
Abstract
Objective:
To compare the operative closure time and early postoperative outcomes between nasal septal retainer and trans-septal suturing techniques in patients undergoing septoplasty.
Methods:
This single-center, prospective, open-label, randomized controlled trial included patients aged 18 to 65 years with nasal obstruction. Participants were randomized to trans-septal suturing or nasal septal retainer after septoplasty. The primary outcome was operative closure time. Secondary outcomes included symptom burden assessed by visual analog scale (VAS) at 48 hours postoperatively, Sino-Nasal Outcome Test-22 (SNOT-22) scores at baseline, 1 week, and 3 months, and postoperative complications.
Results:
A total of 23 patients were randomized (11 to trans-septal suturing and 12 to nasal septal retainer). Baseline characteristics were comparable between groups. The mean closure time was significantly shorter in the septal retainer group than in the trans-septal suturing group (18.1 ± 1.5 seconds vs 763.3 ± 59.9 seconds; P < .001). The nasal septal retainer group reported significantly higher VAS scores for nasal obstruction (3.83 ± 1.34 vs 1.91 ± 1.04), facial pressure (2.33 ± 1.30 vs 0.27 ± 0.65), and dysphagia (2.14 ± 1.98 vs 0.00 ± 0.00) compared to the trans-septal suturing group (all P < .05). No significant differences were observed in SNOT-22 scores or complication rates during follow-up.
Conclusions:
The nasal septal retainer significantly reduced operative closure time compared with trans-septal suturing, with comparable safety profiles and similar patient-reported outcomes at 1 week and 3 months postoperatively, suggesting that it may serve as a reasonable and efficient alternative to trans-septal suturing in septoplasty.
Clinical Trial Registry identifier:
ChiCTR2300073690.
Introduction
Septoplasty is the most common surgical procedure performed by otolaryngologists to correct nasal septal deviation. 1 The procedure commonly starts with the formation of bilateral sub-perichondrial or sub-periosteal flaps, and then proceeds to the precise removal and restructuring of the misaligned cartilage and bone. 2 It is essential to reset and fix the separated mucoperiosteal and mucoperichondrial flaps and to eliminate the resulting dead space to prevent septal hematomas and facilitate optimal healing outcomes. Over the decades, the techniques employed to achieve this crucial objective have undergone significant evolution, reflecting advances in surgical practice and understanding.
The focus of postoperative management strategies for septoplasty varies. Nasal packing and trans-septal suture are the 2 most commonly used methods in clinical practice. Bilateral anterior nasal packing can significantly reduce the risk of postoperative bleeding and prevent the formation of adhesions. 3 However, nasal packing can obstruct nasal breathing and disrupt sleep rhythms, and increase facial pressure, consequently reducing the quality of life of patients.4,5 Moreover, packing removal might induce secondary bleeding and pain. 5 For the adverse events described above, the trans-septal suture has gained more preference and become a preferable alternative to packing. Trans-septal suture can partially preserve the perioperative nasal respiratory function of patients undergoing septoplasty and is more easily accepted by patients. 6 Despite the obvious superiority, placing sutures to reapproximate the mucosa in a narrow nose can be challenging. This procedure varies in duration, taking between 4 and 20 minutes, and has its own complications, including suture or needle breakage, small septal perforations from cutting needles, or trauma to the lateral nasal wall, potentially leading to synechiae formation. 7 Recently, the nasal septal retainer (Changzhou Innovate Medical Instrument & Technology Inc, Jiangsu, China) has been introduced (Figure 1). This retainer comprises 2 blades and 1 nut. When closed, the retainer applies mechanical pressure to the midline, thus compressing the nasal septal mucosa. The retainer is convenient to use, requiring less than 20 seconds to put in place, and may be left in the nasal cavity for 24 to 48 hours. A randomized study by Fang et al evaluated the safety and clinical efficacy of the retainer in septoplasty. 8 The authors found that the postoperative symptoms, such as headache, nasal obstruction, epiphora, and facial pressure, were significantly alleviated in patients using the retainer, compared to Merocel packing. However, the impact of the retainer on the operative time of closure after septoplasty has yet to be investigated.
