
Abstract
The triticeal cartilage is a small cartilage found within the thyrohyoid membrane present in approximately 33%-53% of individuals. Rarely, calcification/ossification of this cartilage can occur, leading to symptoms of dysphagia, odynophagia, or globus sensation. Despite its clinical relevance, symptomatic triticeal cartilage calcification remains poorly characterized in the literature, with only isolated case reports and no established diagnostic or management framework. We present a case of a 44-year-old woman who presented with seven months of atypical throat and neck pain and globus sensation in the setting of prior esophagogastroduodenoscopy with dilation. Medical management, including nortriptyline and hyoscyamine provided no benefit. Physical examination and flexible laryngoscopy were unremarkable, except for focal left-sided neck tenderness. Contrast-enhanced computed tomography of the neck demonstrated a nonspecific 0.3 x 0.3 x 1.0 cm submucosal calcification at the thyrohyoid membrane, suspicious for retained foreign body. The patient underwent left neck exploration which revealed a calcified cartilaginous structure embedded within the pharyngeal constrictors and immediately adjacent to a pharyngeal plexus branch. Final pathology confirmed fibrous tissue and cartilage. The patient reported immediate, complete symptom resolution and remained symptom-free at 13-month follow-up. This case highlights calcified triticeal cartilage as a rare, often overlooked cause of persistent throat symptoms. Recognition of this pathology may prevent misdiagnosis and allow for timely, definitive treatment.
Keywords
Introduction
The triticeal cartilage is a small cartilaginous structure that sits in the lateral thyrohyoid membrane and is considered a normal component of the laryngeal skeleton. 1 Typically subcentimeter in size, it is present in 33-53% of individuals and may undergo progressive ossification or calcification.1-3 While often an incidental and asymptomatic anatomic variant, ossification or calcification of the triticeal cartilage may rarely become clinically significant, producing symptoms such as globus sensation, dysphagia, or odynophagia.2,4,5
Despite its potential to cause clinically significant symptoms, symptomatic calcification of the triticeal cartilage remains poorly characterized in the literature. Existing reports are limited to isolated case descriptions, with little emphasis on the clinical features that distinguish this pathology from more concerning causes of throat or neck pain. Consequently, calcified triticeal cartilage may be misinterpreted on imaging, leading to unnecessary diagnostic workup, patient anxiety, or delayed recognition of a benign but symptomatic condition.2,6 Furthermore, there is no clear consensus regarding the evaluation or management of patients in whom this anatomic variant becomes symptomatic.
We present a case of symptomatic calcified triticeal cartilage presenting with odynophagia and neck pain. We highlight the clinical presentation, radiographic features, and diagnostic considerations that can aid clinicians in recognizing this rare but important entity and distinguishing it from more serious cervical pathology.
Case Presentation
A 44-year-old female presented to the otolaryngology-head and neck surgery clinic with a seven-month history of globus sensation and atypical left-sided throat and neck pain. Her symptoms were first noted following esophagogastroduodenoscopy (EGD) with esophageal dilation for a distal esophageal stricture. A repeat EGD was grossly normal, and medical management with acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs), nortriptyline and hyoscyamine provided minimal to no symptomatic relief. In-office physical examination including flexible fiberoptic laryngoscopy was grossly normal except for focal left-sided neck tenderness to palpation.
