
Abstract
Objective
Surgical correction continues to be the mainstay of treatment for nasal valve collapse. This narrative review explores the efficacy of nasal myofunctional therapy, including biofeedback training, nasal muscle exercises, and electrostimulation, in treating nasal valve collapse.
Review Methods
A search for abstracts was performed in April 2026 using PubMed, Science Direct, and Cochrane databases using the search terms “nasal muscle”, “nasal valve”, “exercise”, “electromyography”, “electric stimulation”, “collapse”, and “obstruction”. Selection criteria were identified and data was extracted by two independent reviewers from the identified studies.
Results
Biofeedback training with nasal muscle exercises showed some improvement in nasal valve function. Electrostimulation resulted in initial improvement but failed to offer long-term benefits. Nasal muscle exercises as a standalone treatment were not found to provide significant subjective improvement. Notably, the addition of electrostimulation to therapy with biofeedback and muscle exercises did not significantly improve nasal valve obstruction.
Discussion
Preliminary evidence suggests that there is insufficient high-quality data to support nasal muscle strengthening therapies, including biofeedback training, as effective treatments for nasal valve collapse. While uncontrolled studies report subjective and objective improvements, the highest level of evidence did not demonstrate statistically significant benefit. The limited and heterogeneous literature, along with potential publication bias, underscores the need for further well-designed studies to clarify efficacy and long-term outcomes.
Keywords
Introduction
The internal nasal valve region represents the narrowest portion of the nasal passage and plays an indispensable role in regulating airflow dynamics. This anatomic region is the area of greatest overall resistance to airflow within the nasal respiratory system. Bordered by the caudal nasal septum, the upper lateral cartilage, and the inferior turbinate, collapse of this narrow space can be understood through the properties of Bernoulli forces and Poiseuille’s law. Nasal valve collapse is characterized by an inward movement of the nasal lateral wall during inspiration. Current literature estimates that up to 67% of patients presenting with complaints of nasal obstruction have symptoms attributable to nasal valve collapse, emphasizing its clinical relevance in otolaryngologic practices. 1 The mechanism of collapse following many of these causes is weakening of the nasal musculature and a reduction in tissue and cartilage structural integrity. 2
The Superficial Musculoaponeurotic System (SMAS), the underlying muscular layer of the nose, provides a semi-rigid scaffold for the soft tissues of the nose and contributes to the strength of the nasal valve.3-5 EMG based studies have shown activity in the dilator naris, nasalis, and apicis nasi during respiration and voluntary nasal movements, likely signaling the role of these muscles in preventing valve collapse and maintaining patency. Understandably, weakening of any of these muscles (as can occur with facial paralysis) results in a narrowing of the nasal valve and predisposes the nasal valve to collapse.5,6
Contemporary interventions range from minimally invasive techniques, such as the use of dilator strips to surgical procedures involving the use of grafts and suture techniques. While surgical interventions are the most common therapeutic approach to nasal valve collapse, surgery is not without its own set of risks.7,8 Additionally, the steady rise in the costs associated with healthcare and the financial burden of surgical treatments can often be a prohibitive factor in patients seeking correction of nasal valve collapse. 9
Myofunctional therapy has been known to be effective in the treatment of facial paralysis, with studies highlighting the improvement of orofacial muscle balance to the point of normal articulation in patients with facial muscular dysfunctions affecting speech.10-13 Vaiman and team were one of the first to identify improvements in nasal breathing function with the use of surface electromyography (sEMG) in biofeedback training in conjunction with home nasal exercises.6,14,15 To date, however, there continues to be a lack of literature that quantifies the improvement in nasal obstructive symptoms following these non-surgical interventions. This was also noted to be less so with prior validated measures, such as the NOSE score. 16
The objective of this study is to review and synthesize available literature on the efficacy of nasal myofunctional therapy, in the management and treatment of nasal valve collapse. Given the paucity of extensive research in this domain, this review aims to consolidate findings from the limited existing studies, which indicate the potential benefits of nasal valve strengthening exercises in enhancing nasal valve rigidity and increasing nasal muscle tone. By gathering and analyzing the current evidence, this review endeavors to provide clarity on the role of nasal myofunctional therapy as a non-invasive intervention for nasal valve collapse and highlight areas warranting future research.
