
Abstract
Background:
Intraoperative bleeding during endoscopic sinus surgery (ESS) impairs visualization and increases operative risks. Hot saline irrigation (HSI) has been proposed as a simple, safe hemostatic adjunct compared with room temperature saline.
Objective:
To evaluate the effects of HSI versus room temperature saline on surgical field visibility, blood loss, operative duration, and hemodynamic stability in ESS.
Methods:
Systematic review and meta-analysis of randomized and nonrandomized controlled trials identified through PubMed, Embase, Cochrane CENTRAL, and ClinicalTrials.gov up to 30 October 2025. Outcomes were pooled using random-effects inverse-variance models in RevMan 5.4.1 by Cochrane.
Results:
Seven studies (n = 453 patients) were included. HSI significantly improved Boezaart bleeding scores (mean difference [MD] −0.68, 95% confidence interval [CI] −1.01 to −0.34; P = .0002; I2 = 79.7%), reduced intraoperative blood loss (MD −56.33 mL, 95% CI −57.22 to −55.44; I2 = 37.1%), and shortened operative time (MD −9.78 minutes, 95% CI −14.62 to −4.94; P < .0001; I2 = 85.0%). No significant difference was observed in mean arterial pressure (MD −0.68 mmHg, 95% CI −2.22 to 0.86; P = .39).
Conclusion:
HSI significantly enhances surgical field visibility, reduces blood loss, and shortens operative duration during ESS without affecting hemodynamic stability. It represents a safe, low-cost alternative or complement to pharmacological hemostatic agents.
Plain Language Summary
Chronic sinusitis is a common condition that causes long-term nasal blockage, facial pain, and other troublesome symptoms. When medications no longer help, doctors often perform a minimally invasive operation called endoscopic sinus surgery (ESS). This procedure uses a small camera and tools inserted through the nose to clear blocked sinuses. A frequent challenge during this surgery is bleeding, which can cloud the surgeon’s view, make the operation longer, and raise the risk of complications.
This review looked at seven clinical studies involving over 450 patients to see if rinsing the surgical area with warm (hot) saline – ordinary saltwater heated to around body temperature or slightly higher – works better than using saline at room temperature.
The results showed clear benefits from using hot saline:
• Surgeons reported much less bleeding and a clearer view of the operating area.
• Patients lost about 56 millilitres less blood on average.
• Operations finished around 10 minutes faster.
• Blood pressure during surgery stayed the same in both groups, meaning the warm saline did not cause any unwanted effects on the heart or circulation.
Hot saline is inexpensive, easy to prepare in any operating room, and has no systemic side effects (unlike some medicines or blood pressure-lowering drugs used for the same purpose). The findings suggest that warming the irrigation fluid is a safe and effective way to improve safety and efficiency during sinus surgery. This simple step could be adopted widely, especially in settings where more expensive hemostatic agents are not available or suitable for the patient.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a persistent inflammatory condition of the sinonasal mucosa that lasts for more than 12 weeks and significantly impacts patients’ quality of life. 1 Patients may experience nasal obstruction, facial pain, rhinorrhea, and reduced olfactory function. 2 When medical therapy is not effective, endoscopic sinus surgery (ESS) is the standard operative approach for restoring ventilation and drainage of the paranasal sinuses. 3 Functional endoscopic sinus surgery (FESS) is the most frequently performed form of ESS, and it aims to remove obstruction while preserving natural anatomy as much as possible.2,3
Despite its minimally invasive nature, ESS is often complicated by intraoperative bleeding that impairs visualization. Even mild bleeding can interfere with the surgeon’s ability to identify anatomical landmarks, increasing the risk of complications involving the orbit or skull base. 4 Effective control of bleeding is critical for maintaining a clear surgical field, which in turn reduces the duration of surgery and minimizes the likelihood of errors. 5 Common strategies to control bleeding include the use of vasoconstrictors (e.g., epinephrine), systemic agents (e.g., tranexamic acid), and hypotensive anesthesia. 6 While effective, these methods have potential drawbacks, such as the systemic absorption of vasoconstrictors, which can lead to cardiovascular complications, especially in high-risk patients, and induced hypotension, which requires careful management to avoid compromising organ perfusion. 7
Hot saline irrigation (HSI) has emerged as an alternative technique that is simple to apply and does not carry systemic risks. 8 Irrigation with saline warmed to approximately 48°C to 50°C can reduce capillary oozing by producing local thermal effects that support hemostasis and reduce mucosal edema. It can also help keep the endoscopic lens clear, which further aids visualization.4,8 Importantly, HSI does not carry the same systemic risks as pharmacological agents, making it a safer option for patients with contraindications to vasoconstrictors or those requiring longer surgical durations. 5
Randomized controlled trials (RCTs) evaluating HSI have shown promising results, including reductions in blood loss, improvements in surgical field grading scores, and shorter operative times. 6 A prior meta-analysis reported that HSI reduced overall blood loss by about 20% and shortened surgery by several minutes compared with room temperature saline irrigation. 3 Other studies have suggested that HSI is as effective as tranexamic acid in improving the operative field during FESS. 5 However, evidence has continued to accumulate in recent years, and heterogeneity across study protocols, irrigation temperatures, and surgical procedures highlights the need for an updated synthesis that reflects the current literature.
The aim of this meta-analysis is to evaluate the effect of HSI on intraoperative bleeding, visualization, operative duration, and hemodynamic stability during ESS. By integrating the most recent randomized trials and using standardized outcome measures, this study seeks to provide a more complete assessment of the role of HSI as a hemostatic adjunct in ESS.
Materials and Methods
This systematic review and meta-analysis were conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines.9,10 The protocol was registered in PROSPERO before commencing the review (PROSPERO ID: CRD420251118404).
