
Abstract
High subjective social status (SSS) is believed to protect health in the current literature. However, high SSS entails social responsibilities that can be stressful in collectivistic cultural contexts. Here, we tested the hypothesis that those socialized in collectivistic societies (e.g., Japan) recognize their high social status as entailing social duties difficult to ignore even when they are excessive. Using cross-cultural survey data (N = 1,289) and a measure of biological health risk (BHR) by biomarkers of inflammation and cardiovascular malfunction, we found that higher SSS predicted lower BHR for American males. In contrast, higher SSS predicted higher BHR for Japanese males, mediated by the perceived difficulty of disengaging from their current goals. In both cultural groups, females showed no association between SSS and BHR. These findings suggest that social status has differing health implications, depending on the relative salience of privileges and burden-producing responsibilities in different cultural contexts.
Keywords
Humans are inherently hierarchical. Higher social status comes with more tangible and symbolic resources (Kraus et al., 2011; Shah et al., 2012). As may be predicted, social status is a robust predictor of better health. Each step up in social hierarchy is associated with health improvements, such as lower rates of morbidity and mortality from all causes (Adler, 2009; Chetty et al., 2016). Of interest, the same effect is even more robust when the status is assessed with one’s perceived social standing in the hierarchy, referred to as subjective social status (SSS) (Adler et al., 2000; Cundiff & Matthews, 2017). In particular, perceived status within one’s self-defined community (Adler & Stewart, 2007) is reliably associated with various health markers, such as health behaviors, self-rated health, and biomarkers of health (see Quon & McGrath, 2014; Zell et al., 2018 for reviews). So far, however, the health impact of SSS has rarely been tested with biological markers of health risk outside of the West. The near-exclusive focus on Western samples is a major limitation because, as we shall elaborate, the meaning and function of social status are culture-dependent and SSS could carry the potential of posing health risks in cultures outside of the West. The current work aimed to address this gap by testing the hypothesis that higher social positions entail stronger role-based expectations and duties in collectivistic cultural contexts (i.e., in Japan). Thus, in Japan, unlike in the United States, higher SSS may predict higher biological health risk (BHR), as revealed in increased levels of inflammation and cardiovascular malfunction.
Culture and Social Status: Privilege and Burden
Higher SSS offers various psychological benefits because it affirms the self’s worth. It may boost one’s self-esteem or confidence and make the person feel that they are respected in their community. Hence, it would seem intuitive that SSS is linked to better health and, indeed, the evidence is mounting that the social status–health gradient is mediated, in part, by increased psychosocial resources, such as feelings of control (Cohen et al., 1999), self-esteem (Schnittker, 2004), and optimism (Matthews et al., 2008). Another pathway involves stress and adversity, which could be less likely or less severe for those with higher social status (Taylor & Seeman, 1999), leading to positive associations between SSS and better health.
However, this literature ignores another, potentially darker aspect of social status. Along with various benefits of higher social status noted above, social status could come with duties and obligations to relevant social entities, such as family, school, and work. Those high in social status may enjoy privileges, but they may also have to assume various responsibilities for their subordinates (Sassenberg et al., 2012; Scholl et al., 2018). For example, they have to make important decisions for the group and ensure that important goals are being met for the group. Furthermore, such work-related duties may entail another responsibility to maintain social harmony or smooth social relations in the section they manage (Chen et al., 2001; Torelli & Shavitt, 2010). This social maintenance function even extends beyond work contexts. The higher one’s social status becomes, the more pressure they may experience to take care of their local communities. When the amount of expected responsibility exceeds one’s capacity, and thus, is perceived as demanding, individuals with high status may experience stress, including physiological threat responses (Scholl et al., 2018). Such threat, accumulated over time, may increase health risks.
Critically, the salience of such obligations and duties associated with high status may differ between Western and Eastern societies (Miyamoto et al., 2018; Zhong et al., 2006). Compared with Western societies, East Asian societies are lower in individualism or higher in collectivism (Hofstede, 1980)—a finding verified more recently by various researchers using multiple indicators of the values favoring social welfare over individual rights or freedom (Schulz et al., 2019; Welzel, 2013). Moreover, there is an increasing consensus that collectivism, common in East Asia, comes with tighter social norms (Gelfand et al., 2011). These norms may enforce social hierarchy strongly in East Asia, which is thought to be quite high in “power distance,” especially compared with most Western societies (e.g., Hofstede’s power distance score of 54 in Japan vs. 40 in the United States). Defined as the perception and acceptance of power inequality, power distance implies conformity to supervisors at workplaces and those who are above in the hierarchy more broadly. Consistent with this, East Asian societies are higher in “vertical collectivism,” emphasizing the maintenance of hierarchical systems through self-sacrifice and group conformity (Triandis & Gelfand, 1998). The combination of collectivism, tightness, and power distance that characterizes East Asian societies likely increases obligations and duties of higher status. Indeed, Miyamoto et al. (2018) showed that high-status people in East Asian societies tend to endorse more other-oriented socialization values, including a sense of responsibility, whereas such an association is either nonexistent or reversed in Western societies. Similarly, the mental representation of power involves influence and entitlement in Western societies, whereas it is associated with responsibility in East Asian societies (Zhong et al., 2006).
We thus propose that in East Asian societies, including Japan, the status-based obligations and duties of high social status are rigidly enforced and cognitively highly salient for those working in the system. In these cultural contexts, the demand associated with such obligations and duties could easily overwhelm any privileges and benefits that could come with higher social status. Consistent with this hypothesis, contrary to the standard finding in the West (Mackenbach et al., 2008), the mortality rate is higher for Japanese workers with higher status jobs (e.g., administrative, professional, and/or engineering jobs) than those with menial jobs (Wada et al., 2012). However, it is not clear whether this pattern extends to biological health with a direct measure of social status. The first aim of this work was to address this gap by examining the effect of SSS on biomarkers of inflammation and cardiovascular malfunction in American and Japanese midlife adults.
Goal Disengagement as a Mediating Mechanism
Our hypothesis holds that people with high SSS are stressed out in East Asian societies, including Japan, because they consider it their duty and obligation to meet role expectations. Social duties and obligations may become their personal goals. Moreover, because of their identities as group members, they may find it very hard to disengage themselves from such goals even when the work demands exceed the maximum they can handle. In other words, as individuals move up the ladder, they will find it increasingly more difficult to adopt goal disengagement as a possible coping strategy in mitigating the adverse health impact of high role-based social demands. Accordingly, we may expect that higher SSS predicts worse biological health among Japanese, mediated by the perceived difficulty of disengaging from the current goals—that is, higher social status → difficulty in goal disengagement → impaired health.
Our second aim was to test this prediction. In the current stress and coping literature, goal disengagement is conceptualized as a coping strategy to change the self to adjust to situational constraints by lowering one’s aspirations and challenges. Such a strategy (called the secondary control strategy) is typically distinguished from a primary control strategy, which involves changing the environment to satisfy one’s needs and desires (Rothbaum et al., 1982). Both types of coping strategies may afford a sense of control, thus predicting better adjustment and health (Wrosch et al., 2011). But whereas the primary control strategy is effective if stressors are acute and temporary, the secondary control strategy tends to be more adaptive for chronic and recurrent stressors (Heckhausen, 1997). For example, prior evidence links goal disengagement to better adjustment and wellbeing outcomes among those suffering from chronic health conditions (Hall et al., 2010; Thompson et al., 1994). Because social obligations and duties are constant and ongoing tasks in one’s social life, stresses linked to them are likely both chronic and recurrent. Hence, goal disengagement can be a particularly effective coping strategy to deal with such stresses. Conversely, high-status Japanese may not be able to readily adopt this coping strategy because of social expectations they face, resulting in a particularly high risk of impairing their health. Accordingly, Japanese with higher SSS would find it hard to use goal disengagement as a coping strategy, and consequently, they would exhibit evidence of impaired health.