Methods
The objective of this review was to evaluate whether patients with a history of nasal obstruction due to nasal valve dysfunction (population), through the use of non-invasive management techniques based on nasal muscle strengthening exercises, biofeedback training, and electrostimulation (interventions), were able to obtain clinically significant treatment responses as indicated by either subjective improvement in nasal breathing and/or objective increase in muscle tone on rhinomanometry, acoustic rhinometry, and EMG (outcomes); there was no comparison group as the studies utilizing nasal muscle exercises were primarily observational. This study did not require approval by the Cedars-Sinai Medical Center Institutional Review Board. There are no human participants in this article and informed consent is not required.
Databases and Search Terms
A search for abstracts was performed in April 2026 using PubMed, Science Direct, and Cochrane databases using the search terms “nasal muscle”, “nasal valve”, “exercise”, “electromyography”, “electric stimulation”, “collapse”, and “obstruction” as well as their various derivatives and combinations. For example, searches for “nasal” often also included the word “nose”.
Selection Criteria
The inclusion criteria sought to identify studies that (1) examined the efficacy of nasal myofunctional therapy, particularly through home-based nasal strengthening and toning exercises, for the management of nasal valve collapse; (2) utilized surface electromyography (sEMG) as part of biofeedback training in conjunction with nasal exercises; (3) utilized nasal electrostimulation therapy to activate the muscles of the nasal valve; (4) were randomized controlled trials, observational studies, case series and case studies; (5) were published in peer-reviewed journals; and (6) were published in the English language. Studies were excluded if they: (1) did not specifically investigate nasal valve collapse, nasal muscle strengthening, the measurement of nasal muscle tone, or the influence of muscle tonicity on nasal breathing; (2) were duplicates or had overlapping data; and (3) involved non-human subjects.
Data Extraction and Quality Assessment
Two investigators (JKS and SR) independently performed data extraction from the selected studies identified through PRISMA guidelines (Figure 1). Likewise, the quality of each included article was independently evaluated by the same two investigators. Patient characteristic and demographic data was summated and averaged between studies. Outcomes data was derived from the parent study without further need for additional data analysis. Evaluation for the risk of bias was conducted on a study-to-study basis and any inconsistencies in study bias classification was discussed among the authors until a consensus was reached. Prisma flow diagram
Data Analysis
We conducted a qualitative synthesis of the data extracted from the selected studies. The focus of this analysis was to discern patterns and consistencies relating to the efficacy of nasal myofunctional therapy in the management and treatment of nasal valve collapse. Comparisons were drawn based on the study design, sample size, intervention methods, and outcome measures. Any patterns, trends, or disparities in findings were highlighted, with the intent to provide a comprehensive understanding of the role of nasal myofunctional therapy as a non-invasive treatment option for nasal valve collapse. This approach also aimed to identify gaps in the existing literature, thereby offering directions for future research in otolaryngology-head and neck surgery.
Results
Study Characteristics and Patient Demographics
A total of four studies met the criteria for this review, including two randomized controlled trials and two pilot studies. All studies were published between 2004 and 2022. The average number of subjects included in each study was 36 (range: 15-56). Among all the studies, the weighted average age of subjects was 33.2 ± 6.59 years. Breakdown by gender revealed an average of 64.1% male subjects and 35.9% female subjects in each study. The average length of follow-up among all of the studies was 8.4 months.
