
Abstract
Background:
Radiofrequency ablation (RFA) is a mucosal-sparing, in-office technique for inferior turbinate hypertrophy (ITH) with favorable short-term outcomes. Data regarding the efficacy of revision RFA in patients with treatment failure are limited.
Objectives:
To identify predictors of RFA failure requiring revision and to evaluate the safety and efficacy of revision RFA.
Methods:
A retrospective cohort study was conducted, including patients with ITH who underwent RFA between 2016 and 2023 at a tertiary referral center. Patients requiring revision treatment were identified and compared with those who did not require revision.
Results:
The cohort included 260 patients (66.9% male; age range, 18-88 years). Thirty-three patients (12.7%) required revision treatment, of whom 24 (9.2%) underwent revision RFA. No post-revision RFA complications were observed. The overall revision rates were higher among older patients (P = .015), patients with medical comorbidities (P < .001), and those with middle turbinate hypertrophy (P = .047). Short-term revision (<6 months) was more common among patients with diabetes (P < .001) and obstructive sleep apnea (OSA; P = .012), while revision in the long term (<24 months) was associated with diabetes (P < .001), hypertension (P = .019), and rhinitis medicamentosa (P = .045). On multivariate Cox proportional hazards analysis, diabetes mellitus, OSA, and rhinitis medicamentosa were independently associated with an increased risk of revision for both short and long term.
Conclusions:
Revision RFA is a safe and effective treatment option for selected patients with recurrent nasal obstruction due to ITH. Higher revision rates were observed in older patients and those with medical comorbidities and rhinitis medicamentosa. Revision RFA should be considered as a conservative second-line treatment in appropriately selected patients.
Key Points
- Revision RFA of the inferior turbinate was a safe and effective procedure, with high patient satisfaction and no major complications.
- Patients with medical comorbidities, older age, and rhinitis medicamentosa had higher revision rates.
- Medical comorbidities predictors for revision RFA may vary between patients, necessitating long-term to short-term revision: The short-term (<6 months) revision rates were higher among patients with obstructive sleep apnea, whereas revision rates in the medium follow-up period (<24 months) were higher among patients with hypertension.
- Patients with diabetes mellitus and rhinitis medicamentosa had higher revision rates, necessitating both short- and long-term revision.
- We recommend that revision RFA for inferior turbinate volume be considered as part of a more conservative approach to patients with nasal obstruction failing primary RFA.
Introduction
Nasal obstruction is common in the rhinology clinic, with nasal airflow disturbances reported in up to 30% of patients.1 -3 It significantly impairs quality of life (QOL) and daily functioning.4,5 Inferior turbinate hypertrophy (ITH) is a leading cause of nasal obstruction, and failure of conservative topical therapy is an indication for surgical intervention.
Radiofrequency ablation (RFA) is a wave-based technology that induces submucosal tissue contraction and fibrosis and is widely used to reduce inferior turbinate volume.
Its main advantage is mucosal preservation, achieved by delivering controlled radiofrequency energy to the submucosal tissue while maintaining low energy levels and precise direction.5 -10 RFA is a quick, safe procedure with minimal morbidity, can be performed in-office under local anesthesia, and does not require postoperative nasal packing, allowing for an easier recovery.6 -8
Alternative surgical techniques for ITH, including turbinectomy, submucosal turbinate resection, laser-assisted turbinoplasty, cryotherapy, and chemical, electrical, or diathermic coagulation, are effective but generally non-mucosa-sparing. 6 These procedures are associated with increased morbidity, such as pain, bleeding, crusting, synechiae, and hyposmia, and often require postoperative nasal packing, which may cause patient discomfort.
Patient satisfaction following RFA is generally high, with multiple studies demonstrating short-term improvement in nasal obstruction and QOL using validated questionnaires such as SNOT-22 and NOSE. However, RFA failure and long-term outcomes are less well defined, with symptom recurrence often reported within 1 to 2 years.4,11 Patients with recurrent symptoms are frequently referred for surgical intervention, likely to address both mucosal and bony components of nasal obstruction.12,13
This study aimed to identify predictive factors for RFA failure and the need for revision treatment, and to evaluate the efficacy and safety of revision RFA. Defining these factors may improve clinical decision-making and expand second-line treatment options for patients reluctant to undergo more extensive surgical procedures.
Materials and Methods
Study Design and Patient Sample
In this retrospective cohort study, consenting patients were assessed for their suitability as candidates for RFA as first-line treatment. The study was approved by the Institutional Review Board (0367-18). We enrolled patients with nasal airway obstruction due to ITH who underwent an RFA procedure between March 2016 and May 2023. All of the patients underwent a physical examination that included anterior rhinoscopy and nasal cavity evaluation with flexible endoscopy. All procedures, including revisions and follow-up, were performed by a single fellowship-trained rhinology specialist, with 15 years of practice, in an urban tertiary referral center. Data collected from the patients’ medical charts consisted of their general medical history and comorbidities, smoking habits, as well as their presenting nasal symptoms, prior procedures, medical treatment, imaging findings, procedure description, postoperative course, and subjective improvement. Data on the length of time for symptom recurrence and subsequent procedures (revision RFA, septoplasty and inferior turbinectomy, and functional endoscopic sinus surgery) were retrieved for patients who required revisions. The data were reported via Strengthening the Reporting of Observational Studies in Epidemiology Statement guidelines for reporting observational studies. 14
The inclusion criteria were individuals aged >16 years, able to provide informed consent. Excluded were patients who were unable to complete their RFA procedure in-office under local anesthesia (due to significant pain despite local anesthetics, discomfort, and anxiety), patients who did not adhere to follow-up (including in-office and telephonic follow-up), and patients who refused to participate in the study (Figure 1). Patients with clinical features deemed unsuitable for RFA (such as sinus disease, severe septal deviation, 15 etc.) were managed with alternative treatment strategies and were therefore not referred for RFA. These features included significant nasal-related history (eg, nasal cavity tumor resection), medical history of diagnosed rhinosinusitis or a high index of clinical suspicion for rhinosinusitis, very anterior or severe degree of septal deviation, pregnancy, the presence of major nasal valve disorder, nonremovable electronic devices affected by the radiofrequency waves, and contraindication or inability to tolerate local anesthesia. The study cohort, therefore, represents patients who were clinically selected for RFA rather than all patients presenting with ITH.
