
Abstract
Introduction:
Although the literature indicates an increased incidence of voice disorders among older adults, data regarding the etiological distribution of dysphonia across different age subgroups remain limited. Therefore, the present study aimed to evaluate the distribution of voice disorder etiologies among dysphonic patients aged 65 years and older, stratified by age subgroup.
Materials and Methods:
Patients aged 65 years and older presenting with voice complaints were stratified into 3 age subgroups: 65 to 74, 75 to 84, and ≥85 years. The etiological diagnoses of voice disorders were classified into 8 categories based on clinical and literature-supported definitions.
Results:
The most common voice disorder among patients aged ≥65 years and older was malignant vocal fold pathology (28.0%), followed by vocal fold immobility (20.0%), vocal fold atrophy (12.1%), and chronic laryngitis (12.1%).
Conclusion:
This study underscores that most cases of geriatric dysphonia arise from pathological rather than from age-related causes. These findings highlight the importance of thorough laryngeal evaluation in elderly patients presenting with hoarseness.
Introduction
Phonation is a complex function involving multiple physiological systems.1,2 Although the larynx serves as the primary source of sound production, healthy voice generation depends on the coordinated and optimal functioning of the respiratory, cardiovascular, musculoskeletal, neurological, and psychosocial systems.2,3 A voice disorder is defined as an abnormality in voice quality, and age-related changes in 1 or more of these systems may lead to alterations in vocal characteristics.1,4,5
While the reported prevalence of voice disorders in the general elderly population ranges from 4.8% to 29.0%, accurately determining this rate remains challenging.5,6 Many older individuals perceive a certain degree of voice impairment as a natural part of aging and therefore do not seek medical attention.3,7,8 Furthermore, the presence of age-related comorbidities may cause hoarseness to be perceived as a minor issue, leading to the underrecognition of presbyphonia—a treatable condition—and a lack of awareness regarding available therapeutic options.1,3,6 These factors contribute to the underreporting of voice disorders in the elderly, despite their high prevalence.4,6
It is important to recognize that this attitude of acceptance among older adults may result in impaired communication and/or social withdrawal.3,5,7 Identifying the potential etiology of dysphonia is critical for the appropriate evaluation and management of elderly patients with voice disorders. However, individuals aged 65 years and older do not constitute a homogeneous group. Due to anatomical, physiological, and psychosocial differences that emerge with aging, the geriatric population is commonly categorized into 3 subgroups: young-old (65-74 years), middle-old (75-84 years), and oldest-old (85 years and above).8,9
This study was conducted based on the findings reported by Applebaum et al, 8 with the aim of examining these results within a different population and clinical setting. The objective of the study was to evaluate the etiological distribution of voice disorders across age subgroups among dysphonic patients aged 65 years and older presenting to a general otolaryngology clinic in a tertiary referral hospital, and to explore whether age-related patterns described in previous studies are applicable to a different patient cohort.
Materials and Methods
This single-center, retrospective observational study was conducted by reviewing the medical records of patients aged 65 years and older who presented with voice complaints to the Voice Clinic of Antalya Training and Research Hospital between January 2022 and May 2025. The study was approved by the institutional ethics committee (date: 2023, no.: 14) and carried out in accordance with the principles of the Declaration of Helsinki. Patients who presented solely with dysphagia, those younger than 65 years, and those with incomplete data were excluded from the study.
Patient age, sex, and clinical diagnoses were recorded. Video laryngoscopic and stroboscopic examination records of all included patients were reviewed.
To evaluate the etiology of voice disorders across age groups in accordance with the literature, patients were stratified into 3 subgroups: 65 to 74, 75 to 84, and ≥85 years. The etiological diagnoses of voice disorders were classified into 8 categories based on clinical and literature-supported definitions8,9:
Benign vocal fold lesions
Vocal fold immobility (paresis/paralysis)
Vocal fold atrophy (presbyphonia)
Muscle tension dysphonia
Chronic laryngitis (including laryngopharyngeal reflux [LPR])
Infectious laryngitis
Neurologic disorders (central nervous system diseases affecting laryngeal function)
Malignant vocal fold lesions
The accuracy of benign and malignant vocal fold lesion diagnoses was confirmed through histopathological examination. Patients with multiple voice disorder diagnoses were classified under a single category based on the primary cause of dysphonia.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24.0. Continuous variables were presented as median (interquartile range), and categorical variables as frequency (%). The Shapiro-Wilk test was used to assess the normality of distribution for continuous variables. Comparisons of continuous variables between independent groups were conducted using the Kruskal-Wallis test, with Bonferroni correction applied for post hoc analysis when significant differences were found. The chi-squared test was used for comparisons of categorical variables. Logistic regression analysis was performed to evaluate the association of age and gender with different diagnostic categories, and adjusted odds ratios (ORs) were calculated. A P < .05 was considered statistically significant.