Literature Search Strategy
A comprehensive search was performed across Medline (PubMed), Embase, ClinicalTrials.gov, and the Cochrane Central Register of Controlled Trials, covering the literature from inception to October 30, 2025. The full reproducible search strategy for PubMed is provided in Supplemental Material; equivalent strategies were adapted for Embase (using Emtree terms), Cochrane CENTRAL, and ClinicalTrials.gov (e.g., replacing MeSH with keyword variants). In addition, the reference lists of the included studies were manually reviewed to identify any further eligible trials. Gray literature, including theses and unpublished research, was excluded.
Inclusion Criteria (PICO)
Studies were eligible if they met the following criteria: Population: Adult patients undergoing ESS. Intervention: Intraoperative HSI; comparator: room temperature normal saline, and Outcome: Intraoperative outcomes, that is, Boezaart score, intraoperative blood loss, surgical time, etc. Studies that were either randomized or non-RCTs were included. Observational designs (cohorts, case reports, and series), animal research, reviews, and studies not in the English language were excluded.
Screening and Data Extraction
Articles identified through the database search were imported into Rayyan AI (Rayyan Systems, Inc), where duplicates were removed automatically. 11 Two independent reviewers (A.R. and S.M.) screened the titles, abstracts, and full text according to the eligibility criteria. Discrepancies were resolved by consensus with the senior investigator (S.C.). Data extraction was performed using a structured Excel spreadsheet (M.I. and A.R.), collecting details such as author, publication year, study location, sample size, study design, and demographics, such as mean age in years, sex distribution, Boezaart score, intraoperative blood loss, operative time, and mean arterial pressure (MAP).
Use of Artificial Intelligence Tools
During the study selection process, the Rayyan AI platform (web-based version, accessed November 2025; Rayyan Systems Inc) was used to assist with duplicate removal and to facilitate the title and abstract screening of retrieved records. Only bibliographic metadata (titles, abstracts, and DOIs) from publicly available studies were uploaded, with no patient or identifiable data involved. All screening decisions suggested by Rayyan were independently verified by 2 reviewers (A.R. and R.G.O.), and discrepancies were resolved by consensus with the senior investigator to ensure accuracy and reduce bias (S.C.).
Outcomes
Boezaart intraoperative bleeding score was used to measure the primary outcome. 12 It is a validated instrument for quantifying intraoperative bleeding. It uses a 5-point scale. Grade 0 is set for a field without bleeding, 1 for slight bleeding without suction, 2 for slight bleeding with suction required, 3 for moderate bleeding that improves for several seconds after suction is removed, 4 for moderate bleeding that occurs immediately when suction is removed, and 5 for severe bleeding that requires constant suction where bleeding occurs more than can be removed. It is assessed by the operating surgeon throughout the length of the surgery.
Mean intraoperative blood loss, mean surgical time, and MAP were the secondary outcomes assessed.
Risk of Bias Assessment