Contrast-enhanced computed tomography (CT) of the neck (Figure 1A-B) demonstrated a 0.3 x 0.3 x 1.0 cm submucosal calcification at the junction of the left inferior oropharynx and superior hypopharynx, raising concern for a retained foreign body. Subsequent magnetic resonance imaging (MRI) with and without contrast revealed a 1.0 cm elongated hyperdense submucosal structure within the left piriform sinus, distinct and non-contiguous with adjacent laryngeal cartilages. Targeted ultrasound (Figure 1C) confirmed a corresponding echogenic linear structure deep and medial to the carotid bifurcation. A videofluoroscopic swallow study was unrevealing. Differential diagnoses included a retained submucosal foreign body versus calcified ligament. (A-C) Multimodal neck imaging demonstrating a calcified lesion within the left thyrohyoid membrane consistent with a calcified triticeal cartilage. (A) Contrast-enhanced computed tomography (CT), coronal view, demonstrating a submucosal calcification (arrow) at the junction of the left inferior oropharynx and superior hypopharynx. (B) Contrast-enhanced CT, sagittal view, showing the elongated calcified structure (arrow) within the left thyrohyoid membrane. (C) Ultrasound of the neck demonstrating a linear echogenic structure (arrow) located deep and medial to the carotid bifurcation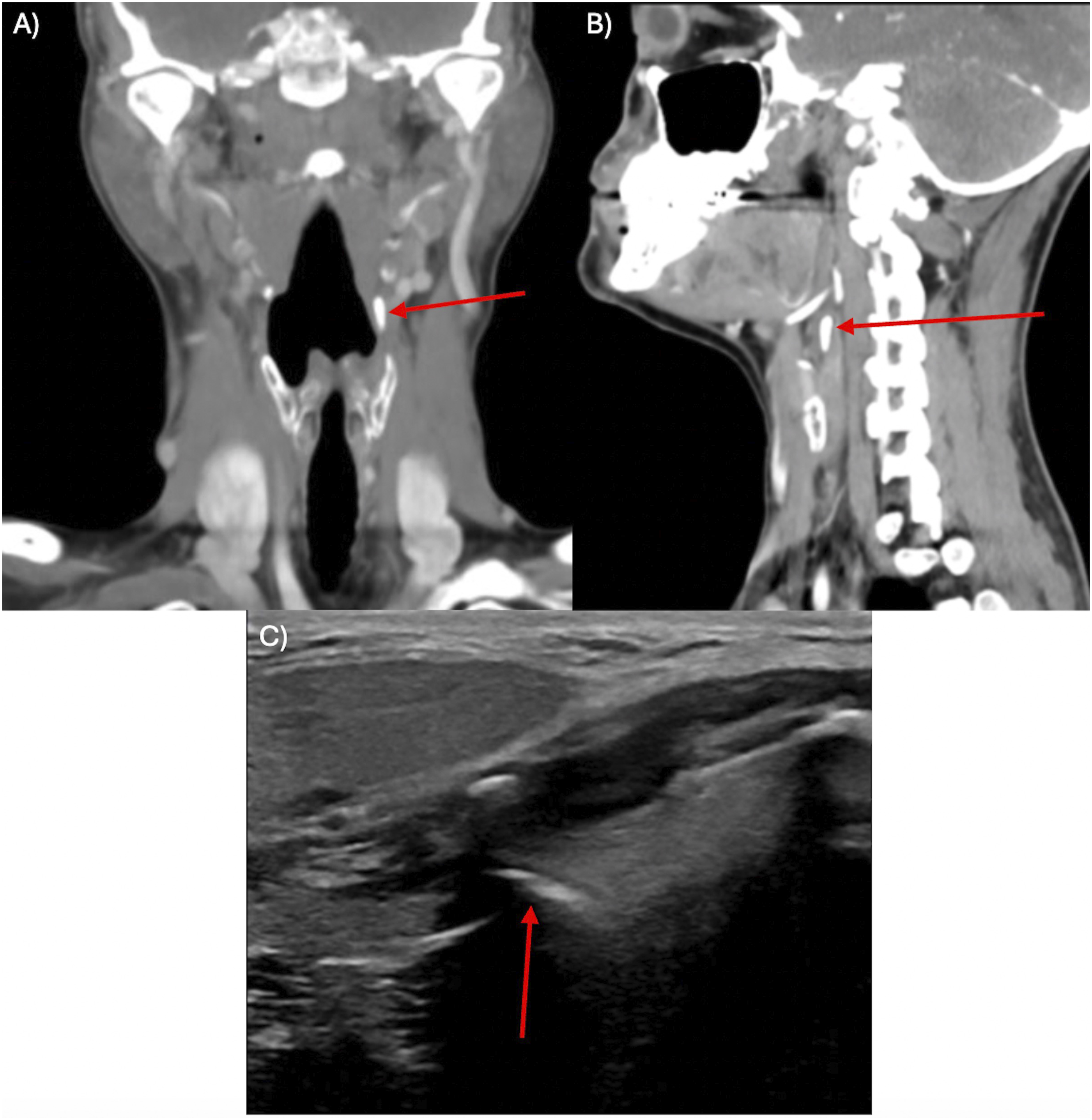
One week after initial clinic evaluation, the patient presented to the emergency department with worsening throat pain, difficulty speaking, and markedly decreased oral intake. Given persistent, worsening symptoms despite extensive gastroenterologic evaluation and inconclusive imaging findings, she was admitted and taken for operative intervention. Direct laryngoscopy demonstrated mild edema of the left piriform sinus without mucosal lesions. On bimanual palpation, a firm lesion was appreciated between the hyoid bone and thyroid cartilage. Left neck exploration revealed a white, calcified cartilaginous structure embedded within and partially surrounded by pharyngeal constrictor musculature, immediately adjacent to a branch of the pharyngeal plexus which was carefully dissected free and preserved. The lesion was excised entirely, measuring approximately 1.0 cm (Figure 2). No pharyngotomy was made. The patient tolerated the procedure without complication. Gross pathology revealed fragmented pink-tan soft tissue admixed with calcifications measuring 0.7 x 0.5 x 0.3 cm. Histopathologic analysis displayed fragments of fibrous tissue and calcified cartilage, confirming a diagnosis of calcified triticeal cartilage. At a two-week follow-up, the patient reported completed resolution of odynophagia and globus sensation. After 13 months, the patient remained symptom free. Gross photograph of the resected lesion demonstrating pink-tan soft tissue admixed with calcifications, consistent with calcified triticeal cartilage
Discussion
The triticeal cartilage is a small ovoid structure composed of hyaline cartilage embedded within the lateral thyrohyoid membrane and exhibits considerable morphologic variability.1,3,7 It may undergo progressive ossification or calcification with age, although the specific mechanisms driving this process remain poorly understood. Understanding from broader cartilage physiology suggests that calcification is an active, regulated process involving chondrocyte-mediated mineralization and inflammatory signaling. 