
Abstract
We report a case of cervical upper digestive tract reconstruction using a laryngotracheal flap following resection of hypopharyngeal carcinoma. A 53-year-old man presented with a 1-year history of dysphagia accompanied by a persistent sensation of obstruction. Gastroscopy revealed a cauliflower-like mass involving the right pyriform sinus and postcricoid region, extending to the esophageal inlet. Histopathological examination of biopsy specimens confirmed squamous cell carcinoma. Reconstruction of the surgical defect was achieved by anastomosing the hypopharynx to the cervical esophagus using the preserved larynx and the first 3 tracheal rings. This approach allowed circumferential reconstruction of the defect with the laryngeal cavity and a segment of the cervical trachea. At 46 months of follow-up, the patient was able to maintain oral intake without restriction, and no evidence of tumor recurrence was observed.
Keywords
Introduction
Data from the Global Burden of Disease study indicate that the age-standardized incidence rate of head and neck malignancies is approximately 21.3 per 100 000 population. 1 Hypopharyngeal carcinoma accounts for nearly 15% of all head and neck squamous cell carcinomas and is characterized by a high propensity for lymph node metastasis, invasion of adjacent neurovascular structures, and distant spread. Consequently, the reported 5-year overall survival rate remains poor, ranging from 25% to 45%. 2 Most patients are diagnosed at a locally advanced stage, typically presenting with symptoms such as dysphagia or pain. Approximately 10% of patients are found to have synchronous second primary tumors involving the upper digestive tract, lung, or trachea at the time of diagnosis. 3 Both the natural course of the disease and its treatment can profoundly affect critical functions, including respiration, phonation, swallowing, and immune competence. Moreover, tumor stage, baseline physical condition, comorbidities, and patient preferences further complicate clinical decision-making. In the present case, radical resection for hypopharyngeal carcinoma was followed by reconstruction of a circumferential defect in the cervical upper digestive tract using the larynx and a segment of the cervical trachea. This technique represents a novel reconstructive option for patients with hypopharyngeal carcinoma who are not suitable candidates for laryngeal preservation.
Case Presentation
The patient was a 53-year-old man who presented with a 1-year history of a sensation of obstruction and discomfort during swallowing. Flexible electronic laryngoscopy revealed a cauliflower-like mass involving the right pyriform sinus and postcricoid region of the hypopharynx. Histopathological examination of biopsy specimens demonstrated moderately differentiated squamous cell carcinoma. Contrast-enhanced computed tomography showed that the lesion extended from the right pyriform sinus posteriorly to the contralateral posterior pharyngeal wall (Figure 1). Gastroscopy confirmed involvement of the esophageal inlet, with no evidence of neoplastic lesions in the esophagus or stomach. The tumor was diagnosed as hypopharyngeal squamous cell carcinoma and staged as T3N0M0. After obtaining informed consent, the patient underwent radical resection of the hypopharyngeal carcinoma, followed by reconstruction of the upper digestive tract defect using a total laryngeal and partial cervical tracheal anastomosis.