To evaluate methodological quality, the Cochrane risk of bias tool for randomized trials (RoB-2) was used across all RCTs. 13 For the nonrandomized trial, the ROBINs V2 tool was used. 14 Two reviewers independently performed the assessments (S.M. and M.I.) to ensure methodological rigor and reproducibility. Any discrepancies were resolved collaboratively through consensus with a senior investigator (S.C.), thereby maintaining consistency and reliability in bias evaluation.
Statistical Analysis
Statistical analyses were conducted using R Studio 2025.09.2, by Posit, PBC, by 2 authors (T.I. and A.R.). For continuous outcomes, the inverse-variance method was used, and the results were expressed as mean difference (MD) or standardized mean differences and 95% confidence intervals (CIs). Where studies reported medians and interquartile ranges, data were converted to mean ± standard deviation (SD) using a standardized method. Dichotomous outcomes were analyzed using the Mantel-Haenszel method, with results presented as risk ratios and 95% CIs. 15 A random-effects model was applied to account for inter-study variability, and pooled estimates were visualized using forest plots. 16 Heterogeneity was quantified using the Higgins I2 statistic. 17 Publication bias was not formally assessed due to the limited number of included studies (n = 7, below the recommended threshold of 10 for reliable tests such as funnel plots or Egger’s regression), as this would lack statistical power. 10 Both RCTs and non-RCTs were pooled, given their comparable controlled designs and focus on the intervention; however, a sensitivity analysis excluding each study one at a time was conducted to evaluate robustness and explore heterogeneity. Certainty of evidence for each outcome was formally assessed using the GRADE approach. 18
Results
Study Characteristics
A total of 262 articles were identified from the searches; 4 duplicate records were removed. Two hundred thirty articles were excluded during the primary screening using their titles and abstracts. Nineteen full articles were assessed for their eligibility, and 12 were removed. These included 6 review articles,3,19 -22 5 observational studies,23 -27 and 1 study 1 adenoidectomy. 28 Seven studies, including 6 RCTs and 1 quasi-experimental study with a total sample size of 453 patients, comprising 226 participants in the HIS group and 227 in the room temperature saline group, conducted between 2014 and 2025 across various countries (Canada, Egypt, Japan, Jordan, and Pakistan), were included in this meta-analysis. These studies evaluated the intraoperative application of HSI during FESS in adult patients undergoing the procedure for CRS. The included trials compared HSI (temperatures ranging from 42°C to 55°C) with room temperature saline irrigation (temperatures ranging from 18°C to 25°C), with primary focus on intraoperative outcomes such as bleeding control, blood loss, surgical duration, and hemodynamic stability. Figure 1 shows a PRISMA flowchart of the screening process. Finally, 6 RCTs and 1 nonrandomized clinical trial were selected that fulfilled the selection criteria completely.4 -7,29 -31
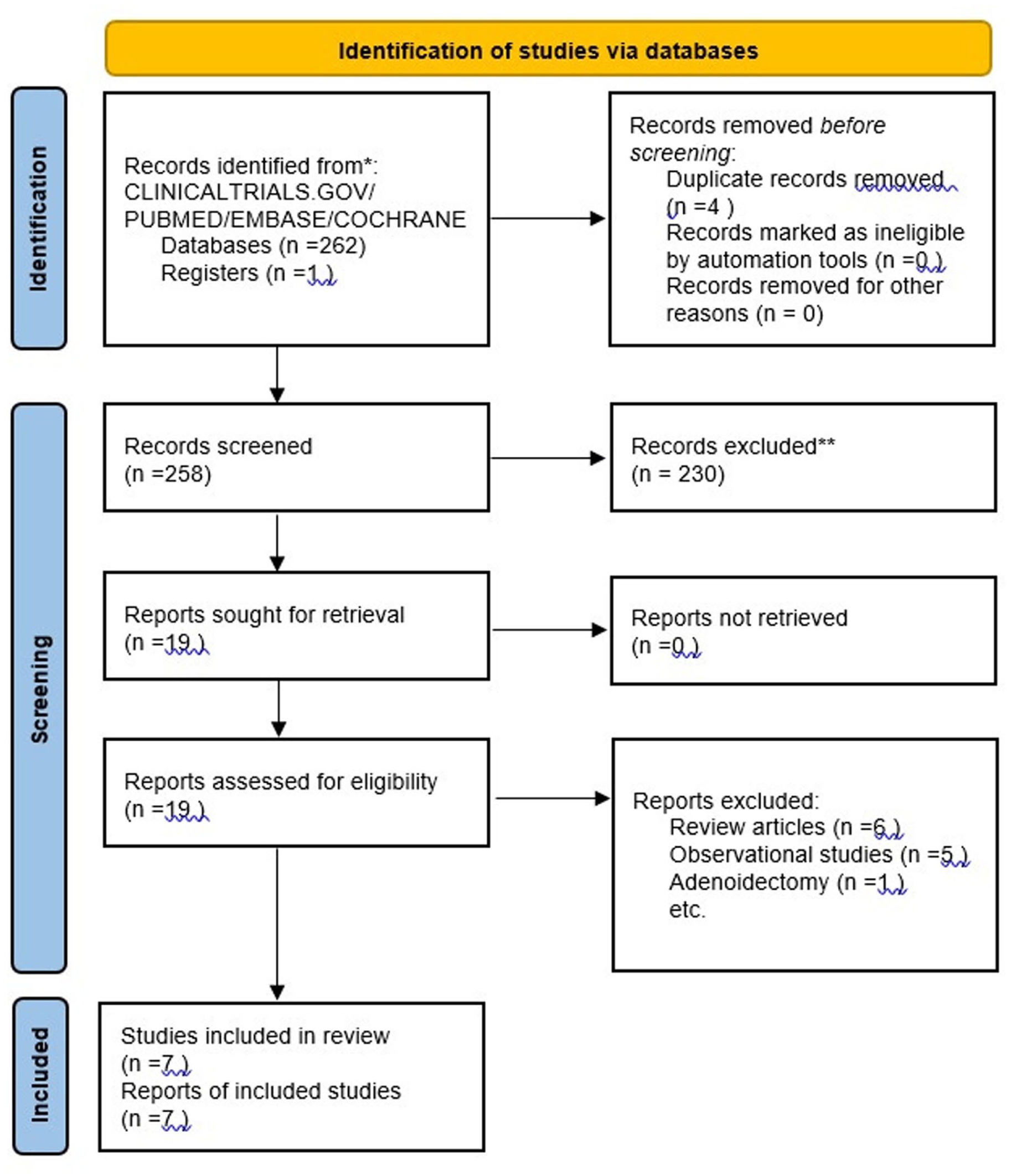
Flowchart illustrating the study selection process according to the PRISMA 2020 guidelines. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The sample sizes varied significantly, with participant numbers per group ranging from 6 to 50, a mean male percentage of 61.3%, and an overall mean age of 41.1 ± 12.7 years. The population characteristics are presented in Table 1.
Study Characteristics Table.
