavaan (Rosseel, 2012). More details on the model specification can be found on OSF https://osf.io/hq48z.
Results
RQ1. Is a Higher Quantity of Social Interaction Associated With Changes—Specifically a Reduction of—Depressive Symptoms?
Table 1 shows the results of the general random intercept multilevel model—where M0 represents the model estimated with correspondence as a predictor (RQ3a) and M0’ the model with overwarming (instead of correspondence) as a predictor (RQ3b). The results in Table 1 indicates that individuals who generally report a higher number of social interactions in between-person comparison are significantly more likely to show a reduction of depressive symptoms than individuals with fewer social interaction reports (
Multilevel Random Intercept Model Results Predicting Change in Depressive Symptoms (
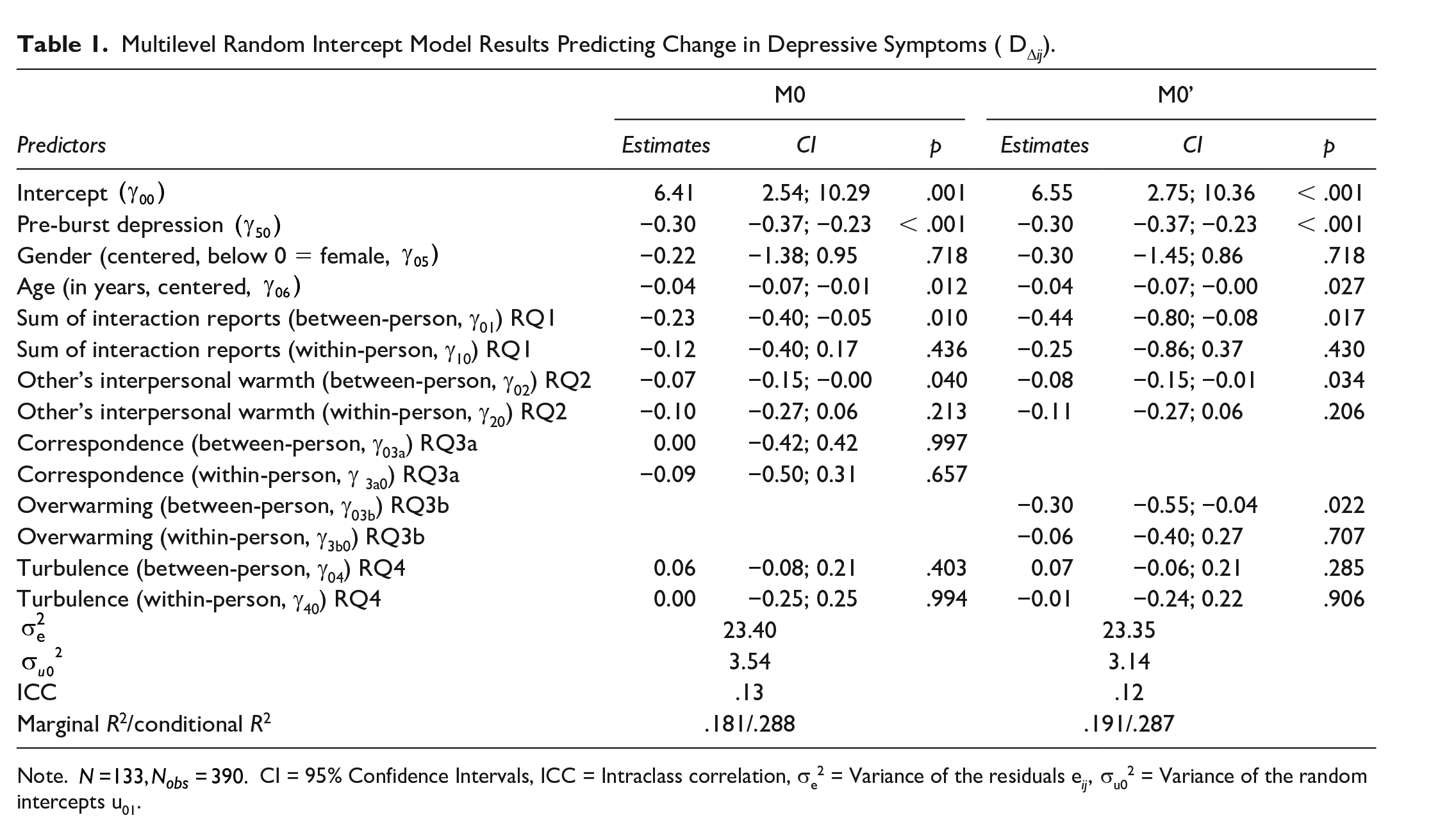
Note.
