
Abstract
Background and Objectives
Hearing impairment (HI) is one of the most common disabilities in older adults. This cross-sectional study examined the descriptive epidemiology of HI in 15,179 older adults in the 2016-2018 wave of the Health and Retirement Study.
Research Design and Methods
Hearing was assessed at two pitches (1000, 3000 Hz) and 3 loudness levels (35, 55, 75 dB HL). HI was defined as hearing <50% of tones in one or both ears. Demographics (age, race, ethnicity, sex, education), noisy occupation, smoking status, and medical comorbidities (diabetes, CVD, hypertension, cancer, stroke, dementia) were assessed via survey. Associations between HI and these factors were evaluated using Poisson regression.
Results
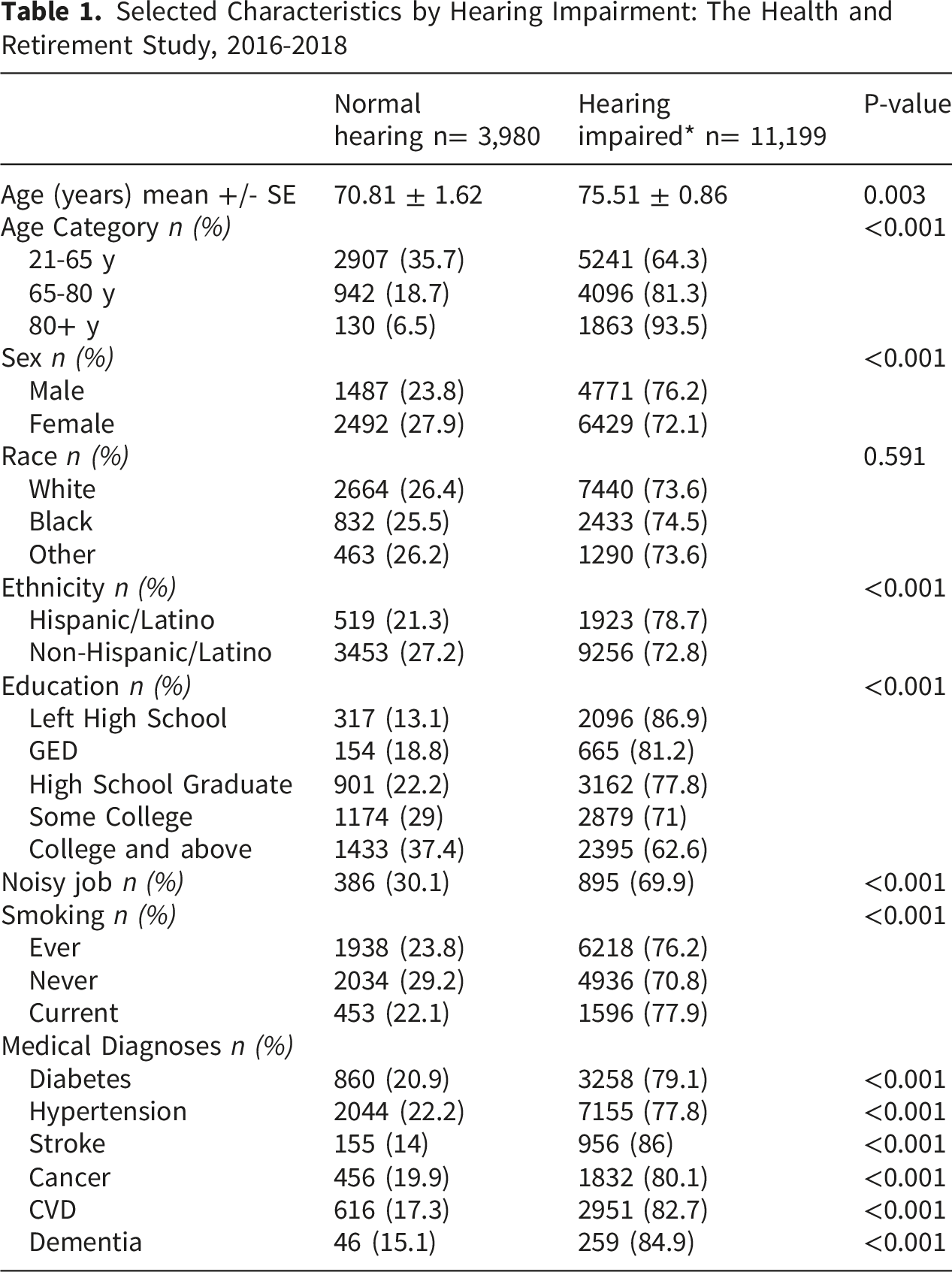
HI was highly prevalent (74% overall), and varied by sex (76.2% men, 72.1% women), ethnicity (78.7% Hispanic, 72.8% non-Hispanic) and age (21-65 years-old 64.3%, 65-80 years-old 81.3%, 80+ years-old 93.5%). After multivariable adjustment, HI was less common in women compared to men (IRR: 0.92; CI: 0.87-0.98) and was more common in those with Hispanic/Latino ethnicity compared to White (IRR:1.13, CI: 1.03-1.23). HI was more common in those with less than a college degree (less than high school: IRR = 1.47, CI = 1.34-1.61; high school graduate: IRR = 1.24, CI = 1.13-1.35; some college: IRR = 1.15, CI = 1.06-1.24). Compared to non-smokers, current smokers had higher risk of HI (IRR = 1.19, CI = 1.11-1.28). Lastly, history of stroke was associated with a greater risk of HI (IRR = 1.06, CI = 1.02-1.11).
