
Abstract
Introduction
To evaluate short-term postoperative intralaryngeal findings and subjective voice outcomes following transcervical chondrolaryngoplasty with endoscopic vocal fold localization.
Methods
A retrospective review was performed of 35 patients undergoing transcervical chondrolaryngoplasty by a single surgeon. Three patients were excluded because of incomplete documentation, leaving 32 patients for analysis. All patients underwent preoperative and 1-week postoperative flexible laryngoscopy and completed the Voice Handicap Index-10 (VHI-10) at both time points. Postoperative endoscopic findings, including anterior commissure integrity, true vocal fold injury, and false vocal fold (FVF) hemorrhage, were recorded and compared with changes in patient-reported voice outcomes.
Results
No patients demonstrated anterior commissure detachment, true vocal fold injury, or visible glottic damage on postoperative endoscopy. FVF hemorrhage was observed in 12 of 32 patients (37.5%). Mean VHI-10 score increased by 0.5 points postoperatively (SE 0.85), which was not statistically significant (p = 0.5), with a median change of 0. No significant association was observed between postoperative FVF hemorrhage and change in VHI-10 score. All hemorrhages resolved spontaneously without intervention.
Conclusion
In this small single-institution series, transcervical chondrolaryngoplasty with endoscopic vocal fold localization was associated with no observed anterior commissure injury and no significant short-term change in patient-reported VHI-10 scores. FVF hemorrhage was relatively common on early postoperative endoscopy but was self-limited and not associated with worsened short-term subjective voice outcomes.
Lay Summary
This study reviewed patients undergoing chondrolaryngoplasty, a surgery to reduce the Adam’s apple, and found that damage to the front of the vocal cords was rare, while minor bleeding in the false vocal folds occurred in about one-third of cases but resolved on its own without affecting voice. Overall, the procedure had no significant impact on patients’ perceived vocal function.
Introduction
Chondrolaryngoplasty, commonly known as tracheal shave or Adam’s apple reduction, is a surgical procedure frequently performed to reduce the prominence of the thyroid cartilage. This procedure is often sought by transgender women as part of their gender-affirming surgical journey, as well as by individuals seeking a less prominent neck profile for aesthetic reasons, promoting self-confidence and psychological well-being in transgender and nonbinary individuals.1,2
Given the proximity of critical laryngeal structures, chondrolaryngoplasty has inherent risks, including the potential for anterior commissure detachment, vocal fold damage, and hemorrhage, and voice change.3-7 Understanding the incidence and management of these complications is crucial for improving patient outcomes and informing surgical practice.5,8 Despite its growing popularity and importance in the realm of gender affirming surgery, comprehensive data on the complications and outcomes associated with chondrolaryngoplasty remain limited. 4
Despite the increasing use of transcervical chondrolaryngoplasty, detailed postoperative observational data regarding intralaryngeal findings and short-term patient-reported voice outcomes remain limited, particularly in patients undergoing routine endoscopic localization of the anterior commissure. Existing literature has largely focused on case reports of severe complications or broad clinician- and patient-reported voice impressions, with little systematic postoperative endoscopic surveillance.5-7,9 In the present study, we sought to characterize early postoperative intralaryngeal findings, including false vocal fold (FVF) hemorrhage and anterior commissure integrity, and to evaluate associated short-term subjective voice outcomes using the Voice Handicap Index-10 (VHI-10).
Methods
This retrospective cohort study was approved by the Institutional Review Board of Mass General Brigham (2021P000027).
Data Collection
A retrospective review was conducted of 35 consecutive patients who underwent transcervical chondrolaryngoplasty at our institution between January 2020 and December 2023. Patients presenting to the Division of Laryngology were identified through billing records using CPT code 31599 (unlisted laryngeal procedure). Cases were manually reviewed to exclude unrelated unlisted procedures, including glottoplasty, advanced airway reconstruction, and oncologic airway procedures. Only patients with complete operative reports and both preoperative and postoperative documentation were included. Demographic variables collected included age, sex assigned at birth, and gender identity.