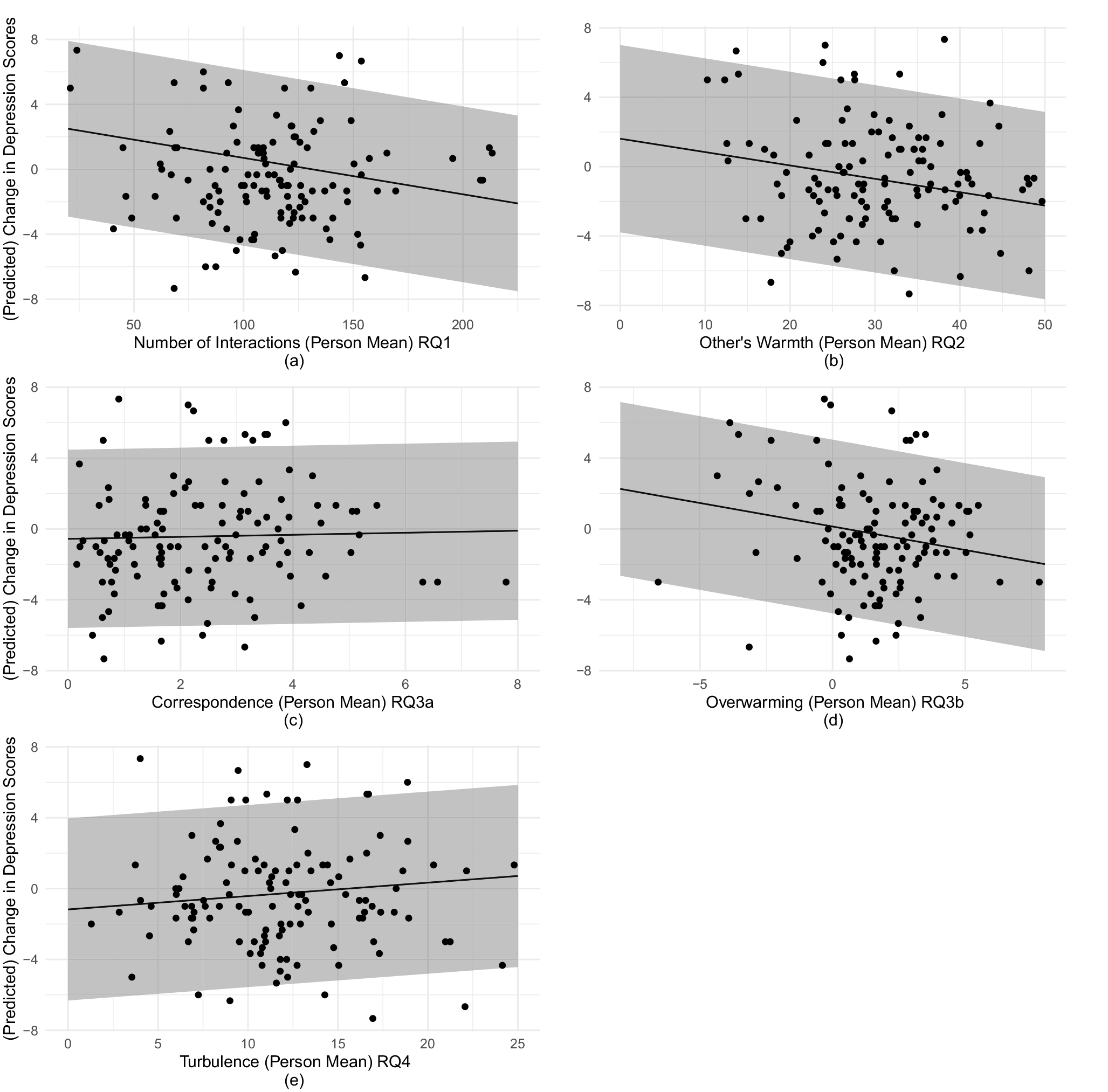
Between-Person Scatterplots With Model-Implied Associations (M1-M4) of Key Interaction Quantity and Quality Variables With Depression Change Scores (A) Number of Interactions (Person Mean) RQ1 (B) Other’s Warmth (Person Mean) RQ2 (C) Correspondence (Person Mean) RQ3a (D) Overwarming (Person Mean) RQ3b (E) Turbulence (Person Mean) RQ4.