Does Gender Matter?
In addressing our aims, we further explored how gender may be implicated in the cultural differences expected in the social status–health link. We might expect the impact of social status to be less pronounced for women than for men. Such a possibility is suggested by a growing body of work on gender stereotypes in achievement domains. A strong desire to attain social status conveys masculinity (Rudman & Kilianski, 2000; Sczesny et al., 2018) and thus is incongruent with prescribed gender stereotypes of femininity (Eagly & Karau, 2002), thereby inviting a backlash against women seeking higher status (Rudman et al., 2012). Conversely, when women behave in stereotypically feminine ways, they conform to the gender norms, but in part, because of this, they may be perceived as inferior and incompetent, thereby undermining their opportunity to climb up the social hierarchy (Heilman, 2012). The resulting conflict between gender norms and achievement may diminish many women’s interest in power and status (Schwartz & Rubel, 2005). Conversely, men are relatively free from such a conflict, and consequently, they may be more unequivocally motivated to achieve higher status and be dominant (Carré & Olmstead, 2015; Eisenegger et al., 2011).
Consistent with the analysis above, growing evidence suggests that the association between social status and various health markers, including inflammation (Freeman et al., 2016) and respiratory illness (Singh-Manoux et al., 2003), is weaker among women than men. Building on this initial evidence, we explored whether the hypothesized cultural difference in the SSS–BHR link might be stronger for men than women.
The Present Research
To test our analysis, we drew on representative samples of American and Japanese adults from the cross-culturally matched surveys—Midlife in the United States (MIDUS) and Midlife in Japan (MIDJA), which included the MacArthur community ladder index of SSS (Adler & Stewart, 2007). Following prior work in the area (Hartanto et al., 2020; Kitayama & Park, 2021; Kitayama et al., 2015, 2018; Park et al., 2020), we tested BHR by combining two biomarkers of inflammation (interleukin-6 [IL-6] and C-reactive protein [CRP]) and two biomarkers of cardiovascular malfunction (systolic blood pressure [SBP] and the ratio of total to high-density lipoprotein choesterol [T/HDL]).
Researchers used the same dataset to test how culture may moderate the association between BHR and various psychosocial variables. The variables tested include negative affect (Park et al., 2020), anger expression (Kitayama et al., 2015), neuroticism (Kitayama et al., 2018), and conscientiousness (Kitayama & Park, 2021). However, none tested the association between SSS and BHR. One recent study focused on one of the four markers constituting BHR (i.e., CRP) and found that higher SSS predicted lower CRP levels among Americans but not among Japanese (Yong et al., 2021). We went beyond this study in three ways. First, we used a more encompassing measure of BHR, including three theoretically relevant biomarkers besides CRP. Second, we explored whether gender might moderate the predicted cultural difference in the association between SSS and BHR. Third, we tested whether the positive association between SSS and BHR, expected for Japanese, possibly, especially for Japanese males, might be mediated by goal disengagement. That is, among Japanese, those high in social status may find it hard to disengage themselves from their goals (of performing their role-based duties). This difficulty in goal disengagement, in turn, may result in greater BHR.
Method
Participants
The American participants were from the MIDUS survey, which began in 1995 based on a national sample of noninstitutionalized adults, recruited from the 48 contiguous states via random digit dialing (MIDUS I; N = 7,108). The second wave was conducted 9 to 10 years later (MIDUS II; N = 4,963; retention rate = 75%) and involved five projects (psychosocial assessment, daily diary study, cognitive function assessment, biomarker assessment, and neuroscience assessment). Our analysis focused on a subsample of the MIDUS II participants who completed both psychosocial and biomarker assessments. After completing the self-administered survey for psychosocial assessment, participants traveled to one of the three General Clinical Research Centers (Madison, WI; Washington, DC; or Los Angeles, CA) for an overnight visit, where they provided blood samples for biomarker assays (N = 1,054; 578 females, Mage = 58.04, SDage = 11.62). The American sample consisted of mostly European Americans and a small number of racial minorities (32 African Americans, six Native Americans, five Asian Americans, one Multiracial, 30 others, and four missing race information). We excluded racial minorities and focused on 976 European Americans (531 females, Mage = 58.36, SDage = 11.69) to maximize the cultural contrast with Japanese (see Kitayama et al., 2018; Park et al., 2020 for the same approach).
The Japanese data were drawn from a companion survey conducted in Japan, called MIDJA. The first wave of this survey began in 2008 with 1,027 Japanese recruited from the Basic Resident Register Book for the Tokyo metropolitan area (23 wards) (522 females, Mage = 54.36, SDage = 14.15). The sample was stratified by gender (two groups: men and women) and age (five groups defined in a 10-year bracket: 30–39, 40–49, 50–59, 60–69, and 70–79 years), resulting in a total of 100 people in each of the 10 strata. The 100 people in each stratum were recruited proportionally based on the number of registered residents in each ward to obtain a representative sample of respondents across the 23 wards. Biomarker data were collected from a subsample of the MIDJA I participants who provided blood samples at a medical clinic near the University of Tokyo (N = 382; 214 females, Mage = 55.47, SDage = 14.04).
We did not estimate a sample size based on an a priori power analysis because the present work was based on the secondary analysis of archival data (https://www.icpsr.umich.edu/icpsrweb/). Given that the sample size was known, we conducted a sensitivity power analysis using G*Power (version 3.1; Faul et al., 2009) to determine the minimum effect size that our regression analysis with three predictors (culture, gender, and SSS) could detect. With the final sample size of 1,289 (after listwise deletion of the cases with missing data), there was an 80% chance of detecting a small effect (f2 = .01) (α = .05, two-tailed).
Measures
Subjective Social Status
SSS was measured with the MacArthur community ladder (Adler & Stewart, 2007). Participants were presented with an illustration of a 10-rung ladder and asked to indicate which rung corresponded to their relative standing within their community (1 = lowest standing, 10 = highest standing). Participants were instructed to choose a community that was most meaningful to them.
Biological Health Risk
A composite index of BHR was created by combining two biomarkers of pro-inflammatory cytokines (IL-6 and CRP) and two biomarkers of cardiovascular health (SBP and the ratio of T/HDL cholesterol). During the clinic visit, a trained staff obtained resting levels of SBP. Participants were asked to relax in a seated position while their SBP levels were measured three times, with 30-second intervals. The two most similar readings were averaged to yield an index of SBP. Fasting blood samples were also collected at the clinic visit. For Americans, blood samples were collected in (a) three 10-mL serum separator tubes, (b) two 4-mL ethylenediaminetetraacetic acid (EDTA) tubes, and (c) one 4- or 2.7-mL sodium citrate tube. For Japanese, the samples were collected in (a) two 8.5-mL serum separator tubes, (b) two 1.8-mL citrated tubes, (c) one 2.0-mL FNa tube, and (d) one 2.0-mL EDTA2K tube. The samples from both cultural groups were frozen and stored in a −60°C to −80°C freezer before being shipped to the Biocore Laboratory at the University of Wisconsin, Madison, WI.