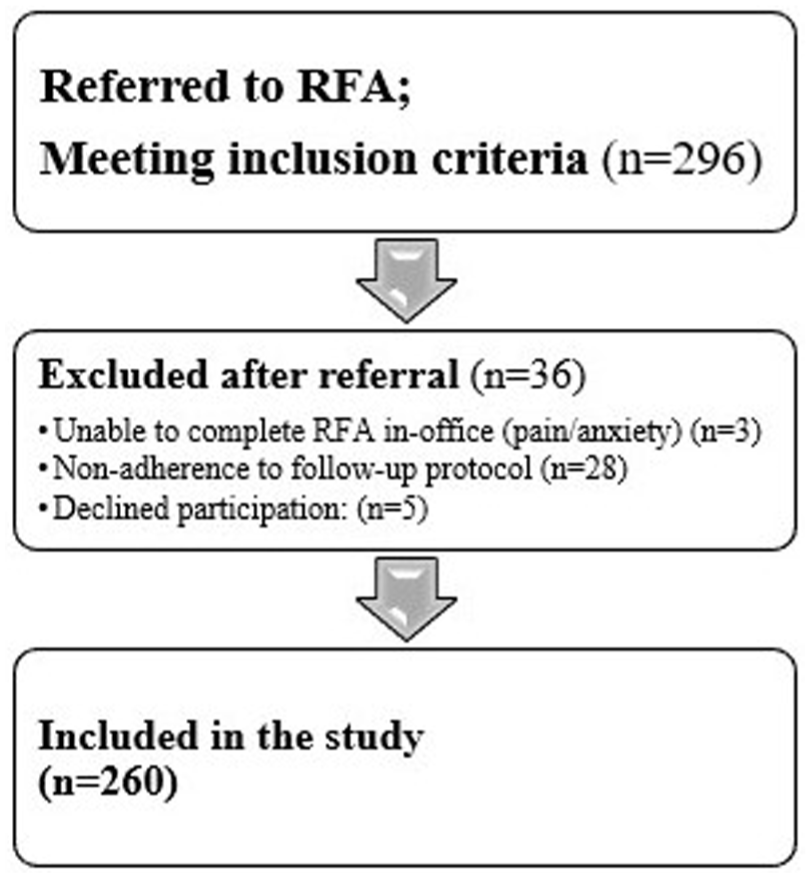
Flow chart diagram of patient selection, exclusion, and inclusion in the study cohort. RFA, radiofrequency ablation.
The study participants were followed in the outpatient clinic from initial presentation following surgical intervention, and those who reported being dissatisfied with the initial procedure were reevaluated in our clinic. Failure of primary RFA was defined as recurrent or persistent nasal obstruction that was found to be necessitated the pursuit of an additional intervention, including revision RFA or surgical treatment, in a shared decision. A revision RFA was offered to the patients with isolated nasal obstruction due to persistent ITH following a minimum of 6 months of follow-up from the initial procedure, while personalized treatment was tailored according to physical examination findings for the other patients. All revision procedures were discussed with the patient, and a joint patient-physician decision was made, taking into account patient characteristics, medical comorbidities, American Society of Anesthesiologists scores, and general surgical risk. Patients who underwent revision procedures were compared for the presence of various parameters to those who did not require further intervention. Those parameters included medical comorbidities, symptoms, physical examination, medical treatment, prior rhinoseptoplasty with or without turbinectomy, and prior imaging findings. Patients were followed up in the outpatient clinic 2 to 6 months post-procedure and then continued telephonically follow-up addressing QOL questionnaires, subjective improvement, cessation of nasal decongestants, and need for further evaluation in the outpatient clinic. Patients who were unsatisfied with the results of the procedure were re-assessed in our outpatient clinic as needed. Those who were satisfied with the procedure continued telephonic follow-up upon patient request.
Surgical Technique
Local anesthesia was carried out by placing a cotton pledget soaked with tetracaine 2% solution with oxymetazoline (1:1) in the middle and inferior meatus for 15 to 20 minutes. Then, 5 cc of 2% lidocaine was injected bilaterally into the inferior turbinates under endoscopic vision. The turbinate reduction was carried out with a bipolar radiofrequency electrode (Aftmost 15 W automated mode) by creating 4 to 5 lesions along the inferior turbinate bilaterally. Lateralization of the turbinates was performed when needed. Revision RFA was performed in a similar manner. Following the procedure, patients performed high-flow nasal rinses with saline 0.9% per nostril. Rinses with a bottle or syringe to squirt the solution into the nose were begun 1 to 2 days after surgery and carried out 3 to 4 times a day for 2 weeks, and then 1 to 2 times a day until the first postoperative clinic visit that took place 2 months after surgery.
Statistical Analysis
Categorical variables were summarized as frequency and percentage. Age distribution was evaluated with histograms. Since age was not normally distributed, it was reported as median and interquartile range (IQR). A reverse centering method was used to evaluate the length of the follow-up period. Kaplan-Meier curve and a Log-Rank test were used to study the association between categorical variables and revision event during the follow-up period, and patients were censored if either revision event occurred, they were lost to follow-up, or until the end of the study’s determined time period. Univariate Cox regression was used to study the association between age and revision event during the follow-up period. All of the statistical tests were 2-sided, and statistical significance was defined by a P value < .05.
A multivariate Cox regression was performed. Hypertension (HTN), diabetes mellitus, obstructive sleep apnea (OSA), and rhinitis medicamentosa were entered into the regression model. A backward method was applied using P > .1 in the Wald test as criteria for variable removal.
All statistical analyses were performed with SPSS software (IBM SPSS Statistics for Windows, version 28; IBM Corp, New York, USA, 2021).
Results
Study Population
A total of 260 patients (174 [66.9%] males and 86 [33.1%] females) met the inclusion criteria and participated in the study between March 2016 and May 2023. The cohort’s median age was 36.5 years (IQR: 26-57). The median length of follow-up was 29.3 months (IQR: 17-60). Data on demographics, medical comorbidities, symptoms, prior rhinoseptoplasty with or without turbinectomy, physical examination, prior radiological studies, and postoperative complications are provided in Table 1. The initial recommendation for all patients was to initiate conservative topical treatment with local steroid spray for 3 months. The beneficial value of conservative treatment was re-evaluated in the outpatient clinic after a 3-month trial.