Results
Between January 2022 and May 2025, a total of 411 patient records were identified for individuals aged 65 years and older who presented to the voice clinic with complaints of voice disorders. Of these, 47 patients were excluded from the study (42 due to a diagnosis of dysphagia and 5 due to incomplete data). Ultimately, data from 364 patients were analyzed, including 215 patients (59.1%) aged 65 to 74 years, 114 patients (31.3%) aged 75 to 84 years, and 35 patients (9.6%) aged ≥85 years. Among the study population, 203 patients (55.8%) were male and 161 (44.2%) were female.
The most common voice disorder among patients aged 65 years and older was malignant vocal fold pathology (28.0%), followed by vocal fold immobility (20.0%), vocal fold atrophy (12.1%), and chronic laryngitis (12.1%). The distribution of voice disorders across age groups is presented in Figure 1.
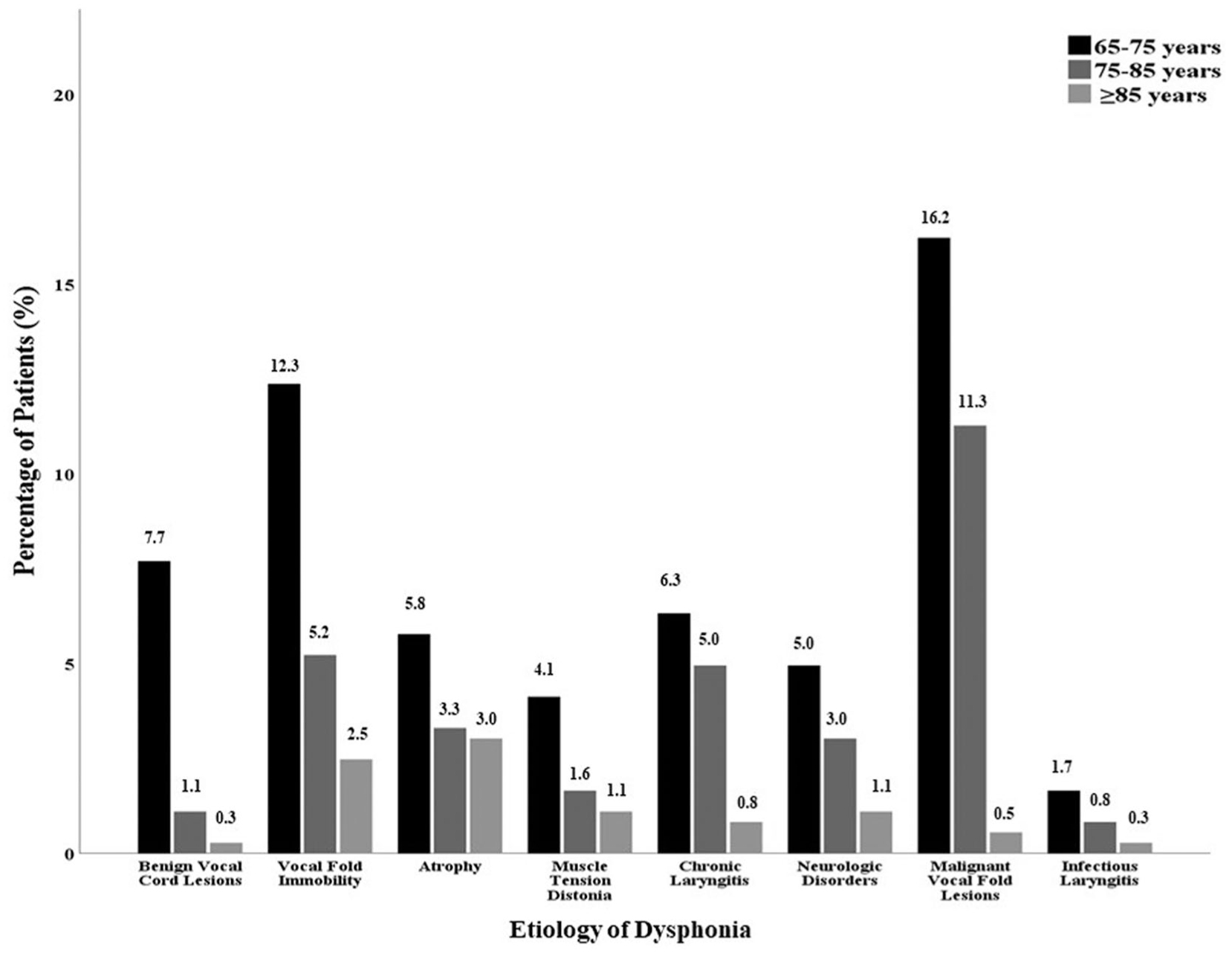
Percentage of patients by age.