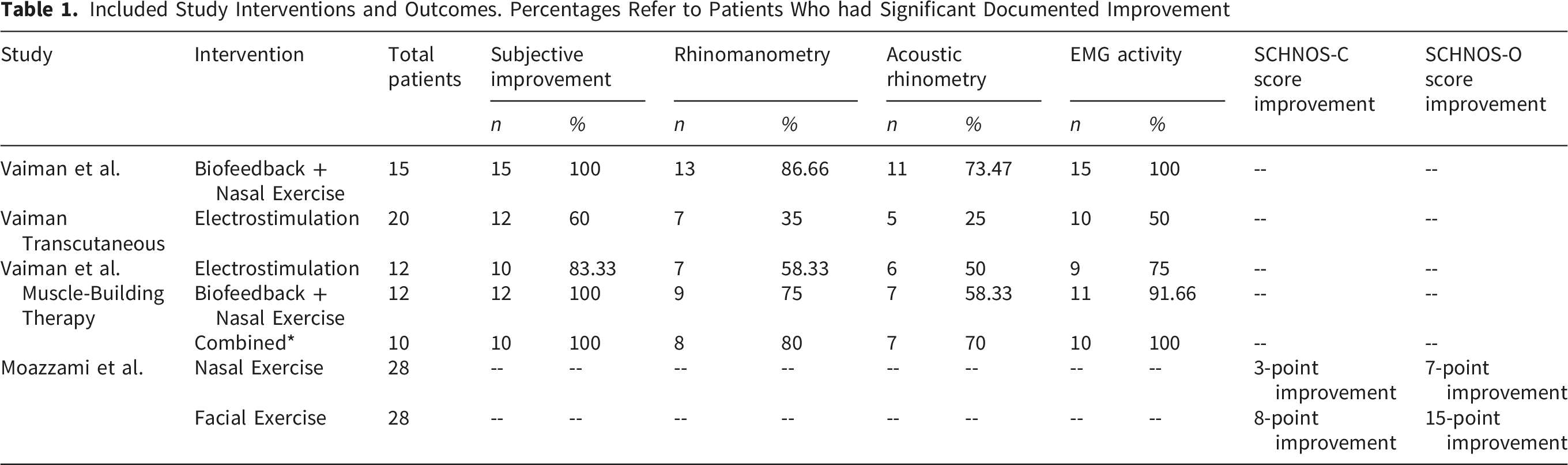
The primary endpoint for all of the studies was an improvement in nasal valve obstruction, and all four studies included some level of subjective measures of improvement. The study by Moazzami et al, used the Standardized Cosmesis and Health Nasal Outcomes Survey (SCHNOS) to measure subjective improvements in nasal valve obstruction. 17 Conversely, the three studies by Vaiman et al reported subjective improvement in nasal obstruction, without the use of a validated patient-reported outcome measure (PROM) or non-validated patient survey data.6,14,15 In addition to patient-reported improvements, Vaiman’s research also assessed objective measures to evaluate improvement in nasal valve obstruction, utilizing methods such as rhinomanometry, acoustic rhinometry, and electromyography (EMG). The initial studies by Vaiman et al, focused on (1) biofeedback training and (2) transcutaneous electrical stimulation as individual treatment modalities for nasal obstruction due to nasal valve collapse before comparing the two modalities with each other as well as a dual-therapy approach. The study by Moazzami et al focused only on nasal muscle exercises as a treatment for nasal valve collapse. Only two studies, Vaiman et al (2004) and Moazzami et al, addressed the possibility of complications or adverse effects, including facial wrinkling.15,17 Neither study reported the development of any adverse effects in any subjects.