Discussion and Implications
HI is highly prevalent in the HRS sample and is correlated with chronic diseases and demographic factors. This study underscores the need for regular hearing screening and intervention among older US adults.
Introduction
Hearing impairment (HI) affects nearly thirty-two million Americans and is the second most common disabling condition (after arthritis). 1 HI prevalence increases with age, affecting 45% of adults in the sixth decade, and increasing to 89% of those in the eighth decade.2,3 Recent estimates suggest approximately thirty-five to forty million older adults will have hearing loss by 2030.4-10 Hearing loss in older adults has been associated with social isolation, 4 loneliness 11 depression and cognitive decline.4,6-8
Previous population-based studies have found that HI is more prevalent in men than women,5,12-14 more common in White participants than other race-ethnic groups,7,11 and more common among those with less education.9,12,13 This investigation also seeks to support existing literature showing associations between hearing loss and age,14-17 gender,5,13,14,16,18 race,13,19 education,14,20,21 smoking,14,22 cardiovascular disease13,22,23 and diabetes.13,17,23
The purpose of this study was to characterize the prevalence and correlates of hearing impairment in the longitudinal, biennial, nationally representative Health and Retirement Study (HRS), the largest and most comprehensive nationally representative multi-disciplinary panel study of Americans over the age of 50. 24 HRS survey content is comprehensive, covering questions about health, utilization of health services, labor force, economic status, family structure, expectations, and end-of-life.
While previous studies have used HRS data to examine relationships between hearing sensitivity and cognition, 25 loneliness and social isolation, 26 and the end of life, 27 to our knowledge, no paper has explicitly evaluated instrumentally measured hearing sensitivity in this large, uniquely older cohort of older Americans in terms of demographics, medical comorbidities, occupational status and smoking. This analysis evaluates a large recent cohort of uniquely older U.S. adults with objective instrumental measures which has yet to be done, in addition to investigation of known associations of HI in one large cohort to support existing literature.
Methods
Sample
Data for this study came from the Health and Retirement Survey (HRS), a study of United States adults aged 50 and older which has been ongoing since 1990.24,28 The cohort is surveyed biennially. A rotating 50% of participants undergo face-to-face interviews with physical and biological measures and a mail-back psychosocial questionnaire, while the other half of the sample receives telephone follow-up surveys only. The survey is conducted in either English or Spanish based on participant preference. Data for the current study came from the 2016-2018 wave of the study, when instrumental measurement of hearing sensitivity took place. 24 In survey years 2016 through 2018, there was a 74% response rate. Of the 15,499 participants surveyed in 2016-2018, 15,179 had hearing data and were included in the study. Every six years a new six-year birth cohort is introduced, with over 43,000 respondents interviewed since the HRS’s inception. In any given wave, there are about 20,000 respondents. In the 2016 – 2018 wave of the study, the sample was 50.2% male, 49.8% female; 83.2% Caucasian, 12.9% Black/African American, 3.9% Other Race, with 9% identifying as Hispanic. The mean age of the sample in 2016 was 65.7 years (SD 11.8 years) and in 2018, 67.0 years (SD 11.4 years).