When analyzed by gender, the most frequent etiologies in male patients were malignant vocal fold lesions (20.3%), vocal fold immobility (11.0%), and atrophy (6.9%). In female patients, the most common etiologies were vocal fold immobility (9.0%), malignant vocal fold lesions (7.7%), and chronic laryngitis (7.1%; Figure 2). The etiological distribution of dysphonia by age and gender is summarized in Table 1.
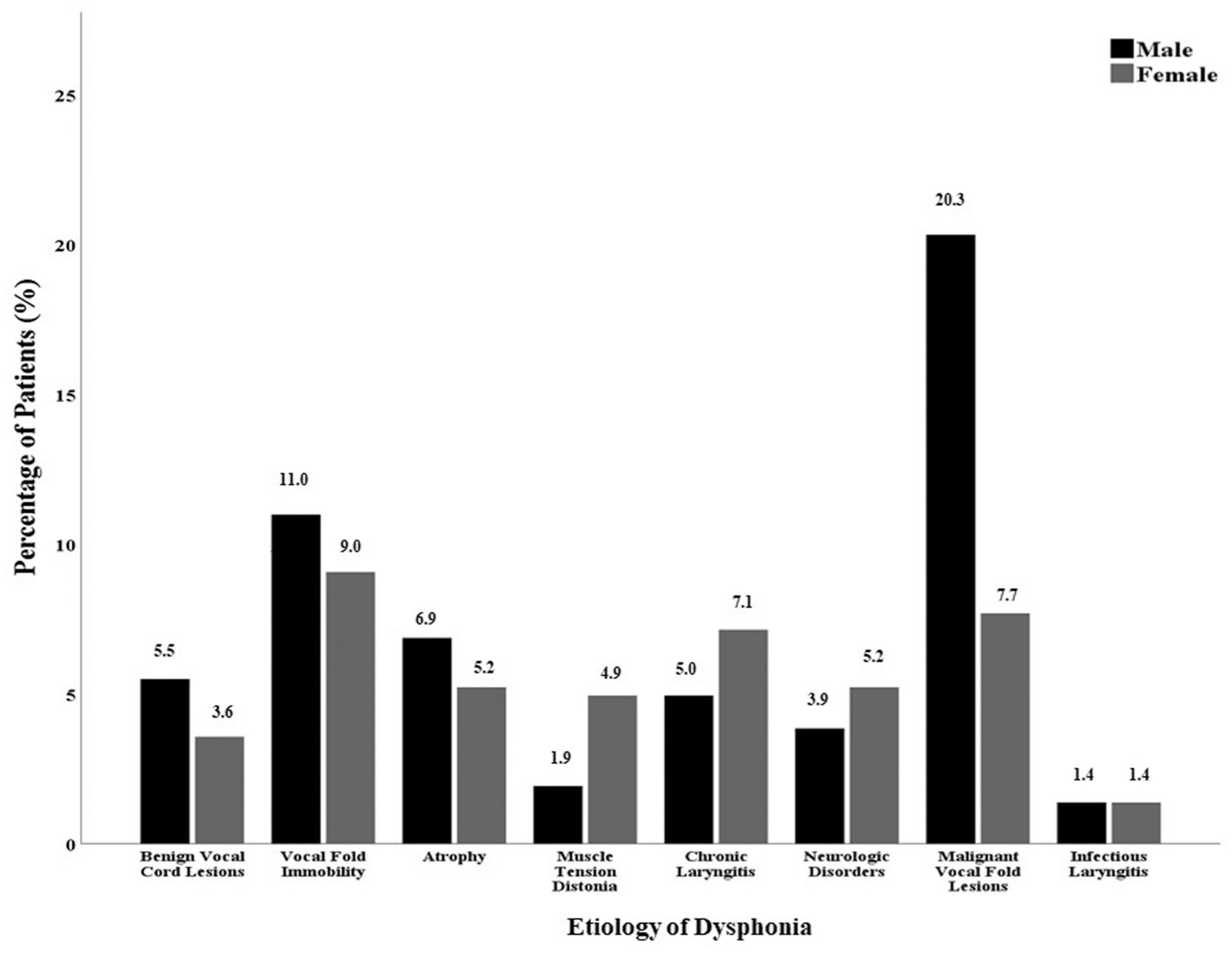
Percentage of patients by gender.