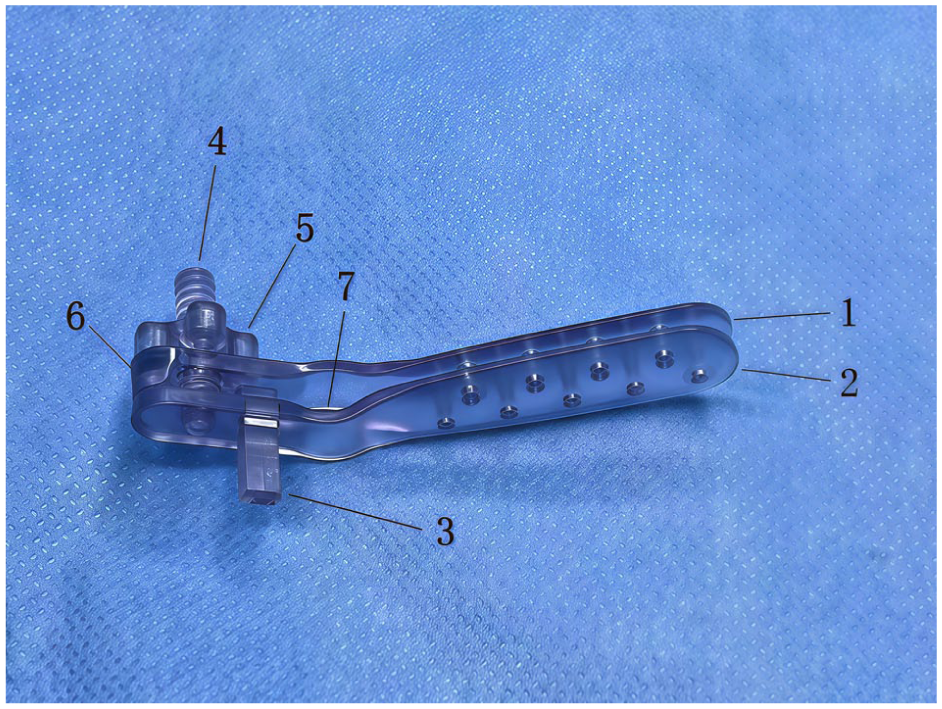
Actual photograph of a nasal septal retainer. 1. First blade; 2. Second blade; 3. Positioning post; 4. Screw; 5. Locking nut; 6. Pressure plate; and 7. Columella protection area.
The primary objective of this study is to compare the operative time of closure between the septal retainer and trans-septal suturing in septoplasty. In addition, as a secondary objective, this study aimed to compare the clinical effectiveness of the septal retainer group with trans-septal suturing.
Materials and Methods
Patients and Groups
This study was a single-center, prospective, open-label, randomized, controlled clinical study. The study protocol was approved by the Institutional Review Board of Shanghai East Hospital and registered at the Chinese Clinical Trial Registry (ChiCTR2300073690). Written informed consent was obtained from all participating patients. Patients aged 18 to 65 years, experiencing nasal obstruction, were enrolled in this study. Patients who had a history of previous septoplasty, allergy, asthma, concurrent sinusitis, or systemic diseases were excluded.
Sample Size Calculation
The sample size calculation and power analysis were meticulously conducted by researchers and statisticians on April 14, 2023, utilizing PASS 2024 (NCSS, LLC, Kaysville, Utah, USA). This analysis was grounded in the operational time findings from Sowerby and Wright’s study, 7 adhering to a significance level (α) of .05 and aiming for a robust target power of 95%. To adequately mitigate the constraints associated with power analysis and potential patient attrition, a balanced distribution was employed, allocating samples equally across 2 groups. Totally, this study necessitated to enroll 10 patients, with 5 participants in each group.