Assessment of HI
Hearing sensitivity (without hearing aids) was assessed in both ears with the Siemens HearCheck™ screening device. Siemens HearCheck™ has been validated against the gold standard of air conduction pure tone air averages for moderate or worse hearing loss (PTA≥41 dB HL), showing a sensitivity of 85.7% and specificity of 92.4%. 29 Participants were asked if they wear a hearing aid in one or both ears, and if they would be willing to remove the hearing aid(s) for the purpose of the test. Hearing assessments were conducted in person during home visits by trained HRS staff. Hearing sensitivity was evaluated at two frequencies important for speech comprehension (1000 Hz and 3000 Hz) and three loudness levels (35, 55, and 75 dB HL). Number of tones heard per ear was recorded. Hearing impairment was defined as hearing fewer than three tones in the best ear, the screening threshold associated with moderate or severe hearing impairment. The WHO guidelines currently define adults with hearing impairment above a 40 dB hearing level in the better ear. 30 This definition was chosen to identify potentially disabling hearing loss. In addition to the instrumental hearing screening, respondents were asked “Is your hearing excellent, very good, good, fair, or poor?”.
Assessment of Potential Correlates of HI
Demographic factors were measured via survey. Age was calculated as the age at study baseline plus the difference in years between age at baseline and 2017. Race (White, Black, other), sex (male or female), and education (left high school, GED, high school graduate, some college, college and above) were measured at the baseline visit. Smoking (ever smoked, never smoked, current smokers) was assessed in the same visit as the hearing assessment, as were prevalent medical comorbidities (hypertension, heart disease, diabetes, stroke and cancer), which were identified based on self-report of diagnosed conditions by a medical professional.
Statistical Methods
Characteristics of the population were summarized using means with standard deviations for continuous variables and frequencies (weighted percentages) for categorical variables. Unadjusted associations between HI and correlates of interest were assessed with t-tests and chi-square tests. Age- and multivariable-adjusted odds of hearing impairment associated with correlates of interest were calculated using Poisson regression models. The multivariable-adjusted model included age, sex, race, medical comorbidities (diabetes, hypertension, stroke, cancer, cardiovascular disease, and dementia), smoking, and history of a noisy job. All analyses were performed using complex survey analysis approach with standard error computed using Taylor’s series linearization and employed HRS sample weighting for generalization to the US older adult population. Results of the regression models are reported as incidence rate ratios (IRRs) with 95% confidence intervals (CIs). STATA 18 SE was used for all analyses, and results with p-value < 0.05 were considered significant. The reporting guidelines used in the analysis were the Preferred Reporting Items for Complex Survey Analysis (PRICSSA). 31
Results
Selected Characteristics by Hearing Impairment: The Health and Retirement Study, 2016-2018
After multivariable adjustment, compared to those aged 50-65 years, those aged 65-80 years were 35% more likely to have HI (IRR =1.35; CI =1.28-1.43), and those 80 years and older had 70% higher likelihood (IRR =1.70; CI =1.56-1.86). Women were 9% less likely than men to have HI after age-adjustment (IRR =0.91; CI =0.86-0.97) and 8% less likely after multivariable adjustment (IRR =0.92; CI =0.87-0.98). Compared to White participants, those who identified as “other” race were 7% more likely to have HI after age-adjustment (IRR =1.07; CI =1.03-1.14), and 9% more likely to have HI after multivariable adjustment (IRR=1.09; CI =1.01-1.17). No significant differences were seen between White and Black participants. Compared to those without Hispanic ethnicity, those with Hispanic ethnicity were 12% more likely to have HI after age-adjustment (IRR =1.12; CI =1.03, 1.23) and 13% more likely to have HI after multivariable adjustment (IRR =1.13; CI =1.03, 1.23). After multivariable adjustment, compared to college graduates, HI was 14% more likely among those with some college (IRR =1.14; CI =1.10, 1.19), 23% more likely among high school graduates (IRR =1.23; CI =1.18-1.28), 32% more likely among those with a GED (CI =1.24-1.41), and 37% more likely among those who left high school (IRR =1.37; CI =1.31-1.42). Surprisingly, in both age- and multivariable-adjusted models, there was no difference in the likelihood of HI by history of noisy occupation. Current smokers were 13% more likely to have HI after age-adjustment (IRR =1.13; CI =1.06, 1.21) and 17% more likely to have HI after multivariable adjustment (IRR =1.17; CI=1.09, 1.25). Stroke was associated with a 20% higher likelihood of HI after age adjustment (IRR =1.20; CI =1.10, 1.30) and a 19% higher likelihood of HI after multivariable adjustment (IRR =1.19; CI =1.09, 1.29). CVD was associated with a 10% increased likelihood of HI after age-adjustment (IRR =1.10; CI =1.02, 1.18), but was no longer associated with HI after multivariable adjustment. Cancer, diabetes, and hypertension were not associated with HI in either age- or multivariable-adjusted models.