The frozen serum and plasma samples were then assayed for IL-6, CRP, and cholesterol. IL-6 was assayed at the Biocore Laboratory, while CRP and cholesterol assays were performed at the Laboratory for Clinical Biochemistry Research (University of Vermont, Burlington, VT) and at the Meriter Laboratories (GML) (Madison, WI), respectively. High-sensitivity enzyme-linked immunosorbent assay (ELISA) method (Quantikine; R&D Systems, Minneapolis, MN) was utilized to determine serum IL-6 levels, with a lower sensitivity of detection at 0.16 pg/mL. Duplicate determinations were performed for each sample and values that are higher than 10 pg/mL were rerun in diluted sera so that all values would fall on the standard reference curve (0.45–9.96 pg/mL). The intra-assay and inter-assay coefficients of variation (CV) values of IL-6 were 3.2% and 12.3%, respectively. A BNII immunonephelometry (BNII Nephelometer 100 Analyzer; Dade Behring Inc., Deerfield, IL) was utilized to determine plasma CRP levels, with a reference assay range of ≤3 µg/mL. For CRP, the intra-assay and inter-assay CVs were 2.3% to 4.4% and 2.1% to 5.7%, respectively. Cholesterol data (total and HDL) were assayed using a Cobas Integra analyzer (Roche Diagnostics, Indianapolis, IN), with reference ranges of <200 and >40 mg/dL, respectively. The intra-assay and inter-assay CVs of total cholesterol were 0.5% to 0.8% and 2.6%, while those of HLD cholesterol were 1.1% to 1.4% and 6.5%, respectively.
As displayed in Table 1, the four biomarkers were positively correlated for both cultural groups. To formally test whether these four indices coherently represent a single latent construct of BHR, we conducted culture-wise principal component analyses (PCAs) and found that the four biomarkers loaded on a single factor, accounting for 41.1% and 50.1% of the variance for Americans and Japanese, respectively (see Table 1 for factor loadings). Following prior work (Hartanto et al., 2020; Kitayama & Park, 2021; Kitayama et al., 2015, 2018; Park et al., 2020), we conducted the PCA on the total sample and used the resulting factor scores as an index of BHR.
Factor Loadings and Intercorrelations among the Four Biomarkers.
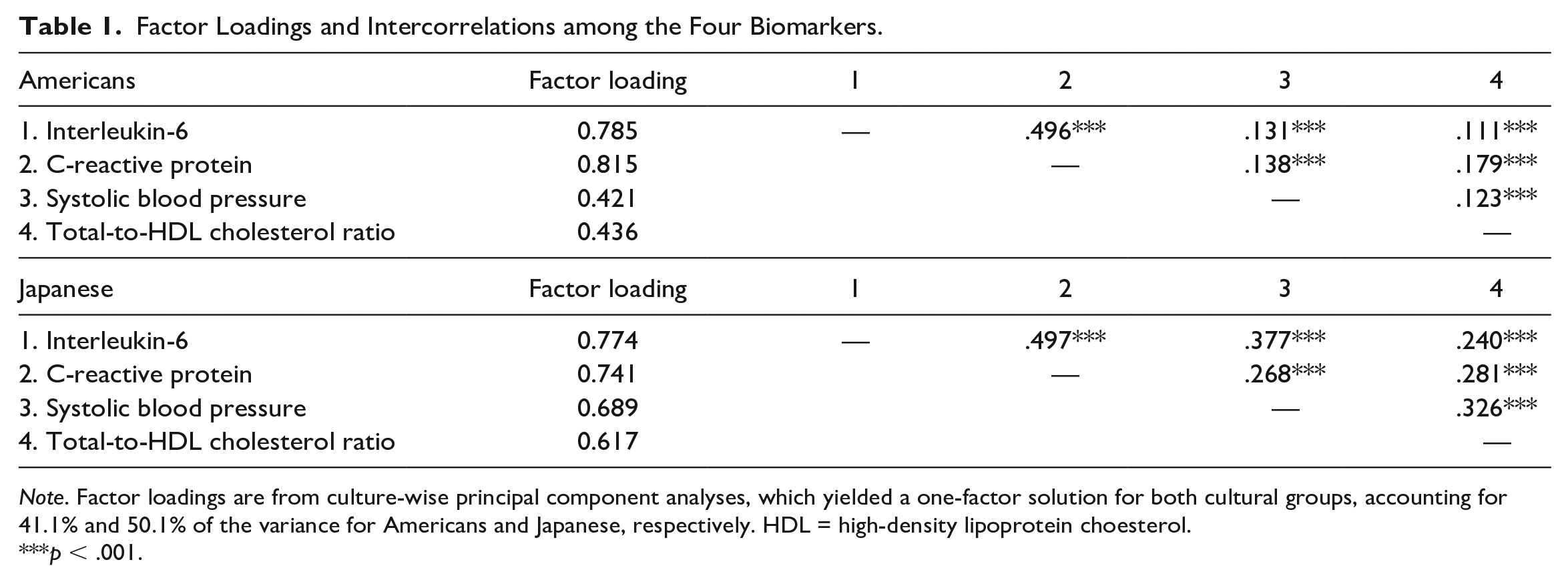
Note. Factor loadings are from culture-wise principal component analyses, which yielded a one-factor solution for both cultural groups, accounting for 41.1% and 50.1% of the variance for Americans and Japanese, respectively. HDL = high-density lipoprotein choesterol.
p < .001.
Self-Rated Health
We assessed participants’ perceived health to examine whether the hypothesized cultural difference in the health effect of SSS is equally pronounced for both objective and subjective indicators of health. Participants answered a single-item question about their current health status using a 11-point scale (0 = worst possible health, 10 = best possible heath) (Prenda & Lachman, 2001).
Goal Disengagement and Other Coping Strategies
We hypothesized that the health-compromising effect of high social status in Japan would be accounted for by the reduced use of goal disengagement. To test this hypothesis, we assessed goal disengagement with one of the subscales of secondary control, lowering aspirations, developed by Wrosch et al. (2000). Participants read five statements (e.g., “When my expectations are not being met, I lower my expectations”) and indicated how well each item described them using a 4-point scale (1 = not at all, 4 = a lot; αs = .59 and .67 for Americans and Japanese, respectively). In addition, the scale also assessed two other control strategies—(a) persistence in goal striving as a primary control strategy (five items; e.g., “When faced with a bad situation, I do what I can do to change it for the better”; αs = .77 and .80) and (b) positive reappraisals as another type of secondary control strategy (four items; e.g., “I can find something positive, even in the worst situations”; αs = .78 and .79). For an exploratory purpose, we also tested possible mediating effects of these two control strategies.
Covariates
In all analyses, we adjusted for the effects of potential confounding variables that might account for the relationship between SSS and BHR, including demographic variables (age and objective social status), health behaviors (smoking status and alcohol consumption), and health status (chronic conditions and body mass index [BMI]).
Demographic Variables
Participants’ age ranged from 35 to 86 for Americans and 31 to 80 for Japanese. Objective social status was assessed as a composite index of educational attainment and occupational type. Educational attainment was originally assessed with a 12-point scale in the United States (1 = 8th grade, junior high school, 12 = PhD or other professional degree) and an 8-point scale in Japan (1 = 8th grade, junior high school graduate, 8 = graduate school). The responses were rescaled using a 7-point scale (1 = 8th grade, junior high school, 7 = attended or graduated from graduate school) to make the scores comparable across the cultural groups. Occupational type was measured using a 3-point scale (1 = manual, blue-collar, or service, 2 = nonmanual, white-collar, or clerical, 3 = managerial or professional). The measures of educational attainment and occupational type were then standardized and averaged to create a single index of objective social status (see also Kitayama et al., 2015; Park et al., 2013).
Health Behaviors
Because smoking and alcohol consumption are two major behavioral risk factors for inflammation and cardiovascular malfunction (O’Connor et al., 2009; O’Connor & Irwin, 2010), we controlled for these variables. Two dummy-coded variables were created to compare non-smokers as the reference group with former-smokers and current-smokers, respectively. Alcohol consumption was measured as an average number of alcohol drinks participants consumed per week.