Intervention and Assessment
The patients were randomized 1:1 to either the trans-septal suturing group or the nasal septal retainer group. All surgical procedures were performed by a single senior otolaryngologist (Weihua Wang) to ensure consistency in surgical technique. Following septoplasty, the nasal septal retainer was strategically placed within the nasal septum. This involved careful adjustment of the columellar protection area and subsequent tightening of the retainer’s nut (Figure 2A). By contrast, trans-septal suturing involved the placement of 4 sutures, with their locations determined by the surgical needs and the extent of the mucosal separation (Figure 2B). The operative time of closure of septoplasty was recorded in the operating room. Researchers conducted nasal endoscopies and administered the Sino-Nasal Outcome Test-22 (SNOT-22) questionnaires at 3 key intervals: baseline, 1-week follow-up, and 3-month follow-up. In addition, Visual Analog Scale (VAS) scores were recorded as a measure of symptom burden at 48 hours after septoplasty. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
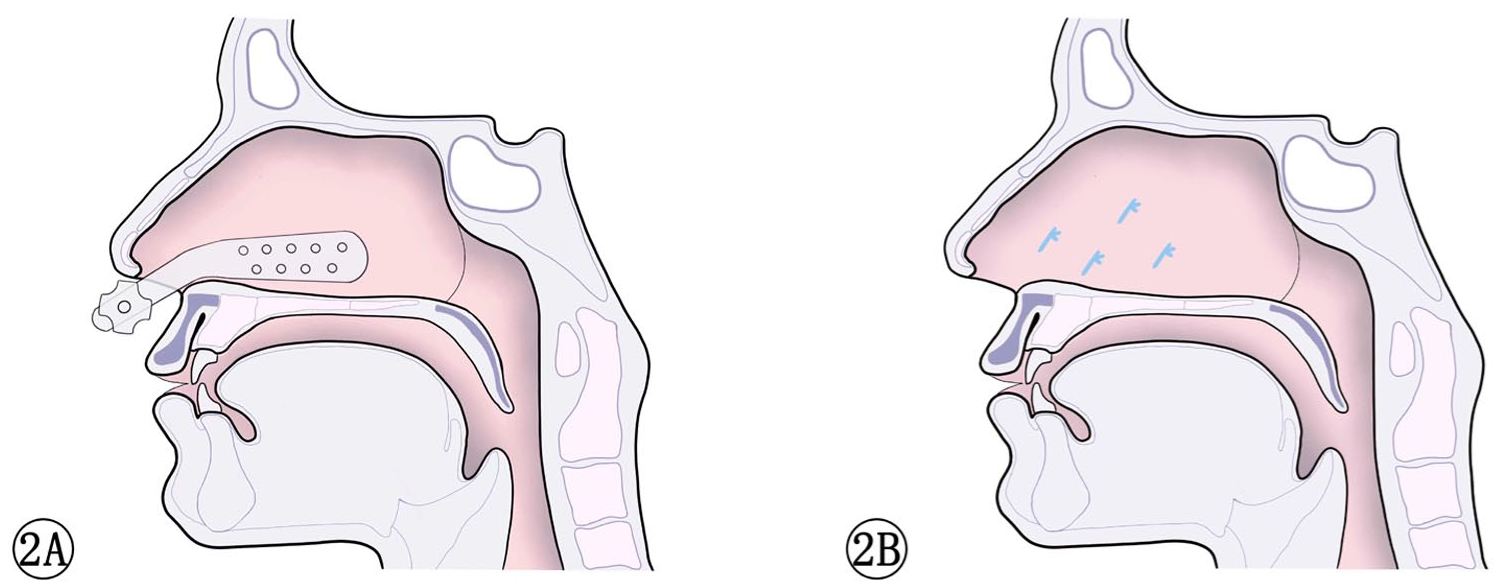
(A) Schematic illustration of nasal septal retainer application.
Statistical Analysis
This study employs an intention-to-treat analysis approach. All analyses were performed using SPSS version 27.0 (IBM Inc, Armonk, NY, USA). Data regarding baseline and follow-up demographic and outcomes were analyzed. Continuous variables are presented as mean (standard deviation) or median (interquartile range [IQR]). The median difference and 95% confidence interval were calculated using the Hodges-Lehmann method, which was applied to non-normally distributed variables. For variables conforming to a normal distribution, the Student’s t-test was utilized to evaluate the statistical significance of the differences observed between groups. Categorical variables are presented as frequency and percentage. All statistical tests were 2-sided, and P < .05 was considered statistically significant.