Patient Characteristics (N = 260).
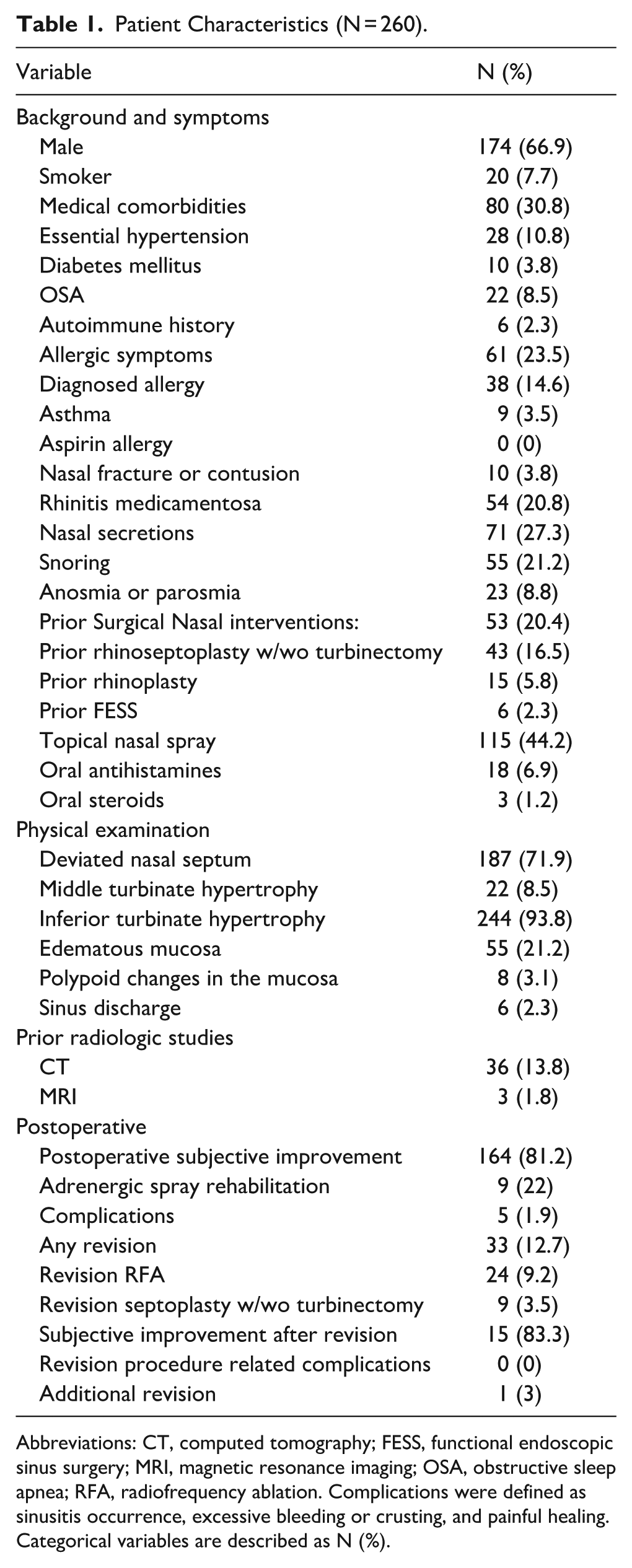
Abbreviations: CT, computed tomography; FESS, functional endoscopic sinus surgery; MRI, magnetic resonance imaging; OSA, obstructive sleep apnea; RFA, radiofrequency ablation. Complications were defined as sinusitis occurrence, excessive bleeding or crusting, and painful healing.
Categorical variables are described as N (%).
Fifty-four patients (20.8%) with rhinitis medicamentosa (RM) self-reported regular use of an adrenergic spray for alleviation of nasal obstruction symptoms. Physical examination findings at the initial evaluation revealed hypertrophied inferior turbinates in most patients (n = 244, 93.8%), while the inferior turbinates were not hypertrophied but contributed considerably to the nasal airway obstruction due to a very narrow nasal cavity in the remaining patients. Middle turbinate hypertrophy (MTH) was detected in far fewer patients (n = 22, 8.5%). All patients underwent RFA uneventfully.
Only 5 patients (1.9%) experienced complications following RFA. One patient reported severe local pain lasting for about 3 weeks, with a gradual resolution in pain over time with over-the-counter analgesics. The remaining 4 patients sustained excessive crusting, which resolved after several weeks of topical treatment with nasal douches and topical steroid spray.
Revision Rates and Revision Complications
A revision procedure was indicated in patients with recurrent or persistent symptoms of nasal obstruction following primary RFA treatment. Thirty-three patients (12.7%) underwent revision procedures, of whom 24 (9.2% of the entire cohort; 73% of patients who underwent revision procedures) underwent a revision RFA procedure. Only 1 patient who underwent revision RFA proceeded to septoplasty and turbinectomy due to unresolved symptoms. The remaining 9 patients (3.5%) proceeded to revision surgery under general anesthesia (septoplasty w/wo turbinectomy). No postoperative complications were noted following revision RFA procedures, and 31 patients (94%) who underwent revision procedures reported subjective improvement shortly thereafter.
Predictors for Requiring a Revision RFA
We investigated possible predictors for RFA failure and the need for revision procedures. It emerged that patients who underwent revision were older than those who did not (median age:49.0 [31.5-66.0] vs median 36.0 [25.0-55.0] years, respectively, P = .015). Revision rates were higher among patients with diabetes mellitus (DM), compared to those without DM (n = 4 [40%] vs n = 29 patients [18%], P < .001). Patients using oral steroids as a medical intervention for long-standing nasal obstruction had higher rates of revision (n = 2 [100%] vs n = 31 [18%], P = .002). Lastly, revision rates were higher among patients with MTH compared to those without MTH (n = 6 [36%] vs n = 27 [18%], P = .047). No further differences were identified in medical history (including smoking status and allergic symptoms), prior nasal surgical interventions, physical examination findings (including septal deviation), or radiologic findings (Table 2). In multivariate Cox proportional hazards regression analysis (see Table 3) followed by backward Wald elimination, diabetes mellitus remained independently associated with revision (hazard ratio [HR] 4.36, 95% confidence interval [CI] 1.40-13.45, P = .010), while age showed a trend toward significance (HR 1.02, 95% CI 1.00-1.037, P = .06).