Health Status
We also controlled two markers of current health status that could predict inflammation and cardiovascular functioning, including chronic health conditions and obesity. Chronic conditions were assessed as the number of chronic health problems (e.g., diabetes, asthma, tuberculosis; up to 30) participants reported having experienced in the past year. BMI was used as an index of obesity, computed using the measurements of weight and height obtained during the clinic visit (kg/m2). The BMI scores were log-transformed to normalize the distribution.
Data Processing and Analytic Strategies
We inspected the raw data for all variables and found a small number of outliers (i.e., extreme values exceeding 3 standard deviations from their mean) across variables, including the four biomarkers (ns < 29), alcohol consumption (n = 27), and BMI (n = 11). Following the standard approach in MIDUS and MIDJA, we winsorized these values at ±3 standard deviations from its mean within each culture (see Kitayama & Park, 2021; Kitayama et al., 2015, 2018; Miyamoto et al., 2013; Park et al., 2020 for the same approach). As noted above, because the winsorized scores for the four biomarkers and BMI did not follow normal distributions, these values were log-transformed before submitting to analyses.
Observations were available for all predictor and outcome variables, including covariates, for most participants (94.9%). For the final analysis, we focused on this subsample after listwise deletion of the cases with missing data (n = 69). This approach, known as a complete case analysis (CCA), provides unbiased results for regression models when the chance of having complete (vs. missing) data does not depend on an outcome after taking into account covariates (Bartlett et al., 2014; Hughes et al., 2019). In the current sample, participants who have complete data and those who do not did not differ in BHR after controlling for the covariates, F(1, 1297) = 1.66, p = .198, suggesting that the CCA is an appropriate analytic approach. To ensure that the results are robust, we also used multiple imputation of the missing data and confirmed that the results did not change (see Note 1). See Table 2 for descriptive statistics of all study variables. We report all measures and exclusions in this study.
Descriptive Statistics of Study Variables for Two Cultural Groups.
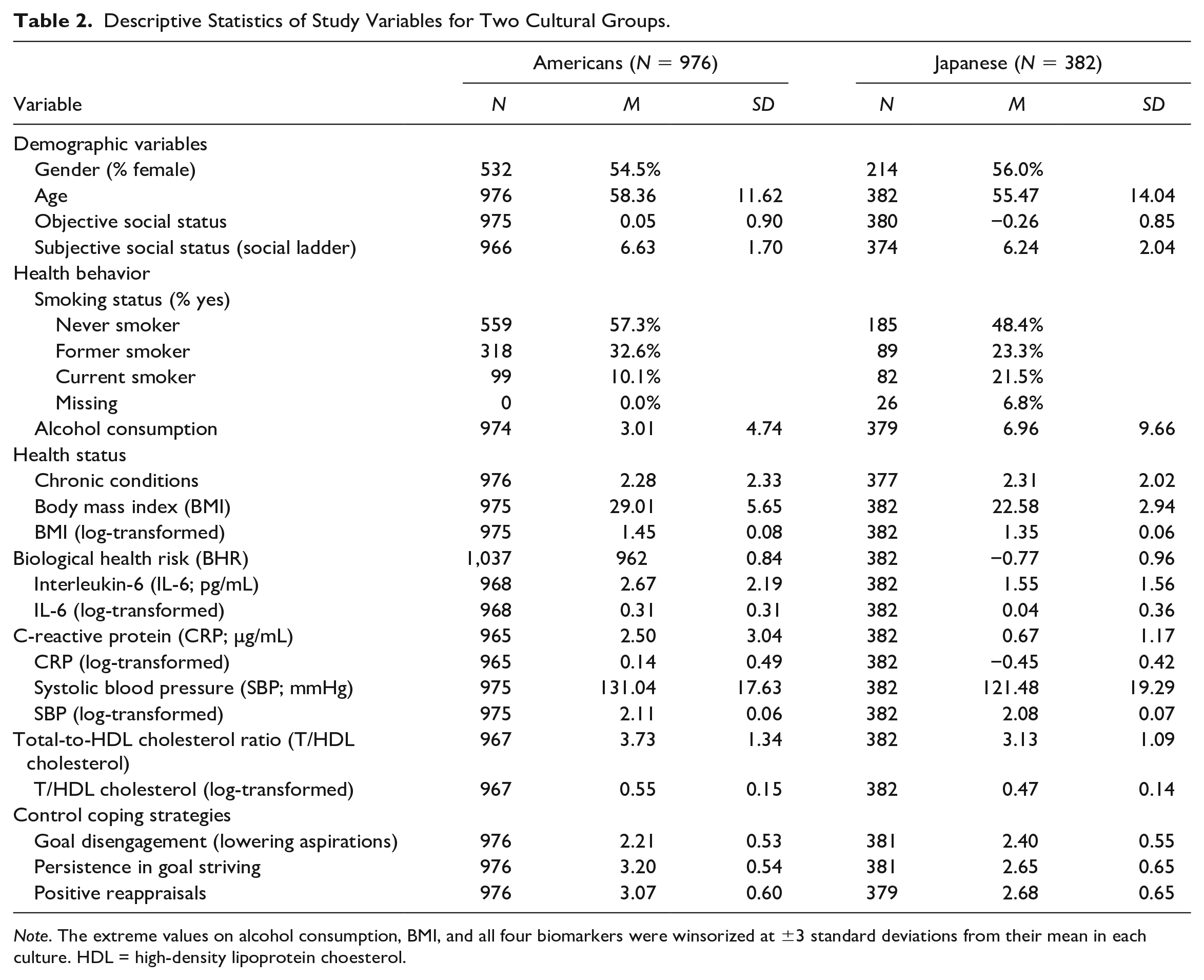
Note. The extreme values on alcohol consumption, BMI, and all four biomarkers were winsorized at ±3 standard deviations from their mean in each culture. HDL = high-density lipoprotein choesterol.
Results
Descriptive Statistics
To examine whether cultural and/or gender groups differed in key variables, we first conducted a Culture (Americans vs. Japanese) × Gender (Males vs. Females) analysis of variance (ANOVA) on SSS. The main effect of culture was statistically significant, F(1, 1336) = 11.21, p = .001,
When we performed the same analysis on BHR, both main effects of culture and gender were significant, F(1, 1340) = 404.99, p < .001,
Subjective Social Status and Biological Health Risk
We predicted that for Americans, higher SSS would be associated with reduced BHR. In contrast, we predicted that this relationship would be reversed for Japanese. We also explored whether gender might moderate the hypothesized cultural difference. Such a moderation would imply a three-way interaction between culture, gender, and SSS. We tested this model by performing a multiple regression analysis after controlling for age, objective social status, smoking status, alcohol consumption, chronic conditions, and BMI. SSS was grand-mean centered before computing the interaction terms (see Table 3A for regression coefficients).
Regression Coefficients in Predicting (A) Biological Health Risk and (B) Self-Rated Health as a Function of Culture, Gender, and SSS.