Biofeedback and Strengthening Exercises of the Nasal Musculature
The use of biofeedback training of nasal musculature was studied twice by Vaiman et al, and in both situations, 100% of the patients reported subjective improvement (n=27). Both studies also reported objective measures of improvement via rhinomanometry, electromyography (EMG), and nasal endoscopic findings. The combined rhinomanometric results showed that 22 patients (81.4%) exhibited significantly increased bilateral inspiratory nasal flow and 14 patients exhibited a significant decrease in nasal inspiratory resistance (51.8%). In 18 patients (66.7%), acoustic rhinometry of the cross-sectional area of the nasal valve showed a statistically significant increase from an average of 0.49 ± 0.17 cm2 to 0.84 ± 0.26 cm2. Notably, four other patients were found to have some increase in cross-sectional area of the nasal valve, though this was statistically insignificant. 14 Changes in EMG, reflective of strengthening of the nasal musculature, were found to be statistically significant in 26 patients (96.3%). In Vaiman’s study focused only on biofeedback training and home exercise, two patients (7%) were found to have no significant objective findings of improvement even in the setting of subjective reports of improvement. 14
Included Study Interventions and Outcomes. Percentages Refer to Patients Who had Significant Documented Improvement
Electrical Stimulation
Vaiman et al, also explored high-frequency electrostimulation of the nasal muscles as a method of increasing nasal muscle tone across two separate studies involving a total of 32 patients.6,15 Between both studies, 22 patients (68.8%) who underwent electrostimulation therapy reported subjective improvement. Fourteen patients (43.8%) showed a significant increase in bilateral inspiratory nasal flow while 12 patients (37.5%) showed a significant decrease in inspiratory nasal resistance. Acoustic rhinometry revealed a significant increase in nasal valve cross-sectional area in 11 patients (34.4%) from 0.48 ± 0.19 cm2. EMG activity showed a statistically significant increase of muscle tension in 19 patients (59%). When using electrical stimulation alone and not in conjunction with biofeedback training and nasal strengthening exercises, 12 patients (60%) were found to have no significant objective improvement based on evaluation via rhinomanometry, acoustic rhinometry, and EMG. These patients were recommended to receive endonasal surgery.
Follow up using rhinomanometry and EMG showed decline in results within one month of treatment discontinuation. By 3-4 months after completion of treatment, EMG and rhinomanometry showed return to baseline pre-treatment values. 15
Dual Therapy
One study by Vaiman et al, explored the differences in efficacy between biofeedback-based muscle exercises, electrostimulation, and incorporation of both modalities. 6 This study found that 100% of subjects (n=10) reported a subjective improvement in their symptoms. On rhinomanometry, eight patients (80%) were found to have a statistically significant increase in bilateral inspiratory nasal flow, while seven patients (70%) were found to have a statistically significant decrease in nasal inspiratory resistance. Acoustic rhinometry showed an increase in cross-sectional area of the nasal cavity in seven patients (70%). EMG showed a statistically significant increase in tension of the nasal musculature in all 10 patients (100%), indicative of a global increase in the strength of the nasal musculature. Dual therapy was found to be significantly more effective than electrostimulation alone. However, no statistically significant difference was identified between sole therapy with nasal muscular exercises and dual therapy.
Discussion
The primary aim of this review was to evaluate the impact that strengthening of the nasal musculature can have on the management and treatment of nasal valve collapse. Drawing from a limited body of literature, the study seeks to clarify the potential utility of this non-invasive treatment approach in enhancing nasal valve rigidity and muscle tone, while also identifying gaps in current research within the field of otolaryngology-head and neck surgery. Bruintjes and Kienstra et al demonstrated that increased contraction force and tone of certain nasal muscles can increase structural rigidity of the internal and external nasal valve, thereby improving nasal valve patency and ultimately optimizing nasal airflow and reducing the likelihood of collapse during inspiration.5,18 To date, studies evaluating methods for strengthening of these muscles have been focused on electrostimulation therapy and myofunctional exercise therapy, often in conjunction with biofeedback.6,14,15,17
Comparing myofunctional therapy through home-based nasal muscle exercises with electrostimulation therapy and biofeedback-based therapy allows a critical look at the similarities and discrepancies of each method in regard to the efficiency, efficacy, and practicality as a treatment model for nasal valve collapse. Importantly, the highest level of evidence identified in this review - the randomized controlled trial by Moazzami et al - demonstrated an overall improvement in SCHNOS-O scores following nasal muscle exercises; however, this change did not reach statistical significance. 17 This finding suggests that, based on the most methodologically robust data currently available, there is insufficient evidence to support a definitive clinical benefit of isolated nasal muscle strengthening. In contrast, studies by Vaiman et al reported significant improvements in both subjective and objective measures following biofeedback training and home-based nasal exercise programs.6,14 However, these findings are derived from uncontrolled study designs with limited quantitative outcome reporting, and therefore should be interpreted cautiously within the context of a lower evidentiary hierarchy. While these results may suggest a potential signal toward benefit, they do not provide definitive support for efficacy.