Results
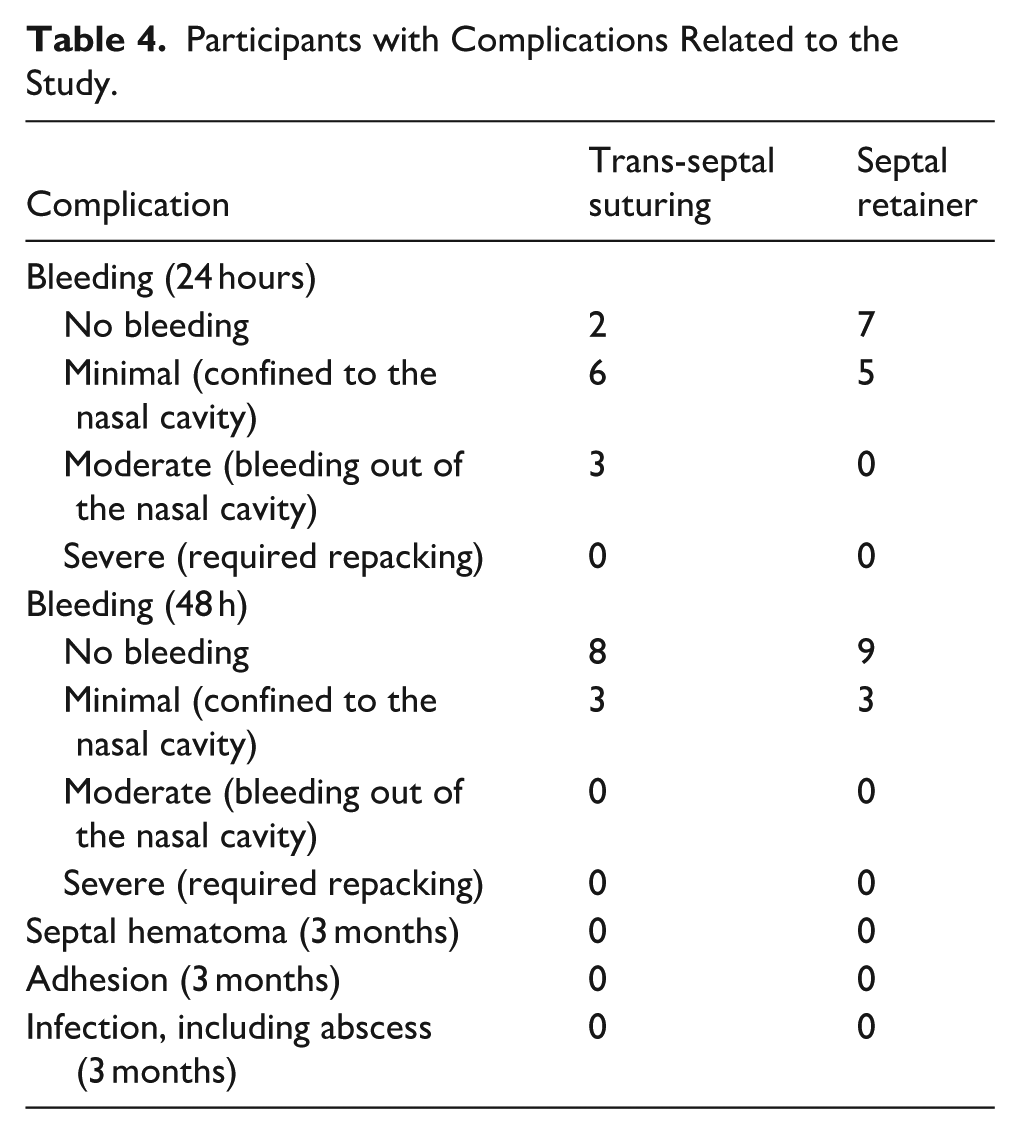
The flow of participants is shown in Figure 3. Between June 2023 and December 2024, 23 patients were randomized to undergo trans-septal suturing or nasal septal retainer after septoplasty. 69.6% patients were male (16) and 30.4% were female (7). The median (IQR) age of participants is 34 (29, 39) years. Table 1 depicts a comparison of the baseline demographic characteristics between the trans-septal suturing group and the nasal septal retainer group. There was no statistically significant difference in age, gender, and SNOT-22 scores between the 2 groups at baseline. The mean time for closure with septal retainer was 18.1 ± 1.5 seconds versus 763.3 ± 59.9 seconds for trans-septal suturing closure (P < .001; Table 2). The mean VAS scores of nasal obstructions (3.83 ± 1.34), facial pressure (2.33 ± 1.30), and dysphagia (2.14 ± 1.98) in the retainer group were significantly higher than in the trans-septal suturing