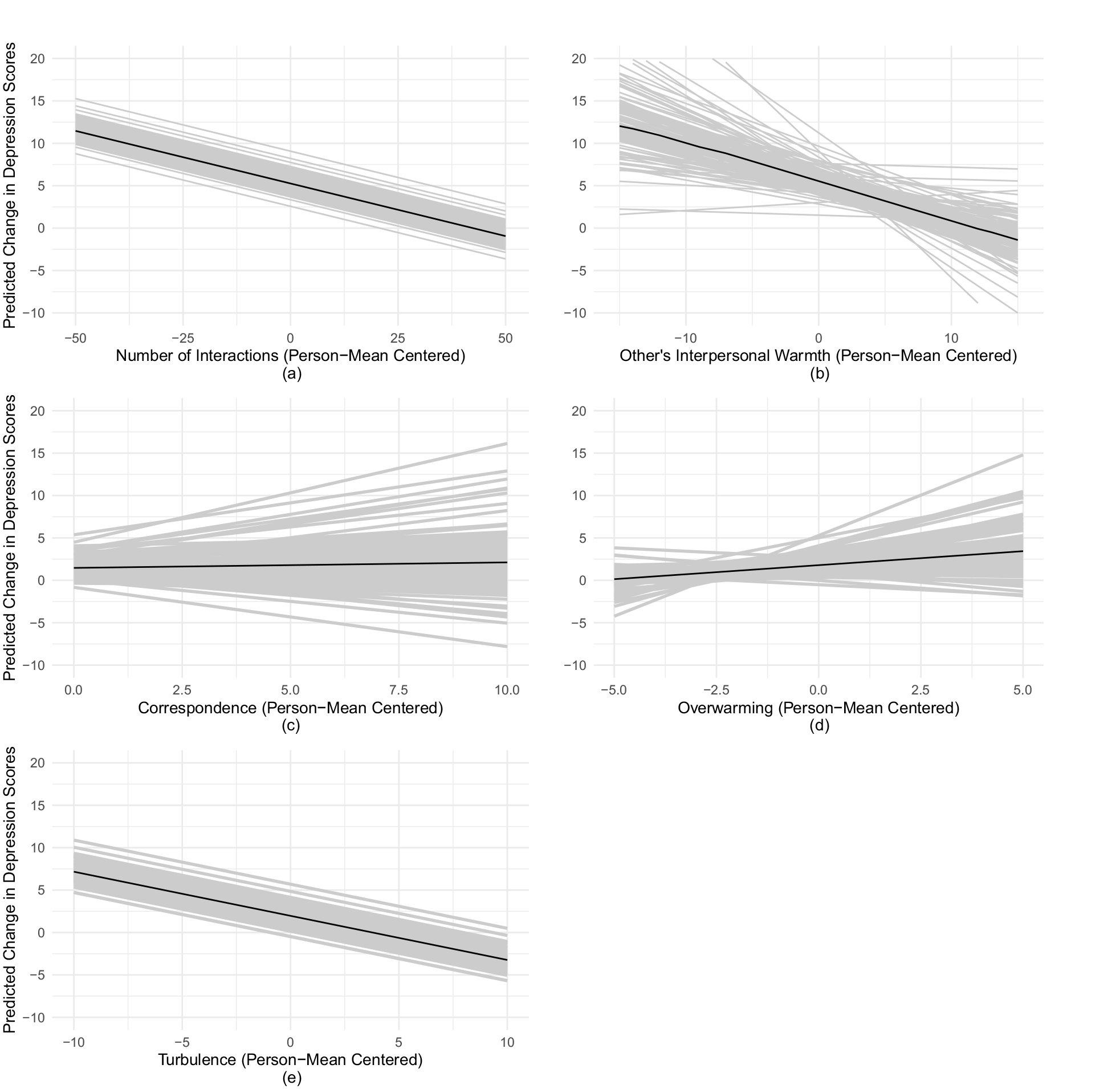
Predicted Within-Person Association (Black Line) and Random Slopes (Gray Lines) of Other’s Interpersonal Warmth (Left Panel) and Overwarming (Right Panel) With Changes in Depressive Symptoms (A) Number of Interactions (Person-Mean Centered) (B) Level of Other’s Interpersonal Warmth (Person-Mean Centered) (C) Correspondence (Person-Mean Centered) (D) Level of Overwarming (Person-Mean Centered) (E) Turbulence (Person-Mean Centered).