Comparing Revision Rates Among Patients with versus those without Clinical Parameters (N = 260).
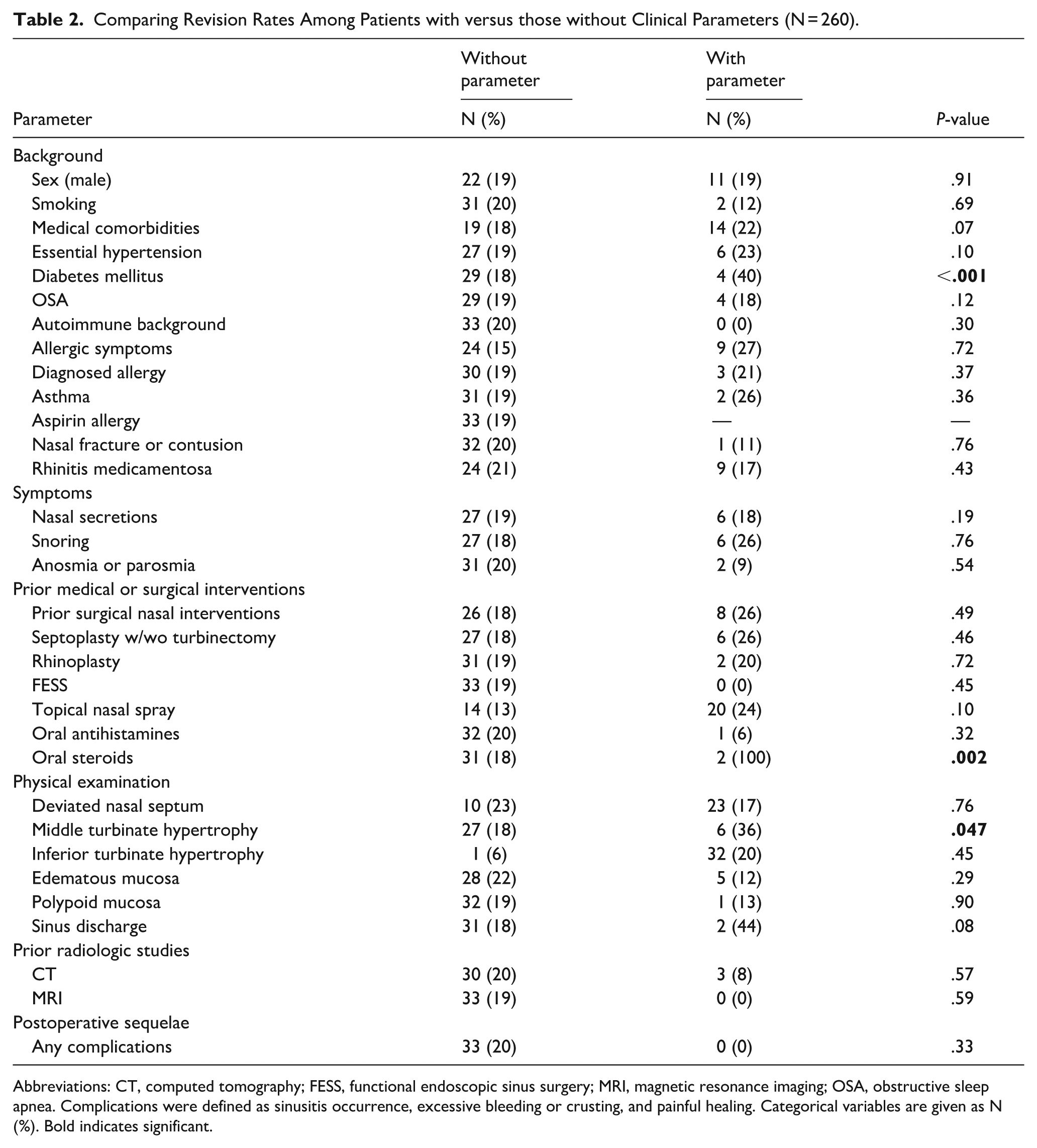
Abbreviations: CT, computed tomography; FESS, functional endoscopic sinus surgery; MRI, magnetic resonance imaging; OSA, obstructive sleep apnea. Complications were defined as sinusitis occurrence, excessive bleeding or crusting, and painful healing. Categorical variables are given as N (%). Bold indicates significant.
Multivariable Cox Regression for Comorbidities – Overall.
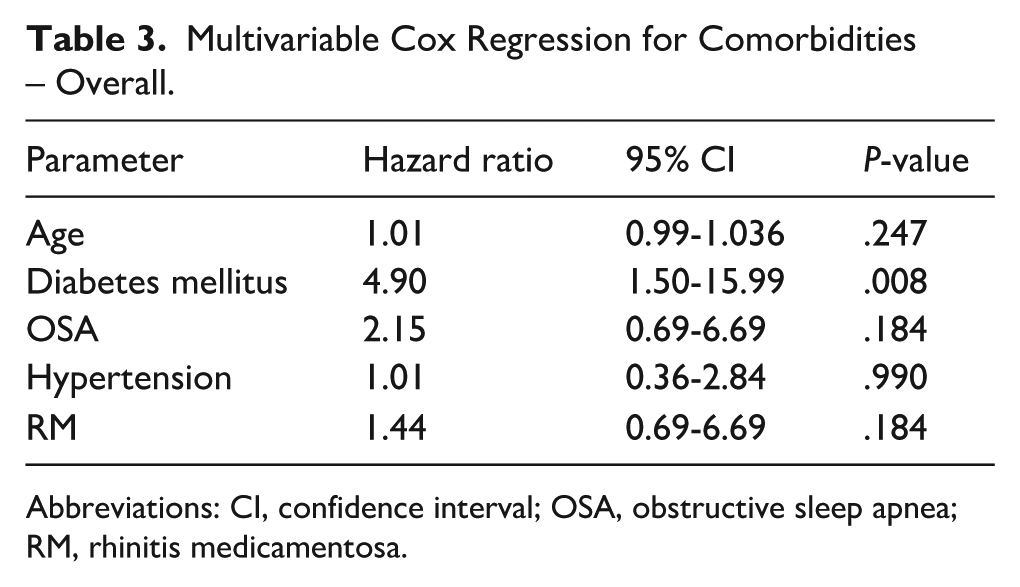
Abbreviations: CI, confidence interval; OSA, obstructive sleep apnea; RM, rhinitis medicamentosa.