group (1.91 ± 1.04, 0.27 ± 0.65, and 0.00 ± 0.00, respectively, P < .05; Table 3). There were no statistically significant differences in the SNOT-22 scores between the 2 groups at 1 week (5.67 ± 2.84, 5.09 ± 3.08, P = .646) and 3 months postoperatively (3.17 ± 1.53, 3.00 ± 2.10, P = .829). The incidence of postoperative nasal bleeding at both 24 and 48 hours, as well as the prevalence of adhesions and infections, is detailed in Table 4. There were no cases of severe bleeding in either group. During the use of trans-septal suturing or the septal retainer, no additional packing was required in either group to control bleeding. In addition, no cases of adhesion, infection, septal abscess, or septal hematoma were observed in the 3-month follow-up. Furthermore, no device-related mechanical failures, such as loosening of the nut or displacement of the retainer, were observed in the retainer group.
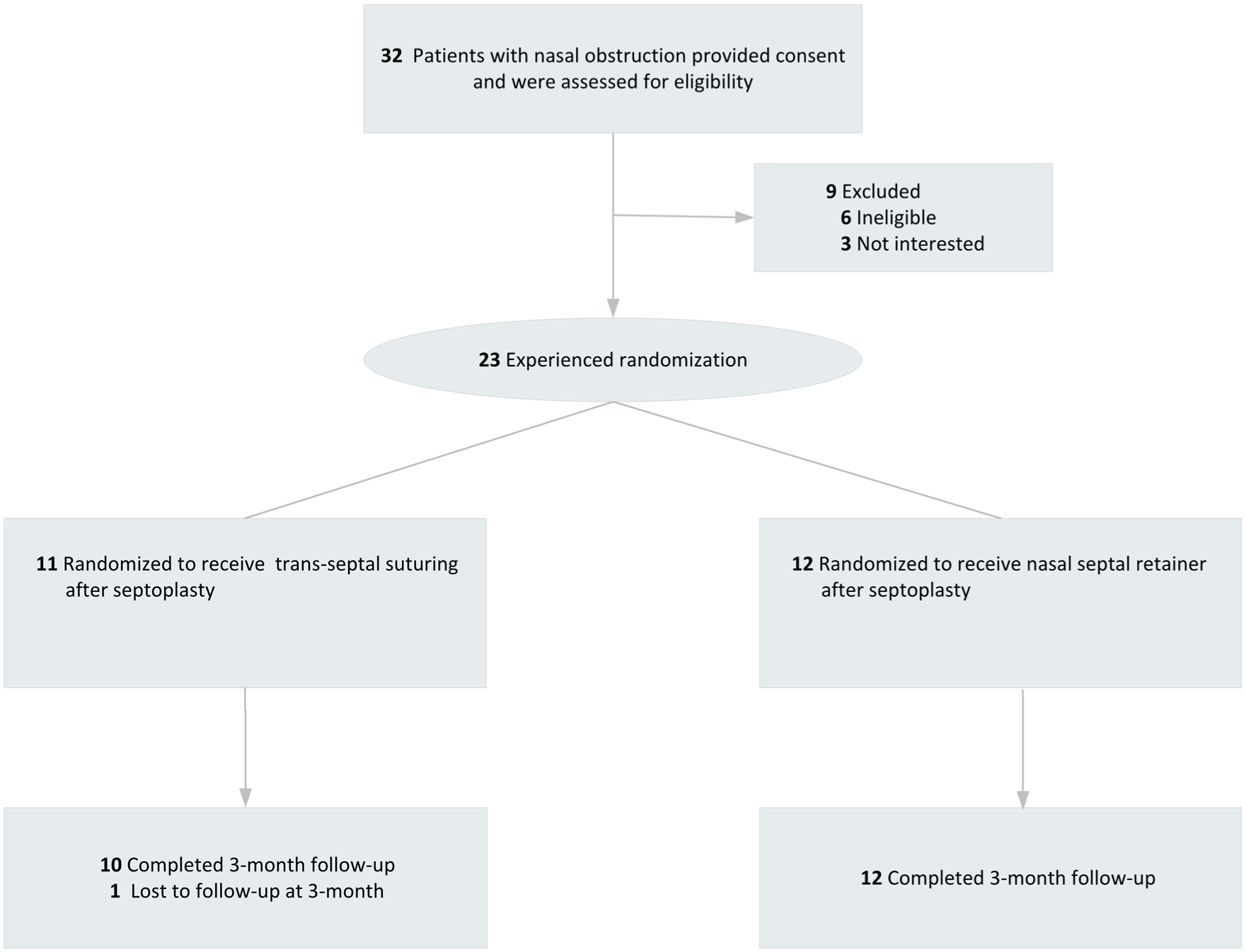
Flowchart of the study.