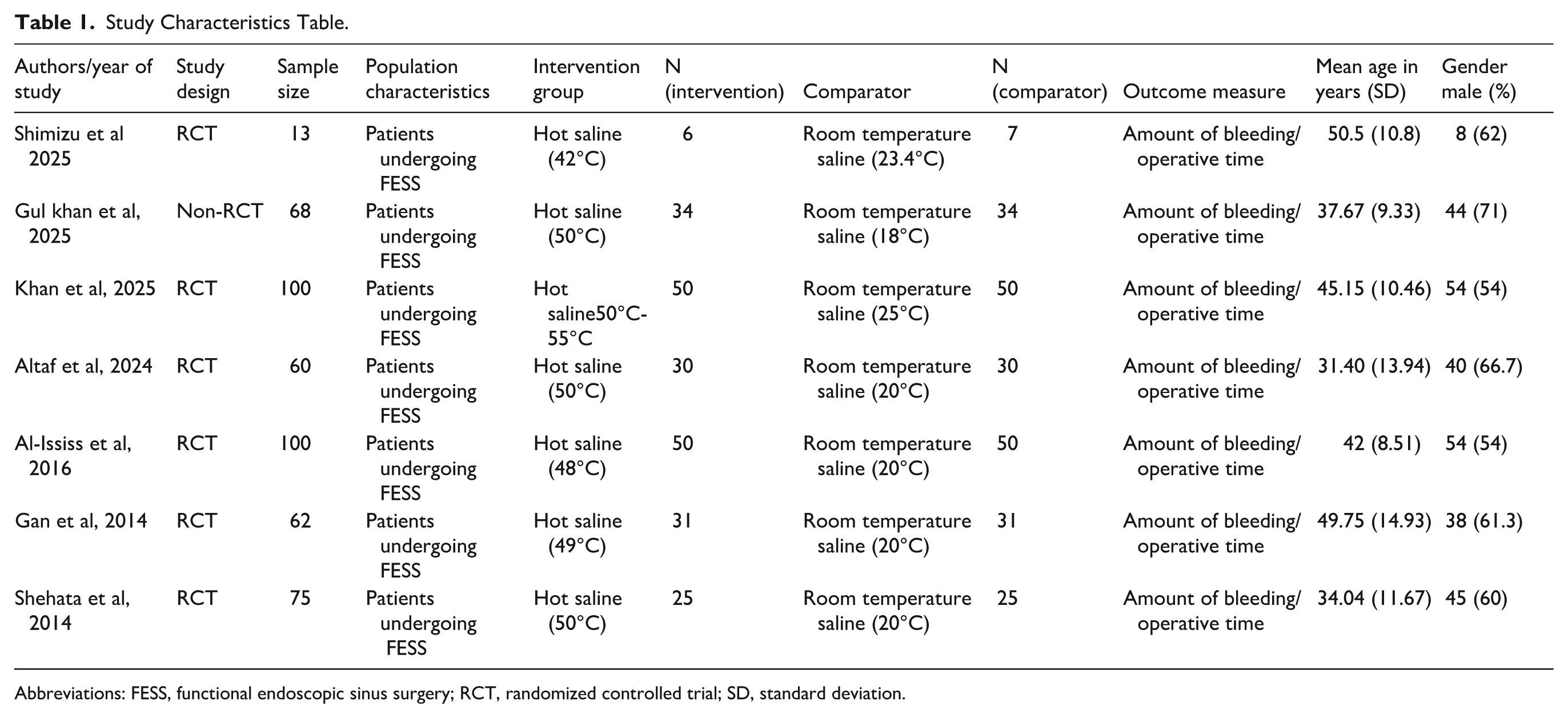
Abbreviations: FESS, functional endoscopic sinus surgery; RCT, randomized controlled trial; SD, standard deviation.
Traffic Light Plot for RoB Analysis
Most studies were assessed as having a low risk of bias across all the domains, except for Shimizu et al which showed a high risk. Details of the RoB analysis are shown in Supplemental Material.
Outcomes
Boezaart Intraoperative Bleeding Score
Six studies involving 347 patients reported the Boezaart intraoperative bleeding score. Meta-analysis demonstrated that HSI significantly improved the surgical field compared with room temperature saline, with a pooled MD of −0.68 (95% CI: −1.01 to −0.34). Heterogeneity was high (I2 = 79.7%), indicating variability in operative conditions across studies (Figure 2).
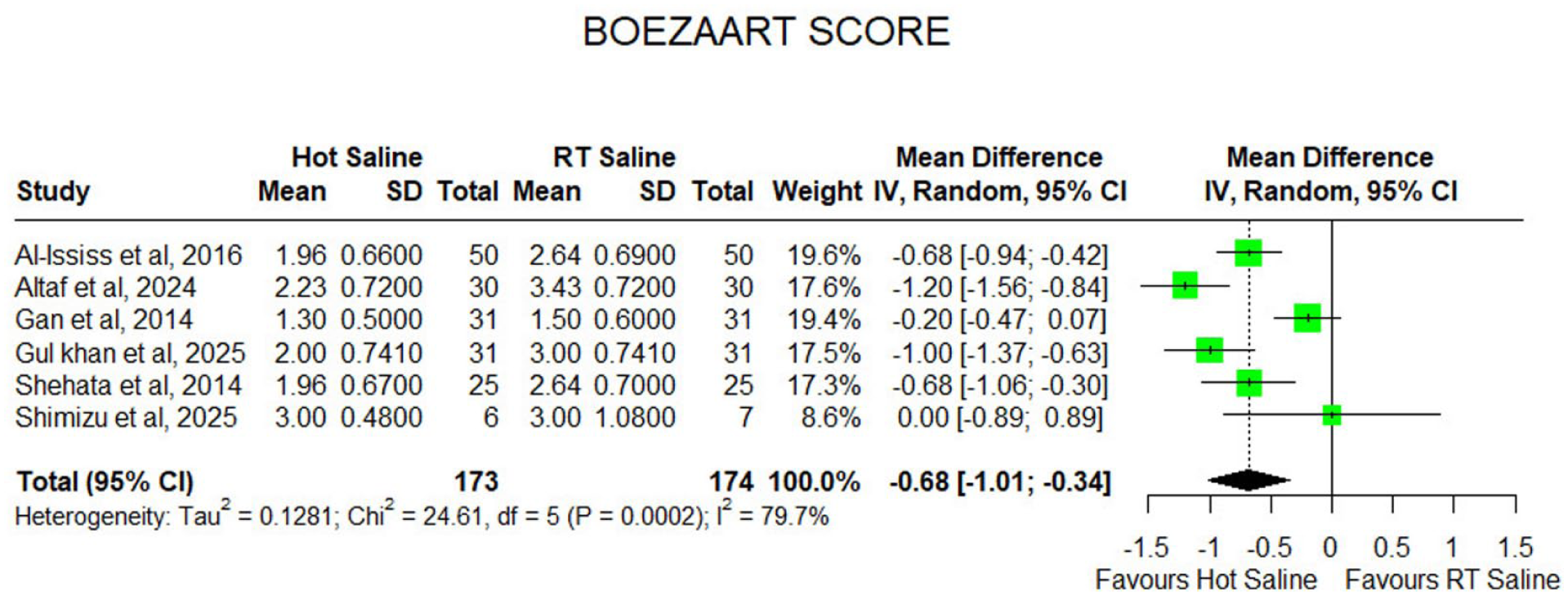
Forest plot of Boezaart bleeding score comparing hot saline irrigation versus room temperature saline in endoscopic sinus surgery.