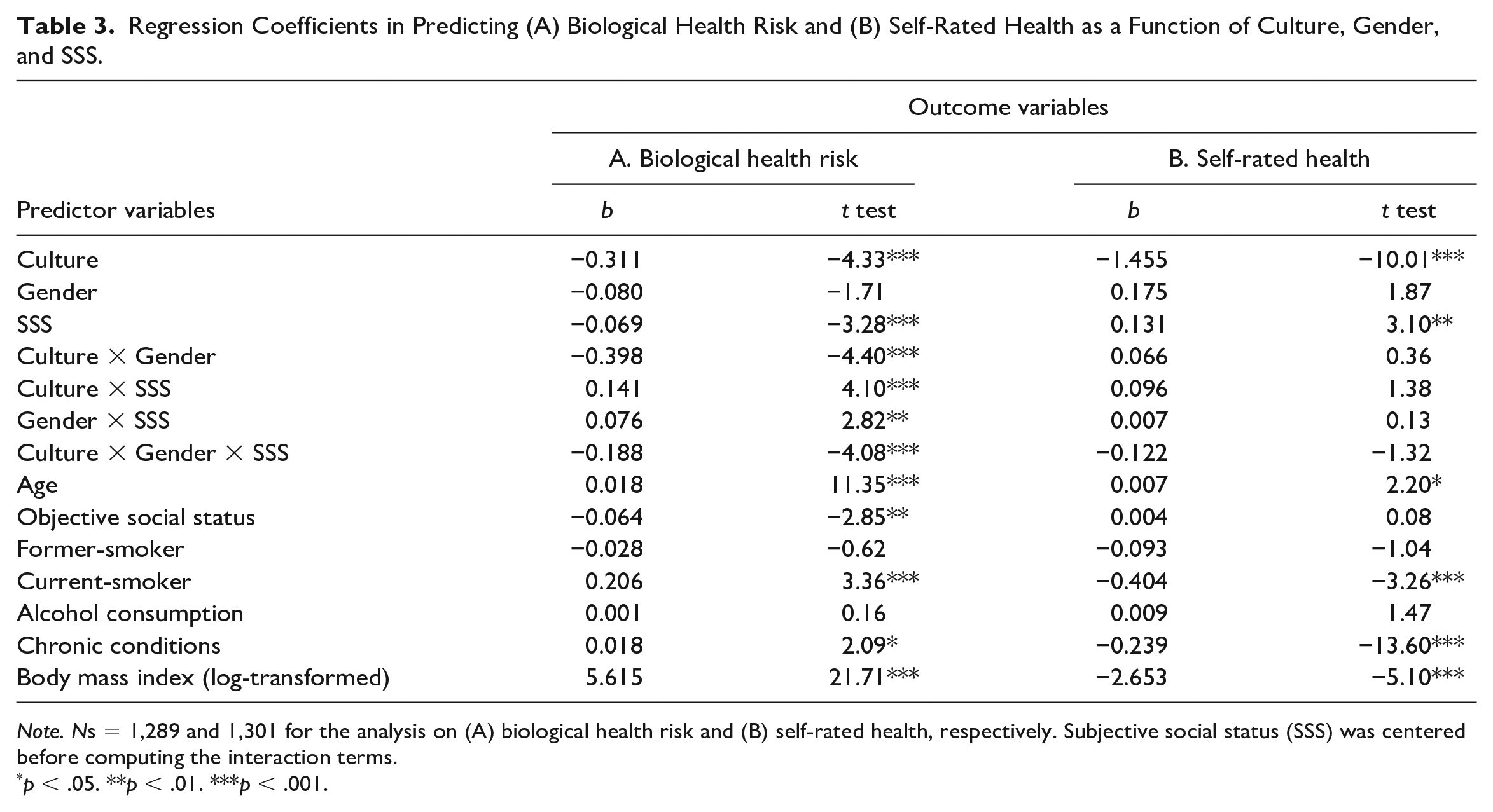
Note. Ns = 1,289 and 1,301 for the analysis on (A) biological health risk and (B) self-rated health, respectively. Subjective social status (SSS) was centered before computing the interaction terms.
p < .05. **p < .01. ***p < .001.
First, the main effect of culture was significant, b = −0.311, 95% CI = [−.452, −.170], t(1274) = −4.33, p < .001. As reported above, Americans showed higher levels of BHR than did Japanese. The main effect of gender was not statistically significant, b = −0.080, 95% CI = [−.171, .012], t(1274) = −1.71, p = .087. Of note, there was a significant main effect of SSS, b = −0.069, 95% CI = [−.111, −.028], t(1274) = −3.28, p = .001, with higher social standing linked to reduced BHR. However, this SSS main effect must be interpreted in the context of all three two-way interactions, which proved statistically significant, ts < 2.82, ps < .005, including the critical Culture × SSS interaction effect. Moreover, the three-way interaction involving culture, gender, and SSS proved significant, b = −0.188, 95% CI = [−.278, −.098], t(1274) = −4.08, p < .001.
To interpret the three-way interaction effect, we examined the Culture × SSS interaction separately for each gender group. The interaction effect was statistically significant among men, b = 0.141, 95% CI = [.071, .211], t(581) = 3.96, p < .001. As shown in Figure 1A, for American males, higher SSS was linked to decreases in BHR (i.e., improved health), b = −0.065, 95% CI = [−.108, −.022], t(581) = −2.97, p = .003. In contrast, this effect was completely reversed for Japanese males, with higher SSS linked to elevated levels of BHR (i.e., compromised health), b = 0.076, 95% CI = [.019, .132], t(581) = 2.64, p = .009. In contrast, the Culture × SSS interaction was not significant among females, b = −0.043, 95% CI = [−.101, .015], t(686) = −1.44, p = .149. The relationship between SSS and BHR was negligible for both American females, b = 0.000, 95% CI = [−.034, .034], t(686) = 0.02, p = .988, and Japanese females, b = −0.043, 95% CI = [−.091, .006], t(686) = −1.73, p = .084 (see Figure 1B). 1
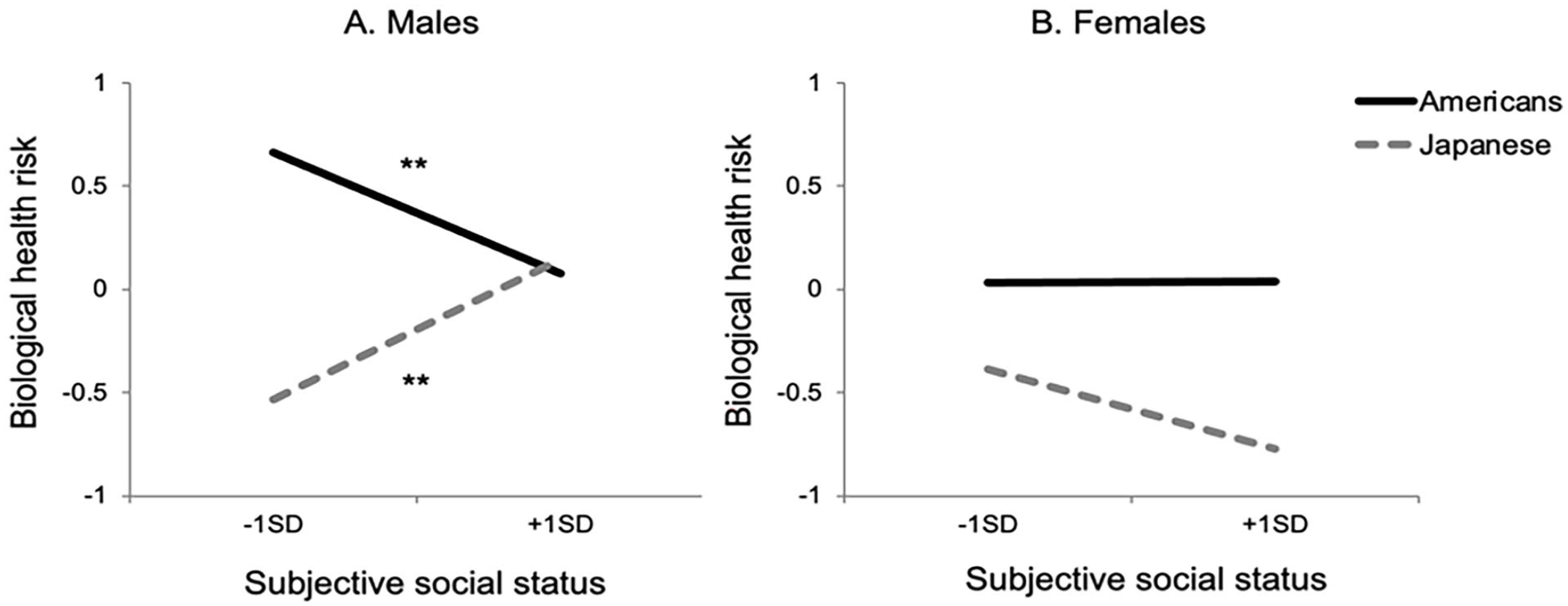
Biological Health Risk as a Function of Subjective Social Status for Americans (Solid Line) and Japanese (Dotted Line) for (A) Males and (B) Females.