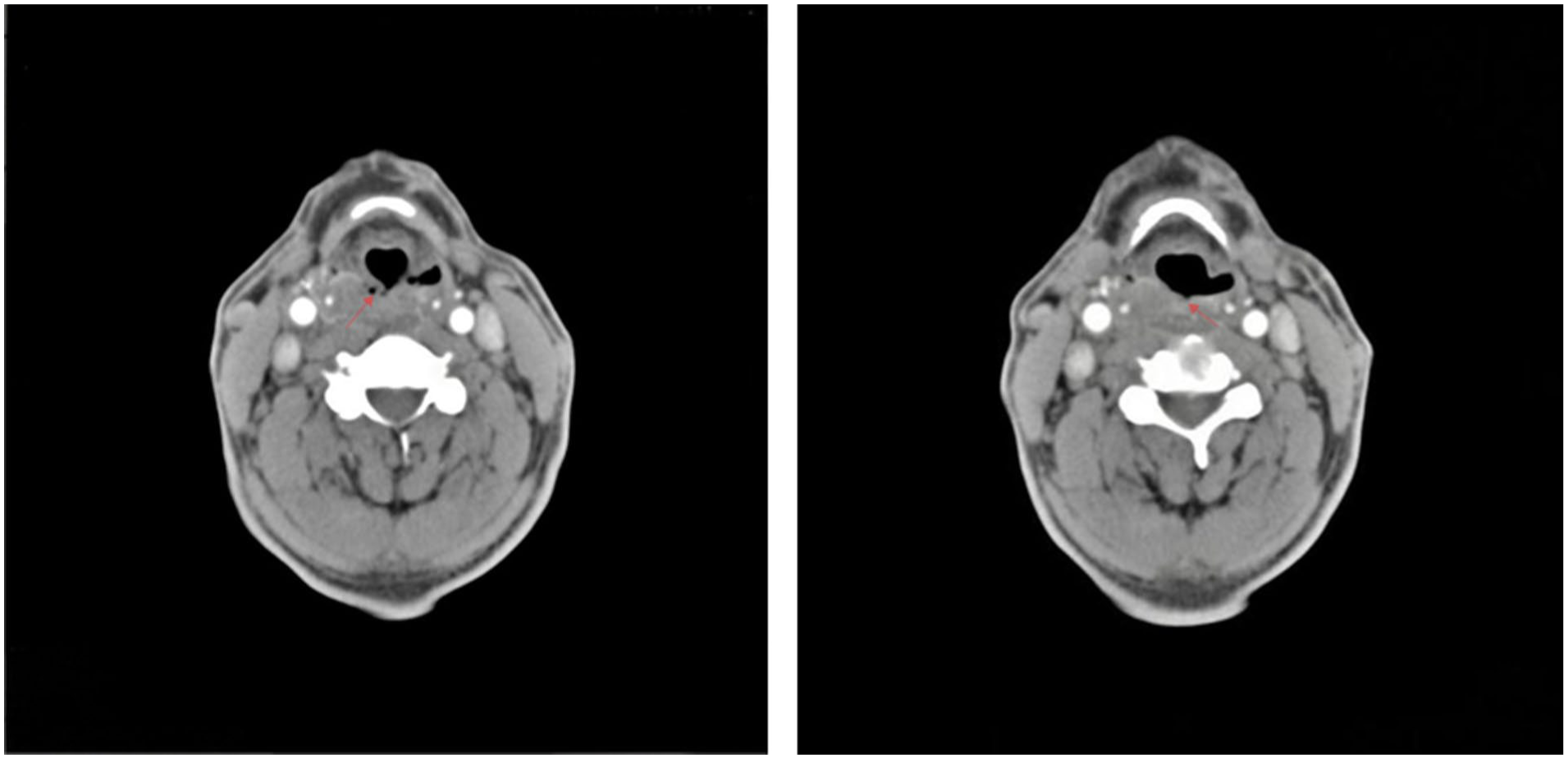
A lesion in the right pyriform sinus is shown on laryngeal contrast-enhanced CT, extending to the contralateral (left) posterior pharyngeal wall (arrows). CT, computed tomography.
Intraoperatively, the hypopharyngeal constrictor muscles were dissected, and the right hyoid bone together with the lateral portion of the thyroid cartilage lamina was resected. The tumor was located in the right hypopharynx, extending superiorly to the inferior pole of the right tonsil and inferiorly to the esophageal inlet. Anteriorly, it extensively involved the postcricoid region and, posteriorly, crossed the midline of the posterior pharyngeal wall to invade the left hypopharynx, while the laryngeal mucosa remained intact. Following tumor resection with a 2-cm safety margin, a circumferential defect of the upper digestive tract was created. Both superior laryngeal nerves and recurrent laryngeal nerves were identified and transected. The trachea was divided between the third and fourth tracheal rings, and the esophageal stump was adequately mobilized. The third tracheal ring was anastomosed to the mobilized esophageal stump, and the hypopharyngeal mucosal margin was sutured to the postcricoid mucosa of the laryngeal remnant. Reconstruction of the upper digestive tract was achieved using the entire larynx in continuity with a segment of the cervical trachea, and a permanent tracheostomy was established (Figure 2). Histopathological examination confirmed negative surgical margins in all specimens. Postoperatively, the patient received nasogastric tube feeding for 2 weeks, after which oral intake was initiated. A liquid diet was maintained for 2 months before gradual progression to a regular diet, with eventual restoration of normal swallowing function.