Predictors for Requiring Revision in the Short Term (<6 Months)
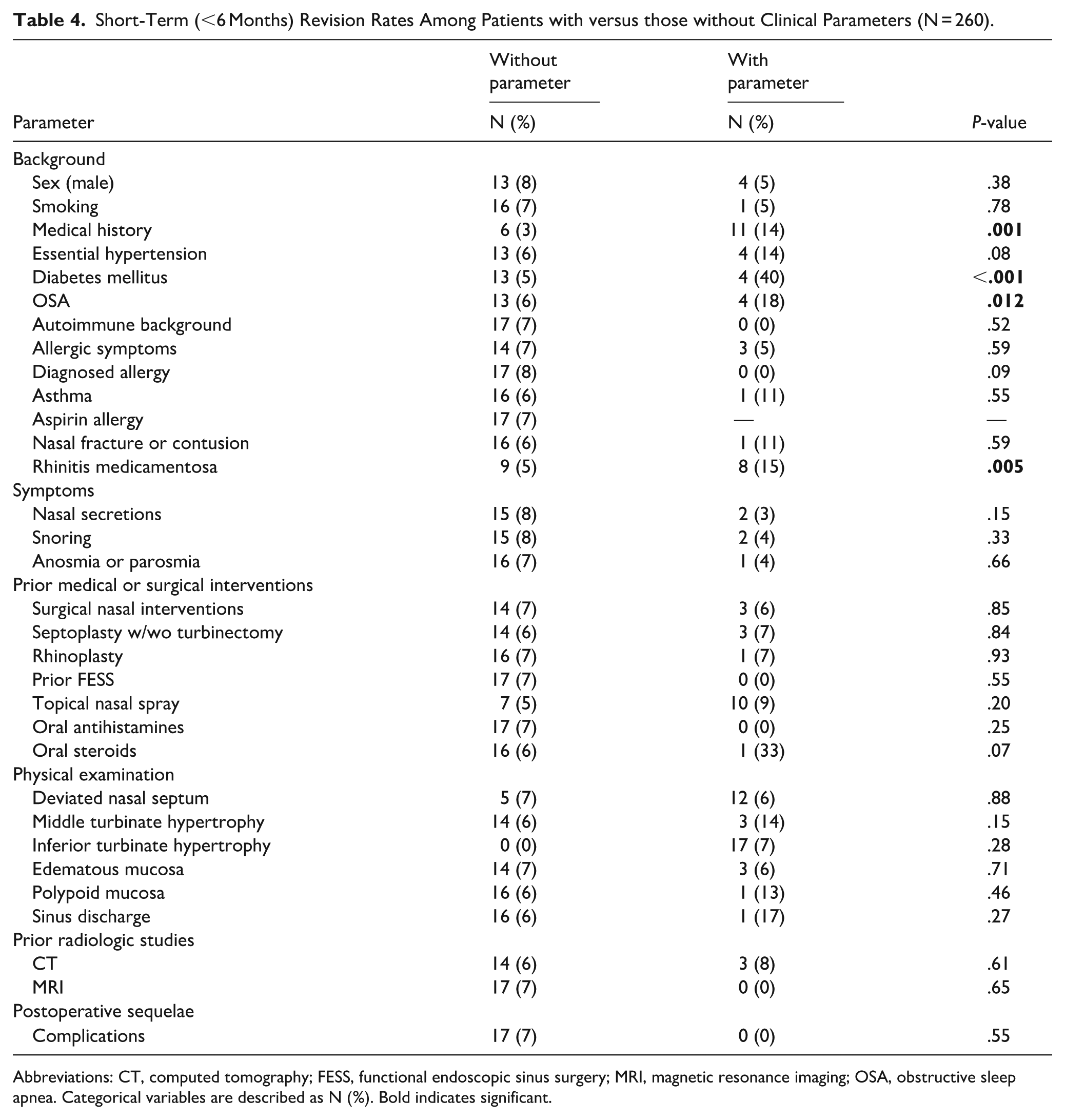
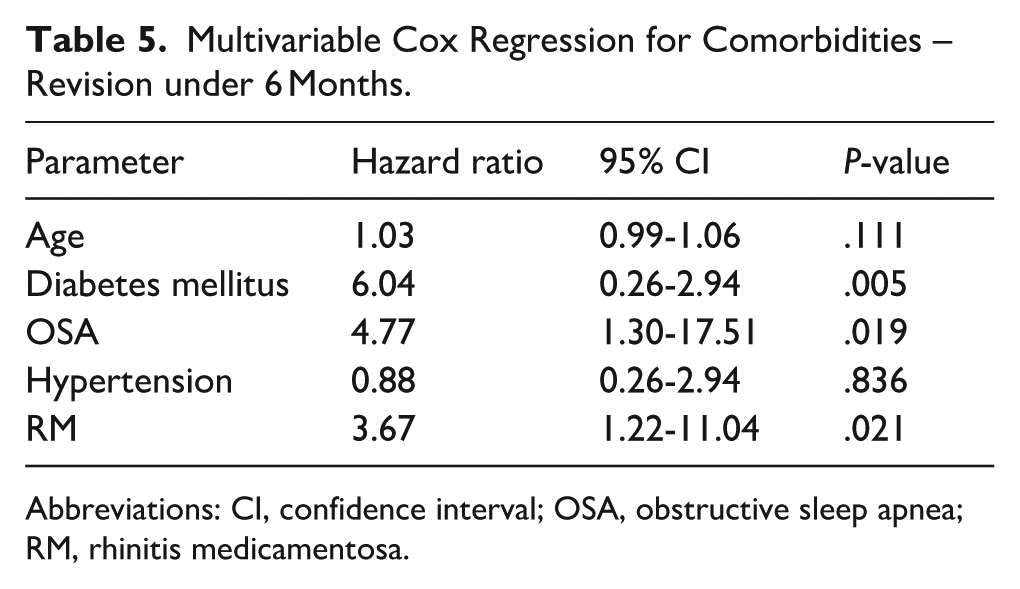
We further investigated predictors for the need for short-term revision (<6 months following the initial RFA procedure). Age remained significantly higher among patients who required short-term revision (median age: 62.0 [47.5-71.5]) than among those who required any revision compared to 35.0 [25.0-54.0] among those who did not (P < .001). Revision rates were higher among patients with medical comorbidities, with 11 of them (14%) requiring early revision versus 6 (3%) without any documented medical comorbidities (P = .001). Specific background medical conditions revealed higher early revision rates for DM and OSA, with 4 patients (40%) with DM and 4 patients (18%) with OSA requiring early revision versus 13 (5%) without DM and 13 (6%) without OSA (P < .001 and P = .012, respectively). Early revision rates were also higher for patients with RM, with 8 of them (15%) requiring early revision versus 9 non-RM patients (5%) (P = .005) (Table 4). Multivariate Cox regression analysis identified diabetes mellitus (HR 10.20, 95% CI 3.30-32.00, P < .001), OSA (HR 6.67, 95% CI 1.90-23.38, P = .003), and rhinitis medicamentosa (HR 4.79, 95% CI 1.67-13.77, P = .004) as independent predictors of short-term revision (Table 5).