When we examined each biomarker constituting the composite index of BHR separately, the three-way interaction between culture, gender, and SSS was significant on three out of the four biomarkers, including CRP, SBP, and T/HDL cholesterol, b = −0.069, 95% CI = [−.124, −.013], t(1277) = −2.44, p = .015, b = −0.008, 95% CI = [−.015, −.001], t(1287) = −2.21, p = .027, and b = −0.034, 95% CI = [−.051, −.018], t(1279) = −4.02, p < .001, respectively (see Supplemental Table S1 for full regression results). Although the three-way interaction effect was not significant for IL-6, b = −0.024, 95% CI = [−.062, .014], t(1280) = −1.26, p = .208, a similar pattern of the results was also observed on this variable. The Culture × SSS interaction effect tended to be pronounced among males, b = 0.027, 95% CI = [−.001, .055], t(585) = 1.88, p = .061, but not among females, b = −0.001, 95% CI = [−.026, .024], t(688) = −0.08, p = .939. 2
Mediation by Goal Disengagement
Next, we tested whether the relationship between higher SSS and increased BHR, observed among Japanese males, was mediated by reduced use of goal disengagement strategy (i.e., lowering aspirations)—that is, higher SSS → less use of goal disengagement → higher BHR. Because the adverse effect of high SSS is apparent only among males, this mediation was expected for males, but not for females. This implies a moderated mediation, in which the indirect effect of goal disengagement (mediator) on the association between SSS (predictor) and BHR (outcome variable) is contingent on gender (moderator) (Hayes, 2012). We tested this model in SPSS using Hayes PROCESS Model 8 with 5,000 bootstrapping samples. The same set of the covariates included in the main analysis was also included in this model as additional predictors.
As hypothesized, the mediating path was significant among Japanese males, 95% bootstrapping CI = [.002, .032]. Higher SSS was associated with lower levels of goal disengagement, b = −0.056, 95% CI = [−.101, −.012], t(328) = −2.48, p = .014, which, in turn, was associated with increased BHR, b = −0.232, 95% CI = [−.368, −.096], t(327) = −3.35, p < .001 (see Figure 2A). In contrast, the same mediation was not significant for Japanese females, 95% bootstrapping CI = [−.015, .007], because their SSS did not predict goal disengagement, b = 0.013, 95% CI = [−.027, .053], t(328) = 0.64, p = .526. As implied by this pattern of gender difference, the moderated mediation was statistically significant, Hayes index = −.016, 95% bootstrapping CI = [−.040, −.003]. For an exploratory purpose, we also tested whether other indices of control coping strategies (persistence in goal striving and positive reappraisals) mediated the SSS–BHR link among Japanese males (but not among Japanese females) by conducting the same moderated mediation analysis separately for each coping strategy. The moderated mediation was not statistically significant for both persistence in goal striving and positive reappraisals, 95% bootstrapping CIs = [−.015, .002] and [−.015, .006], respectively, as there was no gender difference in the association between SSS and each coping strategy, ts < 1.47, ps > .142.
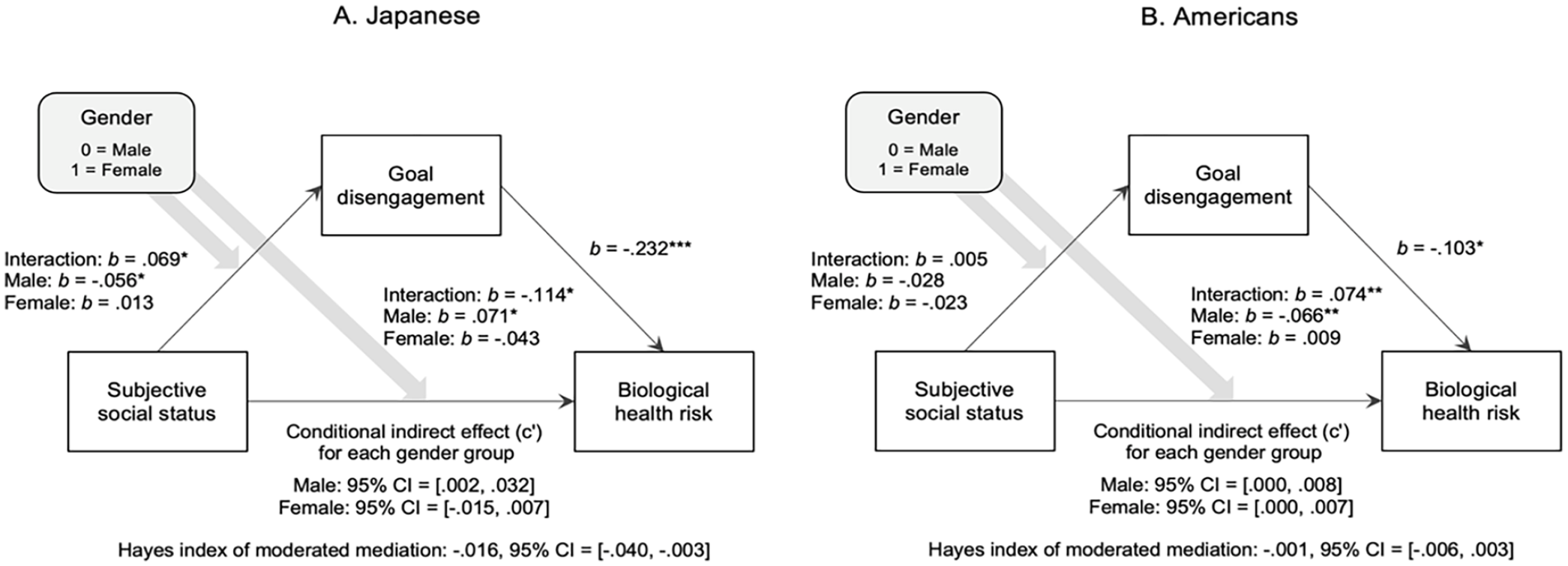
Indirect Effects of Goal Disengagement on the Relationship Between Subjective Social Status and Biological Health Risk among (A) Japanese and (B) Americans.
We did not have any a priori prediction regarding the role of goal disengagement strategy among Americans. Nonetheless, given that we found a significant association between SSS and BHR among American males, we explored whether increased use of goal disengagement (as well as other control coping strategies, see below) accounted for the salubrious effect of high status among American males—that is, higher SSS → greater use of goal disengagement → lower BHR. As we found no association between SSS and BHR among American females, we conducted the same moderated mediation analysis described above to examine whether the indirect effect of goal disengagement would be moderated by gender. As shown in Figure 2B, the moderated mediation model was not statistically significant, Hayes index = −.001, 95% bootstrapping CI = [−.006, .003], because there was no interaction effect between gender and SSS in predicting goal disengagement, b = 0.005, 95% CI = [−.035, .045], t(938) = 0.23, p = .819. Critically, there was no evidence that the increased use of goal disengagement accounted for the SSS–BHR link among American males, as their social status did not predict the use of goal disengagement strategy, b = −0.028, 95% CI = [−.059 .004], t(938) = −1.72, p = .085. We also conducted the same exploratory analyses to test whether persistence in goal striving and positive reappraisals each contributed to the SSS–BHR link among American males (but not among American females), and neither did, 95% bootstrapping CIs = [−.002, .005] and [−.006, .001], respectively. For both coping strategies, there was no evidence of the interaction between gender and SSS, ts <|−1.69|, ps > .092.