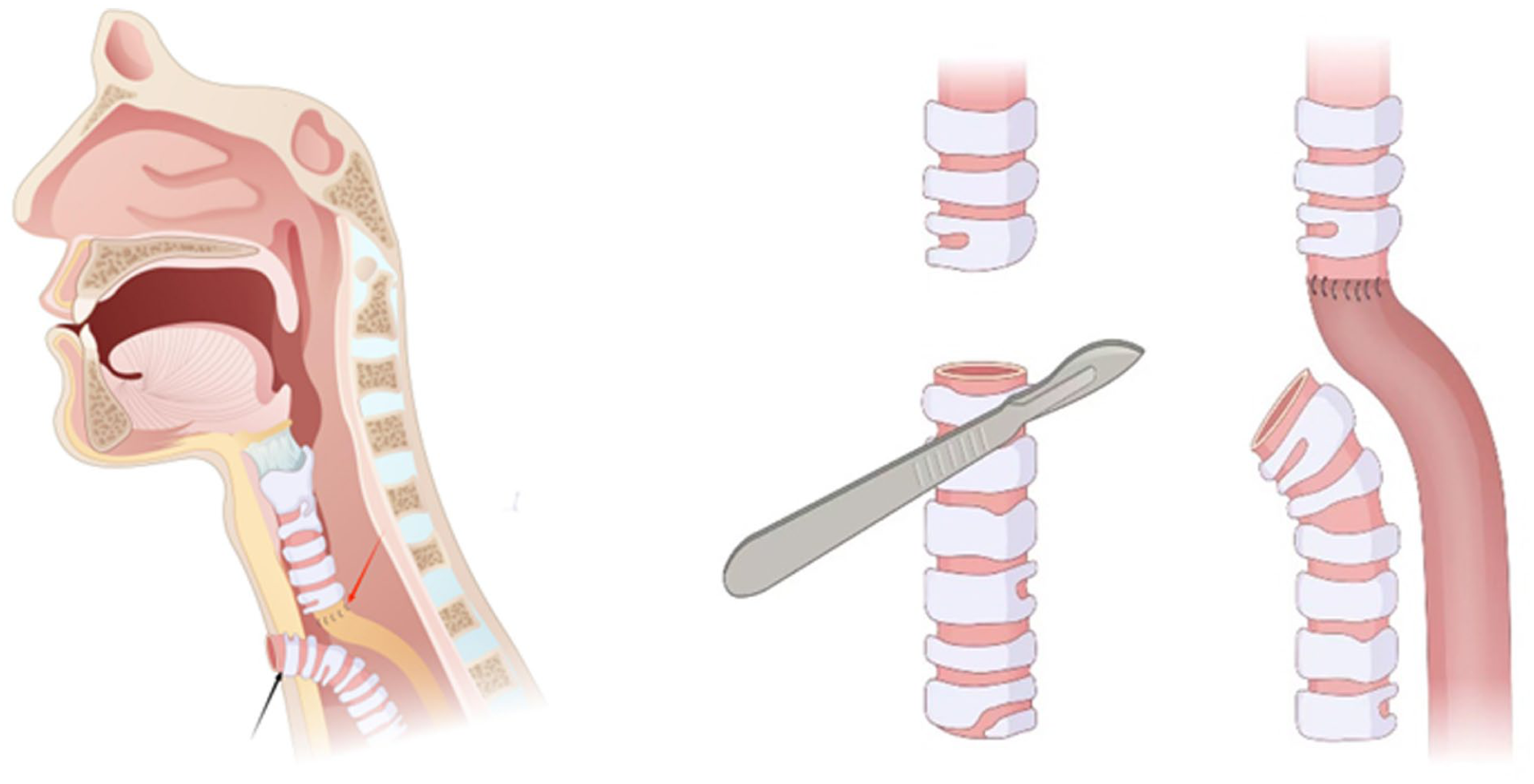
Schematic diagram illustrating reconstruction of the alimentary tract using the total larynx and a segment of the cervical trachea. The red arrow indicates the anastomosis and reconstructed conduit; the black arrow indicates the direction of the permanent tracheostomy.