Baseline Characteristics of Trial Participants.
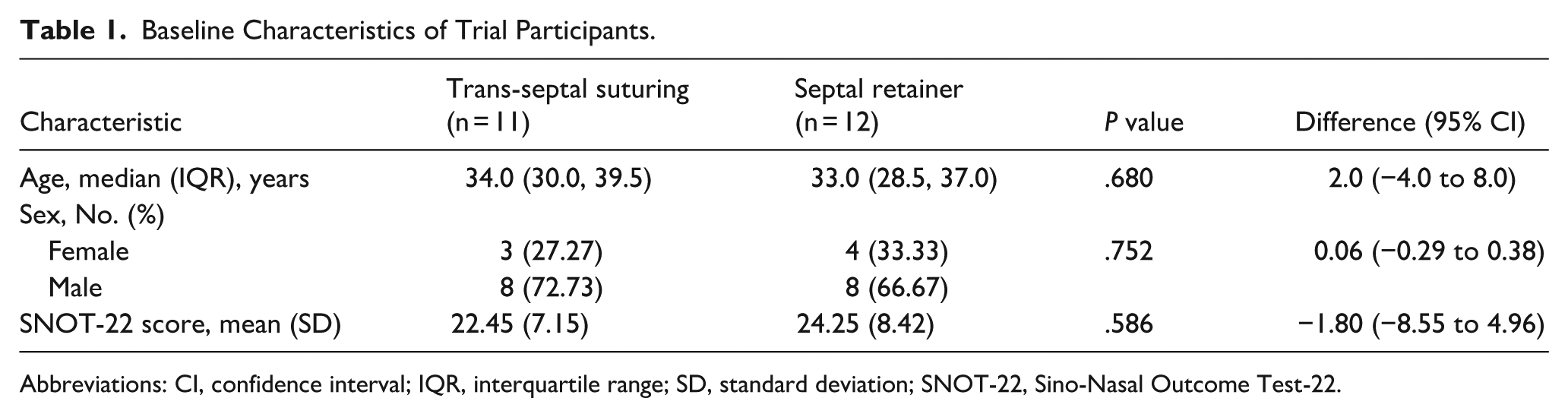
Abbreviations: CI, confidence interval; IQR, interquartile range; SD, standard deviation; SNOT-22, Sino-Nasal Outcome Test-22.
Operative Time of Closure for Trans-Septal Suturing and Septal Retainer Group.

Abbreviation: CI, confidence interval.
P < .05 indicates that the difference is statistically significant.
Visual Analog Scale Scores During the 24 Hours After Septoplasty.