Voice and Endoscopic Assessment
All patients underwent both preoperative and postoperative flexible laryngoscopic examinations. Postoperative laryngoscopy was performed at the routine 1-week postoperative visit. During this evaluation, the presence or absence of true or false vocal fold hemorrhage, anterior commissure integrity, and any visible vocal fold injury were recorded based on direct endoscopic visualization.
Subjective voice outcomes were assessed using the Voice Handicap Index-10 (VHI-10), a validated patient-reported measure of perceived vocal handicap. VHI-10 scores were obtained at the preoperative visit and repeated at the 1-week postoperative follow-up. Scores range from 0 to 40, with higher values indicating greater perceived vocal handicap.
Statistical Analysis
Descriptive statistics were calculated for demographic, operative, and postoperative outcome variables. Changes in VHI-10 scores from preoperative to postoperative assessment were evaluated descriptively, and associations between postoperative hemorrhage and VHI-10 score change were assessed. Statistical significance was defined as p < 0.05 (Figure 1). Bilateral FVF hemorrhage in 34-year-old patient following chondrolaryngoplasty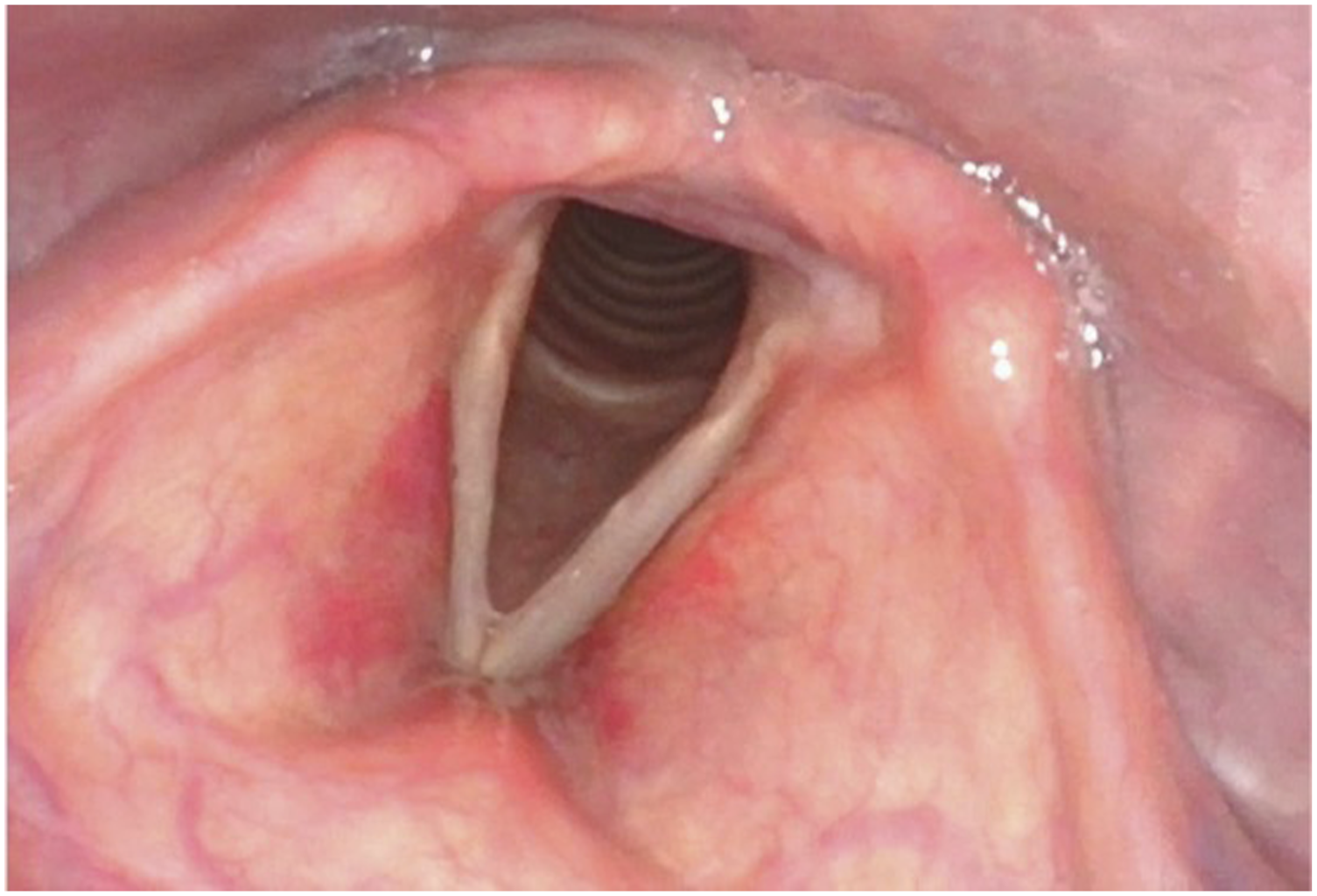
Operative Technique
The patient undergoes general anesthesia, and a laryngeal mask airway (LMA) is placed. A swivel adapter is used to allow access for laryngoscopy through the LMA to evaluate the vocal folds. Laryngoscopy through the LMA is performed before prepping the patient to ensure that visualization will be adequate during the procedure. The thyroid cartilage is exposed and a 22-gauge needle is placed through the cartilage slightly above the midpoint between the inferior border of the