Discussion
Age- and Multivariable-Adjusted Likelihood of Hearing Impairment: The Health and Retirement Study 2016-2018
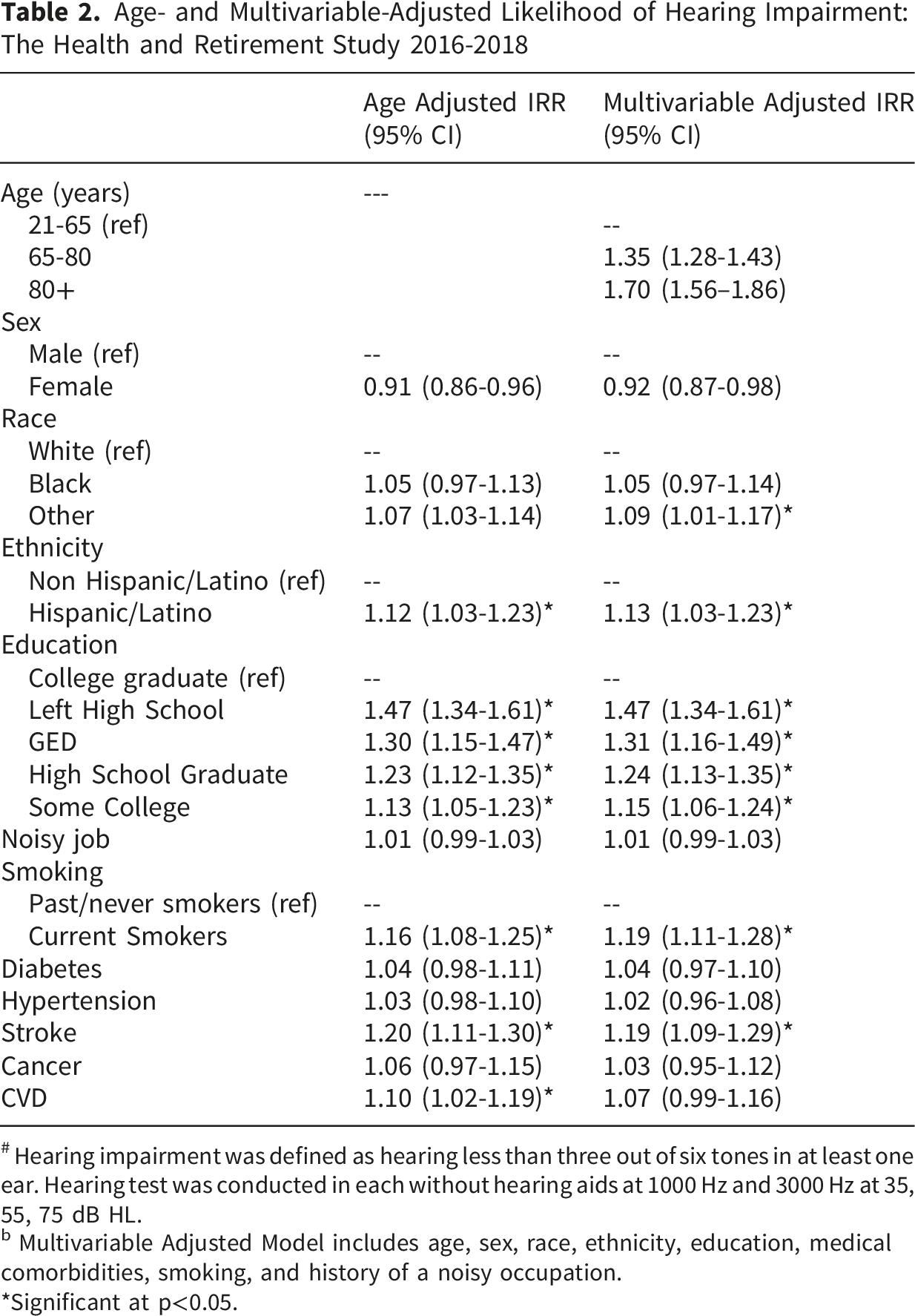
# Hearing impairment was defined as hearing less than three out of six tones in at least one ear. Hearing test was conducted in each without hearing aids at 1000 Hz and 3000 Hz at 35, 55, 75 dB HL.
b Multivariable Adjusted Model includes age, sex, race, ethnicity, education, medical comorbidities, smoking, and history of a noisy occupation.