8 Calcification of the triticeal cartilage is suspected to be chronic. However, local inflammation or biomechanical changes, such as those potentially associated with esophageal instrumentation as in this case, may exacerbate or unmask symptoms in patients with previously asymptomatic cartilage. It should be noted that this temporal association does not establish causality, and the relationship between instrumentation and symptom onset remains speculative. Given its location within the elastic thyrohyoid membrane, which facilitates laryngeal elevation toward the hyoid bone during swallowing, calcification or associated inflammation may impair normal laryngeal mobility and provoke symptoms such as dysphagia, odynophagia, and globus sensation. 9 These effects may be further amplified by the cartilage’s proximity to the pharyngeal wall and adjacent neurovascular structures, including the internal branch of the superior laryngeal nerve.2,6,9 While symptomatic triticeal cartilage has not been commonly linked to direct neck trauma, prior literature highlights its clinical relevance in the setting of anterior neck surgery. 10 The internal laryngeal nerve has been shown to cross directly over the triticeal cartilage, creating a potential site for iatrogenic injury. 10 In this context, mechanical irritation, localized inflammation, or transient nerve compression, may represent plausible mechanisms by which manipulation or instrumentation could precipitate symptoms in patients with pre-existing calcified cartilage. Our case underscores the clinical relevance of this anatomy, as progressive symptoms ultimately necessitated operative intervention.
Calcified triticeal cartilage is a recognized diagnostic mimic and may be mistaken for a retained foreign body, carotid artery calcification, or superior thyroid horn fracture.1,4-7 Radiographic findings may appear concerning, while endoscopic examination and swallow studies remain normal, as observed in this case. Prior reports describe successful symptom management with conservative therapy in select patients. 6 However, our patient failed medical treatment and experienced worsening functional impairment, necessitating surgical excision. This case highlights a stepwise diagnostic dilemma, emphasizing the importance of including calcified triticeal cartilage in the differential diagnosis of submucosal hypopharyngeal calcifications, particularly in the context of ambiguous imaging findings.
Prior literature describing symptomatic calcified triticeal cartilage is limited to isolated case reports, with management strategies ranging from conservative therapy to surgical excision. Alsarraf et al reported a 54-year-old man with progressive dysphagia in whom imaging suggested a retained foreign body; surgical exploration revealed a calcified triticeal cartilage embedded within the thyrohyoid membrane, and surgical excision resulted in full symptom resolution similar to our case. 4 Conversely, conservative management has also been described. In one report, a 78-year-old man with unilateral throat discomfort and odynophagia due to an ossified triticeal cartilage compressing the posterior pharyngeal wall experienced complete symptom resolution following a 12-week course of NSAIDs. 6 These reports suggest that while a trial of anti-inflammatory therapy may be reasonable in mild cases, surgical excision should be considered when symptoms are severe, persistent, or when imaging raises concern for alternative diagnoses. Our case adds to this limited body of literature by demonstrating complete and sustained symptom resolution following surgical excision after failure of medical management, reinforcing excision as an option in patients with refractory or debilitating symptoms.