RQ2. Are Higher Levels of Perceived Interpersonal Warmth Displayed by Interaction Partners Associated with Changes—Specifically a Reduction of—Depressive Symptoms?
As shown in M0 in Table 1 the between-person effect of other’s interpersonal warmth was significantly and positively associated with a change in depression: Individuals who generally perceive other’s interpersonal warmth as one unit higher (on the -50 to 50 scale) showed a change in depressive symptoms of
RQ3a. Are Higher Levels of Correspondence Associated With Changes in Depressive Symptoms?
As shown in M0 in Table 1 indicates that there are no significant between- or within-person effects of the correspondence in interpersonal warmth on changes in depressive symptoms
RQ3b. How is the Level of Overwarming Associated With Changes in Depressive Symptoms?
As shown in M0’ in Table 1, overwarming on the between-person level is positively and significantly associated with a reduction of depressive symptoms
RQ4. Is Interpersonal Turbulence in Interpersonal Warmth Associated With Changes in Depressive Symptoms?
The results of M0’ in Table 1 indicate that there is no significant within- or between-person association of interpersonal turbulence with changes in depressive symptoms
Robustness Analyses
In this subsection, we report on robustness analyses, including (a) random slope models, (b) alternative model specifications, and (c) latent change score models.
Random Slope Models
Tables S2 and S3 in the Supplementary Materials report on multilevel regression models, in which also random slope terms for within-person variables are estimated. The additional estimation of random slope effects together with person-level variables as moderators, did not change the substantive interpretation of the findings reported above.
Figure 2 shows the model-implied within-person associations of interaction quantity and quality measures with changes in depressive symptoms. As visible in Figure 2, these random slopes vary considerably between individuals, suggesting that some individuals may be more affected in their depressive symptoms by burst-level changes in how they perceive other’s interpersonal warmth. Yet, none of the person-level variables that we included in the level 2 equation were moderator variables of the within-person effect of interaction characteristics on depression change (see interaction terms in M2 of Tables S1 and S2 for details).
Alternative Model Specifications
Table S4 and S5 in the Supplementary Materials report on random intercept multilevel regression models, in which (a) gender and age was not controlled for and (b) where
In the residualized change score model with
Latent Change Score Model
In Table 2, the fixed effect estimates for the latent change score model are presented. The detailed results of the latent change model results can be inspected in the R-Markdown script on OSF https://osf.io/hq48z.
Fixed Regression Slopes of the Latent Change Score Model Predicting the Latent Depression Change Score.
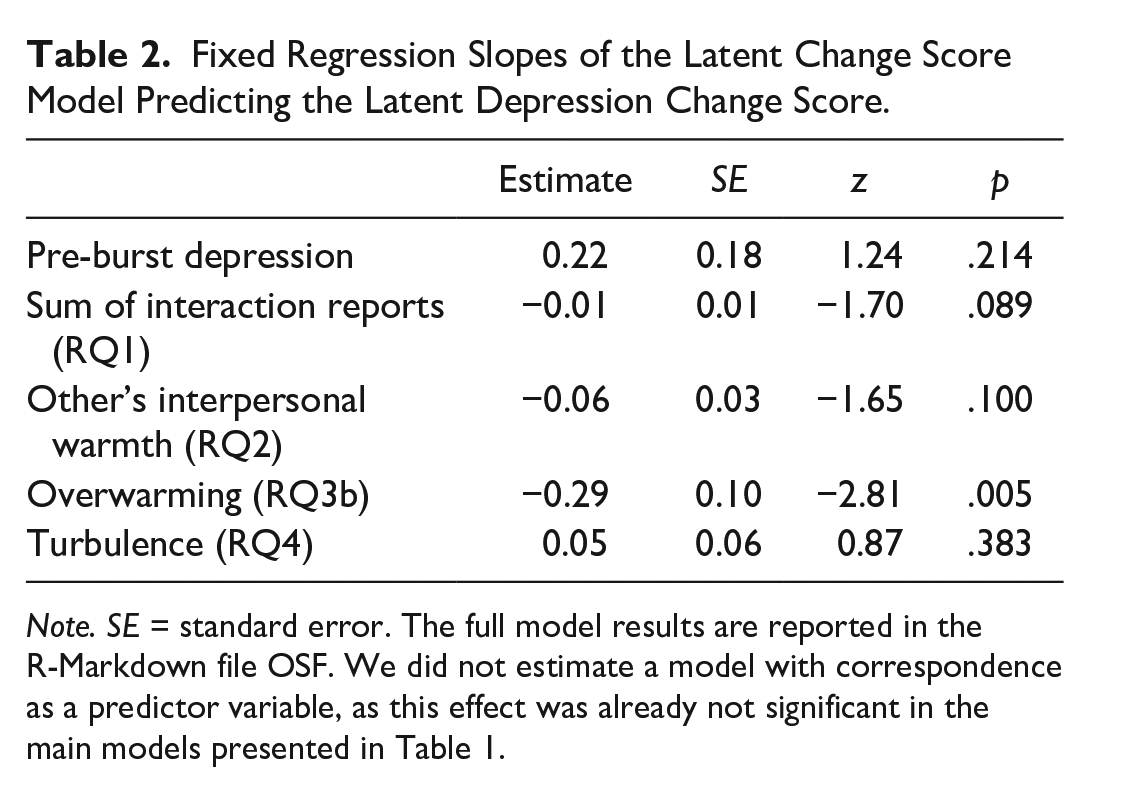
Note. SE = standard error. The full model results are reported in the R-Markdown file OSF. We did not estimate a model with correspondence as a predictor variable, as this effect was already not significant in the main models presented in Table 1.
