
Abstract

Significance Statement
Lemierre syndrome is a rare, potentially life-threatening condition characterized by internal jugular vein (IJV) septic thrombophlebitis caused by the spread of an oropharyngeal infection into the lateral pharyngeal spaces and surrounding neck soft tissues. 1 An even more rare subvariant, termed incomplete Lemierre syndrome, presents without internal jugular thrombosis but shares the remaining diagnostic criteria. 2 Few cases in the literature describe incomplete Lemierre syndrome, which may cause delays in diagnosis and treatment. 3
Case Description
We present a case of a 75-year-old man who presented with firm right-sided neck swelling, dysphagia, and poor oral intake for 7 days, unrelieved by antibiotic treatment following an upper respiratory infection, leading him to present to the emergency department.
Physical examination revealed firm swelling of the right lateral neck with no oropharyngeal swelling, scattered petechiae on the roof of the mouth, and right-sided cervical lymphadenopathy. Patient was afebrile with stable vital signs and mild leukocytosis.
Ultrasound of the neck soft tissues demonstrated diffuse smooth wall thickening of the right IJV without a focal thrombus and a narrow caliber lumen compromised by external compression with associated scattered right cervical lymphadenopathy (Figure 1).
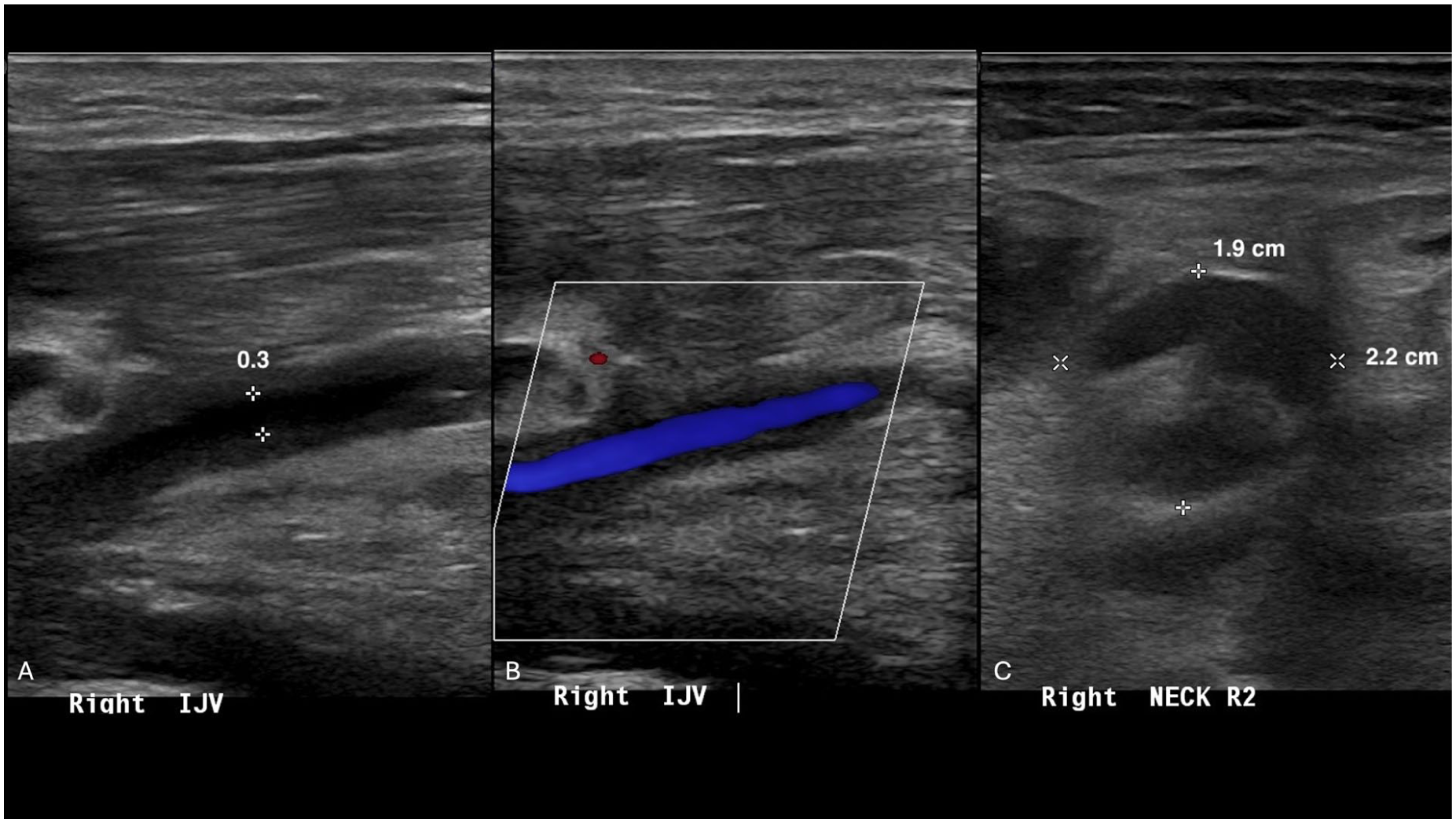
Ultrasound of neck soft tissues using gray scale, spectral and color Doppler demonstrates diffuse, long-segment smooth wall thickening throughout the visualized right internal jugular vein (A). (B) Patency of the vessel without a focal thrombus. (C) Scattered right cervical lymphadenopathy.