Intraoperative Blood Loss
Six studies involving 434 patients (217 per group) reported the mean intraoperative blood loss. Using a random-effects model, HIS was associated with a marked reduction in blood loss, yielding a pooled MD of −56.33 mL (95% CI: −57.22 to −55.44). This large effect consistently favored HIS across the included trials. Moderate heterogeneity was observed (I2 = 37.1%), likely reflecting differences in temperature protocols, surgical technique, and intraoperative measurement methods (Figure 3).
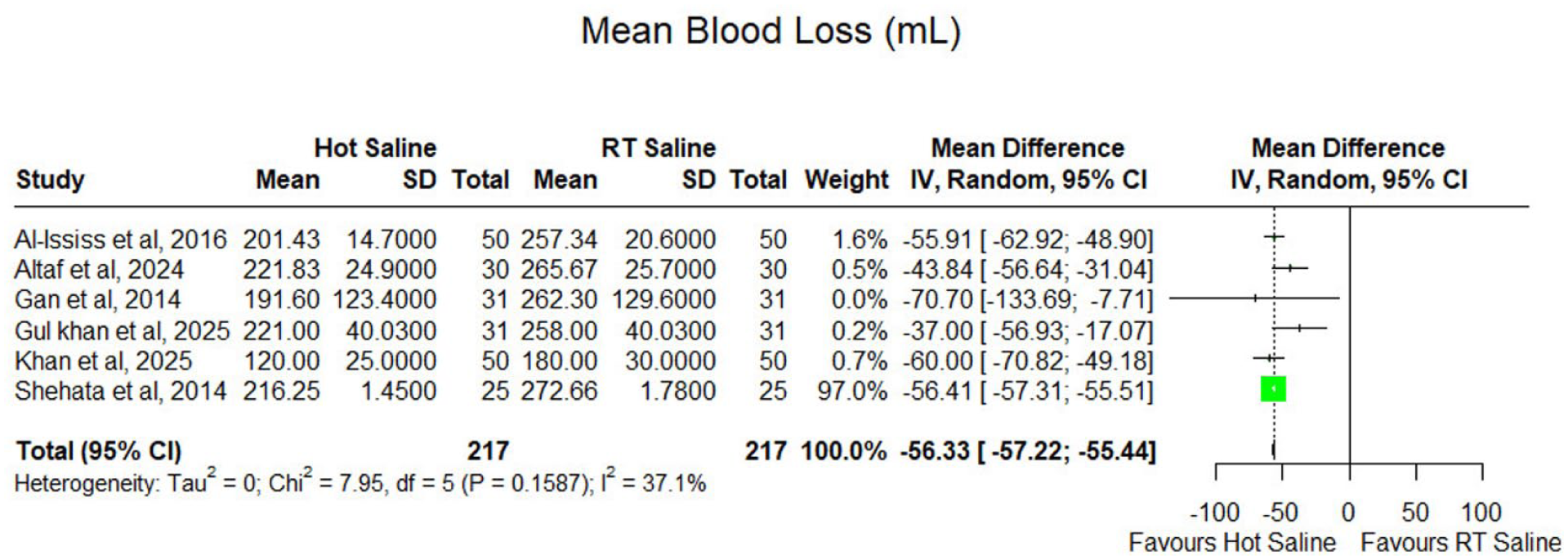
Forest plot of intraoperative blood loss (mL) comparing hot saline irrigation versus room temperature saline in endoscopic sinus surgery.
Duration of Surgery
Seven studies with 447 patients reported operative time. A random-effects model demonstrated that HSI significantly shortened the duration of surgery compared with room temperature saline, with a pooled MD of −9.78 minutes (95% CI: −14.62 to −4.94). Although heterogeneity was considerable (I2 = 85%), the direction of effect was uniform across nearly all studies, suggesting that HSI enhances surgical efficiency during ESS (Figure 4).
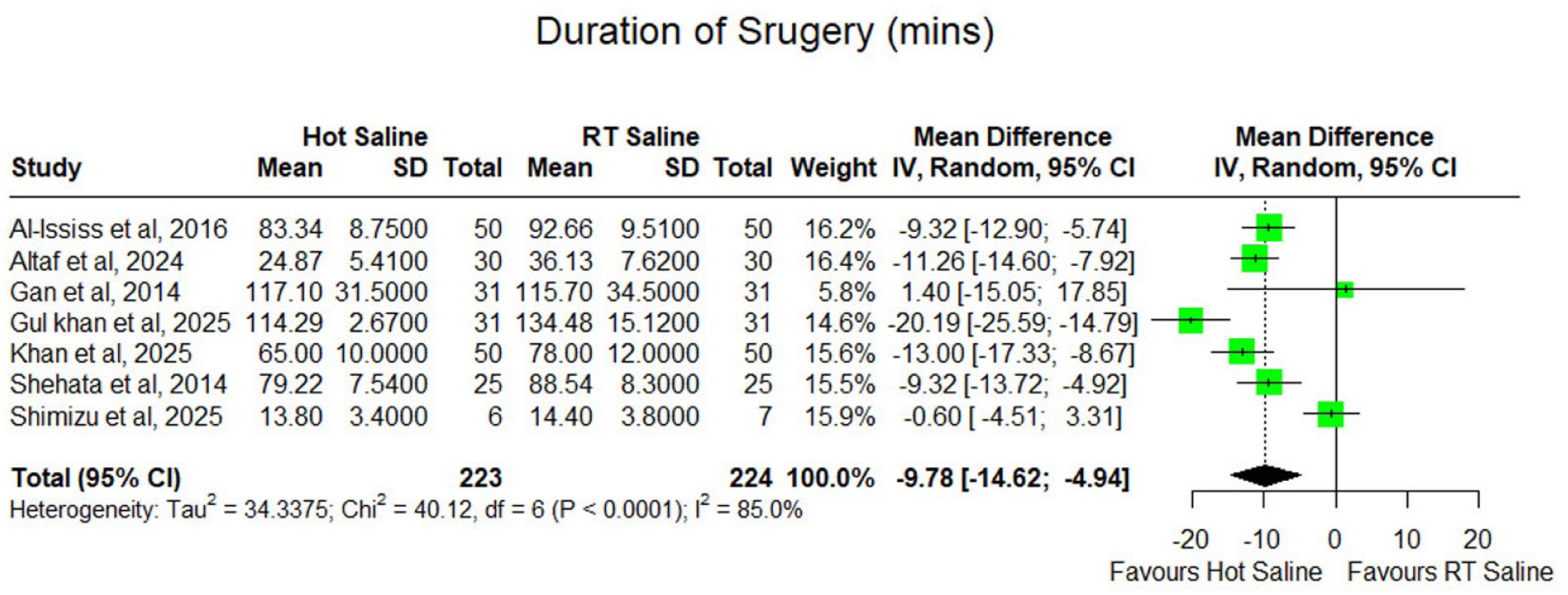
Forest plot of duration of surgery (minutes) comparing hot saline irrigation versus room temperature saline in endoscopic sinus surgery.