Short-Term (<6 Months) Revision Rates Among Patients with versus those without Clinical Parameters (N = 260).
Abbreviations: CT, computed tomography; FESS, functional endoscopic sinus surgery; MRI, magnetic resonance imaging; OSA, obstructive sleep apnea. Categorical variables are described as N (%). Bold indicates significant.
Multivariable Cox Regression for Comorbidities – Revision under 6 Months.
Abbreviations: CI, confidence interval; OSA, obstructive sleep apnea; RM, rhinitis medicamentosa.
Predictors for Requiring Revision in the Long-Term (<24 Months)
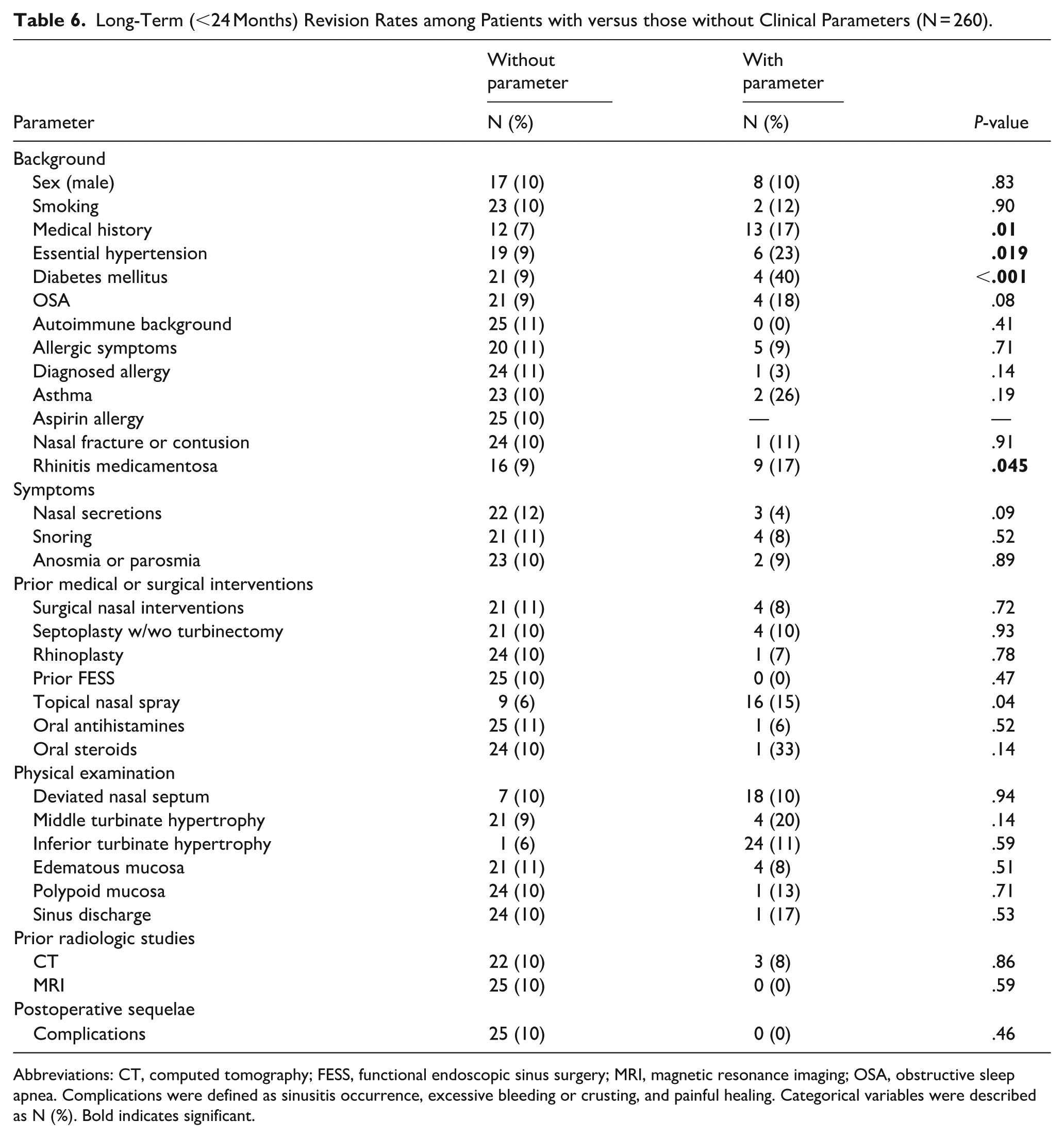
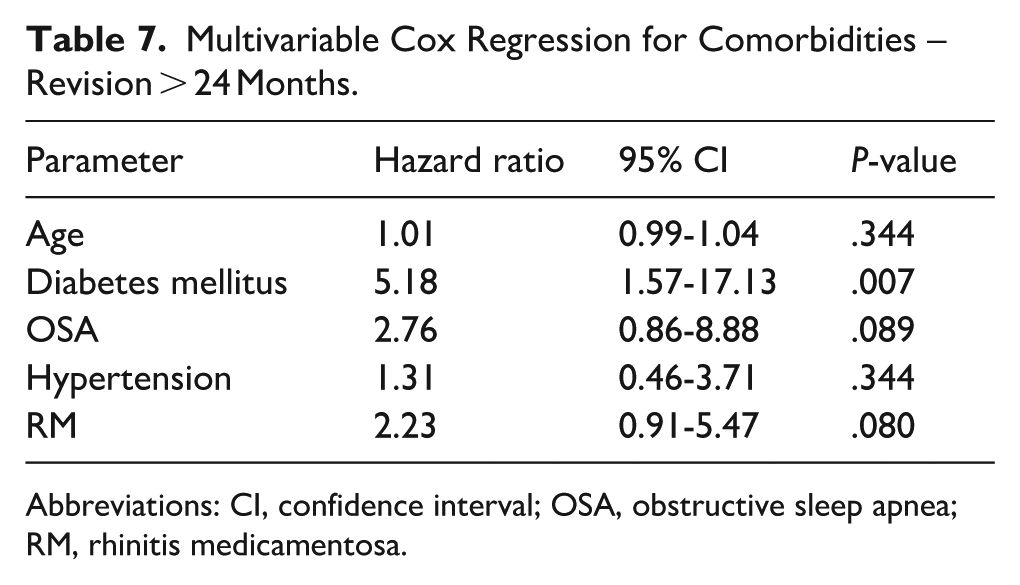
Similarly, we investigated predictors for revision among patients <24 months following initial RFA procedure and found that age was once again significantly higher among patients requiring long-term revision, with a median age of 57.0 (IQR: 32.5-70.0) vs 36.0 (IQR 25.0-54.0) who did not. The longer-term revision rates were also higher among patients with medical comorbidities: 13 patients (17%) with comorbidities versus 12 (7%) without (P = .01). Six patients (23%) with a background of essential HTN required revision throughout their long-term follow-up versus 19 patients (9%) without HTN who did not (P = .019). Similarly, patients with DM had higher revision rates (4 patients [40%] vs 21 patients [9%] without DM (P < .001). Revision rates were also higher among patients with RM (9 patients [17%] vs 16 patients [9%] without RM (P = .045) (Table 6). In multivariate Cox proportional hazards regression, diabetes mellitus (HR 7.47, 95% CI 2.50-22.10, P < .001), OSA (HR 3.39, 95% CI 1.10-10.46, P = .033), and rhinitis medicamentosa (HR 2.57, 95% CI 1.10-6.06, P = .030) remained independently associated with long-term revision (Table 7).
Long-Term (<24 Months) Revision Rates among Patients with versus those without Clinical Parameters (N = 260).
Abbreviations: CT, computed tomography; FESS, functional endoscopic sinus surgery; MRI, magnetic resonance imaging; OSA, obstructive sleep apnea. Complications were defined as sinusitis occurrence, excessive bleeding or crusting, and painful healing. Categorical variables were described as N (%). Bold indicates significant.
Multivariable Cox Regression for Comorbidities – Revision > 24 Months.