Contrast-enhanced computed tomography (CT) of the neck soft tissues demonstrated a diffuse inflammatory process with right prevertebral soft tissue swelling without a definable retropharyngeal fluid collection (Figure 2). Findings were compatible with septic phlebitis of the right IJV without thrombus, consistent with incomplete Lemierre syndrome.

Contrast-enhanced CT of neck soft tissues. (A, B) Coronal and axial reformats demonstrate diffuse inflammatory stranding (blue arrows) of the soft tissues of the neck deep to the right platysma muscle and a 9 cm craniocaudal segment of the right internal jugular vein (red arrows) with diffuse peripheral thickening and associated right cervical lymphadenopathy (yellow arrows). (C) Axial reformat of contrast-enhanced CT obtained 3 days after antibiotic initiation demonstrates improvement of inflammatory stranding (blue arrow), cervical lymphadenopathy (yellow arrow), and peripheral thickening of the right internal jugular vein (red arrow). CT, computed tomography.
The patient was subsequently treated with steroids and broad-spectrum antibiotic coverage, including metronidazole to ensure Fusobacterium coverage and piperacillin-tazobactam. Following infectious disease consultation, antibiotics were adjusted to ceftriaxone and metronidazole, and the patient was transferred to the intensive care unit for airway monitoring and management. The following morning, flexible laryngoscopy was performed, demonstrating nasopharyngeal, oropharyngeal, glottic, and laryngeal edema. The patient elected to continue conservative airway management rather than undergo a tracheotomy. No clinical signs or symptoms were present to suggest developing venous thromboembolism.
Subsequent imaging demonstrated improved cervical lymphadenopathy, right IJV wall thickening, and soft tissue inflammation with persistent edema in the retropharyngeal space. The patient was discharged with a 3-week course of Augmentin. Unfortunately, no throat specimen was collected prior to antibiotic administration, and a causative microorganism was not identified on blood and throat cultures.
Discussion
To date, only 3 other cases have been identified as Lemierre syndrome with the absence of IJV thrombosis, coined incomplete Lemierre syndrome.2,4,5 Lemierre syndrome is most frequently associated with the obligate anaerobic, gram-negative bacillus Fusobacterium necrophorum—although other microorganisms, such as Streptococcus species, Staphylococcus species, Bacteroides fragilis, and Klebsiella pneumoniae, have also been implicated.1,6 Epstein-Barr virus has also been described as a potential precipitating infection in Lemierre syndrome, either alone or in association with secondary bacterial superinfection due to virus-induced mucosal damage. 1 Lemierre syndrome incidence is greater in males, with an approximate male-to-female ratio of 2:1. 7
The high frequency of benign oropharyngeal infections in the general population leads to a broad differential diagnosis of early Lemierre syndrome, which can often result in delays in diagnosis and treatment. Such delays increase the risk of complications such as subsequent sepsis with metastatic septic emboli leading to necrotizing pneumonia, lung and brain abscesses, septic arthritis, and osteomyelitis. 8 Therefore, early recognition of Lemierre syndrome is crucial to provide appropriate treatment to prevent disease progression to decrease the mortality rate, which is reported to be between 5% and 18%. 3 Twenty six percent to 45% of cases present with the “cord sign,” swelling at the mandibular angle, suggestive of internal jugular thrombosis. 2
Chest radiographs should be obtained to detect pulmonary/pleural involvement. To evaluate for septic thrombosis of the IJV, ultrasound, CT of the neck with contrast, and magnetic resonance imaging may be utilized. Contrast-enhanced CT is the most widely used due to accessibility and is considered the best diagnostic method due to its ability to visualize vascular thrombosis of the IJV, intraluminal filling defects, enhancement of the IJV, and soft tissue swelling. 1
Broad-spectrum intravenous antibiotics with anaerobic coverage are the cornerstone of treatment. Recommended regimens often include metronidazole, clindamycin, and β-lactams combined with a β-lactamase inhibitor to cover resistant species for a duration of 3 to 6 weeks, with transition to oral medication following 2 weeks of induction intravenous therapy, provided there is clinical improvement. 2 In cases of delayed diagnosis or failure to improve with antibiotic therapy, interventions such as abscess drainage, mastoidectomy, jugular vein ligation, and/or embolectomy (for septic emboli), and, rarely, invasive cranial surgery, may be required. 7
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Author Contributions
Jagan Gupta conceived the case topic and designed the paper methodology. Elizabeth Romantz and Simone Biow conducted the data collection and performed the investigation and analysis. Jagan Gupta, Neel Gupta, Triet Do, Enrique Palacios, Simone Biow, and Elizabeth Romantz interpreted the results and contributed to the manuscript writing. All authors reviewed and approved the final manuscript, ensuring accuracy and integrity in the reported findings.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.