cartilage and the inferior aspect of the thyroid notch (Figure 2). This is visualized on the monitor endoscopically. Typically, the needle is seen 1 mm above the true vocal folds; if too high or too low, the needle is replaced externally. This needle position marks the extent of the cartilage resection externally. If the cartilage is too firm or calcified, an 18-gauge needle is used to slowly drill through the cartilage and provide a passage for the 22-gauge needle. Chondrolaryngoplasty incision site and needle placement. This needle position marks the extent of the cartilage resection externally and is essential in assuring the integrity of the anterior commissure
The cartilage to be removed is then marked in a broad arc, extended from the needle insertion point to the postero-superior aspect of the thyroid cartilage. Stabilization is performed with a single thyroid hook and retractor as needed. A blade, rongeur or drill is instead utilized at the surgeon’s discretion. 8 Care is taken not to enter the airway or detach the anterior commissure. The cut edges are then smoothed and beveled, and the perichondrium, straps, and skin are reapproximated. Skin glue and a dressing are applied. 10
Results
Of 35 consecutive patients identified, 3 were excluded because of incomplete documentation, leaving 32 patients for final analysis. The mean age was 31.0 years (SE 1.95), and the mean operative time was 70.6 minutes (SE 2.18).
On routine 1-week postoperative endoscopic examination, no patients demonstrated anterior commissure detachment, true vocal fold injury, or other visible glottic damage. FVF hemorrhage was observed in 12 of 32 patients (37.5%). All hemorrhages were self-limited and resolved without medical or surgical intervention by follow-up.