Etiology of Dysphonia by Age and Gender.
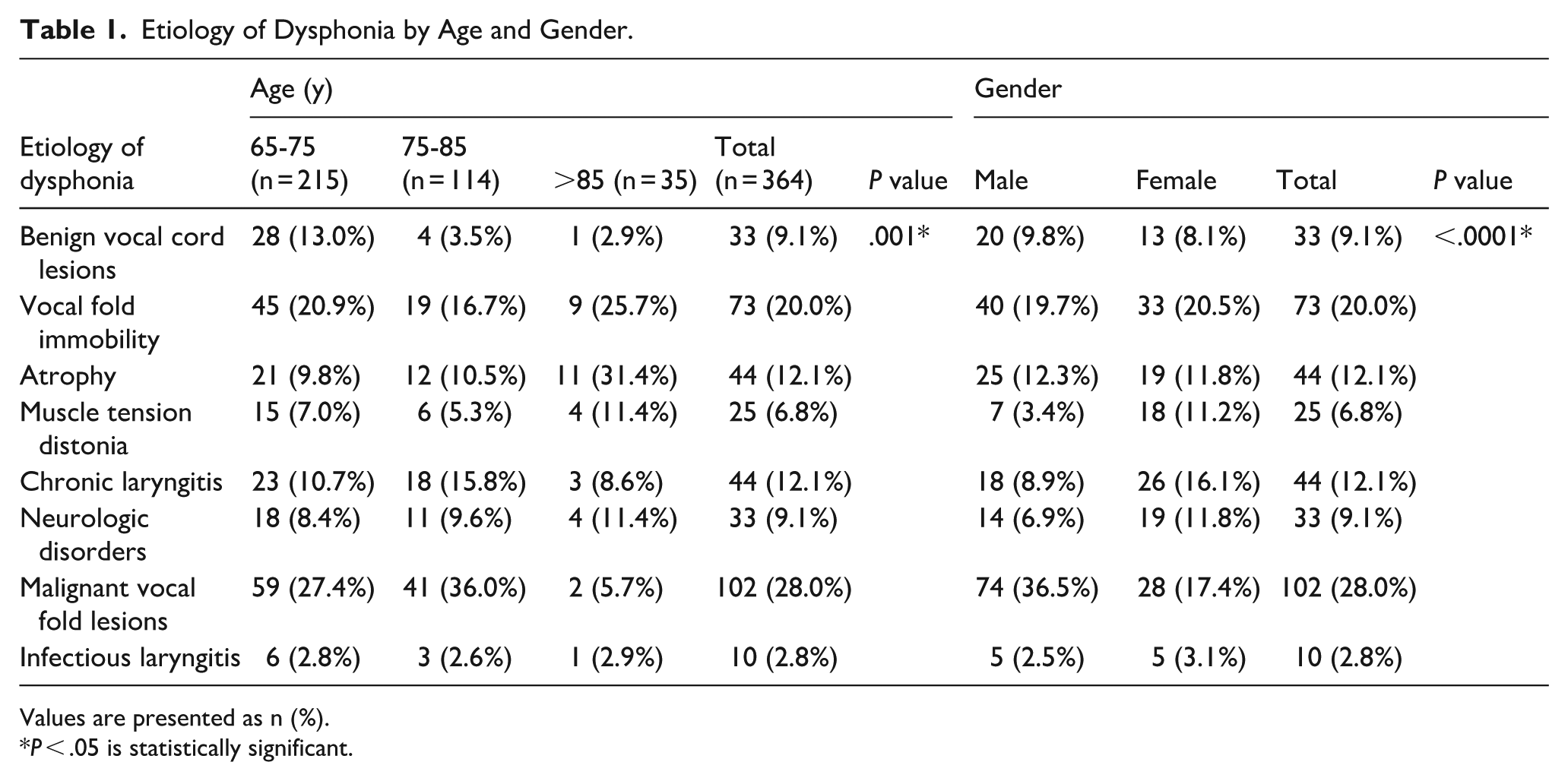
Values are presented as n (%).