Mean Arterial Pressure
Three studies, including 212 patients (106 per group), assessed intraoperative MAP. Meta-analysis using a random-effects model showed no significant difference between HIS and room temperature saline irrigation, with a pooled MD of −0.68 mmHg (95% CI: −2.22 to 0.86). Heterogeneity was negligible (I2 = 0.4%), indicating consistent findings across studies. These results suggest that HSI does not affect intraoperative hemodynamic stability (Figure 5).
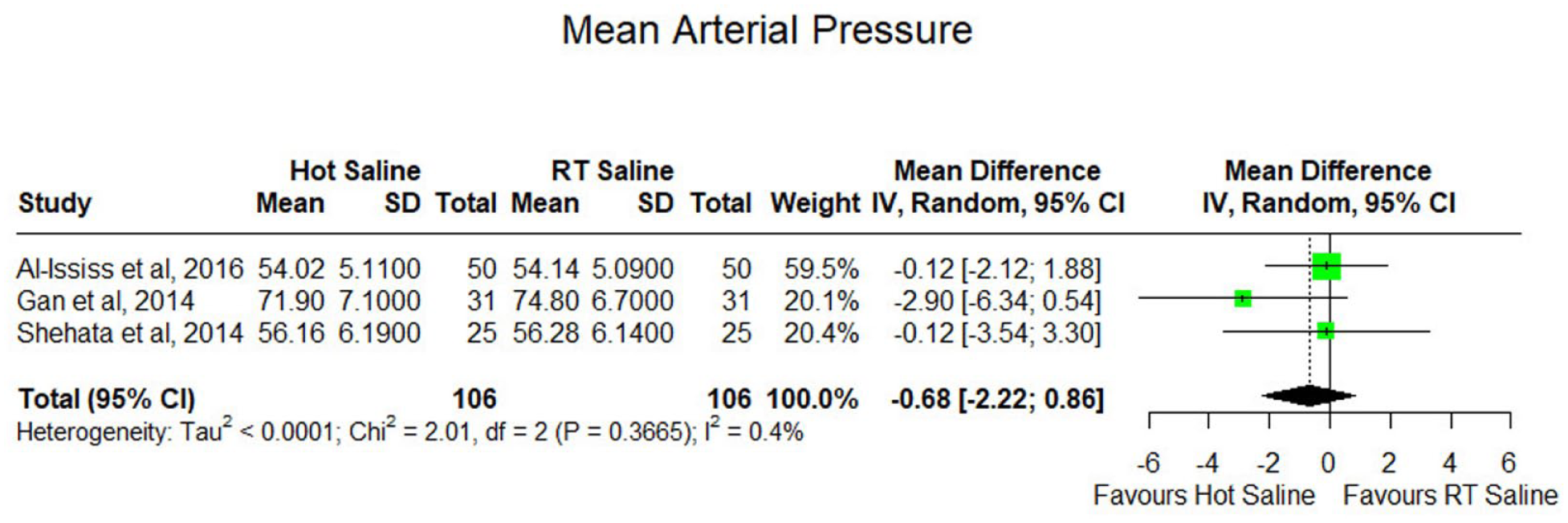
Forest plot of mean arterial pressure (mmHg) comparing hot saline irrigation versus room temperature saline in endoscopic sinus surgery.
Sensitivity Analysis
Sensitivity analysis using a leave-one-out approach demonstrated that the overall findings of this meta-analysis were robust across all outcomes. For the Boezaart score, sequential omission of individual studies did not materially alter the pooled effect (MD = −0.6613; 95% CI −0.8019 to −0.5207; τ2 = 0.1281), indicating stable improvement in intraoperative visualization with HSI (Supplemental Figure 2). Similarly, for the duration of surgery, the effect size remained consistent upon exclusion of each study (MD = −9.6748 minutes; 95% CI −11.3064 to −8.0432; τ2 = 34.3375), confirming a reliable reduction in operative time (Supplemental Figure 3). The blood loss outcome showed exceptionally high stability, with no change in between-study variance (τ2 = 0) and a consistent pooled effect (MD = −56.3303 mL; 95% CI −57.2168 to −55.4438; Supplemental Figure 4). Overall, the leave-one-out analysis confirmed that no single RCT disproportionately influenced the results, supporting the robustness and reliability of the observed benefits of HSI during FESS.