Mean VHI-10 score increased by 0.5 points from preoperative to postoperative assessment (SE 0.85), which was not statistically significant (p = 0.5). The median VHI-10 change was 0, and score distributions are shown in Figure 3. No significant association was observed between the presence of postoperative FVF hemorrhage and change in VHI-10 score. VHI-10 scores before and after intervention. Individual paired scores are shown with lines. The change was not statistically significant (p ≈ 0.5)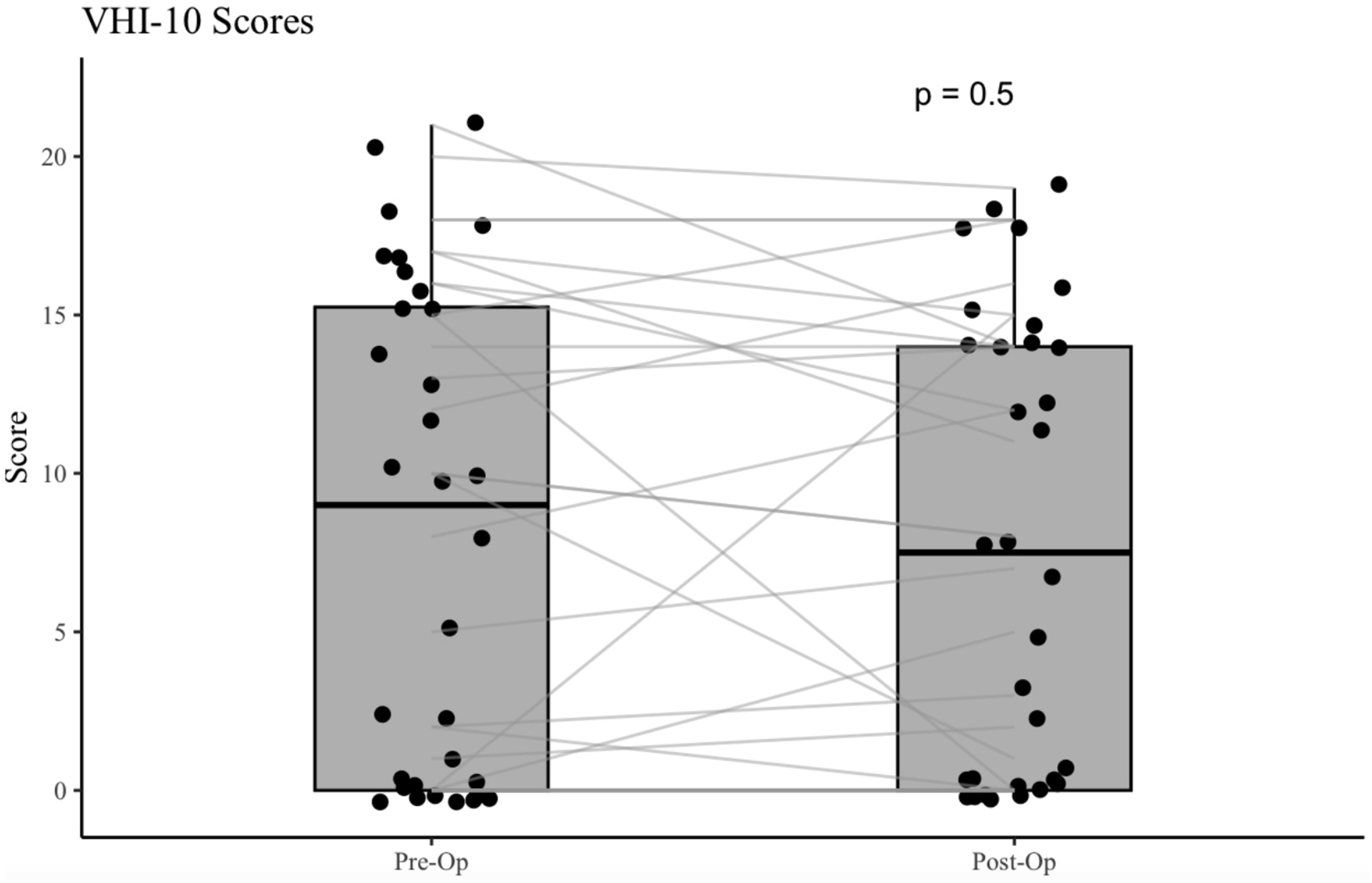
Discussion
In this study, we evaluated complications in patients undergoing chondrolaryngoplasty at our institution, using postoperative endoscopic examinations to identify vocal fold complications. We also assessed whether these findings correlated with changes in patient-reported vocal function, as measured by the VHI-10. 11
Prior reports on chondrolaryngoplasty have described general postoperative issues such as transient hoarseness, odynophagia, and rare airway complications, with most voice changes resolving within weeks.5,7,12 However, detailed observational data on anterior commissure detachment and FVF hemorrhage remain limited. The limited literature that does exist identifies anterior commissure detachment primarily in isolated case reports, where it is regarded as a rare but potentially permanent cause of dysphonia.6,12
In our cohort, no patients were found to have AC detachment. This suggests that, with appropriate surgical technique and postoperative care, the risk of this specific complication can be effectively minimized. 12 This finding is clinically important, as detachment of the AC may alter vocal fold tension, glottic configuration, and long-term phonatory function. 13 Our results align with recent reports suggesting that careful endoscopic visualization and respect for the AC insertion plane can reduce the likelihood of this complication to near zero.7,14
FVF hemorrhage was identified in 37.5% of patients, making it a relatively common early postoperative endoscopic finding in this cohort. Although the literature contains limited discussion of FVF specific hemorrhage after chondrolaryngoplasty, this likely reflects transient submucosal ecchymosis related to manipulation of the thyroid cartilage.6,9,15 Importantly, all cases resolved spontaneously without medical or surgical intervention, supporting the interpretation that this represents a transient intralaryngeal finding in the early postoperative period.