P < .05 is statistically significant.
A statistically-significant difference was found in patient age across the etiological categories of voice disorders (P = .019). Infectious laryngitis and benign vocal fold lesions were more commonly observed in younger patients, whereas vocal fold atrophy and chronic laryngitis were more prevalent in older individuals.
When evaluating the influence of age and gender on the etiology of voice disorders in patients aged 65 years and older, age was found to be significantly associated with the risk of certain conditions. Specifically, increasing age was associated with a decreased risk of benign vocal fold lesions (OR = 0.884; 95% CI: 0.822-0.951) and an increased risk of vocal fold atrophy (OR = 1.060; 95% CI: 1.016-1.107).
Additionally, male sex was found to significantly affect the risk of several etiologies. Male patients had ~0.3 times lower risk of muscle tension dysphonia (OR = 0.299; 95% CI: 0.120-0.740), 0.5 times lower risk of chronic laryngitis (OR = 0.494; 95% CI: 0.260-0.939), and 2.6 times higher risk of malignant vocal fold lesions (OR = 2.600; 95% CI: 1.579-4.281; Table 2).
Regression Model for Odds of Particular Etiologies of Dysphonia.
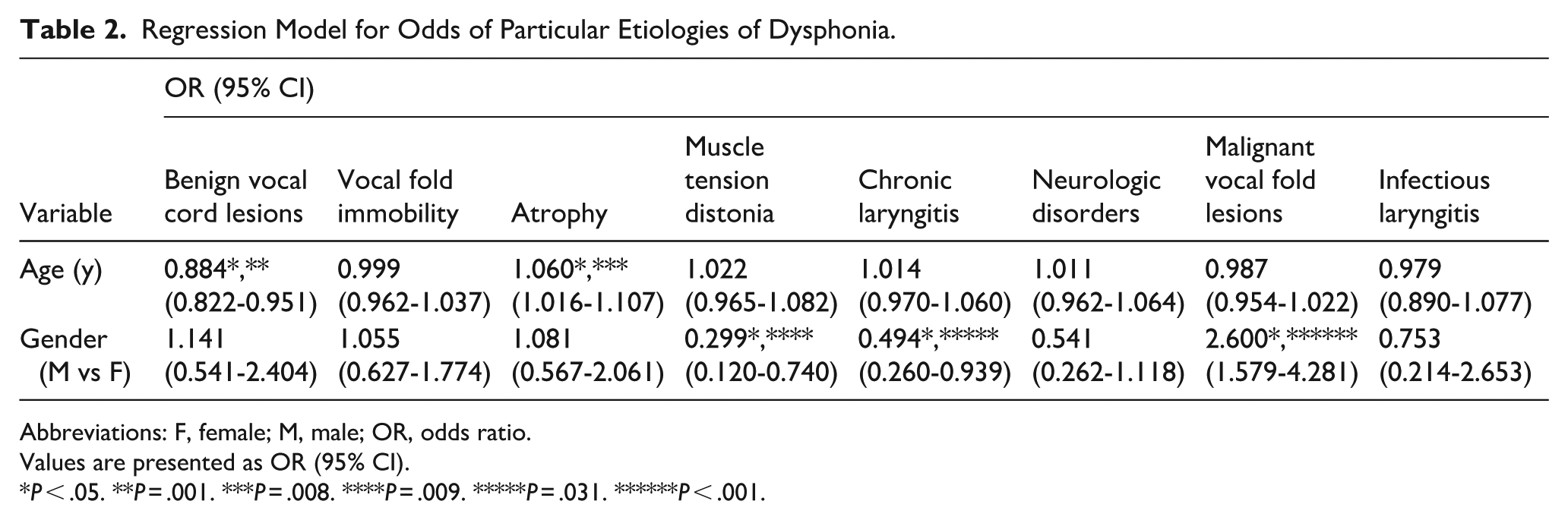
Abbreviations: F, female; M, male; OR, odds ratio.