At 46 months postoperatively, air-insufflated flexible laryngoscopy demonstrated bilateral vocal cord fixation, with the laryngeal cavity mucosa exhibiting a digestive tract-like epithelial transformation. The hypopharyngeal mucosa had healed well in continuity with the laryngeal mucosa (Figure 3), and the upper digestive tract showed satisfactory healing without evidence of tumor recurrence (Figure 4). A barium swallow study confirmed patency of the esophagus. Following esophageal speech training, the patient achieved satisfactory daily verbal communication.
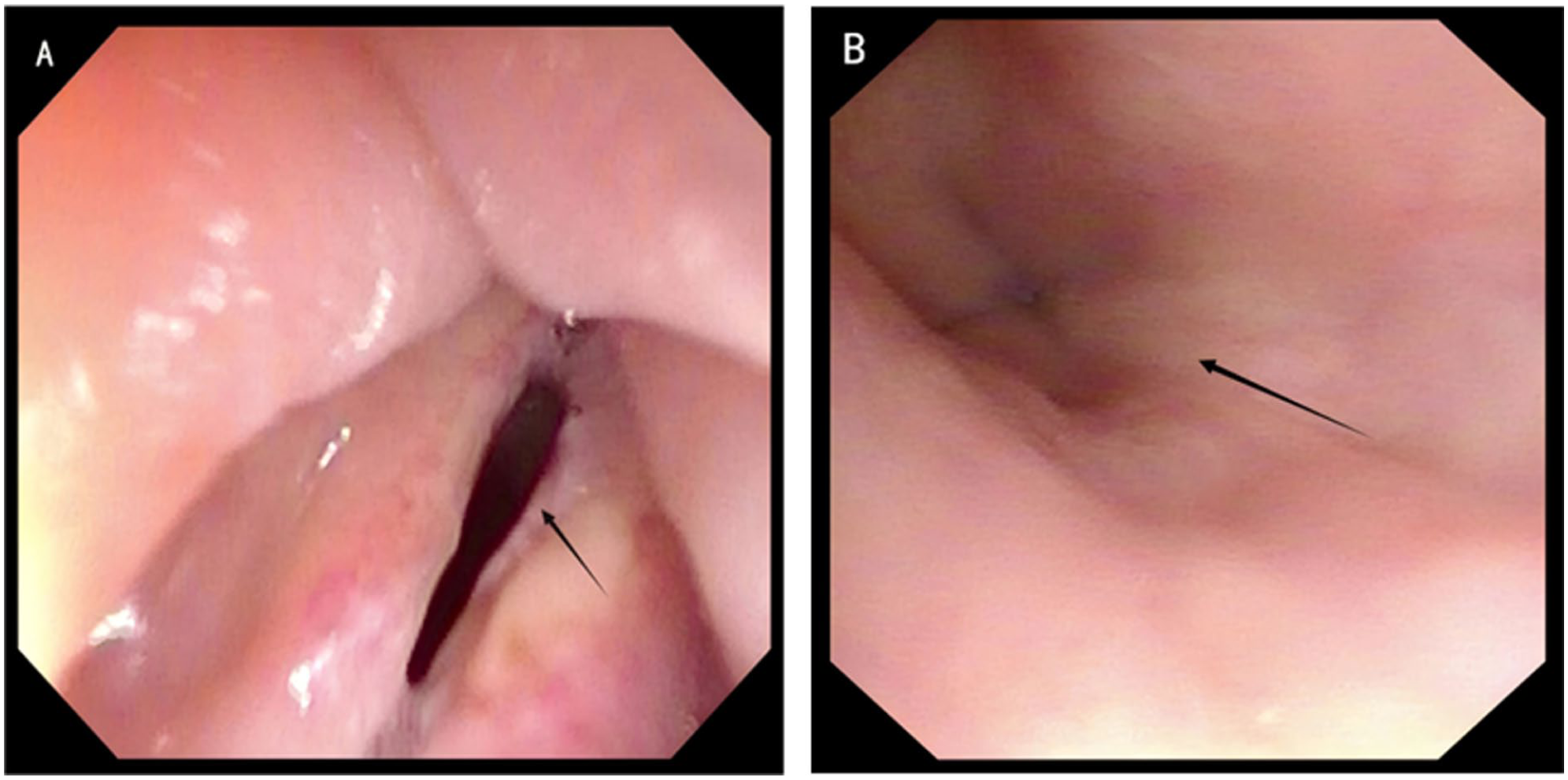
Air-insufflated flexible laryngoscopy showing the laryngo-tracheo-esophageal alimentary tract at 46 months postoperatively. (A) Laryngeal cavity mucosa; the arrow indicates the vocal cord. (B) Subglottic, tracheal, and upper esophageal mucosa; the arrow indicates the esophageal mucosa.