Electrostimulation therapy has also been explored as a modality for nasal muscle strengthening. While it showed initial short-term improvement, electrostimulation therapy failed to provide durable long-term benefits after discontinuation of treatment, with patients returning to their pre-treatment baseline within four months. 15 Even when used in conjunction with biofeedback training, electrostimulation did not contribute significantly to improvement of nasal valve collapse. 6
In addition to the paucity of existing studies, differences in methodology placed additional limitations on our study. A notable difference in methodology lies in the treatment modalities employed. While Vaiman et al focused on nasal muscle exercises as an adjunct to biofeedback therapy, Moazzami et al focused only on nasal muscle exercises.6,14,17 This difference makes it difficult to understand the efficacy of nasal muscle exercises alone versus the synergistic effect of both biofeedback and exercises, and raises the question of how the observed improvement or lack thereof can be attributed to biofeedback. This opens the door for further research on the efficacy of biofeedback versus muscle-strengthening exercises as standalone therapies versus the combined impact between the two.
Another consideration rests in methodology of measuring subjective improvements of symptoms. Vaiman employs an “all-or-none” approach to subjective improvement in symptoms, which does not characterize the nuanced changes in a patient’s condition. Moazzami et al used the SCHNOS-O scale, a validated patient-reported measure of outcomes, which assesses multiple elements of the symptomatic burden associated with nasal obstruction.17,19 This more detailed assessment of patient experiences provides a more comprehensive evaluation of treatment impact. While Vaiman et al reported high rates of subjective improvement, this data was not reported quantitatively. The use of a validated, multidimensional measure in Moazzami’s study allows for a more reliable and nuanced understanding of the true effect of these therapies. Limitations were also present within individual studies. For example, Moazzami et al found that 31 participants (55.4%) had imperfect adherence to the prescribed exercise regimen. Though no significant difference in compliance was found between the control and experimental groups, this further highlights the need for studies using larger, more controlled sample populations.
Beyond study-level limitations, there are additional considerations relevant to this review. The absence of prospective PROSPERO registration represents a methodological limitation, as it may introduce potential bias in study selection or reporting. Additionally, the near-complete paucity of literature in this area over the past two decades raises the possibility of publication bias. This lack of published data may reflect the presence of negative or inconclusive findings that remain unpublished, or alternatively, a relative lack of research interest given the niche nature of these therapies compared to more widely studied surgical interventions for nasal valve collapse. These factors further limit the ability to draw robust conclusions and underscore the preliminary nature of the current evidence base.
The most notable gap in the existing literature is the dearth of long-term evaluation of myofunctional therapy for treatment of nasal valve collapse. Future studies should focus on longitudinal follow-up of patients to assess for symptom relapse, treatment complications, or the development of adverse effects. Additional studies should also be directed toward the evaluation of the comparative efficacy of biofeedback therapy, nasal muscle exercises, and a combination of the two. There is currently insufficient evidence to stratify the individual and synergistic impacts of these treatment modalities on nasal valve collapse. By better understanding the contribution of each modality, otolaryngologists may be better equipped to evaluate their potential role, although at present these approaches should be considered investigational given the limited and inconclusive evidence available.
Conclusion
This review highlights the limited and preliminary nature of the current evidence evaluating nasal muscle strengthening therapies for nasal valve collapse. While lower-level studies suggest potential symptomatic improvement, the most robust available evidence did not demonstrate a statistically significant benefit. As such, the existing data are insufficient to support the routine use of these therapies as a reliable treatment option. Nasal myofunctional therapies may warrant further investigation as a non-invasive approach; however, their clinical role remains undefined. Future high-quality studies with standardized methodologies and long-term follow-up are necessary to determine whether these interventions provide meaningful and durable benefit. Until such data are available, these therapies should be considered investigational, and conclusions regarding their efficacy should remain appropriately cautious.
Footnotes
Author Contributions
Jordan Kai Simmons: Manuscript writing, editing, and review; Sai Reddy: Manuscript writing, editing, and review; Wasiq Nadeem: Manuscript editing and review; Kaitlynne Pak: Manuscript editing and review, Henry Chen: Supervision, Manuscript editing and review; Matthew Lee: Supervision, Manuscript editing and review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.