Abbreviations: CI, confidence interval; OSA, obstructive sleep apnea; RM, rhinitis medicamentosa.
Discussion
Our study describes the consequences of RFA failure and evaluates the feasibility and safety of revision RFA. Overall, 12.7% of patients required a revision procedure, and 9.2% of the entire cohort underwent revision RFA. Revision RFA was associated with sustained subjective patient satisfaction, a low rate of subsequent failure (with only 1 patient requiring surgical revision), and no procedure-related complications during long-term follow-up. Older age, diabetes mellitus (DM), and MTH were more common among patients requiring revision. In subgroup analyses, patients requiring short-term revision were older and more frequently had DM, OSA, and rhinitis medicamentosa (RM), whereas those requiring revision within 24 months more often had DM, HTN, RM, and older age compared with patients who did not require revision.
Chaudhry et al reported a comparable proportion of RFA failures, with 7% of patients ultimately requiring surgical intervention after initial RFA. Notably, most failures in that cohort were attributed to traumatic or anatomical abnormalities necessitating corrective surgery. 12 By contrast, revision RFA was offered as a treatment option in our cohort, and only 1 patient ultimately required surgical revision. While MTH emerged as a predictor of revision in our study, septal deviation was not significantly associated with failure. Differences in patient selection, treatment algorithms, and availability of revision RFA as an alternative to surgery may partly account for these findings.
Previous studies have suggested that the long-term efficacy of RFA may decline over time. Bakshi et al 4 reported gradual deterioration in nasal patency, with recurrence of symptoms approximately 1 year following the procedure. In our cohort, revision procedures occurred across a broad time frame, extending up to 5 years after the initial intervention, as illustrated in the Kaplan-Meier analysis (Figure 2). Despite this, most patients did not report persistent dissatisfaction during either clinical or telephonic follow-up, suggesting that symptom recurrence does not uniformly translate into perceived treatment failure.
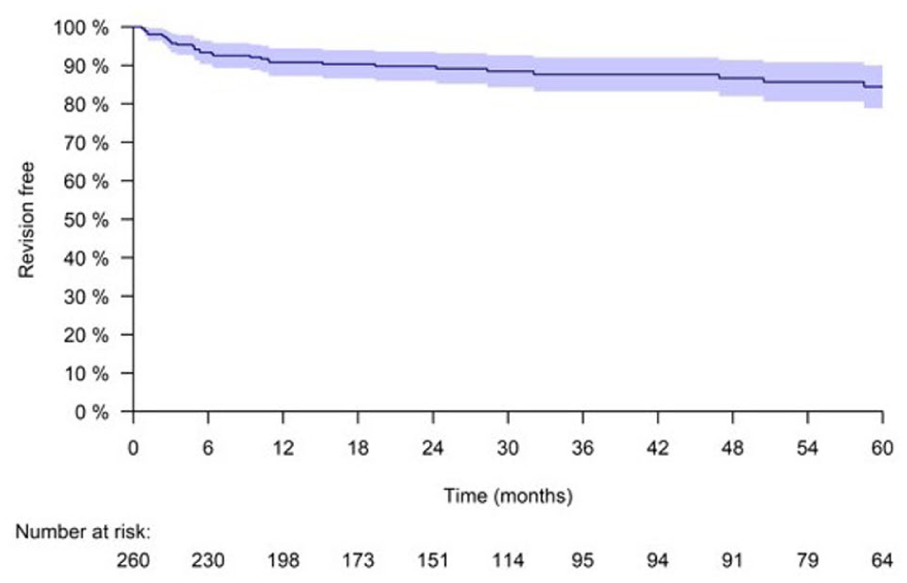
Kaplan-Meier curve of revision RFA events throughout 60 months of follow-up. RFA, radiofrequency ablation.