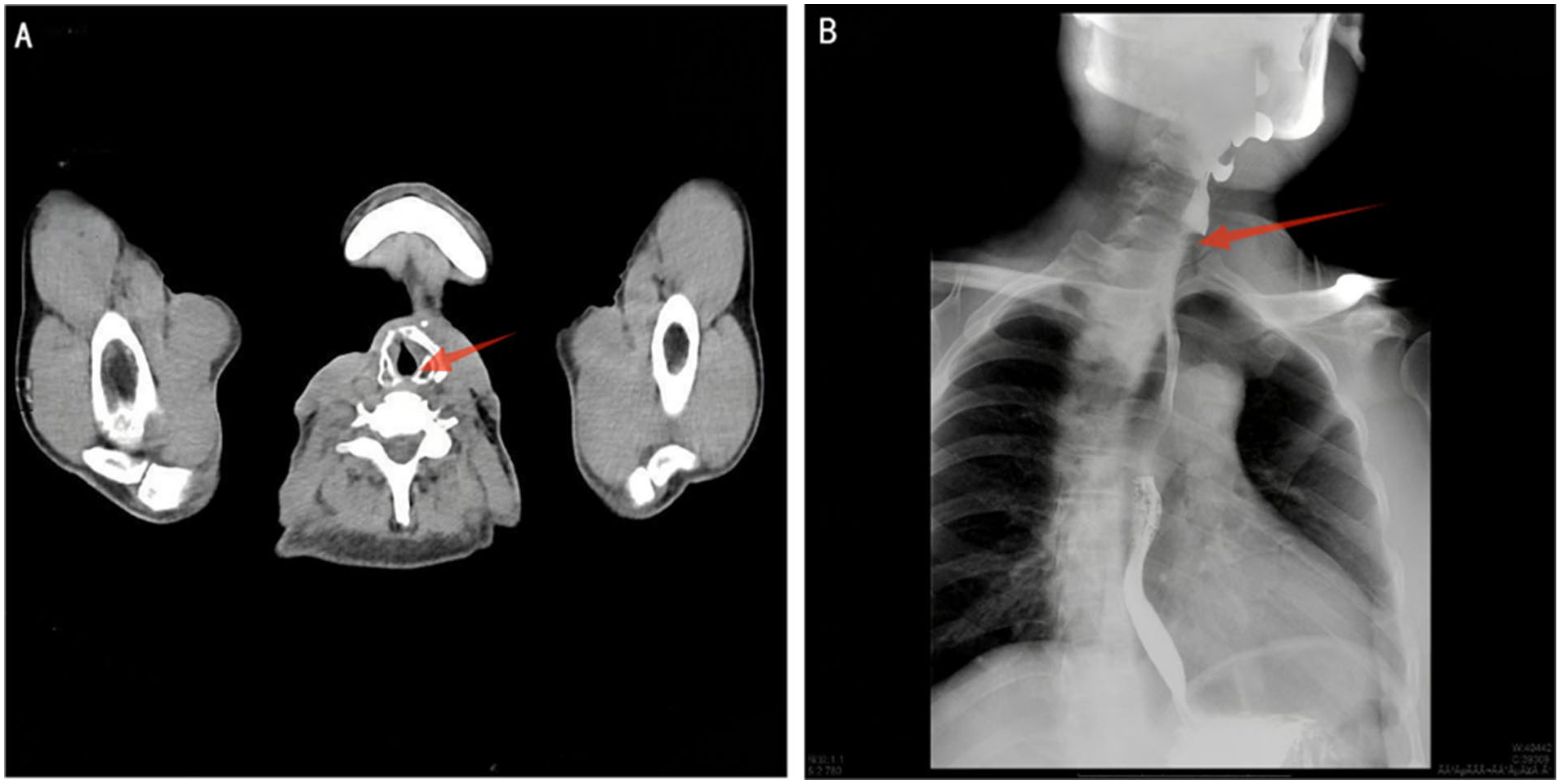
Postoperative imaging of the reconstructed upper alimentary tract (larynx–trachea–esophagus). (A) CT image at the laryngeal level showing the reconstructed conduit (arrows). (B) Barium swallow study demonstrating free passage of contrast through the reconstructed conduit (arrows). CT, computed tomography.