The results of this latent change score model can be interpreted as between-person effects. They indicate that only the overwarming variable is significantly associated with changes in depressive symptoms.
Discussion
This study investigated how the quantity and quality of individuals’ daily social interactions are associated with 3-week changes in depressive symptoms. Specifically, we examined how the number of social interactions (RQ1), the perceived interpersonal warmth of interaction partners (RQ2), the interpersonal correspondence in warmth (RQ3a), the level of overwarming (RQ3b), and interpersonal turbulence (RQ4) are associated with within-person and between-person differences in depressive symptoms change. Self-reported depressive symptoms were measured before and after three experience sampling phases (measurement bursts) during which participants reported on their social interactions an event-contingent manner (Ram et al., 2014). This unique multiple-timescale study design facilitated new analysis of how qualitative and quantitative aspects of social interactions are associated with 3-week changes in depressive symptoms (measured before and after a 3-week ESM period).
Our between-person analyses suggest that individuals who report more social interactions across all measurement phases tend to report a slight decrease of depressive symptoms across 3-week periods (RQ1). The analyses further suggest that individuals who, in general (i.e., over all three observation periods), perceive their interaction partners to display higher levels of interpersonal warmth are more likely to show a reduction in depressive symptoms than those individuals who perceive other’s interpersonal behavior as less warm (RQ2). Although the level of interpersonal correspondence was not associated with three-week changes in depressive symptoms (RQ3a), higher level of overwarming was associated with reduced depressive symptoms across the 3-week periods (RQ3b). Interpersonal turbulence (RQ4) was not significantly associated with changes in depressive symptoms on a between-person level.
To examine the robustness of these effects, we additionally estimated (a) multilevel random slope models, (b) models with alternative specifications (i.e., without gender and sex as covariates, residualized change score model), and (c) a latent change score model (see Table 2 and the OSF page for detailed results). These additional robustness analyses indicate that the overwarming effect (RQ3b) is very robust (i.e., significant effect in every model), the interaction quantity effect (RQ1) is partially robust (only in the model without covariates and latent change score model the effect is barely non-significant, p = .050 and p = .089, respectively), and the effect of other’s warmth (RQ2) is partially robust (not significant in the residualized change score model and in the latent change score model).
At the within-person level, we did not find evidence that burst differences in interaction quantity, interpersonal warmth of others, correspondence of interpersonal warmth, the level of overwarming, or interpersonal turbulence were systematically associated with burst differences in 3-week changes in depressive symptoms.