*Significant at p<0.05.
Population-based prevalence estimates of hearing impairment range from 20.6% in adults forty-eight to fifty-nine years old to 100% in adults over eighty years old. 12 The prevalence of HI found in this study – nearly 74% - is higher than that found in most previous population-based studies. This is likely due to the older age of HRS participants relative to other studies, and it may also be due in part to differences in the way that hearing sensitivity was captured across studies. In the HRS, hearing impairment was based on a screening measurement that captured only two frequencies and three loudness levels rather than the use of more commonly used pure tone averages that capture a broader range of frequencies. Nonetheless, the high prevalence of HI found in this study underscores how common this often-disabling condition is among U.S. adults.
Consistent with previous research3,32,33 we found that HI was more likely with increasing age, and less likely with increasing educational attainment.12,14,34,35 With regard to education, a prior study found a 40% higher risk of 10-year hearing loss in those who had not completed college compared to those who had. 14 Similarly, five year risk of hearing loss was increased (OR = 2.37) in those with less than a high school education compared to college graduates.14,21 Agreeing with these prior findings, our study found 1.37 times greater likelihood of HI in those with less education. A potential reason for the association found between HI and educational attainment is mediation by noise exposure. Excessive noise causes damage to the delicate sound-transducing hair cells of the inner ear, and once these cells are lost they do not regenerate. 13 Age-related damage to the stereocilia in the inner ear underlying the increasing risk of HI with advancing age is the potential reason for the relationship found between hearing and age.14-17
Our findings were consistent with previous studies12,14,19,34 which found that women were less likely than men to have HI. In the Epidemiology of Hearing Loss Study, compared to women, men had 4.42 times higher risk of incident HI over 5 years of follow up, and higher odds of HI were seen for men even after adjusting for age, education, noise exposure and occupation (OR=3.65; CI= 2.97, 4.49). 34 Postulated reasons for the male excess in hearing impairment include relatively higher exposure to occupational noise, and higher prevalence of smoking. Women appear to have a delay in the onset of HI but a slightly faster rate of decline in some frequencies over time. Menopause and changing hormonal levels may be important in explaining these gender patterns. 14
We did not find a significant association between race and HI, in contrast to many previous studies. Most studies have found that black individuals appear to be at lower risk of HI despite having higher rates of other established risk factors such as diabetes. 19 HI has been linked with lower levels of melanocytes in the inner ear, and in previous population-based studies, people with darker skin were less likely to have HI. 13 Despite our null finding with race, we found that those with self-identified Hispanic ethnicity were more likely to have HI compared to non-Hispanics. This is consistent with findings from the NHANES study, which found that compared to those who were White and Black, Hispanics had 2.1 times higher odds of hearing loss among those 60-69 years old, and 11.7 times higher odds among those 70-79 years-old. 3 HI is a common problem for Hispanics as it is associated with socioeconomic factors such as lower education and income, noise exposure, and abnormal glucose metabolism. 36
Smoking has been associated with higher odds of HI in previous studies.12,15,16 In the Epidemiology of Hearing Loss Study, current smoking was associated with a 31% higher risk of incident HI after adjustment for age and sex. 37 Consistent with these findings, we found that current smoking was associated with 17% higher likelihood of HI after multivariable adjustment. Smoking may be associated with HI because nicotine and cigarette smoke interfere with neurotransmitters in the ear, releasing free radical that can damage DNA and becoming more sensitive to loud noises. 13 Additionally, there is a potential synergistic effect between noise exposure and cigarette smoking on hearing loss. 13
Occupational noise exposure is a known risk factor for HI.13,34,38,39 In the EHLS, those whose primary occupations were in production/operations/farming versus other occupations had a 35% higher risk of HI as well as higher risk of HI progression over 5 years.14,34 In contrast, we did not find an association between having had a noisy job and HI. This may be because, in the current study, noisy occupation was defined based on the respondent’s longest occupation sector, so the cumulative effects of noisy work environments may have been underestimated.