SSS and Self-Rated Health
Finally, we examined whether culture and gender would also moderate the relationship between SSS and subjective health by performing a multiple regression analysis with the same set of covariates. We found a significant main effect of culture, b = −1.46, 95% CI = [−1.74, −1.17], t(1286) = −10.01, p < .001, indicating that Americans reported better health than Japanese. The SSS main effect was also significant, b = 0.131, 95% CI = [.048, .214], t(1286) = 3.10, p = .002; higher SSS predicted better subjective health. The gender main effect was not significant, b = 0.175, 95% CI = [−.009, .358], t(1286) = 1.87, p = .062. In addition, neither the two-way interactions nor the three-way interaction was statistically significant, ts < 1.38, ps > .169 (see Table 3B).
Discussion
Subjective Social Status and Biological Health: Culture and Gender Effects
Our work shows that the link between SSS and biological health depends on culture and gender. High SSS predicted better biological health (assessed by inflammation and cardiovascular functions) among American males, consistent with prior work (Cundiff & Matthews, 2017). However, high SSS predicted worse biological health among Japanese males. Females’ biological health had no association with SSS. Note that the culture-dependent effect of SSS did occur after controlling for objective indicators of social status, including education and occupational prestige. Hence, our effects are psychological, independent of objective social resources, such as wealth, income, occupational prestige, and the like.
Our findings go beyond the early work by Yong et al. (2021). Replicating their analysis, we found a negative association between SSS and health risk for Americans, which goes away for Japanese. However, we showed that this cultural difference is limited to males. Moreover, when only males are analyzed, there is an opposite association for Japanese males, with SSS predicting compromised health. As important, we found that the cultural and gender moderation of the association between SSS and health goes beyond the particular biomarker, CRP, which was tested by Yong et al. (2021). We found consistent patterns across four relevant biomarkers, with the findings most clear-cut when the composite measure of BHR was employed.
A Theoretical Integration
Figure 3 shows a theoretical framework to understand the cultural and gender moderation of the association between SSS and biological health. We propose that the perception that one is higher in status in a significant social group entails two possible effects. First, it may come with various psychological benefits based on affirming the self as someone who makes “it.” These benefits are contingent on personal achievement implied by higher social status. Second, however, it can also entail social responsibility of responding to role-based expectations. This responsibility is premised on one’s commitment to the social group.
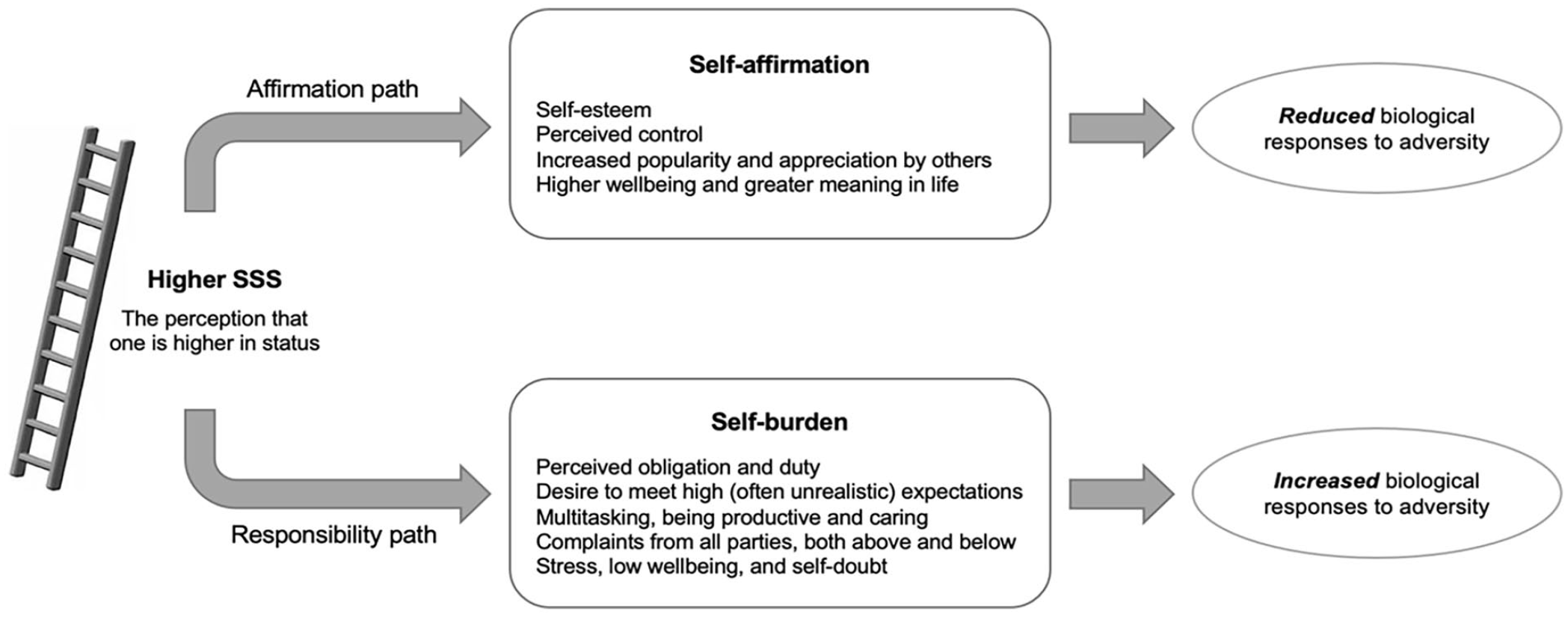
Conceptual Framework Linking SSS to Biological Health Risk.
First, consider individualistic societies. In such societies, the self is construed as independent, which makes the self’s personal attributes, including self-esteem and achievement, highly salient and central to how the self is experienced. In contrast, its more social and relational aspects are neither cognitively salient nor central to each person’s identity (Markus & Kitayama, 1991). They are perhaps acknowledged but unlikely to be elaborated. Hence, the beneficial effects of high SSS may be expected to be more dominant. That is, the perception of the self as high in status is unequivocally positive, confirming the sense of the self as meeting up to the cultural standard of the self as independent. It may therefore down-regulate various adverse biological responses, such as inflammation and secretion of stress hormones (Cole et al., 2015).
Second, consider East Asian collectivistic societies. In these societies, the self is construed as interdependent with others in significant social relations and groups, which makes its relational and collective aspects more salient and central. Hence, it stands to reason that people in these cultures are acutely aware of their social obligations and duties. They may also feel pressured to carry out such obligations and duties. Moreover, this may be the case even when social demands exceed their capacity. The extra effort to address and meet the role-based expectations of one’s group may affirm the self’s interdependence with the group (Markus & Kitayama, 1991). Hence, this effort can easily be excessive, making the negative, adverse impact of high SSS more dominant, overwhelming any beneficial effects it may have. That is, the perception of the self as high in status and thus as being responsible for all role-based expectations will confirm the sense of the self as interdependent. However, it can also entail excessive stress, resulting in up-regulation of various adverse biological responses.