Our findings on the between-person level suggest that the broader perception of social interactions (as indicated by the mean overall rating) might play a more crucial role in predicting depressive symptoms compared with fluctuations in perceived interactions within each observation period (21-day bursts). At the same time, we cannot rule out that perceptual biases that predict both low overwarming and increases in depression, such as a negative attribution style (e.g., Weary et al., 1987), drove these between-person findings. The absence of within-person effects over 21-day periods could indicate that this timeframe might be too short for capturing consistent patterns of day-to-day interaction changes influencing month-to-month shifts in depressive symptoms. Hence, this set of findings only allows us to make statements about how social interaction characteristics are generally (i.e., the average of all observation periods) associated with how much depressive symptoms changed during the 21-day period. It thus remains unclear what the processes underlying changes in depressive symptoms during those 21-day periods are, as our non-significant within-person effects did not provide us with information about these processes.
Quantity of Social Interactions
On the between-person level, we found that those individuals who generally reported fewer social interactions were more likely to report elevated depressive symptoms. This finding is in line with earlier studies on the association between depressive symptoms—however, assessed only before an ambulatory assessment phase—and the quantity of social interactions (Brown et al., 2011; Elmer & Stadtfeld, 2020; Nezlek et al., 1994; Sun et al., 2019; Villanueva et al., 2020). In these studies—including ours—the effect sizes are relatively small. Given this small effect, the findings of our longitudinal study do not suggest that individuals with elevated depressive symptoms should “just interact more” as this would—according to our results—only lead to a small improvement. Nevertheless, behavior activation of individuals with depressive symptoms in sub-clinical populations may still focus on the quantity of interactions, but one should be aware of the potentially limited contribution to changes in depressive symptoms.
Quality of Social Interactions
The finding on the between-person level highlight that qualitative aspects of social interactions may play a significant role in the development depressive symptoms (Fournier, 2009; Rook, 2001; Zuroff et al., 2007). A number of mechanisms could be responsible for these findings. For example, the presence or the sheer perception of more positive social experiences (as captured by our interpersonal warmth variable) could contribute to feeling more socially included and less lonely (as suggested by behavior activation approaches), thus contributing to a reduction of depressive symptoms (Liu & Rook, 2013). Interestingly, we did not find evidence for an effect of correspondence on 3-week changes in depressive symptoms, as the Theory of Interpersonal Complementary may suggest (Sadler et al., 2011).
We further explored the concept of overwarming, as an addition to its predecessor correspondence, capturing the difference between perceived self and other’s interpersonal warmth. This qualitative feature of social interaction showed robust between-person associations with levels of depressive symptoms. Generally, perceiving others to behave more warmly than oneself could be a manifestation of lower self-esteem, which in turn is related to depression (Sowislo & Orth, 2013). Although we cannot differentiate in our data between the (objectively) observed level of interpersonal warmth displayed in social interaction and the subjective perception of social interactions, we still know that the focal individual perceived that a particular level of interpersonal warmth was displayed in the interaction.
Despite self an’ other’s warmth ratings being generally highly correlated, we find that there is some important information in the discrepancy between the perception of own’s and other’s ratings of interpersonal warmth. Our study reveals that this discrepancy, as represented by the construct of overwarming, is associated with depressive symptoms. This novel and robust finding warrants further exploration. This finding highlights the importance of considering the perceptual differences between self and other’s warmth, which may be more relevant to individuals’ depression trajectories than actual levels of warmth, as these results suggest.
Scientific Relevance
This study used unique multiple-timescale longitudinal data to overcome some of the methodological limitations inherent in the study designs used in previous studies assessing how depressive symptoms prior to an ambulatory assessment phase are associated with later social interactions (e.g., Brown et al., 2011; Elmer & Stadtfeld, 2020; Nezlek et al., 1994; Villanueva et al., 2020). For instance, our study design aimed to assess (all) social interactions for a longer period of time (i.e., bursts of 21 days) for a large number of individuals (N = 133), and thus had relatively good statistical power. 4
Or findings suggest that the Theory of Interpersonal Complementary (Sadler et al., 2011) may be limited to explain changes in depressive symptoms, when the measure of complementary is used as an explanatory factor. Instead, overwarming as an explanatory factory, may be better in predicting changes in depressive symptoms. As such, behavior activation, which is specifically focusing on displaying interpersonal warmth rather than the quantity of social interaction, may be beneficial as a protective or therapeutic factors in the progression of depressive symptoms. Given the importance of interaction qualities, future studies—in particular those using ESMs—should not only ask respondents about the presence of social interactions, but also about the quality of those interactions, including how other’s display of interpersonal warmth and its relative relation to one’s own display interpersonal warmth.