GRADE Summary of Findings
The certainty of evidence supporting the efficacy of HSI in ESS was assessed using the GRADE approach (Table 2). Overall, the evidence is of low to moderate certainty. For the primary outcome of improved surgical field visibility (Boezaart bleeding scores), the certainty is low due to serious concerns regarding risk of bias and inconsistency (high heterogeneity, I2 = 79.7%). Intraoperative blood loss and MAP outcomes are supported by moderate certainty evidence, primarily downgraded for risk of bias. Operative duration also rates as low certainty, reflecting both risk of bias and inconsistency (I2 = 85.0%). These ratings indicate that while HSI demonstrates consistent benefits, further high-quality randomized trials are warranted to increase confidence in the estimates.
GRADE Summary of Findings for Key Outcomes.
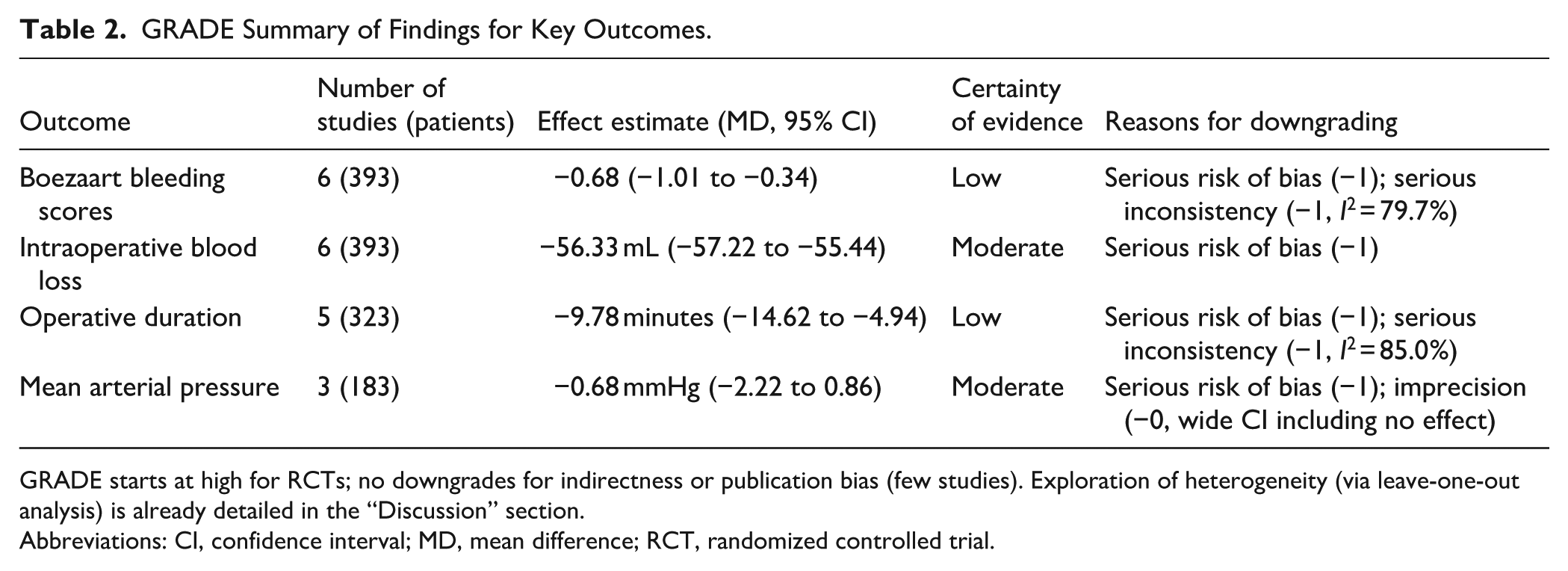
GRADE starts at high for RCTs; no downgrades for indirectness or publication bias (few studies). Exploration of heterogeneity (via leave-one-out analysis) is already detailed in the “Discussion” section.
Abbreviations: CI, confidence interval; MD, mean difference; RCT, randomized controlled trial.
Discussion
This meta-analysis brings together current evidence on the use of HSI during FESS and shows that it consistently improves intraoperative visualization, decreases blood loss, and reduces overall operative time. These findings are important for modern endoscopic practice, as the quality of the surgical field continues to be one of the main factors that influences the difficulty of the procedure, the safety of anatomical dissection, and the surgeon’s ability to maintain an efficient workflow. Two prior systematic reviews have examined HSI in ESS,1,3 each including only 3 studies.3,5 -7,21 The current review, with searches up to 30 October 2025, includes 7 studies (n = 453 patients) and incorporates 4 recent trials.4,29 -31 This provides a larger dataset, broader temperature range (42°C-55°C), and enhanced analysis of heterogeneity via sensitivity testing, yielding a more comprehensive and updated synthesis.
The reduction in blood loss observed in this review aligns closely with the magnitude of effect reported in earlier systematic evaluations of heated irrigation for hemostasis in ESS.3,21 The pooled reduction of 56.33 mL is also similar to the effect sizes documented for tranexamic acid (TXA) in recent high-level evidence syntheses, where TXA has been shown to decrease intraoperative bleeding by roughly 60 to 70 mL and improve the field quality to a similar degree.32,33 The relatively narrow confidence interval reflects consistent measurement approaches across the included studies, where blood loss was primarily quantified by suction canister volume minus irrigation fluid used, with adjustments for gauze where applicable. Minor variations existed in exact methodologies (e.g., some studies incorporated hemovac drainage), but no evidence of systematic bias was identified upon review. In a clinical context, a reduction of approximately 56 mL represents a meaningful decrease, contributing to improved visualization and reduced need for additional hemostatic measures without introducing substantial real-world variability beyond that captured in the controlled trial settings. This suggests that HSI may provide a degree of bleeding control that is broadly comparable to that achieved with antifibrinolytic medication. Trials evaluating topical TXA further support the principle that local interventions applied directly to the nasal mucosa can meaningfully enhance the operative field, although the timing and magnitude of improvement may differ between thermal and pharmacological methods.5,34
The consistent improvement in the Boezaart score across included trials strengthens the validity of the findings. The Boezaart scale and related structured endoscopic grading systems are established, reproducible tools for the assessment of intraoperative field quality and have been validated in multicenter work and anesthetic field studies.35,36 The use of these recognized scoring systems across trials increases confidence that the improvements seen with HSI reflect genuine clinical benefit rather than subjective interpretation.