Across the limited reported cases of symptomatic triticeal cartilage calcification, several common features emerge. Patients typically present with unilateral throat symptoms with imaging findings that are ambiguous or raise concern for alternative diagnoses, and endoscopic exam is consistently unremarkable.1,4-6 Management has been dictated by symptom severity, with conservative NSAID therapy effective in mild cases and surgical excision for severe cases, with complete postoperative symptom resolution.4,6 Anatomically, the cartilage is typically located in the middle to lower third of the thyrohyoid membrane at the C4 vertebral level, placing it in close proximity to the pharyngeal wall and internal branch of the internal branch of the superior laryngeal nerve, which has been shown to cross directly over the cartilage in 59% of cases.1,7,10 This relationship offers a plausible mechanism for symptom generation through either mucosal compression or nerve irritation. Despite a high population prevalence of triticeal cartilage ossification, symptomatic presentations are exceedingly rare, suggesting that factors such as cartilage size, degree of ossification, or precipitating events trigger clinically significant symptoms in this otherwise incidental finding. 3
This report is limited as a single-patient observation, which limits generalizability of symptom presentation, imaging characteristics, and management strategies. Nonetheless, the rarity of symptomatic triticeal cartilage supports case-based reporting, with surgical pathology providing a diagnostic conclusion. Complete postoperative symptom resolution further supports a causal inference between the lesion and the patient’s clinical presentation.
For patients, increased awareness of calcified triticeal cartilage as a potential diagnosis may reduce anxiety and prevent unnecessary diagnostic testing. For clinicians, recognition of this rare pathology may support earlier diagnosis and reduce care delays. Albeit rare, calcified triticeal cartilage should be considered in patients with persistent globus or odynophagia, particularly when imaging reveals submucosal hypopharyngeal calcifications. When symptoms persist despite conservative management and diagnostic uncertainty remains, surgical exploration may be both diagnostic and therapeutic. This case supports consideration of calcified triticeal cartilage as a rare but treatable cause of persistent throat symptoms.
Conclusion
Calcified triticeal cartilage, though typically an incidental anatomic variant, can represent a rare but clinically significant cause of persistent globus sensation, dysphagia, and odynophagia, which may be associated with prior esophageal or neck instrumentation, although a causal relationship has not been established. Radiographic findings may be misleading and mimic more concerning pathology. In patients with persistent symptoms despite conservative management and equivocal diagnostic workup, surgical exploration may be both diagnostic and therapeutic.
Footnotes
Ethical Considerations
Ethical approval was not required to report this case in accordance with Vanderbilt University Medical Center institutional policy, as this manuscript describes a single patient case report without research intervention.
Consent to Participate
Written informed consent to participate was obtained retrospectively from the patient prior to submission of the manuscript. Formal Institutional Review Board approval was not required given the nature of this study as a single case report, in accordance with institutional policy. Written informed consent was obtained retrospectively from the patient for participation in this report and for publication of clinical details and images. The patient was informed that the report would be published in an open-access format and that all identifying information would be removed or anonymized.
Consent for Publication
Written informed consent for publication of this case report and any accompanying images was obtained from the patient. A copy of the written consent is held by the authors and is available for review by the journal upon request. All potentially identifying information has been removed or anonymized to protect patient confidentiality.
Author Contributions
Andreja Radevic, BS: Conceptualization (equal), Data curation (lead), Investigation (lead), Validation (equal), Writing – original draft (lead), Writing – review & editing (lead), Formal analysis (equal); Joaquin Austerlitz, BS: Conceptualization (equal), Data curation (equal), Investigation (equal), Methodology (equal), Validation (equal), Writing – original draft (equal), Writing – review & editing (equal), Formal analysis (equal); Michael C. Topf, MD, MSCI: Investigation (equal), Supervision (lead), Validation (equal), Writing – original draft (equal), Writing – review & editing (equal).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available due to privacy restrictions but can be obtained from the corresponding author upon reasonable request.