Anatomical factors have also been implicated in RFA outcomes. Harju et al 11 demonstrated differences in long-term success between mucosal-sparing and non-mucosal-sparing techniques and proposed anterior septal deviation as a contributor to failure by affecting the nasal valve area. Given that computed tomography (CT)- and cone-beam computed tomography (CBCT)-based studies have demonstrated a correlation between septal deviation severity and increased inferior turbinate volume, this selection criterion may have excluded a subset of patients with turbinate hypertrophy who could potentially benefit from RFA. 16
In our cohort, patients with severe anterior septal deviations were excluded from RFA a priori. Although patients with mild-to-moderate deviations were included, septal deviation was not associated with revision, whereas MTH remained a significant predictor. These findings suggest that turbinate-related rather than septal anatomical factors may play a more prominent role in RFA durability in appropriately selected patients.
Advanced age and medical comorbidities, particularly DM, were consistently associated with higher revision rates. Previous histopathological studies have demonstrated increased venous sinusoid content in hypertrophied inferior turbinates compared with normal mucosa.17,18 Age and DM have also been shown to influence sympathetic tone and microvascular regulation, which may affect turbinate volume and congestion dynamics.19,20 While these mechanisms may contribute to the observed associations, causal relationships cannot be established based on the present data.
Patients requiring revision were more likely to have received systemic corticosteroid therapy prior to intervention, which may reflect a higher overall burden of nasal disease. RM was a significant predictor of revision in both short- and longer-term analyses. This finding may indicate greater symptom sensitivity or lower tolerance to nasal obstruction among patients with RM, rather than reduced procedural efficacy, but further research focusing on patient tolerance and experience is needed to better establish this tendency. 21 Consistent with prior reports, allergy was not more prevalent among revision patients in our cohort, despite its known association with turbinate hypertrophy and mucosal regrowth. 22
Although imaging findings were used to screen for sinus conditions and assess the feasibility of RFA treatment, rather than being in the core of this study the present study, CT and CBCT have been shown to provide valuable information regarding ITH. Patients were referred to CT or CBCT according to their workup and clinical signs and symptoms, the majority of which were facial pain and purulent discharge, or to characterize their septal deviations. Studies have highlighted the correlation between turbinate hypertrophy and increased sinus mucosal lining, suggesting sinonasal disease. This contributed to our selection of patients who were referred to CT prior to surgical intervention. 23
Our study has several limitations that bear mention. It was carried out in a single tertiary center and on an urban population. All procedures and revision decisions were performed by a single, experienced fellowship-trained rhinology surgeon. Although this ensured procedural consistency and uniform clinical judgment, it introduced potential operator and selection bias. Decisions regarding revision treatment were based on mutual decision-making between the surgeon and the patient and were therefore influenced by subjective symptom burden, patient expectations, and clinician judgment. These factors may limit the generalizability of the findings. Since patient-reported outcome measurements were not included in the current study, we could not quantify the reported high level of satisfaction in the long-term follow-up. Not all follow-up assessments included routine endoscopic evaluation in asymptomatic patients. While postoperative follow-up was standardized, initially performed in the clinic and included endoscopic examination (at 2-6 months post-procedure), subsequent telephonic follow-up was used as an adjunct, and additional in-office examinations were conducted when symptoms recurred, or patients requested further evaluation. Therefore, subclinical endoscopic findings may have been missed in asymptomatic patients, although clinically relevant outcomes were captured.
Another major limitation of this study is the definition of treatment failure as a surgical failure or the need for an additional intervention. Surgical failure cases were not assessed by objective or validated outcome measures, such as NOSE or SNOT-22 questionnaires, peak nasal inspiratory flow, rhinomanometry, or standardized endoscopic grading. Instead, revision was determined through a shared decision-making process between patient and surgeon, reflecting subjective symptom burden and patient expectations. As a result, the definition of failure may be influenced by individual patient tolerance to symptoms and clinician judgment. Nevertheless, the requirement for revision treatment represents a clinically meaningful endpoint reflecting real-world decision-making in routine rhinology practice. Another limitation of this study is that some patients discontinued follow-up at our institution and may have undergone additional interventions at other clinics or hospitals. As a result, the reported revision rates may slightly underestimate the true incidence of revision treatment. However, given that our institution is a large tertiary referral center providing long-term care for a substantial proportion of patients with nasal obstruction, we do not believe that loss to follow-up was related to disease severity or medical complexity but rather occurred in a largely random manner. Importantly, telephonic follow-up in our cohort was conducted over the long term, and patients were routinely invited for in-office re-evaluation if recurrent or persistent symptoms were reported during these follow-up encounters.
Conclusion
Revision RFA of the inferior turbinate appears to be a safe and effective procedure with high patient satisfaction and no major complications. Patients with the medical comorbidities of OSA, DM and HTN, older age, and RM tended to require revisions more. An RFA revision procedure is recommended in older patients with medical comorbidities who are reluctant to undergo surgical procedures under general anesthesia, and it should be considered as an alternative to surgery for turbinate regrowth. Revision RFA may alleviate nasal symptoms and possibly contribute to adrenergic spray cessation in patients with lower tolerance to nasal obstruction, such as chronic users of decongestants, bearing in mind, however, that they also tend to fail RFA and more frequently require revisions. We recommend revision RFA for inferior turbinate regrowth as part of a more conservative approach to nasal obstruction in patients who have undergone gradual re-growth and who present with a prominent component of ITH.
Footnotes
Ethical Considerations
The study was approved by the Institutional Review Board (0367-18). Ethical approval was given by the institutional ethics committee – Helsinki Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Dataset available on request.*
Provenance and Peer Review
Not commissioned, externally peer reviewed.