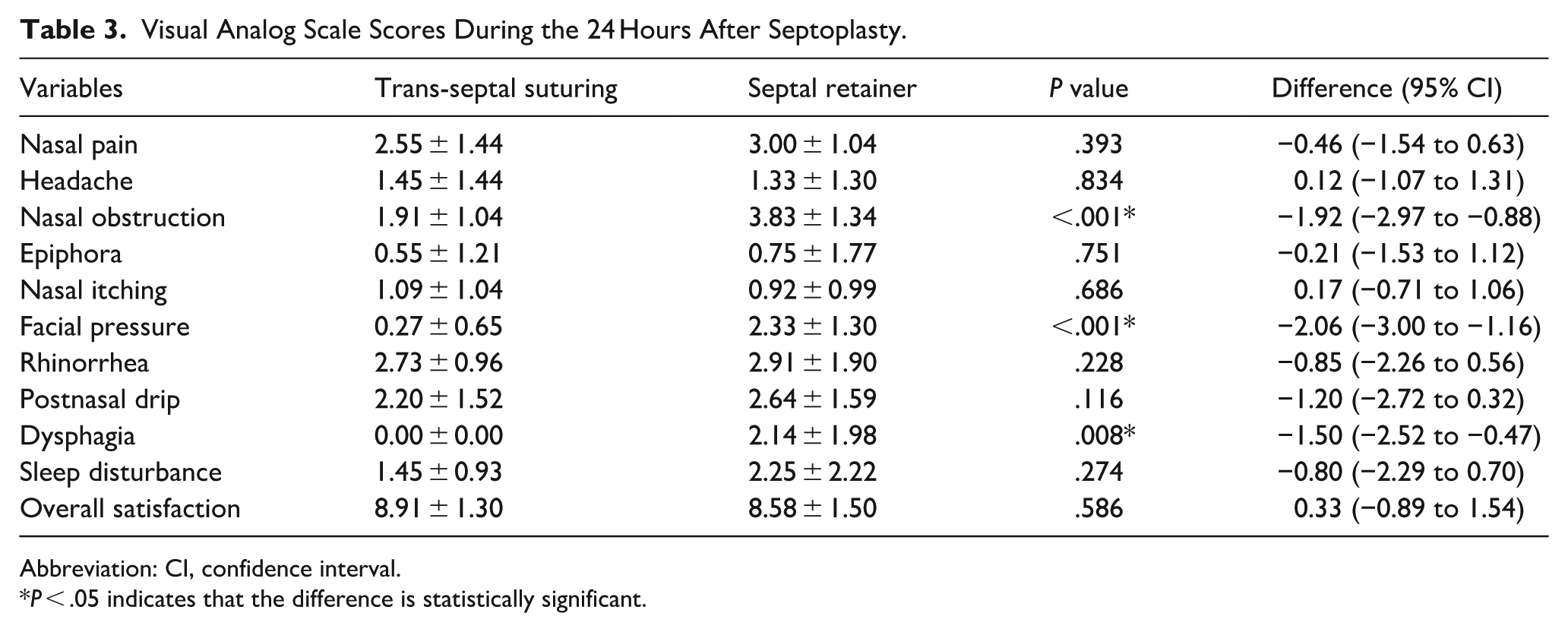
Abbreviation: CI, confidence interval.
P < .05 indicates that the difference is statistically significant.
Participants with Complications Related to the Study.
Discussion
Septoplasty, recognized as the principal surgical intervention for rectifying a deviated septum, is a prevalent practice in the realm of rhinology. Nasal obstruction and the related symptoms caused by septal deviation are the main indications for septoplasty. 9 Surgical intervention is more effective than non-surgical methods for nasal obstruction. 10 In recent years, there has been a sustained and growing focus on the management of post-septoplasty. To our knowledge, this is the first study to quantitatively evaluate the time-saving benefits of using a nasal septal retainer versus trans-septal suturing.
In this study, the use of a septal retainer can significantly reduce the operative time of closure post-septoplasty. Our data showed that the average time for trans-septal suturing was 763.3 ± 59.9 seconds, while the average time for placing a septal retainer was 18.1 ± 1.5 seconds, resulting in a significant time saving of approximately 12 minutes. To reduce operation time, scholars have designed nasal septum suturing devices. Kubok et al found that the average operation time using suturing devices was 299.8 ± 33.7 seconds. 11 Sowerby and Wright compared the operation time between a septal stapler and trans-septal suturing. They found that the operative time of closure for the septal stapler was 35 ± 22 seconds. 7 Consequently, it becomes apparent that the septal retainer is the most time-efficient option when compared to other techniques mentioned above. From a cost perspective, the nasal septal retainer (approximately $89 USD) entails a higher material cost compared to standard absorbable suture material (approximately $10 USD). However, the significant reduction in operative time (mean reduction of ~12 minutes) may offset this direct cost by optimizing operating room utilization. Future studies, including a formal cost-effectiveness analysis, are warranted. It is worth mentioning that the septal retainer is suitable for otolaryngologists of different levels, as it only takes a short time of training to master its use. By contrast, trans-septal suturing in the narrow nasal cavity, which requires repeated threading and suturing to ensure good adhesion of the separated nasal septal mucosa, can be time-consuming.