Limitations and Future Research
Four limitations should not go undiscussed. A first limitation of this study is that self- and other’s behavior was measured solely from the viewpoint of the respondent. Hence, we do not know if interaction partners actually behaved in a warmer way relative to the respondent’s behavior or if the perception of warmth correspondence was more biased for individuals whose depressive symptoms were increasing. The correlational nature of this observational study does not provide clear recommendations whether individuals at risk for depression should be encouraged to enhance the actual quality of their social interactions or whether changing their perception of the quality of social interactions is sufficient in achieving the goal. Hence, the use of difference scores in calculating the respondent’s own and other’s interpersonal warmth score may be limited. As outlined by numerous scholars in the past (e.g., Cronbach, 1958; Johns, 1981), difference scores may have limited scientific utility. Johns (1981) concludes that difference scores from the same source (i.e., respondent) should not be used, as they may be unreliable and provide questionable construct validity. Instead, information (e.g., on the interpersonal warmth) from different sources (i.e., the respondent and the interaction partner) should be used. However, in our research design, this was not possible due to the large number of different interaction partners, which did not participate in this study. Future research might obtain independent perceptions of social interaction quality from the viewpoint of both interaction partners, as typically done in social networks research (e.g., Elmer et al., 2017).
A second limitation is that we aggregated data of interaction quality to the level of measurement bursts to assess how the quantity and quality of individuals’ social interactions were related to depression change. As a result, we disregarded the day-to-day dynamics of social interactions and how they might contribute to fluctuations in individuals’ momentary affective states. It would be interesting to investigate how changes in affect moderate the relationship between interaction qualities and changes in depressive symptoms. Future studies should thus further study the dynamics of correspondence and overwarming within daily life and how they are linked to changes in affective states. Sun et al. (2019)—for instance—have investigated how the quantity and quality of social interactions is associated with momentary states of happiness. Yet, how the effects of social interactions on depressive symptoms are mediated by momentary affective states, remains an open question. Along these lines, more studies on moderators of social interactions and affective responses in daily live are needed and how they relate to changes in depressive symptoms (Gloster et al., 2021), including other qualities of social interaction, such as interpersonal dominance, level of intimacy, and meaningfulness.
A third limitation concerns the level of statistical certainty of our analyses. The 95% CIs of the effects relating to our research questions were relatively wide and often were close to including zero. Despite this level of uncertainty, the main findings of this study showed to be robust under various model specifications (see the “Robustness Analyses” section). Nevertheless, future studies should consider using larger sample sizes to obtain more accurate estimates of the investigated effects. It would furthermore be relevant to replicate these findings in samples, where also interactions that are also shorter than 5 minutes are measured. This way, unbalanced interactions might be better represented (assuming that shorter interactions are less balanced and thus shorter).
Finally, as our analyses were on the level of bursts, there were only three Level 1 observations per participant. From a statistical point of view, this might not be a problem as the number of Level 1 observations per participant (Level 2) can be low without biasing the estimation of Levels 1 and 2 direct effects (Maas & Hox, 2005). However, from a conceptual point of view, averaging over only three observation periods to obtain variables for between-person comparisons (e.g.,
Conclusion
This longitudinal study examined the intricate interplay between the quality and quantity of social interactions in daily life and trajectories of depressive symptoms by combining data on moment-to-moment reports of social interactions with month-to-month assessments of depressive symptoms. With its unique empirical setting, combining classical surveys with ESMs, this study shows that interpersonal warmth experienced in social interactions is an important aspect to consider in research on depressive symptoms.
Supplemental Material
sj-docx-1-psp-10.1177_01461672231211469 – Supplemental material for Studying Daily Social Interaction Quantity and Quality in Relation to Depression Change: A Multi-Phase Experience Sampling Study
Supplemental material, sj-docx-1-psp-10.1177_01461672231211469 for Studying Daily Social Interaction Quantity and Quality in Relation to Depression Change: A Multi-Phase Experience Sampling Study by Timon Elmer, Nilam Ram, Andrew T. Gloster and Laura F. Bringmann in Personality and Social Psychology Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work of Timon Elmer was supported by the Swiss National Science Foundation (Grant number: P2EZP1_188022 and PZ00P1_208742). Data collection was supported by the National Institute on Aging (RC1 AG035645). The authors thank the iSAHIB participants for providing such rich data, and David Conroy, Aaron Pincus, and Amy Lorek for collaboration on data collection.
Supplemental Material
Supplemental material is available online with this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.