Our data proved consistent with this analysis. First, higher SSS was associated with better biological health for American males. The prior evidence suggests that this association is mediated by a sense of control (Cohen et al., 1999), self-esteem (Schnittker, 2004), and optimism (Matthews et al., 2008). Our data are consistent with the hypothesis that high SSS is a resource to draw on in navigating adversities of life (Taylor & Seeman, 1999). Second, higher SSS was associated with compromised biological health for Japanese males. Notably, consistent with the idea that one’s commitment to role-based expectations is responsible for high SSS’s adverse health impact, the association was significantly mediated by lower levels of goal disengagement (a strategy to reduce aspirations to achieve goals, including meeting others’ expectations).
Gender Differences
The finding that the impact of SSS on biological health is limited to males is consistent with prior evidence showing that occupational prestige predicts reduced mortality risk only among males (Wada et al., 2012). Our interpretation of these gender findings holds that because of the stereotypes of females as more caring (Eagly & Karau, 2002), females are less motivated in the domains of power and status (Carré & Olmstead, 2015; Eisenegger et al., 2011). In many cultural contexts, including Japan and the United States, women’s social status may depend on social network quality and familial relationships (Freeman et al., 2016).
Although American and Japanese females were similar in our work, the specific dynamics at play may vary. American females may feel more resentful of the feminine stereotype, especially when it is imposed on them by society (Proudfoot & Kay, 2023). Our findings might indicate that such bitter sentiments may be part of why American women are less interested in their advancement in the power and status domain. We wonder if these resentments of being stereotyped as caring may prove less pervasive among Japanese females because this stereotype is likely to be more positively sanctioned in interdependent cultural contexts, including Japan. Nevertheless, because the care domain is seen as more important, Japanese women may be less interested in the power and status domain.
A Plight of High-Status Japanese Men
Our data suggest that higher social status carries substantial health costs for Japanese men. They appear stuck in an impossible position. Why this might be the case requires careful examination. We assume that Japanese men are expected to perform well at work to make career advancements. Hence, personal achievement and accomplishment may be just as emphasized in Japan as in the United States. However, unlike American males, who can afford to focus primarily on this, Japanese males may have an added burden of managing role-based expectations to manage and harmonize social relations (Miyamoto et al., 2018).
The dual nature of Japanese men’s work may be compounded by the fact that social norms are strong and social institutions are rigid. The effort to change such norms and institutions and promote one’s goals and desires may often fail. Thus, primary control is not viable. However, secondary control, a typical resource prepared for those who face uncontrollable situations (Hall et al., 2010; Thompson et al., 1994), may not be viable either. The reason is that the societal expectations to perform the demanding role-based expectations are also rigid and binding. Hence, high-status Japanese males may not have the luxury of disengaging from these expectations. Future work may build on the evidence that those who disengage from their social expectations may be protected against the health risk of high social status and test the possibility that goal disengagement training could be a promising intervention target to help high-status Japanese males lessen their work burdens.
A Puzzle About Subjective Health
The thesis that SSS’s impact on health depends on culture and gender received strong and consistent support for health biomarkers. Curiously, our measure of subjective health showed no comparable pattern. We wonder if it might be the case that various SSS-related factors, including self-affirmation and role-based expectations (see Figure 3), primarily affect biological pathways. For example, self-affirmation may lessen any threatening experience. Conversely, social burdens imposed by rigid role-based expectations may increase the threat experience (Scholl et al., 2018). In both cases, the threat (or the absence thereof) will likely cause (or silence) an evolutionarily conserved series of epigenetic reactions producing inflammation and other physiological responses against the threat (Cole et al., 2015; Kitayama et al., 2016; Uchida et al., 2018). These reactions may be subtle at any given moment. They may therefore be barely accessible in conscious experience, which could explain why the effects so clear in the relevant biomarkers show no trace in the subjective health measure.
In addition, there may be an important dynamic playing out between subjective health and biological health. For example, we hypothesize that the persistence to keep working to meet social expectations is an important source of compromised biological health for Japanese high-status men. This persistence may well be aided by the subjective assessment of good health. In such circumstances, subjective health may contribute to biological ill-health by exacerbating the excessive persistence in one’s effort to meet role-based social expectations.
Limitations and Future Directions
We wish to acknowledge some limitations of the present work. First, our data are cross-sectional, preventing us from drawing causal claims. Although it is unlikely that BHR leads to varying status, more research is needed to test the causal role of social status in improving or compromising health. Second, our measure of goal disengagement can be better. Future work should use a measure with more items, which could help improve the scale’s reliability (Schmitt, 1996). Third, we hypothesized that the issue high-status Japanese men face might come in part from the burden of being socially responsible, which is added to the demand to perform at high levels in achievement domains. Future work must test the possibility that the conflicting nature of being high-status males in Japan might contribute to their health problems (Boudreaux & Ozer, 2013). Fourth and correspondingly, one might wonder if the pattern we found for Japanese men is limited to work settings—yet another question that should be addressed in future work. Fifth, our work used community social ladder as our SSS measure. This was necessitated by the availability of this measure in the MIDUS/MIDJA dataset. Future work must explore a broader range of SSS measures (Adler et al., 2000). Finally, the MIDJA sample was restricted to Japanese residing in the Tokyo metropolitan area. An extension of this work using a nationally representative sample is needed to test the generalizability of our findings.
Taken together, our findings suggest that the assumption that the higher the better may not always apply to SSS because what it means to be high (or low) in social status depends on specific meanings, expectations, and normative demands that come with it. Our work highlights culture and gender as critical social conditions that determine such meanings and expectations, but future work is necessary to identify other conditions under which high SSS may pose health risks. Previous work suggests that people construe social power differently, either as responsibility or as opportunity, depending on personality traits, such as communal (vs. exchange) relationship orientation (Chen et al., 2001), perspective-taking (Gordon & Chen, 2013; Scholl et al., 2017), and prosocial orientation (Cote et al., 2011). If the meanings of social status also vary as a function of these traits, it stands to reason that the health risk of high SSS might be pronounced among those who construe social status as burden-producing responsibility (rather than as opportunity). This possibility must be tested in future work.
To conclude, the most important contribution of our work lies in the finding that SSS is a double-edged sword. High SSS can be a measure of one’s success in achievement domains. If one’s culture is independent and lets one focus on this aspect of high social status, SSS is likely to predict better health. However, high SSS can also entail various social responsibilities, duties, and obligations, which could be too demanding to maintain good health. If one’s culture is interdependent and lets one focus on this aspect of high social status, SSS is likely to predict worse health. We obtained evidence for these possibilities by testing Japanese and American adults. Altogether, our findings call for a major revision of the accepted wisdom in this literature that SSS is a strong protective factor for health. This conclusion seems applicable only to American males, not to American females. Nor is it applicable to Japanese. The current evidence then strongly calls for a renewed effort to globalize the psychological database and theories based on it.
Supplemental Material
sj-docx-1-psp-10.1177_01461672231162747 – Supplemental material for When High Subjective Social Status Becomes a Burden: A Japan–U.S. Comparison of Biological Health Markers
Supplemental material, sj-docx-1-psp-10.1177_01461672231162747 for When High Subjective Social Status Becomes a Burden: A Japan–U.S. Comparison of Biological Health Markers by Jiyoung Park, Shinobu Kitayama and Yuri Miyamoto in Personality and Social Psychology Bulletin
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institute on Aging (grant no. 5R37AG027343) to conduct a study of Midlife in Japan (MIDJA) for comparative analysis with Midlife in the United States (MIDUS, grant no. P01-AG020166).
Supplemental Material
Supplemental material is available online with this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.