Values are presented as OR (95% CI).
P < .05. **P = .001. ***P = .008. ****P = .009. *****P = .031. ******P < .001.
Discussion
The effects of aging on the human voice are complex, influenced by both anatomical-physiological changes and accompanying medical and social factors.3,9,10 Although these natural changes are referred to as “presbyphonia,” hoarseness in an elderly patient is not always a benign consequence of aging.1,5 The intersection of normal aging and pathological processes presents a diagnostic challenge in geriatric voice disorders.1,2,11 It has been emphasized that distinguishing between normal age-related vocal changes and disease-related alterations can be difficult. 1 In fact, the etiology of dysphonia in older adults often involves multiple contributing factors.3,6,7 For example, an elderly patient may present with vocal fold atrophy, but coexisting conditions such as Parkinson’s disease or poststroke vocal fold paralysis may also contribute to the voice disorder.1,7,8 Additionally, age-related reductions in pulmonary capacity and weakening of thoracic and diaphragmatic muscles may further impair phonation, exacerbating laryngeal dysfunction.1,5,9 Therefore, when evaluating hoarseness in geriatric patients, natural aging changes in the larynx, neurological comorbidities, systemic conditions (eg, chronic obstructive pulmonary disease), and local pathologies must all be considered.1,5,7
Moreover, elderly individuals may differ in how they perceive and report voice complaints, as well as in their health care–seeking behavior. 6 Many older adults consider hoarseness a normal part of aging and may not seek medical attention. 7 Unfortunately, this can lead to delays in the diagnosis of malignant vocal fold lesions.
Geriatric dysphonia is a significant public health concern that can adversely affect the quality of life in older adults.2,6,8 Studies have shown that dysphonia can impair communication, contributing to social isolation, depression, and anxiety.6,8 Older individuals are already at increased risk of depression and loneliness, and when speech difficulties are added, they may withdraw further from social interaction.5,9 In advanced age groups, hearing loss among peers and spouses may also be present, creating a dual communication barrier—one party struggles to hear, the other to speak—resulting in substantial limitations in interpersonal communication.7,8 This isolation can negatively impact both mental and physical health. Furthermore, communication difficulties may hinder elderly patients from adequately expressing their medical needs, indirectly affecting their access to health care services.6 -8
This study retrospectively analyzed data from 364 patients aged 65 years and older who presented with voice disorders. The most common etiologies identified were malignant neoplasms (28.0%) and vocal fold immobility/paralysis (20.0%). Our findings indicate that the etiology of geriatric dysphonia is distributed across various organic and functional causes and that age-related vocal fold changes (presbyphonia) account for only a relatively-small proportion of cases.
Our results show both concordance and divergence with previous studies in the literature regarding the distribution of voice disorders in the elderly population.2,4,7 A similar study conducted in Turkey by Kandogan et al evaluated 98 patients over the age of 60 years and reported benign vocal fold lesions (28.6%) as the most common cause, followed by malignant vocal fold lesions (27.6%) and vocal fold paralysis (25.5). 4 In our study, malignant neoplasms were the most frequent etiology (28.0%), which may reflect our status as a tertiary care center receiving referrals for malignancies from surrounding hospitals. Conversely, the rate of benign lesions in our cohort (9.0%) was lower than that reported by Kandogan et al. Their study included patients aged 60 to 65 years, a group more likely to present with benign lesions such as nodules and polyps. Our study focused exclusively on patients aged 65 years and older, excluding the younger segment of the elderly population, which may explain the lower prevalence of benign vocal fold pathologies.
Studies from different geographic regions also report that pathological processes are predominant in geriatric dysphonia.3,5,7 For example, a study conducted in a rural hospital in India involving 100 patients aged 65 years and older found LPR to be the most common cause (23.0%), followed by laryngeal cancer (12.0%) and presbylarynx/presbyphonia (8.0%). 7 In our cohort, the rate of chronic laryngitis due to reflux was ~12.0%, lower than that reported in the Indian study. Their findings also showed that presbyphonia was a minor contributor overall, with inflammatory and neoplastic processes being more common in the aged 65 to 74 years group, while presbyphonia and systemic conditions became more prominent in older age groups (75-89). This aligns with our subgroup analysis, which showed that age-related vocal fold changes were more pronounced in the oldest patients.