The observed reduction in operative time is likely a result of several factors that accompany better visualization. Surgeons are able to progress through the procedure with fewer interruptions for suctioning, improved exposure of key anatomical landmarks, and less need for reactive hemostatic measures. These relationships between anesthetic conditions, field clarity, and operative efficiency are well documented in the ESS literature, where both anesthetic regimen and the use of controlled hypotension can independently influence visibility and workflow.24,36 The presence of such variability across studies may explain some of the heterogeneity seen in the pooled effects.
The physiological basis for the hemostatic effect of heated saline is supported by earlier experimental and clinical observations. Controlled thermal exposure reduces capillary oozing, promotes local coagulation, and decreases mucosal edema, which together contribute to a clearer surgical field. Clinical studies evaluating heated irrigations in postoperative care and in the management of refractory posterior epistaxis have reported good tolerance without evidence of delayed mucosal healing or other adverse effects, which supports the safety profile of this approach in the short term.25,37 These findings are relevant because, although hot saline lacks the systemic effects seen with pharmacologic agents, its use must also be shown to be safe for mucosal tissue. Available evidence suggests that it meets this standard.
Substantial heterogeneity was observed in Boezaart bleeding scores (I2 = 79.7%) and operative time (I2 = 85.0%). Potential sources include variations in hot saline temperatures (42°C-55°C across studies), surgical techniques, and patient baseline characteristics. Leave-one-out sensitivity analysis confirmed the robustness of findings, with no omission altering the direction or significance of pooled estimates (P < .0001 for all iterations). For Boezaart scores, heterogeneity ranged from I2 = 59.9% to 83.7% upon individual exclusions, with the lowest I2 (59.9%) achieved by omitting Gan et al. 6 For operative time, heterogeneity ranged from I2 = 67.0% to 87.5%, with the lowest I2 (67.0%) upon omitting Shimizu et al, which used the lowest temperature (42°C) and a split-body design. 31 Subgroup analysis by temperature was not feasible due to limited studies per stratum; however, consistent benefits across protocols support the efficacy of HSI.
The present review extends the findings of earlier analyses by incorporating recent randomized trials, which provide updated estimates drawn from diverse surgical settings and irrigation temperatures. The consistency of benefit across these more recent trials reinforces the generalizability of the effect. Despite this, several limitations should be considered. The number of eligible randomized studies remains limited, and sample sizes in some trials are modest. Temperature protocols (ranging from 42°C to 55°C), anesthetic approaches, and irrigation techniques vary between centers, which may influence both surgical field scores and operative duration, contributing to the observed heterogeneity in Boezaart scores (I2 = 79.7%) and operative time (I2 = 85.0%). Reporting of adverse events, postoperative bleeding, and mucosal changes was inconsistent, preventing a reliable pooled assessment of safety outcomes. One included study (Shimizu et al) was assessed as having a high risk of bias, primarily due to its within-person (split-body) design, which may introduce potential carry-over effects or challenges in blinding despite randomization. 31 This study contributed to outcomes exhibiting substantial heterogeneity, particularly Boezaart bleeding scores (I2 = 79.7%) and operative time (I2 = 85.0%). This study, utilizing the lowest irrigation temperature (42°C), contributed to heterogeneity. However, sensitivity analysis excluding this study failed to alter the significance or direction of the pooled estimates, indicating the robustness of the primary findings. Overall, these limitations highlight the need for well-designed future trials with standardized irrigation protocols, controlled anesthetic variables, and longer follow-up to evaluate mucosal recovery and postoperative complications.
Conclusion
Overall, the findings of this meta-analysis indicate that HSI is a low-cost, widely accessible, and easy-to-implement method that improves bleeding control during ESS. Its effect size is similar to that of established agents such as TXA, and it avoids the systemic effects associated with pharmacologic and hypotensive strategies. These characteristics make HSI a practical adjunct in a wide range of surgical contexts, including those where pharmacologic therapies are contraindicated or where limited resources constrain intraoperative options. Continued research that directly compares HSI with TXA and with other established hemostatic strategies would be valuable and would help further clarify its role within contemporary FESS practice.
Supplemental Material
sj-docx-1-ear-10.1177_01455613261423742 – Supplemental material for Hot Saline Irrigation for Improving Surgical Field Visibility in Endoscopic Sinus Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613261423742 for Hot Saline Irrigation for Improving Surgical Field Visibility in Endoscopic Sinus Surgery: A Systematic Review and Meta-Analysis by Abdur Rehman, Shahzaib Maqbool, Muhammad Ibrahim, Taha Iftikhar, Rahmat Gul Omarzai and Sadia Chaudhry in Ear, Nose & Throat Journal
Footnotes
Author Contributions
A.R.: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Writing – original draft.
S.M.: Conceptualization, Writing – original draft, Writing – review and editing.
M.I.: Writing – original draft, Writing – review & editing.
T.I.: Formal analysis, Data curation.
R.G.O.: Investigation, Writing – original draft.
S.C.: Supervision, Writing – review & editing.
All authors have read and agreed to the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
This review only used previously published data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.