Discussion
Surgical intervention should be considered and discussed for all patients with hypopharyngeal carcinoma; however, radical procedures inevitably impair, and may even abolish, critical physiological functions such as speech, swallowing, and respiration. For patients with T1 tumors and selected T2 tumors without cervical lymph node metastasis, tumor resection with laryngeal preservation represents a feasible treatment option. In contrast, patients with more advanced disease defined as T1 tumors with nodal metastasis or T2-T3 tumors generally require laryngopharyngectomy followed by reconstruction of the surgical defect, with adjuvant radiotherapy and/or chemotherapy administered according to pathological findings. 4
In this case, radical resection for hypopharyngeal carcinoma was followed by reconstruction of the oral alimentary conduit using the physiological laryngeal framework in continuity with a segment of the cervical esophagus. This approach offers an alternative reconstructive strategy aimed at preserving oral intake in selected patients undergoing radical surgery for hypopharyngeal carcinoma.
Following resection of hypopharyngeal carcinoma, small local defects can often be closed primarily through mobilization and direct approximation of adjacent tissues. For larger but noncircumferential defects, regional pedicled flaps such as the pectoralis major myocutaneous flap, 5 supraclavicular artery island flap, 6 and submental flap 7 are commonly employed. These techniques are associated with relatively limited surgical trauma and faster postoperative recovery, making them suitable for partial defect reconstruction. In contrast, reconstruction of circumferential defects after hypopharyngeal resection remains particularly challenging. Commonly used approaches include free jejunal transfer, pedicled colonic interposition, and gastric pull-up with pharyngogastric anastomosis. 8 The free jejunal flap is well suited for circumferential reconstruction of the cervical esophagus because of its structural and luminal similarity; however, mismatch between the jejunal segment and the pharyngeal lumen may result in excessive tension at the proximal anastomosis, thereby increasing the risk of anastomotic leakage. 9 Tubed pedicled or free flaps are also associated with complications such as luminal stenosis and pharyngocutaneous fistula, which limits their widespread clinical application. 10 Notably, all of these reconstructive methods require concomitant total laryngectomy. The technique described in the present report utilizes the preserved larynx in continuity with a segment of the cervical trachea to reconstruct the circumferential defect. Potential advantages of this approach include technical simplicity, avoidance of the extensive trauma and complications associated with combined visceral reconstruction, reduced operative time, and more rapid postoperative recovery.
In this case, resection of the malignant tumor resulted in a circumferential defect of the cervical upper alimentary tract. The trachea was divided between the third and fourth tracheal rings, with the superior tracheal stump anastomosed to the esophageal stump and the inferior stump used to create a permanent cervical stoma. When laryngeal preservation is not feasible, this approach utilizing the larynx in continuity with a segment of the cervical trachea effectively restores alimentary tract continuity while preserving oral intake function. The patient subsequently received adjuvant chemoradiotherapy. At 46 months of follow-up, the patient maintained satisfactory oral feeding, with no evidence of complications or tumor recurrence.
Conclusion
This case provides a novel surgical option for reconstructing circumferential cervical upper alimentary tract defects following radical surgery for hypopharyngeal carcinoma where laryngeal preservation is not possible.
Footnotes
Acknowledgements
We would like to express our gratitude to the patient and his family for their cooperation and consent.
Ethical Considerations
Ethical approval to report this case was obtained from the Ethics Committee/Institutional Review Board of Linyi People’s Hospital Affiliated to Shandong Second Medical University, Linyi, China (approval no. 202403-H-007) on March 22, 2024. Written informed consent for publication of the patient’s clinical details and any accompanying images was obtained from the patient.
Consent to Participate
We obtained written informed consent from the patient to publish this case report. The study was carried out in accordance with the principles of the Declaration of Helsinki
Consent for Publication
Written informed consent for publication of the patient’s clinical details and any accompanying images was obtained from the patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this case report are included in this published article. Additional de-identified data are available from the corresponding author upon reasonable request, subject to patient privacy and ethical restrictions.