Studies from the United States present a somewhat different picture of geriatric voice disorders.1,2,6 In particular, patient populations presenting to specialized voice clinics may differ from those seen in general ENT practice.1,8 For instance, Davids et al analyzed patients at Emory Voice Center, a university-based voice clinic, and reported presbylarynx (vocal fold atrophy) as the most common diagnosis (25.0%) among patients aged 65 years and older, followed by neurologically-related voice disorders (23.0%) and vocal fold paralysis/immobility (19.0%). 1 The proportion of elderly patients presenting with malignancy was notably low. In our study, the rate of atrophic (presbyphonic) voice disorders was ~12.0%, lower than that reported by Davids et al. This discrepancy may be due to differences in patient profiles and referral patterns. In specialized voice clinics, cancer cases are often referred to separate oncology units or may not return for follow-up, resulting in a higher proportion of benign and functional disorders. This may explain the low malignancy rate in Davids et al’s cohort.
Similarly, a recent study at Johns Hopkins University by Applebaum et al evaluated 463 newly-presenting dysphonic patients aged 65 years and older and found vocal fold immobility (28.3%) and vocal fold atrophy (21.6%) to be the most common diagnoses. 8 Their data showed that patients aged 65 to 74 years were more likely to present with benign lesions (eg, nodules, polyps) and paralysis, while those aged 75 years and older had a significantly-higher prevalence of presbylarynx. They also calculated that the likelihood of receiving a presbyphonia diagnosis increased by ~7.0% with each advancing year of age. Our finding of a roughly 6.0% increase (OR = 1.06) is remarkably consistent, suggesting that the impact of aging on vocal fold function is robust across different populations. On the other hand, malignancies were not a major category in their study, again reflecting the patient profile of specialized voice clinics. In contrast, malignancy was a prominent category in our general ENT practice, highlighting that cancer remains a significant threat among elderly individuals with specific risk factors.
Risk factors contributing to the development of voice disorders in geriatric patients have also been examined. Gois et al, in their evaluation of data from 2 large epidemiological studies, suggested that both physical and psychosocial factors may play a role. 3 For example, age, gender, existing chronic diseases, occupational voice use, and smoking are physical/behavioral factors, while depression and social isolation are psychosocial factors that can affect vocal health in older individuals. However, the authors emphasized that methodological differences between the studies they reviewed made direct comparisons difficult, highlighting the need for more standardized research in this area.
Although our study presents cross-sectional data from a specific clinical population and does not directly investigate the impact of risk factors on the general population, trends reported in the literature help contextualize our findings.3,5 For instance, the higher prevalence of malignancy in male patients may be associated with greater exposure to tobacco and other physical risk factors. 3 Similarly, the higher rate of functional dysphonia in female patients may reflect psychosocial influences, such as increased awareness of vocal changes and help-seeking behavior, or stress-related vocal impairment.3,8,9 Overall, the broader perspective in the literature supports the notion that geriatric voice disorders are multifactorial in origin rather than attributable to a single cause.
Nevertheless, our study has several limitations. First, it was conducted using a retrospective design, which allows for the evaluation of existing data but carries inherent methodological constraints compared to prospective studies. Second, the research was carried out in a single tertiary care training and research hospital rather than in a dedicated voice clinic. As a result, the patient profile may include a relatively-high proportion of secondary dysphonia cases, such as those related to head and neck cancers or postsurgical vocal fold paralysis. This may limit the generalizability of our sample to the broader elderly population.
Finally, the sample size, particularly in the oldest age subgroup, may have been insufficient to adequately represent certain diagnostic categories. This limitation could reduce the statistical power of subgroup analyses and restrict the generalizability of the findings.
Conclusion
Although dysphonia is common in the geriatric population, it is frequently underrecognized and undertreated. Many elderly individuals perceive hoarseness as a natural consequence of aging and do not seek medical attention, which may lead to delays in the diagnosis of malignant vocal fold lesions. According to our study findings, the most prevalent causes of geriatric dysphonia were malignant neoplasms and vocal fold paralysis, while age-related vocal fold changes (presbyphonia) accounted for only a relatively small proportion of cases. Therefore, increasing awareness of dysphonia among both patients and clinicians is essential for timely diagnosis and appropriate management in elderly populations.