The functional effect of this finding on short-term subjective voice outcomes appeared limited. Mean VHI-10 increased by only 0.5 points postoperatively (SE 0.85), with a median change of 0, and no significant association was observed between FVF hemorrhage and change in VHI-10 score. These findings suggest that self-limited postoperative FVF hemorrhage was not associated with worsened short-term patient-reported vocal handicap in this series.
A major strength of this study is the use of routine postoperative endoscopic evaluation in all patients, allowing direct visualization of anterior commissure integrity, true vocal fold injury, and FVF hemorrhage. This systematic approach minimizes reliance on patient-reported symptoms alone and provides a more accurate estimate of early postoperative intralaryngeal findings. When paired with a validated patient-reported outcome measure such as the VHI-10, this design offers a clinically meaningful assessment of the relationship between endoscopic findings and short-term subjective voice outcomes.
Some limitations should be considered. The study was conducted at a single institution with a limited sample size, which may affect the generalizability of the results. In parallel to this, technique and surgeon-dependent risk factors may be a limiting factor. It should be made abundantly clear that these surgeons at this institution, practicing a particular technique, may not be representative of all surgeons. This data should not be taken as license to falsely reassure patients or to take for granted the importance of precise and careful technique. Follow-up was restricted to the early postoperative period; therefore, long-term data are not typically collected. The sample size may limit the ability to detect subtle or uncommon complications, and the absence of statistically significant differences may reflect limited statistical power. However, patients are instructed to return if they have any further
In this small single-institution case series, transcervical chondrolaryngoplasty performed with careful endoscopic localization was associated with a low observed rate of intralaryngeal injury and no significant short-term change in patient-reported vocal handicap as measured by the VHI-10. FVF hemorrhage was relatively common on early postoperative endoscopy but was self-limited, resolved without intervention, and was not associated with worsened short-term subjective voice outcomes. These findings support the use of careful intraoperative localization and routine postoperative endoscopic surveillance while reinforcing that conclusions remain limited to short-term subjective outcomes. Future studies incorporating objective acoustic measures, stroboscopic evaluation, and longer follow-up are needed to better define the long-term functional significance of these findings.
Conclusion
In this single-institution series, transcervical chondrolaryngoplasty with endoscopic vocal fold localization was associated with no observed anterior commissure injury and no significant short-term change in patient-reported VHI-10 scores. False vocal fold hemorrhage was relatively common on early postoperative endoscopy but was self-limited and not associated with worsened short-term subjective voice outcomes.
Footnotes
Ethical Considerations
This study was reviewed and approved as exempt by the Mass Eye and Ear Institutional Review Board (Protocol #2021P000027; version 6.0).
Consent to Participate
Written informed consent could not be obtained due to the retrospective nature of the study. The requirement for informed consent was waived by the institutional review board. No patients were identifiable in the data or images included in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Disclosures
Dr. Naunheim is a consultant for Kyttaro Limited, Mosanna Therapeutics, and Best-in-Class MD for work unrelated to this paper. No other disclosures.