Irrespective of the postoperative management approach adopted, the symptom burden and quality of life within the initial 48 hours post-surgery are of critical significance for the patient. In this study, patients in the nasal septal retainer group had higher average scores for postoperative nasal congestion, facial pressure, and dysphagia than the mucosal suturing group. Although the application of the nasal septal retainer preserves a certain amount of ventilation space in the nasal cavity, the volume of the retainer itself occupies a small space in the nasal cavity, leading to a higher nasal congestion score 24 hours postoperatively compared to the trans-septal suturing group. Facial pressure associated with the use of a nasal septal retainer may be attributed to the tightening of the locking nuts. Therefore, postoperative adjustment of the locking nuts’ tightness, guided by patient feedback and observation of the nasal columella skin color, is essential. Dysphagia related to the retainer may arise from nasal obstruction, impaired movement of the soft palate, and disrupted temporal coordination between respiration and swallowing.12 -14 Sari et al used the EAT-10 questionnaire and VAS scores to evaluate the function of swallowing after nasal septoplasty in patients with trans-septal suturing, Merocel tampons, and Doyle silicone splints, respectively. The trans-septal suture group had significantly lower EAT-10 and VAS scores on the second postoperative day than the Merocel packing and silicone packing groups. 15 Future studies should employ validated dysphagia questionnaires to conduct randomized controlled trials, assessing the impact of nasal septal retainer on swallowing function.
Limitation
This study still has several limitations. First, while the sample size was adequate to validate the primary outcomes, the absence of significant differences in complications, including bleeding, adhesions, and infections, should be interpreted with caution. Second, the study’s demographic was limited to a single ethnic group, highlighting the need for future research to extend to international multicenter randomized controlled trials that encompass a more ethnically diverse participant base. Lastly, the reliance on subjective questionnaires for postoperative evaluation underscores the importance of integrating objective measures to reduce assessment bias. Future large-scale studies are warranted not only to confirm safety profiles but also to evaluate long-term recurrence rates of septal deviation to compare the structural integrity maintained by the retainer versus suturing.
Conclusion
In summary, our study suggested that applying a nasal septal retainer can significantly reduce the operative time for closure in septoplasty when compared to trans-septal suturing. Although higher short-term scores for nasal obstruction, facial pressure, and dysphagia were observed in the retainer group, no significant differences were found in patient-reported outcomes at 1 week and 3 months postoperatively. These findings suggest that the nasal septal retainer may serve as a safe, efficient, and technically feasible alternative to trans-septal suturing in septoplasty.
Footnotes
Acknowledgements
The authors sincerely thank all the patients who participated in this study for their valuable contributions to medical research.
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board of Shanghai East Hospital, Tongji University School of Medicine (Approval No.: 2023-052).
Consent to Participate
Written informed consent was obtained from all participants prior to enrollment. All procedures were performed in accordance with the Declaration of Helsinki.
Author Contributions
Weihua Wang conceptualized and designed the study. Chao Wang and Liyun Ying conducted a clinic follow-up and statistical analysis. Chao Wang drafted the initial manuscript. Weihua Wang reviewed and modified the manuscript. All authors take responsibility for the appropriateness of the content.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Shanghai Pudong New Area Health Commission (Grant Number: PW2023A-46) and Shanghai Municipal Health Commission Clinical Research Special Project (Grant Number: 202150005).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. Individual participant data are de-identified to protect patient privacy.
Trial Registration
This trial was registered in the Chinese Clinical Trial Registry (ChiCTR), registration number ChiCTR2300073690, registered on July 15, 2023.