Consistent with others17,36,40 we found that HI was associated with self-reported chronic diseases, including hypertension, diabetes, CVD, and stroke, though the magnitude of the associations was attenuated after multivariable adjustment, with the exception of stroke. We found that older adults with a stroke diagnosis had 20% higher odds of HI after multivariable adjustment. Our findings are similar to those found in the National Health Insurance Research Database, who found a 1.64 higher odds of HI among those stroke. 41 Cardiovascular disease was associated with 32% higher odds of HI in the Hispanic Community Health Study/Study of Latinos study, 36 and 63% higher odds of HI in the EHLS. 12 Hearing impairment has been associated with hypertension1,6; potential mechanisms for this association include reductions in blood supply to the inner ear, or medication ototoxicity associated with the use of loop diuretics. 6 Other cardiovascular risk factors such as larger CRVE (central retinal venular equivalent), macrovascular measure IMT (carotid intima-media thickness), statin use, high triglyceride levels, high resting heart rate, fast aortic pulse-wave velocity, and low ankle-arm index have been associated with HI, 12 suggesting that there are likely cardiovascular antecedents of HI.
After multivariable adjustment, we did not find significant associations between HI and diabetes, hypertension, or CVD. It may be that, due to the relatively older age of the HRS sample, the effects of age-related changes to the auditory system and the cumulative effects of noise exposure masked associations between hearing and cardiometabolic conditions, since these associations are often more marked in younger people. 22 Nonetheless, The Health, Aging and Body Composition Study, which had a similar aged sample of older adults, found 45% higher odds of HI associated with diabetes, 18 and in a population-based study in Korea, diabetes was associated with higher odds across all age groups. 1
Strengths of this study include the population-based nature of the HRS, which makes the results of the study generalizable and enhances external validity. The relatively large sample size made it possible to examine multiple potential correlates of HI, including sociodemographic factors, smoking, and medical comorbidities. The HRS employed an instrumental measure of hearing sensitivity rather than relying on survey-based measures, which often underestimate hearing impairment.39,42-44
Despite these strengths this study had several limitations. First, though the HRS used an instrumental hearing assessment, it measured acuity for only two frequencies rather than the gold standard of pure-tone audiometry with a full range of frequencies. While those who heard fewer than three tones in the better ear had significant hearing impairment in line with WHO guidelines, it is possible that some of the participants who heard three or more tones might not have significant hearing impairment but may qualify as having moderate hearing loss. This is a major limitation of the study, as we were only able to compare those with more severe hearing loss to those with normal to moderate hearing loss. Future studies in this cohort should capture a wider range of frequencies and intensity levels so that differences of hearing loss correlates can be examined across hearing loss severity categories. Another limitation is that hearing assessments were not done under soundproofed conditions, which may have overestimated the prevalence of HI we found in the current study.
Most of the correlates of HI we considered were based on self-report. This introduces the possibility of recall bias, response bias, and measurement error. Further, the HRS did not collect data on leisure time noise exposure, and categorization of participants as having a “noisy job” was based on the lengthiest occupation category, rather than capturing all work settings. Thus, we were unable to comprehensively capture the effect of noise exposure, which is one of the most important causes of HI.
The high prevalence of HI found in this study underscores the need for public health campaigns to include universal design features to help those with HI in public spaces, buildings, technologies, and transportation systems.45,46 Hearing screening should be regularly conducted as a routine part of healthcare visits, with appropriate referral as needed to audiological services. The WHO World Report on Hearing emphasizes screening in older adults older than 50 years old (including those without symptoms). 47 In United States there is inconsistent availability and access to hearing screening and amplification for some segments of the population including but not limited to high cost of hearing aids, and lack of insurance to cover the cost. 46 Recent changes in the availability of over-the-counter hearing aids will make hearing remediation accessible to more people, but policymakers should consider programs to assist with costs for people in need.
In conclusion, we found that age-related hearing impairment is highly prevalent in older adults in the U.S., and is associated with advancing age, male sex, Hispanic ethnicity, lower levels of education, smoking, and history of stroke. HI is likely the result of multiple risk factors, and reflects the combined effects of systemic diseases, noise exposure, behavioral factors, and genetics. Future population-based studies of older adults should include the longitudinal assessment of hearing function over time, and should include comprehensive assessments of lifetime noise exposure, lifestyle factors, and genetic risk factors.
Hearing impairment was defined as hearing less than three out of six tones in at least one ear. Hearing test was conducted in each without hearing aids at 1000 Hz and 3000 Hz at 35, 55, 75 dB HL.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.